[ad_1]
The sugar industry responds to evidence implicating sweeteners in the obesity epidemic.
In terms of excess body fat, the “well-documented obesity epidemic may merely be the tip of the overfat iceberg.” It’s been estimated that 91 percent of adults—nine out of ten of us—and 69 percent of children in the United States are overfat, a condition defined as having “excess body fat sufficient to impair health.” This can occur even in individuals who are “normal-weight and non-obese, often due to excess abdominal fat.” The way to tell if you’re overfat is if your waist circumference is more than half your height. What’s causing this epidemic? As I discuss in my video Does Sugar Lead to Weight Gain?, one primary cause may be all the added sugars we’re eating.
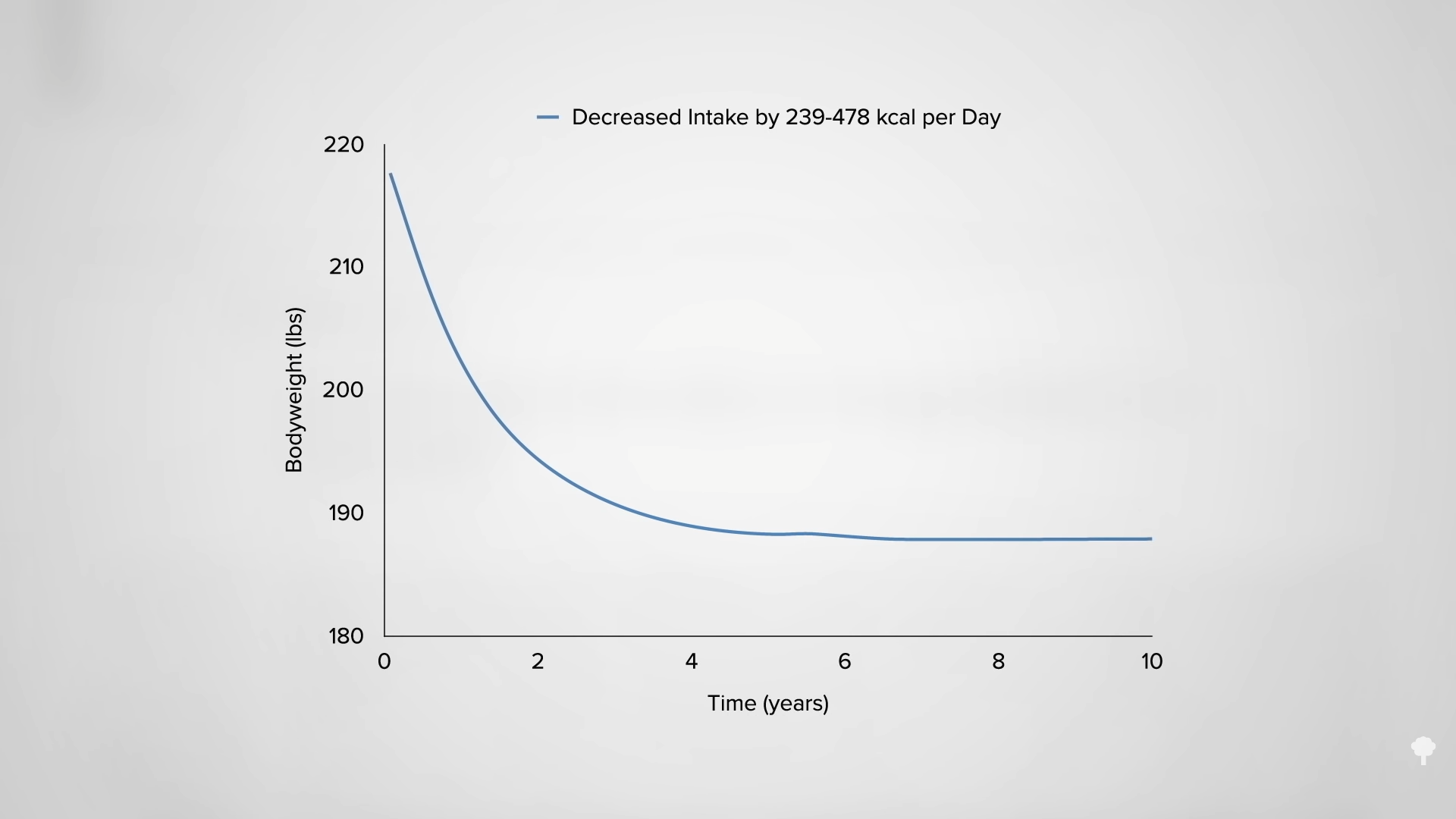
A century ago, sugar was heralded as one of the cheapest forms of calories in the diet. Just ten cents’ worth of sugar could furnish thousands of calories. Dr. Fredrick Stare, “Harvard’s sugar-pushing nutritionist,” bristled at the term “empty calories,” writing that the calories in sugar were “not empty but full of energy”—in other words, full of calories, which we are now getting too much of. The excess bodyweight of the U.S. population corresponds to about a daily 350- to 500-calorie excess on average. So, “to revert the obesity epidemic,” that’s how many calories we have to reduce, but which calories should we cut? As you can see below and at 1:33 in my video, the majority of Americans who fail to meet the Dietary Guidelines’ sugar limit get about that many calories in added sugars every day: Twenty-five teaspoons’ worth of added sugars is about 400 calories.
There are die-hard sugar defenders. James Rippe, for example, was reportedly paid $40,000 a month by the high fructose corn syrup industry—and that was on top of the $10 million it paid for his research. Even Dr. Rippe considers it “undisputable that sugars…contribute to obesity. It is also undisputable that sugar reduction…should be part of any weight loss program.” And, of all sources of calories to limit, since sugar is just empty calories and contains no essential nutrients, “reducing sugar consumption is obviously the place to start.” And, again, this is what the researchers funded by the likes of Dr. Pepper and Coca-Cola are saying. The primary author of “Dietary Sugar and Body Weight: Have We Reached a Crisis in the Epidemic of Obesity and Diabetes?…,” Richard Kahn, is infamous for his defense of the American Beverage Association—the soda industry—and he was the chief science officer at the American Diabetes Association when it signed a million-dollar sponsorship deal with the world’s largest candy company. “Maybe the American Diabetes Association should rename itself the American Junk Food Association,” said the director of a consumer advocacy group. What do you expect from an organization that was started with drug industry funding?
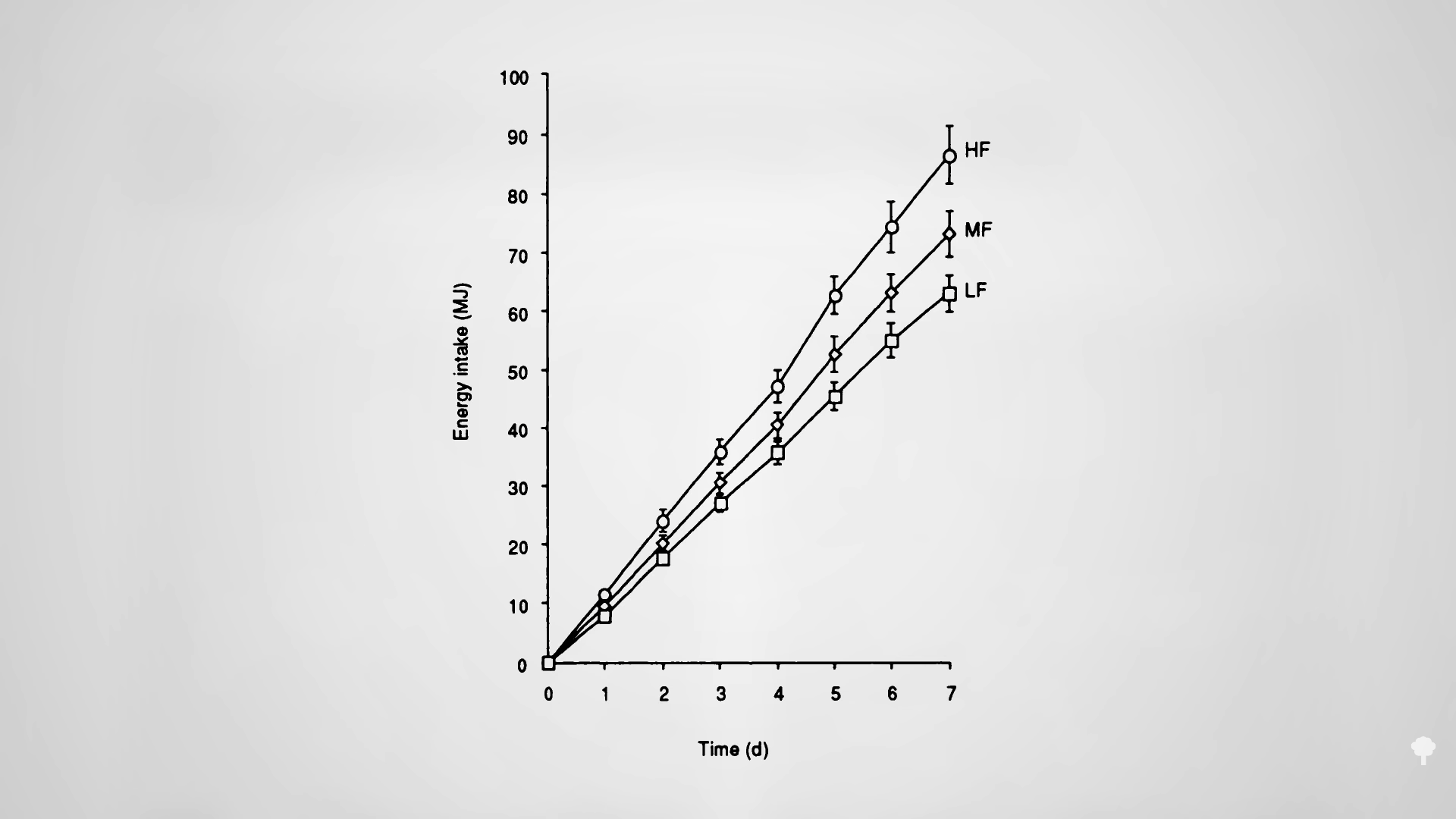
The bottom line is that “randomised controlled trials show that increasing sugars intake increases energy [calorie] intake” and “increasing sugar intake leads to body weight gain in adults, and…sugar reduction leads to body weight loss in children.” For example, when researchers randomized individuals to either increase or decrease their intake of table sugar, the added sugar group gained about three and a half pounds over ten weeks, whereas the reduced sugar group lost about two and a half pounds. A systematic review and meta-analysis of all such ad libitum diet studies—real-life studies where sugar levels were changed but people could otherwise eat whatever they wanted—found that reduced intake of dietary sugars resulted in a decrease in body weight, whereas “increased sugars intake was associated with a comparable weight increase.” The researchers found that, “considering the rapid weight gain that occurs after an increased intake of sugars, it seems reasonable to conclude that advice relating to sugars intake is a relevant component of a strategy to reduce the high risk of overweight and obesity in most countries.” That is, it’s reasonable to advise people to cut down on their sugar consumption.
Findings from observational studies have been “more ambiguous,” though, with an association found between obesity and intake of sweetened beverages, but failing to show consistent correlations with consumption of sugary foods. Most such studies rely on self-reported data, however, and “it is likely that this has introduced bias, especially as underreporting of diet has been found to be more prevalent among obese people and it is sugar-rich foods that are most commonly underreported.” However, one can measure trace sucrose levels in the urine, which gives an objective measure of actual sugar intake and also excludes contributions from other sweeteners such as high fructose corn syrup. When researchers did this, they discovered that, indeed, sugar intake is not only associated with greater odds of obesity and greater waist circumference on a snapshot-in-time cross-sectional basis, but that was also seen in a prospective cohort study over time. “Using urinary sucrose as the measure of sucrose intake,” researchers found that “participants in the highest v. the lowest quintile [fifth] for sucrose intake had 54% greater risk of being overweight or obese.”
“Denying evidence that sugars are harmful to health has always been at the heart of the sugar industry’s defense.” But when the evidence is undeniable, like the link between sugar and cavities, it switches from denial to deflection, like trying to pull attention away from restricting intake to coming up with some kind of “vaccine against tooth decay.” We seem to have reached a similar point with obesity, with the likes of the Sugar Bureau switching from denial to deflection by commissioning research suggesting that obese individuals would not benefit from losing weight, a stance contradicted by hundreds of studies across four continents involving more than ten million participants.
For more on Big Sugar’s influence, check out Sugar Industry Attempts to Manipulate the Science.
You may also be interested in some of my other popular videos on sugar. See related videos below.
[ad_2]
Michael Greger M.D. FACLM
Source link



 In my previous video, I dive into how
In my previous video, I dive into how 

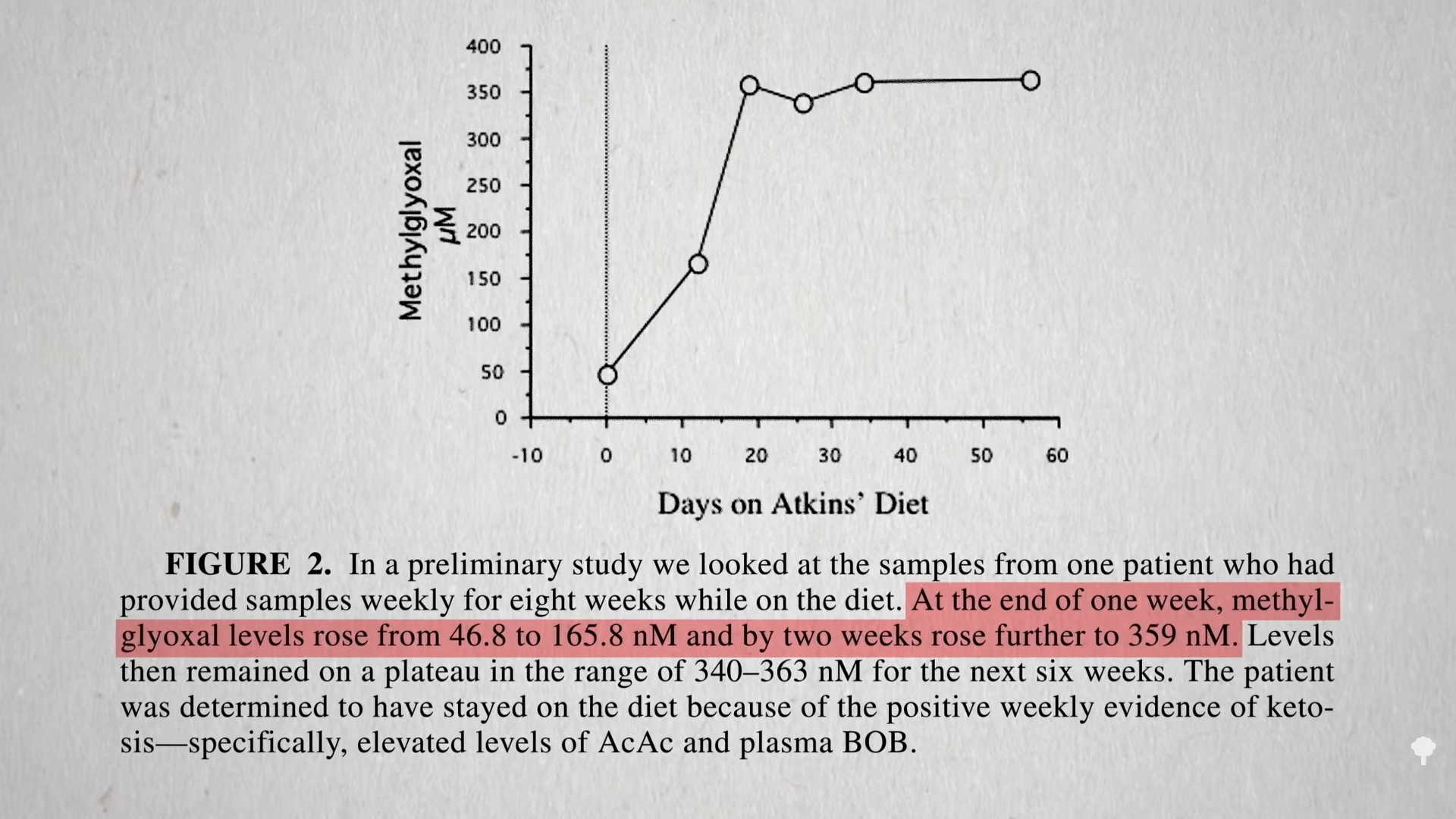
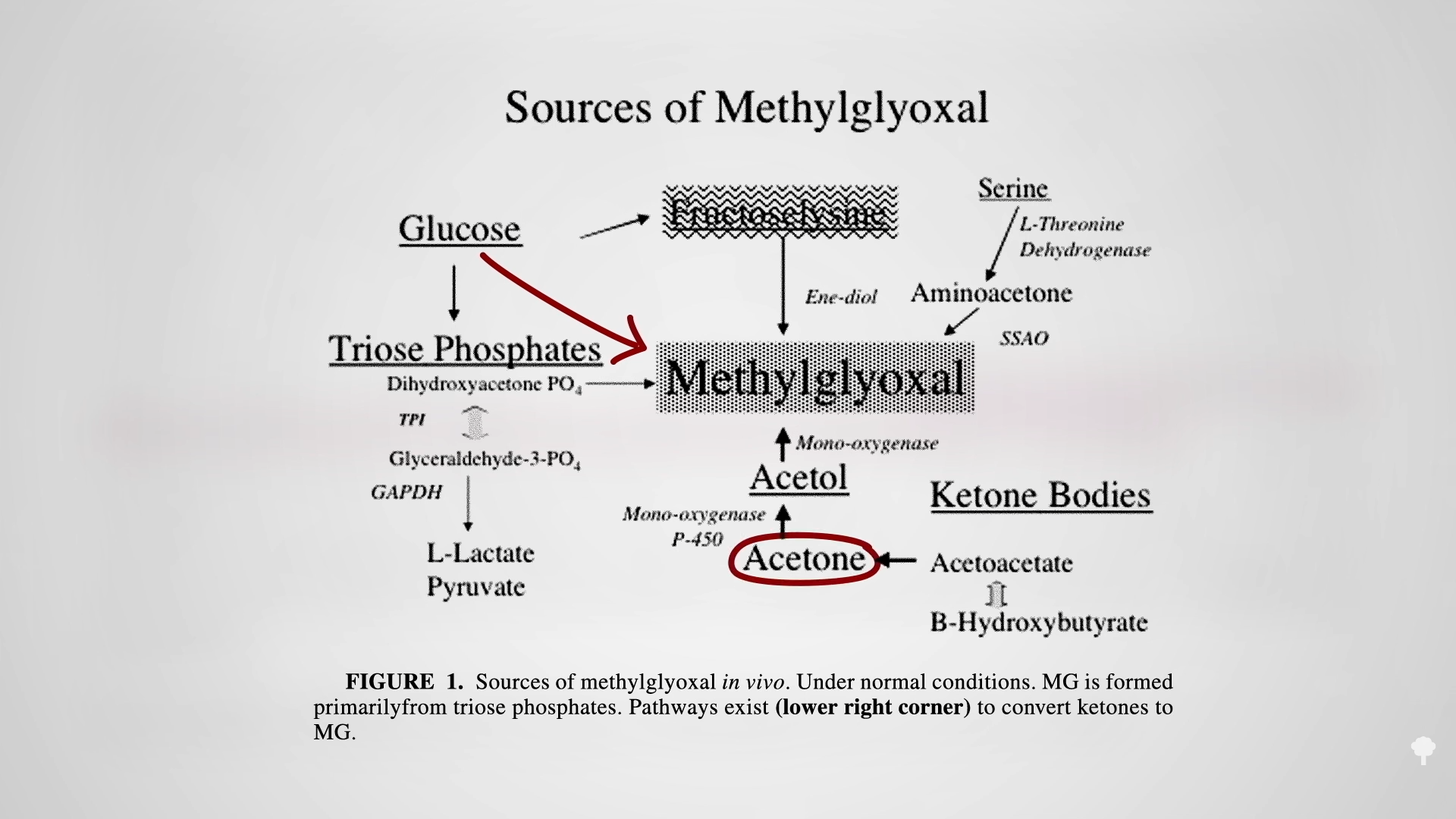
 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal 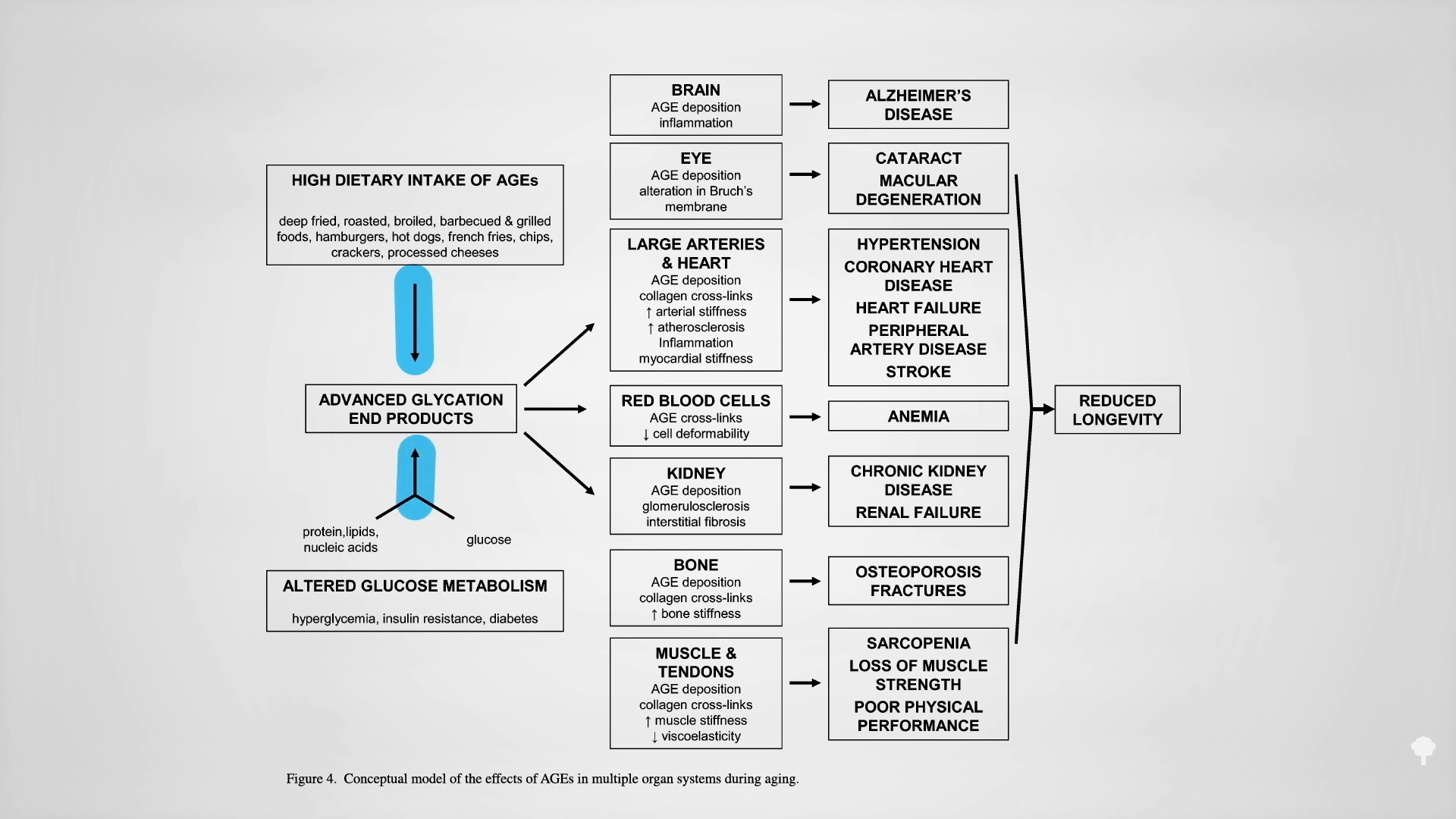

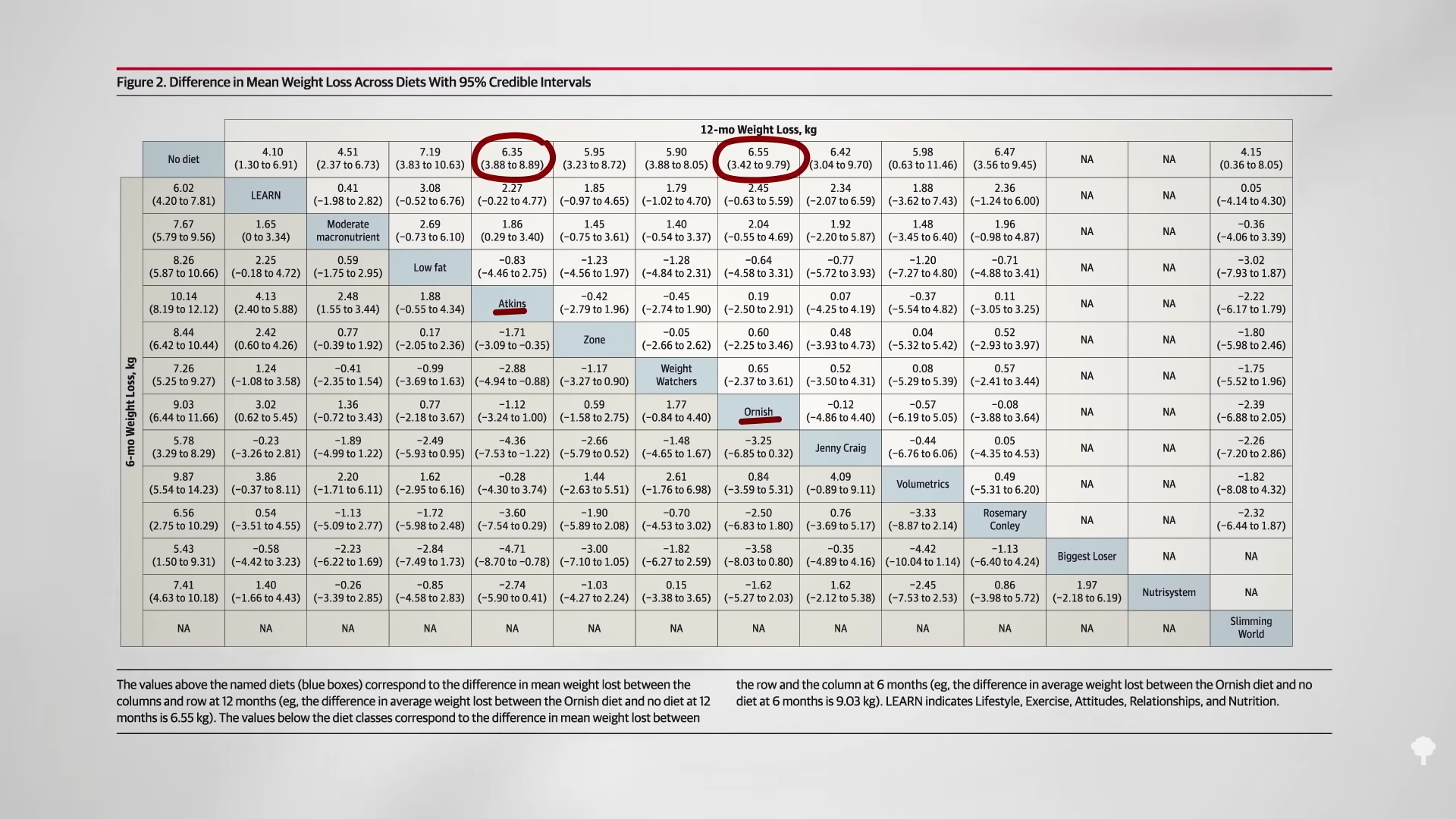
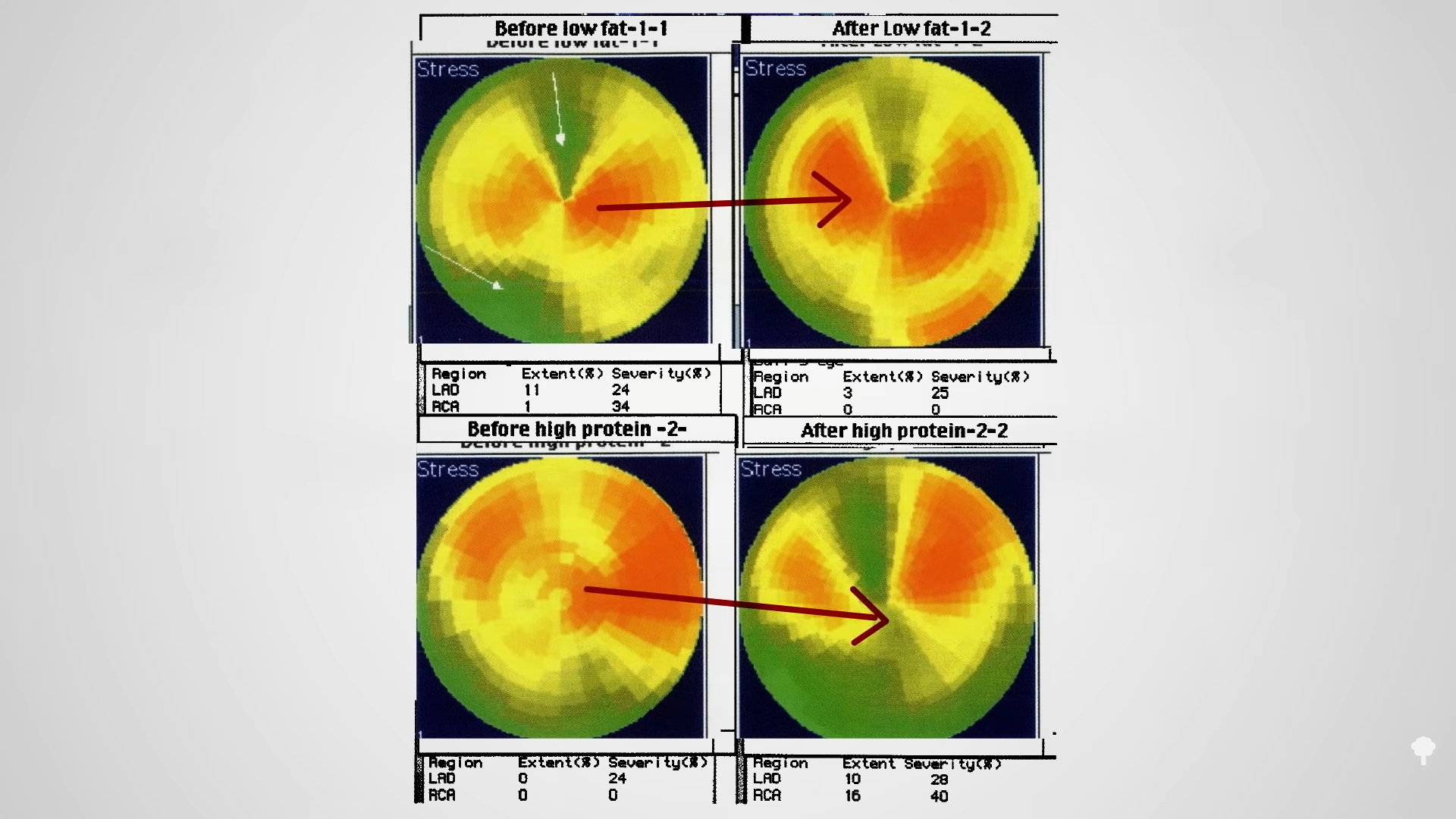





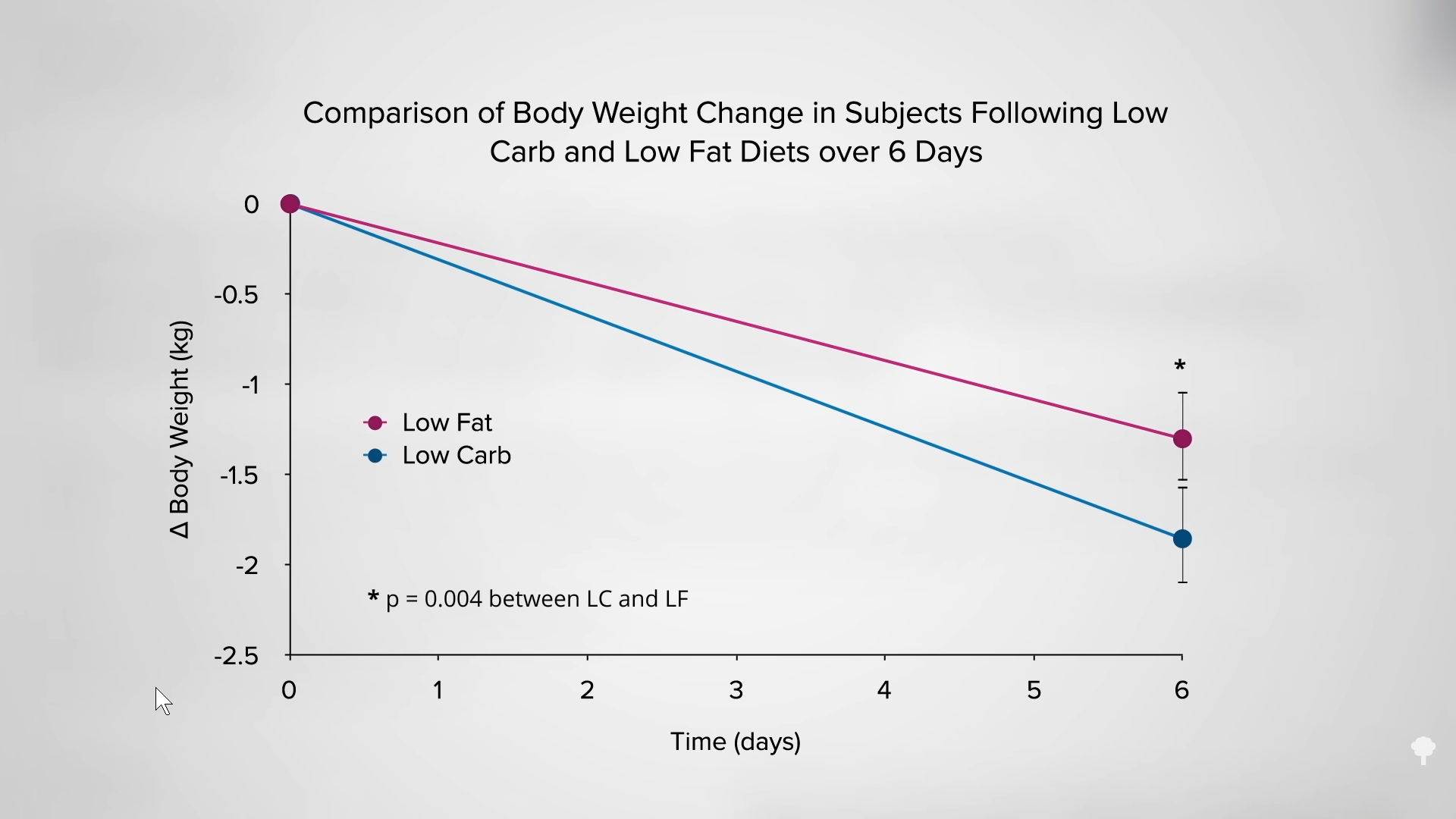
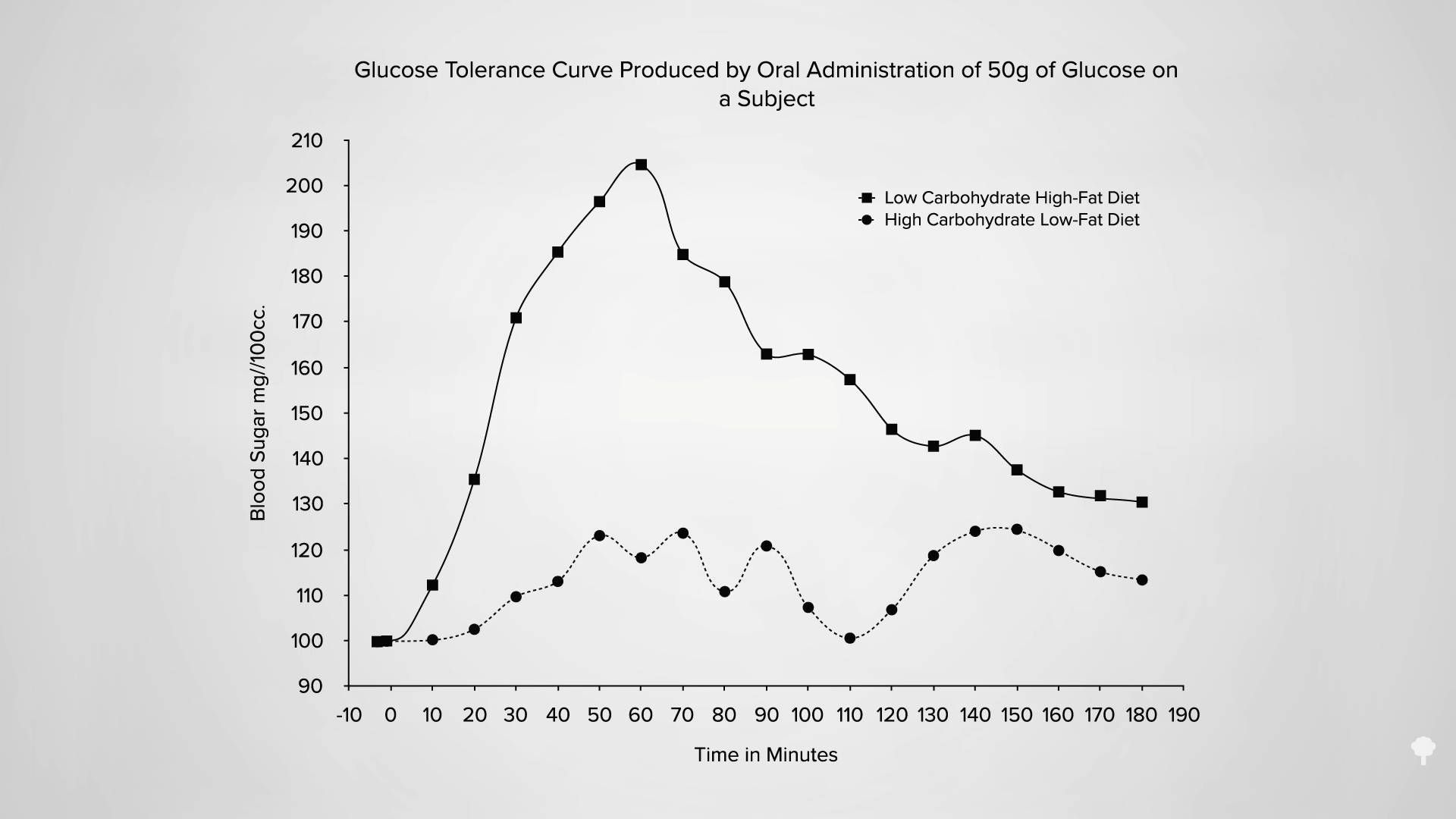
 Low-carb diets cut down on refined grains and added sugars, and low-fat diets tend to cut down on added fats and meat, so they both tell people to cut down on donuts. Any diet that does that already has a leg up. I figure a don’t-eat-anything-that-starts-with-the-letter-D diet could also successfully cause weight loss if it caused people to cut down on donuts, danishes, and Doritos, even if it makes no nutritional sense to exclude something like dill.
Low-carb diets cut down on refined grains and added sugars, and low-fat diets tend to cut down on added fats and meat, so they both tell people to cut down on donuts. Any diet that does that already has a leg up. I figure a don’t-eat-anything-that-starts-with-the-letter-D diet could also successfully cause weight loss if it caused people to cut down on donuts, danishes, and Doritos, even if it makes no nutritional sense to exclude something like dill.