[ad_1]
A calorie is not a calorie. It isn’t only what you eat, but when you eat.
Mice are nocturnal creatures. They eat during the night and sleep during the day. However, if you only feed mice during the day, they gain more weight than if they were fed a similar amount of calories at night. Same food and about the same amount of food, but different weight outcomes, as you can see in the graph below and at 0:18 in my video Eat More Calories in the Morning to Lose Weight, suggesting that eating at the “wrong” time may lead to disproportionate weight gain. In humans, the wrong time would presumably mean eating at night.
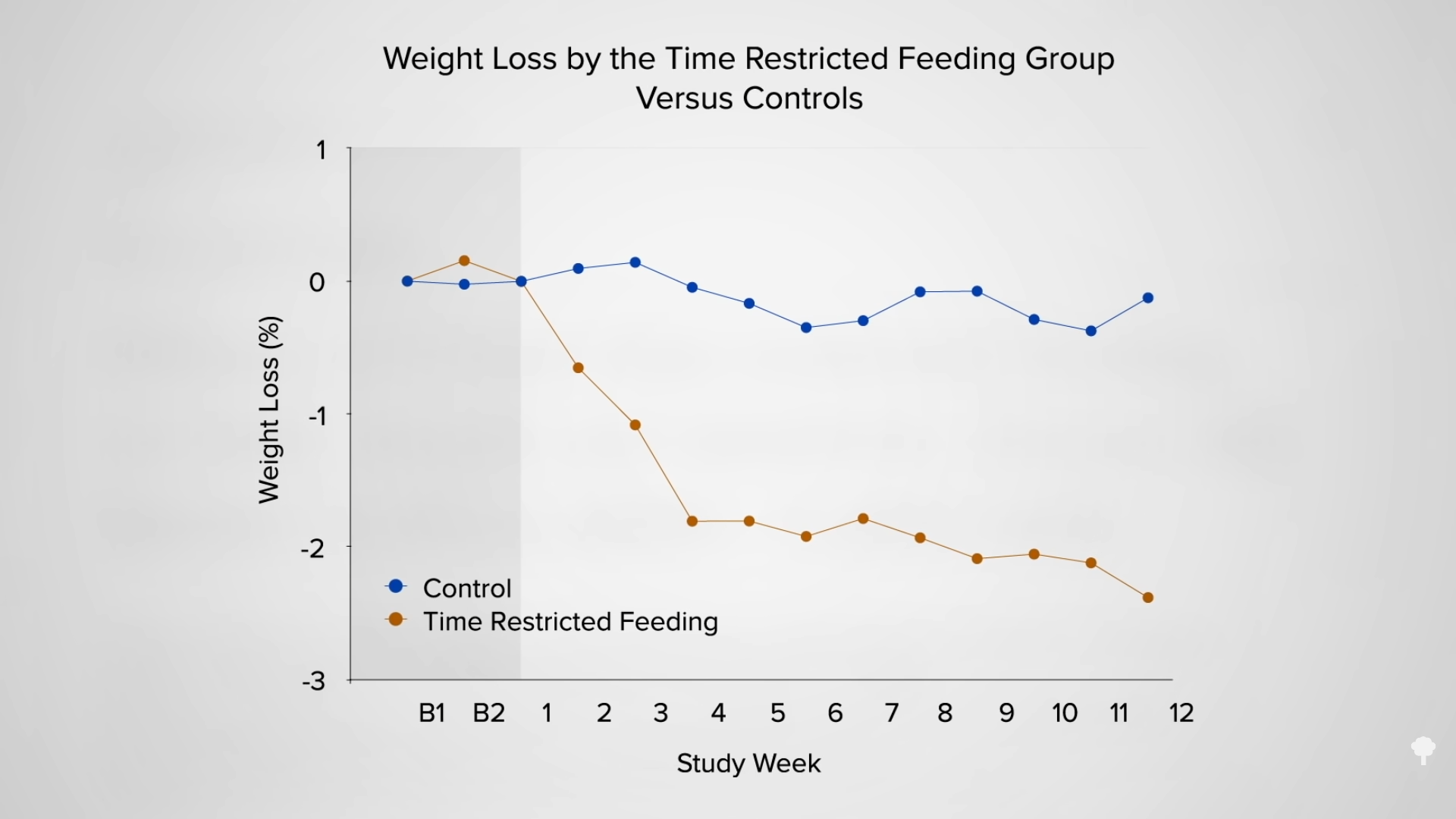
Recommendations for weight management often include advice to limit nighttime food consumption, but this was largely anecdotal until it was first studied experimentally in 2013. Researchers instructed a group of young men not to eat after 7:00 pm for two weeks. Compared to a control period during which they continued their regular habits, they ended up about two pounds lighter after the night-eating restriction. This is not surprising, given that dietary records show the study participants inadvertently ate fewer calories during that time. To see if timing has metabolic effects beyond just foreclosing eating opportunities, you’d have to force people to eat the same amount of the same food, but at different times of the day. The U.S. Army stepped forward to carry out just such an investigation.
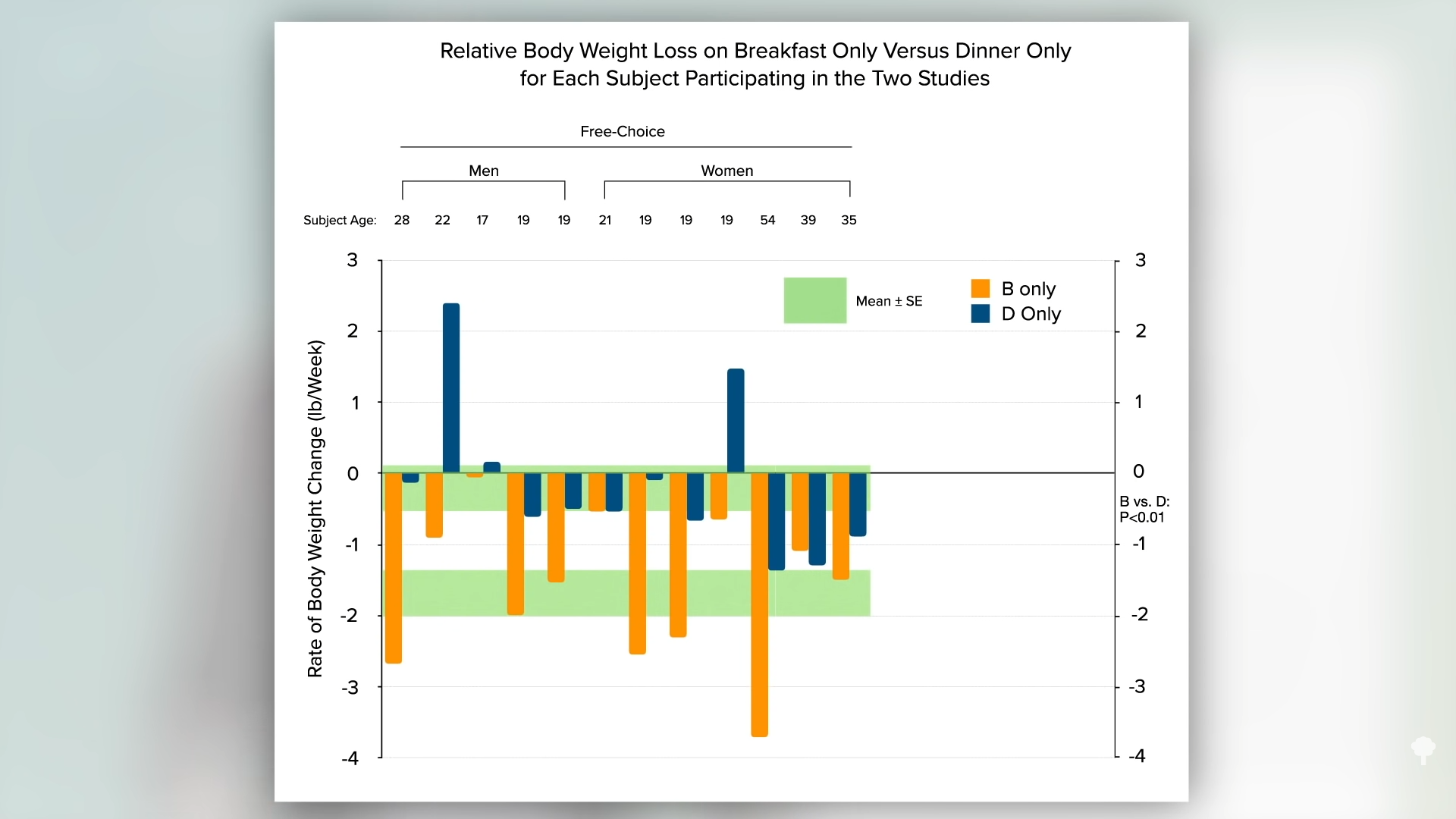
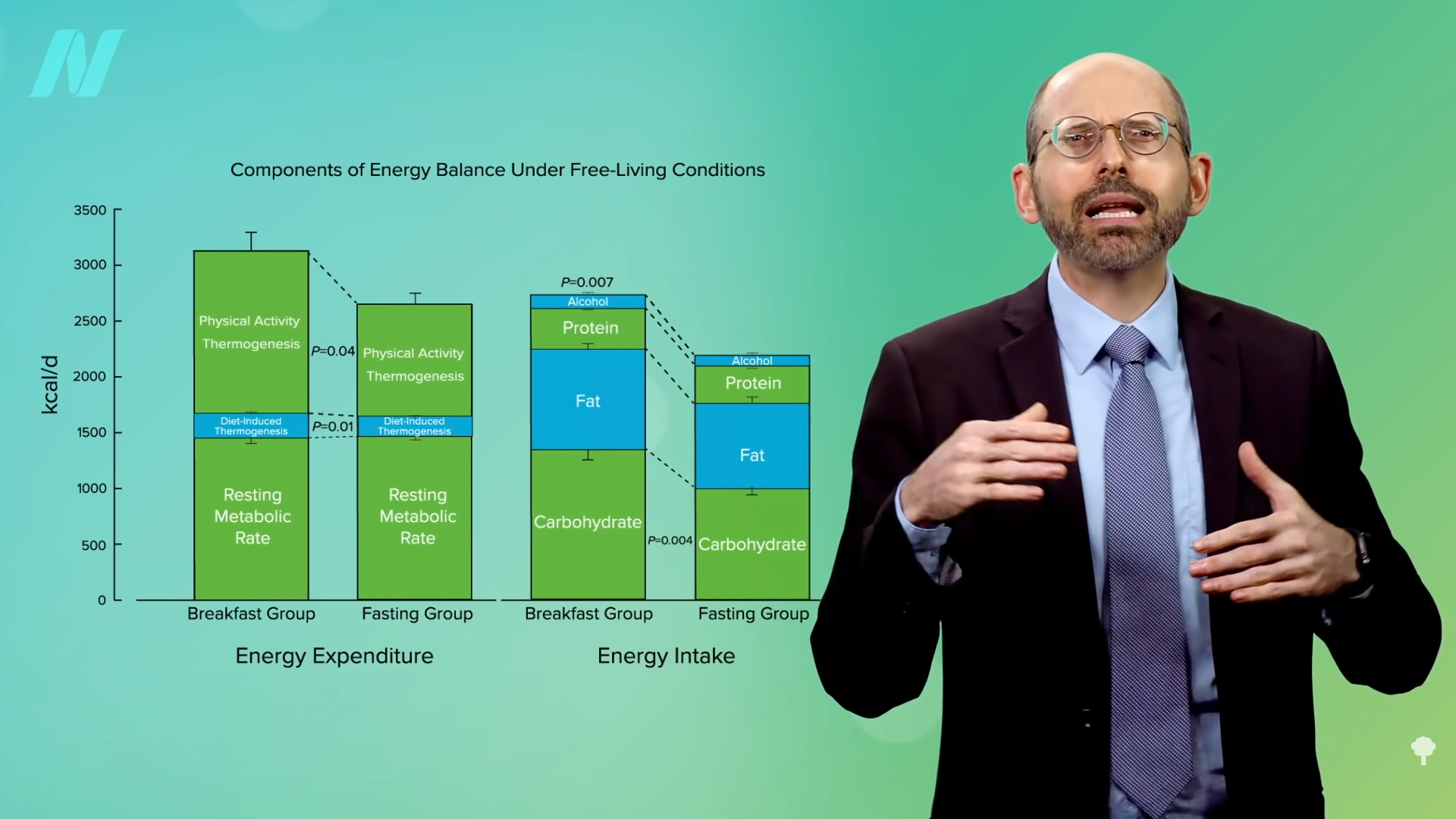
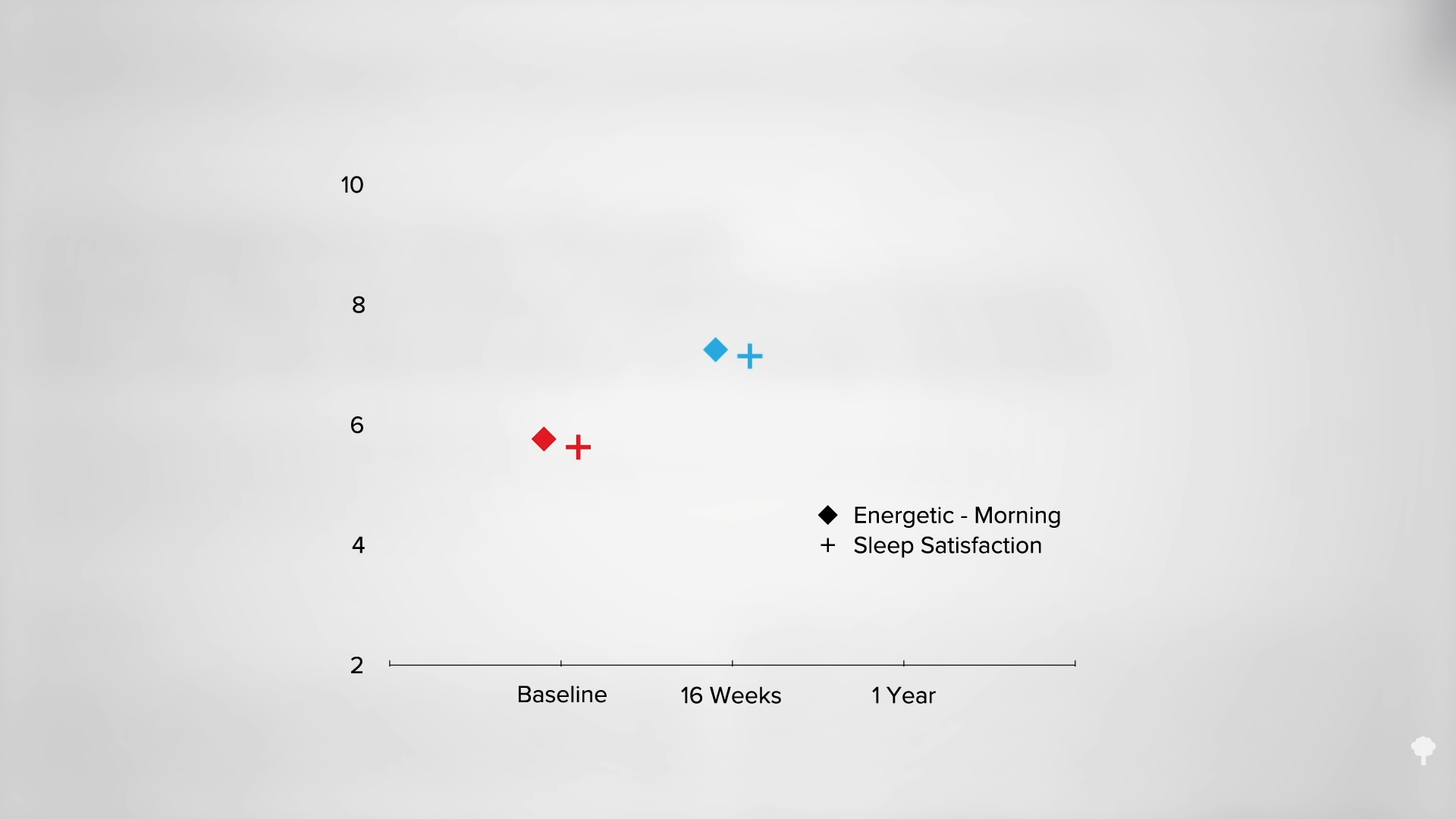
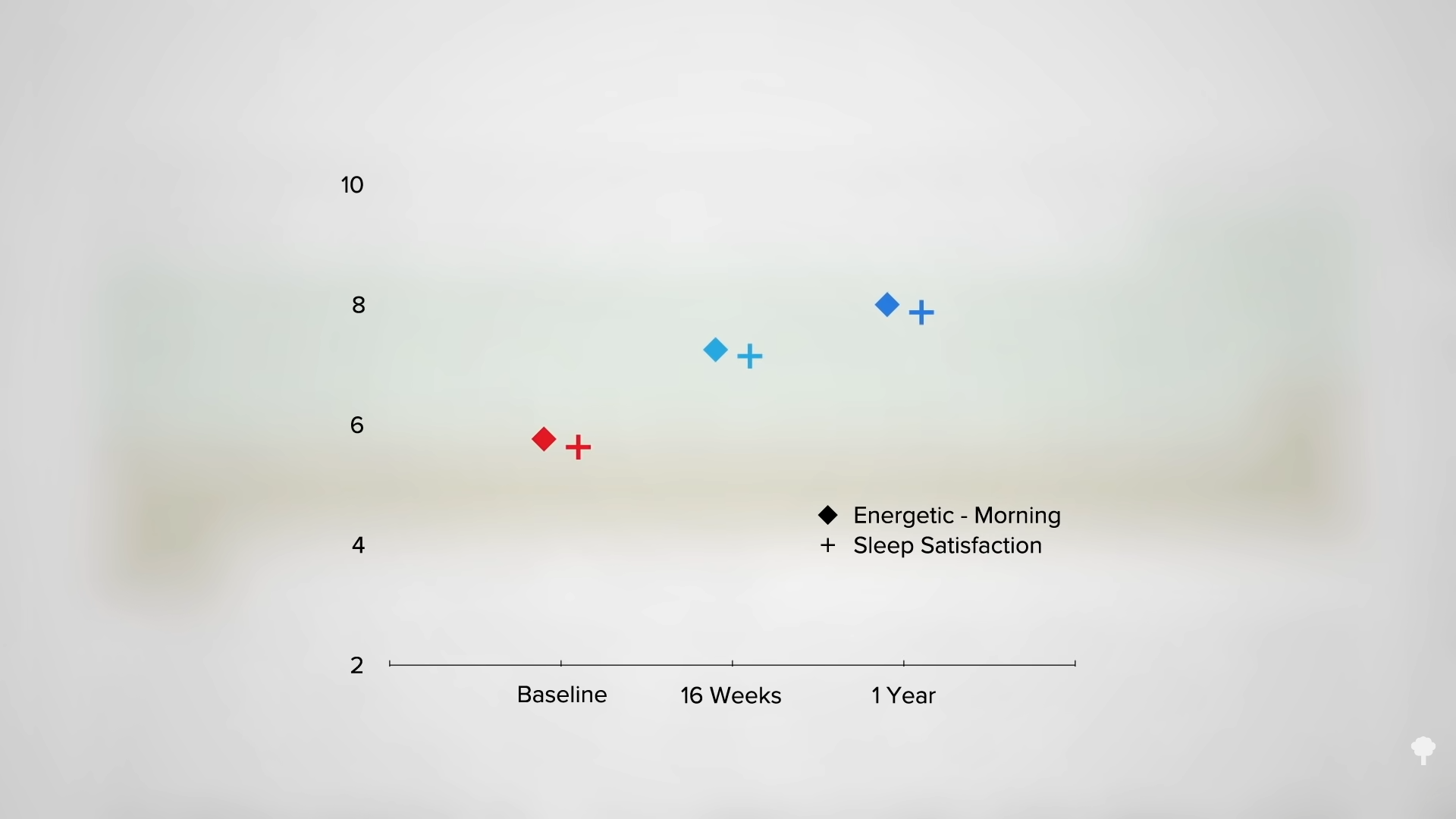
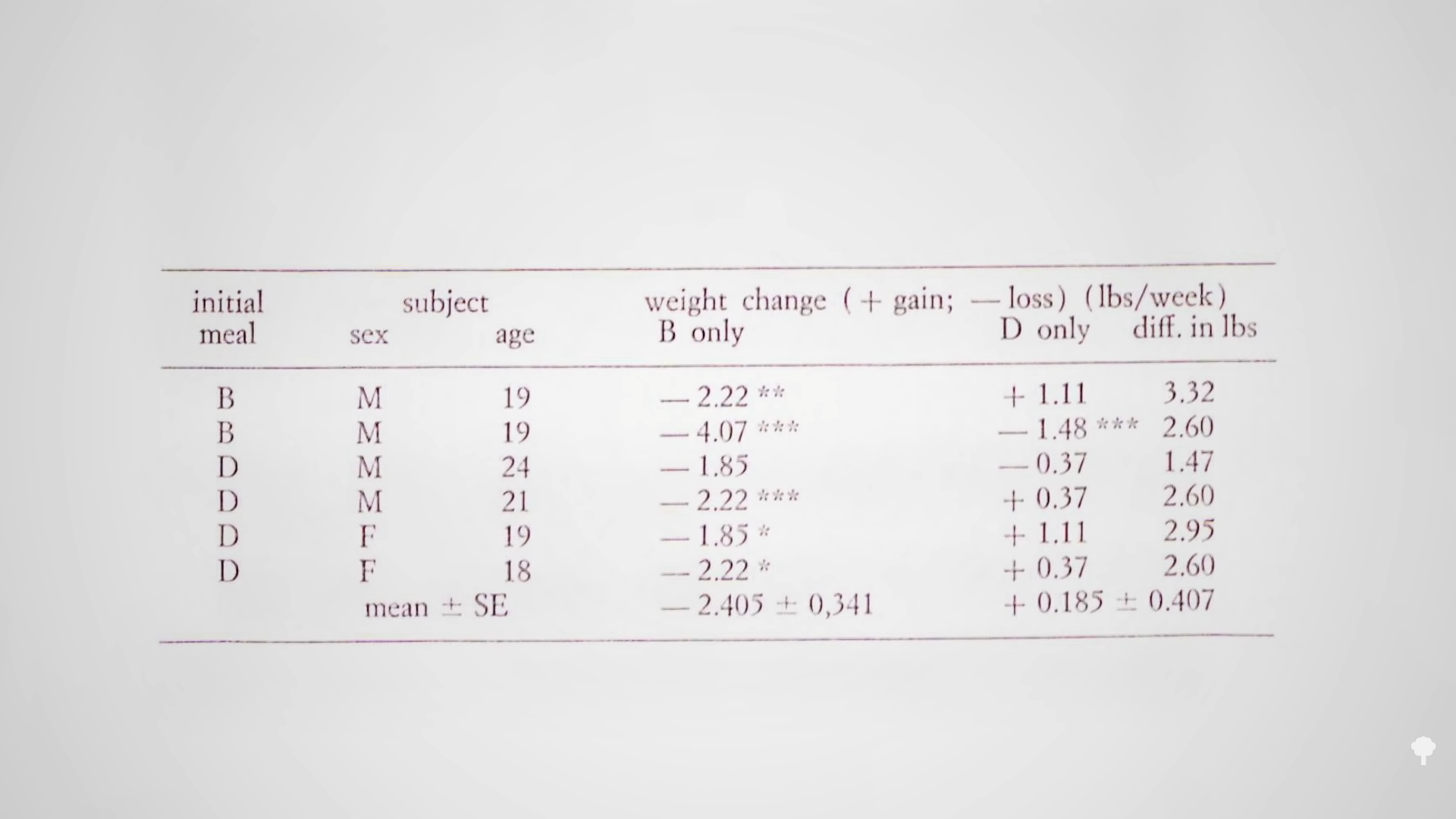
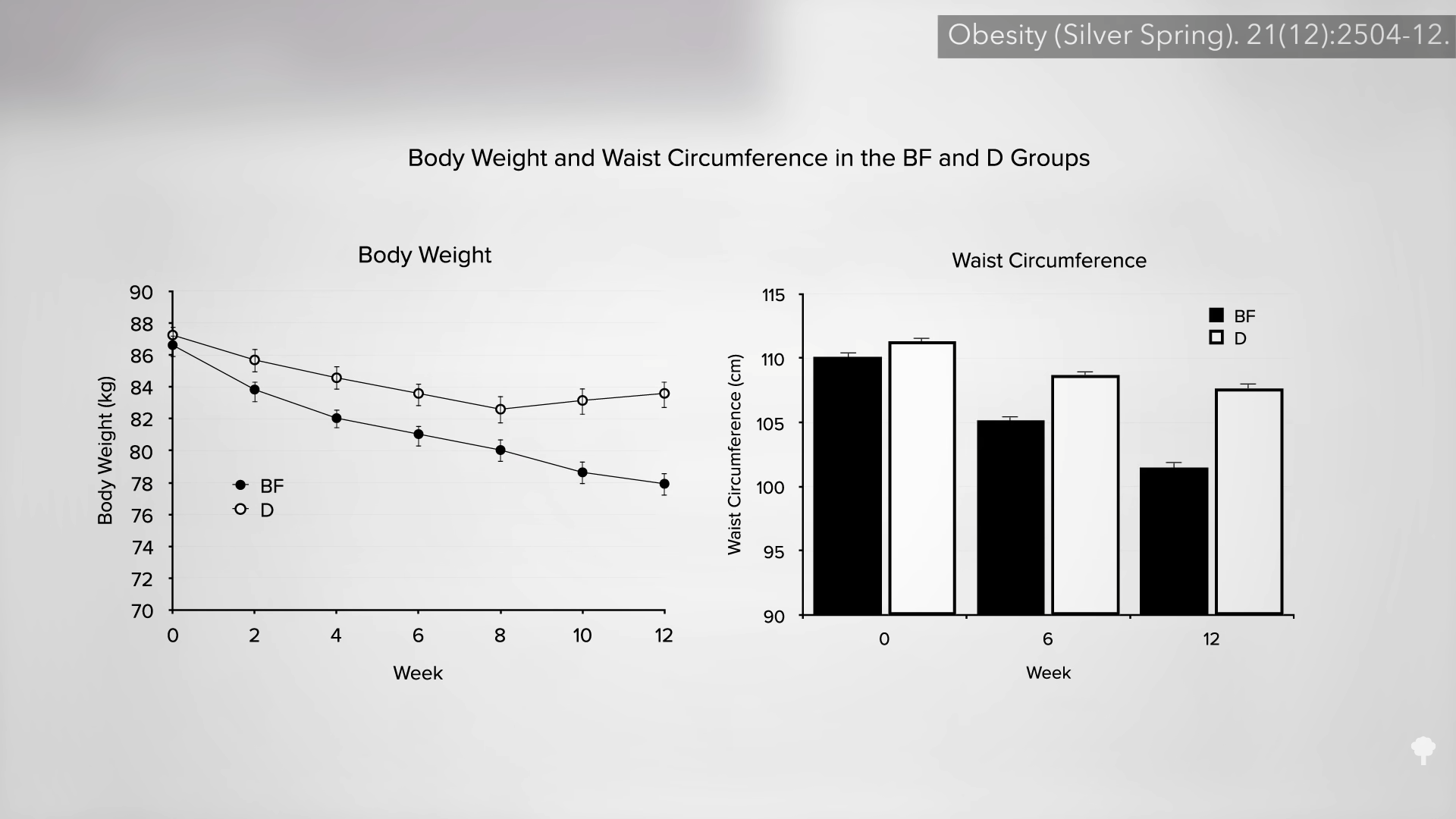
In their first set of experiments, Army researchers had people eat a single meal a day either as breakfast or dinner. The results clearly showed the breakfast group lost more weight, as you can see in the graph below and at 1:35 in my video. When study participants ate only once a day at dinner, their weight didn’t change much, but when they ate once a day at breakfast, they lost about two pounds a week.
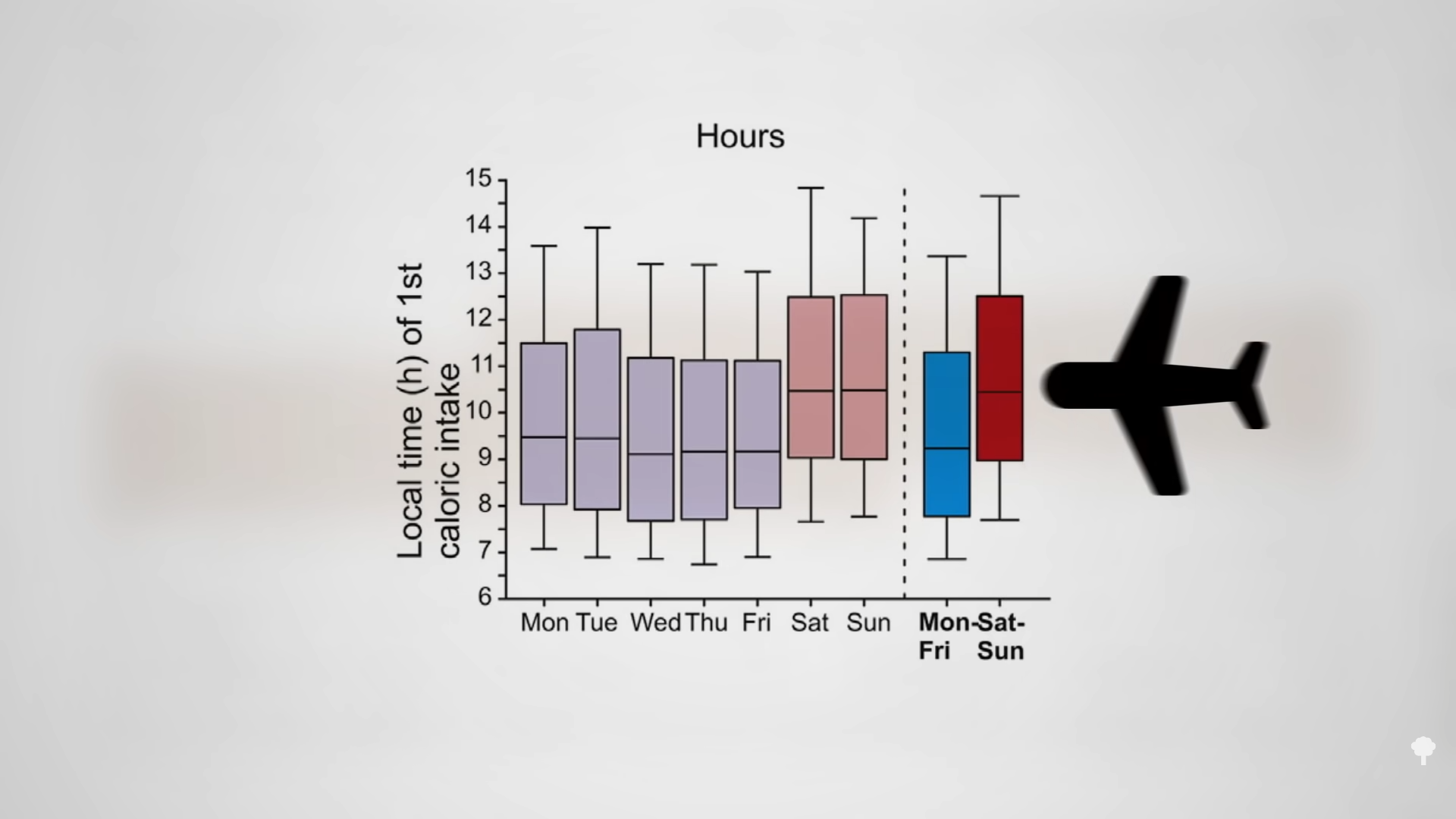
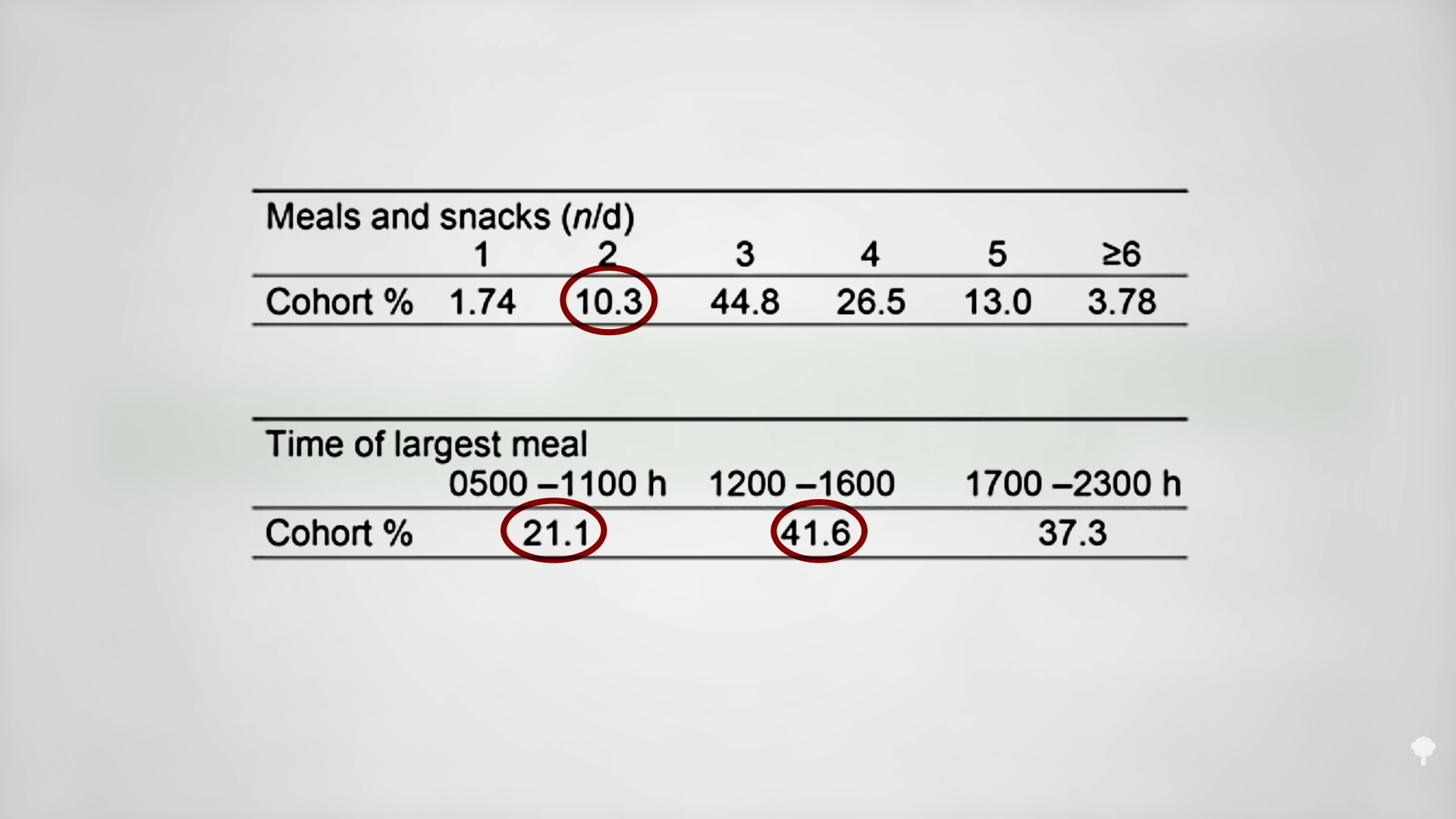
Similar to the night-eating restriction study, this is to be expected, given that people tend to be hungrier in the evening. Think about it. If you went nine hours without eating during the day, you’d be famished, but people go nine hours without eating overnight all the time and don’t wake up ravenous. There is a natural circadian rhythm to hunger that peaks around 8:00 pm and drops to its lowest level around 8:00 am, as you can see in the graph below and at 2:09 in my video. That may be why breakfast is typically the smallest meal of the day.
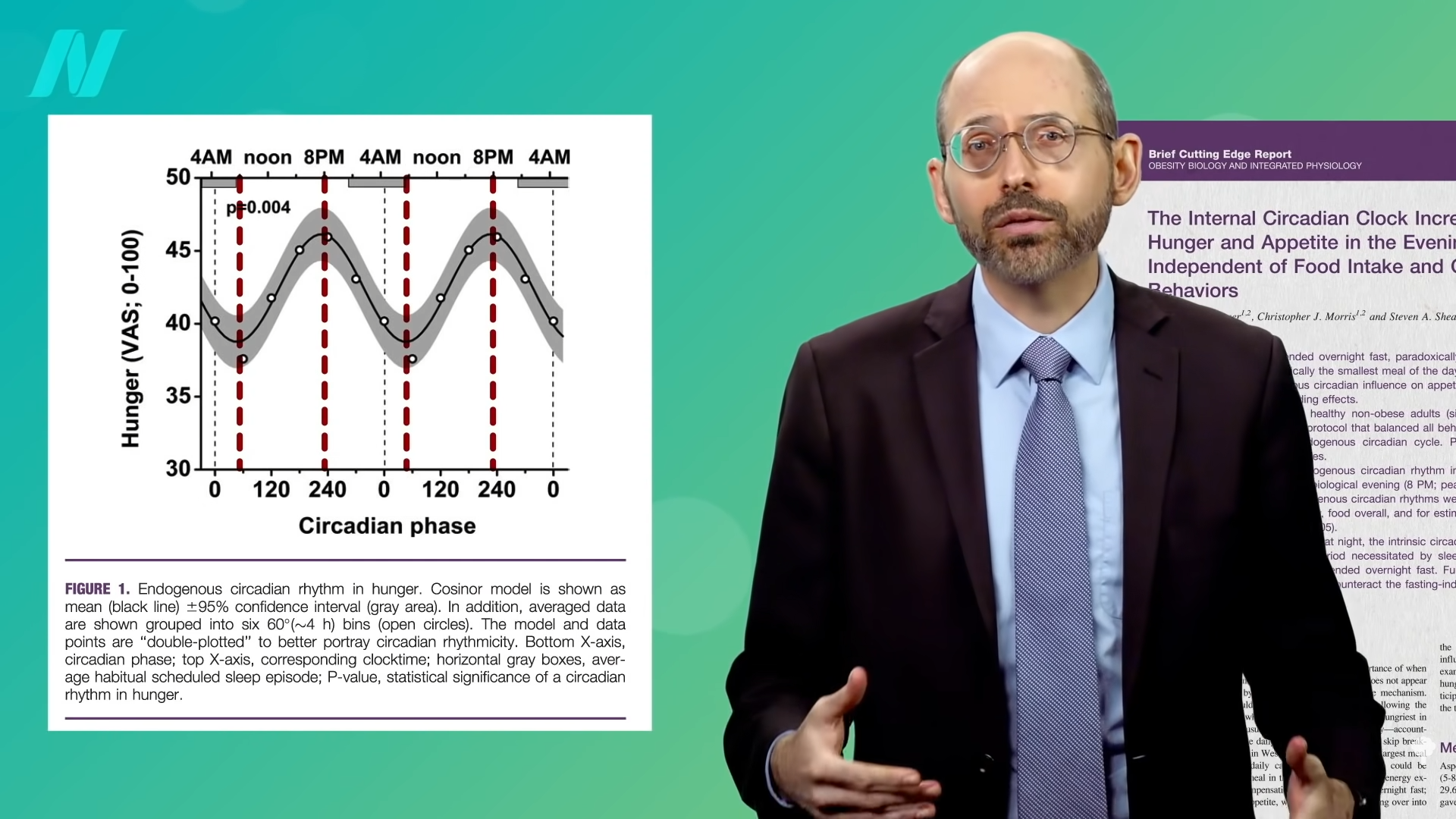
The circadian rhythm of our appetite isn’t just behavioral, but biological, too. It’s not just that we’re hungrier in the evening because we’ve been running around all day. If you stayed up all night and slept all day, you’d still be hungriest when you woke up that evening. To untangle the factors, scientists used what’s called a “forced desynchrony” protocol. Study participants stayed in a room without windows in constant, unchanging, dim light and slept in staggered 20-hour cycles to totally scramble them up. This went on for more than a week, so the subjects ended up eating and sleeping at different times throughout all phases of the day. Then, the researchers could see if cyclical phenomena are truly based on internal clocks or just a consequence of what you happen to be doing at the time.
For instance, there is a daily swing in our core body temperature, blood pressure, hormone production, digestion, immune activity, and almost everything else, but let’s use temperature as an example. As you can see in the graph below and at 3:21 in my video, our body temperature usually bottoms out around 4:00 am, dropping from 98.6°F (37°C) down to more like 97.6°F (36.4°C). Is this just because our body cools down as we sleep? No. By keeping people awake and busy for 24 hours straight, it can be shown experimentally that it happens at about the same time no matter what. It’s part of our circadian rhythm, just like our appetite. It makes sense, then, if you are only eating one meal per day and want to lose weight, you’d want to eat in the morning when your hunger hormones are at their lowest level. 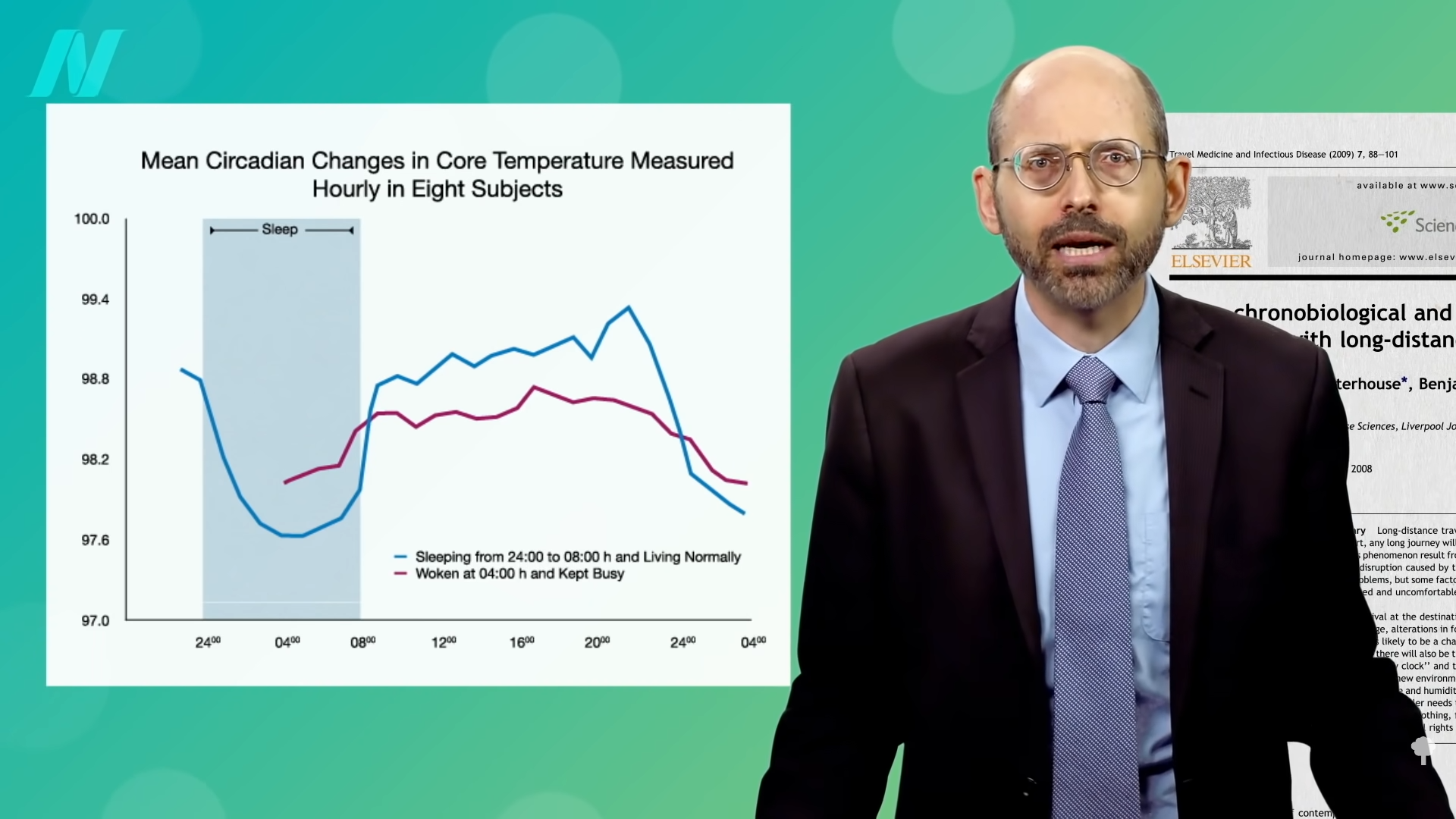
Sounds reasonable, but it starts to get weird.
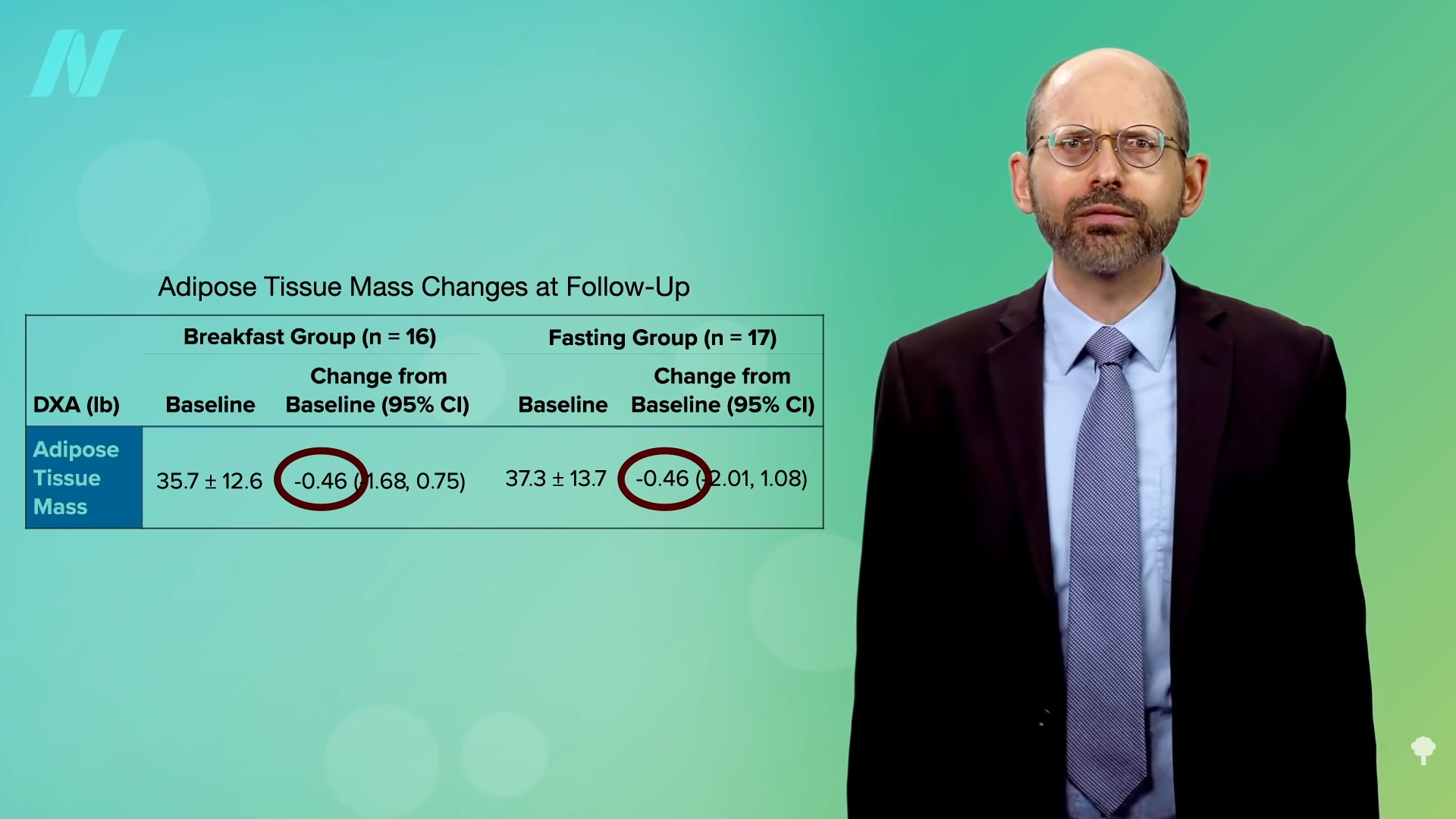
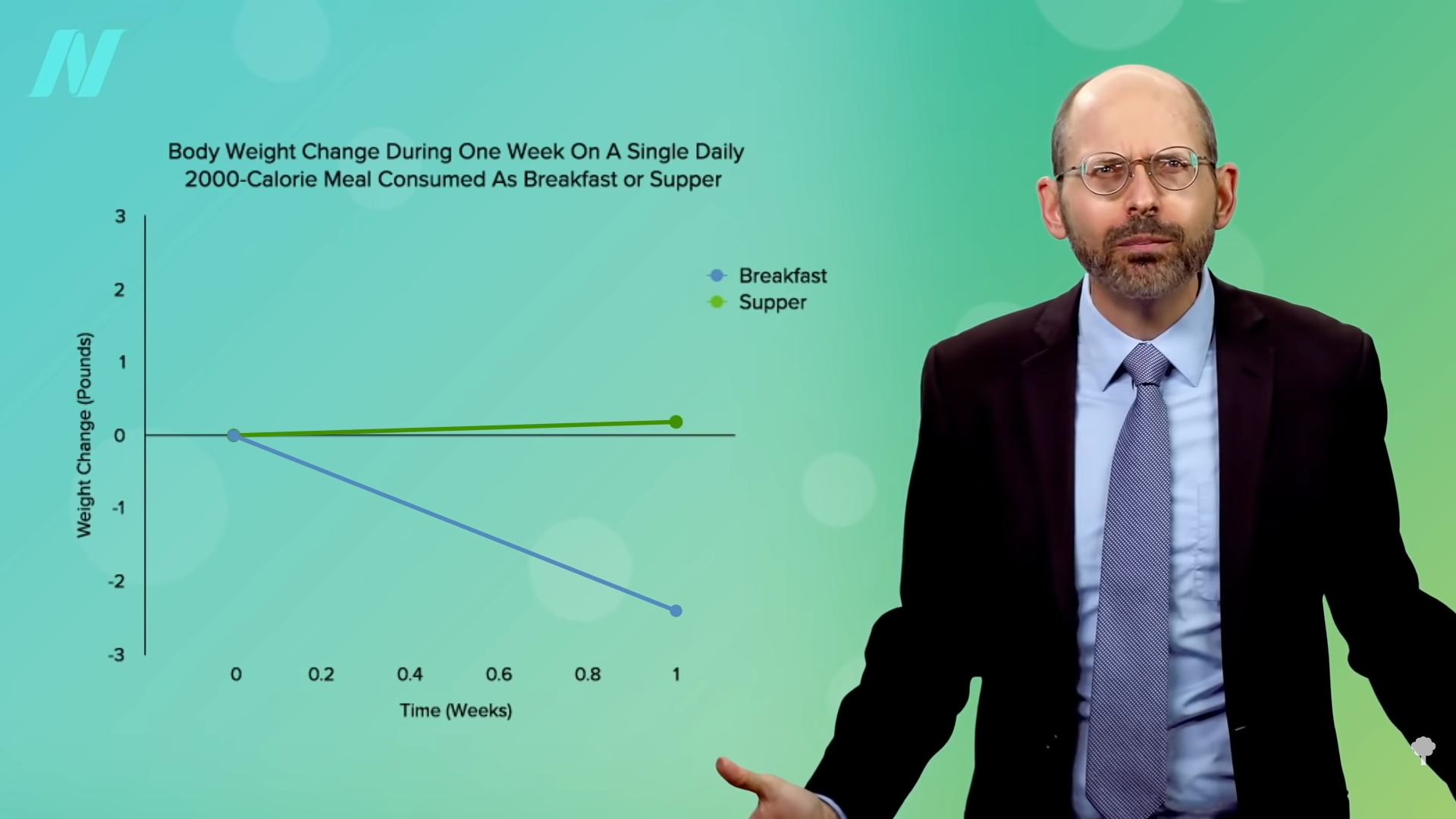
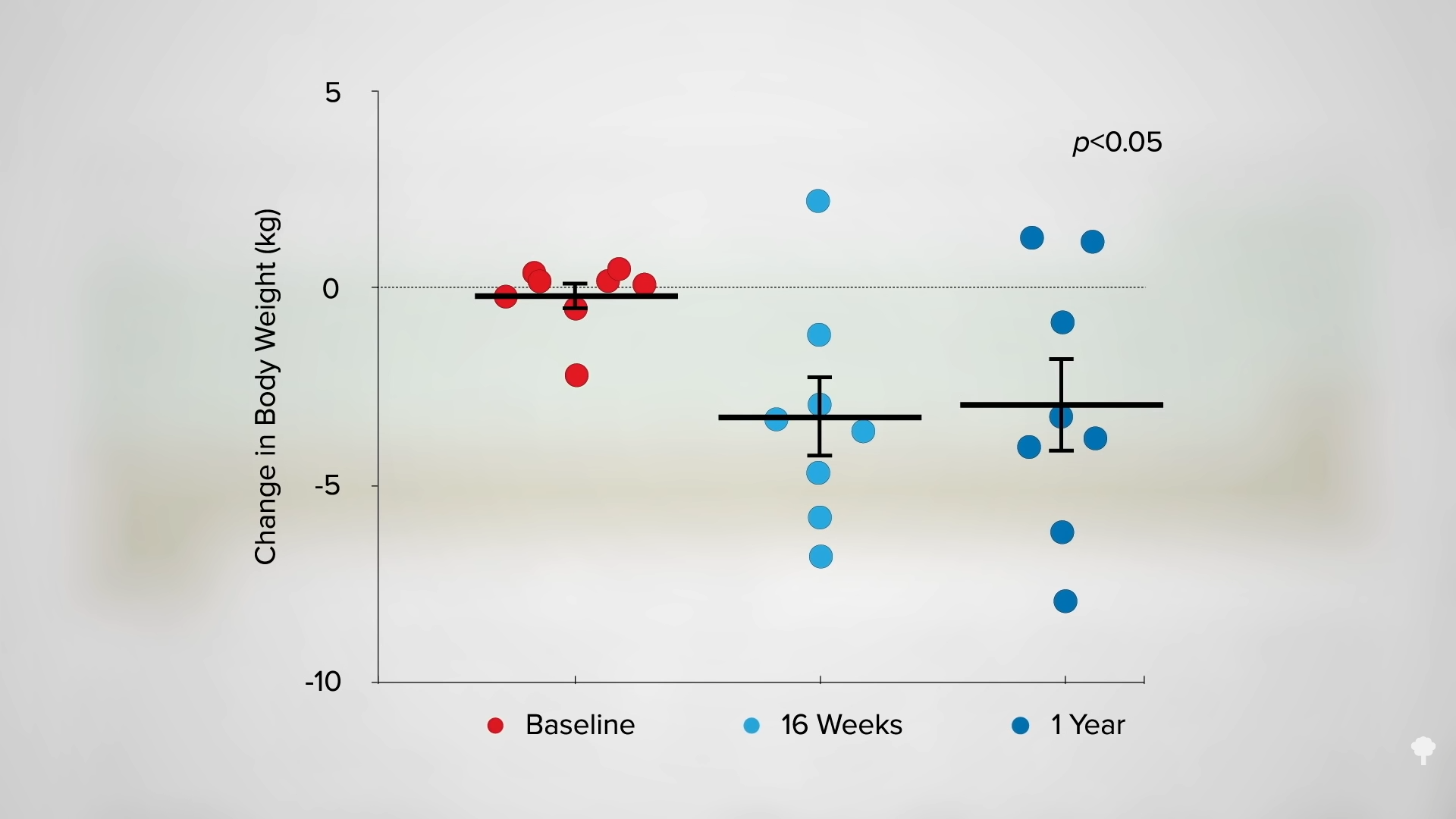
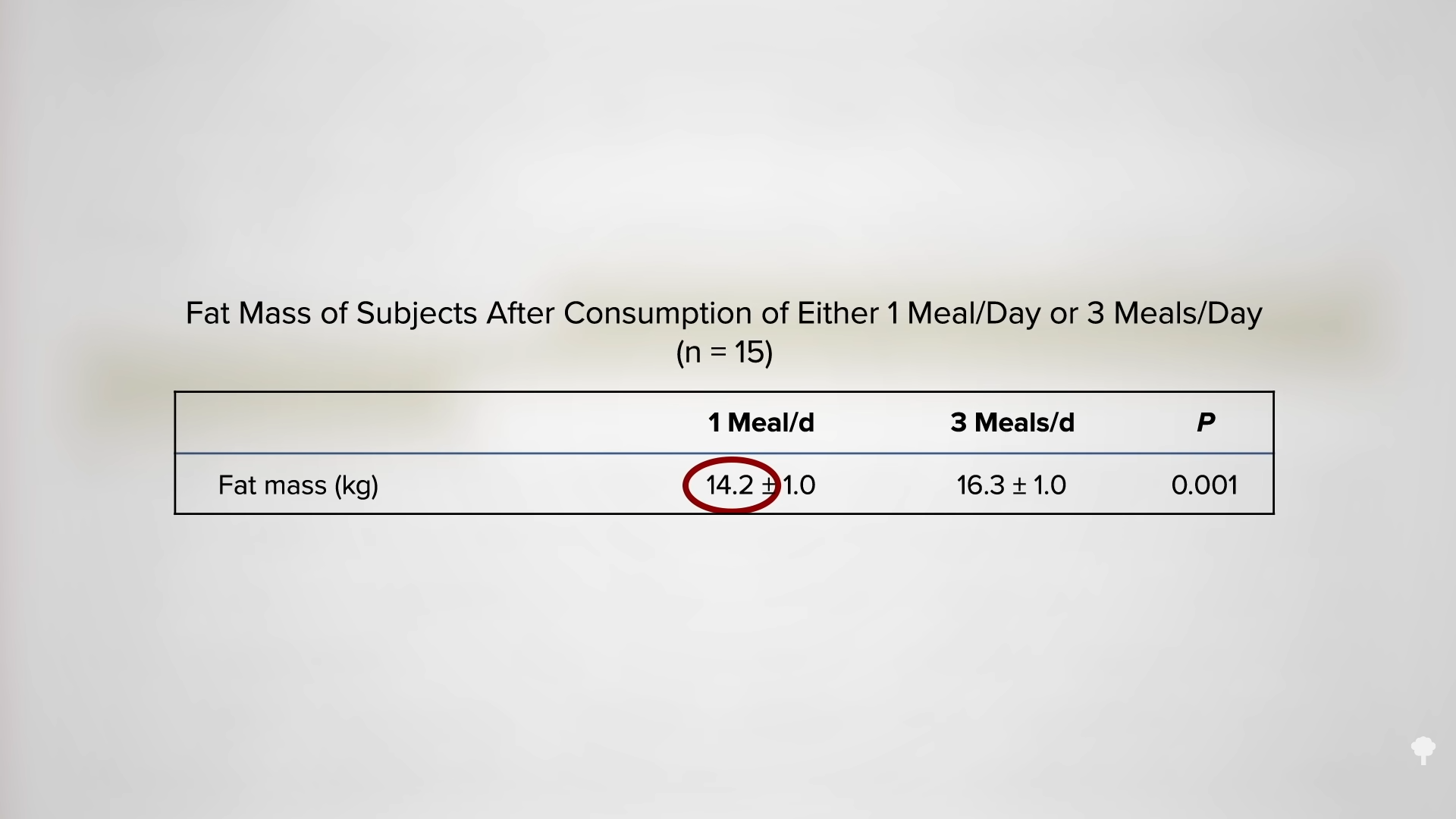
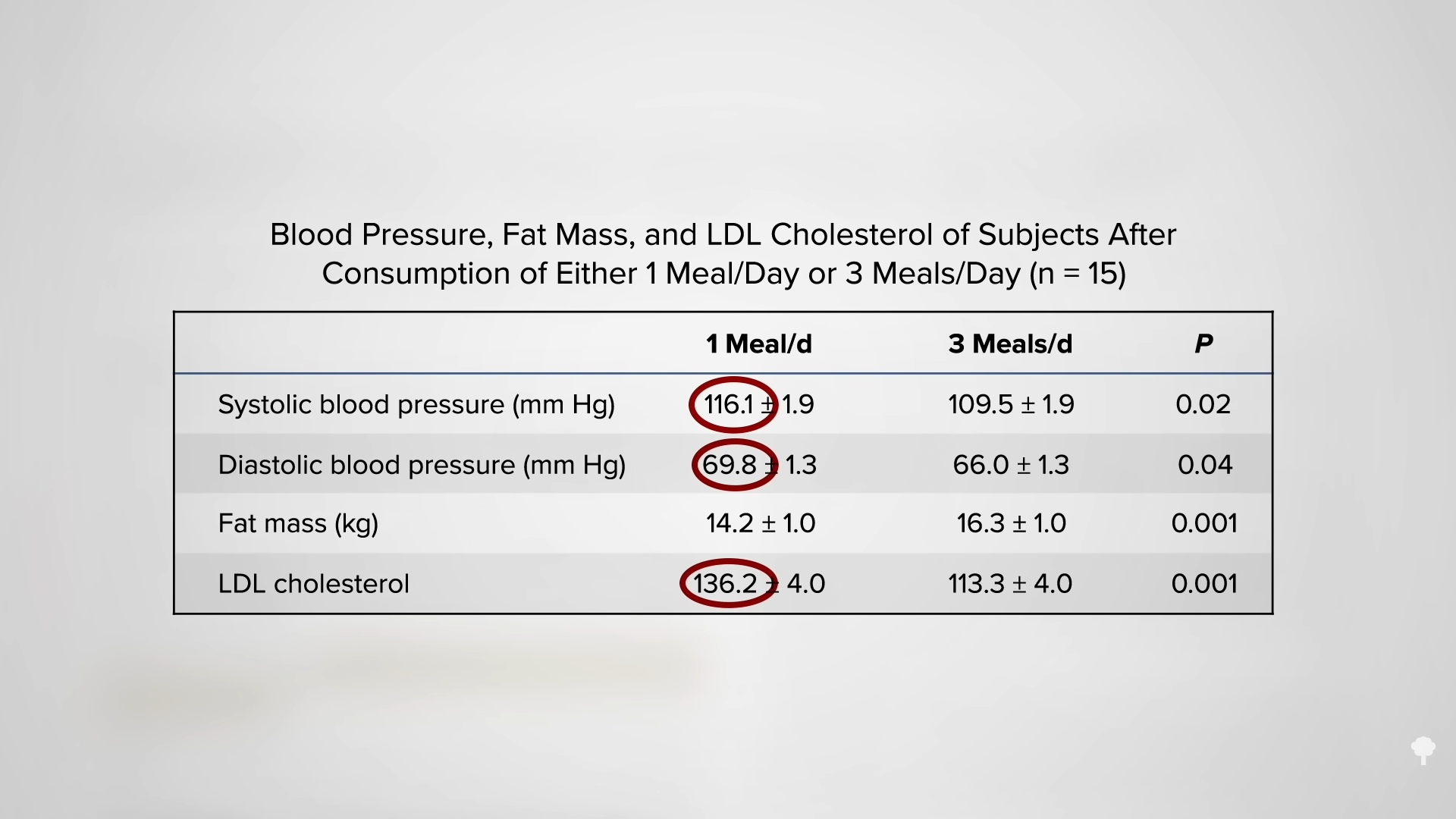
The Army scientists repeated the experiment, but this time, they had the participants eat exactly 2,000 calories either as breakfast or as dinner, taking appetite out of the picture. The subjects weren’t allowed to exercise either. Same number of calories, so the same change in weight, right? No. As you can see in the graph below and at 4:18 in my video, the breakfast-only group still lost about two pounds a week compared to the dinner-only group. Two pounds of weight loss eating the same number of calories. That’s why this concept of chronobiology, meal timing—when to eat—is so important.
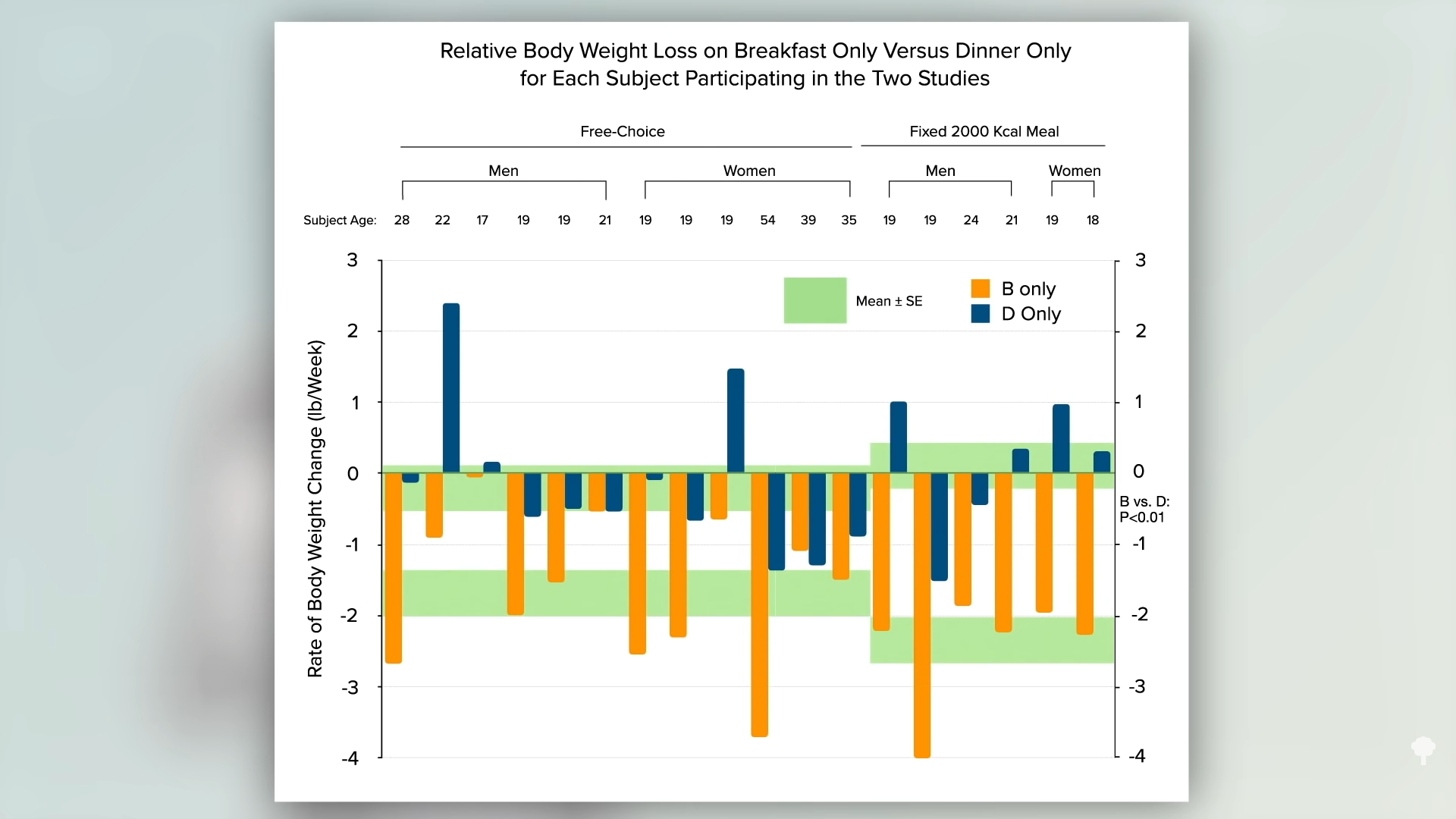
Isn’t that wild? Two pounds of weight loss a week eating the same number of calories! That was a pretty extreme study, though. What about just shifting a greater percentage of calories to earlier in the day? That’s the subject of my next video: Breakfast Like a King, Lunch Like a Prince, Dinner Like a Pauper. First, let’s take a break from chronobiology to look at the Benefits of Garlic for Fighting Cancer and the Common Cold. Then, we’ll resume checking other videos in the related posts below.
If you missed the first three videos in this extended series, also check out related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link

















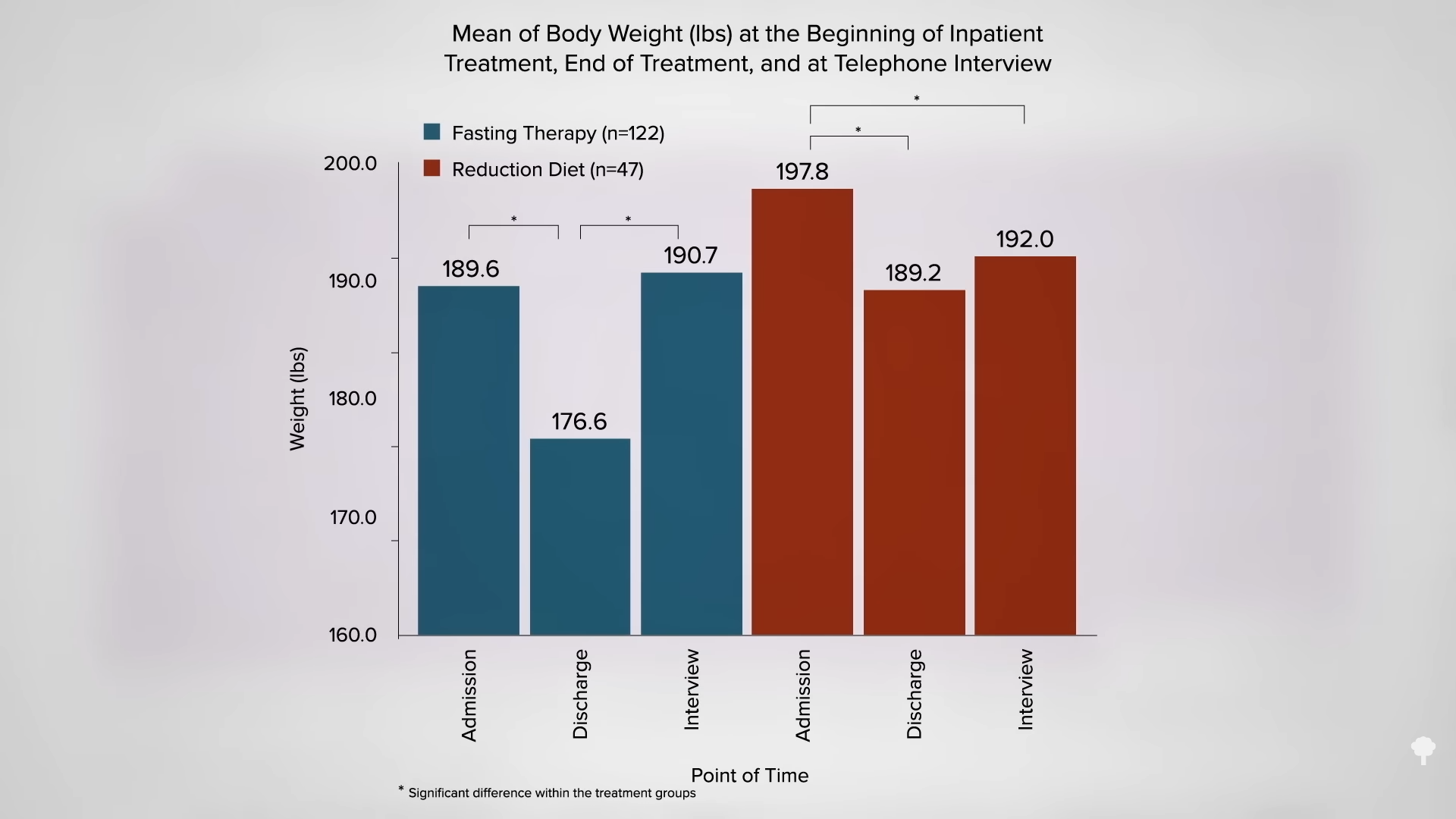
 Medically-supervised fasting has
Medically-supervised fasting has “
“
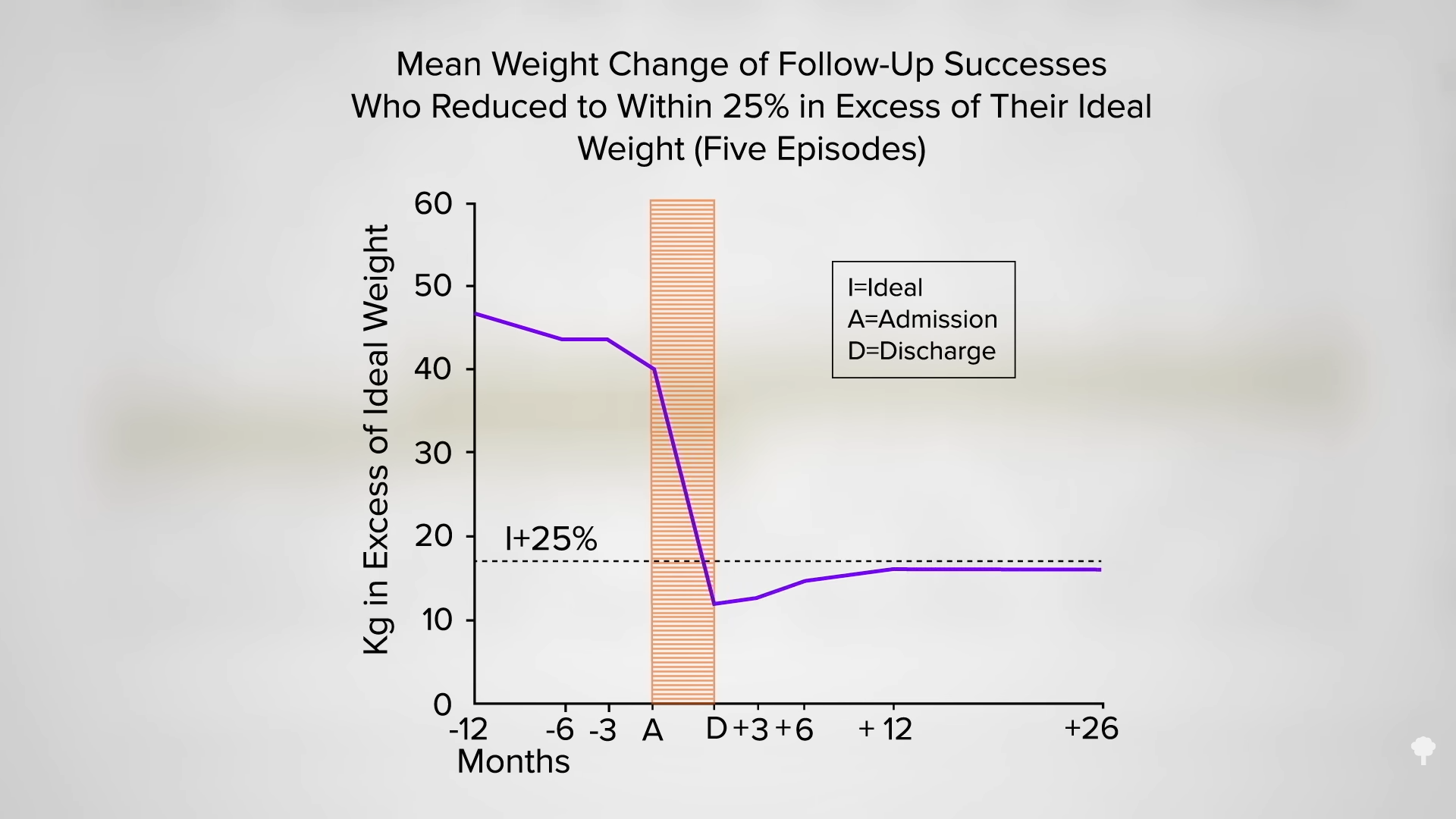
 What happened nine years later? “Therapeutic Fasting in Morbid Obesity”
What happened nine years later? “Therapeutic Fasting in Morbid Obesity” 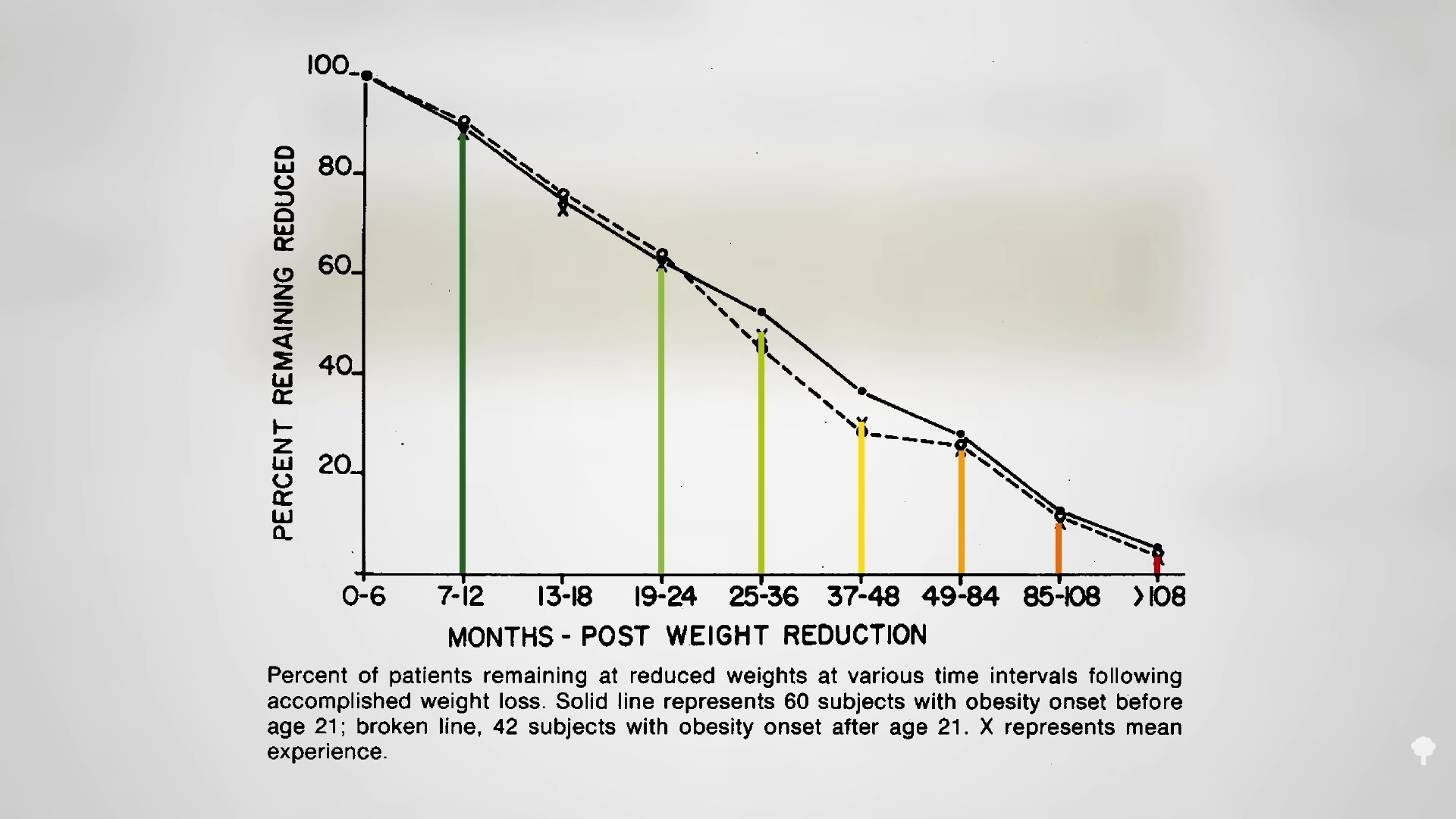 The small minority for whom fasting
The small minority for whom fasting 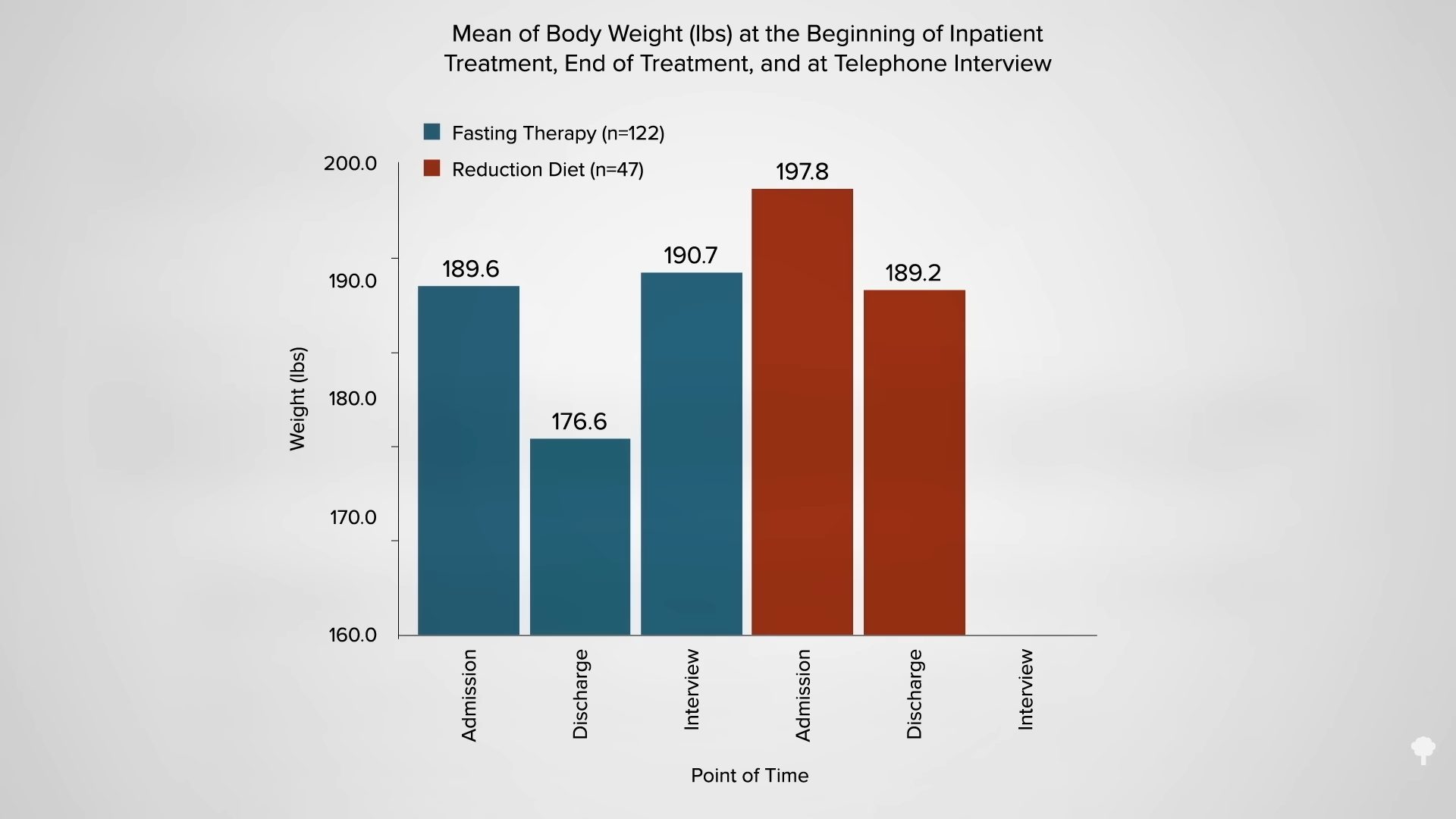
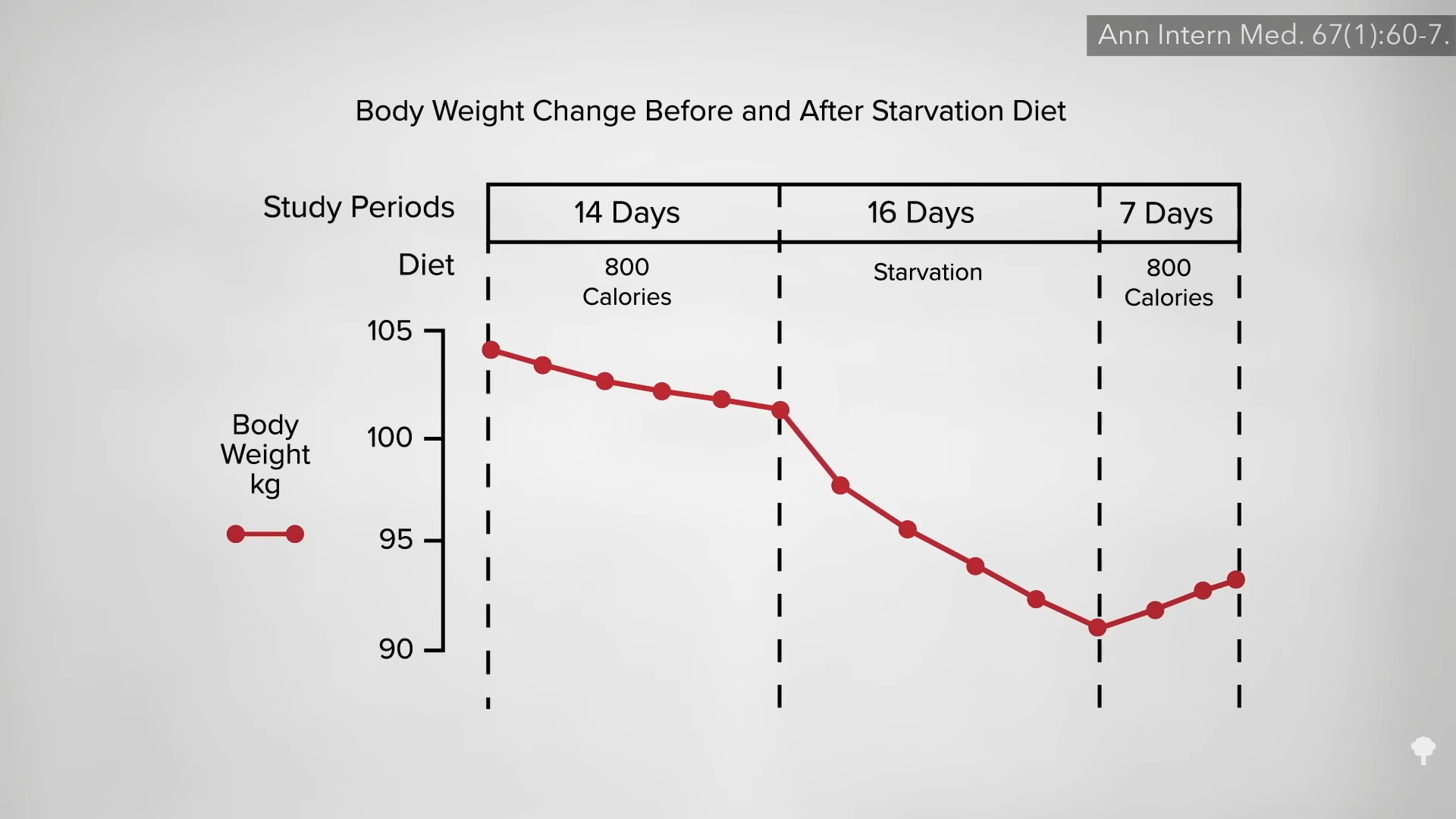
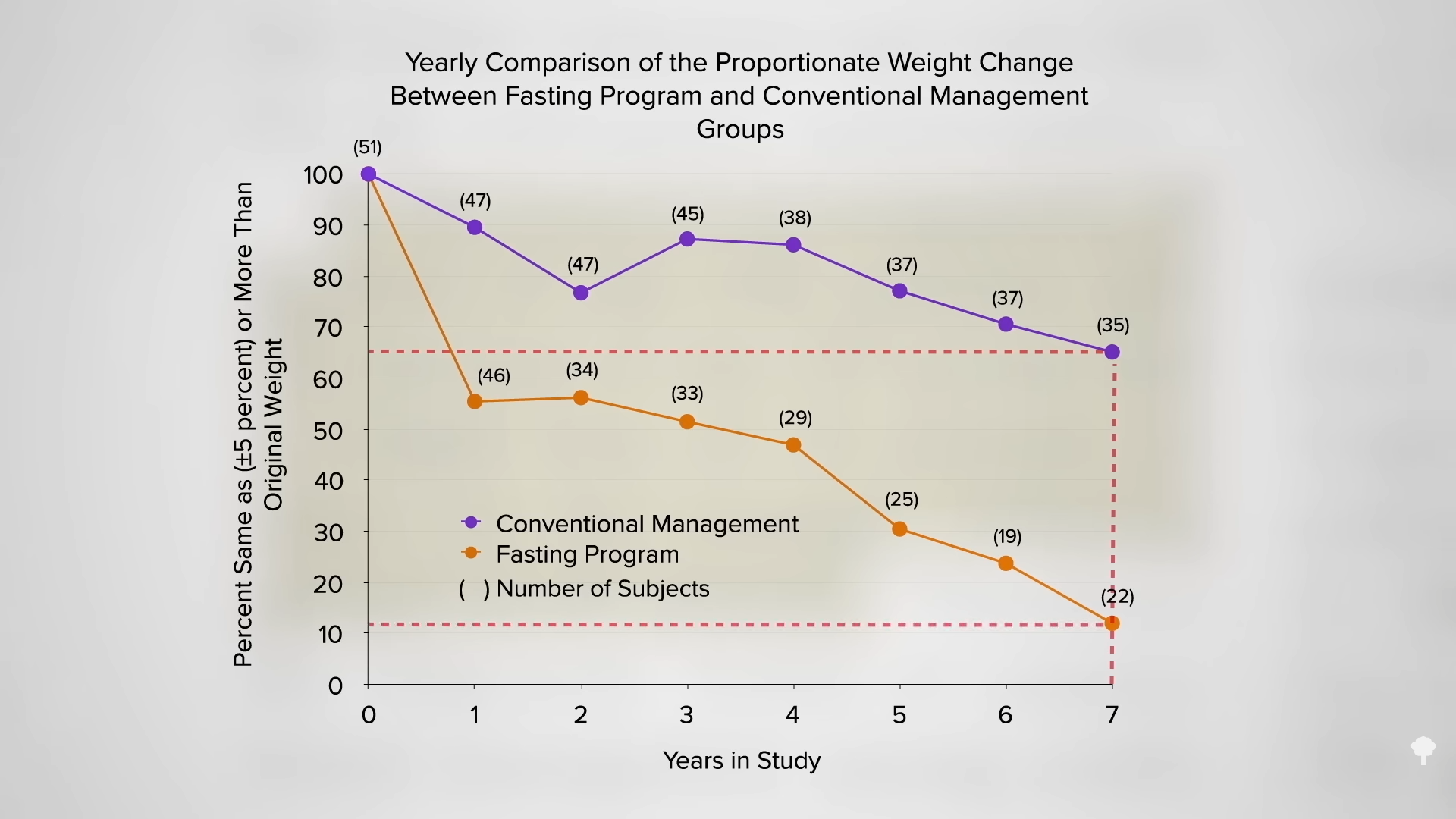
 This is the follow-up to
This is the follow-up to