[ad_1]
CNN
—
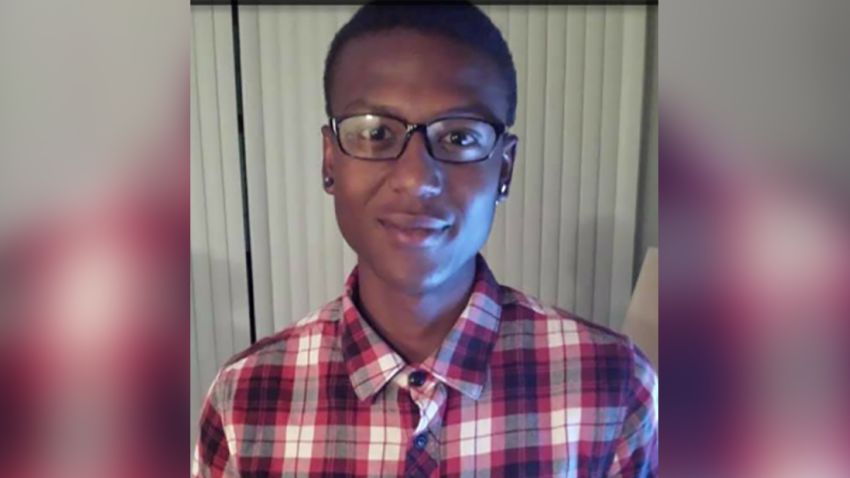
Three police officers and two paramedics have faced juries on charges of manslaughter and criminally negligent homicide stemming from the 2019 death of Elijah McClain in Aurora, Colorado.
But the path to court was anything but straightforward.
McClain, a 23-year-old massage therapist, was confronted by police officers on August 24, 2019, after someone reported seeing a person wearing a ski mask who “looks sketchy.” After officers wrestled him to the ground and paramedics injected him with a potent sedative, McClain suffered a heart attack on the way to a hospital and died days later, authorities said.
Prosecutors initially declined to bring charges in his death, but the case received renewed scrutiny following the nationwide Black Lives Matter protests in spring 2020. Colorado Gov. Jared Polis appointed a special prosecutor to reexamine the case, and in 2021 a grand jury indicted three officers and two paramedics in McClain’s death.
The defendants have now faced juries in three separate trials in 2023, to different results. Officer Randy Roedema was found guilty of criminally negligent homicide and assault, while officers Jason Rosenblatt and Nathan Woodyard were acquitted of all charges. Paramedics Jeremy Cooper and Peter Cichuniec will soon learn their fate.
Here’s a timeline of McClain’s death, the resulting investigation, the protests that brought renewed attention to the case and the criminal trials.
Three White officers stopped McClain in Aurora on August 24, 2019, while he was walking home from a convenience store in the Denver suburb after 10:30 p.m., according to a police overview of the incident.
Carrying iced tea in a plastic bag, McClain eventually was in a physical struggle with the officers after, police say, he resisted arrest.
Early in the encounter, an officer told McClain to stop, and when McClain kept walking, two officers grabbed his arms, the overview reads. McClain says, “Let me go … I’m an introvert, please respect the boundaries that I am speaking,” according to body camera footage from one of the officers.
After an officer asked him to cooperate so they could talk, McClain tells officers he had been trying to pause his music so he could hear them, and tells them to let him go, the overview reads.
Eventually, one officer is heard telling another that McClain tried to grab his gun.
All three officers tackled McClain to the ground, and Woodyard placed him in a carotid hold – in which an officer uses their biceps and forearm to cut off blood flow to a subject’s brain – police said in the overview document. McClain briefly became unconscious, and Woodyard released the hold, the document reads, citing the officers.
Body camera video of the encounter shows McClain at some point saying he couldn’t breathe.
Because the hold was used, department policy compelled the officers to call the fire department for help, authorities said. Aurora Fire Rescue paramedics arrived and saw McClain on the ground and resisting officers, the overview says.
Paramedic Cooper diagnosed McClain with “excited delirium” and decided to inject him with the powerful sedative ketamine, the overview says.
McClain suffered a heart attack on the way to a hospital, authorities said. Three days later, he was declared brain-dead and taken off life support.
The Adams County coroner’s office submitted an autopsy report on November 7, stating the cause and manner of death were “undetermined.” The report cited the scene investigation and examination findings as factors leading to that conclusion.
Roughly two weeks later, the Adams County district attorney, Dave Young, declined to file criminal charges against any of the first responders. In a letter to the Aurora police chief on November 22, Young referred to the undetermined cause of death as one of the factors.
“The evidence does not support a conclusion that Mr. McClain’s death was the direct result of any particular action of any particular individual,” Young wrote. “Under the circumstances of this investigation, it is improbable for the prosecution to prove cause of death beyond a reasonable doubt to a jury of twelve. Consequently, the evidence does not support the prosecution of a homicide.”
Also on November 22, after the district attorney’s decision, Aurora police released the officers’ body camera videos.
“We certainly recognize and understand that this has been an incredibly devastating and difficult process for them over these last several weeks,” then-Police Chief Nick Metz said.
A police review board concluded that the use of force against McClain, including the carotid hold, “was within policy and consistent with training.”
City officials announced on February 6 they would hire an independent expert to review the case.
George Floyd, a 46-year-old Black man, was fatally restrained by police in Minneapolis, Minnesota, on May 25. Bystander video of the encounter sets off outrage and leads to widespread protests, including in Aurora, under the Black Lives Matter movement.
In early June, the three officers who confronted McClain were assigned to administrative duties, primarily due to safety concerns because police and city employees were receiving threats, a police spokesperson said.
On June 9, Aurora police and city officials announced changes to police policies, including a ban on carotid holds.
Ten days later, Gov. Polis signed police accountability legislation into law, requiring all officers to use activated body cameras or dashboard cameras during service calls or officer-initiated public interactions. The measure also barred officers from using chokeholds.
Polis also signed an executive order appointing Colorado Attorney General Phil Weiser to investigate McClain’s case, the governor announced on June 25. More than 2 million people had signed a petition urging officials to conduct a new investigation.
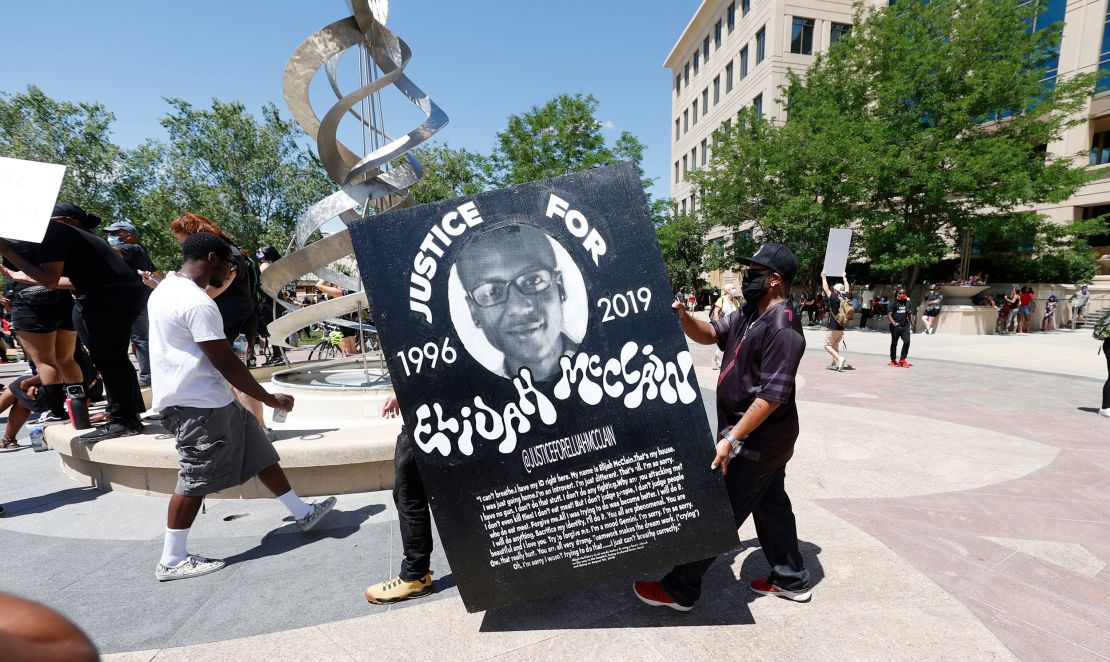
On June 27, protesters in the Aurora area gathered on Highway 225, temporarily shutting it down in a demonstration calling for justice in McClain’s death.
On June 30, the US attorney’s office for Colorado, the US Department of Justice’s civil rights division and the FBI’s Denver division announced they have been reviewing the case since 2019 for potential federal civil rights violations.
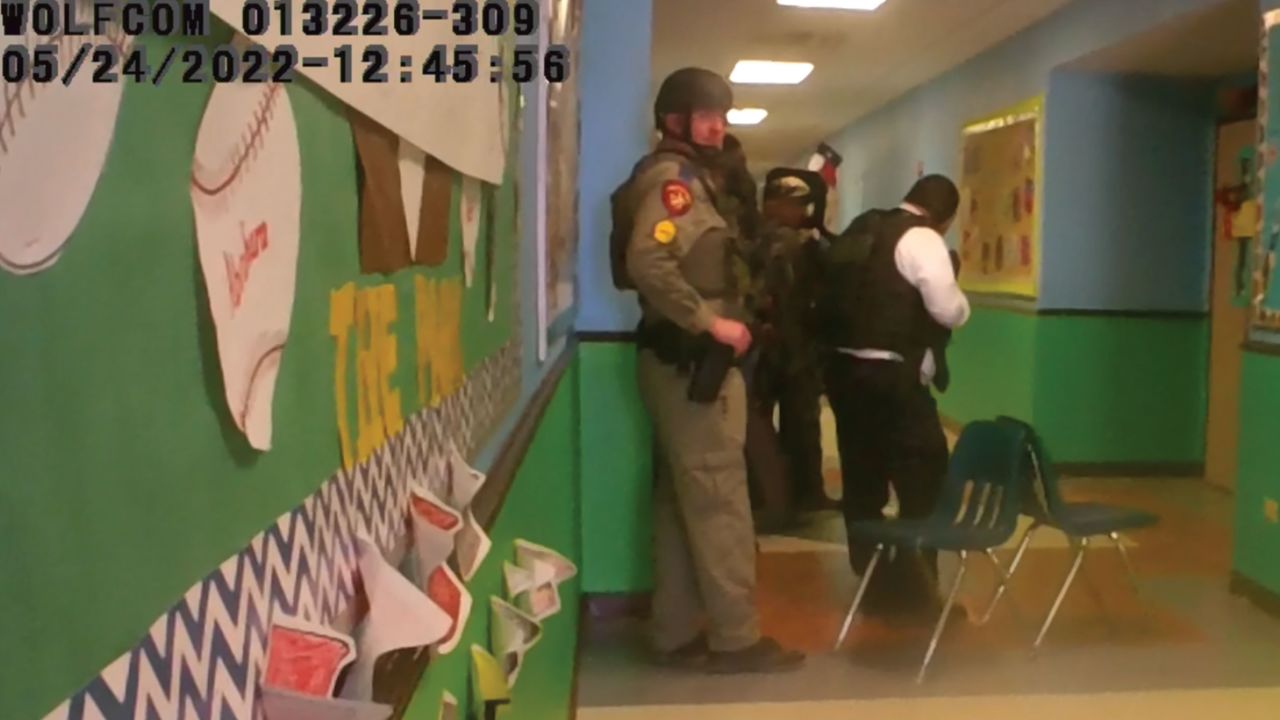
Aurora police on July 3 fired two officers who they say snapped selfie photographs at McClain’s memorial site, located where he was killed, while they were on duty.
Officer Rosenblatt also was fired, with police saying he received the photo in a text and replied, “ha ha,” and did not notify supervisors. The photos were taken on October 20, 2019.
A third officer seen in the photos resigned days before a pre-disciplinary hearing, police said.
On July 20, the Aurora City Council approved a resolution for an independent investigation of McClain’s death to proceed.

The McClain family filed a federal civil rights lawsuit against the city of Aurora on August 11.
“Aurora’s unconstitutional conduct on the night of August 24, 2019, is part of a larger custom, policy, and practice of racism and brutality, as reflected by its conduct both before and after its murder of Elijah McClain, a young Black man,” the lawsuit stated.
On the same day, Aurora city officials announced the police department would undergo a “comprehensive review” by external experts on civil rights and public safety.
Aurora city officials released a 157-page report on February 22, detailing the findings of the independent investigation it commissioned into McClain’s death.
The report asserted that officers did not have the legal basis to stop, frisk or restrain McClain. It also criticized emergency medical responders’ decision to inject him with ketamine and rebuked the police department for failing to seriously question the officers after the death.
Elijah McClain’s mom has watched the bodycam video ‘over and over’
Sheneen McClain, Elijah’s mother, cried while reading the report.
“It was overwhelming knowing my son was innocent the entire time and just waiting on the facts and proof of it,” Sheneen McClain told CNN at the time. “My son’s name is cleared now. He’s no longer labeled a suspect. He is actually a victim.”
Elijah McClain’s father said the report only confirmed what the family already knew. “The Aurora police and medics who murdered my son must be held accountable,” LaWayne Mosley said after the report’s release.
In response to the report, city officials began work on establishing an independent monitor to scrutinize police discipline, Aurora City Manager Jim Twombly said.
“I believe the investigative team has identified the issue that is at the root of the case: the failure of a system of accountability,” Twombly said after the report’s release.
On September 1, the state attorney general announced a grand jury indicted officers Roedema, Rosenblatt and Woodyard and paramedics Cichuniec and Cooper.
Each was charged with manslaughter and criminally negligent homicide as part of a 32-count indictment.
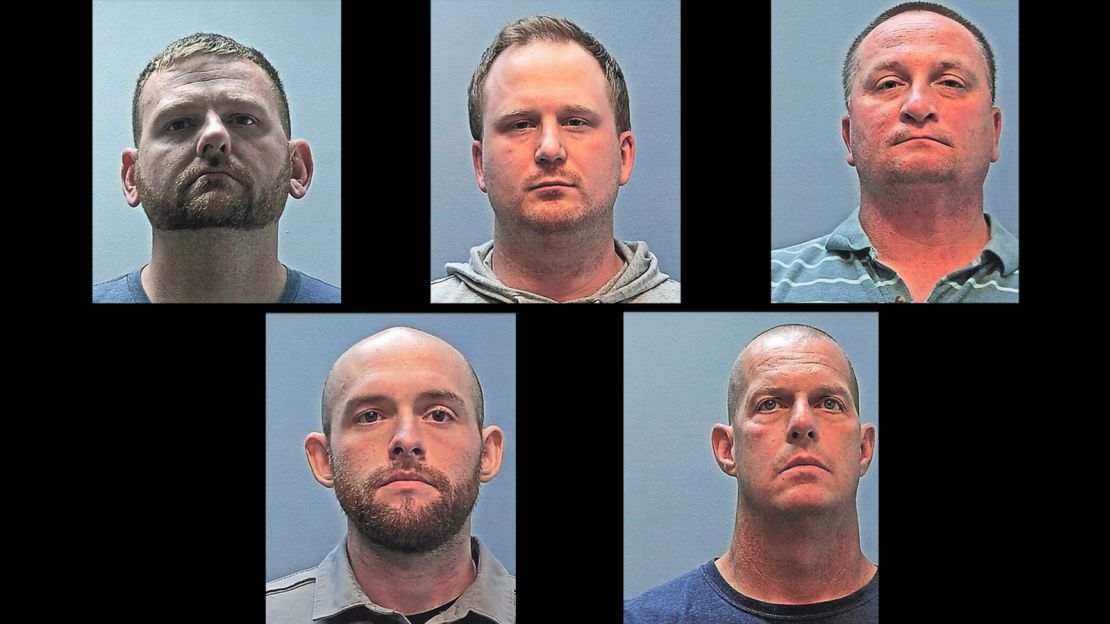
Roedema and Rosenblatt also were indicted on one count of assault and one count of crime of violence. Cooper and Cichuniec were further indicted on three counts of assault and six counts of crime of violence.
“Our goal is to seek justice for Elijah McClain, for his family and friends and for our state,” Weiser, the state attorney general, said. “In so doing, we advance the rule of law and our commitment that everyone is accountable and equal under the law.”
The charges brought McClain’s parents to tears. “I started crying because it’s been two years,” Sheneen McClain said. “It’s been a long journey.”
“Nothing will bring back my son, but I am thankful that his killers will finally be held accountable,” Mosley, his father, said through the attorney’s release.
On September 15, the Colorado attorney general’s office released a 112-page report that found the Aurora police had a pattern of practicing racially biased policing, excessive force, and had failed to record legally required information when interacting with the community. The report also found the police department used force against people of color almost 2.5 times more than against White people.
The state investigation also revealed the fire department had a pattern and practice of administering ketamine illegally, the attorney general’s office said.
The state attorney general’s office and the city of Aurora agreed November 16 on terms of a consent decree to address the issues raised in the office’s report two months earlier.
On November 19, the city finalized an agreement to pay $15 million to McClain’s family to settle the federal civil rights lawsuit.
The cause of death in McClain’s case was changed in light of evidence from the grand jury’s investigation, according to an amended autopsy report publicly released September 23.
The initial autopsy report had said the cause of death was undetermined. But the amended report listed “complications of ketamine administration following forcible restraint” as the cause of death.
The manner of death remained undetermined in the amended report.
“Simply put, this dosage of ketamine was too much for this individual and it resulted in an overdose, even though the blood ketamine level was consistent with a ‘therapeutic’ concentration,” pathologist Dr. Stephen Cina wrote in the amended autopsy report. “I believe that Mr. McClain would most likely be alive but for the administration of ketamine.”
Cina could not determine whether the carotid hold contributed to the death, but “I have seen no evidence that injuries inflicted by the police contributed,” he wrote.
On September 20, Roedema and Rosenblatt, two of the officers who arrested McClain, stood trial on charges of manslaughter, criminally negligent homicide and assault.
Prosecutors said they used excessive force on McClain, failed to follow their training and misled paramedics about his health status. In contrast, defense attorneys placed blame on McClain for resisting arrest and on the paramedics who treated him.
Roedema was found guilty of criminally negligent homicide and assault. Rosenblatt was acquitted of all charges.
On October 16, the third officer, Woodyard, stood trial on charges of reckless manslaughter and criminally negligent homicide. Like in the earlier trial, prosecutors argued he used excessive force on McClain, while defense attorneys argued the force was necessary and blamed the paramedics.
Woodyard was found not guilty on all charges.
McClain’s mother Sheneen told CNN affiliate KUSA she no longer has faith in the justice system after Woodyard’s acquittal.
“It lets us down, not just people of color, it lets down everybody,” she said. “They don’t do the right thing, they always do the bare minimum.”
Cooper and Cichuniec, the paramedics who treated McClain, stood trial on charges of reckless manslaughter and criminally negligent homicide.
Both paramedics testified they believed McClain was experiencing “excited delirium” during his confrontation with Aurora police officers, and their treatment protocol was to administer a ketamine dose they believed was safe and would not kill a person.
Prosecutors said the paramedics “didn’t take any accountability for any single one of their actions” while testifying at their trial.
“They both stood there while Elijah got worse and worse and did nothing,” Colorado Solicitor General Shannon Stevenson said. “They are both responsible.”
Cooper and Cichuniec were found guilty of criminally negligent homicide Friday.
Cichuniec was also found guilty of a second-degree unlawful administration of drugs assault charge.
[ad_2]