[ad_1]
Eating every other day can raise your cholesterol.
Are there any downsides to fasting every other day? For example, might go all day without eating impair your ability to think clearly? Surprisingly, as I discuss in my video Is Alternate-Day Intermittent Fasting Safe?, the results appear to be “equivocal.” Some studies show no measurable effects and the ones that do fail to agree on which cognitive domains are affected. Might the cycles of fasting and feasting cause eating disorder–type behaviors, like bingeing? So far, no harmful psychological effects have been found. In fact, there may be some benefit. However, the studies that have put it to the test specifically excluded those with a documented history of eating disorders, for whom the effects may differ.
What about bone health? No change in bone mineral density was noted after six months of alternate-day fasting despite about 16 pounds of weight loss, which would typically result in a dip in bone mass. However, the researchers did not note any skeletal changes in the control group either, and they lost a similar amount of weight using continuous caloric restriction. They suggested this is because both groups tended to be “more physically active than the average obese American,” getting about 1,000 to 2,000 more steps a day.
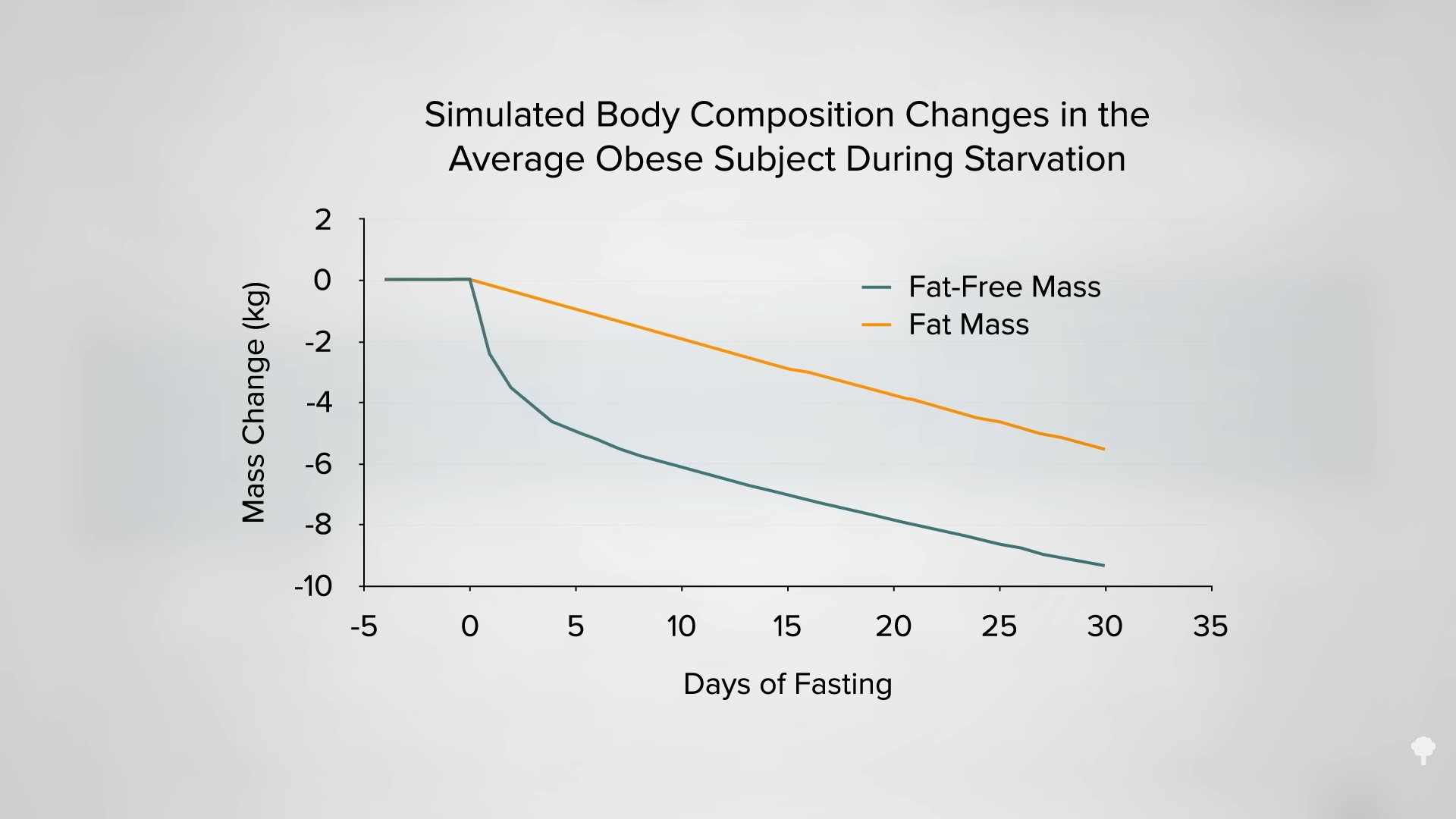
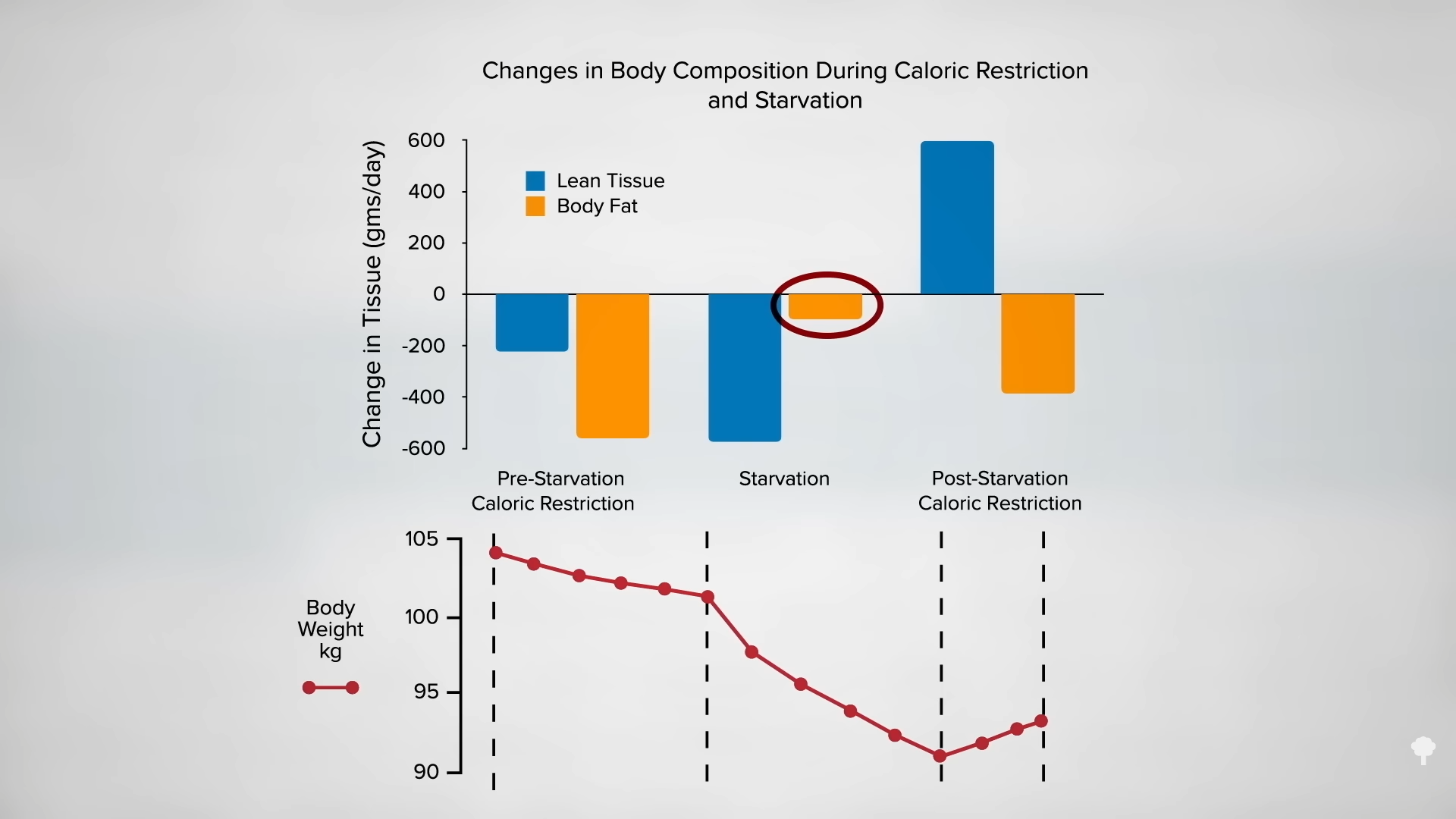
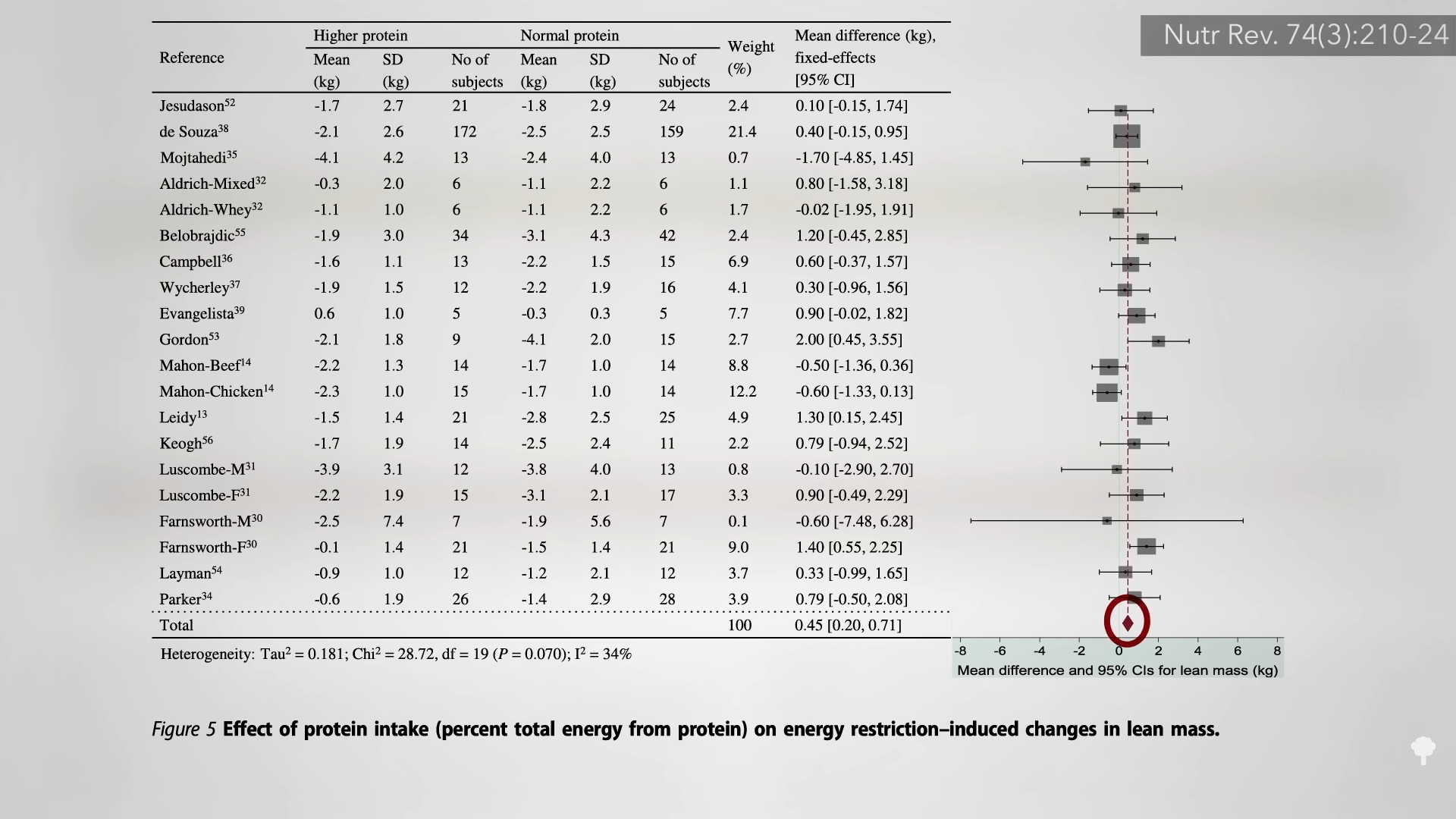
Proponents of intermittent fasting suggest it can better protect lean body mass, but most of the intermittent trials have employed less accurate methods of body composition analysis, whereas the majority of continuous caloric restriction trials used “vastly more accurate techniques.” So, to date, it is not clear if there’s a difference in lean mass preservation.
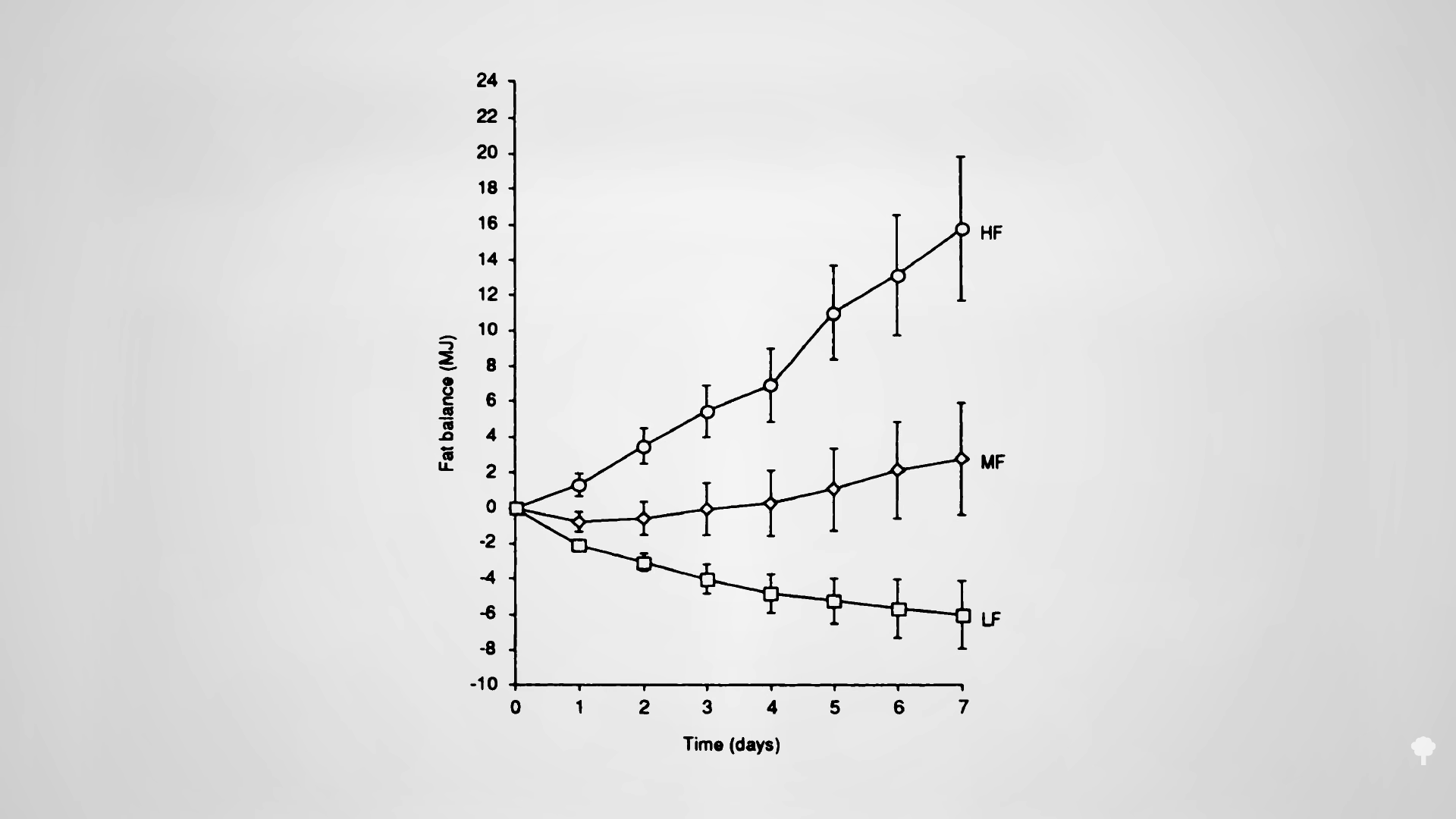
Improvements in blood pressure and triglycerides have been noted on intermittent fasting regimens, though this is presumed to be due to the reduction in body fat since the effect appears to be “dependent on the amount of weight lost.” Alternate-day fasting can improve artery function, too, as you can see in the graph below and at 1:55 in my video, though it does depend on what you’re eating on the non-fasting day. For study participants randomized to an alternate-day diet high in saturated fat, their artery function worsened despite a ten-pound weight loss, whereas it improved, as expected, in the lower-fat group. The decline in artery function was presumed to be because of the pro-inflammatory nature of saturated fat.
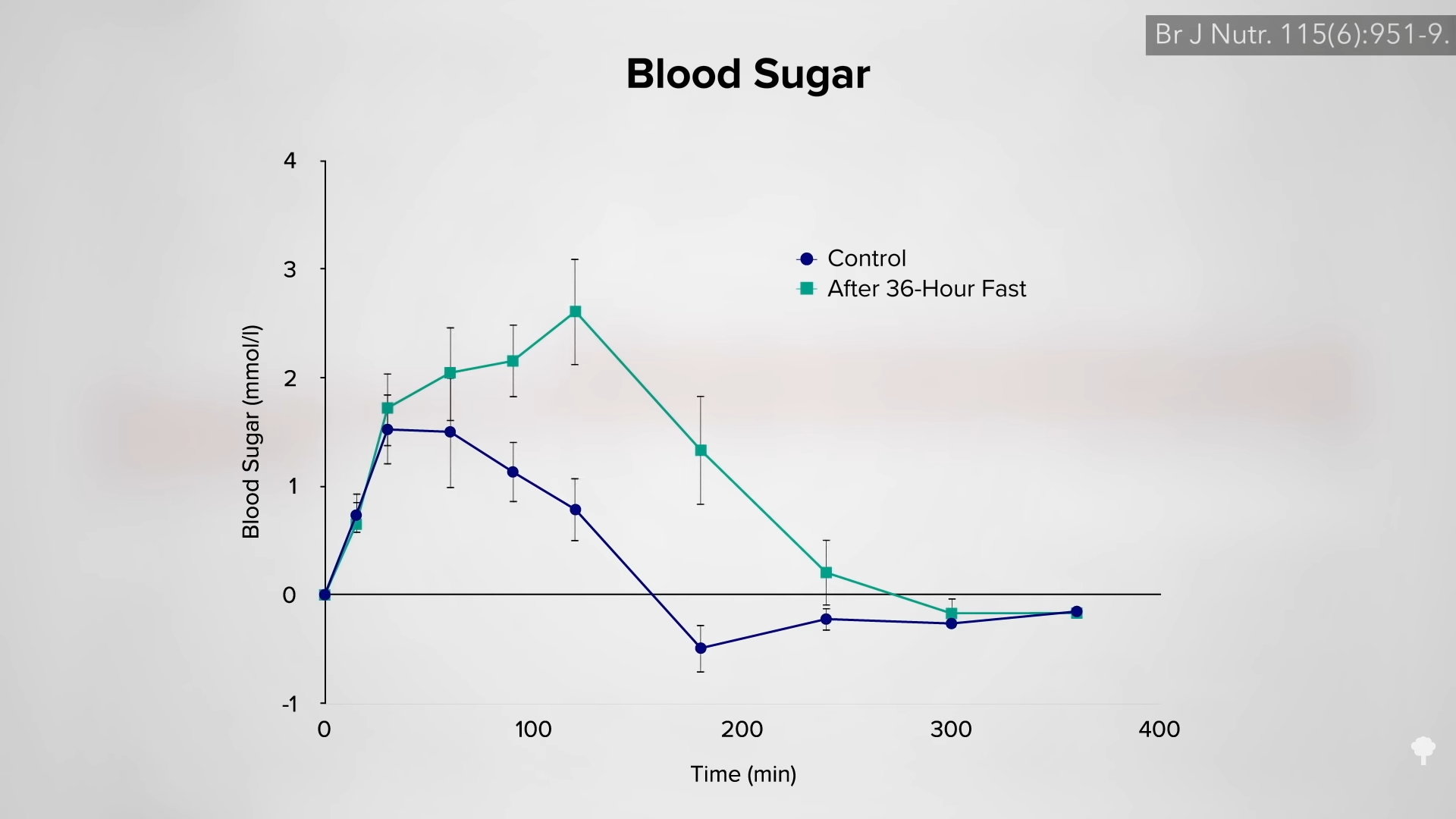
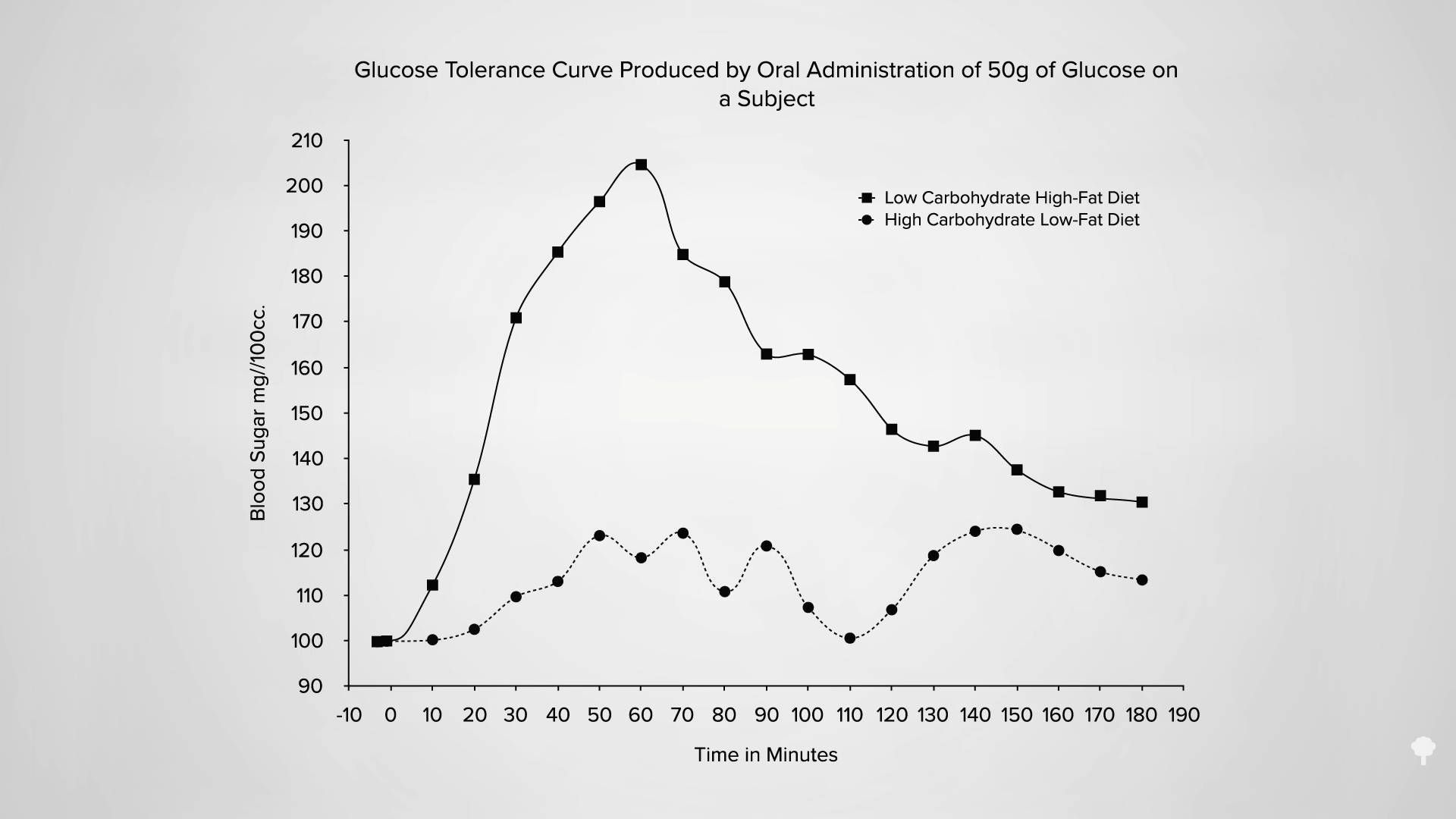
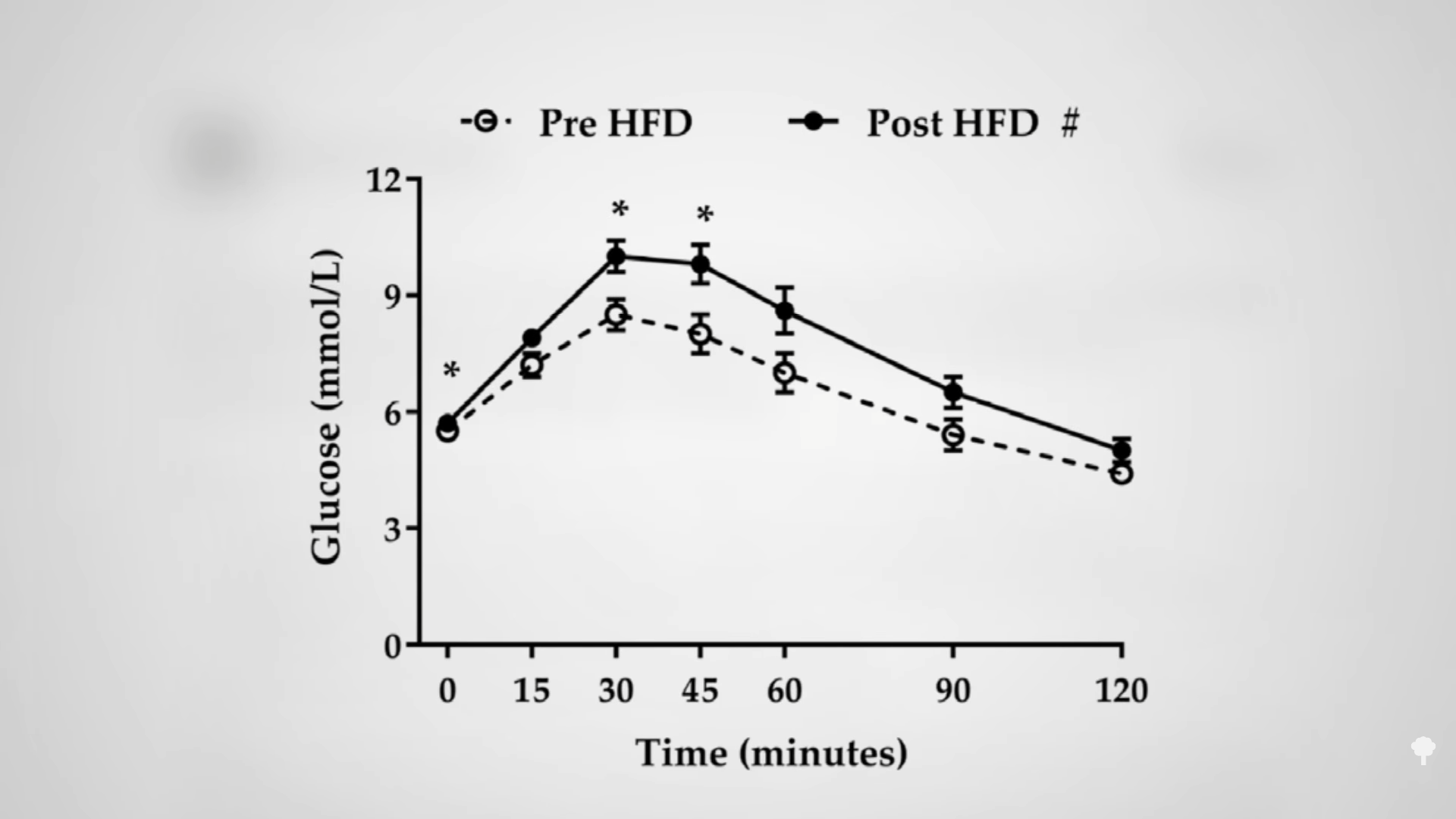
A concern has been raised about the effects of alternate-day fasting on cholesterol. After 24 hours without food, LDL cholesterol may temporarily bump up, but this is presumably because so much fat is being released into the system by the fast. As you can see in the graph below and at 2:33 in my video, an immediate negative effect on carbohydrate tolerance may stem from the same phenomenon—the repeated elevations of free fat floating around in the bloodstream. After a few weeks, though, LDL levels start to drop as the weight comes off. However, results from the largest and longest trial of alternate-day fasting have given me pause.
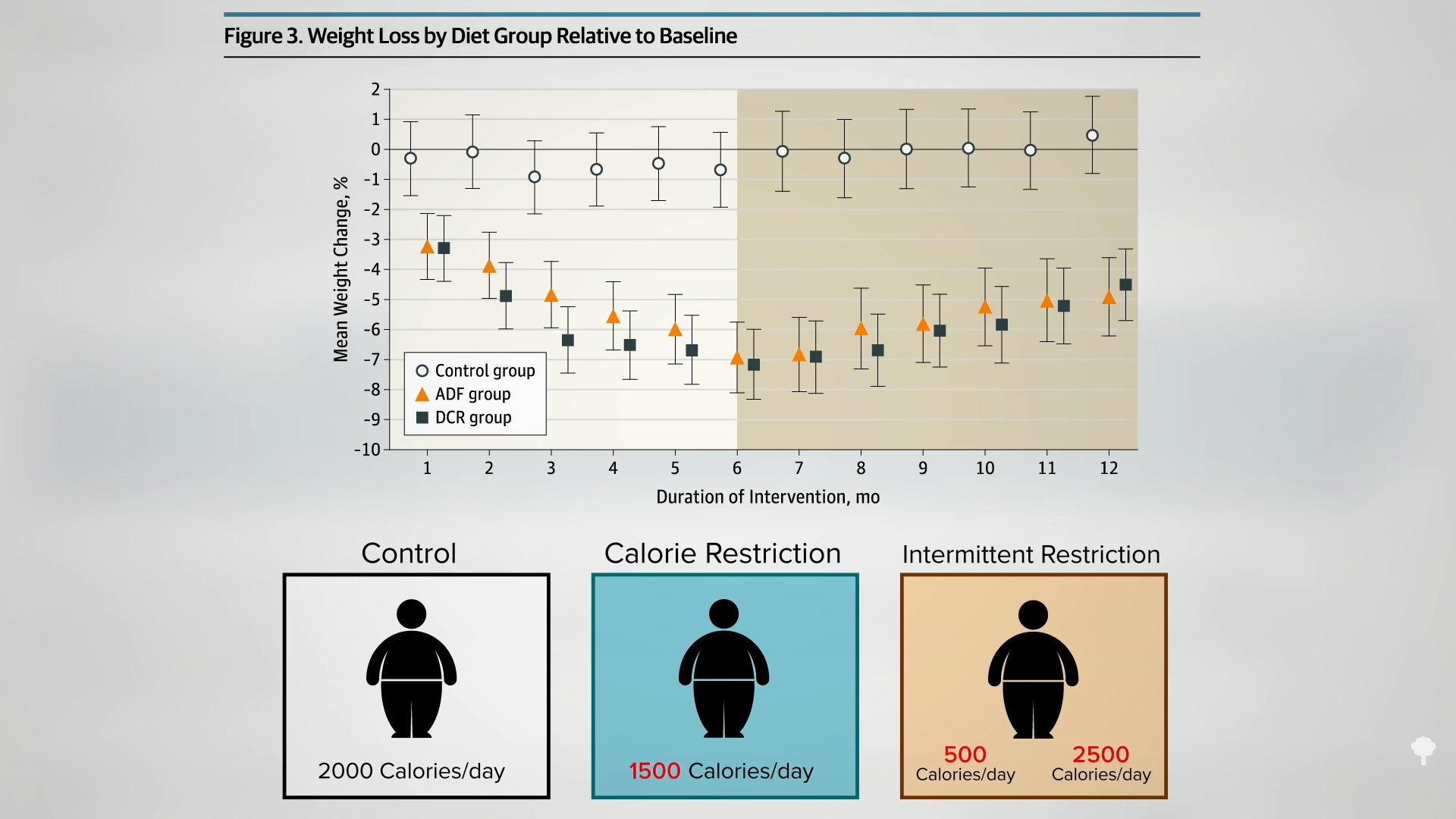
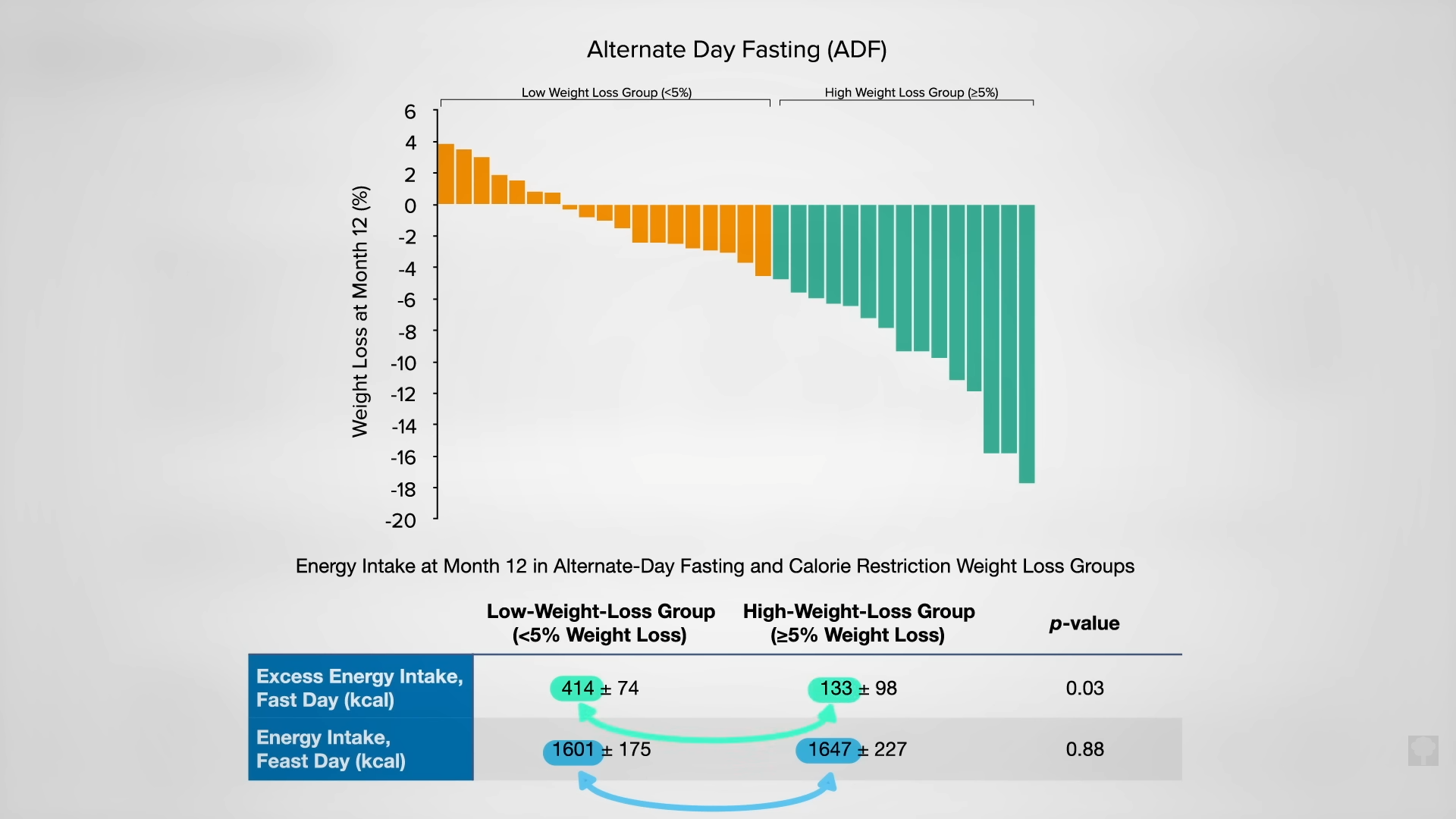
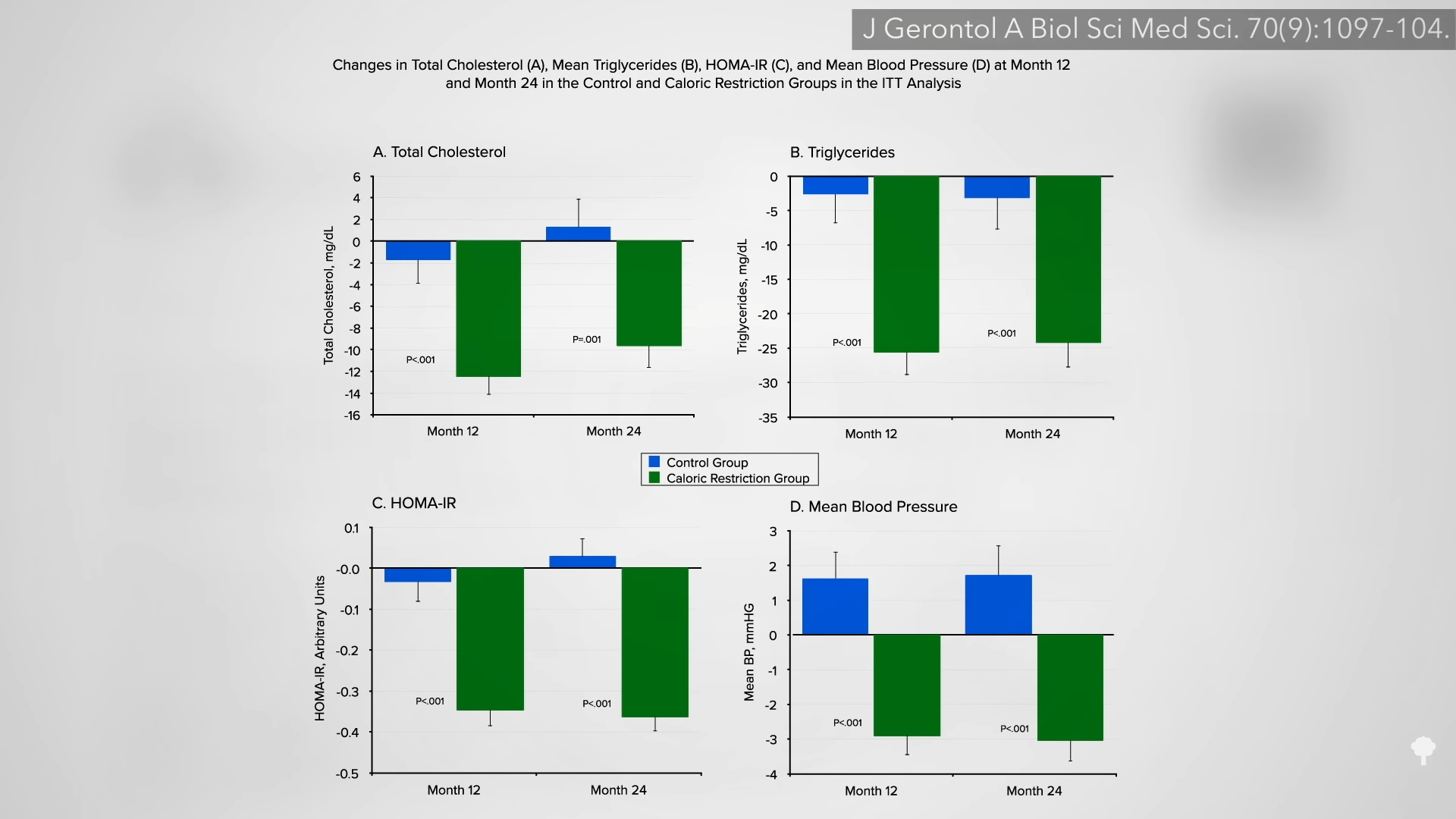
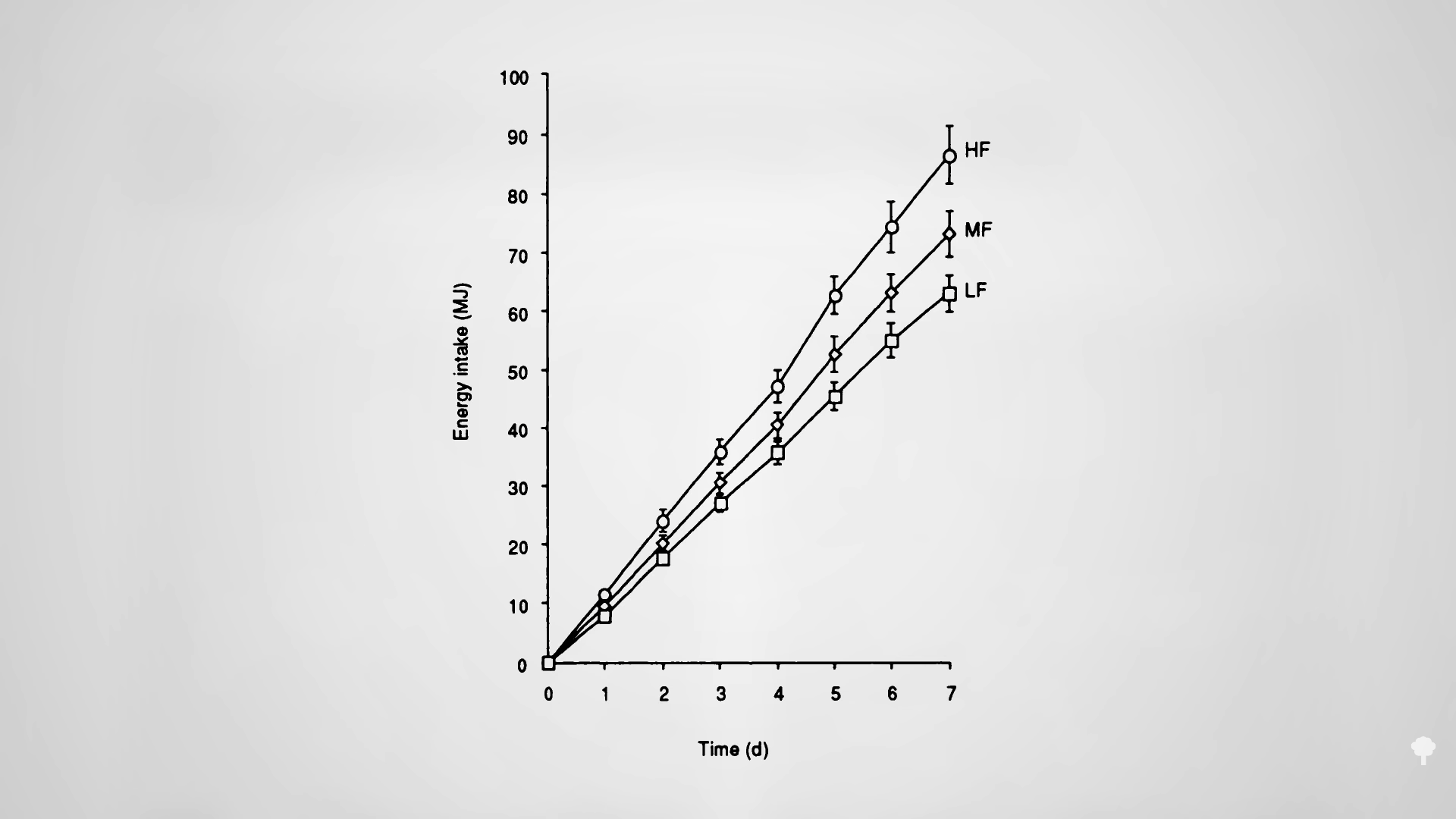
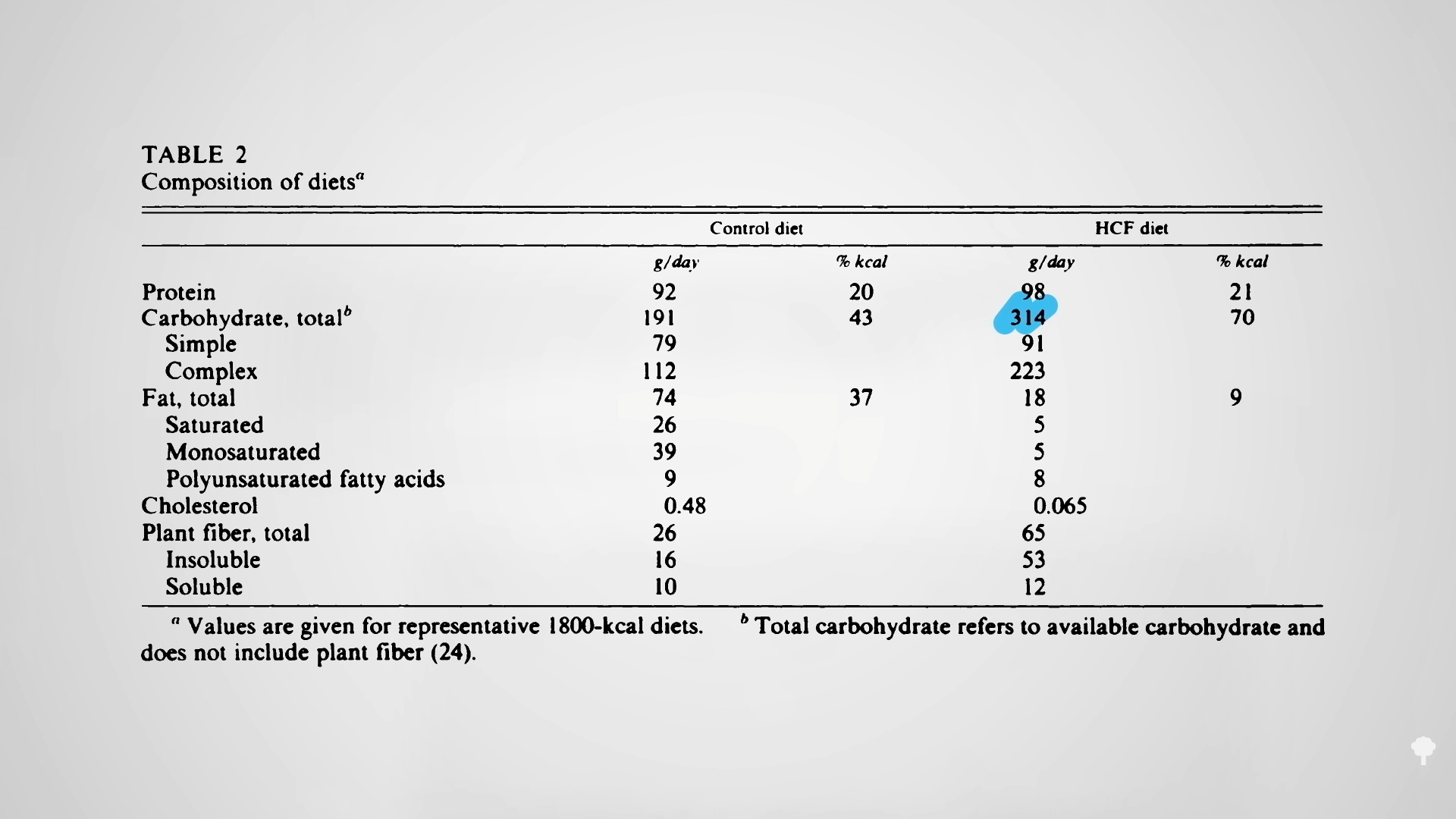
A hundred obese men and women were randomized into one of three groups: alternate-day modified fasting (25 percent of their baseline calories on fasting days and 125 percent calories on eating days), continuous, daily caloric restriction (75 percent of baseline), or a control group instructed to maintain their regular diet. So, for those going into the trial eating 2,000 calories a day, they would continue to eat 2,000 calories a day in the control group. The calorie-restriction group would get 1,500 calories every day, and the intermittent-restriction group would alternate between 500 calories a day and 2,500 calories the next.
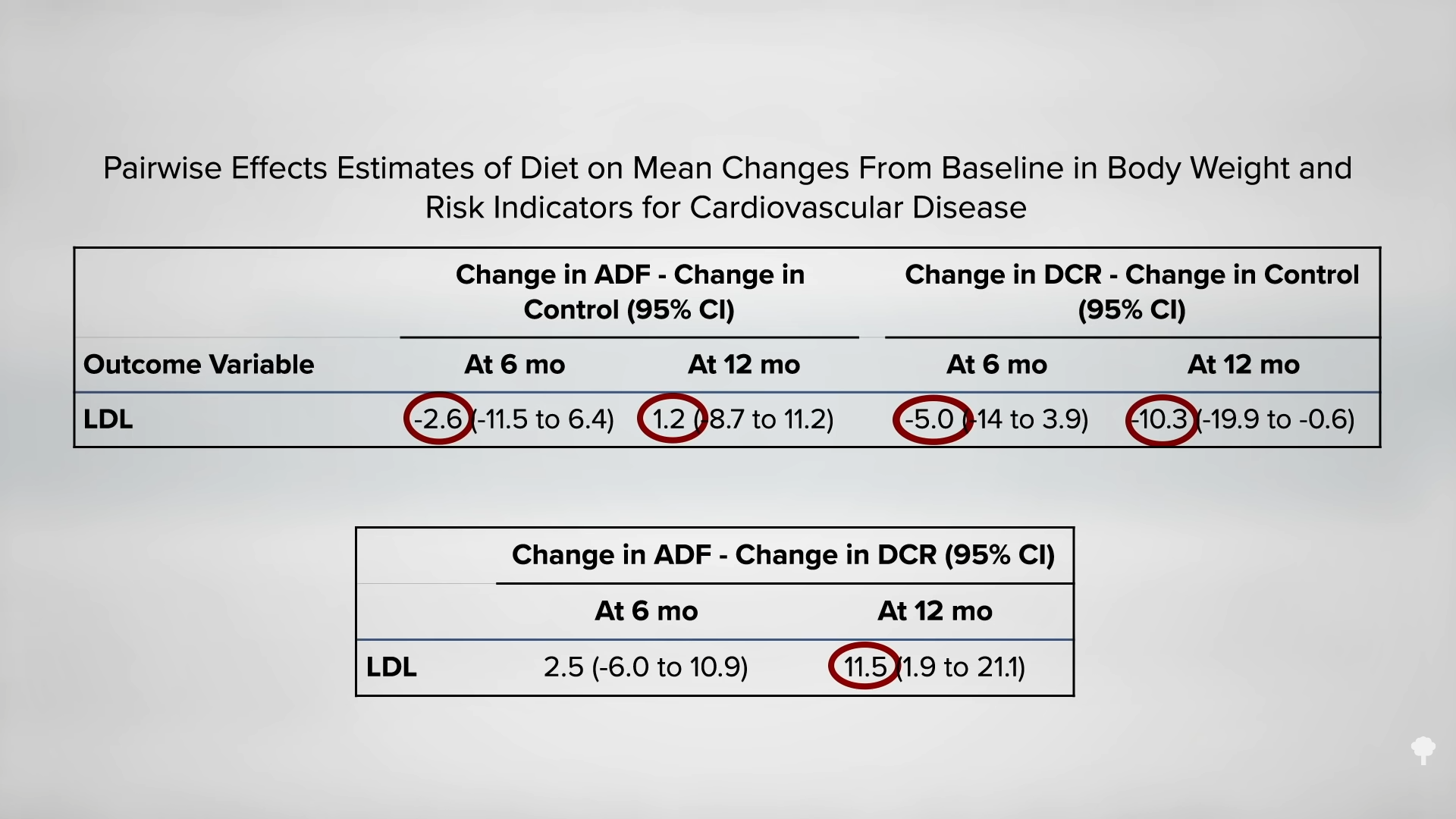
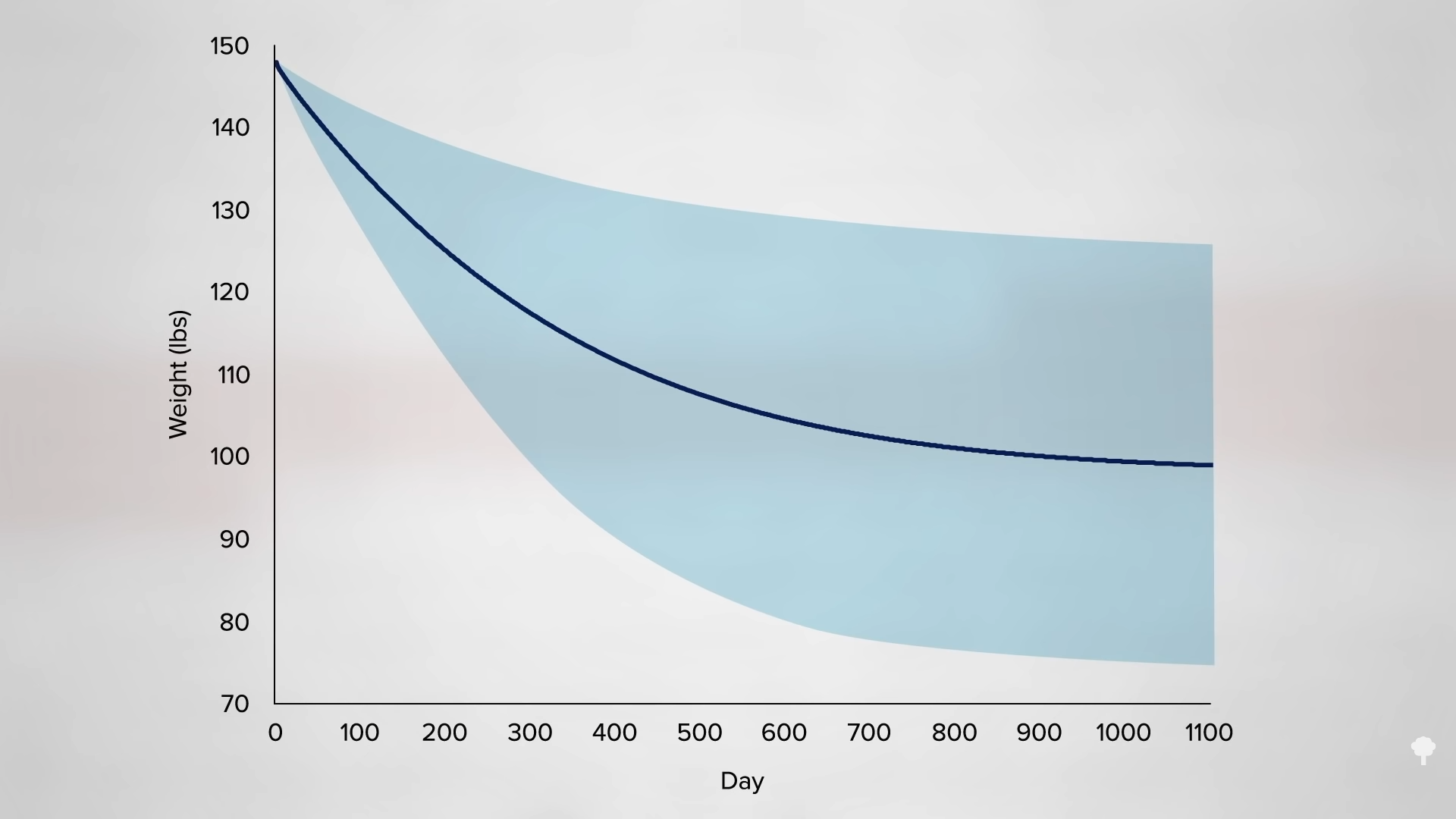
As you can see in the graph below and at 3:32 in my video, with the same overall, average, prescribed calorie cutting in the two weight-loss groups, they both lost about the same amount of weight, but, surprisingly, the cholesterol effects were different. In the continuous calorie-restriction group, the LDL levels dropped as expected compared to the control group as the pounds came off.
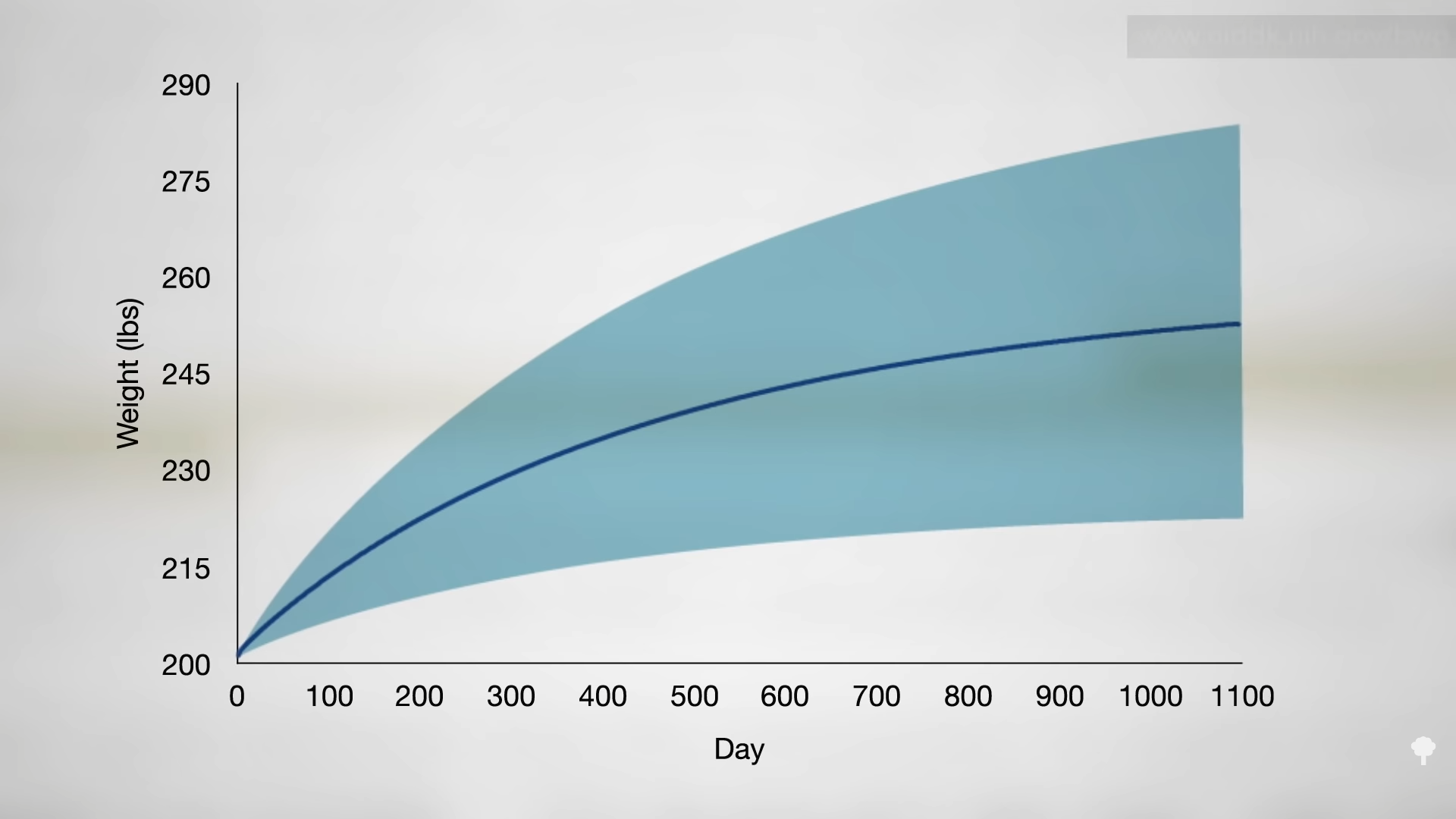
But, in the alternate-day modified fasting group, they didn’t, as you can see below, and at 3:55 in my video. At the end of the year, the LDL cholesterol in the intermittent fasting group ended up being 10 percent higher than in the constant calorie-restriction group—despite the same loss of body fat. Given that LDL cholesterol is a prime causal risk factor for heart disease, our number one killer—or is even the prime risk factor—this strikes a significant blow against alternate-day fasting. If you want to try it anyway, I would advise you to have your cholesterol monitored to make sure it comes down with your weight.
If you’re diabetic, you must talk with your physician about medication adjustment for any changes in diet, including fasting of any duration. Even with proactive medication reduction, advice to immediately break the fast should sugars drop too low, and weekly medical supervision, people with type 2 diabetes who fasted for even just two days a week were twice as likely to suffer from hypoglycemic episodes compared to an unfasted control group. We still don’t know the best way to tweak blood sugar medications to prevent blood sugar from dropping too low on fasting days.
Even fasting for just one day can significantly slow the clearance of some drugs (like the blood-thinning drug Coumadin) or increase the clearance of others (like caffeine). Fasting for 36 hours can cut your caffeine buzz by 20 percent. So, consultation with your medical professional before fasting is an especially good idea for anyone on any kind of medication.
If you missed it, check out Alternate-Day Intermittent Fasting Put to the Test.
So, with ambiguous cognitive, lean mass, and bone effects, plus these cholesterol findings, I wouldn’t suggest alternate-day fasting for weight loss, but dropping pounds isn’t the only thing this way of eating is purported to do. Check out Does Intermittent Fasting Increase Human Life Expectancy?.
For other types of intermittent fasting, total fasting, and more on fasting, check out the related videos below.
[ad_2]
Michael Greger M.D. FACLM
Source link









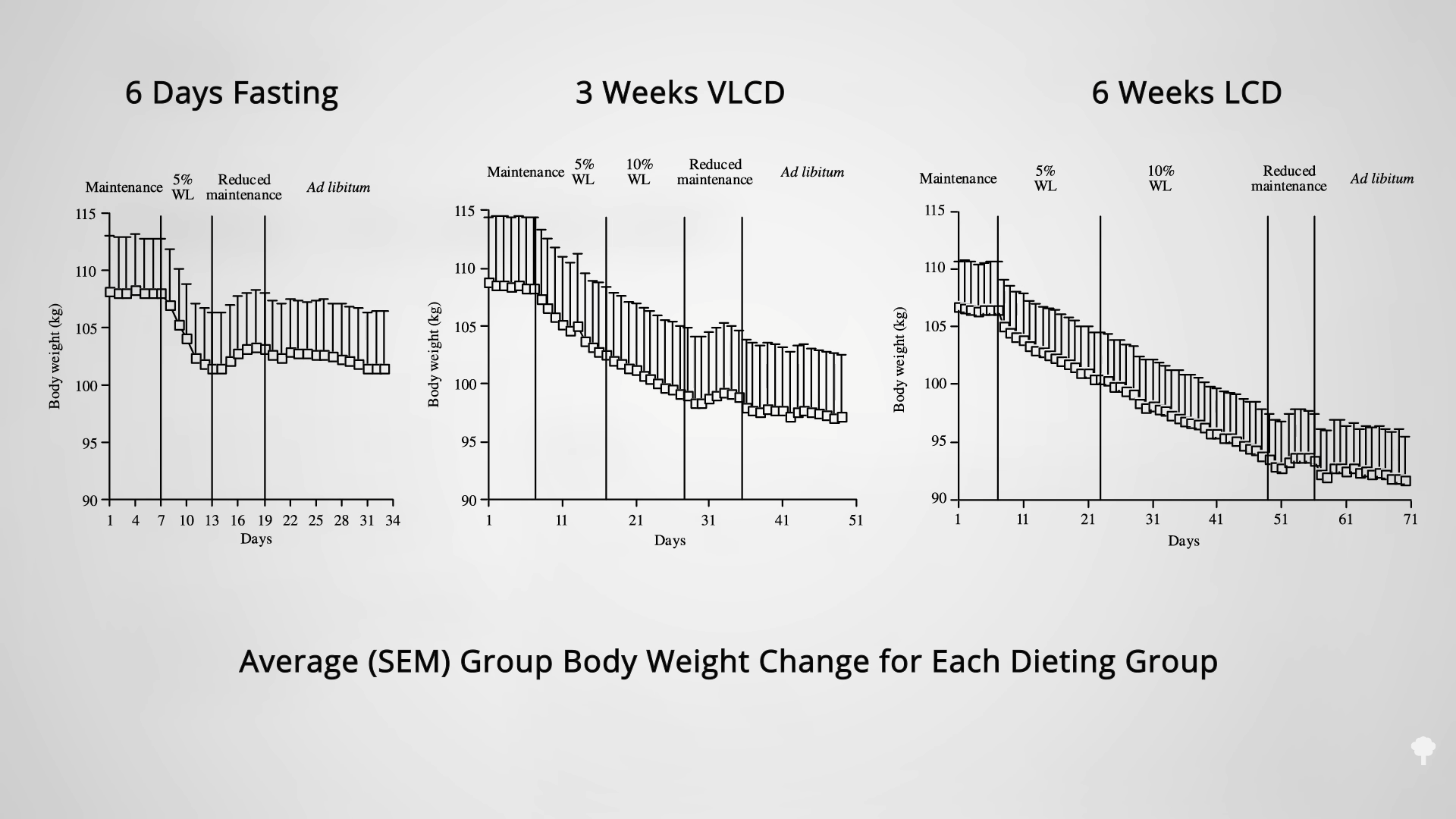
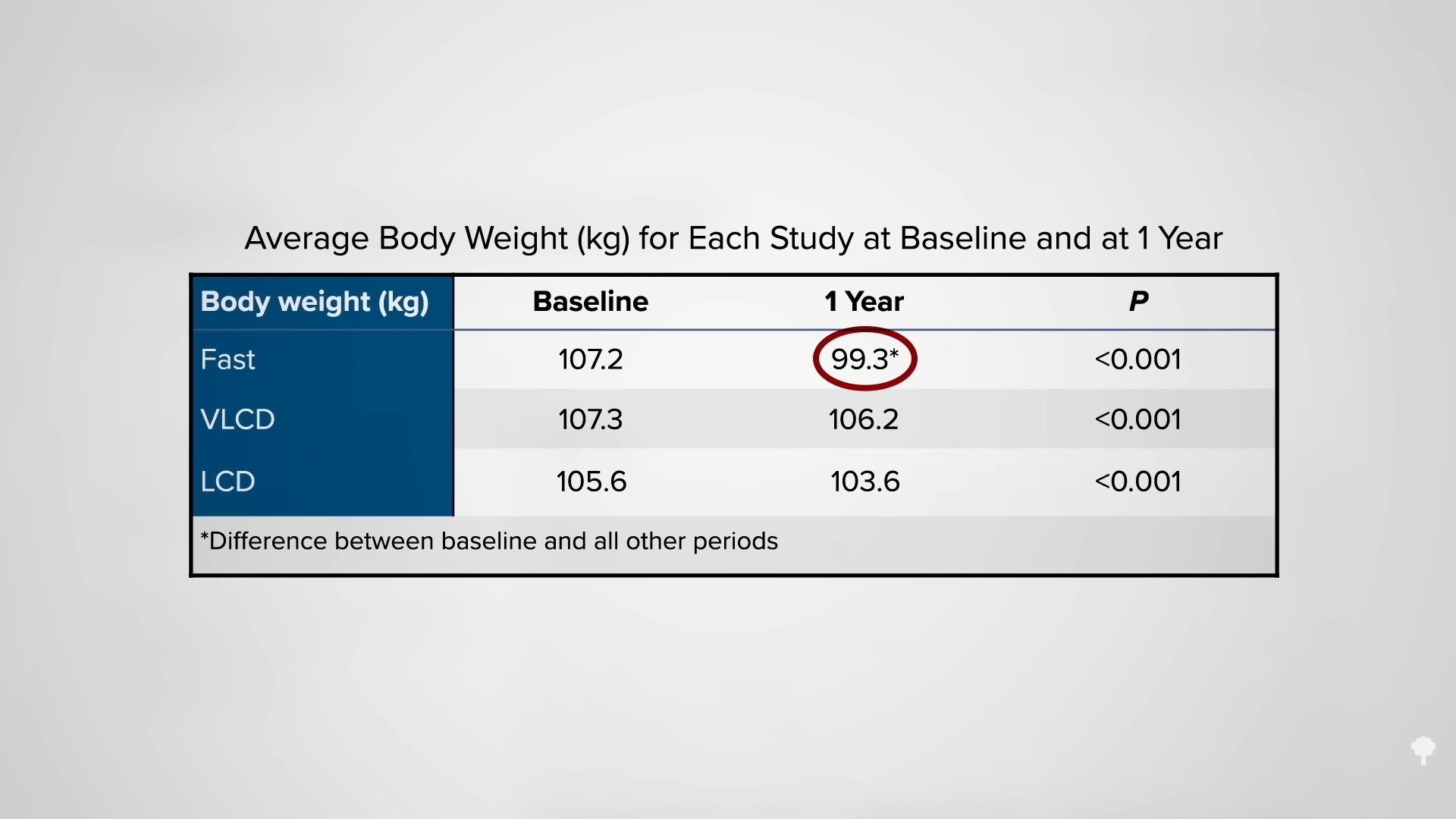
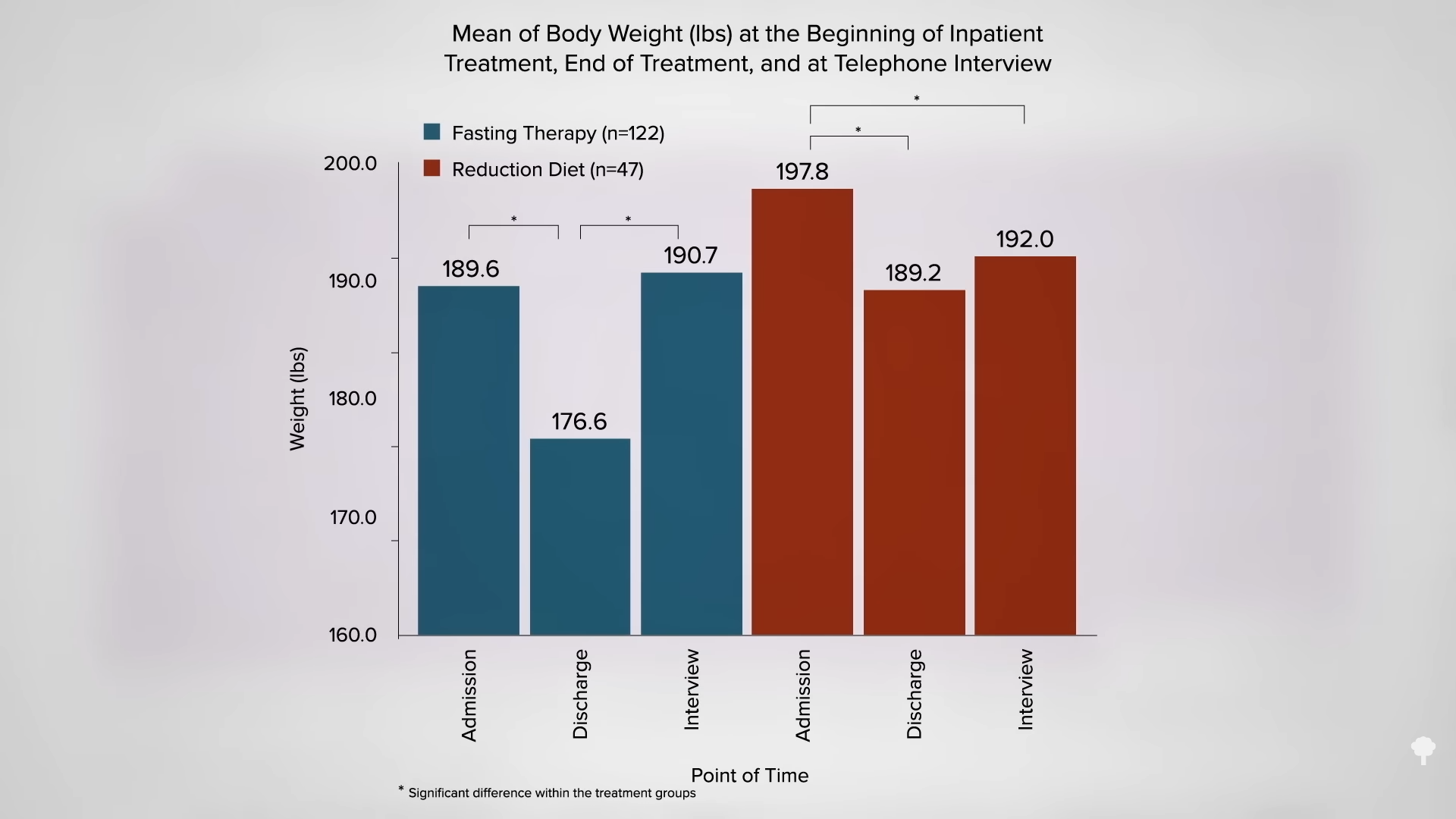
 Medically-supervised fasting has
Medically-supervised fasting has “
“
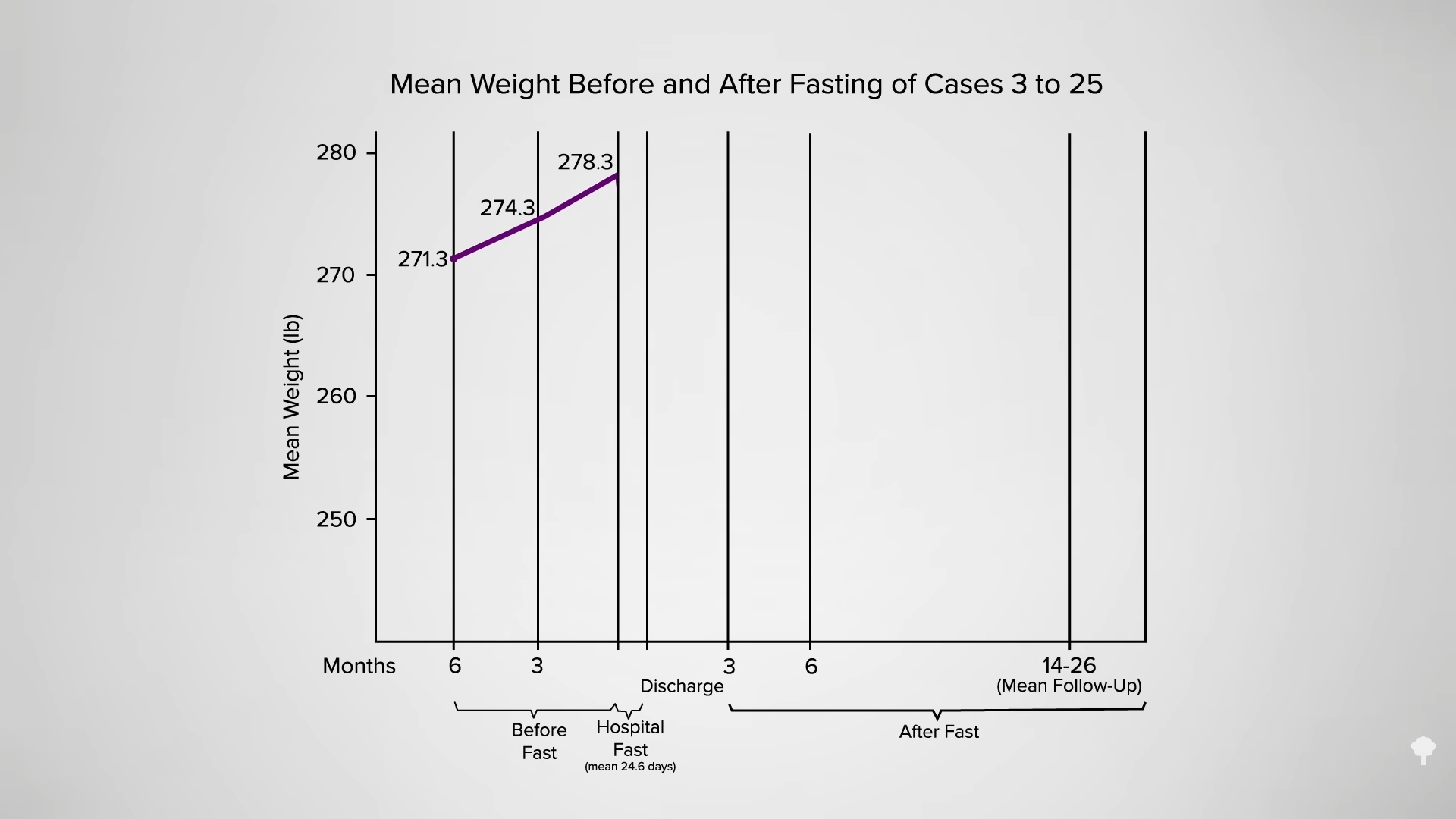
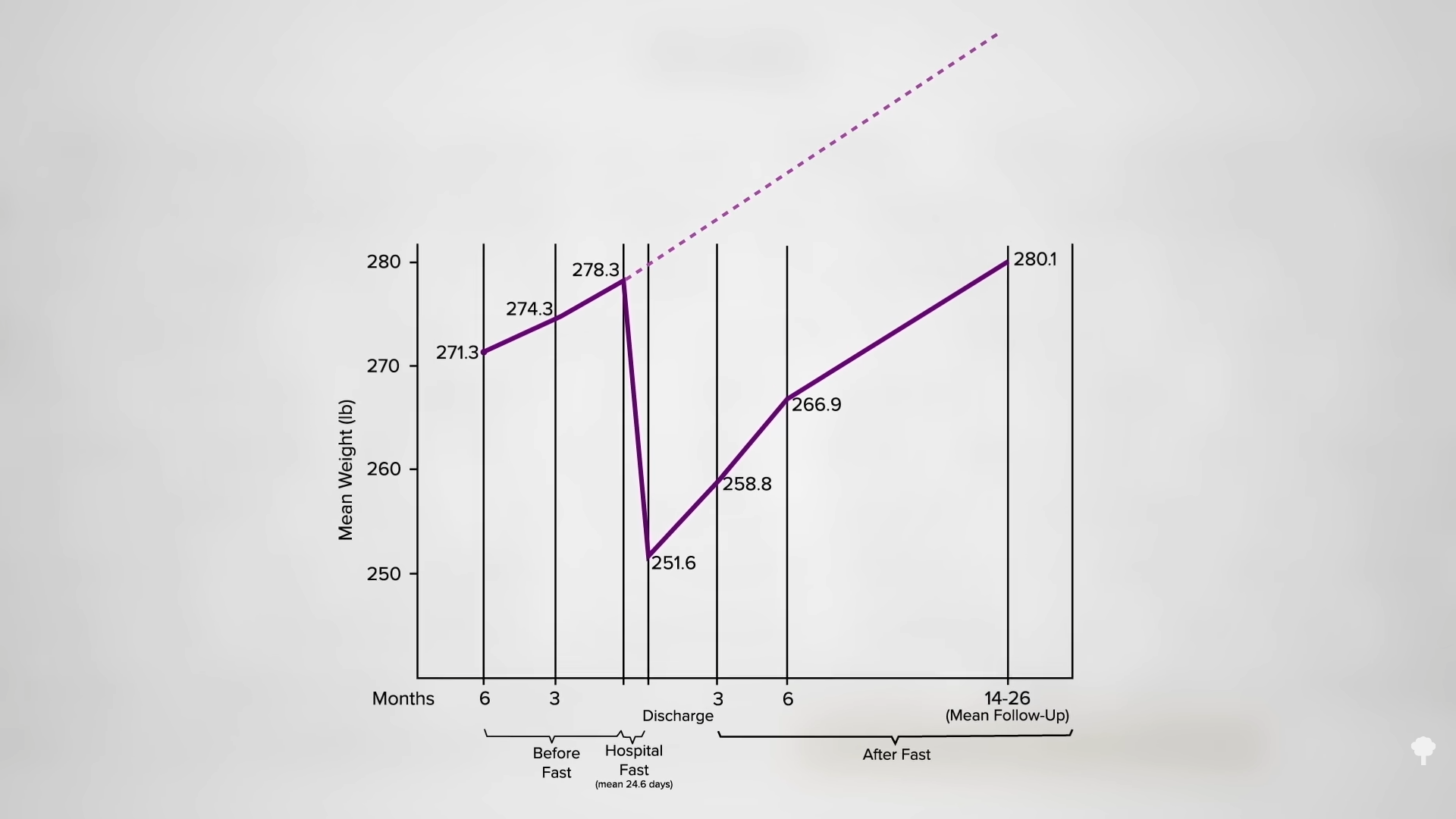
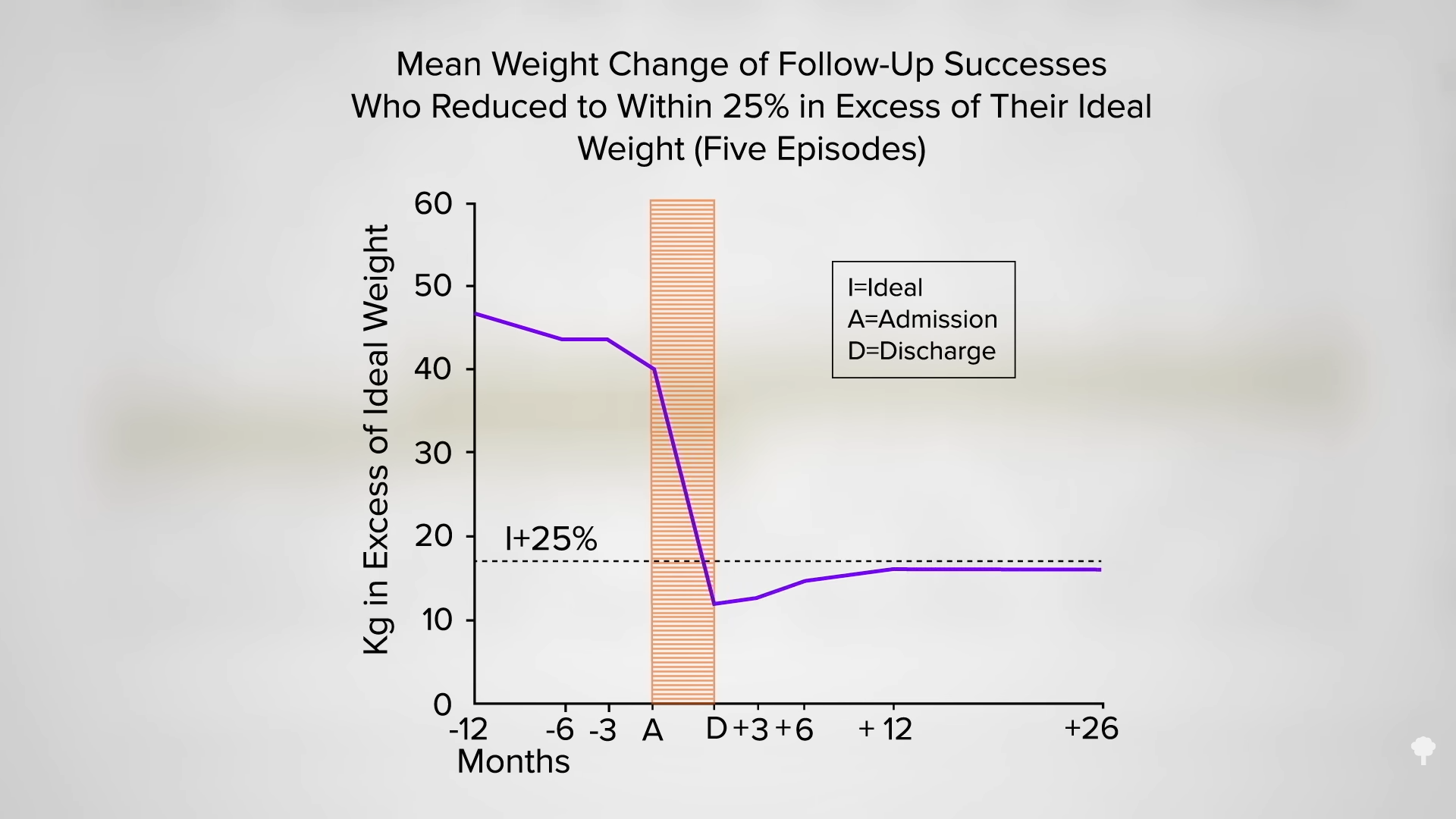
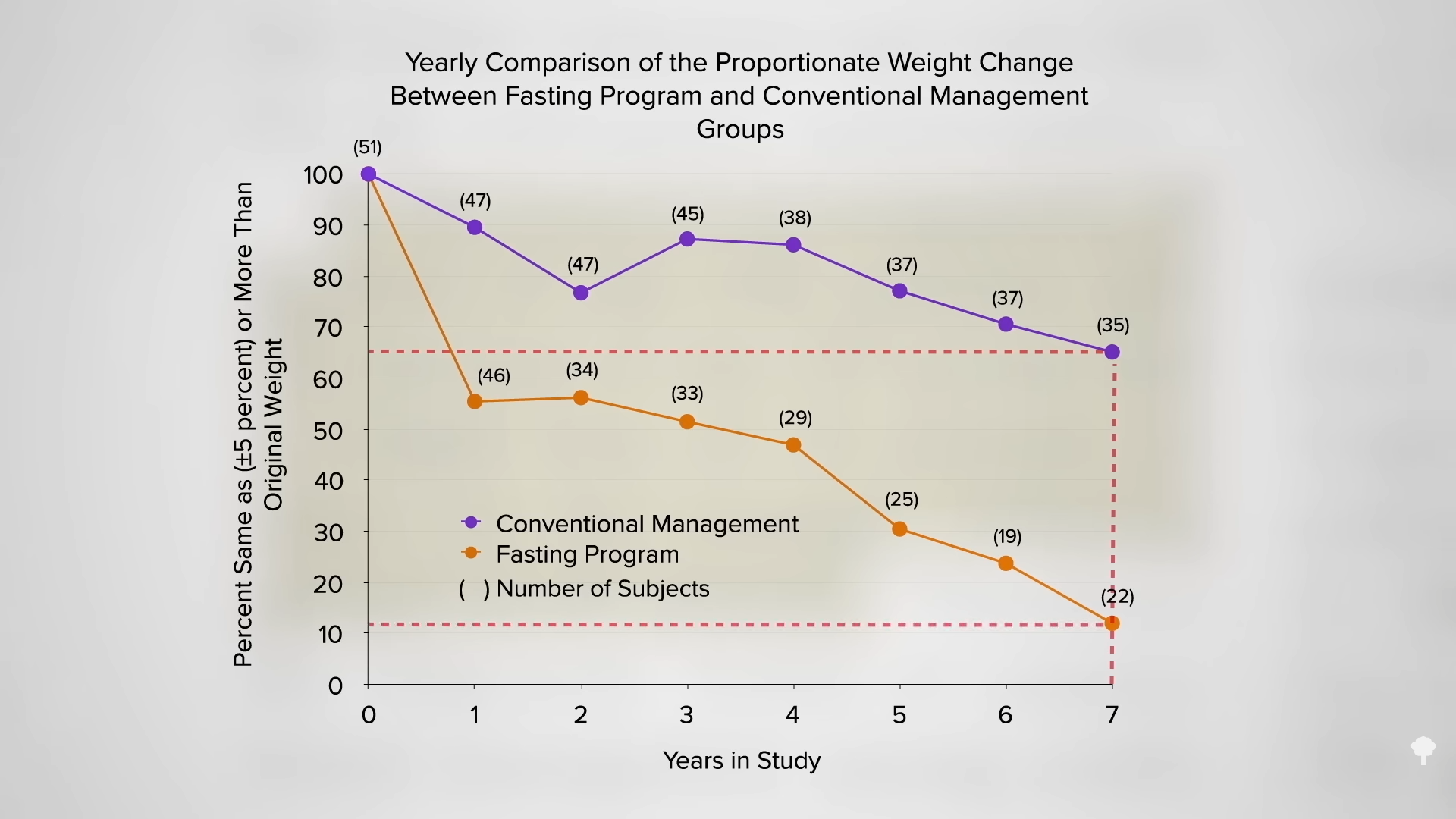
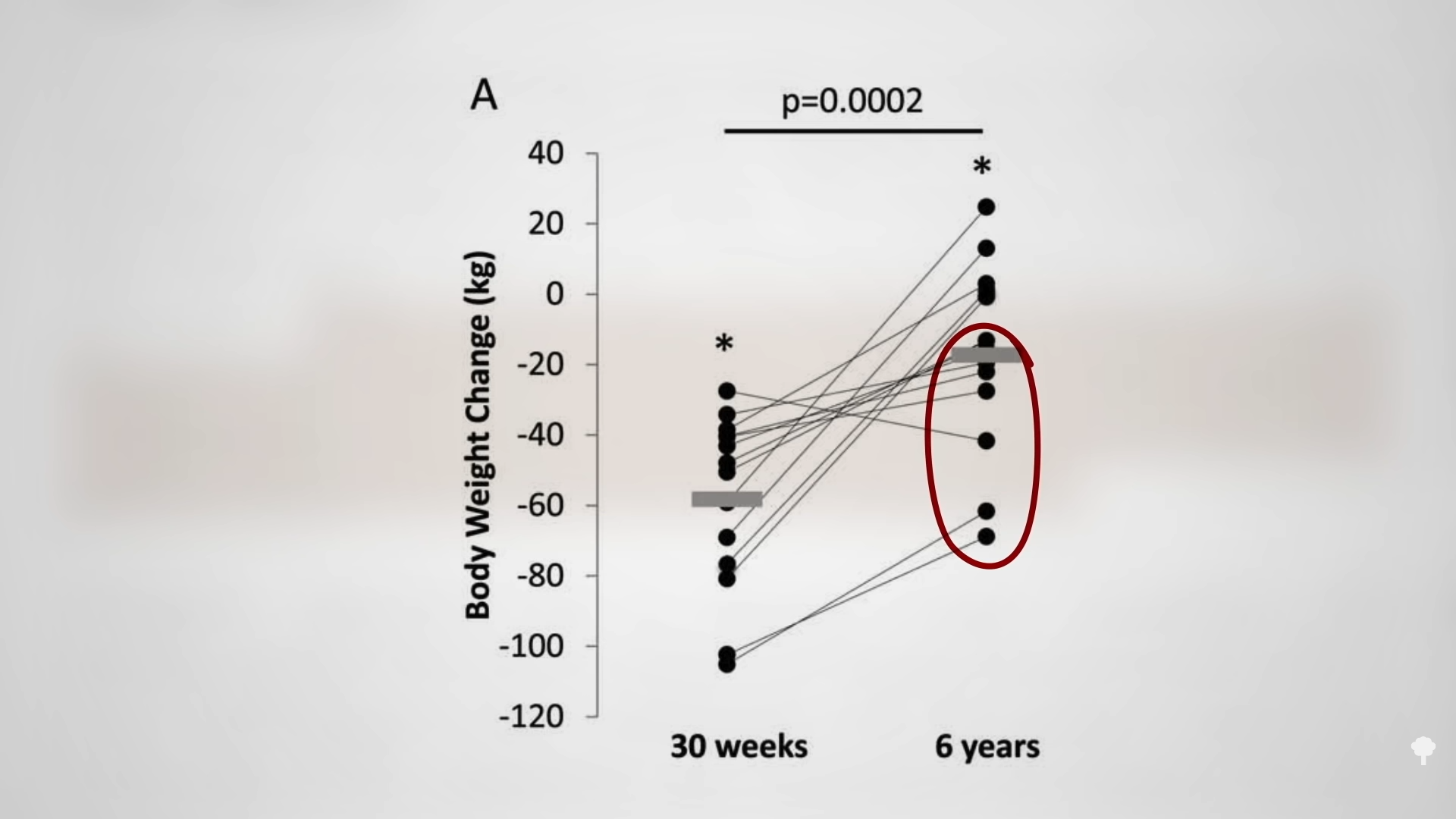
 What happened nine years later? “Therapeutic Fasting in Morbid Obesity”
What happened nine years later? “Therapeutic Fasting in Morbid Obesity” 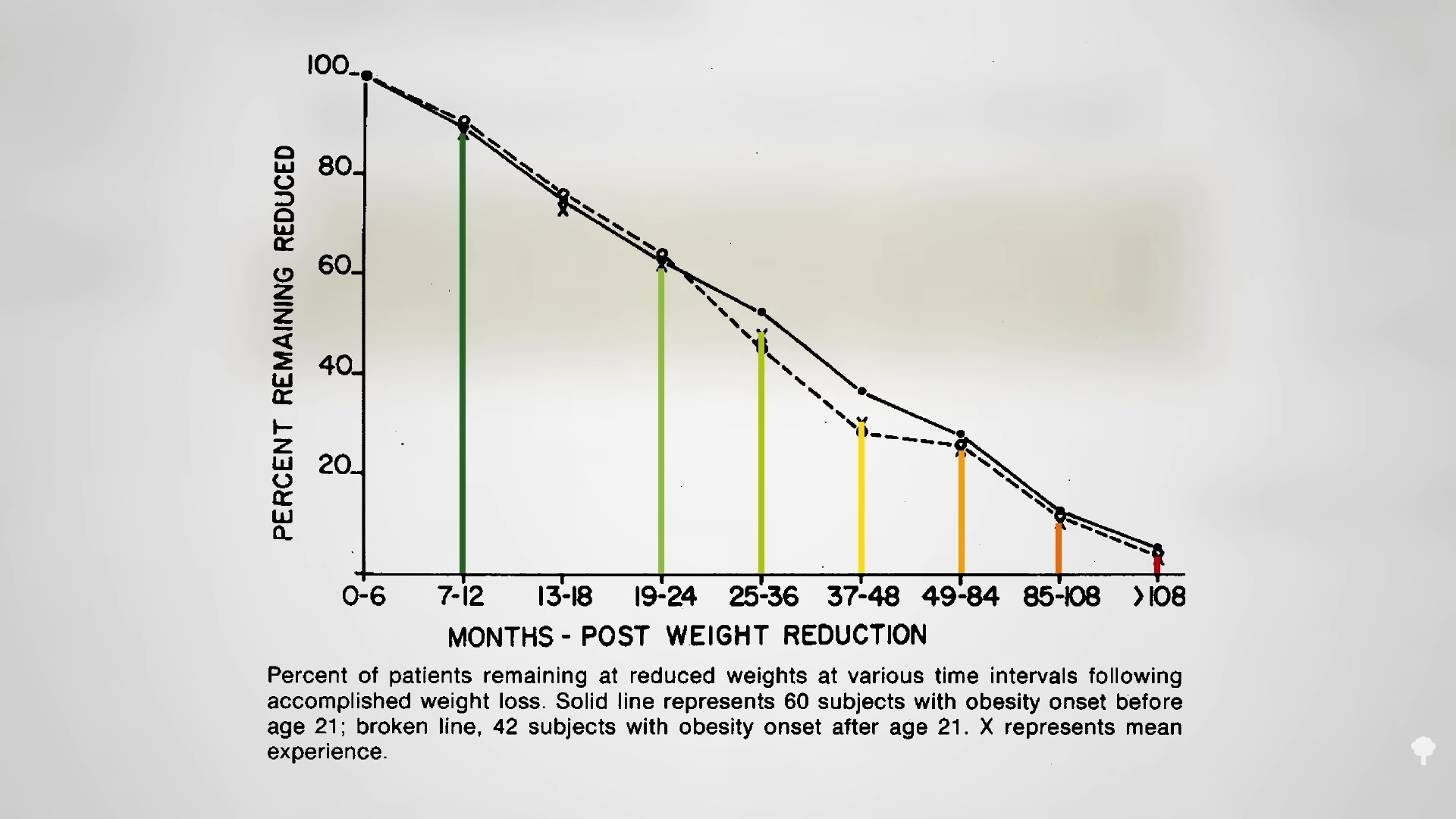 The small minority for whom fasting
The small minority for whom fasting 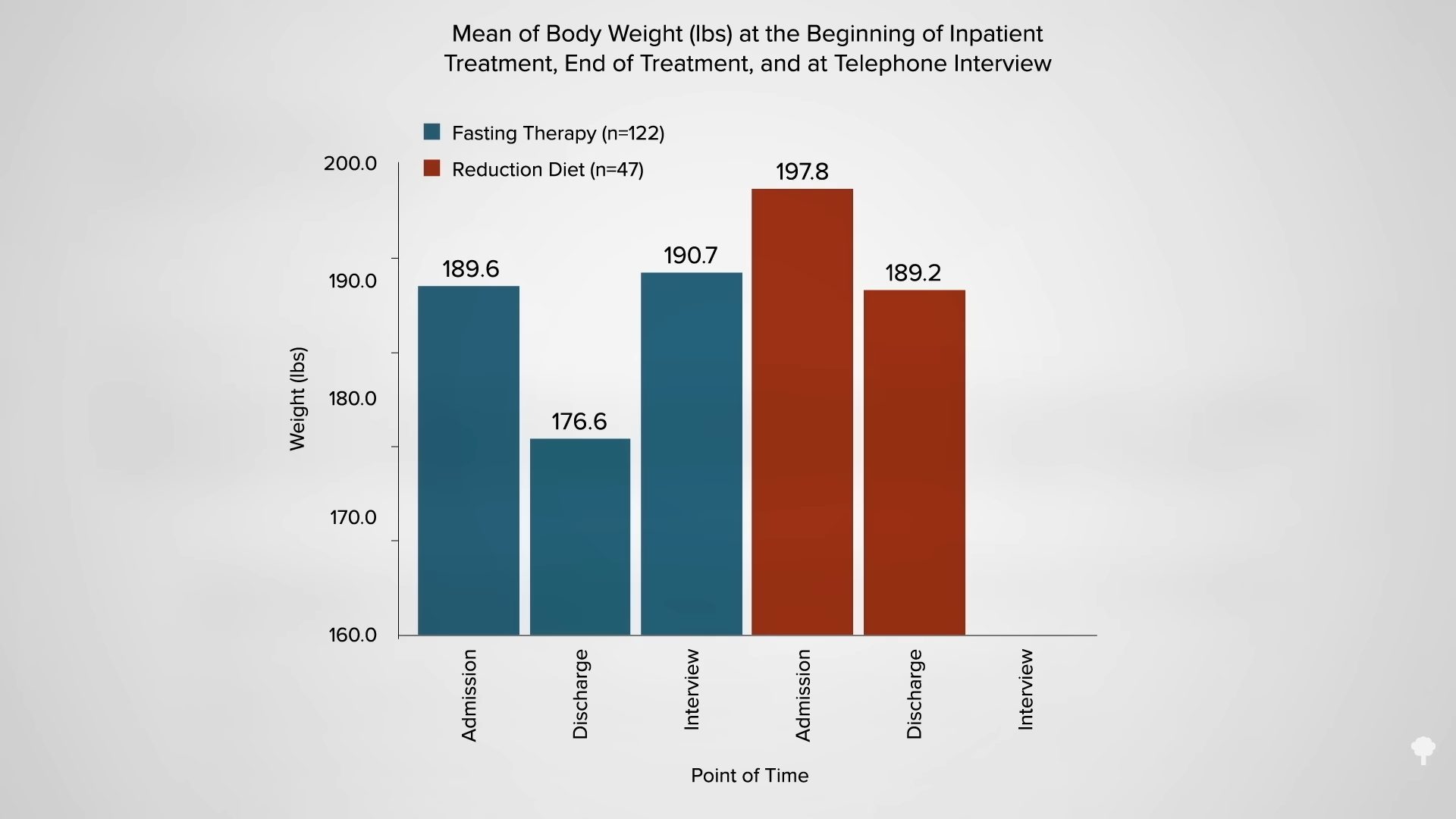
 This is the follow-up to
This is the follow-up to 









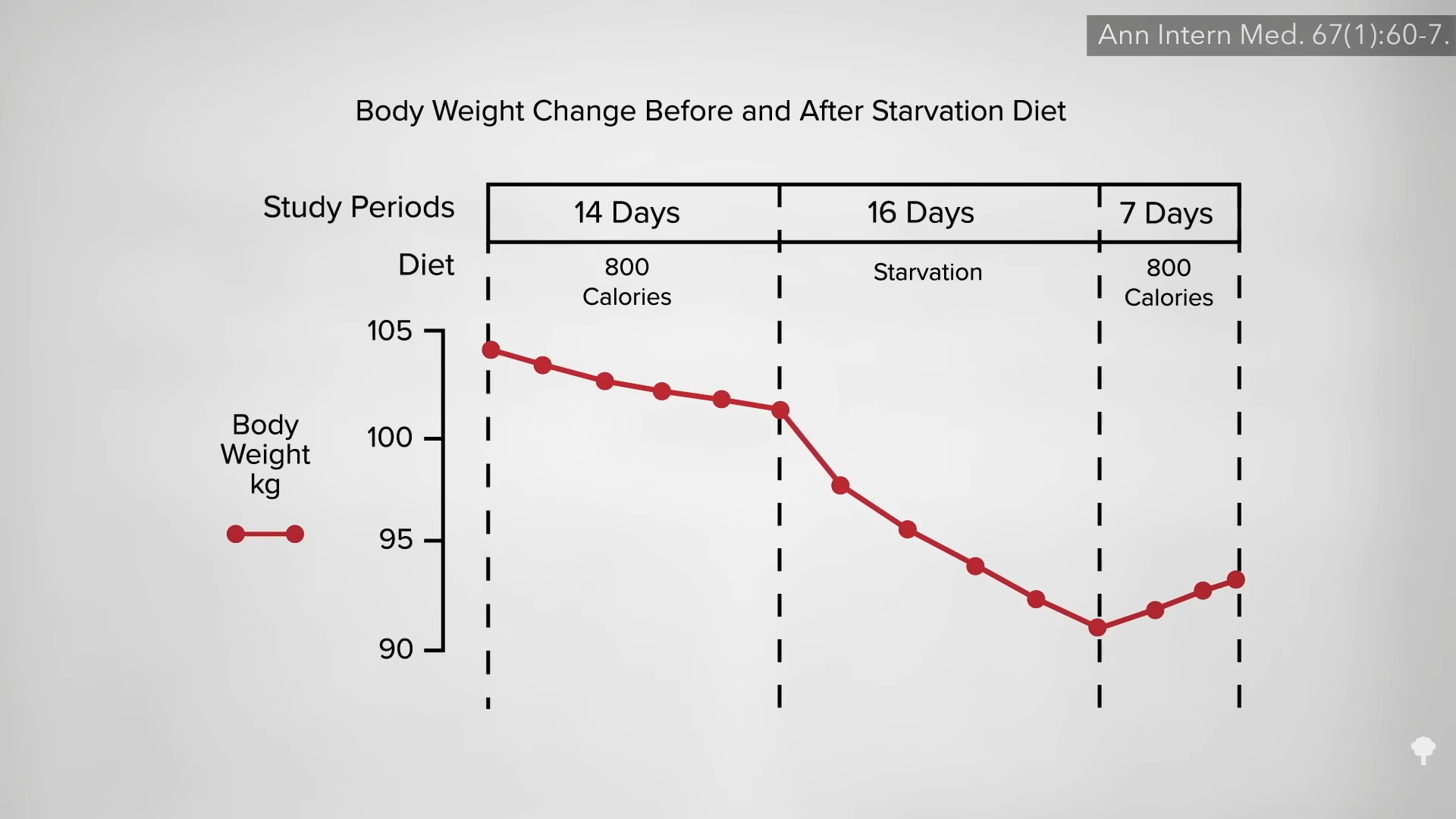
 In my previous video, I dive into how
In my previous video, I dive into how 


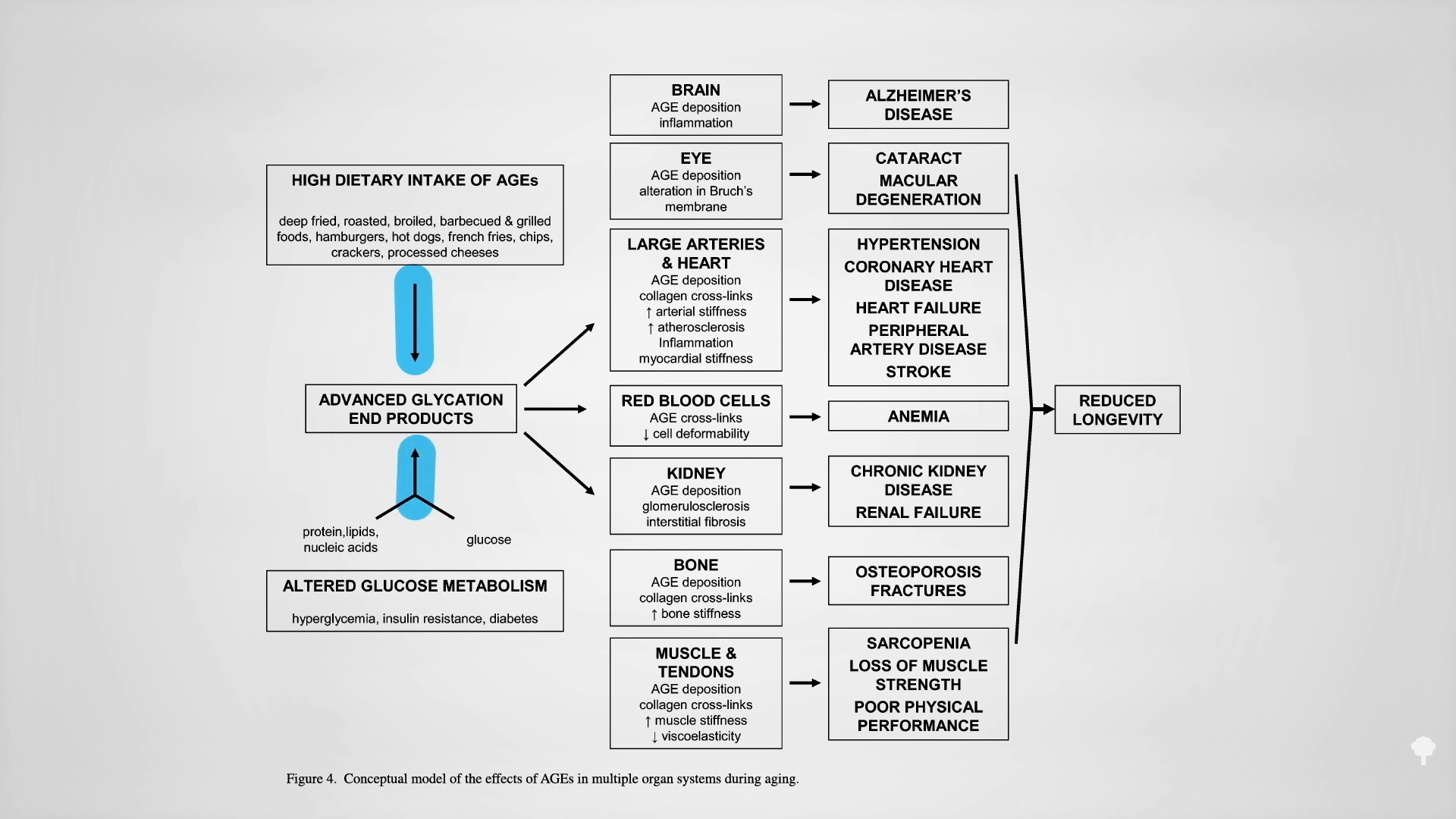
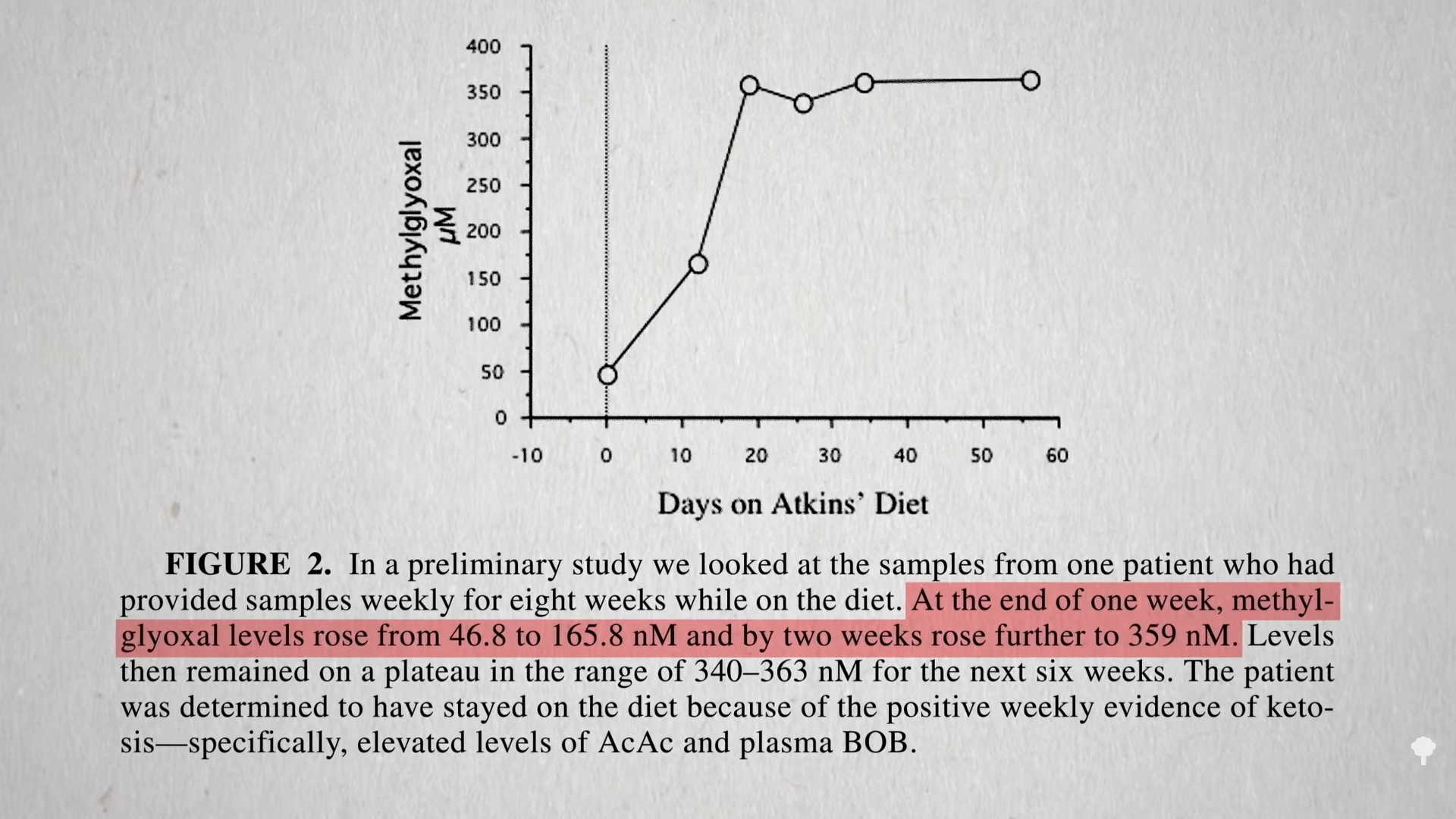
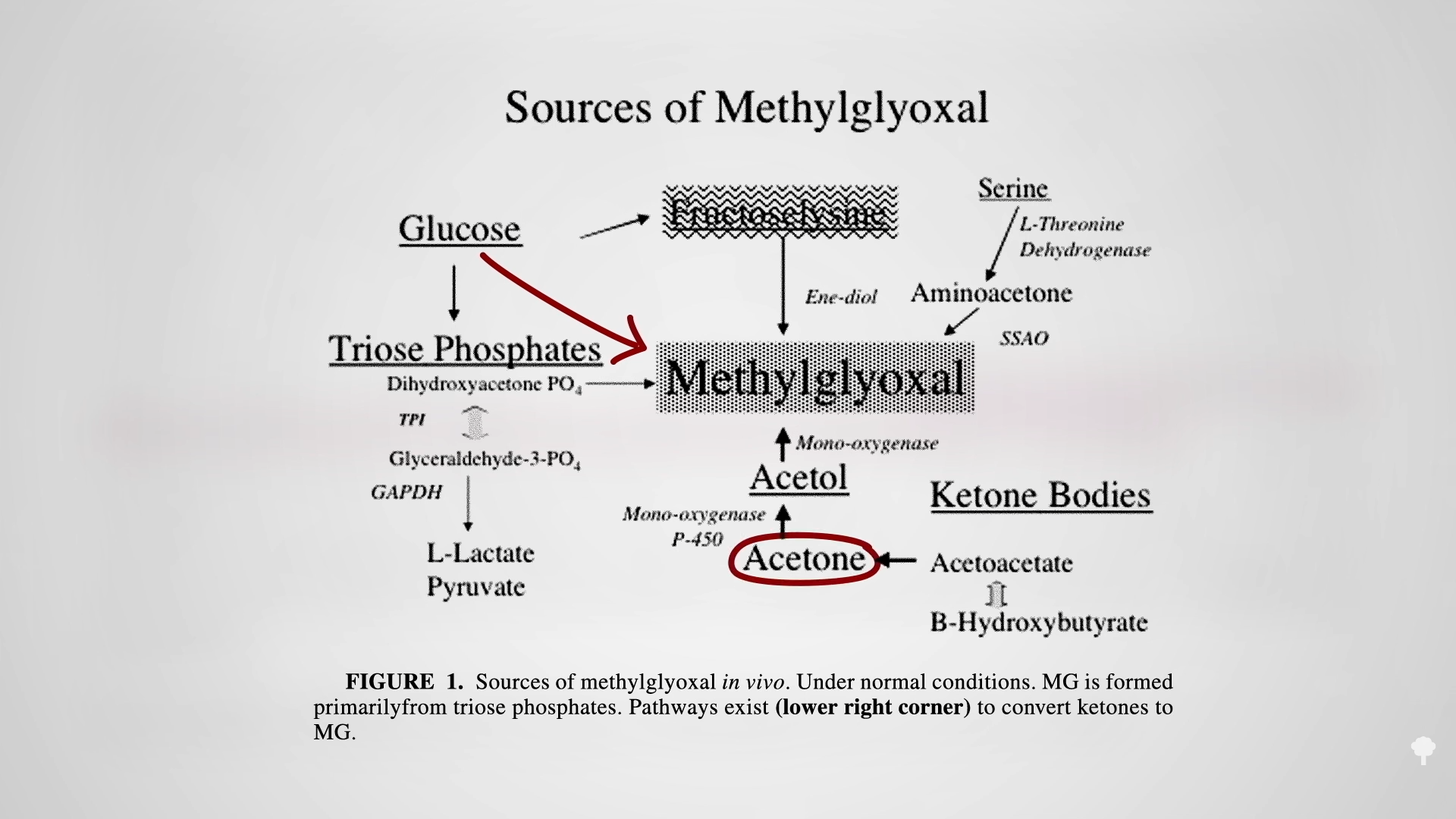
 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal