SLOVIANSK, Ukraine — Mykola Soloviov, 88, is a painter the world does not know. His landscapes of eastern Ukraine, records of a lost time, lie tucked away in a modest home under threat of Russian attack.
Soloviov can’t hear or walk and barely speaks. Disabled since a 2017 stroke, he spends his days bedridden in an apartment in Sloviansk, a city 25 kilometers (15 miles) from the front line in the region of Donetsk.
Waves of Russian missile attacks have continued to pound civilian areas across Ukraine as the war approaches its second anniversary next month, killing scores of Ukrainian civilians, often in their own homes. Eastern Ukraine, where troops live among the civilian population, is often hit the hardest.
But his wife, Liudymla, doesn’t want Mykola and his paintings to die in anonymity. She wants the world to know he’s not just another civilian caught in the middle of a war.
From the sofa where he lies motionless for much of the day, Mykola’s lively eyes are fixed on the window, his only view into the changing world he can no longer comprehend.
He’d paint the same scenes again and again. “It’s not about what you paint, it’s about how you paint it,” he used to tell his wife when she asked why.
Employed for much of his life as a painter in a factory, Mykola would spend hours by the window, gazing at the view and producing his works. Liudmyla, 78, held up a painting of that view: expertly layered soft colors bring out the purity of fresh winter snow.
On Saturday, the window was a hole framed by shattered glass, showing emergency crews cleaning up debris from the kindergarten across the yard. Men in military fatigues picked their way across ground pockmarked by artillery craters and covered in debris left in the wake of a Russian air attack.
Earlier that day, a Russian Iskander missile hit a ceramics workshop a few meters away from the Soloviovs’ home, leveling it and shattering their windows.
The blast jolted Liudymla awake, who ran to her paralyzed husband’s side and covered him with blankets as bitterly cold air wafted in.
“How can I feel? There is no joy in my life,” she said. “We are living on needles.” Her mind is occupied with all the things she must do for her husband. “I already changed (the blankets) and cooked for him, but it is cold inside my house.”
Sloviansk was never a luxurious place but it had allowed the couple to build a life. Both were the children of parents who moved to the city, known for its factories and riverside resorts, looking for work. Mykola’s family came from Russia, and Liudmyla’s from western Ukraine. When she was 16, she helped her father build them a house, making cinder blocks and planing boards after school.
On Saturday, she watched as workers sliced wooden boards to cover the holes left when the Russian attack shattered windows in dozens of apartments.
The Associated Press asked her about the explosion, but she changed the subject back to her husband’s paintings.
Liudmyla leafs through an old photo album containing images of Mykola’s paintings, the closest thing he has to an artist’s monograph, and then brings out a few of the originals she’s packed away for safe-keeping.
The paintings are unknown in Sloviansk, let alone the world. An old newspaper clipping contains a short article, describing a gallery of 60 of his works “charming” and “cleverly composed.”
Occasionally Mykola glances at her holding up his paintings, his face brightening.
“He has been drawing since childhood,” she said, “but stopped when he got sick.”
Soloviov often returned to the banks of the Kazenny Torets River to capture the changing seasons. “He was painting this river all the time, in summer, winter,” Liudymla said, her voice trailing off.
Mykola never aimed for realism, but his paintings captured the feeling of the pastoral landscapes, waterways and abundant greenery that defined Sloviansk’s landscape before the war. His loose and fluid brush work convey vibrancy and nostalgia for the passing seasons; vivid colors show his deep attachment to the land.
In 2014, Sloviansk was a flashpoint in the war against Russia’s invasion and one of the first cities to be seized by Moscow’s forces. Liudmyla’s sister was badly wounded by shrapnel during the fighting, dying of complications four years later.
By the time of Russia’s full-scale invasion in 2022, Mykola was too sick to be moved. His family, including his 49-year-old son Vitallii, stayed in Sloviansk, despite rapidly deteriorating conditions.
“There are places to go, for example, to western Ukraine or the Vinnytsia region, where my cousin lives,” Liudmyla said, “but it is very problematic because he cannot move around on his own. And now I don’t know what to do and where to go.”
In recent months a missile strike destroyed Vitallii’s home and he moved in with his parents.
“I will never leave my father,” he said, rolling cigarettes in the kitchen. “No matter the bombs.”
Outside, the screech of a saw cutting wood rang out. Her neighbors were still in line, waiting for their turn to seal off their homes from the elements.
Internet searches yield no results for Mykola’s name, or his art, but Liudymla preserves his paintings and his clippings as though they were important historical documents.
Just then, Vitallii tells her the heating system is damaged.
“One problem after another,” she sighs.
Soloviov has not uttered a word throughout the interview. His shriveled hand motions for the blanket, but his gaze is fixed on that window.






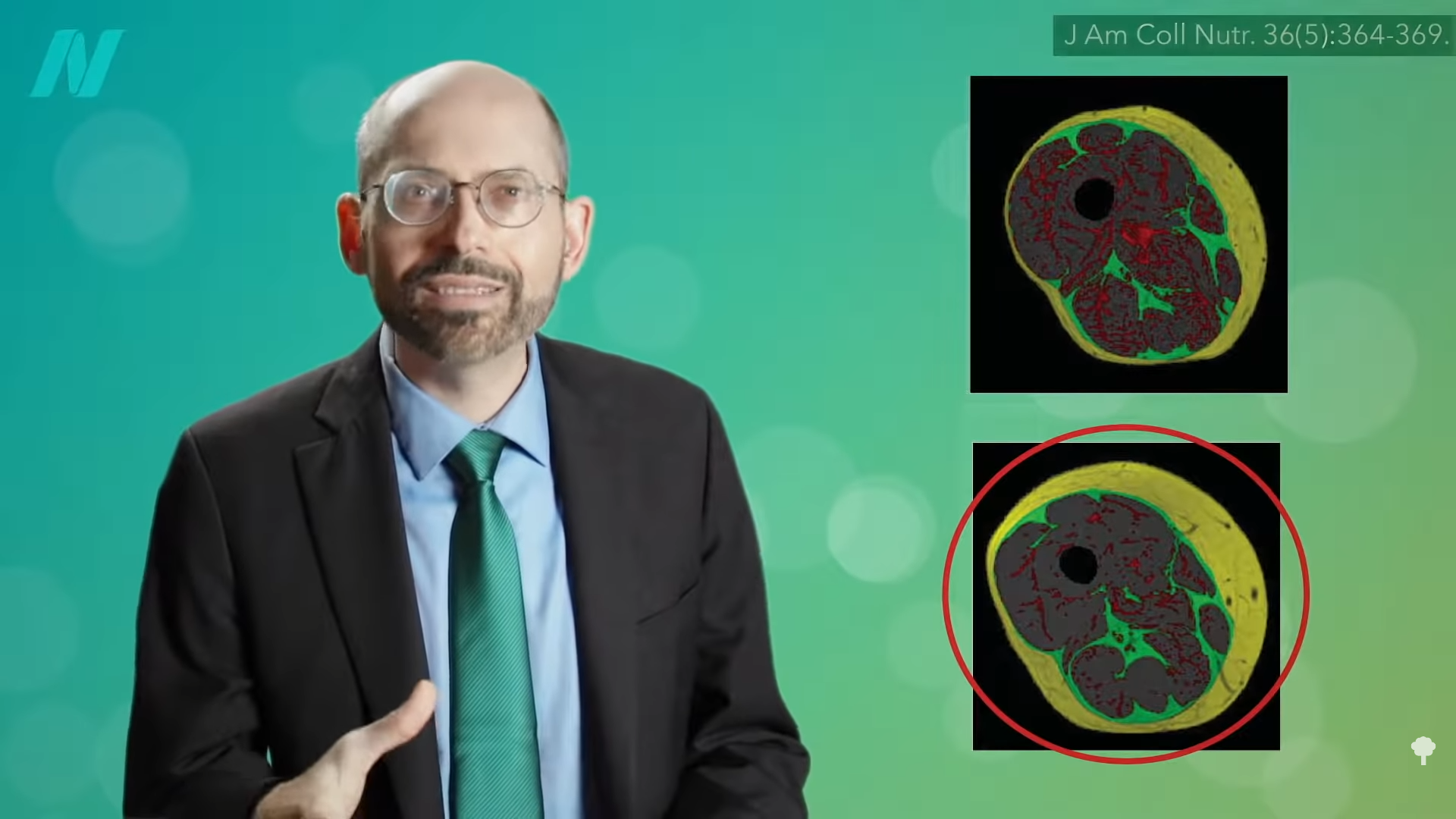






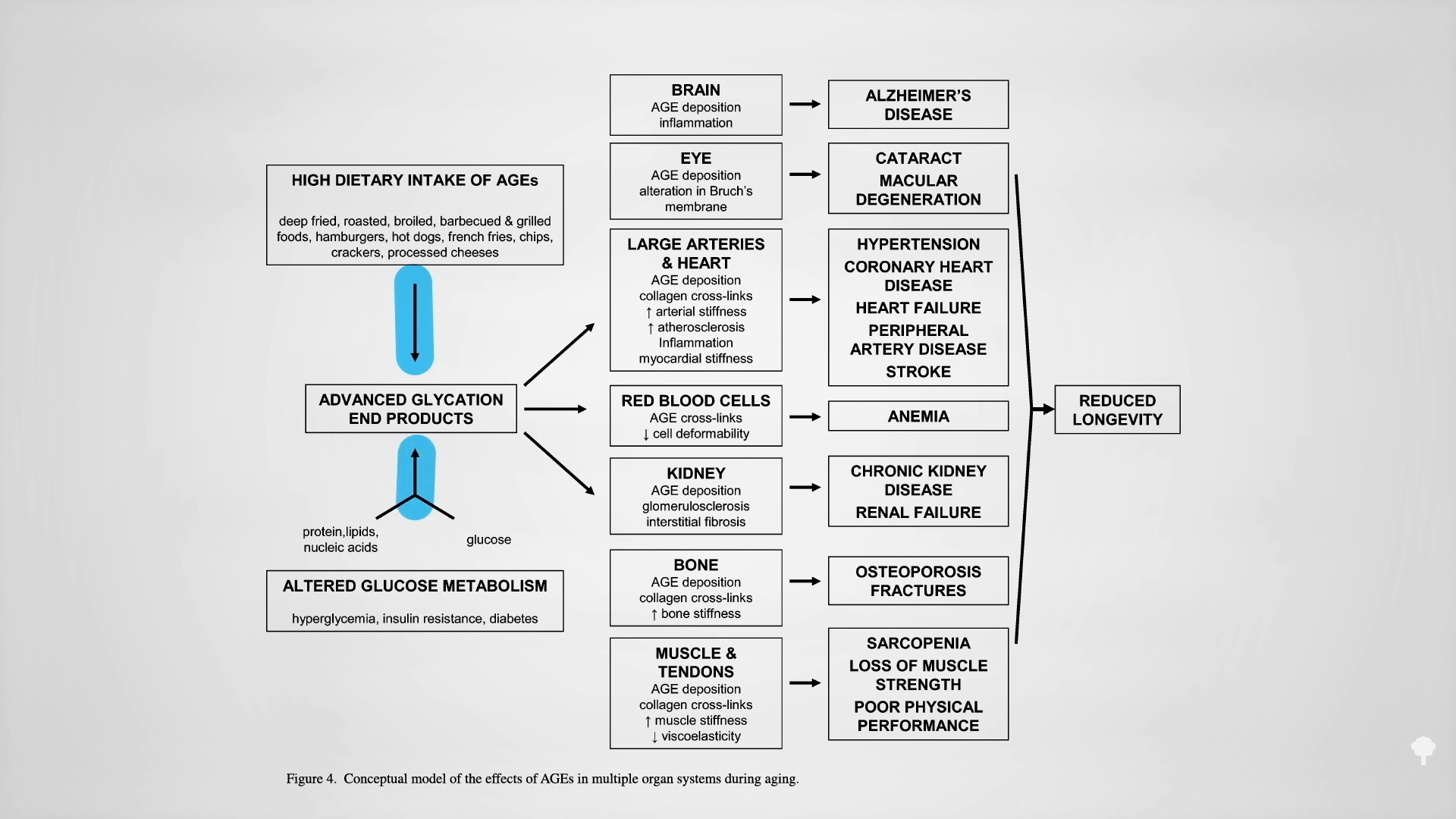
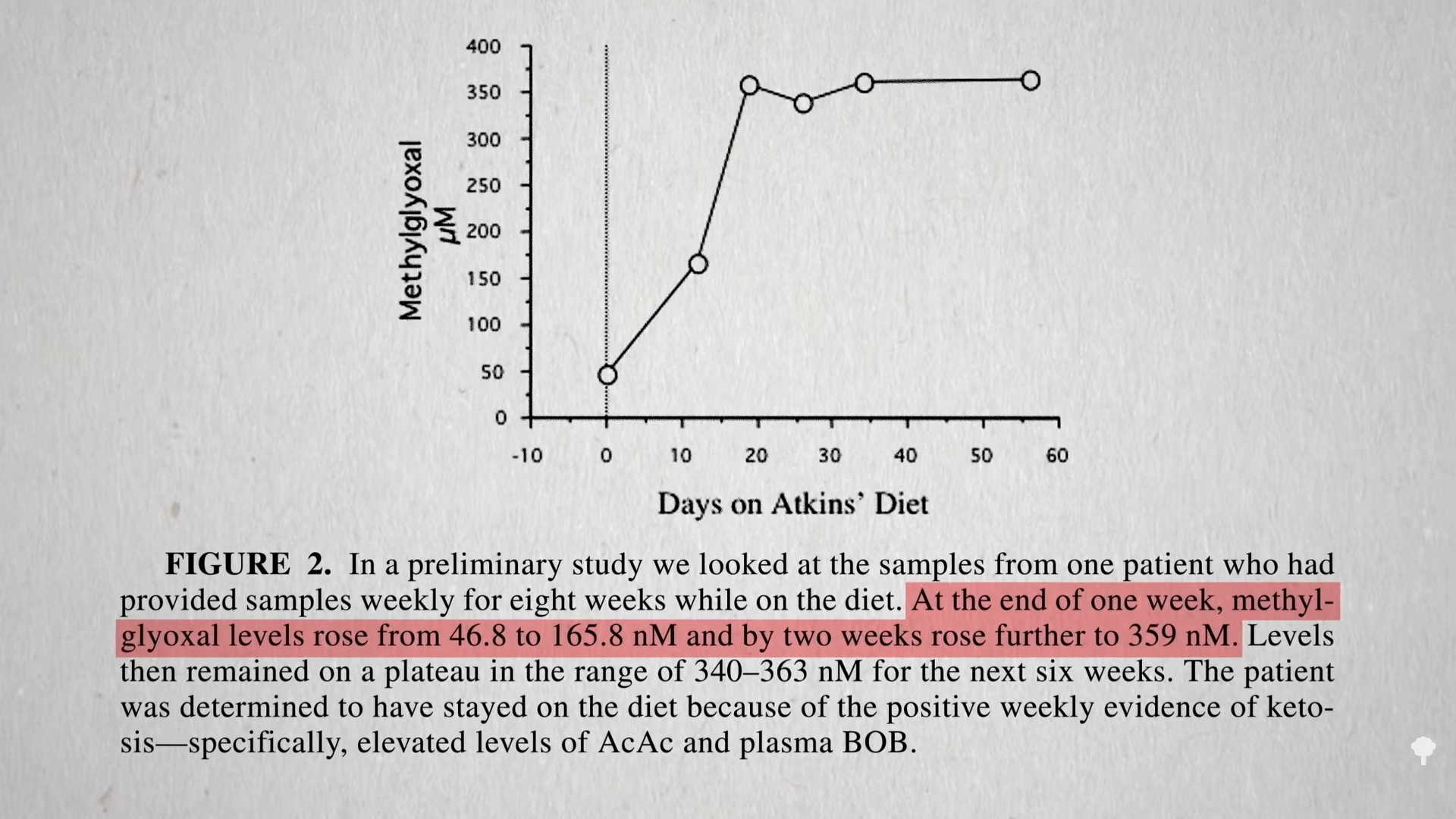
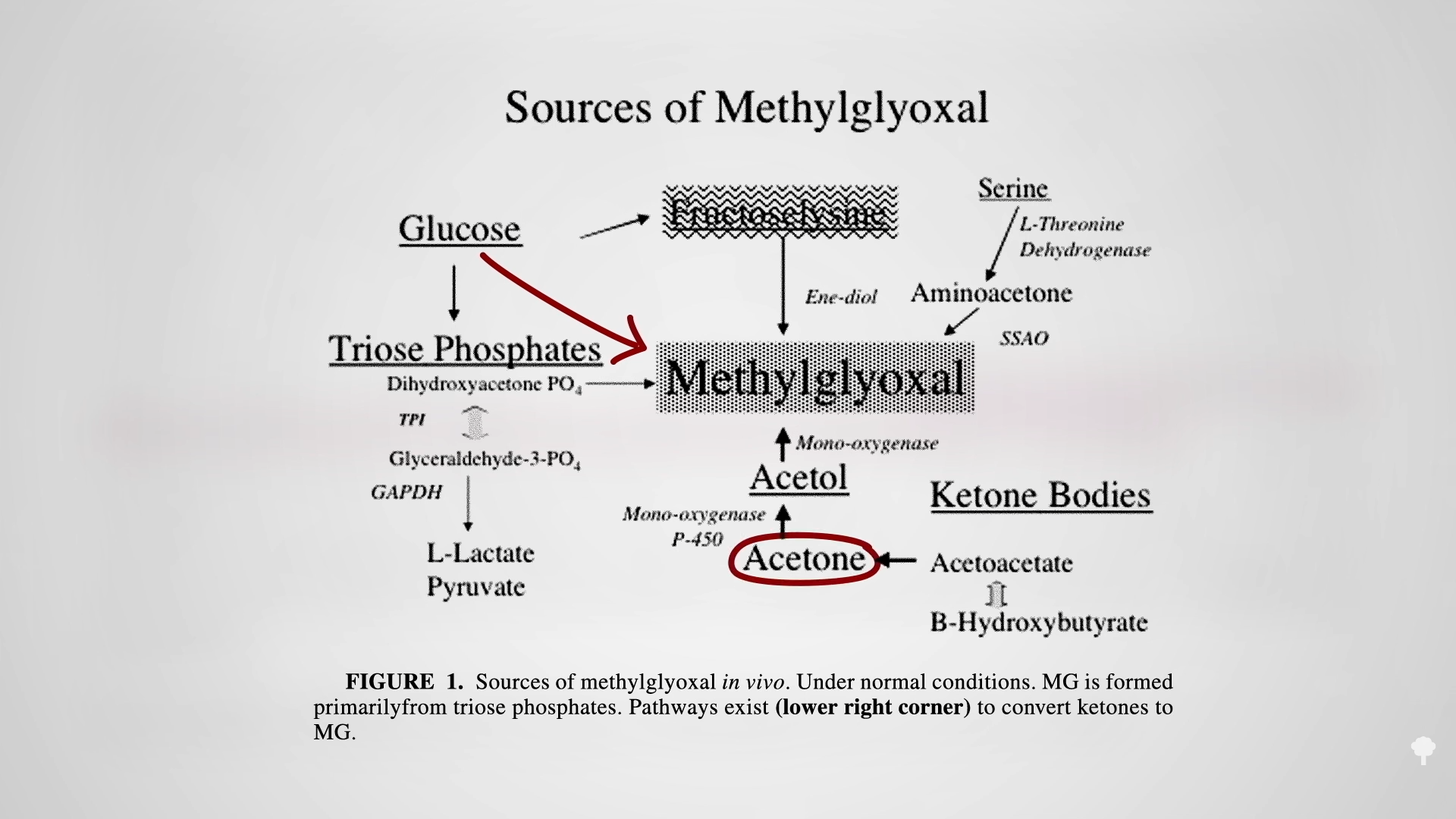
 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal