[ad_1]
WASHINGTON (AP) — President Donald Trump unveiled a deal Thursday with drugmakers Eli Lilly and Novo Nordisk to expand coverage and reduce prices for the popular obesity treatments Zepbound and Wegovy.
Known as GLP-1 receptor agonists, the drugs have soared in popularity in recent years, but patient access has been a consistent problem because of their cost — around $500 a month for higher doses — and insurance coverage has been spotty. More than 100 million American adults are obese, according to federal estimates.
Coverage of the drugs for obesity will expand to Medicare patients starting next year, according to the administration, which said some lower prices also will be phased in for patients without coverage. Starting doses of new, pill versions of the treatments also will cost $149 a month if they are approved.
“(It) will save lives, improve the health of millions and millions of Americans,” said Trump, in an Oval Office announcement in which he referred to GLP-1s as a “fat drug.”
Thursday’s announcement is the latest attempt by the Trump administration to rein in soaring drug prices in its efforts to address cost-of-living concerns among voters. Pfizer and AstraZeneca recently agreed to lower the cost of prescription drugs for Medicaid after an executive order in May set a deadline for drugmakers to electively lower prices or face new limits on what the government will pay.
As with the other deals, it’s not clear how much the price drop will be felt by consumers. Drug prices can vary based on the competition for treatments and insurance coverage.
Obesity drugs are popular, but costly
The obesity drugs work by targeting hormones in the gut and brain that affect appetite and feelings of fullness. In clinical trials, they helped people shed 15% to 22% of their body weight — up to 50 pounds or more in many cases.
Patients usually start on smaller doses and then work up to larger amounts, depending on their needs. They need to stay on the the treatments indefinitely or risk regaining weight, experts say.
The medications have proven especially lucrative for Lilly and Novo. Lilly said recently that sales of Zepbound have tripled so far this year to more than $9 billion.
But for many Americans, their cost has made them out of reach.
Medicare, the federally funded coverage program mainly for people ages 65 and over, now covers the cost of the drugs for conditions such as type 2 diabetes and cardiovascular disease, but not for weight loss alone. Trump’s predecessor, Joe Biden, proposed a rule last November that would have changed that, but the Trump administration nixed it.
Few state and federally funded Medicaid programs, for people with low incomes, offer coverage. And employers and insurers that provide commercial coverage are wary of paying for these drugs in part because so many people might use them.
The $500 monthly price for higher doses of the treatments also makes them unaffordable for those without insurance, doctors say.
Trump tries to show he is in touch with cost-of-living concerns
Thursday’s announcement comes as the White House is looking to demonstrate that Trump is in touch with Americans’ frustrations with rising costs for food, housing, health care and other necessities.
“Trump is the friend of the forgotten American,” said Health and Human Services Secretary Robert F. Kennedy, Jr. at Thursday’s announcement. “Obesity is a disease of poverty. And overwhelmingly, these drugs have only been available for people who have wealth.”
(Obesity rates actually are slightly higher for middle-income Americans than they are for those with the lowest and highest incomes, according to 2017-2020 data collected by the U.S. Centers for Disease Control and Prevention.)
Kennedy had previously expressed skepticism about GLP-1s, but he was full of praise for Trump for pushing to help a broader segment of Americans have access to the drug.
Trump, who has a history of commenting on people’s appearance, asked the officials who joined him in the Oval Office whether they had used the weight-loss medications.
“Do you take any of this stuff, Howard?” Trump asked Commerce Secretary Howard Lutnick. “Not yet,” Lutnick replied. “He’s taking it,” the president said of Steven Cheung, who is the White House director of communications.
The drug-pricing announcement came days after Democrats swept elections in races across the country. Economic worries were the dominant concern for those casting their ballots, according to findings from the AP voter poll.
Plan calls for phased-in price reductions
The White House sought to diminish price-reduction efforts by the previous Democratic administration as a gift to the pharmaceutical industry.
Trump, instead, consummated a deal that ensures Americans aren’t unfairly financing the pharmaceutical industry’s innovation, claimed a senior administration official, who briefed reporters ahead of Thursday’s Oval Office announcement.
Another senior administration official said coverage of the drugs will expand to Medicare patients starting next year. The program will start covering the treatments for people who have severe obesity and others who are overweight or obese and have serious health problems, the official said. Those who qualify will pay $50 copays for the medicine.
Lower prices also will be phased in for people without coverage through the administration’s TrumpRx program, which will allow people to buy drugs directly from manufacturers, starting in January.
Administration officials said the average price of the drugs sold on TrumpRx will start at around $350 and then drop to $245 over the next two years.
A Novo Nordisk spokesperson declined to provide details on their pricing changes.
Lilly said it will sell a starter dose of Zepbound for $299 a month and additional doses at up to $449. Both represent $50 reductions from current prices for doses it sells directly to patients.
Administration officials said lower prices also will be provided for state and federally funded Medicaid programs. And starting doses of new, pill versions of the obesity treatments will cost $149 a month if they are approved.
U.S. health regulators on Thursday separately agreed to dramatically expedite review of Lilly’s obesity pill, orforglipron. An FDA decision on Novo Nordisk’s Wegovy pill is expected later this year.
Doctors who treat patients for obesity say help is needed to improve access. Dr. Leslie Golden says she has roughly 600 patients taking one of these treatments, and at least 75% struggle to afford them. Even with coverage, some face $150 copayments for refills.
“Every visit it’s, ‘How long can we continue to do this? What’s the plan if I can’t continue?’” said Golden, an obesity medicine specialist in Watertown, Wisconsin. “Some of them are working additional jobs or delaying retirement so they can continue to pay for it.”
___
AP Health Writer Matthew Perrone contributed to this report.
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Department of Science Education and the Robert Wood Johnson Foundation. The AP is solely responsible for all content.
[ad_2]

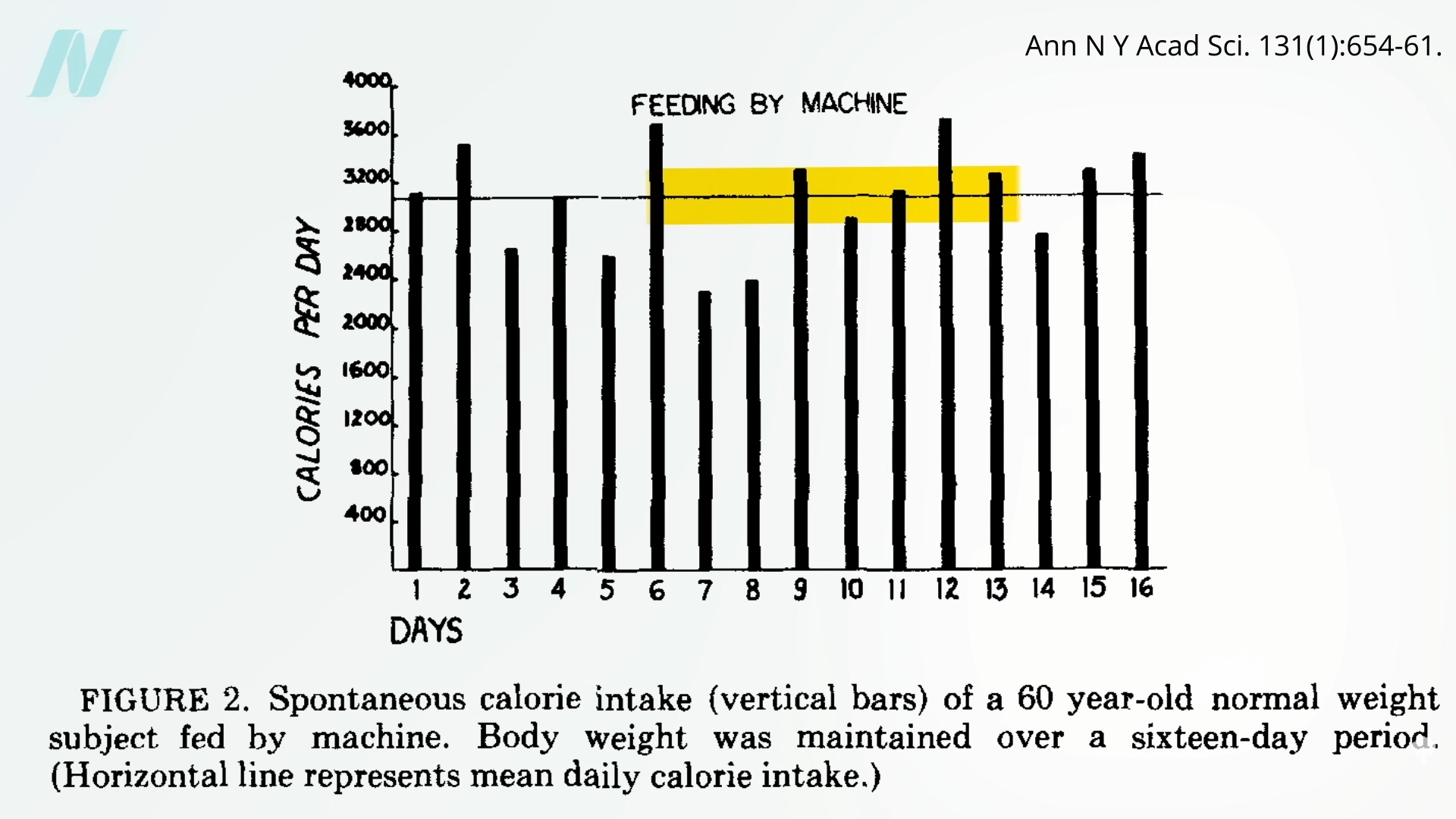
 We appear to
We appear to 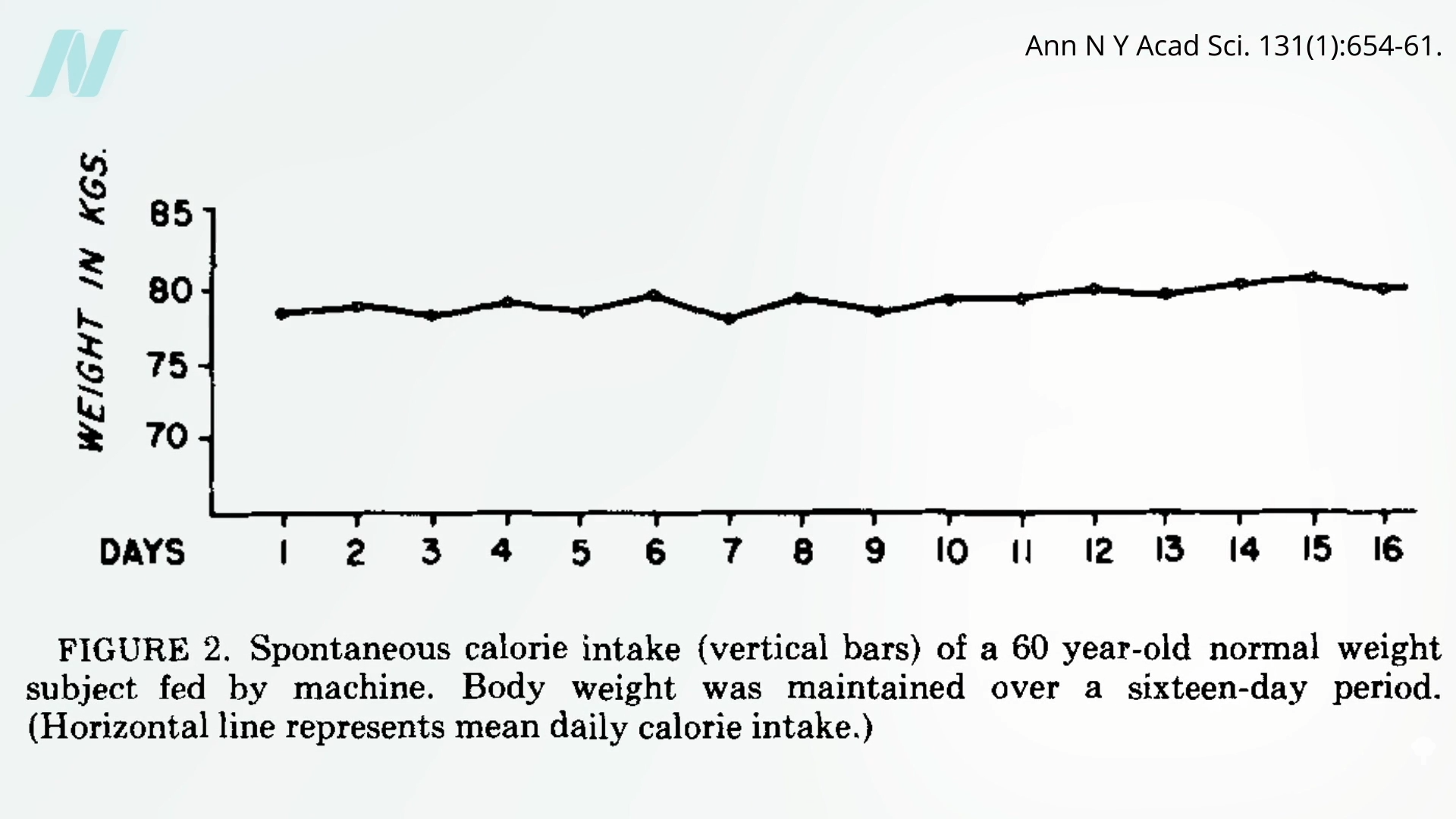
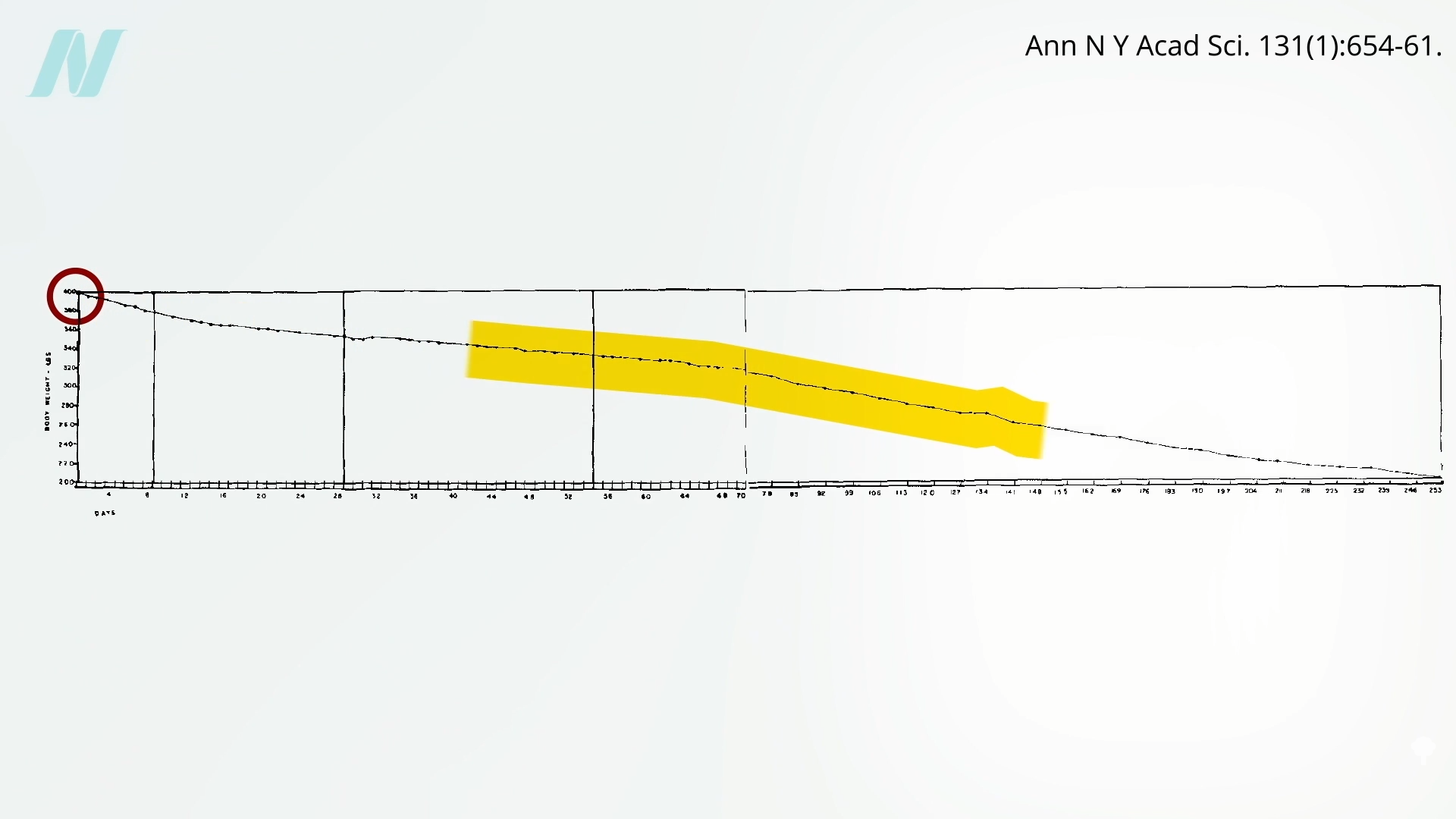
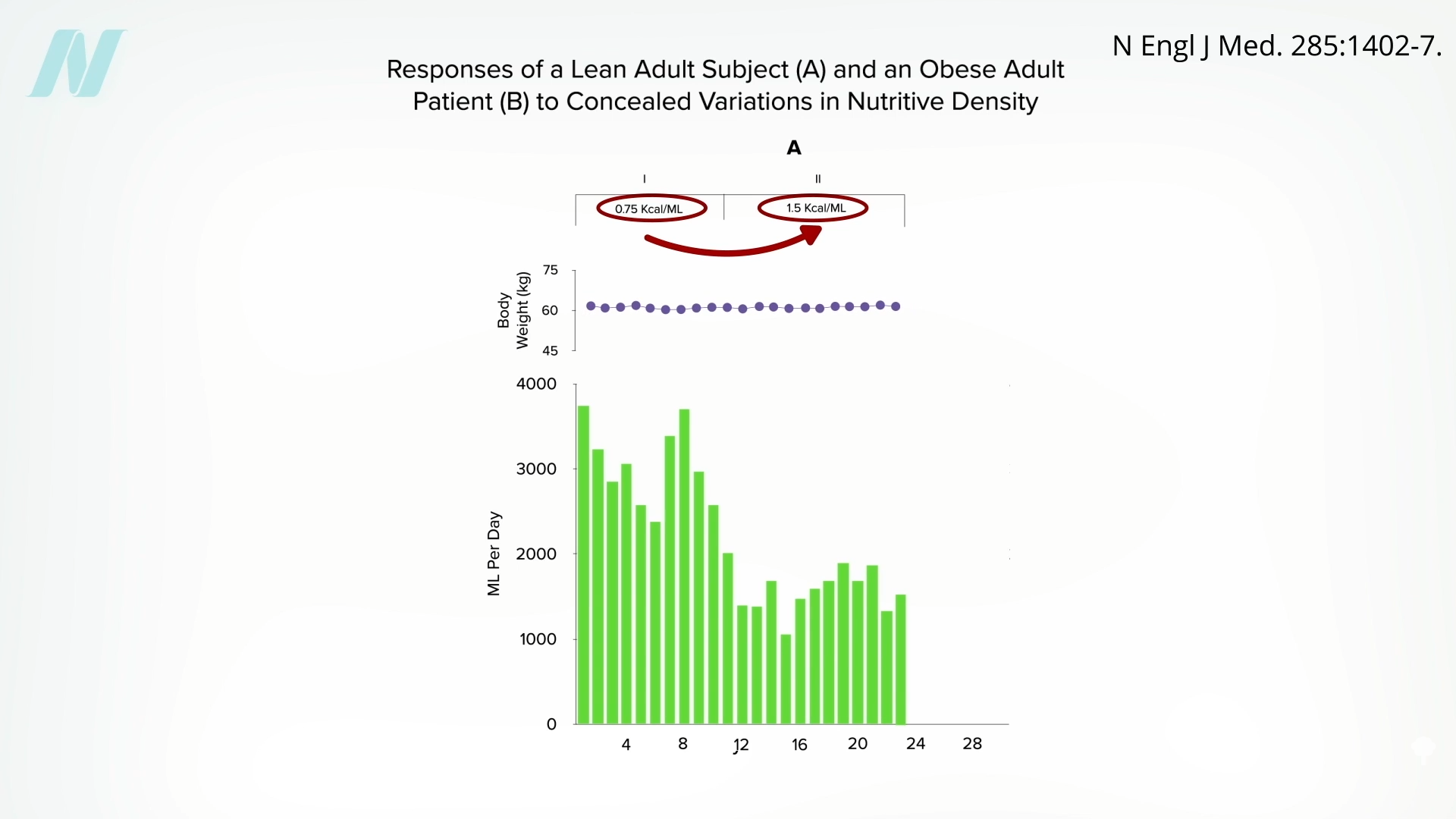
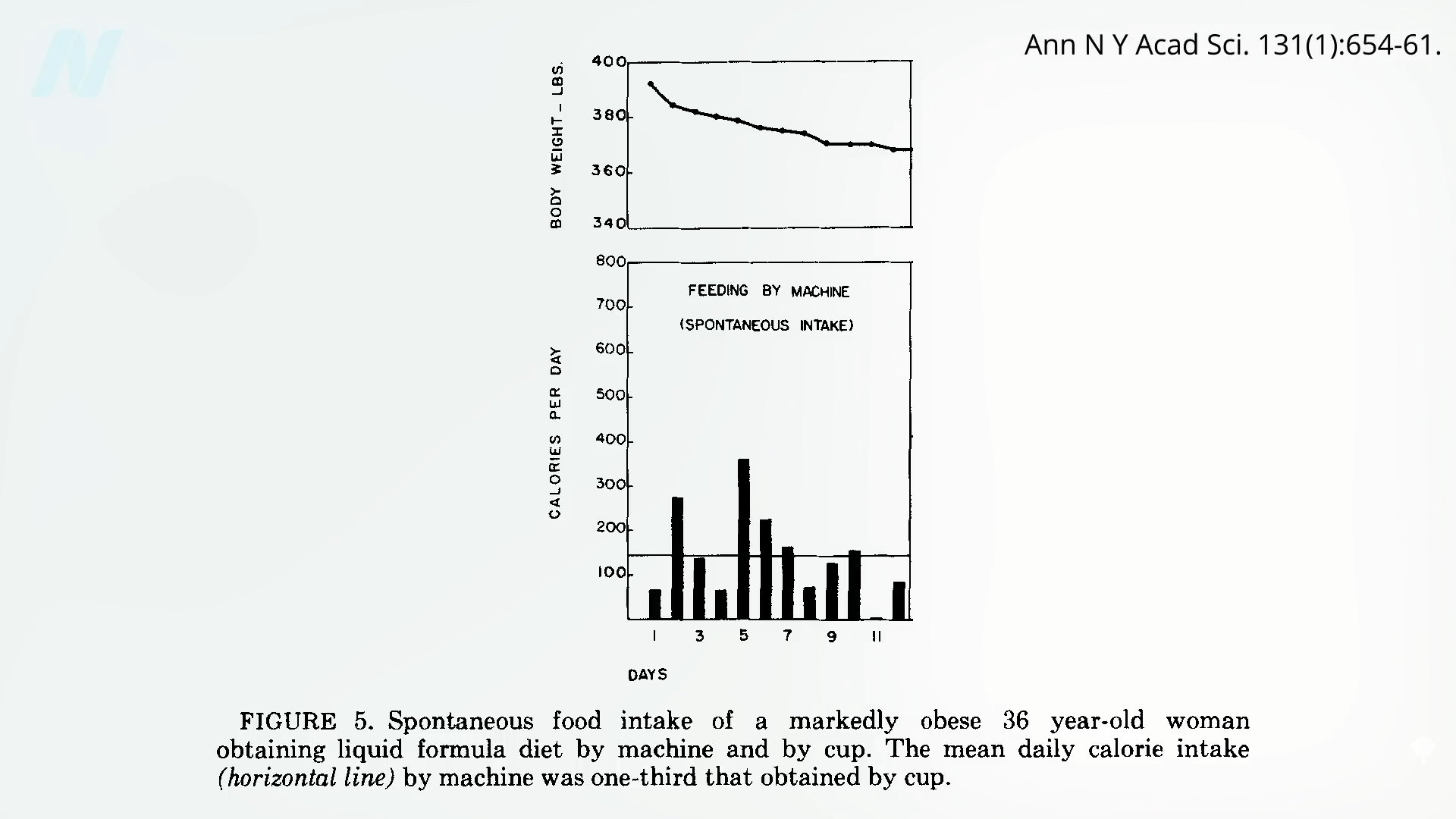
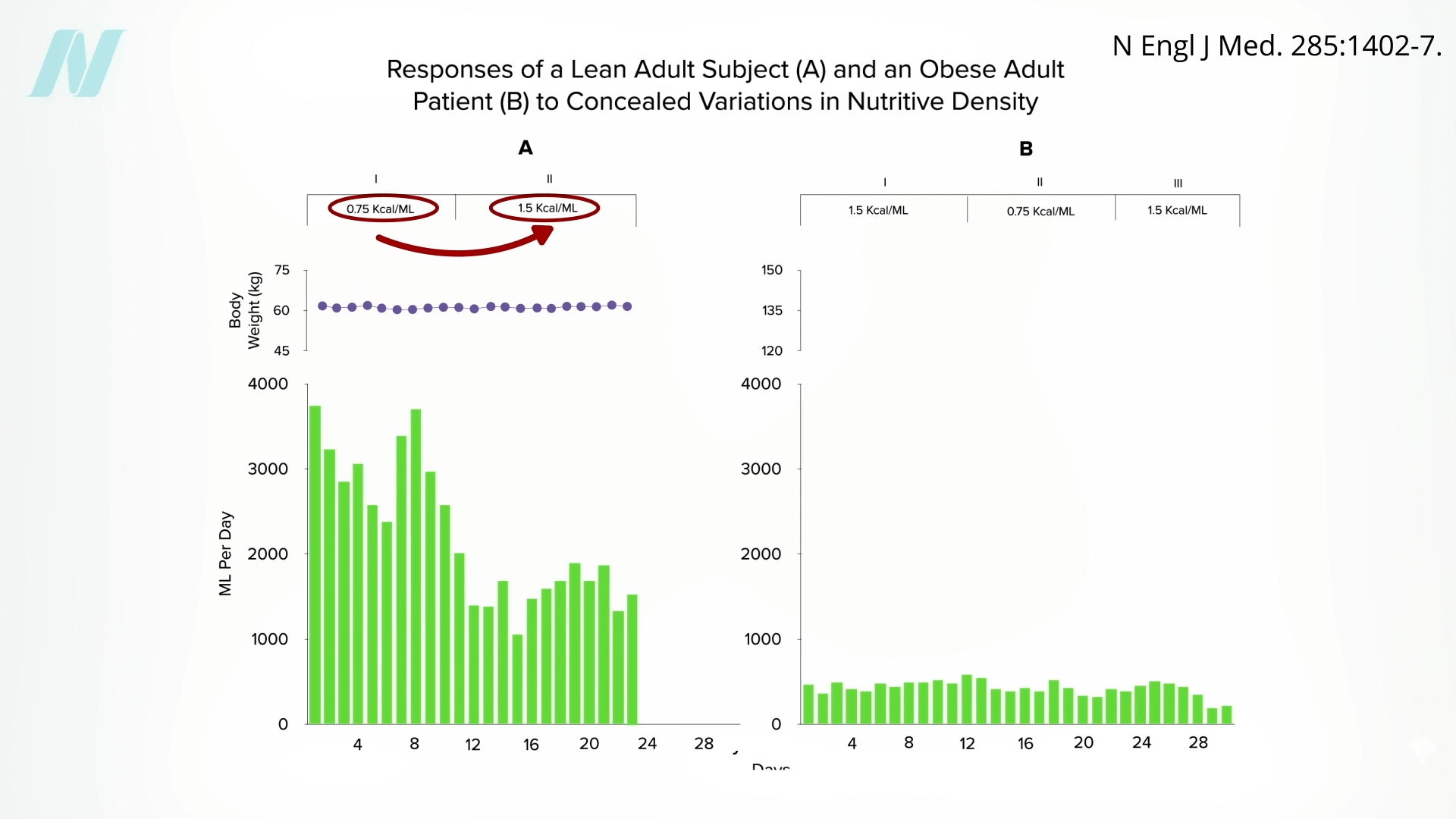 Might the brains of persons with obesity somehow
Might the brains of persons with obesity somehow 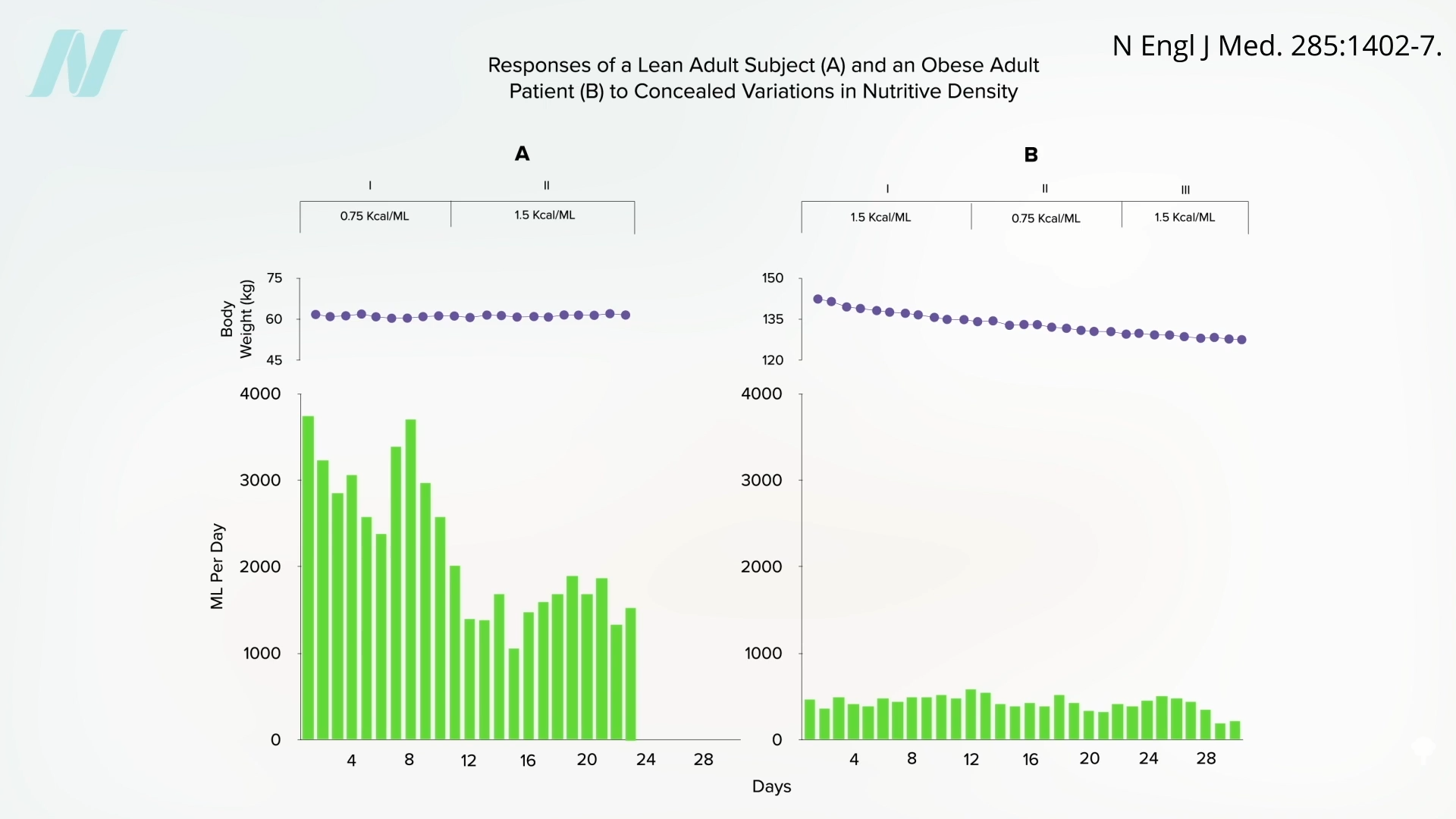 It would be interesting to see if they regained the ability to respond to changing calorie intake once they reached their ideal weight. Regardless, what can we apply from these remarkable studies to facilitate weight loss out in the real world? We’ll explore just that question next.
It would be interesting to see if they regained the ability to respond to changing calorie intake once they reached their ideal weight. Regardless, what can we apply from these remarkable studies to facilitate weight loss out in the real world? We’ll explore just that question next.