[ad_1]
The “fat gene” accounts for less than 1 percent of the differences in size between people.
To date, about a hundred genetic markers have been linked to obesity, but when you put them all together, overall, they account for less than 3 percent of the difference in body mass index (BMI) between people. You may have heard about the “fat gene,” called FTO, short for FaT mass and Obesity-associated). It’s the gene most strongly linked to obesity, but it explains less than 1 percent of the difference in BMI between people, a mere 0.34 percent.
As I discuss in my video The Role of Genes in the Obesity Epidemic, FTO codes for a brain protein that appears to affect our appetite. Are you one of the billion people who carry the FTO susceptibility genes? It doesn’t matter because it only appears to result in a difference in intake of a few hundred extra calories a year. The energy imbalance that led to the obesity epidemic is on the order of hundreds of calories a day, and that’s the gene known so far to have the most effect. The chances of accurately predicting obesity risk based on FTO status is “only slightly better than tossing a coin.” In other words, no, those genes don’t make you look fat.
When it comes to obesity, the power of our genes is nothing compared to the power of our fork. Even the small influence the FTO gene does have appears to be weaker among those who are physically active and may be abolished completely in those eating healthier diets. FTO only appears to affect those eating diets higher in saturated fat, which is predominantly found in meat, dairy, and junk food. Those eating more healthfully appear to be at no greater risk of weight gain, even if they inherited the “fat gene” from both of their parents.
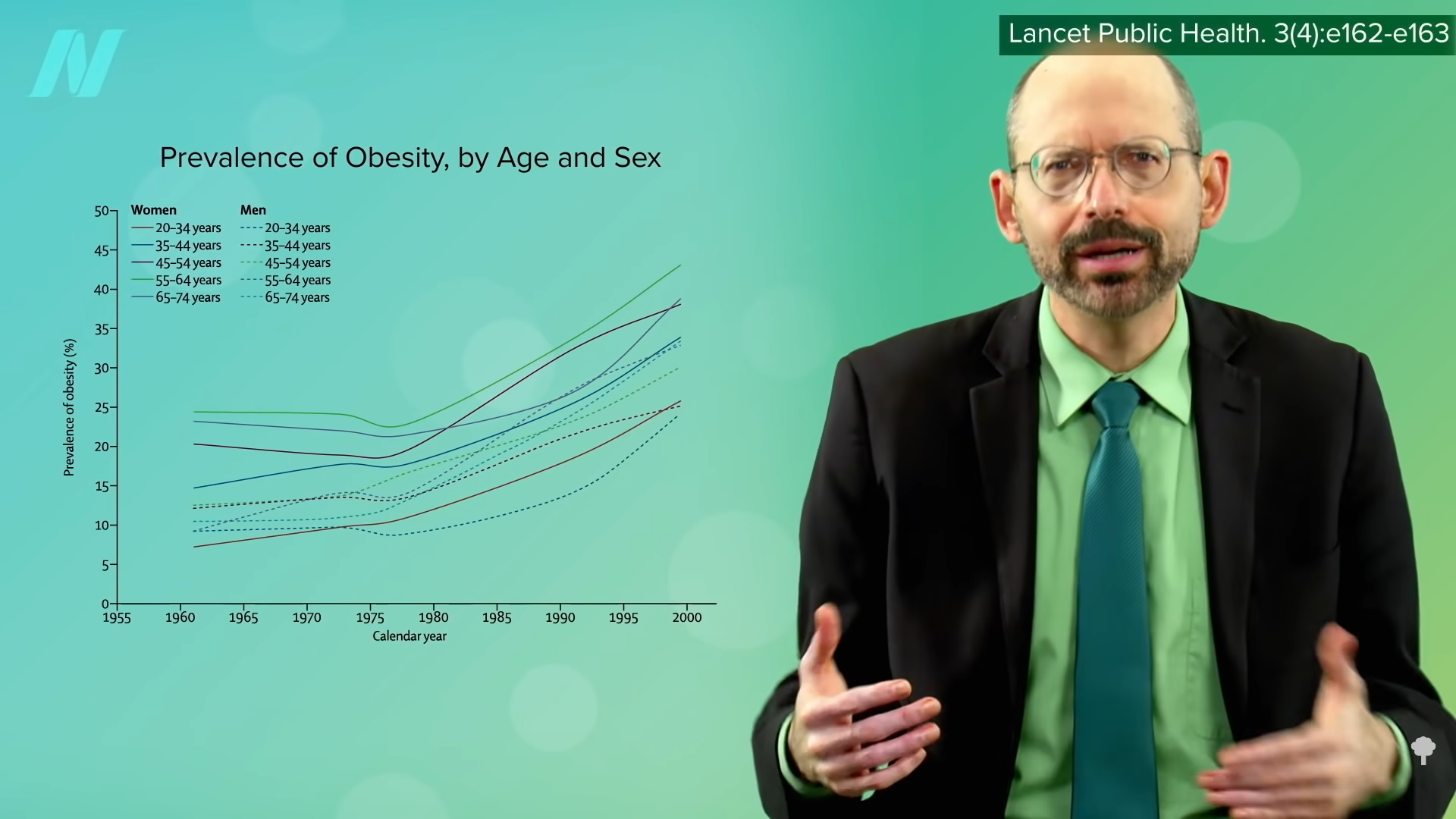
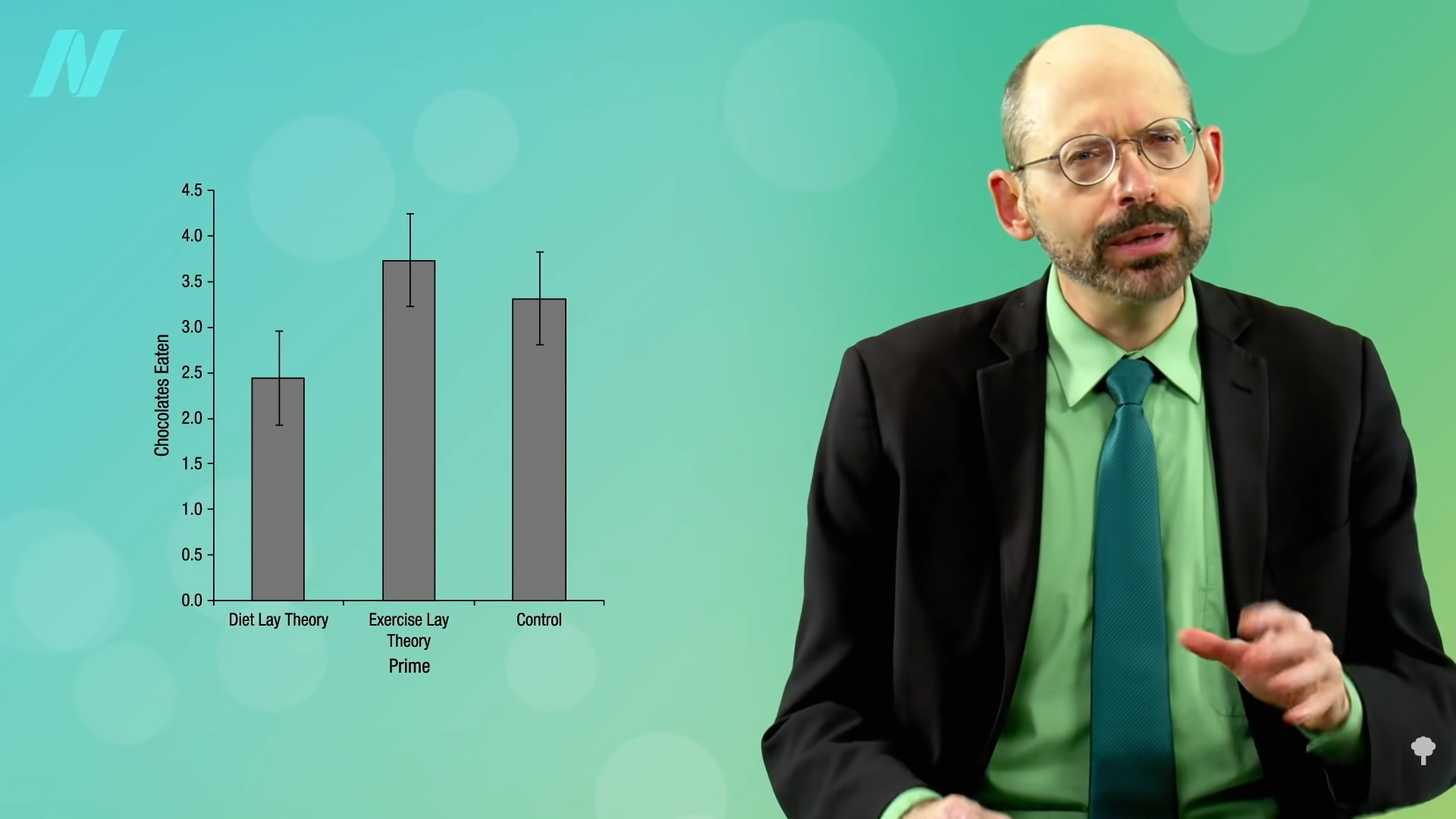
Physiologically, FTO gene status does not appear to affect our ability to lose weight. Psychologically, knowing we’re at increased genetic risk for obesity may motivate some people to eat and live more healthfully, but it may cause others to fatalistically throw their hands up in the air and resign themselves to thinking that it just runs in their family, as you can see in the graph below and at 2:11 in my video. Obesity does tend to run in families, but so do lousy diets.
Comparing the weight of biological versus adopted children can help tease out the contributions of lifestyles versus genetics. Children growing up with two overweight biological parents were found to be 27 percent more likely to be overweight themselves, whereas adopted children placed in a home with two overweight parents were 21 percent more likely to be overweight. So, genetics do play a role, but this suggests that it’s more the children’s environment than their DNA.
One of the most dramatic examples of the power of diet over DNA comes from the Pima Indians of Arizona. As you can see in the graph below and at 3:05 in my video, they not only have among the highest rates of obesity, but they also have the highest rates of diabetes in the world. This has been ascribed to their relatively fuel-efficient genetic makeup. Their propensity to store calories may have served them well in times of scarcity when they were living off of corn, beans, and squash, but when the area became “settled,” their source of water, the Gila River, was diverted upstream. Those who survived the ensuing famine had to abandon their traditional diet to live off of government food programs and chronic disease rates skyrocketed. Same genes, but different diet, different result.
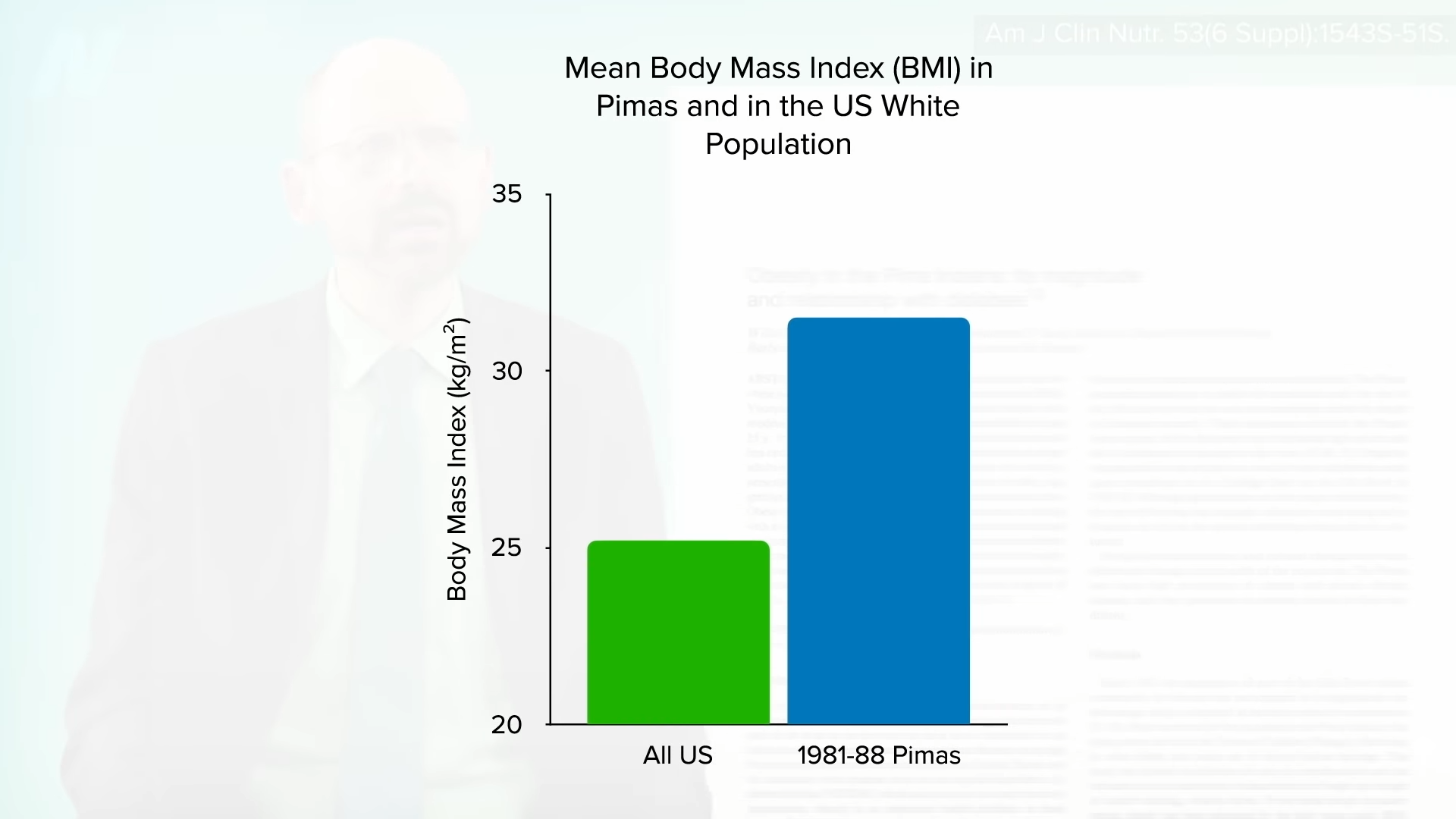
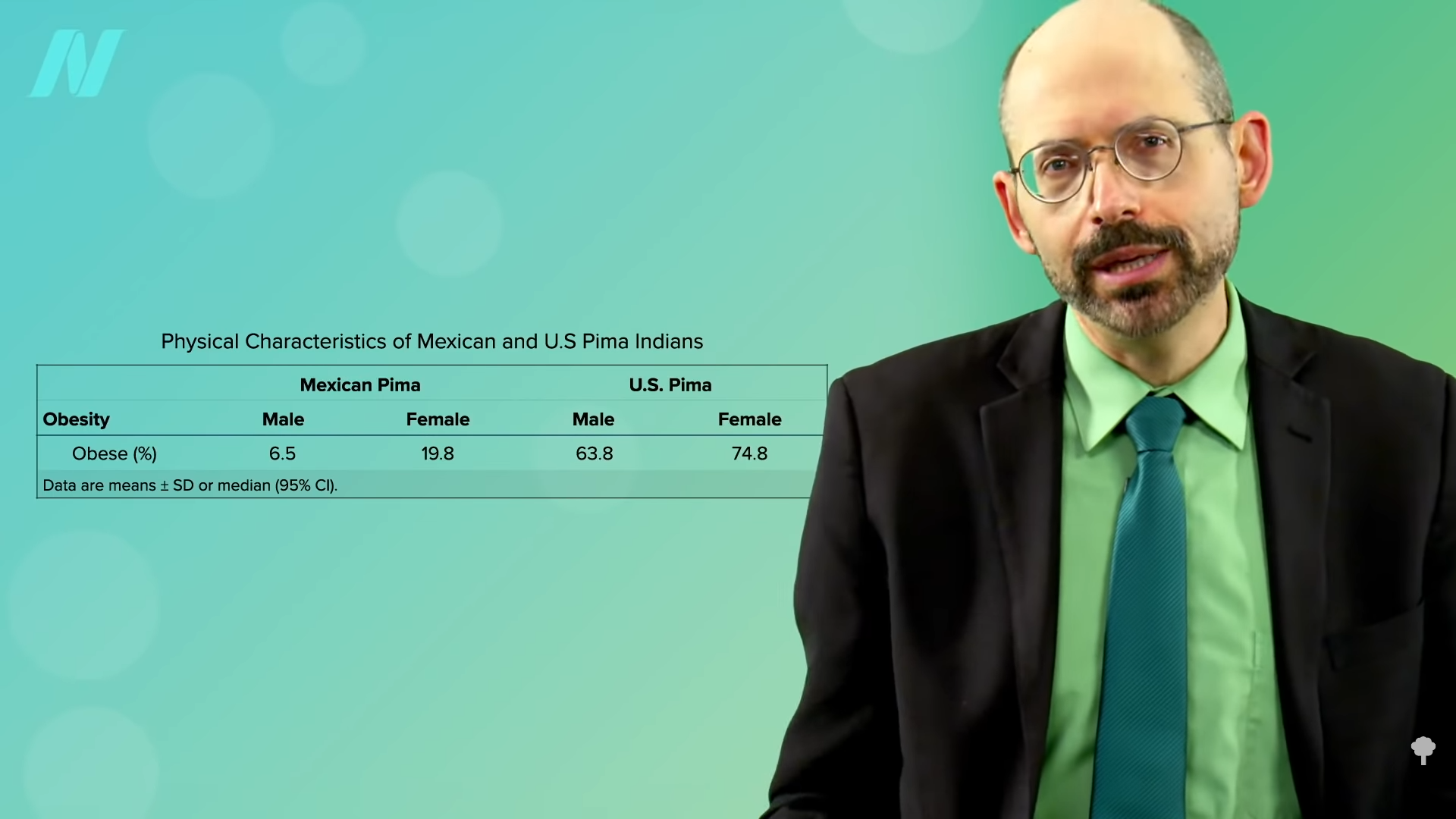
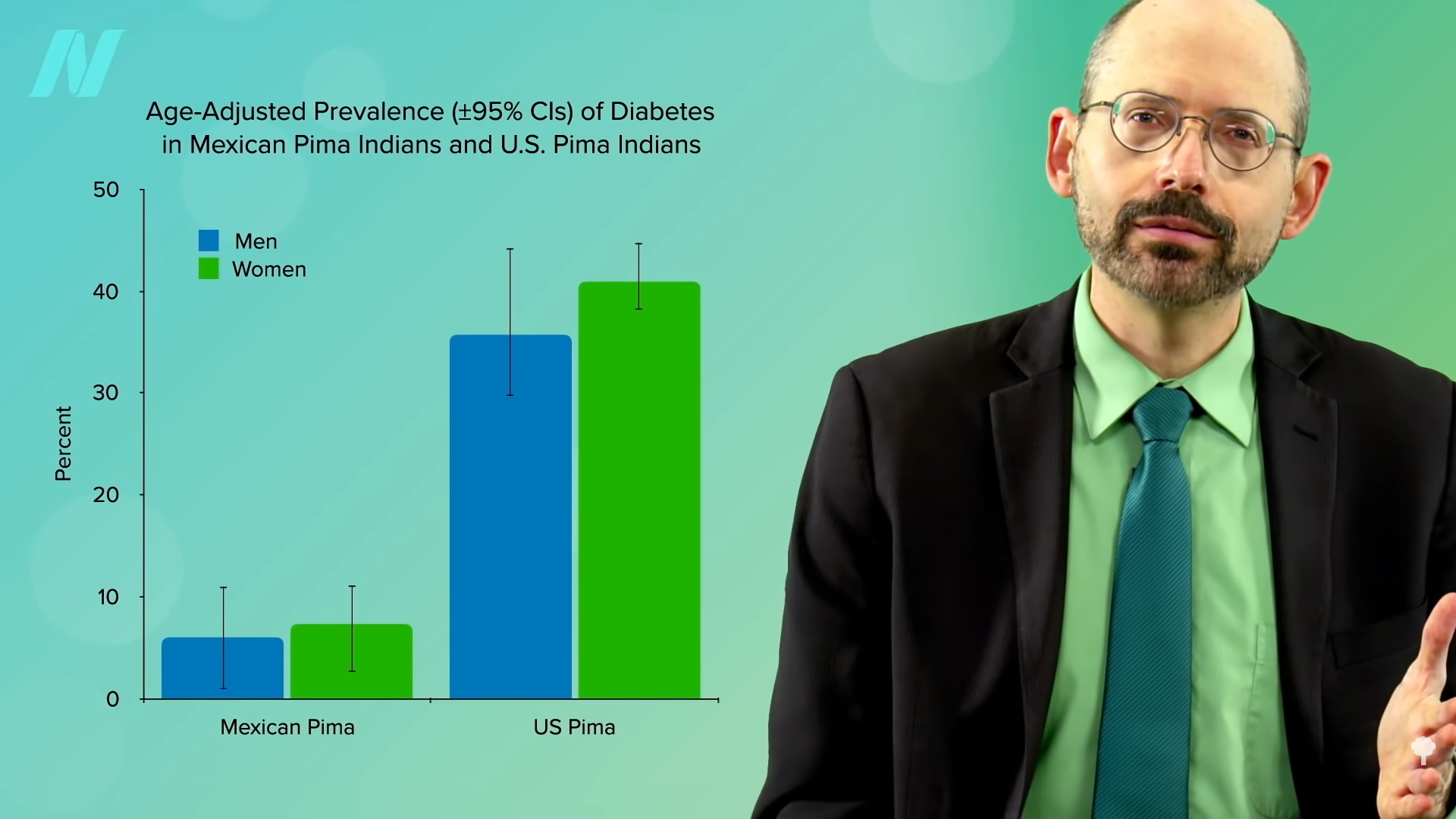
In fact, a natural experiment was set up. The Pima living over the border in Mexico come from the same genetic pool but were able to maintain more of their traditional lifestyle, sticking with their main staples of beans, wheat flour tortillas, and potatoes. Same genes, but seven times less obesity and about four times less diabetes. You can see those graphs below and at 3:58 and 4:02 in my video. Genes may load the gun, but diet pulls the trigger.
Of course, it’s not our genes! Our genes didn’t suddenly change 40 years ago. At the same time, though, in a certain sense, it could be thought of as all in our genes. That’s the topic of my next video The Thrifty Gene Theory: Survival of the Fattest.
This is the second in an 11-video series on the obesity epidemic. If you missed the first one, check out The Role of Diet vs. Exercise in the Obesity Epidemic.
[ad_2]
Michael Greger M.D. FACLM
Source link

















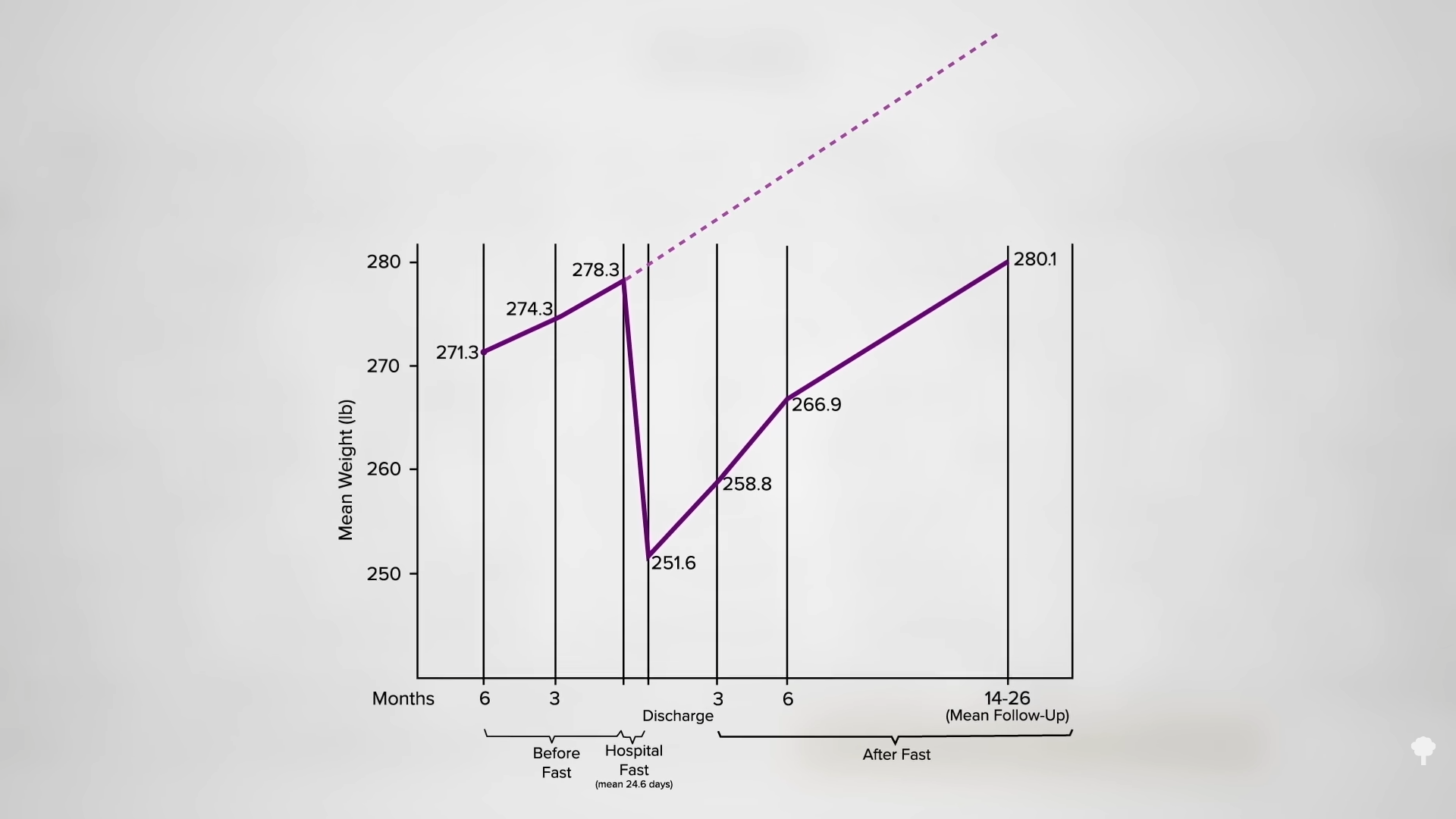
 Medically-supervised fasting has
Medically-supervised fasting has “
“
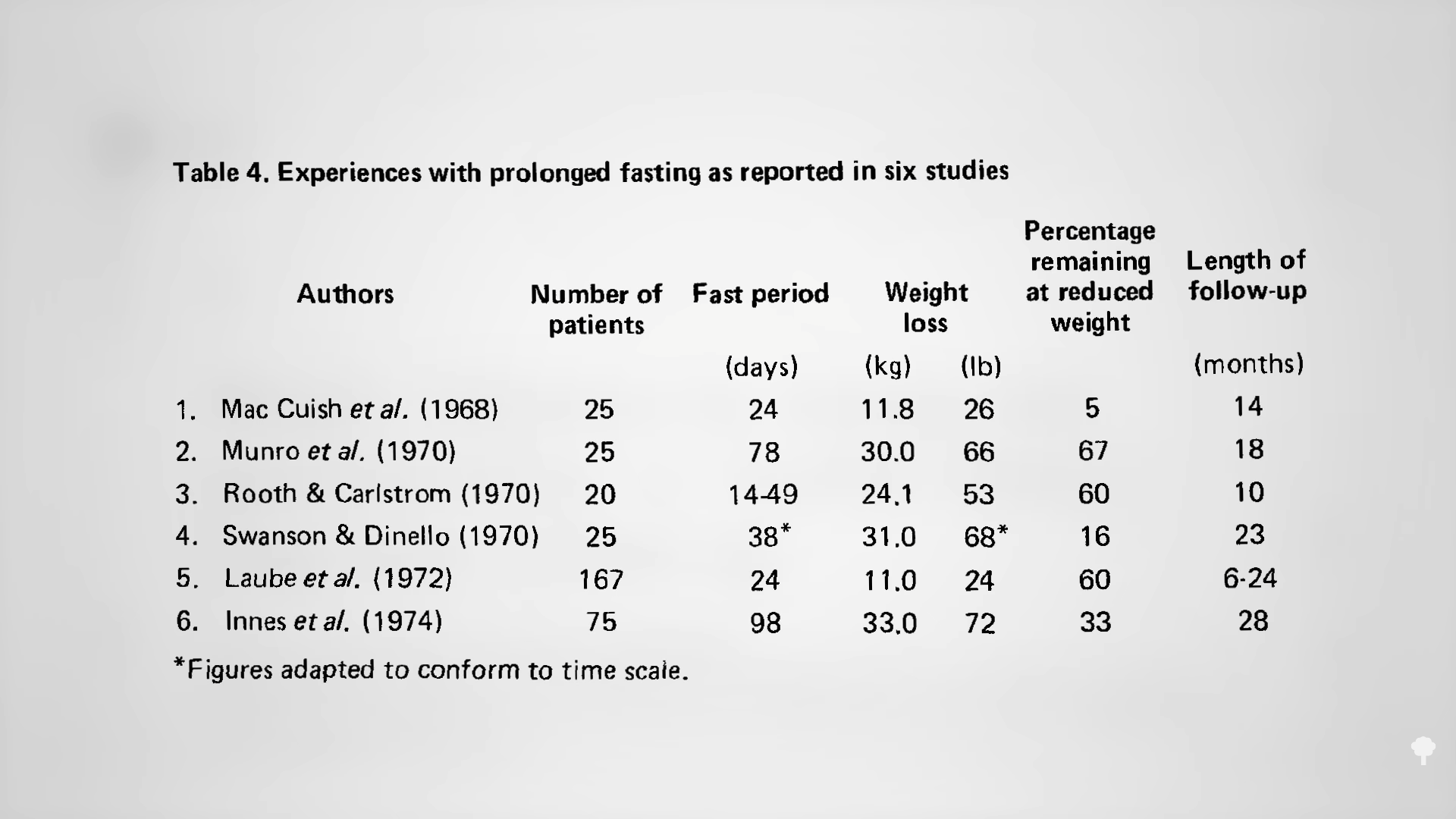
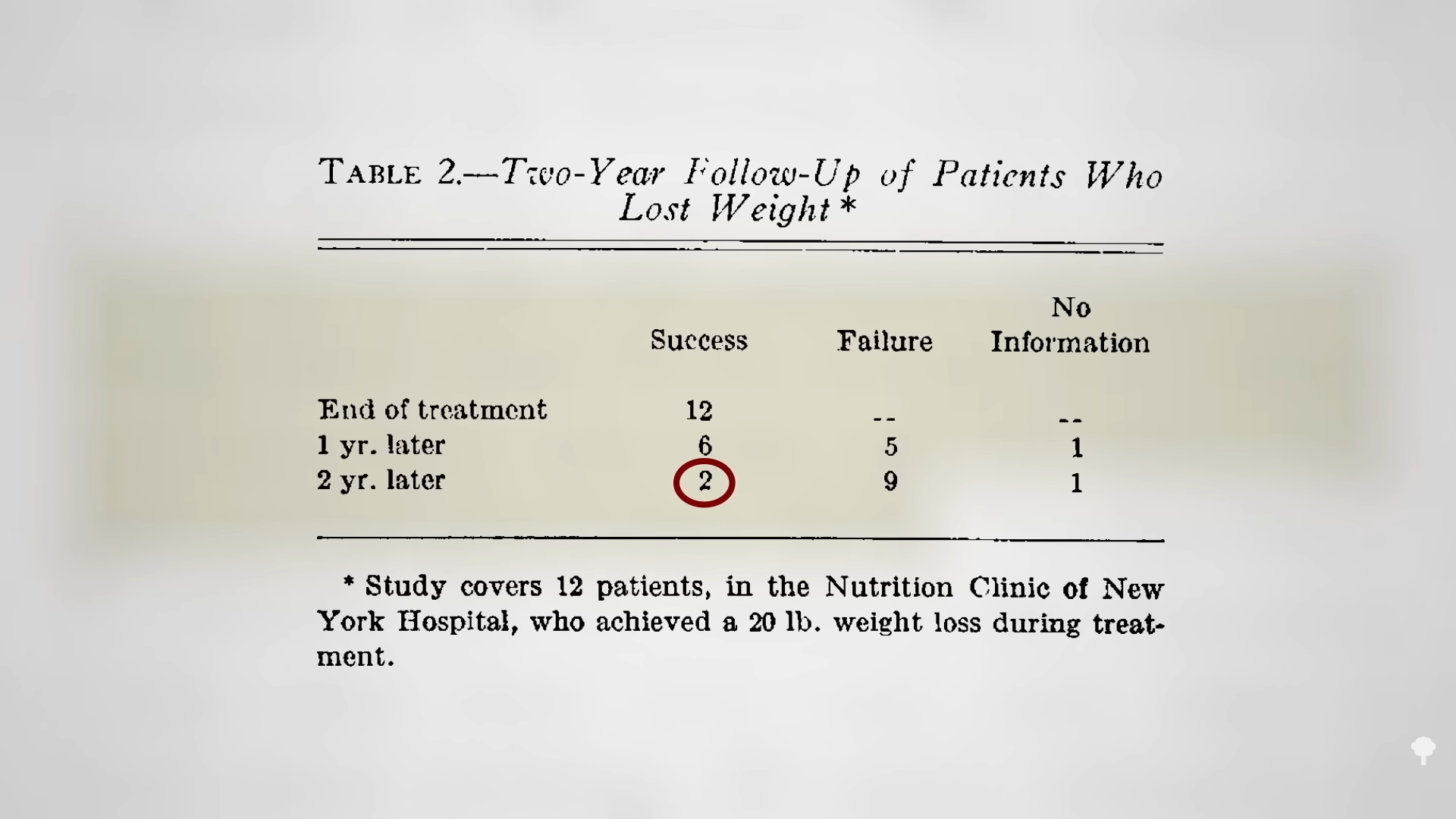
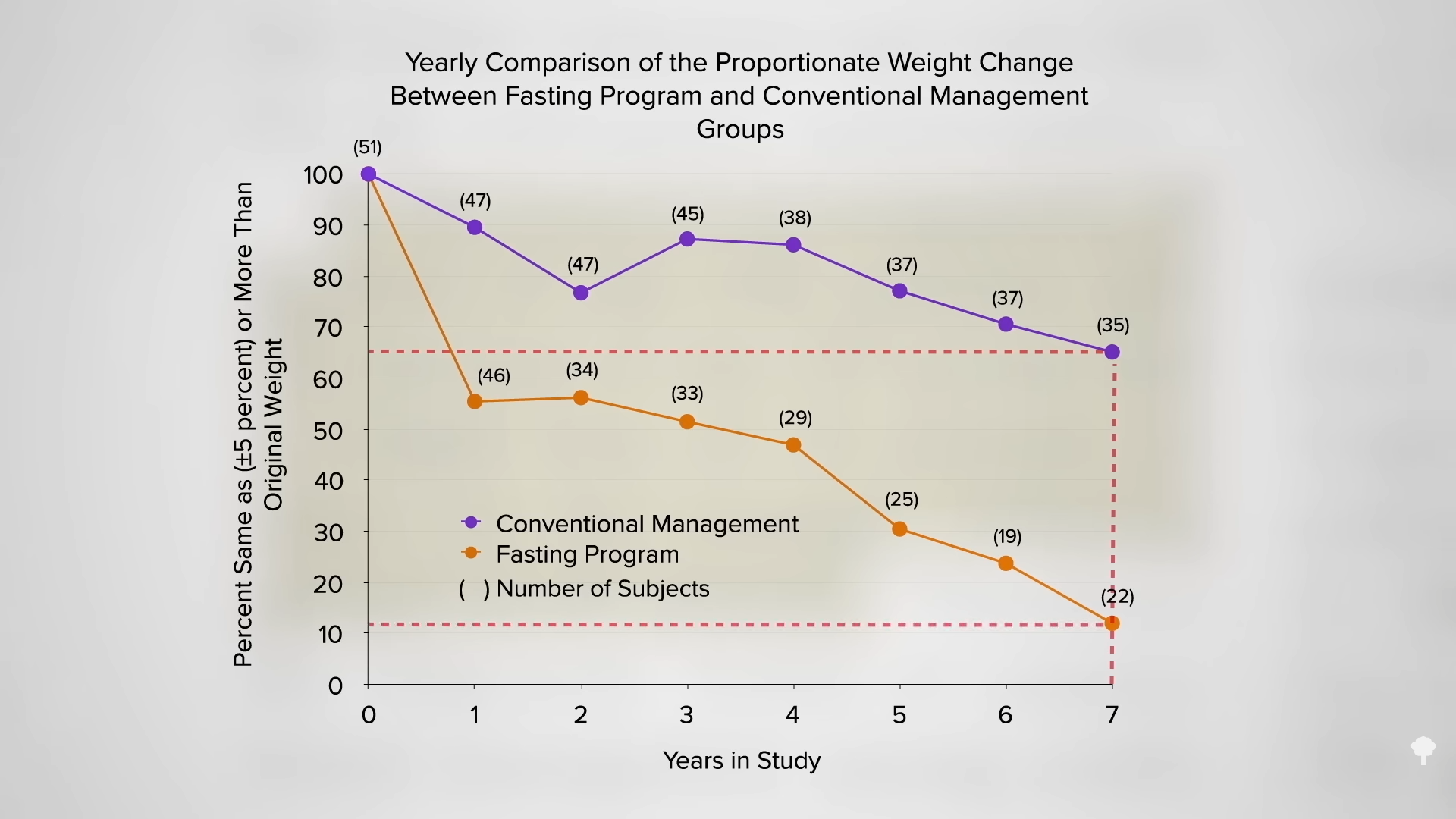
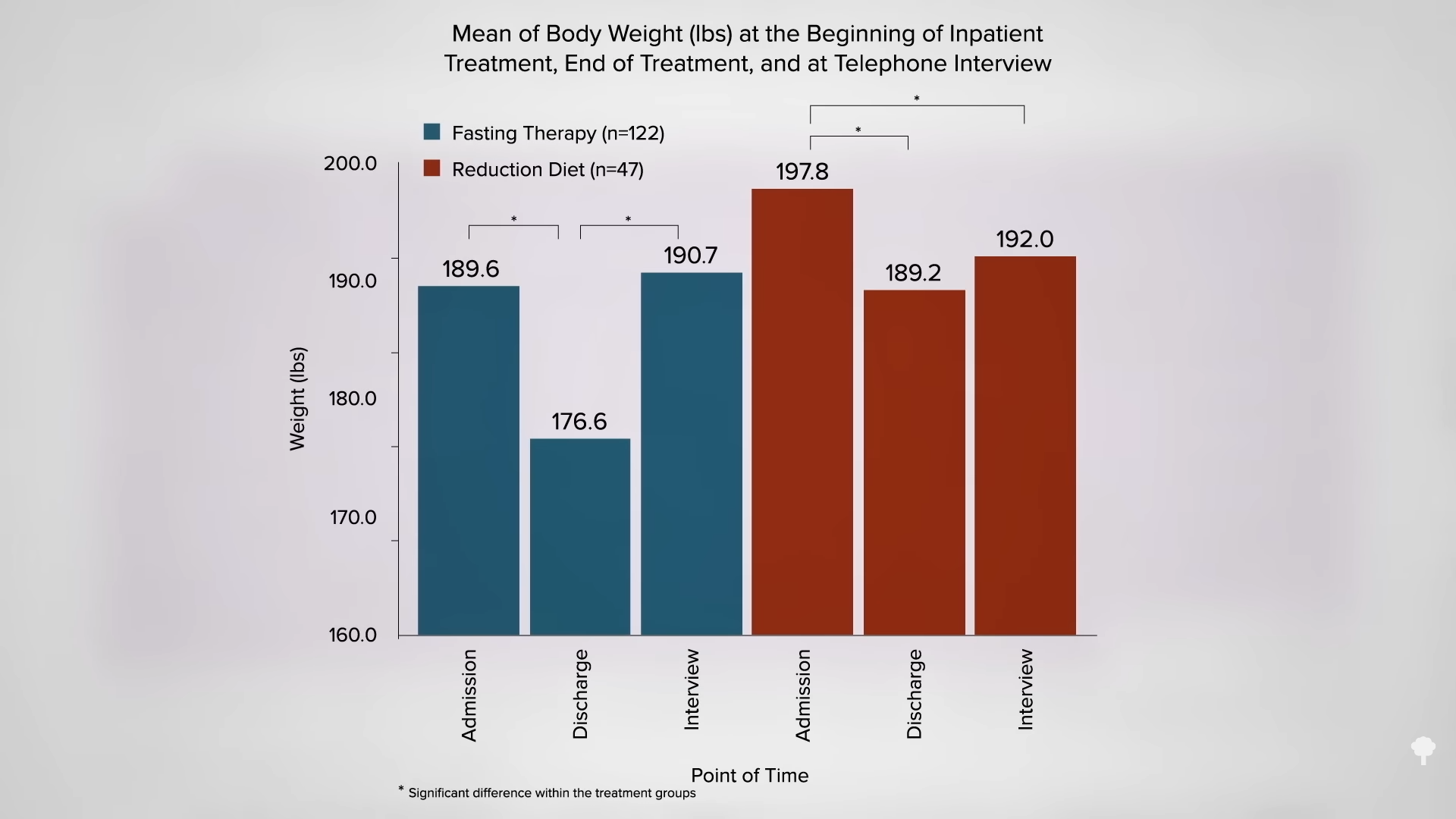
 What happened nine years later? “Therapeutic Fasting in Morbid Obesity”
What happened nine years later? “Therapeutic Fasting in Morbid Obesity” 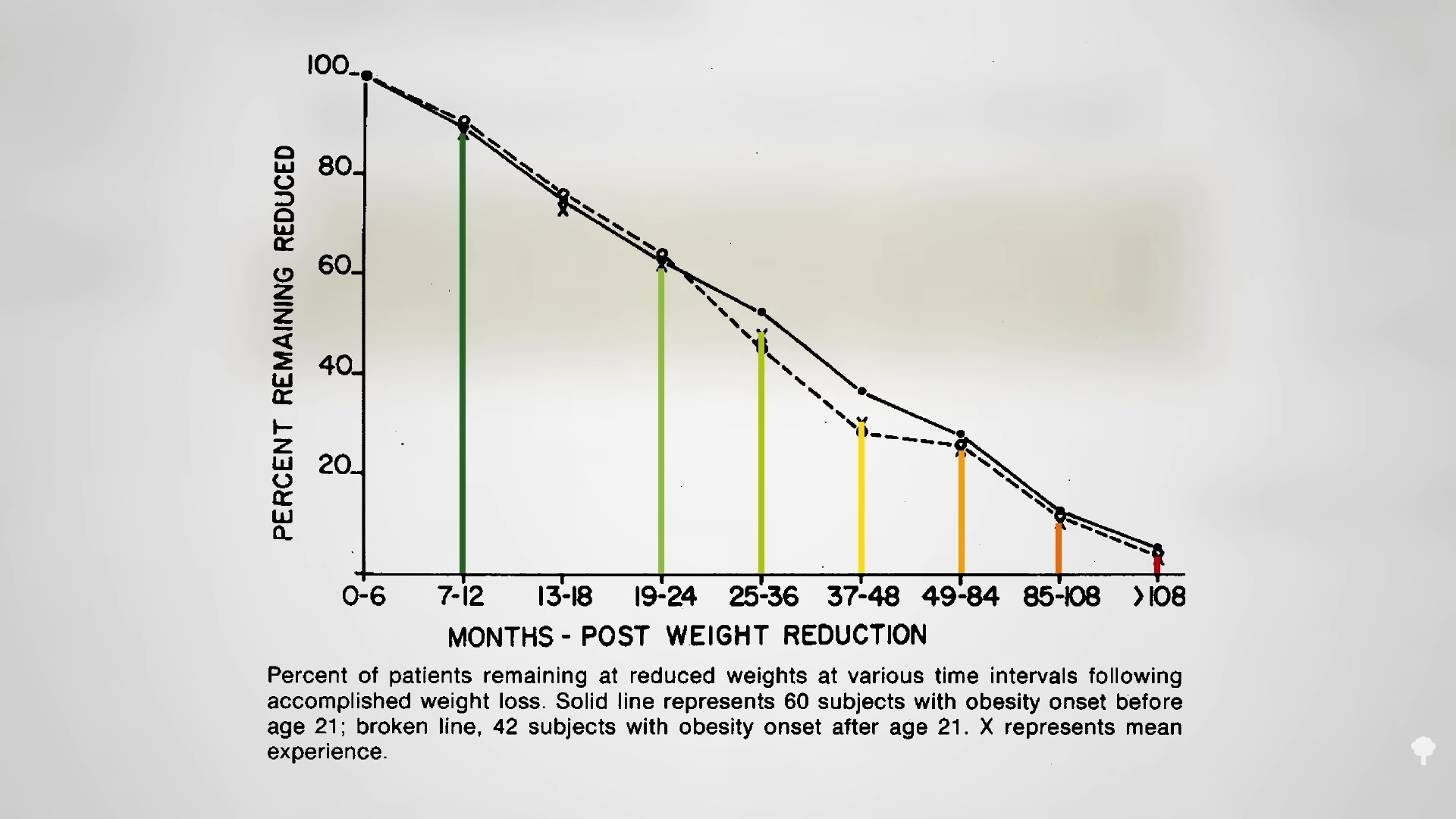 The small minority for whom fasting
The small minority for whom fasting 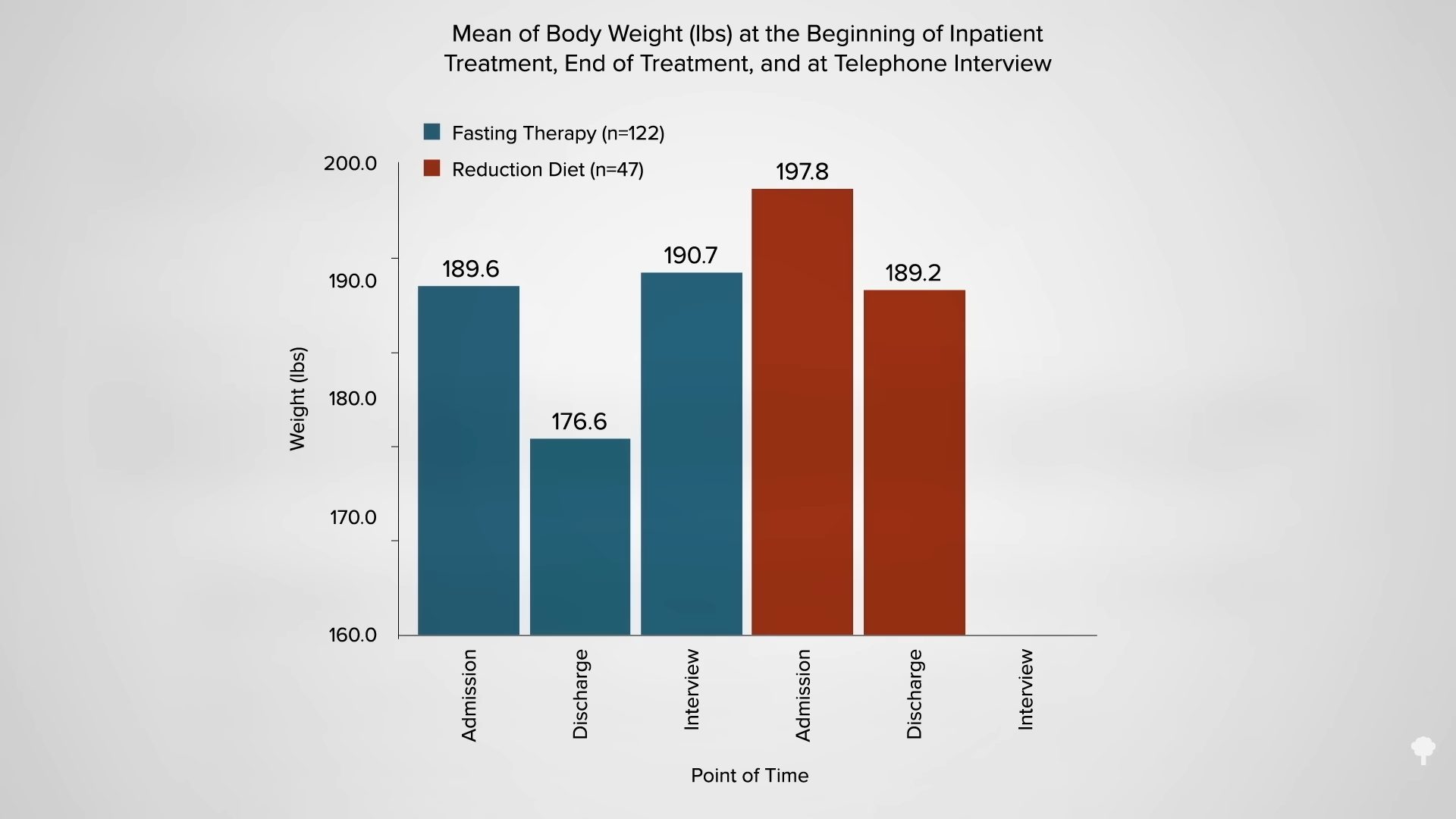
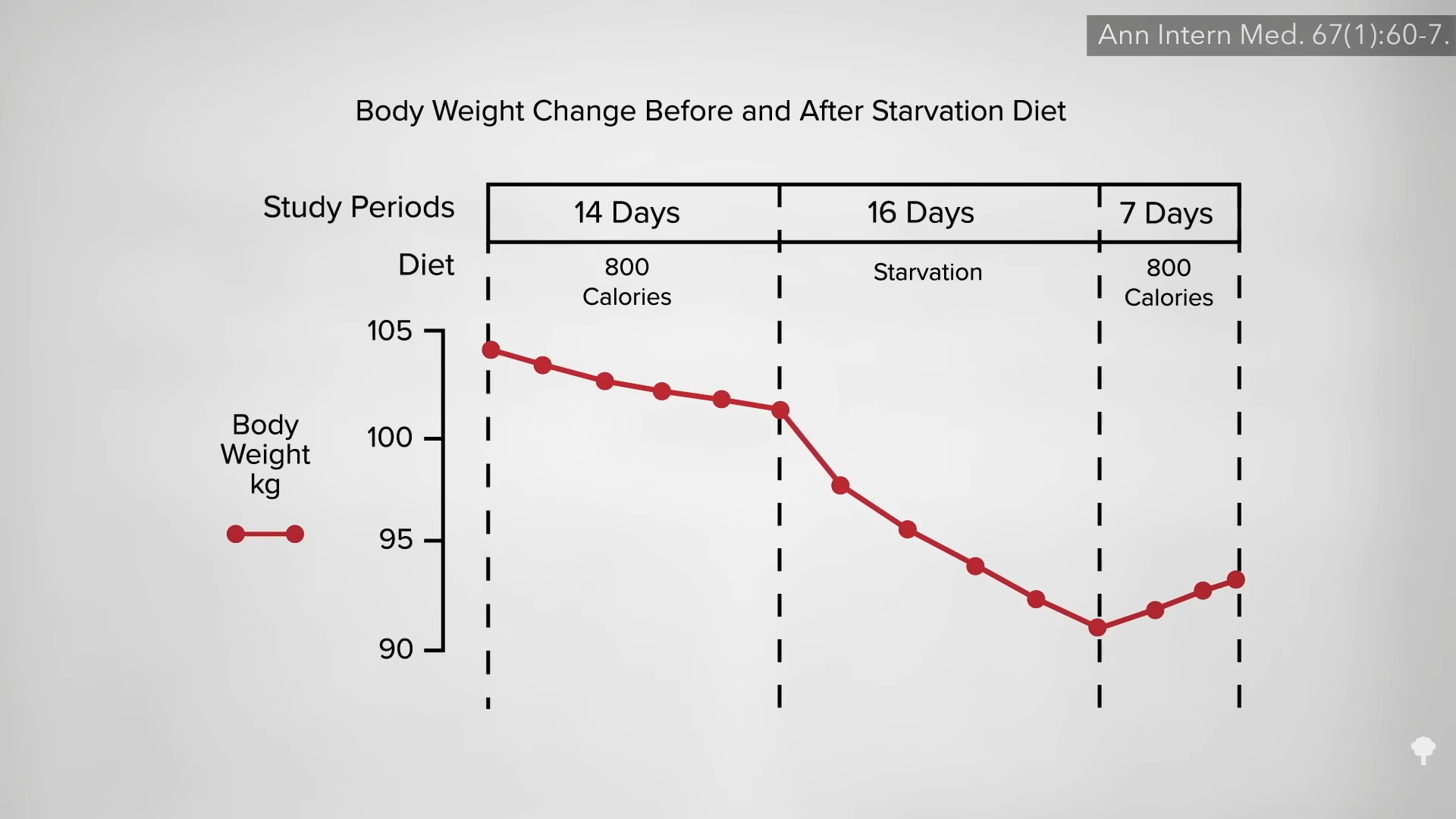
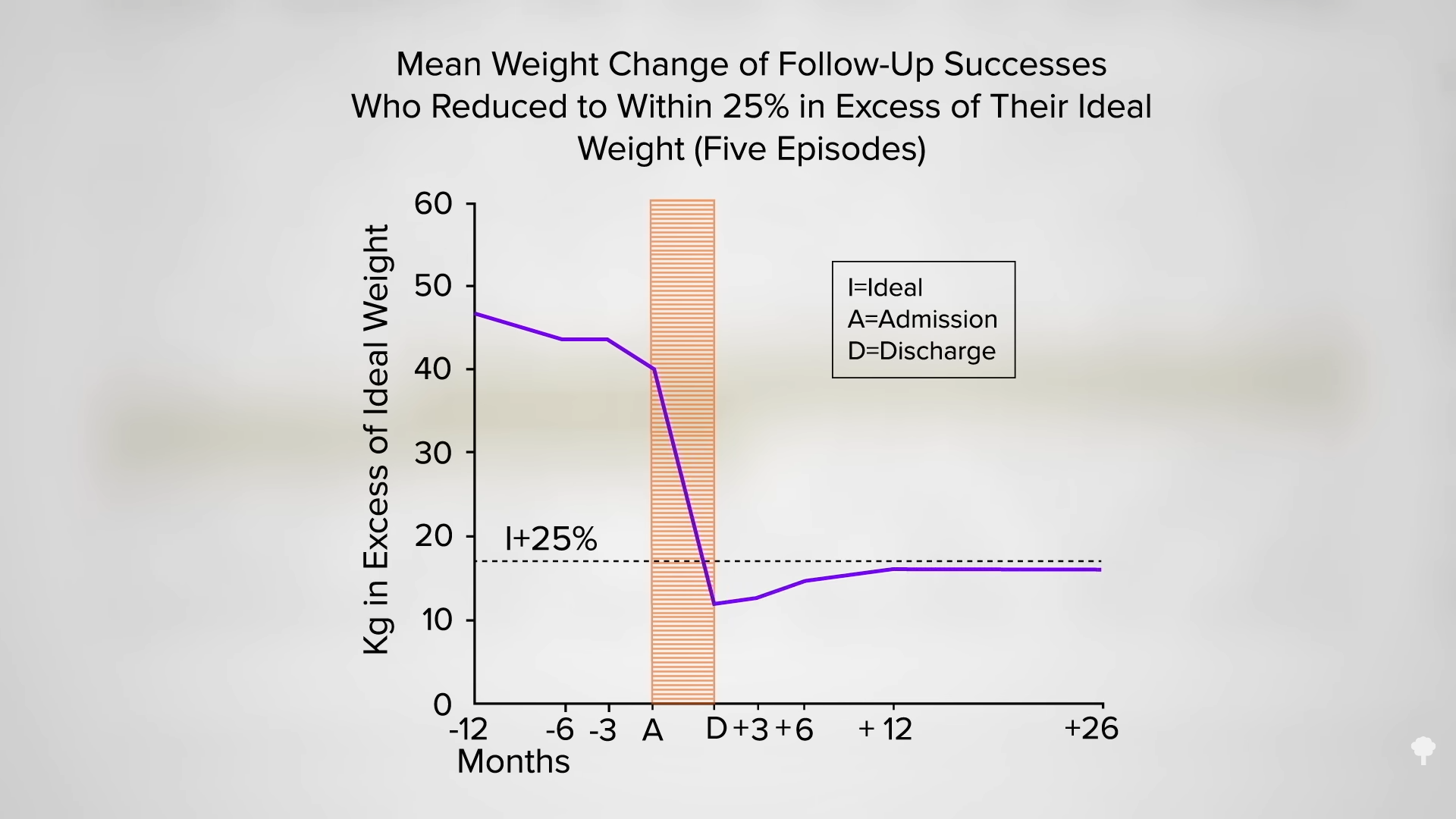
 This is the follow-up to
This is the follow-up to