
[ad_1]
[ad_2]

[ad_1]
Take a drive down Main Street of just about any major city in the country, and—with the housing market ground to a halt—you might pass more churches for sale than homes. This phenomenon isn’t likely to change anytime soon; according to the author of a 2021 report on the future of religion in America, 30 percent of congregations are not likely to survive the next 20 years. Add in declining attendance and dwindling affiliation rates, and you’d be forgiven for concluding that American religion is heading toward extinction.
But the old metrics of success—attendance and affiliation, or, more colloquially, “butts, budgets, and buildings”—may no longer capture the state of American religion. Although participation in traditional religious settings (churches, synagogues, mosques, schools, etc.) is in decline, signs of life are popping up elsewhere: in conversations with chaplains, in communities started online that end up forming in-person bonds as well, in social-justice groups rooted in shared faith.
For centuries, houses of worship have been the center of their communities, where people met their friends and partners, where they raised their kids, where they found solace, where they broke bread, where they organized around important issues.
As Robert D. Putnam and David E. Campbell demonstrated in their 2010 book, American Grace: How Religion Divides and Unites Us, most Americans no longer orient their lives around houses of worship. And that loss is about more than just missing out on prayer services. It means that when people move to a new city, they have to work much harder to find new friends than previous generations did. When someone falls ill, they might not have a cadre of their fellow faithful to offer home-cooked meals and prayers for healing. This reorientation away from houses of worship is one of the factors that has led to the decline of a sense of community, the rise of social isolation, and the corresponding negative effects on public health, especially for older adults.
Religion has historically done four main “jobs.” First, it provides a framework for meaning-making, whether helping our ancient ancestors explain why it rained when it rained, or helping us today make sense of why bad things happen to good people. Second, religion offers rituals that enable us to mark time, process loss, and celebrate joys—from births to coming of age to family formation to death. Third, it creates and supports communities, allowing each of us to find a place of belonging. And finally, fueled by each of the first three, religion inspires us to take prophetic action—to partake in building a world that is more just, more kind, and more loving. Through the pursuit of these four jobs, religious folks might also experience a sense of wonder, discover some new truth about themselves or the world, or even have an encounter with the divine.
So rather than asking how many people went to church last Sunday morning, we should ask, “Where are Americans finding meaning in their lives? How are they marking the passing of sacred time? Where are they building pockets of vibrant communities? And what are they doing to answer the prophetic call, however it is that they hear it?”
There have never been more ways to answer these questions, even if fewer and fewer people are stepping into a sanctuary. People are meaning-making in one-on-one sessions with spiritual directors and chaplains. One in four Americans—across racial and religious (and nonreligious) backgrounds—has met with a chaplain in their lifetime, according to a recent survey that Gallup conducted for the Chaplaincy Innovation Lab, of which one of us, Wendy, is a founder. Most find their time with chaplains valuable.
People are preparing for the end of life with the Shomer Collective, a group that helps people as they prepare for and navigate the end of life, offering wisdom from the Jewish tradition. Death doulas now work with people from a variety of backgrounds, giving hand massages, preparing food, and doing much more for dying people and their loved ones.
These spiritual offerings are not just for individuals. People are gathering in communities in new ways to celebrate Shabbat rituals with OneTable, and mourning the loss of their loved ones with the Dinner Party. They’re joining small groups through the New Wine Collective, a movement helping people build spiritual communities, and the Nearness, a platform for nurturing your spiritual life while discovering community online. And they’re pursuing faith-driven justice work with organizations such as the Faith Matters Network and Living Redemption.
Many theological schools aren’t yet training their students to reimagine how to serve people outside traditional religious contexts. Most are still preparing clergy to serve in congregations, a job with diminishing prospects these days. However, a growing number of groups, many of them led by seminary graduates, support spiritual leaders who are fostering new kinds of spirituality in their flocks.
The Glean Network, of which Elan is the founding director, has incubated more than 100 faith-rooted ventures over the past seven years through its partnership with Columbia Business School. Some of these programs focus on meaning-making, many on building communities, others on creative rituals, and still others on answering a prophetic call. The Chaplaincy Innovation Lab brings chaplains traditionally siloed in the settings where they work—health care, the military, higher education, prisons—into a broader learning community. More than 4,000 chaplains belong to the Lab’s private Facebook group—what we believe to be the largest virtual gathering of chaplains in the world—sharing advice, insights, and improvisational rituals from around the globe. These networks and a growing number of others equip spiritual leaders from a broad range of faith traditions to do their best work, and challenge theological schools to make their education more responsive, expansive, accessible, and practical.
This swell of spiritual creativity comes at a time when Americans seem to need it most. We are more lonely, more divided, less hopeful, and less trusting than in previous decades. And while there is much to celebrate as these new offerings take shape, their growth comes alongside an unprecedented decline in religious affiliation, which does entail losing some things that are unlikely to be replaced by these creative efforts.
We are witnessing a tectonic shift in the landscape of American religious life. Putnam was right when he declared a decade ago that religious disaffiliation has “the potential for completely transforming American society.” But he also predicted that it “has the potential for just eliminating religion,” and we beg to differ. Before we conclude that this transformation is solely about decline, let’s make sure we’re looking in all the right places.
[ad_2]
Wendy Cadge
Source link

[ad_1]
A new subvariant of SARS-CoV-2 is rapidly taking over in the U.S.—the most transmissible that has ever been detected. It’s called XBB.1.5, in reference to its status as a hybrid of two prior strains of Omicron, BA.2.10.1 and BA.2.75. It’s also called “Kraken.”
Not by everyone, though. The nickname Kraken was ginned up by an informal group of scientists on Twitter and has caught on at some—but only some—major news outlets. As one evolutionary virologist told The Atlantic earlier this week, the name—at first glance, a reference to a folkloric sea monster—“seems obviously intended to scare the shit out of people” and serves no substantive purpose for communicating science.
Yes, Kraken is klickbait. It’s arbitrary, unofficial, and untethered to specific facts of evolution or epidemiology—a desperate play to get attention. And mazel tov for that. We should all rejoice at this stupid name’s arrival. Long live the Kraken! May XBB.1.5 sink into the sea.
Since Omicron spread around the world in the fall of 2021, we’ve been subject to a stultifying slew of jargon from the health authorities: Miniature waves of new infections keep lapping at our shores, while the names of the Omicron subvariants that produce them slop together in a cryptic muck: XBB.1.5 has overtaken BA.5 in recent weeks, and also BF.7, as well as BQ.1 and BQ.1.1; in China, BA.5.2 is quickly spreading too. One might ask, without a shred of undue panic, how worried we should be—but the naming scheme itself precludes an answer. You don’t even need to ask, it says. You’ll never fully understand.
This isn’t subtext; it’s explicit. A spokesperson for the World Health Organization told my colleague Jacob Stern that people should be grateful for the arcane pronouncements of our leading international consortia. “The public doesn’t need to distinguish between these Omicron subvariants in order to better understand their risk or the measures they need to take to protect themselves,” he said. “If there is a new variant that requires public communication and discourse, it would be designated a new variant of concern and assigned a new label.” In other words: None of what we’re seeing now is bad enough to merit much attention. You don’t need to make any brand-new precautions, so we don’t need to talk about it.
The public may not need to draw distinctions. But do those distinctions really need to be obscured? A different set of names, one that isn’t precision-engineered to harpoon people’s interest, wouldn’t have to fool us into feeling false alarm. It’s not as though our habit of assigning common names to storms leads to widespread panic starting every summer. When Hurricane Earl appeared last September, no one rushed into a bunker just because they knew what it was called. Then Ian came a few weeks later, and millions evacuated.
Granted, Kraken sounds a bit more ominous than Earl. (Of all the labels that could be given to the latest version of a deadly virus, it’s not the best.) But the name is more befuddling than terrifying: a nitwitted reference, somehow, to ferocity, absurdity, and conspiratorial delusion all at once. Even so, a silly name still has the virtue of being a name, while a string of numbers and letters is just an entry in a database. Kraken doesn’t care if you’re afraid of COVID, and it doesn’t mind if you’re indifferent. It only wishes to be understood.
Isn’t that important? A proper name eases conversation (wherever that might lead), and makes it possible to talk about what matters (and what doesn’t). Just try telling the public that Hurricane Earl will be no big deal but Ian is a mortal threat, if instead of “Earl” and “Ian” you had to say “BA.2.12.1” and “B.1.1.529.” The committee that names our storms is chasing clouds instead of clout; it knows that branding efforts make it easier for everyone to stay informed. We might have done the same for SARS-CoV-2, and handed out simple, easy-to-remember names for all the leading Omicron subvariants. (Through 2021, we used Greek letters to describe each major variant.) If Kraken seems alarmist now, that’s because we’re living in a different, dumber timeline, where public legibility has been forbidden. Why give this subvariant a name, the global health officials ask, when it isn’t really that much worse than any other? But that’s a problem of their own creation. If Kraken seems too gaudy, that’s because every other recent name has been too drab.
Having useful, catchy names doesn’t mean avoiding all abstraction. Florida residents were glad to know, last fall, which hurricanes were Category 2 and which were Category 5; and it may be just as useful to remind yourself that Kraken is not now, of its own accord, a “variant of concern,” let alone a “variant of high consequence.” Our trust in those distinctions is a product of their formality: A special group of experts has decided which public threats are the most important. The Kraken name, if it continues to spread, could undermine this useful sense of deference—and leave us in an awkward free-for-all where anyone could give a name to any variant at any time.
For the moment, though, our only recourse is to the numbing nomenclature that is now in place, and to the creaking bureaucracy that delivers it. Any other name for XBB.1.5—any better one than Kraken—would have to come from the WHO, an organization that recently spent five months rebranding monkeypox as “mpox” and that has warned that disease names like “paralytic shellfish poisoning” are unduly stigmatizing to shellfish. Kraken has the crucial benefit of being right in front of us. It’s a stupid name, but it’s a name—and names are good.
[ad_2]
Daniel Engber
Source link

[ad_1]
Roughly a century ago, a new fad diet began to sweep the United States. Hollywood starlets such as Ethel Barrymore supposedly swore by it; the citrus industry hopped on board. All a figure-conscious girl had to do was eat a lot of grapefruit for a week, or two, or three.
The Grapefruit Diet, like pretty much all other fad diets, is mostly bunk. If people were losing weight with the regimen, that’s because the citrus was being recommended as part of a portion-controlled, low-calorie, low-carbohydrate diet—not because it had exceptional flab-blasting powers. And yet, the diet has survived through the decades, spawning a revival in the 1970s and ’80s, a dangerous juice-exclusive spin-off called the grapefruit fast, and even a shout-out from Weird Al; its hype still plagues nutritionists today.
But for every grapefruit evangelist, there is a critic warning of its dangers—probably one with a background in pharmacology. The fruit, for all its tastiness and dietetic appeal, has another, more sinister trait: It raises the level of dozens of FDA-approved medications in the body, and for a select few drugs, the amplification can be potent enough to trigger a life-threatening overdose. For most people, chowing down on grapefruit is completely safe; it would take “a perfect storm” of factors—say, a vulnerable person taking an especially grapefruit-sensitive medication within a certain window of drinking a particular amount of grapefruit juice—for disaster to unfurl, says Emily Heil, an infectious-disease pharmacist at the University of Maryland. But that leaves grapefruit in a bit of a weird position. No one can agree on exactly how much the world should worry about this bittersweet treat whose chemical properties scientists still don’t fully understand.
Grapefruit’s medication-concentrating powers were discovered only because of a culinary accident. Some three decades ago, the clinical pharmacologist David Bailey (who died earlier this year) was running a trial testing the effects of alcohol consumption on a blood-pressure medication called felodipine. Hoping to mask the distinctive taste of booze for his volunteers, Bailey mixed it with grapefruit juice, and was shocked to discover that blood levels of felodipine were suddenly skyrocketing in everyone—even those in the control group, who were drinking virgin grapefruit juice.
After running experiments on himself, Bailey confirmed that the juice was to blame. Some chemical in grapefruit was messing with the body’s natural ability to break down felodipine in the hours after it was taken, causing the drug to accumulate in the blood. It’s the rough physiological equivalent of jamming a garbage disposal: Waste that normally gets flushed just builds, and builds, and builds. In this case, the garbage disposal is an enzyme called cytochrome P450 3A4—CYP3A4 for short—capable of breaking down a whole slate of potentially harmful chemicals found in foods and meds. And the jamming culprit is a compound found in the pulp and peel of grapefruit and related citrus, including pomelos and Seville oranges. It doesn’t take much: Even half a grapefruit can be enough to trigger a noticeable interaction, says George Dresser, a pharmacologist at Western University, in Ontario.
The possible consequences of these molecular clogs can sometimes get intense. “On the list of concerning food-drug interactions,” Dresser told me, “arguably, this is the most important one.” When paired with certain heart medications, grapefruit could potentially cause arrhythmias; with some antidepressants, it might induce nausea, vomiting, and an elevated heart rate. Grapefruit can also raise blood levels of the cholesterol drugs atorvastatin and simvastatin, prompting muscle pain and, eventually, muscle breakdown. One of the fruit’s most worrying interactions occurs with an immunosuppressive drug called tacrolimus, frequently prescribed to organ-transplant patients, that may, when amped up by grapefruit, spark headaches, tremors, hypoglycemia, and kidney problems. The citrus even has the ability to lift blood levels of drugs of abuse, including fentanyl, oxycodone, and ketamine.
The full list of potential interactions is long. “More than 50 percent of drugs on the market are metabolized by CYP3A4,” which inhabits both the liver and the gut, says Mary Paine, a pharmacologist at Washington State University. That said, grapefruit can really affect only intestinal CYP3A4, and will cause only a small fraction of those medications to reach notably higher concentrations in the blood (and sometimes only when fairly large quantities of juice are consumed—a quart or more). And only a small fraction of those medications will, when amassed, threaten true toxicity. Our bodies are always making more CYP3A4; stop eating grapefruit and, within a day or two, levels of the protein should more or less reset.
Professionals disagree on how to characterize grapefruit’s risks. To Shirley Tsunoda, a pharmacist at UC San Diego, “it’s definitely a big deal,” especially for the organ-transplant patients to whom she prescribes tacrolimus. Her advice to them is to indulge in grapefruit exactly never—and ideally, tacrolimus-takers should skip related citrus too. Tsunoda even advises people to check the labels of mixed-fruit juices, just in case the makers sneaked some grapefruit in, and she thinks twice when considering noshing on it herself. Paul Watkins, a pharmacologist at the University of North Carolina at Chapel Hill, is much less worried; his bigger concern, he told me, is that the fruit’s reputation as a nemesis of oral medications has been way overblown. He used to study grapefruit-drug interaction but abandoned it years ago, after “I came to the conclusion that it wasn’t very important,” he told me. Some concern is absolutely warranted for certain people on certain meds, he noted. But “I think the actual incidence of patients who have gotten into any kind of trouble or had serious adverse reactions due to taking their drugs with grapefruit juice is very, very small.”
Even the FDA seems a bit unsure of how it feels about the fruit. The agency has stamped the documentation of several grapefruit-sensitive medications with official warnings. But fact sheets for other drugs merely mention that they can interact with grapefruit, say to consult a health-care professional, or just counsel people to avoid drinking the juice in “large amounts.” And as Dan Nosowitz has reported for Atlas Obscura, several interacting drugs that bear warnings in Canada—among them, Viagra, oxycodone, the HIV antiviral Edurant, and the blood pressure medication verapamil—don’t mention any issues with grapefruit in the United States. (When I asked the agency about these discrepancies, a spokesperson wrote, “The FDA is continuously reviewing new information about approved drugs, including studies and reports of adverse events. If the FDA determines there is a safety concern, the agency will take appropriate action.”)
Very little solid data can precisely quantify grapefruit’s perils. Over the years, researchers have documented a number of isolated cases of citrus-drug interactions that prompted urgent medical care. But some of them involved truly exceptional amounts of juice. And citrus stans aren’t constantly dropping dead in clinical trials or nursing homes. Even when Bailey first presented his findings to the greater medical community, “people asked, ‘Where are all the bodies?’” Dresser, who was mentored by Bailey, told me. The paucity of data, Dresser contends, stems in part from health-care workers neglecting to check their patients for a history of juice-chugging.
For now, the conversation has mostly stalled, while grapefruit has served up even more mysteries. In the years since Bailey’s discovery, researchers have found that the fruit might lower the concentration of certain drugs, such as the allergy med fexofenadine, perhaps by keeping the lining of the intestines from absorbing certain compounds. New drugs are a particularly murky area, especially because grapefruit interactions aren’t a typical first priority when a new medication hits the market. The popular COVID antiviral pill Paxlovid, for instance, contains the CYP3A4-susceptible ingredient ritonavir. A Pfizer representative told me that the company is not concerned about toxicity. But Heil wonders whether grapefruit could mildly aggravate some of Paxlovid’s irksome side effects: diarrhea, for instance, or maybe the sour, metallic taste that reminds many people of … well, grapefruit.
That said, most grapefruit lovers need not despair. The fruit is still healthy—chock-full of vitamins and flavor—and yet is often overlooked, says Heidi Silver, a nutrition scientist at Vanderbilt University. Silver and researchers have shown that consuming grapefruit flesh or juice might be able to slightly lower levels of triglycerides and cholesterol. Technically, it can even play a role in weight loss: Snacking on a small portion before a meal can help people feel full faster. Then again, a glass of water will too. Just as grapefruit is not a miraculous vanquisher of fat, it isn’t a ubiquitous killer.
Even people on certain medications may be able to enjoy it if they consult an expert first. Heil’s own father absolutely adores grapefruit, and also happens to take an oral medication that can interact. Swallow them too close together, and he risks dizziness and fatigue. But he and Heil have found a compromise: He can have small portions of grapefruit or its juice in the morning, spaced about 12 hours out from when he takes his meds at bedtime. A few weeks ago, Heil (who thinks grapefruit is disgusting) even gave her dad the green light to enjoy a dinnertime cocktail that contained a small splash of the juice. Maybe the smidge of fruit affected his meds that day. But “it wasn’t going to be the end of the world,” Heil told me. To say that, after all, would have been an exaggeration.
[ad_2]
Katherine J. Wu
Source link

[ad_1]
Winter is here, and so, once more, are mask mandates. After last winter’s crushing Omicron spike, much of America did away with masking requirements. But with cases once again on the rise and other respiratory illnesses such as RSV and influenza wreaking havoc, some scattered institutions have begun reinstating them. On Monday, one of Iowa’s largest health systems reissued its mandate for staff. That same day, the Oakland, California, city council voted unanimously to again require people to mask up in government buildings. A New Jersey school district revived its own mandate, and the Philadelphia school district announced that it would temporarily do the same after winter break.
The reinstated mandates are by no means widespread, and that seems unlikely to change any time soon. But as we trudge into yet another pandemic winter, they do raise some questions. What role should masking play in winters to come? Is every winter going to be like this? Should we now consider the holiday season … masking season?
These questions don’t have simple answers. Regardless of what public-health research tells us we should do, we’ve clearly seen throughout the pandemic that limits exist to what Americans will do. Predictably, the few recent mandates have elicited a good deal of aggrievement and derision from the anti-masking set. But even many Americans who diligently masked earlier in the pandemic seem to have lost their appetite for this sort of intervention as the pandemic has eased. In its most recent national survey of health behavior, the COVID States Project found that only about a quarter of Americans still mask when they go out, down from more than 80 percent at its peak. Some steadfast maskers have started feeling awkward: “I have personally felt like I get weird looks now wearing a mask,” Saskia Popescu, an epidemiologist at George Mason University, told me.
Even so, masking remains one of the best and least obtrusive infection-prevention measures we have at our disposal. We haven’t yet been slammed this winter by another Omicronlike variant, but the pandemic is still here. COVID cases, hospitalizations, and deaths are all rising nationally, possibly the signs of another wave. Kids have been hit especially hard by the unwelcome return of influenza, RSV, and other respiratory viruses. All of this is playing out against the backdrop of low COVID-19-booster uptake, leaving people more vulnerable to death and severe disease if they get infected.
All of which is to say: If you’re only going to mask for a couple of months of the year, now is a good time. “Should people be masking? Absolutely yes, right now,” Seema Lakdawala, a flu-transmission expert at Emory University, told me. That doesn’t mean masking everywhere all the time. Lakdawala masks at the grocery store, at the office, and while using public transportation, but not when she goes out to dinner or attends parties. Those activities pose a risk of infection, but Lakdawala’s goal is to reduce her risk, not to minimize it at all costs. A strategy that prevents you from enjoying the things you love most is not sustainable.
Both Lakdawala and Popescu were willing to go so far as to suggest that masking should indeed become a seasonal fixture—just like skiing and snowmen, only potentially lifesaving and politically radioactive. Even before the pandemic, influenza alone killed tens of thousands of Americans every year, and more masking, even if only in certain targeted settings, could go a long way toward reducing the toll. “If we could just say, Hey, from November to February, we should all just mask indoors,” Lakdawala said, that would do a lot of good. “The idea of the unknown and the perpetualness of two years of things coming on and off, and then the confusing CDC county-by-county guideline—it just sort of makes it harder for everybody than if we had a simple message.” Universal mandates or recommendations that people mask at small social gatherings are probably too much to ask, Lakdawala told me. Instead, she favors some limited, seasonal mandates, such as on public transportation or in schools dealing with viral surges.
David Dowdy, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health, is all for masking season, he told me, but he’d be more hesitant to resort to mandates. “It’s hard to impose mandates without a very strong public-health rationale,” he said, especially in our current, hyperpolarized climate. And although that rationale clearly existed for much of the past two crisis-ridden years, it’s less clear now. “COVID is no longer this public-health emergency, but it’s still killing thousands of people every week, hundreds a day … so it becomes a more challenging balancing act,” Dowdy said.
Rather than requirements, he favors broad recommendations. The CDC, for instance, could suggest that during flu season, people should consider wearing masks in crowded indoor spaces, the same way it recommends that everyone old enough get a flu shot each year. (Although the agency has hardly updated its “Interim Guidance” on masks and the flu since 2004, Director Rochelle Walensky has encouraged people to mask up this winter.) Another strategy, Dowdy said, could be making masks more accessible to people, so that every time they enter a public indoor space, they have the option of grabbing an N95.
The course of the pandemic has both demonstrated the efficacy of widespread masking and rendered that strategy so controversial in America as to be virtually impossible. The question now is how to negotiate those two realities. Whatever answer we come up with this year, the question will remain next year, and for years after that. The pandemic will fade, but the coronavirus, like the other surging viruses this winter, will continue to haunt us in one form or another. “These viruses are here,” Lakdawala said. “They’re not going anywhere.”
[ad_2]
Jacob Stern
Source link

[ad_1]
This past spring, Amanda Goldberg crouched in the leafy undergrowth of a southwestern Virginia forest and attempted to swab a mouse for COVID. No luck; its nose was too tiny for her tools. “You never think about nostrils until you start having to swab an animal,” Goldberg, a conservation biologist at Virginia Tech University, told me. Larger-nosed creatures that she and her team had trapped, such as raccoons and foxes, had no issue with nose swabs—but for mice, throat samples had to do. The swabs fit reasonably well into their mouths, she said, though they endured a fair bit of munching.
Goldberg’s throat-swabbing endeavors were part of a study she and her colleagues devised to answer an unexplored question: How common is COVID in wildlife? Of the 333 forest animals her team swabbed around Blacksburg, Virginia, spanning 18 species, one—an opossum—tested positive. This was to be expected, Goldberg said; catching a wild animal that happened to have an active infection right when it was swabbed was like finding Waldo. But the researchers also collected blood samples, and those were more telling about whether the animals had experienced previous bouts with COVID. Analysis by the Molecular Diagnostics Lab and the Fralin Biomedical Research Institute at Virginia Tech revealed antibodies across 24 animals spanning six species, including the opossum, the Eastern gray squirrel, and two types of mice. “Our minds were blown,” Goldberg said. “It was basically every species we sent” to the lab.
That animals can get COVID is one of the earliest things we learned about the virus. Despite the endless debate over its origins, SARS-CoV-2 most likely jumped from an animal through an intermediate host to humans in Wuhan. Since then, it has since spread back to a range of animals. People have passed it to household pets, such as dogs and cats, and to a Disney movie’s worth of beasts, including lions, hippos, hyenas, tigers, mink, and hamsters. Three years into the pandemic, animals are still falling sick with COVID, just as we are. COVID is likely circulating more widely in animals than we are aware of, Edward Holmes, a biologist at the University of Sydney, told me. “In all my 30-plus years of doing work on this subject, I have never seen a virus that can infect so many animal species,” he said. More than 500 other mammal species are predicted to be highly susceptible to infection.
Given that most people nowadays aren’t fretting too much about human-to-human spread, it makes sense that animal-to-human spread has largely been forgotten. But even when there are so many other pandemic concerns, animal COVID can’t be ignored. The consequences of sustained animal transmission are exactly the same as they are in people: The more COVID spreads, the more opportunities the virus has to evolve into new variants. What’s most alarming is the chance that one of those variants could spill back into humans. As we’ve known since the pandemic started, SARS-CoV-2 is not a human virus, but one that can infect multiple animals, including humans. As long as animals are still getting COVID, we’re not out of the doghouse either.
Perhaps part of the reason COVID in animals has been overlooked—apart from the fact that they’re not people—is that most species don’t seem to get very sick. Animals that have gotten infected generally exhibit mild symptoms—typically some coughing and sluggishness, as in pumas and lions. But our research has gone only fur-deep. “We certainly can’t ask them, ‘Are you feeling headaches, or sluggish?’” said Goldberg, who worries about long-term or invisible symptoms going undiagnosed in species. And so animal COVID has lingered unchecked, increasing the chances that it could mean something bad for us.
The good news is that the overall risk of getting COVID from animals is considered low, according to the CDC. This is partly explained by evolutionary theory, which predicts that most variants that emerge in an animal population will have adapted to become better at infecting the host animal—not us. But some of them, strictly by chance, “could be highly transmissible or virulent in humans,” Holmes said. “It’s an unpredictable process.” His concern is not that animals will start infecting people en masse—your neighbors are far likelier to do that than raccoons—but that in animals, SARS-CoV-2 could form new variants that can spill over into people. Some scientists believe that Omicron emerged this way in mice, though evidence remains scant.
A troubling sign is that there’s already some evidence that COVID has made its way from humans to animals, where it mutated, and then made its way back into humans. Take white-tailed deer, by now a well-known COVID host. Every fall, hunters take to the golden meadows and reddening forests of southwestern Ontario to shoot the deer, giving researchers an opportunity to test some of the hunted animals for COVID. The species has been infected with the same variants circulating widely in humans—a handful of Staten Island deer caught Omicron last winter, for example—which suggests that people are infecting them. How the deer get infected still isn’t clear: Extended face time with humans, nosing around in trash, or slurping up our wastewater are all possibilities.
The researchers in Canada found not only that some of the animals tested positive, but also that the variant they carried had never before been seen in humans, indicating that the virus had been spreading and mutating within the population for a long time, Brad Pickering, a research scientist for the Canadian government who studied the deer, told me. In fact, the new variant is among the most evolutionarily divergent ones identified so far. But despite its differences, it appeared to have infected at least one person who had interacted with deer the week before falling ill. “We can’t make a direct link between them,” Pickering said, but the fact that such a highly diverged deer variant was detected in a human is very suggestive of how that person got sick.
This research adds to the small but growing body of evidence that the COVID we spread to animals could come back to bite us. Fortunately, this particular spillback does not appear to have had serious consequences for humans; rogue deer variants don’t seem to be circulating in southern Canada. But this is not the sole documented instance of animal-to-human spread: People have been infected by mink in the Netherlands, hamsters in Hong Kong, and a cat in Thailand. Other spillbacks have probably occurred and gone unnoticed. So far, no data show that the animal variants that have spread to humans are more dangerous for us. Even if a potential animal variant isn’t the next Omicron, it could still be better at dodging our existing treatments and vaccines, Pickering said.
But there is also, frankly, a lack of data. Local wildlife-surveillance efforts led by researchers like Goldberg and Pickering are ongoing, but they do not exist in most countries, Holmes said. An international database of known animal infections, maintained by Complexity Science Hub Vienna, is a promising start. An interactive map shows the locations of previously infected animals, including large hairy armadillos (Argentina), manatees (Brazil), and cats (everywhere). At the very least, with animal COVID, “we need to know what species it’s in, in what abundance, and genetically, what those variants look like,” Holmes said. “It’s absolutely critical to know where [the virus] is going.” Without this, there is no way of knowing how often spillback occurs and whether it puts humans at risk. And we can’t tell whether new COVID variants are also putting animals in danger, Goldberg said; a devastating Omicron-like variant could emerge in their populations too.
The steps we need to take to mitigate the animal-COVID problem—and prevent other zoonotic diseases from jumping into humans—are clear, even if they don’t seem to be happening. Eliminating wet markets where wild animals are sold is an obvious preventive measure, but it has been difficult to implement because the livelihoods and diets of many people, especially in the global South, depend on them. As climate change and land development decimate even more habitats, wildlife will be forced into ever-closer quarters with us, fostering an even more efficient exchange of viruses between species. Unlike mask wearing and other straightforward options for curbing the human spread of COVID, preventing its transmission to, from, and among animals will require major upheavals to the way our societies run, likely far greater than we are willing to commit to.
Humans tend to act like COVID ends up afflicting us after traveling through a long chain of species. But to think so is like living in the Middle Ages, Holmes said, when the Earth was considered the center of the universe. As we learned then, we are not that important: Humans are but a node in an immense network of species that viruses move through in many directions. Just as animal viruses infect us, human viruses can spread to animals (measles, for example, kills a variety of great apes). There are definitely bigger problems than animal COVID—no one needs to hunker down for fear of sneezing deer—but as long as animals keep getting infected, we can’t overlook what that means for us. Paying attention to animal COVID often starts with a single swab—and a snout to stick it in.
[ad_2]
Yasmin Tayag
Source link

[ad_1]
My father was a registered independent for most of my childhood because he resented having to choose. But choosing was not hard for my mother. She was an MSNBC devotee, a liberal Pennsylvania transplant who took her adopted role as an Iowa Democrat seriously. She wanted me to take politics seriously, too.
Which is why, on a freezing January night in 2000, Mom zipped up our coats, buckled 7-year-old me into our white Toyota Previa, and drove us along five miles of gravel to the nearest town: Danville, population 919. It would be my very first Iowa caucus, with New Jersey Senator Bill Bradley and Vice President Al Gore vying for the Democratic nomination. Mom thought Bradley had more personality, so she stood, with me at her side, in his corner of the Danville Elementary School gymnasium. When Bradley was considered not “viable,” per caucus rules, Mom walked us over to Gore’s group, and he was soon declared the winner. Mom recounted all of this recently; I remember little from that night, except the outlines of bulky puffer jackets and a general tingliness at being the only kid in a room full of adults doing something that seemed important.
Accuse me of harboring a pro-caucus bias and you’d be right; I love them and I always have. A caucus is like a primary, but not: There’s no secret ballot. You demonstrate your preference for a candidate by physically moving your body to a different chair or another corner of the gym. Only a few states do it this way, and “this way” looks different everywhere.
After that night in 2000, Mom took me with her at each opportunity. Every four or eight years, we held hands and navigated icy sidewalks after dark. We explored student-less school hallways and cozy church luncheon rooms. We stood under basketball hoops and listened to neighbors argue about candidates as though their opinions really mattered, because that night they actually did.
Over the past half century, Iowa’s prominence in politics became part of its identity—something the state was known for besides its acres of corn and millions of hogs. Iowa doesn’t have any major-league teams to root for, or the kind of glittering cities that draw visitors from all corners of the world. But the caucuses helped make Iowa special—and on the national political stage, they made it relevant.
Still, it’s possible to hold two truths in tension. The caucus is part of Iowa’s identity, and deeply rooted in my own, yet the process has never really been fair—not to many Iowans, and not to other Americans. So, even though I felt a sharp pang of sorrow earlier this month when President Joe Biden suggested that my home state should give up its spot on the early-voting roster, I wasn’t surprised. Most Iowans have seen this day coming. Some are more prepared than others.
Thanks to the caucus, I never thought it was strange that I’d met Barack Obama twice before I turned 20. Nothing seemed shocking about Newt Gingrich showing up to speak at the restaurant where my parents have happy hour on Fridays. I was only slightly unsettled to discover that my high-school friend was having a summertime fling with a political reporter I knew from D.C.
For 50 years, these meet-cutes and history-making appearances have been normal, tradition. Iowans heard Howard Dean make the animalistic roar that supposedly ended his campaign. They sheltered in place with Elizabeth Warren during a tornado. They watched Fred Thompson rolling around the state fair in style, and bore witness to John Delaney’s sad ride down the Giant Slide.
Iowa’s prominence in the process dates back to the 1970s, when the caucuses helped put George McGovern, and later Jimmy Carter, on the proverbial map. State law requires that Iowa holds its caucuses eight days before the first primary happens, hence the quadrennial Iowa–New Hampshire pairing. Most people know this by now; it’s the process they don’t get—the appeal of the thing. The magic.
That’s how many Iowans see the caucus: a messy, intimate project that represents politics in its most sublime form—a dose of pure democracy smack-dab in the middle of Iowa’s fields and farms. I’m not sure about all that. But the caucuses are intimate. You discuss electability with your legs wedged beneath a lunch table designed for children. You look your neighbor in the eye and tell him why he’s wrong. On a school night! During one of his first-ever caucuses, my father, sitting at Senator Bernie Sanders’s table, was approached by a neighbor from Hillary Clinton’s. “Didn’t you hear that Sanders was a conscientious objector?” the man asked. Dad replied that he didn’t realize it was a liability for a presidential candidate to have a conscience. I remember thinking that this was a good comeback.
As a sophomore in college, I viewed the caucus as a noble process, probably because I was reading a lot of Hannah Arendt for class. The German philosopher wrote often about the polis—from which politics is derived—and in The Human Condition she defined it as “the organization of the people as it arises out of acting and speaking together.” The caucus, I thought. How romantic. But at the time, I was unaware—being young and able-bodied and generally self-absorbed—that caucuses don’t allow all people to act and speak together.
Mailing in your candidate preferences has never been an option in the caucuses. And many Iowans are not free at seven on a weeknight in January or February. That includes people working shift jobs, people working late, people with little kids, people with relatives to take care of, people with disabilities, people who don’t drive at night, people who have important plans, people who are simply out of town. Over the summer, state Democratic officials, in a bid to keep their place, finally did propose an absentee option. The DNC was apparently unimpressed.
The other most common criticism of the caucus is that Iowa is too white to make a decision that sets the political tempo for the rest of the country. Iowans would counter that their state proved to be the launching pad for America’s first Black president, but the point is well taken. In 2020, Biden finished fourth in mostly white Iowa, and it took the Black voters of South Carolina to push him to the front of the pack.
Iowa’s critics were vindicated that year, when the caucus became synonymous with chaos. The actual process went relatively smoothly, but a faulty new app and jammed phone lines disrupted the reporting of the results. That year, I’d invited my boyfriend to come to my hometown while I covered the caucuses. I’d wanted him to be charmed by the quaint small-town-ness of it all; instead, I was embarrassed. The entire state was. That was the final straw. This summer, a Democratic National Committee panel required every state to make the case for going early in the primary season. Earlier this month, with Biden’s support, the committee passed a proposal that would reorder which states vote first: South Carolina would start, and Michigan and Georgia would be part of the first five. Iowa was not on the list.
Long-time party activists are suffering varying degrees of disappointment at the news. Some lean more toward acceptance. “We’ve taken our role seriously. I think that it was probably time to move on,” Kurt Meyer, a retiree who’s led caucuses for years in northeast Mitchell County, told me. “As an Iowan who cares about such things, I’m sorry to see it go … but it’s okay.” Then he chuckled: “It’s like an aging ball player saying, It was a good run and I enjoyed those World Series games, but now I’m ready to watch from the comfort of the den with a drink in my hand.”
Others are left with a bitter taste. They have some arguments in their favor, after all: Candidates with no money can travel across Iowa easily and purchase ads cheaply. The caucus process itself allows people to rank their preferences and enables coalition-building among supporters of different candidates. “I don’t think people understood the nuance that was there, and that might be the party’s biggest failure,” Sandy Dockendorff, a longtime caucus leader in the southeast, told me. The result, she said, is that people in flyover country will feel even more neglected than they already do.
“That’s telling a lot of rural folks—a lot of the breadbasket—that we don’t matter,” Dockendorff said. “That’ll be felt for generations.”
Three years ago, I wrote a story about the Iowa Democratic Party’s plan to offer “satellite” caucuses that would let some people with work commitments or disabilities participate remotely. I was critical of the proposal because it wouldn’t solve all of the caucus’s inclusivity problems. After my article ran, a well-known Iowa labor leader emailed me. “I can tell you really dislike Iowa!” he wrote. The note was short, and I was crushed. My chest hurt. Had I betrayed my state with a single, 1,300-word article? But I think I understand how he was feeling. I get it now.
Americans outside the Midwest may soon forget about the Butter Cow. Iowa will take an economic hit if the state doesn’t go first in the Democrats’ nominating process. The restaurants serving tenderloins and chicken lips to eager-to-please politicians won’t make as much; the hotels and bars frequented by the national press corps will suffer. But the real reason these changes will be hard for many Iowans to accept is that a whole lot of pride is tied up in this thing. I hear it when I’m talking on the phone with my parents, and when I’m listening to people like Dockendorff and Meyer reminisce. Caucus advocates claim that Iowans are perfectly suited for the part because they are a particularly discerning people. I don’t think that’s true. But Iowans do take the role seriously—at least the ones who participate.
Iowa Democrats have invested decades of effort into hosting bright-eyed, young campaign staffers from California and Massachusetts in their homes. They’ve given rookie candidates with few resources the space to make a case and a name for themselves. That all of this might soon be ripped away by a faceless group of people in D.C.—who seem to harbor, if not ill will, then at least a light disdain toward Iowa—is hard to swallow. Identity is a tricky thing.
No one is totally sure what happens next. The DNC will vote on the new order in February, and this summer, states will submit plans for the upcoming election. Iowa will have to decide how to play it. If state Democrats agree to move the caucus, in theory that breaks state law; the state attorney general could sue them. Some party leaders seem eager to say “Screw it!” and hold a first-in-the-nation caucus anyway, which could mean that Iowa’s delegates aren’t counted at the national convention. Candidates who campaign for such an unsanctioned event could face repercussions. But whatever happens, after committee members vote and state leaders draw their line in the sand, the Iowa caucus probably won’t look the same.
I don’t get to decide what the best outcome would be, for the state or for the process itself. But for all of my life and 20 years before that, Iowa has enjoyed a very particular feeling—a heady mix of relevance and attention—that has become enmeshed, irrevocably, into Iowans’ sense of their home and themselves. I learned to cherish that feeling as a 7-year-old. Maybe it’s time for other people, in some other state, to feel it, too. It will be hard to let go.
[ad_2]
Elaine Godfrey
Source link

[ad_1]
When I called the epidemiologist Denis Nash this week to discuss the country’s worsening COVID numbers, he was about to take a rapid test. “I came in on the subway to work this morning, and I got a text from home,” Nash, a professor at the City University of New York, told me. “My daughter tested positive for COVID.”
Here we go again: For the first time in several months, another wave seems to be on the horizon in the United States. In the past two weeks, reported cases have increased by 53 percent, and hospitalizations have risen by 31 percent. Virus levels in wastewater, which can provide an advance warning of spread, are following a similar trajectory. After the past two years, a winter surge “was always expected,” Nash said. Respiratory illnesses thrive in colder weather, when people tend to spend more time indoors. Thanksgiving travel and gatherings were likewise predicted to drive cases, Anne Rimoin, an epidemiologist at UCLA, told me. If people were infected then, their illnesses will probably start showing up in the data around now. “We’re going to see a surge [that is] likely going to start really increasing in velocity,” she said.
Winter has ushered in some of the pandemic’s worst moments. Last year, Omicron’s unwanted arrival led to a level of mass infection across the country that we had not previously seen. The good news this year is that the current rise will almost certainly not be as bad as last year’s. But beyond that, experts told me, we don’t know much about what will happen next. We could be in for any type of surge—big or small, long or short, national or regional. The only certain thing is that cases and hospitalizations are rising, and that’s not good.
The pandemic numbers are ticking upward across the country, but so far the recent increases seem especially sharp in the South and West. The daily average of reported cases in Mississippi, Georgia, Texas, South Carolina, and Alabama has doubled in the past two weeks. Hospitalizations have been slower to rise, but over the same time frame, daily hospitalizations in California have jumped 57 percent and are now higher than anywhere else in the United States. Other areas of the country, such as New York City, have also seen troubling increases.
Whether the nationwide spike constitutes the long-predicted winter wave, and not just an intermittent rise in cases, depends on whom you ask. “I think it will continue,” Gregory Poland, a professor of medicine at the Mayo Clinic, told me. “We will pour more gas on the fire with Christmas travel.” Others hesitated to classify the uptick as such, because it has just begun. “It’s hard to know, but the case numbers are moving in the wrong direction,” Rimoin said. Case counts are unreliable as people have turned to at-home testing (or just not testing at all), though hospitalizations and wastewater readings remain reliable, albeit imperfect, metrics. “I’ve not seen a big enough change to call it a wave,” Susan Kline, an infectious-diseases expert at the University of Minnesota Medical School, told me.
But what to call the ongoing trend matters less than the fact that it exists. For now, what happens next is anyone’s guess. The dominant variants—the Omicron offshoots BQ.1 and BQ.1.1—are worrying, but they don’t pose the same challenges as what hit us last winter. Omicron drove that wave, taking us and our immune systems by surprise. The emergence of a completely new variant is possible this year—and would change everything—but that is considered unlikely.
The lack of data on people’s immune status makes it especially difficult to predict the outcome of the current rise. Widespread vaccination and infection mean we have a stronger wall of immunity now compared with the previous two winters, but that protection inevitably fades with time. The problem is, people fall sick asynchronously and get boosted on their own schedules, so the timing varies for everyone. “We don’t know anything about how long ago people were [vaccinated], and we don’t know anything about hybrid immunity, so it’s impossible to predict” just how bad things could get, Nash said.
Still, a confluence of factors has created the ideal conditions for a sustained surge with serious consequences for those who get sick. Fading immunity, frustratingly low booster uptake, and the near-total abandonment of COVID precautions create ideal conditions for the virus to spread. Meanwhile, treatments for those who do get very sick are dwindling. None of the FDA-approved monoclonal antibodies, which are especially useful for the immunocompromised, works against BQ.1 and BQ.1.1., which make up about 68 percent of cases nationwide. Paxlovid is still effective, but it’s underprescribed by providers and, by one medical director’s estimate, refused by 20 to 30 percent of patients.
The upside is that few people who get COVID now will get very sick—fewer than in previous winters. Even if cases continue to surge, most infections will not lead to severe illness because the bulk of the population has some level of immunity from vaccination, previous infection, or both. Still, long COVID can be “devastating,” Poland said, and it can develop after mild or even asymptomatic cases. But any sort of wave would in all likelihood lead to an uptick in deaths, too. So far, the death rate has remained stable, but 90 percent of people dying now are 65 and older, and only a third of them have the latest booster. Such low uptake “just drives home the fact that we have not really done a good job of targeting the right people around the country,” Nash said.
Even if the winter COVID wave is not ultimately a big one, it will likely be bad news for hospitals, which are already filling up with adults with flu and children with respiratory syncytial virus, or RSV. Many health-care facilities are swamped; the situation will only worsen if there is a big wave. If you need help for severe COVID—or any kind of medical issue—more than likely, “you’re not going to get the same level of care that you would have without these surges,” Poland said. Critically ill kids are routinely turned away from overflowing emergency rooms, my colleague Katherine J. Wu recently reported.
We can do little to predict how the ongoing surge might develop other than simply wait. Soon we should have a better sense of whether this is a blip in the pandemic or something more serious, and the trends of winters past can be helpful, Kline said. Last year, the Omicron-fueled surge did not begin in earnest until mid-December. “We haven’t even gotten to January yet, so I really think we’re not going to know [how bad this surge will be] for two months,” Kline said. Until then, “we just have to stay put and watch.”
It is maddening that, this far into the pandemic, “stay put and watch” seems to be the only option when cases start to rise. It is not, of course: Plenty of tools—masking, testing, boosters—are within our power to deploy to great effect. They could flatten the wave, if enough people use them. “We have the tools,” said Nash, whose rapid test came out negative, “but the collective will is not really there to do anything about it.”
[ad_2]
Yasmin Tayag
Source link

[ad_1]
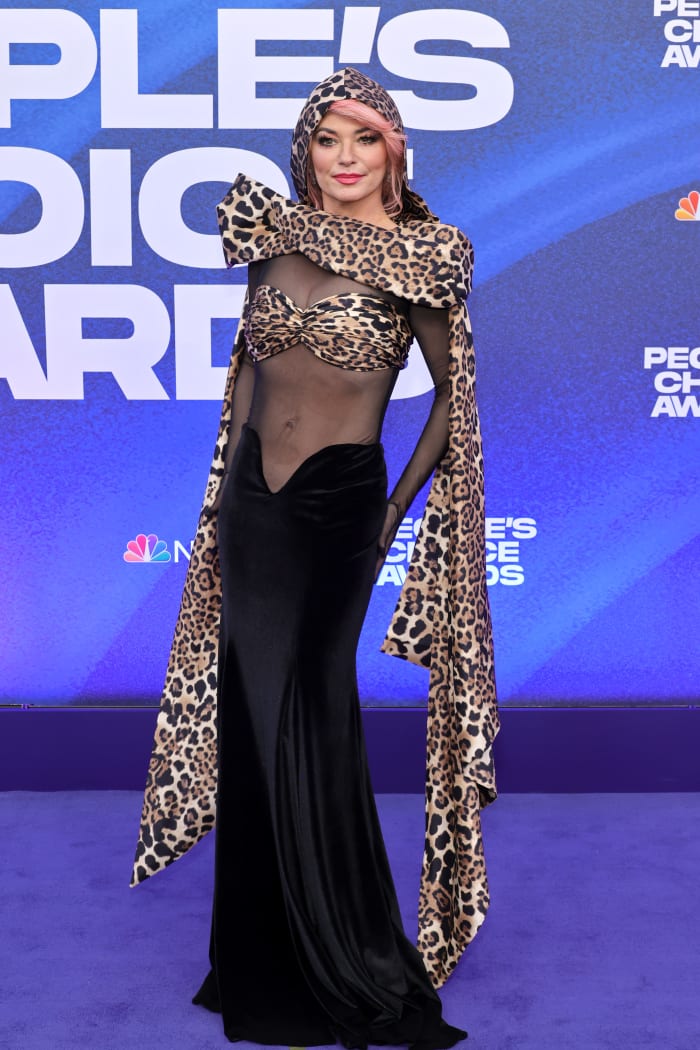
It’s officially award season, with the annual People’s Choice Awards taking place on Tuesday, Dec. 6. Hosted by comedian Kenan Thompson at the Barker Hanger in Santa Monica, the event brought out some of the biggest names in Hollywood. The ceremony honored fan-favorite stars across movies, television and music – and awardees included Selena Gomez, Lizzo, Khloé Kardashian and more.
Outside the venue, the red carpet featured some head-turning looks that deserve their flowers. Before accepting her award for Music Icon of the year, Shania Twain wore Rodarte‘s sheer leopard print dress (an homage to her “That Don’t Impress Me Much” music video). Olivia Wilde, whose film “Don’t Worry Darling” won the Best Drama Movie category, rocked a black see-through Dior gown. Head-to-toe black was a common theme on the red carpet, but some celebs opted for pops of color, like MJ Rodriguez in a flowy white Giambattista Valli ensemble and Laverne Cox in a corseted number from Collina Strada‘s Spring 2023 collection.
Check out all the standout looks from the 2022 People’s Choice Awards red carpet, below.
Scroll to Continue







Want the latest fashion industry news first? Sign up for our daily newsletter.
[ad_2]
India Roby
Source link

[ad_1]
People’s Champion Award: Lizzo
Music Icon Award: Shania Twain
People’s Icon of 2022: Ryan Reynolds
The Movie of 2022
Bullet Train
Doctor Strange in the Multiverse of Madness
Elvis
Jurassic World Dominion
Nope
The Batman
Thor: Love and Thunder
Top Gun: Maverick
The Comedy Movie of 2022
Fire Island
Hustle
Hocus Pocus 2
Marry Me
Senior Year
The Adam Project
The Lost City
Ticket To Paradise
The Action Movie of 2022
Black Adam
Bullet Train
Doctor Strange in the Multiverse of Madness
Jurassic World Dominion
The Batman
The Woman King
Thor: Love and Thunder
Top Gun: Maverick
The Drama Movie of 2022
Nope
Death on the Nile
Don’t Worry Darling
Elvis
Halloween Ends
Luckiest Girl Alive
Scream
Where the Crawdads Sing
The Male Movie Star of 2022
Brad Pitt, Bullet Train
Chris Hemsworth, Thor: Love and Thunder
Chris Pratt, Jurassic World Dominion
Daniel Kaluuya, Nope
Dwayne Johnson, Black Adam
Miles Teller, Top Gun: Maverick
Ryan Reynolds, The Adam Project
Tom Cruise, Top Gun: Maverick
The Female Movie Star of 2022
Elizabeth Olsen, Doctor Strange in the Multiverse of Madness
Gal Gadot, Death on the Nile
Jennifer Garner, The Adam Project
Jennifer Lopez, Marry Me
Joey King , Bullet Train
Keke Palmer, Nope
Queen Latifah, Hustle
Viola Davis, The Woman King
The Drama Movie Star of 2022
Austin Butler, Elvis
Daniel Kaluuya, Nope
Florence Pugh, Don’t Worry Darling
Gal Gadot, Death on the Nile
Harry Styles, Don’t Worry Darling
Jamie Lee Curtis, Halloween Ends
Keke Palmer, Nope
Mila Kunis, Luckiest Girl Alive
The Comedy Movie Star of 2022
Adam Sandler, Hustle
Channing Tatum, The Lost City
Jennifer Garner, The Adam Project
Jennifer Lopez, Marry Me
Julia Roberts, Ticket To Paradise
Queen Latifah, Hustle
Ryan Reynolds, The Adam Project
Sandra Bullock, The Lost City
The Action Movie Star of 2022
Chris Hemsworth – Thor: Love and Thunder
Chris Pratt – Jurassic World Dominion
Dwayne Johnson – Black Adam
Elizabeth Olsen – Doctor Strange in the Multiverse of Madness
Joey King – Bullet Train
Tom Cruise – Top Gun: Maverick
Viola Davis – The Woman King
Zöe Kravitz – The Batman
The Show of 2022
Abbott Elementary
Better Call Saul
Grey’s Anatomy
House of the Dragon
Obi-Wan Kenobi
Saturday Night Live
Stranger Things
This Is Us
The Drama Show of 2022
Better Call Saul
Cobra Kai
Euphoria
Grey’s Anatomy
Law & Order: Special Victims Unit
Ozark
The Walking Dead
This Is Us
The Comedy Show of 2022
Abbott Elementary
Black-ish
Only Murders in the Building
Never Have I Ever
Saturday Night Live
The Woman in the House Across the Street from the Girl in the Window
Young Rock
Young Sheldon
The Reality Show of 2022
90 Day Fiancé: Before the 90 Days
Below Deck Sailing Yacht
Jersey Shore: Family Vacation
Love & Hip Hop: Atlanta
The Kardashians
The Real Housewives of Beverly Hills
Selling Sunset
The Competition Show of 2022
America’s Got Talent
American Idol
Dancing with the Stars
RuPaul’s Drag Race
The Bachelorette
The Masked Singer
Lizzo’s Watch Out for the Big Grrrls
The Voice
The Male TV Star of 2022
Dwayne Johnson, Young Rock
Ewan McGregor, Obi-Wan Kenobi
Ice-T, Law & Order: Special Victims Unit
Jason Bateman, Ozark
Noah Schnapp, Stranger Things
Norman Reedus, The Walking Dead
Oscar Isaac, Moon Knight
Sterling K. Brown, This Is Us
The Female Star of 2022
Millie Bobby Brown, Stranger Things
Ellen Pompeo, Grey’s Anatomy
Kristen Bell, The Woman in the House Across the Street from the Girl in the Window
Maitreyi Ramakrishnan, Never Have I Ever
Mandy Moore, This Is Us
Mariska Hargitay, Law &Order: Special Victims Unit
Quinta Brunson, Abbott Elementary
Selena Gomez, Only Murders in the Building
The Drama TV Star of 2022
Ellen Pompeo, Grey’s Anatomy
Jason Bateman, Ozark
Mandy Moore, This Is Us
Mariska Hargitay, Law & Order: Special Victims Unit
Norman Reedus, The Walking Dead
Sterling K. Brown, This Is Us
Sydney Sweeney, Euphoria
Zendaya, Euphoria
The Comedy TV Star of 2022
Bowen Yang, Saturday Night Live
Dwayne Johnson, Young Rock
Kenan Thompson, Saturday Night Live
Kristen Bell, The Woman in the House Across the Street from the Girl in the Window
Maitreyi Ramakrishnan, Never Have I Ever
Quinta Brunson, Abbott Elementary
Selena Gomez, Only Murders in the Building
Tracee Ellis Ross, Black-Ish
The Daytime Talk Show of 2022
Good Morning America
Live with Kelly and Ryan
The Drew Barrymore Show
The Ellen DeGeneres Show
The Jennifer Hudson Show
The Kelly Clarkson Show
The View
Today with Hoda and Jenna
The Nighttime Talk Show of 2022
Jimmy Kimmel Live!
Last Week Tonight with John Oliver
Late Night with Seth Meyers
The Daily Show
The Late Late Show with James Corden
The Late Show with Stephen Colbert
The Tonight Show Starring Jimmy Fallon
Watch What Happens Live with Andy Cohen
The Competition Contestant of 2022
Charli D’Amelio, Dancing with the Stars
Bosco, RuPaul’s Drag Race
Gabby Windey, The Bachelorette
Mayyas, America’s Got Talent
Noah Thompson, American Idol
Selma Blair, Dancing with the Stars
Teyana Taylor, The Masked Singer
Willow Pill, RuPaul’s Drag Race
The Reality TV Star of 2022
Chrishell Stause, Selling Sunset
Garcelle Beauvais, The Real Housewives of Beverly Hills
Kandi Burruss, The Real Housewives of Atlanta
Kenya Moore, The Real Housewives of Atlanta
Khloé Kardashian, The Kardashians
Kim Kardashian, The Kardashians
Kyle Richards, The Real Housewives of Beverly Hills
Mike “The Situation” Sorrentino, Jersey Shore: Family Vacation
The Bingeworthy Show of 2022
Bridgerton
Bel-Air
Dahmer-Monster: The Jeffrey Dahmer Story
Inventing Anna
Severance
The Bear
The Boys
The Thing About Pam
The Sci-Fi/Fantasy Show of 2022
House of The Dragon
La Brea
Moon Knight
Obi-Wan Kenobi
She-Hulk: Attorney at Law
Stranger Things
The Lord of the Rings: The Rings of Power
The Umbrella Academy
The Male Artist of 2022
Bad Bunny
Charlie Puth
Drake
Harry Styles
Jack Harlow
Kendrick Lamar
Luke Combs
The Weeknd
The Female Artist of 2022
Beyoncé
Camila Cabello
Doja Cat
Lady Gaga
Lizzo
Megan Thee Stallion
Nicki Minaj
Taylor Swift
The Group of 2022
BTS
5 Seconds of Summer
BLACKPINK
Coldplay
Imagine Dragons
Måneskin
OneRepublic
Panic! At The Disco
The Song of 2022
About Damn Time – Lizzo
As It Was – Harry Styles
Break My Soul – Beyoncé
First Class – Jack Harlow
Hold My Hand – Lady Gaga
Me Porto Bonito – Bad Bunny & Chencho Corleone
Super Freaky Girl – Nicki Minaj
Wait For U – Future Featuring Drake & Tems
The Album of 2022
Dawn FM – The Weeknd
Growin’ Up – Luke Combs
Harry’s House – Harry Styles
Midnights – Taylor Swift
Mr. Morale & The Big Steppers – Kendrick Lamar
Renaissance – Beyoncé
Special – Lizzo
Un Verano Sin Ti – Bad Bunny
The Country Artist of 2022
Carrie Underwood
Kane Brown
Kelsea Ballerini
Luke Combs
Maren Morris
Miranda Lambert
Morgan Wallen
Thomas Rhett
The Latin Artist of 2022
Anitta
Bad Bunny
Becky G
Shakira
Karol G
Rauw Alejandro
Rosalía
Sebastián Yatra
The New Artist of 2022
Chlöe
Dove Cameron
GAYLE
Latto
Lauren Spencer-Smith
Muni Long
Saucy Santana
Steve Lacy
The Music Video of 2022
Anti-Hero – Taylor Swift
As It Was – Harry Styles
Left And Right (feat. Jung Kook of BTS) – Charlie Puth
Let Somebody Go – Coldplay X Selena Gomez
Oh My God – Adele
Pink Venom – BLACKPINK
PROVENZA – KAROL G
Yet To Come (The Most Beautiful Moment) Official – BTS
The Collaboration Song of 2022
Left And Right – Charlie Puth Featuring Jung Kook
Bam Bam – Camila Cabello Featuring Ed Sheeran
Do We Have A Problem? – Nicki Minaj X Lil Baby
Freaky Deaky – Tyga X Doja Cat
Hold Me Closer – Elton John & Britney Spears
Jimmy Cooks – Drake Featuring 21 Savage
Party – Bad Bunny & Rauw Alejandro
Sweetest Pie – Megan Thee Stallion & Dua Lipa
The Concert Tour of 2022
BTS, Permission to Dance on Stage
Bad Bunny: World’s Hottest Tour
Billie Eilish: Happier Than Ever, The World Tour
Dua Lipa Future Nostalgia Tour
Ed Sheeran Tour
Harry Styles Love On Tour
Lady Gaga: The Chromatica Ball
Luke Combs: The Middle of Somewhere Tour
The Social Celebrity of 2022
Bad Bunny
Charlie Puth
Doja Cat
Lil Nas X
Lizzo
Reese Witherspoon
Selena Gomez
Snoop Dogg
The Social Star of 2022
Addison Rae
Brent Rivera
Charli D’Amelio
Jay Shetty
Khaby Lame
Mikayla Jane Nogueira
Mr Beast
Noah Beck
The Comedy Act of 2022
Amy Schumer, Whore Tour
Chris Rock, Ego Death World Tour 2022
David Spade, Nothing Personal
Jo Koy, Live from the LA Forum
Kevin Hart, Reality Check
Steve Martin & Martin Short, You Won’t Believe What They Look Like Today
Wanda Sykes, Stand Out: An LGBTQ+ Celebration
Whitney Cummings, Jokes
The Game Changer of 2022
Chloe Kim
LeBron James
Megan Rapinoe
Nathan Chen
Rafael Nadal
Russell Wilson
Serena Williams
Steph Curry
The Pop Podcast of 2022
Anything Goes with Emma Chamberlain
Archetypes
Armchair Expert with Dax Shepard
Call Her Daddy
Conan O’Brien Needs A Friend
Not Skinny But Not Fat
SmartLess
[ad_2]
1096815
Source link

[ad_1]
In China, a dam seems on the verge of breaking. Following a wave of protests, the government has begun to relax some of its most stringent zero-COVID protocols, and regional authorities have trimmed back a slew of requirements for mass testing, quarantine, and isolation. The rollbacks are coming as a relief for the many Chinese residents who have been clamoring for change. But they’re also swiftly tilting the nation toward a future that’s felt inevitable for nearly three years: a flood of infections—accompanied, perhaps, by an uncharted morass of disease and death. A rise in new cases has already begun to manifest in urban centers such as Chongqing, Beijing, and Guangzhou. Now experts are waiting to see just how serious China’s outbreak will be, and whether the country can cleanly extricate itself from the epidemic ahead.
For now, the forecast “is full of ifs and buts and maybes,” says Salim Abdool Karim, an epidemiologist at the Centre for the AIDS Programme of Research in South Africa. Perhaps the worst can be averted if the government does more to vaccinate the vulnerable and prep hospitals for a protracted influx of COVID patients; and if the community at large reinvests in a subset of mitigation measures as cases rise. “There is still the possibility that they may muddle through it without a mass die-off,” says Yanzhong Huang, a senior fellow for global health at the Council on Foreign Relations. “But even the most smooth and orderly transition,” he told me, “will not prevent a surge of cases.”
China represents, in many ways, SARS-CoV-2’s final frontier. With its under-vaccinated residents and sparse infection history, the nation harbors “a more susceptible population than really any other large population I can think of,” says Sarah Cobey, an computational epidemiologist at the University of Chicago. Soon, SARS-CoV-2 will infiltrate that group of hosts so thoroughly that it will be nearly impossible to purge again. “Eventually, just like everyone else on Earth, everyone in China should expect to be infected,” says Michael Worobey, an evolutionary virologist at the University of Arizona.
Whatever happens, though, China’s coming wave won’t recapitulate the one that swept most of the world in early 2020. Though it’s hard to say which versions of the virus are circulating in the country, a smattering of reports confirm the likeliest scenario: BF.7 and other Omicron subvariants predominate. Several of these versions of the virus seem to be a bit less likely than their predecessors to trigger severe disease. That, combined with the relatively high proportion of residents—roughly 95 percent—who have received at least one dose of a COVID vaccine, might keep many people from falling dangerously ill. The latest figures out of China’s CDC marked some 90 percent of the country’s cases as asymptomatic. “That’s an enormous fraction” compared with what’s been documented elsewhere, says Ben Cowling, an epidemiologist at the University of Hong Kong.
That percentage, however, is undoubtedly increased by the country’s ultra-rigorous testing practices, which have been catching silent cases that other places might miss. All of Omicron’s iterations also remain capable of triggering severe disease and long COVID. And there are still plenty of worrying omens that climbing cases could reach a horrific peak, sit on a prolonged plateau, or both.
One of China’s biggest weak spots is its immunity, or lack thereof. Although more than 90 percent of all people in the country have received at least two COVID shots, those over the age of 80 were not prioritized in the country’s initial rollout, and their rate of dual-dose coverage hovers around just 66 percent. An even paltrier fraction of older people have received a third dose, which the World Health Organization recommends for better protection. Chinese officials have vowed to buoy those numbers in the weeks ahead. But vaccination sites have been tougher to access than testing sites, and with few freedoms offered to the immunized, “the incentive structure is not built,” says Xi Chen, a global-health expert at Yale. Some residents are also distrustful of COVID vaccines. Even some health-care workers are wary of delivering the shots, Chen told me, because they’re fearful of liability for side effects.
Regardless of the progress China makes in plugging the holes in its immunity shield, COVID vaccines won’t prevent all infections. China’s shots, most of which are based on chemically inactivated particles of the 2020 version of SARS-CoV-2, seem to be less effective and less durable than mRNA recipes, especially against Omicron variants. And many of China’s residents received their third doses many months ago. That means even people who are currently counted as “boosted” aren’t as protected as they could be.
All of this and more could position China to be worse off than other places—among them, Australia, New Zealand, and Singapore—that have navigated out of a zero-COVID state, says Caitlin Rivers, a senior scholar at the Johns Hopkins Center for Health Security. Australia, for instance, didn’t soften its mitigations until it had achieved high levels of vaccine coverage among older adults, Rivers told me. China has also clung to its zero-COVID philosophy far longer than any other nation, leaving itself to contend with variants that are better at spreading than those that came before. Other countries charted their own path out of their restrictions; China is being forced into an unplanned exit.
What Hong Kong endured earlier this year may hint at what’s ahead. “They had a really, really bad wave,” Kayoko Shioda, an epidemiologist at Emory University, told me—far dwarfing the four that the city had battled previously. Researchers have estimated that nearly half the city’s population—more than 3 million people—ended up catching the virus. More than 9,000 residents died. And Hong Kong was, in some respects, in a better place to ease its restrictions than the mainland is. This past winter and spring, the city’s main adversary was BA.2, a less vaccine-evasive Omicron subvariant than the ones circulating now; officials had Pfizer’s mRNA-based shot on hand, and quickly began offering fourth doses. Hong Kong also has more ICU beds per capita. Map a new Omicron outbreak onto mainland China, and the prognosis is poor: A recent modeling paper estimated that the country could experience up to 1.55 million deaths in the span of just a few months. (Other analyses offer less pessimistic estimates.)
Lackluster vaccination isn’t China’s only issue. The country has accumulated almost no infection-induced immunity that might otherwise have updated people’s bodies on recent coronavirus strains. The country’s health-care system is also ill-equipped to handle a surge in demand: For every 100,000 Chinese residents, just 3.6 ICU beds exist, concentrated in wealthier cities; in an out-of-control-infection scenario, even a variant with a relatively low severe-disease risk would prove disastrous, Chen told me. Nor does the system have the slack to accommodate a rush of patients. China’s culture of care seeking is such that “even when you have minor illness, you seek help in urban health centers,” Huang told me, and not enough efforts have been made to bolster triage protocols. More health-care workers may become infected; patients may be more likely to slip through the cracks. Next month’s Lunar New Year celebration, too, could spark further spread. And as the weather cools and restrictions relax, other respiratory viruses, such as RSV and flu, could drive epidemics of their own.
That said, spikes of illness are unlikely to peak across China at the same time, which could offer some relief. The country’s coming surge “could be explosive,” Cobey told me, “or it could be more of a slow burn.” Already, the country is displaying a patchwork of waxing and waning regulations across jurisdictions, as some cities tighten their restrictions to combat the virus while others loosen up. Experts told me that more measures may return as cases ratchet up—and unlike people in many other countries, the Chinese may be more eager to readopt them to quash a ballooning outbreak.
A major COVID outbreak in China would also have unpredictable effects on the virus. The world’s most populous country includes a large number of immunocompromised people, who can harbor the virus for months—chronic infections that are thought to have produced variants of concern before. The world may be about to witness “a billion or more opportunities for the virus to evolve,” Cowling told me. In the coming months, the coronavirus could also exploit the Chinese’s close interactions with farmed animals, such as raccoon dogs and mink (both of which can be infected by SARS-CoV-2), and become enmeshed in local fauna. “We’ve certainly seen animal reservoirs becoming established in other parts of the world,” Worobey told me. “We should expect the same thing there.”
Then again, the risk of new variants spinning out of a Chinese outbreak may be a bit less than it seems, Abdool Karim and other experts told me. China has stuck with zero COVID so long that its population has, by and large, never encountered Omicron subvariants; people’s immune systems remain trained almost exclusively on the original version of the coronavirus, raising only defenses that currently circulating strains can easily get around. It’s possible that “there will be less pressure for the virus to evolve to evade immunity further,” says Emma Hodcroft, a molecular epidemiologist at the University of Bern; and any new versions of the virus that do emerge might not fare particularly well outside of China. In other words, the virus could end up trapped in the very country that tried to keep it out the longest. Still, with so many people susceptible, Cobey told me, there are zero guarantees.
Either way, viral evolution will plod on—and as it does, the rest of the world may struggle to track it in real time, especially as the cadence of Chinese testing ebbs. Cowling worries that China will have trouble monitoring the number of cases in the country, much less which subvariants are causing them. “There’s going to be a challenge in having situational awareness,” he told me. Shioda, too, worries that China will remain tight-lipped about the scale of the outbreak, a pattern that could have serious implications for residents as well.
Even without a spike in severe disease, a wide-ranging outbreak is likely to put immense strain on China—which may weigh heavily on its economy and residents for years to come. After the SARS outbreak that began in 2002, rates of burnout and post-traumatic stress among health-care workers in affected countries swelled. Chinese citizens have not experienced an epidemic of this scale in recent memory, Chen told me. “A lot of people think it is over, that they can go back to their normal lives.” But once SARS-CoV-2 embeds itself in the country, it won’t be apt to leave. There will not be any going back to normal, not after this.
[ad_2]
Katherine J. Wu
Source link

[ad_1]
Anti-lockdown protests erupted across China following a deadly apartment fire in Xinjiang last week. The country’s zero-COVID policy may have been to blame, as first responders were apparently restricted from accessing the scene. Heavy-handed quarantines and endless testing are causing many harms, including food shortages and widespread unemployment. But they’re also keeping China’s COVID death toll very, very low: A study out in May from Nature Medicine, led by Shanghai researchers, estimated that without these strict measures in place, a massive wave of new Omicron infections could overwhelm critical-care units and leave 1.55 million people dead. As protesters call on the government to loosen up, how do they make sense of this potential trade-off?
Few, if any, of the people in the street are asking for a total rollback of the country’s COVID measures. Global public-health experts and China scholars who have been following the protests either from the ground in China or through contacts overseas told me that the movement lacks a precise set of demands. In general, however, the protesters have expressed a wish for easing restrictions, rather than a to-hell-with-it approach. They may not be opposed to post-exposure quarantine, for example, but they’d like to do it in their homes rather than inside government facilities. And footage of the demonstrations shows that many of the protesters are wearing masks (presumably to protect themselves from the coronavirus) even as they agitate for less aggressive testing programs and greater freedom of movement.
It’s not that people don’t understand the seriousness of COVID, especially in a nation where only two-thirds of those over the age of 80 are fully vaccinated. “People are very much aware of COVID infection, and to some extent, they may even overestimate some of the immediate health risks,” Jeremiah Jenne, a historian and writer based in Beijing, told me. Propaganda circulated by the government has painted other countries as being overrun with deaths from the disease, and China as the only place where people can be safe. But a growing number of citizens, particularly in urban areas and among those who are more internationally aware, are adjusting how they weigh the risks of COVID against the economic hardships and other costs of permanent, draconian restrictions.
The World Cup has helped fuel this change in attitude, China scholars told me. David Moser, a professor at Beijing Capital Normal University who’s been in China for 35 years, pointed to the broadcasts of the matches, which showed crowds of unmasked people in the stands, leading undisturbed lives. Chinese observers “got a sense that other countries are handling this by self-quarantining, by allowing a certain amount of infections, and letting people make their own medical decisions,” he said. Protesters may not expect to venture into stadiums without a mask anytime soon, or travel without restrictions, but they would like to see some steps in that direction. “They’re asking for a plan that provides an effective way to deal with the pandemic and keep people safe,” Jenne said, “not to go to Paris in March.”
Xi Chen, a health-policy professor at the Yale School of Public Health, told me that many young people protesting think the risks are much smaller than the ones described in the study from last May, which predicted 1.55 million deaths. “I was circulating the number from that Nature paper to younger friends in my network earlier this year, [and] they don’t buy this idea.” They know that easing off the zero-COVID policy will lead to people dying, but they don’t imagine it would reach that scale. According to Chen, some protesters are asking that public resources be prioritized for helping older adults and other vulnerable people in an attempt to mitigate the harm. The Nature study, for what it’s worth, estimated that if the Chinese government could fill the gaps in vaccination and provide shots for every eligible senior, the death toll from a rampant COVID outbreak would be roughly 600,000, while adding widespread use of antiviral therapies would drive it down much further. (The numbers from that model might not be exactly right, says Albert Ko, an infectious-disease epidemiologist and physician at the Yale School of Public Health, but they’re within the realm of possibility. “Whether it’s 1 million or 1.5 million or 2 million, that’s a huge burden.”)
Whatever the costs, the protesters are convinced that the zero-COVID policy is unsustainable. Public-health experts agree. “The government should address these concerns, because without jobs, people cannot pay for food and medications,” Chen said. In the end, China will need to navigate reopening while attempting to mitigate loss, Ko told me. “This should have been done much earlier.”
[ad_2]
Zoya Qureshi
Source link

[ad_1]
A canker sore—a painful white ulcer inside the mouth—might be brought on by stress. Or the wrong toothpaste. Or certain foods: tomatoes, peanuts, cinnamon. Or an iron deficiency. Or an allergy. Or a new prescription. Or an underlying autoimmune disease.
Even though millions of people suffer from them every year, researchers still don’t know much about what fundamentally causes these sores. This leaves doctors and dentists stuck playing detective with their patients—running down a checklist, trying to figure out which of more than a dozen potential triggers could’ve set off the gnarly little lesions.
That list is long and spans different specialties in medicine. It includes trauma to the mouth, stress, diet, genetics, hormones, allergies, vitamin deficiencies, autoimmune diseases, and gastrointestinal diseases. Diana V. Messadi, a professor at the UCLA School of Dentistry, told me that canker sores are multifactorial, which makes them hard to study. Cold sores, by comparison, offer a much tidier story: They’re viral infections (herpes simplex) and thus are treatable with antivirals. (Cold sores are pimplelike blisters that usually form around the lips, whereas canker sores are white ulcers that occur inside the mouth.)
Canker sores can be loosely sorted into two buckets. In Bucket A are the smaller, more common sores, the kind a person might get two or three times a year. These sores are bright, nagging, and painful, and they make eating and talking difficult. They usually aren’t life-threatening. In Bucket B are larger cankers, usually more than a centimeter wide. (Technically, a third bucket exists that includes herpetiform, or clustered, sores—but this type is rare.)
Big or small, some sores are linked to an underlying disease, like Crohn’s, Behçet’s, HIV/AIDS, or celiac disease. In a way, these cases are better understood: The sores are a secondary effect of something else going on in the body—something a doctor can test for and identify.
The human mouth is a weird place. Canker sores occur in what’s called the oral mucosa, which is doctor-speak for the skin (it’s not actually skin) inside your mouth. Even though the mucosa is tucked away inside your cheeks, it gets exposed to a lot. Salsa, notes Nasim Fazel, a former professor at UC Davis who started the college’s oral-mucosal clinic, “is a chemical irritant. You don’t rub salsa on your skin.” But people do eat salsa—and chips, nuts, and other foods that are spicy or acidic or sharp, and that can damage the lining of the mouth. Some of these wounds later develop into canker sores.
Because the mouth is dirty, white blood cells like to hang out there; Andres Pinto, a professor at the Case Western Reserve University’s school of Dental Medicine, told me that this way, they can react quickly to a potential infection. But sometimes, this surveillance system fails, and the body can actually self-injure. This is thought to be part of what causes typical canker sores, Pinto explained: Immune dysregulation is the “common denominator” behind the ulcers. Inflammation can help the body heal, but too much inflation can cause the mucosa to break down, which is what we see when we look at the oval-shaped wounds.
Beyond that, canker sores are still idiopathic, meaning doctors don’t really know why they happen. The body’s immune system is deeply complicated; as my colleague Ed Yong wrote in 2020, it’s where “intuition goes to die.” “The problem with all these immune-mediated conditions, oftentimes, is we still don’t know why they come,” Alessandro Villa, the chief of oral medicine at the Miami Cancer Institute, told me. “At the end of the day, it’s still a big mystery.”
Another lingering mystery is why some people get canker sores while others live in ignorant bliss, free of their specific kind of torture. Genetics is starting to help solve that one. “Using sophisticated computers, we can actually detect which genes are associated with what we see in the mouth,” Pinto told me. “What I just said is a big step,” he added. “It took probably 30 years to develop that last sentence.”
More research is needed to better treat patients, especially those with bad or chronic sores. Topical steroids can help, but they don’t address the underlying causes. A spokesperson for the FDA told me there are no available FDA-approved prescription options specifically for canker sores.
Comparatively speaking, the United States does not have a lot of providers that specialize in this area. Fazel, formerly of UC Davis, is a rare combination of dentist and dermatologist who sometimes sees patients with debilitating cases. “I’m kind of using the same meds as I was using 10 years ago,” she told me. “It’s kind of sad.”
Oral-medicine specialists are dentists with extra training in such ailments. But only about 400 practice in the United States, Pinto estimated. A representative for the American Academy of Oral Medicine told me the organization currently has 281 active members (although it noted that there may be additional nonmembers practicing). Fazel, for her part, thinks dermatologists are better equipped to treat canker sores, because dentists “can’t prescribe the big guns.” (The “big guns,” in this case, are medicines that modulate the immune system to calm inflammation.) Even if a patient does manage to see the right provider, that’s only the first step. They’ll still need to go through the checklist, trying to determine what their triggers are—while the bigger question of what actually causes the sores remains unknown.
[ad_2]
Caroline Mimbs Nyce
Source link

[ad_1]
After nearly three years of constantly thinking about COVID, it’s alarming how easily I can stop. The truth is, as a healthy, vaxxed-to-the-brim young person who has already had COVID, the pandemic now often feels more like an abstraction than a crisis. My perception of personal risk has dropped in recent months, as has my stamina for precautions. I still care about COVID, but I also eat in crowded cafés and go mask-free at parties.
Heading into the third pandemic winter, things have changed. Most Americans seem to have tuned out COVID. Precautions have virtually disappeared; except for in the deepest-blue cities, wearing a mask is, well, weird. Reported cases are way down since the spring and summer, but perhaps the biggest reason for America’s behavioral let-up is that much of the country sees COVID as a minor nuisance, no more bothersome than a cold or the flu.
And to a certain degree, they’re right: Most healthy, working-age adults who are up-to-date on their vaccinations won’t get severely ill—especially now that antivirals such as Paxlovid are available. Other treatments can help if a patient does get very sick. “People who are vaccinated and relatively healthy who are getting COVID are not getting that sick,” Lisa Lee, an epidemiologist at Virginia Tech, told me. “And so people are thinking, Wow, I’ve had COVID. It wasn’t that bad. I don’t really care anymore.”
Still, there are many reasons to continue caring about COVID. About 300 people are still dying every day; COVID is on track to be the third-leading cause of death in the U.S. for the third year running. The prospect of developing long COVID is real and terrifying, as are mounting concerns about reinfections. But admittedly, these sometimes manifest in my mind as a dull, omnipresent horror, not an urgent affront. Continuing to care about COVID while also loosening up behaviors is an uncomfortable position to be in. Most of the time, I just try to ignore the guilt gnawing at my brain. At this point, when so few people feel that the potential benefit of dodging an infection is worth the inconvenience of precautions, what does it even mean to care about COVID?
In an ideal epidemiological scenario, everyone would willingly deploy the full arsenal of COVID precautions, such as masking and forgoing crowded indoor activities, especially during waves. But that kind of all-out response no longer makes sense. “It’s probably not realistic to expect people to take precautions every time, perpetually, or even every winter or fall, unless there is a particularly concerning reason to do that,” Jennifer Nuzzo, an epidemiologist at Brown University, told me.
But, now more than ever, we must remember that COVID is not just a personal threat but a community one. For older and immunocompromised people, the risks are still significant. For example, people over 50 account for 93 percent of COVID-related deaths in the U.S., even though they represent just 35.7 percent of the population. As long as the death rate remains as high as it is, caring about COVID should mean orienting precautions to protect them. This idea has been around since the pandemic began, but its prominence faded as Americans put their personal health first. “If you’re otherwise healthy, it’s so easy just to think about yourself,” Lee said. “We have to think very carefully about that other part of infectious disease, which is the part where we can potentially hurt other people.”
Orienting behavior in this way gives low-risk people a way to care about COVID that doesn’t entail constant masking or skipping all indoor activities: They can relax when they know they aren’t going to encounter vulnerable people. Like the productivity adage “work smarter, not harder,” this perspective allows people to take precautions strategically, not always. In practice, all it takes is some foresight. If you don’t live with vulnerable people, make it second nature to ask: Will I be seeing vulnerable people anytime soon? If the answer is no, do whatever you’re comfortable with given your own risk. If you are a healthy 30-something who lives alone, going to a Friendsgiving with other people your age is different from spending Thanksgiving dinner with parents and grandparents.
If you will be seeing someone vulnerable, the most straightforward way to avoid giving them COVID is to avoid getting infected yourself, which means wearing a good mask in public settings and minimizing your interactions with others the week before, in what some experts have called a “mini-quarantine.” Not everyone has that luxury: Parents, for example, have to send their kids to school.
Spontaneous interactions with vulnerable people are trickier to plan for, but they follow the same principle. On a crowded bus, for example, “there’s no question that if you’re close enough to someone who could be hurt by getting COVID and you could have it, then, yeah, a mask is the way to go,” Lee said. Of course, it isn’t always possible to know when someone is high-risk; young people, too, can be medically vulnerable. There’s no clear guidance for those situations, but remaining cautious doesn’t require much effort. “Carry a mask with you,” Lee said. “It’s not a big lift.”
Get boosted—if not for yourself, then for them. Just 11.3 percent of eligible Americans have gotten the latest, bivalent shot, which potentially reduces your chances of getting COVID and passing it along. It also means getting tested, so you know when you’re infectious, and being aware of respiratory symptoms—of any kind. Alongside COVID, the flu and RSV are putting many people in the hospital, especially the very young and the very old. No matter how low your personal risk, if you have symptoms, avoiding transmission is crucial. “A reasonable thing to prioritize is: If you have symptoms, take care to prevent it from spreading,” Caitlin Rivers, an epidemiologist at Johns Hopkins University, told me.
As we move away from a personal approach to COVID, we have an opportunity to expand the idea of what caring looks like. Low-risk people can, and should, take an active role in bolstering the protection of vulnerable people they know. In practical terms, this means ensuring that people in your life who are over 50—especially those over 65—are boosted and have a plan to get Paxlovid if they fall sick, Nuzzo said. “I think our biggest problem right now is that not everybody has enough access to the tools, and that’s a place where people can help.” She noted that she is particularly concerned about older people who struggle to book vaccine appointments online. Caring “doesn’t mean abstaining, per se. It means facilitating. It means enabling and helping people in your community.” This holiday season, caring could mean sitting down at a computer to make Grandma’s booster appointment, or driving her to the drugstore to get it.
If you have lost your motivation to care about COVID, you might find it in the people you love. I didn’t feel a personal need to wear a mask at the concert I attended yesterday, but I did it because I don’t want to accidentally infect my partner’s 94-year-old grandfather when I see him next week. To have this experience of the pandemic is a privilege. Many don’t have the option to stop caring, even for a moment.
Barring another Omicron-esque event, we thankfully won’t ever return to a moment where Americans obsess over COVID en masse. But this virus isn’t going away, so we can’t escape having a population that is split between the high-risk minority and the low-risk majority. Rethinking what it means to care allows for a more nuanced and liveable idea of what responsible behavior looks like. Right now, Nuzzo told me, the language we use to describe one’s position on COVID is “black-and-white, absolutist—you either care or you don’t.” There is space between those extremes. At least for now, it’s the only way to compromise between the world we have and the world we want.
[ad_2]
Yasmin Tayag
Source link

[ad_1]
This piece was originally published by Undark Magazine.
Ben Salentine, the associate director of health-sciences managed care at the University of Illinois Hospital and Health Sciences System, hasn’t been weighed in more than a decade. His doctors “just kind of guess” his weight, he says, because they don’t have a wheelchair-accessible scale.
He’s far from alone. Many people with disabilities describe challenges in finding physicians prepared to care for them. “You would assume that medical spaces would be the most accessible places there are, and they’re not,” says Angel Miles, a rehabilitation-program specialist at the Administration for Community Living, part of the Department of Health and Human Services.
Not only do many clinics lack the necessary equipment—such as scales that can accommodate people who use wheelchairs—but at least some physicians actively avoid patients with disabilities, using excuses like “I’m not taking new patients” or “You need a specialist,” according to a paper in the October 2022 issue of Health Affairs.
The work, which analyzed focus-group discussions with 22 physicians, adds context to a larger study published in February 2021 (also in Health Affairs) that showed that only 56 percent of doctors “strongly” welcome patients with disabilities into their practice. Less than half were “very confident” that they could provide the same quality of care to people with disabilities as they could to other patients. The studies add to a larger body of research suggesting that patients with conditions that doctors may deem difficult to treat often struggle to find quality care. The Americans With Disabilities Act of 1990 (ADA) theoretically protects the one in four adults in the U.S. with a disability from discrimination in public and private medical practices—but enforcing it is a challenge.
Laura VanPuymbrouck, an assistant professor in the Department of Occupational Therapy at Rush University, calls the 2021 survey “groundbreaking—it was the crack that broke the dam a little bit.” Now researchers are hoping that medical schools, payers, and the Joint Commission (a group that accredits hospitals) will push health-care providers for more equitable care.
Due in part to scant data, information about health care for people with disabilities is limited, according to Tara Lagu, a co-author of both the 2021 and 2022 papers and the director of the Institute for Public Health and Medicine’s Center for Health Services & Outcomes Research at Northwestern University Feinberg School of Medicine. The few studies that have been done suggest that people with disabilities get preventive care less frequently and have worse outcomes than their nondisabled counterparts.
About a decade ago, Lagu was discharging a patient who was partially paralyzed and used a wheelchair. The patient’s discharge notes repeatedly recommended an appointment with a specialist, but it hadn’t happened. Lagu asked why. Eventually, the patient’s adult daughter told Lagu that she hadn’t been able to find a specialist who would see a patient in a wheelchair. Incredulous, Lagu started making calls. “I could not find that kind of doctor within 100 miles of her house who would see her,” she says, “unless she came in an ambulance and was transferred to an exam table by EMS—which would have cost her family more than $1,000 out of pocket.”
In recent years, studies have shown that even when patients with disabilities can see physicians, their doctors’ biases toward conditions such as obesity, intellectual disabilities, and substance-use disorders can have profound impacts on the care they receive. Physicians may assume that an individual’s symptoms are caused by obesity and tell them to lose weight before considering tests.
For one patient, this meant a seriously delayed diagnosis of lung cancer. Patients with mobility or intellectual challenges are often assumed to be celibate, so their providers skip any discussion of sexual health. Those in wheelchairs may not get weighed even if they’re pregnant—a time when tracking one’s weight is especially important, because gaining too little or too much is associated with the baby being at risk for developmental delays or the mother being at risk for complications during delivery.
These issues are well known to Lisa Iezzoni, a health-policy researcher at Massachusetts General Hospital and a professor of medicine at Harvard Medical School. Over the past 25 years, Iezzoni has interviewed about 300 people with disabilities for her research into their health-care experiences and outcomes, and she realized that “every single person with a disability tells me their doctors don’t respect them, has erroneous assumptions about them, or is clueless about how to provide care.” In 2016, she decided it was time to talk to doctors. Once the National Institutes of Health funded the work, she and Lagu recruited the 714 physicians that took the survey for the study published in 2021 in Health Affairs.
Not only did many doctors report feeling incapable of properly caring for people with disabilities, but a large majority held the false belief that those patients have a worse quality of life, which could prompt them to offer fewer treatment options.
During the 2021 study, Iezzoni’s team recorded three focus-group discussions with 22 anonymous physicians. Although the open-ended discussions weren’t included in the initial publication, Lagu says she was “completely shocked” by some of the comments. Some doctors in the focus groups welcomed the idea of additional education to help them better care for patients with disabilities, but others said that they were overburdened and that the 15 minutes typically allotted for office visits aren’t enough to provide these patients with proper care. Still others “started to describe that they felt these patients were a burden and that they would discharge patients with disability from their practice,” Lagu says. “We had to write it up.”
The American Medical Association, the largest professional organization representing doctors, declined an interview request and would not comment on the most recent Health Affairs study. When asked about the organization’s policies on caring for patients with disabilities, a representative pointed to the AMA’s strategic plan, which includes a commitment to equity.
Patients with disabilities are supposed to be protected by law. Nearly 50 years ago, Congress passed Section 504 of the Rehabilitation Act of 1973, which prohibited any programs that receive federal funding, such as Medicare and Medicaid, from excluding or discriminating against individuals with disabilities. In 1990, the ADA mandated that public and private institutions also provide these protections.
The ADA offers some guidelines for accessible buildings, including requiring ramps, but it does not specify details about medical equipment, such as adjustable exam tables and wheelchair-accessible scales. Although these items are necessary to provide adequate care for many people with disabilities, many facilities lack them: In a recent California survey, for instance, only 19.1 percent of doctor’s offices had adjustable exam tables, and only 10.9 percent had wheelchair-accessible scales.
Miles says she’s noticed an improvement in care since the ADA went into effect, but she still frequently experiences challenges in health care as a Black woman who uses a wheelchair. “We need to keep in mind the ADA is not a building code. It’s a civil-rights law,” says Heidi Johnson-Wright, an ADA coordinator for Miami-Dade County in Florida, who was not speaking on behalf of the county. “If I don’t have access to a wellness check at a doctor’s office or treatment at a hospital, then you’re basically denying me my civil rights.”
The ADA isn’t easy to enforce. There are no “ADA police,” Johnson-Wright says, to check if doctor’s offices and hospitals are accessible. In many cases, a private citizen or the Department of Justice has to sue a business or an institution believed to be in violation of the ADA. Lawyers have filed more than 10,000 ADA Title III lawsuits each year since 2018. Some people, sympathizing with businesses and doctors, accuse the plaintiffs of profiteering.
And it’s not just about accessible equipment. In 2018, the Justice Department sued a skilled nursing facility for violating the ADA, after the facility refused to treat a patient with a substance-use disorder who needed medication to help maintain sobriety. Since then, the department settled with eight other skilled nursing facilities for similar discrimination. “It is a violation of the ADA” to deny someone care based on the medications they need, Sarah Wakeman, an addiction-medicine specialist at Massachusetts General Hospital, wrote in an email, “and yet continues to happen.”
Indeed, in the focus groups led by Lagu and Iezzoni, some of the doctors revealed that they view the ADA and the people it protects with contempt. One called people with disabilities “an entitled population.” Another said that the ADA works “against physicians.”
The Department of Health and Human Services is aware of the issue. In a response to emailed questions, an HHS spokesperson wrote, “While we recognize the progress of the ADA, important work remains to uphold the rights of people with disabilities.” The Office of Civil Rights, the spokesperson continued, “has taken a number of important actions to ensure that health care providers do not deny health care to individuals on the basis of disability and to guarantee that people with disabilities have full access to reasonable accommodations when receiving health care and human services, free of discriminatory barriers and bias.”
Researchers and advocates told me that the key to improving health care for those with disabilities is addressing it directly in medical education and training. “People with disabilities are probably one of the larger populations” that physicians serve, Salentine said.
Ryan McGraw, a community organizer with Access Living, helps provide education about treating patients with disabilities to medical schools in the Chicago area. He regularly receives positive feedback from medical students but says the information needs to be embedded in the medical-school curriculum, so it’s not “one and done.”
In one effort to address the issue, the Alliance for Disabilities in Health Care Education, a coalition of professionals and educators of which McGraw is a member, put together a list of 10 core competencies that should be included in a doctor’s education, including considerations for accessibility, effective communication, and patient-centered decision making.
One of the simplest solutions might be hanging signs or providing accessible information in exam rooms on patients’ rights. “It’d be there for patients, but it’d be also there as a reminder to the providers. I think that’s a super easy thing to do,” Laura VanPuymbrouck says. Miles says this could be a good start, but “it’s not enough to just give people a little pamphlet that tells you about your rights as a patient.” Although all doctors should be willing and able to care for patients with disabilities, she thinks a registry that shows which providers take certain types of insurance, such as Medicaid, and also have disability accommodations, such as wheelchair-accessible equipment, would go a long way.
Some advocates have called on the Joint Commission for more than 10 years to require disability accommodations for hospitals that want accreditation. The step could be effective, because accreditation “is extremely important” to hospitals, Lagu says.
On January 1, 2023, new Joint Commission guidelines will require that hospitals create plans to identify and reduce at least one health-care disparity among their patients. Improving outcomes for people with disabilities could be one such goal. However, Maureen Lyons, a spokesperson for the Joint Commission, adds, “if individuals circumvent the law, standards won’t be any more effective.”
Finally, Lagu says, “we have to pay more when you are providing accommodations that take time or cost money. There’s got to be some accounting for that in the way we pay physicians.”
One of the most basic things people with disabilities are asking for is respect. The biggest finding of the 2021 survey, Iezzoni says, is that doctors don’t realize that the proper way to determine what accommodations a facility needs for patients with disabilities is to just ask the patients.
“I can’t tell you how many times I go to a doctor’s office and I’m talking, but they’re not hearing anything,” Salentine says. “They’re ready to speak over me.”
[ad_2]
Emma Yasinski
Source link

[ad_1]
In COVID terms, the middle of last autumn looked a lot like this one. After a rough summer, SARS-CoV-2 infections were down; hospitalizations and deaths were in a relative trough. Kids and workers were back in schools and offices, and another round of COVID shots was rolling out. Things weren’t great … but they weren’t the most terrible they’d ever been. There were vaccines; there were tests; there were drugs. The worst winter development the virus might produce, some experts thought, might involve the spawning of some nasty Delta offshoot.
Then, one year ago this week, Omicron appeared. The first documented infection with the variant was identified from a specimen collected in South Africa on November 9, 2021; by December 1, public-health officials had detected cases in countries all around the globe, including the United States. Twenty days later, Omicron had unseated Delta as America’s dominant SARS-CoV-2 morph. The new, highly mutated variant could infect just about anyone it encountered—even if they’d already caught a previous version of the virus or gotten several shots of a vaccine. At the beginning of December, and nearly two years into the pandemic, researchers estimated that roughly one-third of Americans had contracted SARS-CoV-2. By the middle of February this year, that proportion had nearly doubled.
Omicron’s arrival and rapid spread around the world was, and remains, this crisis’s largest inflection point to date. The variant upended scientists’ expectations about SARS-CoV-2’s evolution; it turned having COVID into a horrific norm. Now, as the U.S. approaches its Omicronniversary, conditions may seem ripe for an encore. Some experts worry that the emergence of another Greek-letter variant is overdue. “I’m at a loss as to why we haven’t seen Pi yet,” says Salim Abdool Karim, an epidemiologist at the Centre for the AIDS Programme of Research in South Africa. “I think there’s a chance we still will.”
A repeat of last winter seems pretty unlikely, experts told me. But with a virus this unpredictable, there’s no guarantee that we won’t see disaster unspool again.
A lot has changed since last year. For one thing, population immunity to SARS-CoV-2 is higher. Far more people have received additional doses of vaccine, many of them quite recently, with an updated formula that’s better tailored to the variants du jour. Plus, at this point, nearly every American has been infected at least once—and most of them with at least some subvariant of Omicron, says Shaun Truelove, an epidemiologist and a modeler at Johns Hopkins University. These multiple layers of protection make it more challenging for the average SARS-CoV-2 spin-off to severely sicken people. They also raise transmission obstacles for the coronavirus in whatever form it takes.
Omicron does seem to have ushered in “a different phase of the pandemic,” says Verity Hill, an evolutionary virologist at Yale. The variants that took over different parts of the world in 2021 rose in a rapid succession of monarchies: Alpha, Beta, Gamma, Delta. But in the U.S. and elsewhere, 2022 has so far been an oligarchy of Omicron offshoots. Perhaps the members of the Omicron lineage are already so good at moving among hosts that the virus hasn’t needed a major upgrade since.
If that’s the case, SARS-CoV-2 may end up a victim of its own success. The Omicron subvariants BQ.1 and BQ1.1 appear capable of spreading up to twice as fast as BA.5, according to laboratory data. But their takeover in the U.S. has been slow and halting, perhaps because they’re slogging through a morass of immunity to the Omicron family. That alone makes it less likely that any single Omicron subvariant will re-create the sudden surge of late 2021 anytime soon. In South Africa and the United Kingdom, for instance, different iterations of Omicron seem to have triggered just modest bumps in sickness in recent months. (That said, those countries—with their distinct demographics and vaccination and infection histories—aren’t a perfect bellwether for the U.S.)
For an Omicron 2021 redux to happen, SARS-CoV-2 might need to undergo a substantial genetic makeover—which Abdool Karim thinks would be very difficult for the virus to manage. In theory, there are only so many ways that SARS-CoV-2 can scramble its appearance while retaining its ability to latch onto our cells; by now, its options should be somewhat slimmed. And the longer the Omicron line of succession persists, the tougher it may be to upend. “It’s just getting harder to compete,” Hill told me.
But the world has gotten overconfident before. Even if SARS-CoV-2 doesn’t produce a brand-new version of itself, low uptake of the bivalent vaccine could allow our defenses to wither, driving a surge all the same, Truelove told me. Our transmission-dampening behaviors too are slacker than they’ve been since the pandemic’s start. This time last year, 50 to 60 percent of Americans were regularly wearing masks. The latest figures, many of them several months old, are closer to 30 percent. “The more opportunities you give the virus to get into somebody,” Hill said, “the more chances you give it to get the group of mutations that could help it take off.” Immunocompromised people who remain chronically infected with older variants, such as Alpha or Delta, could also become the sites of new viral offshoots. (That may be how the world got Omicron to begin with.)
Going on probability alone, “it seems more likely that we’ll keep going with these subvariants of Omicron rather than dealing with something wholly brand-new,” says Maia Majumder, an epidemiologist at Boston Children’s Hospital. But Lauren Ancel Meyers, an infectious-disease modeler at the University of Texas at Austin, warns that plenty of uncertainty remains. “What we don’t have is a really data-driven model right now that tells us if, when, where, and what kind of variants will be emerging in the coming months and years,” she told me. Our window into the future is only getting foggier too as fewer people submit their test results—or take any test at all—and surveillance systems continue to go offline.
It wouldn’t take another Omicron-type event to hurl us into disarray. Maybe none of the Omicron subvariants currently jockeying for control will surge ahead of the pack. But several of them might yet drive regional epidemics, Majumder told me, depending on the local nitty-gritty of who’s susceptible to what. And as winter looms, some of the biggest holes in our COVID shield remain unpatched. People who are immunocompromised are losing their last monoclonal-antibody treatments, and although powerful drugs exist to slash the risk of severe disease and death, useful preventives and treatments for long COVID remain sparse.
Our nation’s capacity to handle new COVID cases is also low, Majumder said. Already, hospitals around the country are being inundated with other respiratory viruses—RSV, flu, rhinovirus, enterovirus—all while COVID is still kicking in the background. “If flu has taken over hospital beds,” says Srini Venkatramanan, an infectious-disease modeler at the University of Virginia, even a low-key wave will “feel like it’s having a much bigger impact.”
As the country approaches its second holiday season with Omicron on deck, this version of the virus may “feel familiar,” Majumder pointed out. “I think people perceive the current circumstances to be safer than they were last year,” she said—and certainly, some of them are. But the fact that Omicron has lingered is not entirely a comfort. It is also, in its way, a reminder of how bad things once were, and how bad they could still get.
[ad_2]
Katherine J. Wu
Source link

[ad_1]
[ad_2]


