After AARP published interviews with Vice President Kamala Harris and former President Donald Trump, a PolitiFact reader noticed that the organization did not fact-check the candidates’ responses.
The presidential candidates spoke by phone with Robert Love, vice president and editor-in-chief of AARP Publications, in late August. On Oct. 2, AARP published the Q&A’s, in which each candidate was asked the same questions, focused on inflation, Social Security, Medicare and drug prices.
To serve our readers, we fact-checked some of the candidates’ claims:
Economy
Harris: “In terms of the price of groceries, one of the issues that we’ve seen is the price-gouging issue, where bad actors actually hike up the cost of everyday essentials, including groceries.”
This lacks context, experts have told PolitiFact. Price gouging sometimes happens, but inflation has largely stemmed from other factors.
Some examples of price-gouging include a 2023 antitrust lawsuit in which the Justice Department accused Agri Stats Inc. a data analytics and consulting company, of harming grocery stores and consumers by illegally “collecting, integrating and distributing competitively sensitive information related to price, cost and output among competing meat processors.” Agri Stats also occasionally, “encouraged meat processors to raise prices and reduce supply,” the Justice Department said. The lawsuit is pending.
In another example, the Washington state attorney general won price-fixing lawsuits against tuna companies and broiler chicken producers.
A 2023 paper from the Federal Reserve Bank of Kansas City (Missouri) found that growth of price markups — how much a product’s sale price exceeds its cost to the company — contributed more than 50% to inflation in 2021. However, researchers concluded that the markups could be explained as ones companies took “in anticipation of future cost pressures” rather than purely to extract profits.
More broadly, economists told PolitiFact that rising production costs — including rising wages and raw materials and real estate prices — are high consumer prices’ primary causes, not price gouging.
A 2024 Federal Reserve Bank of San Francisco study found that corporations’ price markups were not the recent inflation surge’s main driver.
Joseph Balagtas, an agricultural economics professor at Purdue University, said the COVID-19 pandemic caused supply-chain disruptions in 2020 that sparked high inflation through the summer of 2022, when year-to-year inflation hit a 40-year high of 9%. These snags increased production costs, the pandemic altered consumer behavior and fiscal and monetary policy increased consumer demand. These forces combined to drive prices higher, Balagtas said.
Trump: I signed the “largest tax cut in the history of our country.”
False.
In inflation-adjusted dollars, the tax bill Trump signed was the fourth-largest since 1940, and as a percentage of gross domestic product — the total monetary value of the goods and services produced a nation produces — it ranked seventh.
Our colleagues at the Washington Post Fact Checker found that this was Trump’s second-most-commonly repeated false claim, shared 295 times as president.
Trump: During the Trump administration, Americans “had low interest rates and no inflation” while under Biden, “they have high interest rates and the worst inflation we’ve ever had.”
Interest rates under Biden have been higher than under Trump, but Trump is wrong to call Biden-era inflation a historic worst.
During Trump’s prepandemic period, the year-over-year inflation rate ranged from 1.5% to 3%. After hitting a peak in mid-2022 of 9% under Biden, it is now 2.6%, which is lower than it was at some points under Trump, but far from all.
At its highest under Biden, inflation was not at a record high. The highest sustained, year-over-year U.S. inflation rates were recorded in the 1970s and early 1980s, when the price increase sometimes ranged from 12% to 15%. For one year — 1946, after the U.S. won World War II — the overall year-over-year inflation rate exceeded 18%.
Even before the pandemic sent interest rates plummeting, mortgage interest rates under Trump ranged from 3.5% to 5%. Under Biden, they approached 7.6% due to Federal Reserve interest rate hikes designed to restrain inflation. They have since fallen back to just more than 6%, but that was still higher than at any point during Trump’s presidency.
Health and human services
Harris: “For our seniors, (Social Security) is their only source of income.”
This is exaggerated.
The most recent data we found comes from a 2020 report by the National Institute on Retirement Security, a Washington, D.C.-based think tank.
The report found that about 40% of Americans 60 and older had only Social Security income, not income from defined benefit plans (such as company pensions) or defined contribution plans (such as 401(k) accounts). However, some of this 40% may have had income from working part time.
Harris: Donald Trump “tried 60 times” to end the Affordable Care Act “when in office.”
Trump did try to kill the act, which passed in 2010 during the Obama administration. But Harris exaggerated how often he tried this.
As president, Trump cut millions of dollars in federal funding for Affordable Care Act outreach and navigators who help people sign up for health coverage. He enabled the sale of short-term health plans that don’t comply with the act’s consumer protections and allowed them to be sold for longer durations, which siphoned people away from the health law’s marketplaces.
Trump’s administration also backed state Medicaid waivers that imposed the first-ever work requirements, which reduced enrollment. He also ended insurance company subsidies that helped offset costs for low-income enrollees, backed an unsuccessful repeal of the law and supported ending a penalty for failing to purchase health insurance.
During Trump’s presidency, Affordable Care Act enrollment declined by more than 2 million people and the number of uninsured Americans rose by 2.3 million, including 726,000 children.
However, getting to 60 specific actions under Trump requires counting dozens of attempts from 2010 to 2017. This period includes time before Trump was elected, and, in some cases, before he was active in politics.
Trump: “Massive Medicare premium increases (resulted) from the Biden-Harris Inflation Reduction Act.”
A few months ago, health policy analysts said this was a legitimate concern. However, Biden administration actions seem to have avoided creating “massive” increases for beneficiaries, at least for now.
One provision of the Inflation Reduction Act, which Biden signed in 2022, was a $2,000 cap on out-of-pocket spending Medicare Part D, the portion the health insurance program that pays for prescription drugs. The enactment was a boost for beneficiaries but troubling for insurers, who would be left to pay a greater share of costs.
For a while, it looked as if this would drive insurers to increase premiums sharply to recover some of those costs.
But the Biden administration invoked its authority to create a “demonstration” program that provided additional money to insurers who limited their premium increases to $35 a month, easing the premium hit.
An October analysis by KFF. a health research organization, found that the federal efforts largely “moderated” insurers’ 2025 premium increases.
Some congressional Republicans have criticized the administration’s election-eve move. Republicans used the same authority before the 2006 midterm elections, and in 2007, to cushion the blow after then-President George W. Bush’s administration introduced the Medicare prescription drug benefit.
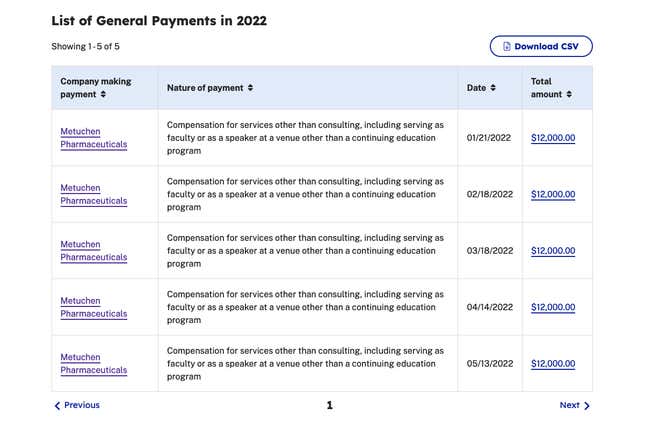
Trump: The Trump administration instituted “rules giving seniors $35 … insulin.”
This lacks context.
Trump’s administration enacted a program to lower insulin costs for some Medicare patients, but it was limited.
In 2020, the Trump administration “established a voluntary, time-limited model under the Center for Medicare and Medicaid Innovation known as the Part D Senior Savings Model,” according to KFF. “Under this model, participating Medicare Part D prescription drug plans covered at least one of each dosage form and type of insulin product at no more than $35 per month. The model was in effect from 2021 through 2023, and less than half of all Part D plans chose to participate in each year.”
In 2022, the program included a total of 2,159 Medicare drug plans, and the Centers for Medicare and Medicaid Services estimated that more than 800,000 Medicare beneficiaries who use insulin could have benefited from it that year. The Department of Health and Human Services has estimated that more than 1.5 million Medicare beneficiaries paid more than $35 a month for insulin in 2020, before Trump’s program took effect.
The Inflation Reduction Act, which Congress passed and Biden signed into law in August 2022, included an insulin provision that went further than Trump’s voluntary initiative.
The act capped out-of-pocket costs of insulin for Medicare patients at $35 per month. But, whereas the Trump program applied only to certain Medicare Part D plans, the Biden-era act mandated that all Medicare drug programs cap out-of-pocket insulin costs — including those in what’s known as Medicare Part B, which pays for medical equipment such as insulin pumps.
The act also mandated that the out-of-pocket price cap apply to all insulin products a given Medicare plan covers, not just a subset.
Trump also signed an executive order that would have reduced insulin prices, but only for low-income patients at Federally Qualified Health Centers, which serve 10% of Americans. Biden paused and then rescinded the order, so it never took effect.
Energy
Trump: “Energy prices (are) what really led to the problem of inflation.”
This is partially accurate.
Economists say Russia’s 2022 invasion of Ukraine worsened inflation by spiking oil prices and interfering with global trade. The invasion happened just a few months before inflation in the U.S. peaked around 9% under Biden in the summer of 2022.
But economists also widely agree that supply chain shortages starting a year or more earlier, during the COVID-19 pandemic, ignited the inflation increase, and that Biden’s pandemic relief bill, the American Rescue Plan Act, exacerbated it by putting too much money in Americans’ pockets at a time when supplies were low.
Inflation has fallen from its 2022 level by about two-thirds to 2.6% year over year, which is close to what the Federal Reserve wants to see before it cuts interest rates.
Oil prices and inflation have both fallen since their mid-2022 peaks.
Trump: During the Trump administration, “we were energy independent.”
This lacks context.
Some Trump policies led to the U.S. meeting some definitions of “energy independence,” but not others. Trump also ignores that Biden, too, has met some benchmarks of energy independence.
One definition met under both Trump and Biden is the U.S. exporting more energy than it imports.
The Energy Information Administration, a federal office that tracks energy statistics, found that in 2019 — when Trump was president — the United States became a net exporter of overall energy for the first time since 1952.
That has continued ever since, with the gap widening to a record level in 2023, the most recent full year with available statistics.
Another, narrower, measure of energy independence is whether the U.S. is a net exporter of petroleum specifically. In 2020, the last year of Trump’s term, the U.S. became a net exporter of petroleum for the first time since at least 1949. That has continued through 2022, the last year with available data.
A third form of energy independence occurs when domestic energy production exceeds domestic consumption. This has been so from 2019 to 2023, under both presidents.
There is one important metric keeping the U.S. from complete energy independence: The data for crude oil — which is used to manufacture gasoline, a key consumer commodity — has not followed the same pattern as energy overall. Crude oil imports outpaced exports in each of the four years Trump was president, and during Biden’s first three years in office.
Although the U.S. theoretically produces enough crude oil to satisfy its consumption, the U.S. cannot refine all of the crude oil it produces because its refineries are built to process heavy, sour crude from the Middle East and other overseas suppliers, not domestically produced light, sweet crude. (Crude is graded by its weight and “sweetness,” a measure of sulfur content.)
This means the U.S. is exporting a lot of its domestically produced crude on the international market. To make up for this, the U.S. still must import a substantial amount of oil for domestic use. That leaves the U.S. at the mercy of international events to keep its supply coming in.
Trump: “We have more oil and gas than any other country in the world by far.”
This is False.
On oil, Venezuela ranked first in 2021 with 304 billion barrels of proven crude oil reserves, followed by Saudi Arabia, Iran, Canada, Iraq, the United Arab Emirates, Kuwait and Russia, the U.S. Energy Information Administration reported. The U.S. ranked ninth internationally, with 61 billion barrels.
On natural gas, the U.S, ranks No. 4.
The U.S. ranks No. 1 internationally in coal reserves.