The American Medical Association passed a resolution encouraging hospitals to offer healthy plant-based food options.
“Globally, 11 million deaths annually are attributable to dietary factors, placing poor diet ahead of any other risk factor for death in the world.” Given that diet is our leading killer, you’d think that nutrition education would be emphasized during medical school and training, but there is a deficiency. A systematic review found that, “despite the centrality of nutrition to a healthy lifestyle, graduating medical students are not supported through their education to provide high-quality, effective nutrition care to patients…”
It could start in undergrad. What’s more important? Learning about humanity’s leading killer or organic chemistry?
In medical school, students may average only 19 hours of nutrition out of thousands of hours of instruction, and they aren’t even being taught what’s most useful. How many cases of scurvy and beriberi, diseases of dietary deficiency, will they encounter in clinical practice? In contrast, how many of their future patients will be suffering from dietary excesses—obesity, diabetes, hypertension, and heart disease? Those are probably a little more common than scurvy or beriberi. “Nevertheless, fully 95% of cardiologists [surveyed] believe that their role includes personally providing patients with at least basic nutrition information,” yet not even one in ten feels they have an “expert” grasp on the subject.
If you look at the clinical guidelines for what we should do for our patients with regard to our number one killer, atherosclerotic cardiovascular disease, all treatment begins with a healthy lifestyle, as shown below and at 1:50 in my video Hospitals with 100-Percent Plant-Based Menus.
“Yet, how can clinicians put these guidelines into practice without adequate training in nutrition?”
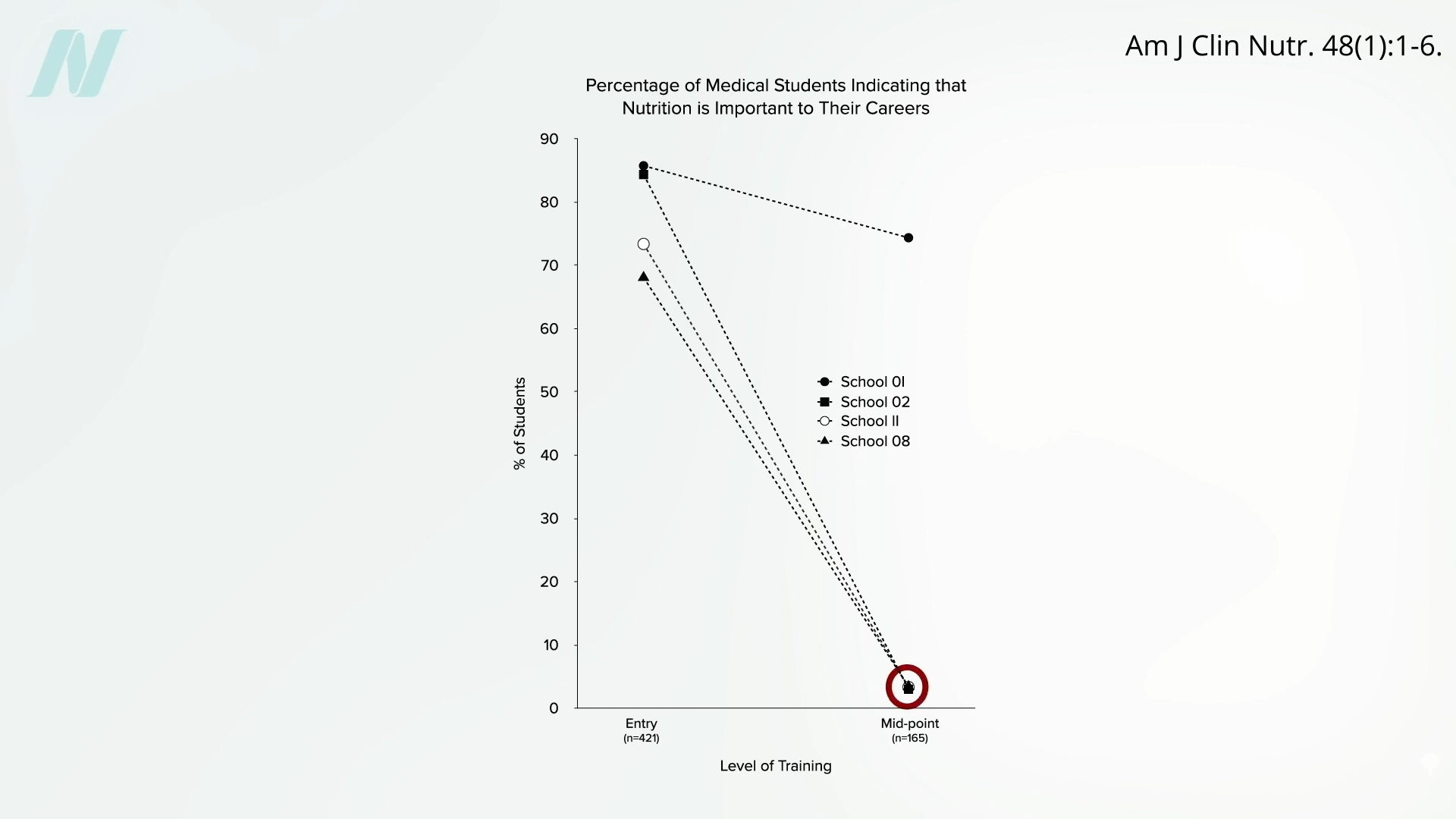
Less than half of medical schools report teaching any nutrition in clinical practice. In fact, they may be effectively teaching anti-nutrition, as “students typically begin medical school with a greater appreciation for the role of nutrition in health than when they leave.” Below and at 2:36 in my video is a figure entitled “Percentage of Medical Students Indicating that Nutrition is Important to Their Careers.” Upon entry to different medical schools, about three-quarters on average felt that nutrition is important to their careers. Smart bunch. Then, after two years of instruction, they were asked the same question, and the numbers plummeted. In fact, at most schools, it fell to 0%. Instead of being educated, they got de-educated. They had the notion that nutrition is important washed right out of their brains. “Thus, preclinical teaching”— the first two years of medical school—“engenders a loss of a sense of the relevance of the applied discipline of nutrition.”
Following medical school, during residency, nutrition education is “minimal or, more typically, absent.” “Major updates” were released in 2018 for residency and fellowship training requirements, and there were zero requirements for nutrition. “So you could have an internal medicine graduate who comes out of a terrific program and has learned nothing—literally nothing—about nutrition.”
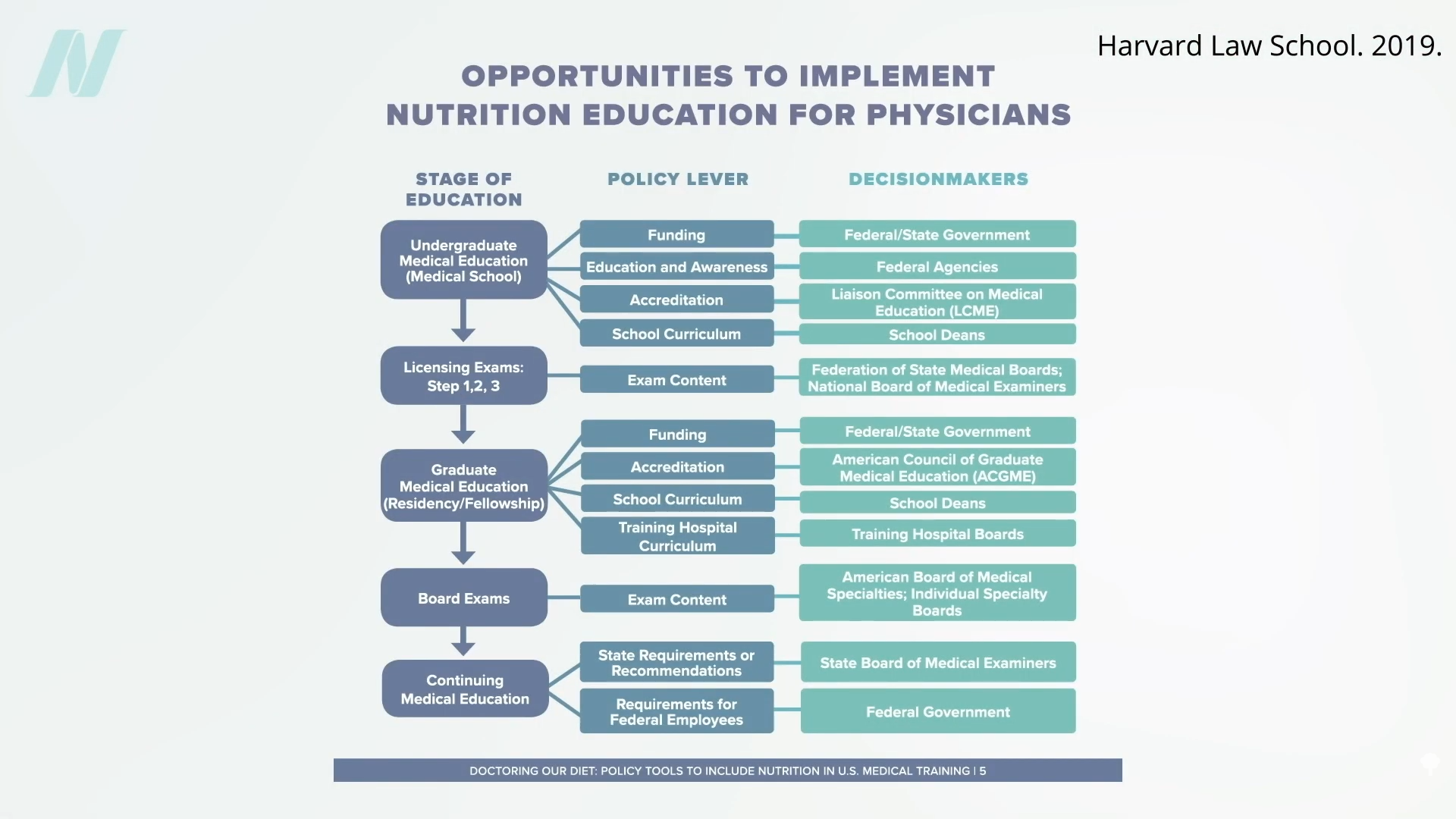
“Why is diet not routinely addressed in both medical education and practice already, and what should be done about that?” One of the “reasons for the medical silence in nutrition” is that, “sadly…nutrition takes a back seat…because there are few financial incentives to support it.” What can we do about that? The Food Law and Policy Clinic at Harvard Law School identified a dozen different policy levers at all stages of medical education and the kinds of policy recommendations there could be for the decision-makers, as you can see here and at 3:48 in my video.
For instance, the government could require doctors working for Veterans Affairs (VA) to get at least some courses in nutrition, or we could put questions about nutrition on the board exams so schools would be pressured to teach it. As we are now, even patients who have just had a heart attack aren’t changing their diet. Doctors may not be telling them to do so, and hospitals may be actively undermining their future with the food they serve.
The good news is that the American Medical Association (AMA) has passed a resolution encouraging hospitals to offer healthy food options. What a concept! “Our AMA hereby calls on [U.S.] Health Care Facilities to improve the health of patients, staff, and visitors by: (a) providing a variety of healthy food, including plant-based meals, and meals that are low in saturated and trans fat, sodium, and added sugars; (b) eliminating processed meats from menus; and (c) providing and promoting healthy beverages.” Nice!
“Similarly, in 2018, the State of California mandated the availability of plant-based meals for hospital patients,” and there are hospitals in Gainesville (FL), the Bronx, Manhattan, Denver, and Tampa (FL) that “all provide 100% plant-based meals to their patients on a separate menu and provide educational materials to inpatients to improve education on the role of diet, especially plant-based diets, in chronic illness.”
Let’s check out some of their menu offerings: How about some lentil Bolognese? Or a cauliflower scramble with baked hash browns for breakfast, mushroom ragu for lunch, and, for supper, white bean stew, salad, and fruit for dessert. (This is the first time a hospital menu has ever made me hungry!)
The key to these transformations was “having a physician advocate and increasing education of staff and patients on the benefits of eating more plant-based foods.” A single clinician can spark change in a whole system, because science is on their side. “Doctors have a unique position in society” to influence policy at all levels; it’s about time we used it.
For more on the ingrained ignorance of basic clinical nutrition in medicine, see the related posts below.
After being diagnosed with breast cancer in 2021, advocate Daphne Meyers decided to elevate her mission of creating safe spaces and encouraging early detection by launching EmpowHer and Him. The organization aims to empower those who have been diagnosed and increase the visibility of men in the breast cancer conversation.
The Atlanta Voice talked with Meyers about the organization’s annual brunch, the importance of early detection, and what it means to be on the frontline of this fight.
Photo by Laura Nwogu/The Atlanta Voice
The Atlanta Voice: EmpowHER and HIM recently held its annual breast cancer awareness brunch. What’s been the most important part of getting to see how much this organization and the people who support it have grown?
Daphne Myers: “When we started, it was called the Tatas and Tutus. I was an advocate for breast cancer, but had never really thought much about the men. It wasn’t until the second year that I was like, ‘Well, men can get breast cancer, so why am I not getting men to come to this event?’ The first year, none. In the second year, we probably had four, and one of them was my son. So I said, ‘Okay, I’m getting interest. Men are buying the tickets, but they’re sending their wives or sisters or daughters; they’re not coming.’
“I changed the name in the third year to Tatas, Tutus, and Ties. The most rewarding aspect of that is seeing how it has grown from year one to year five. We probably had at least 60 men this year, and that’s grown from having none, to a year of four, and then maybe double that the following year. And so now it seems as if we have just as many men in there.”
AV: “I love that. Let’s go back a little. EmpowHer and Him is about uplifting every fighter, men and women, going through this battle. Can you talk about how the organization began?
DM: “I was diagnosed with breast cancer in 2021. Based on my diagnosis, I thought, ‘I’ve always been an advocate, so where do I go from here to raise more awareness among men and women?’ Being diagnosed with breast cancer, you’re all over the place. First, you have to accept it, and then second, you have to figure out how to navigate. You’ve got to decide whether to do treatment or not, and how it’s going to affect your livelihood. So the questions that were in my mind as someone with breast cancer at that particular time prompted me to say, ‘You know what? If I had those questions, there are millions of other people who have those same questions. And if I have the answer to it, then I need to open up my mouth and be able to give the gift of awareness.
“This is bigger than me. It’s bigger than the Tatas, Tutus, and Ties. It’s about bringing about awareness, not just for women, but also for men. In the past year, I found myself doing a lot of speaking engagements, and a lot of men, just like women, don’t know about breast cancer. That’s where EmpowHER and HIM came about. I had to use this mouthpiece to bring about awareness so that people know that early detection is key. If I tell one person, then that person tells someone else; it becomes a domino effect. Your work is not done, but it keeps going.”
AV: I think that’s so admirable that your fight became perspective, and it became this thing about you wanting to lend a helping hand and be a support system for other people who may be going through their own breast cancer journey or fight.
When it comes to the aspect of men being diagnosed with breast cancer, why do you think there’s not a lot of visibility in their fight?
DM: “There’s no talk about it. Even from the medical profession, there’s not a lot of talk about it. I did an interview, probably about two or three weeks ago, and I was talking to this man about breast cancer, and he said, ‘Yeah, you don’t think about men with breast cancer.’ I said, ‘But you have a chest.’ He says, ‘OK, well, let’s maybe say breast and chest cancer.’
“People don’t understand that they have breast tissue; this is our breastplate. It’s not just prostate [cancer], and it’s not just colon. We have to come together and understand that yeah, it may be a small percentage, but it is there. When you see the Susan G. Komen’s or the American Cancer Society, you see women, and the men are in the background. With EmpowHer and Him, we’re both standing there side by side. So that’s why the ribbon is half pink and half blue. It’s about making it more relatable to them. Men don’t know that they can get a mammogram. When you go to fill out your paperwork, it says, when was your last period? How many pregnancies? You’re putting on this pink robe to get your mammogram, all of that. Our medical society doesn’t even pay attention to it as much as we should.”
AV: What do you think there needs to be more awareness about when it comes to breast cancer?
DM: “Early detection. That’s the key to anything. I know it sounds cliché-ish, but we have to start with checking our breasts and our chest at an early age, and especially if you have a history of it in your family. Because I was diagnosed with breast cancer, it kind of moves the scale up for my children to be checked.
“People of color, our breast tissue is more dense, so it goes undetected. On a regular mammogram mine was missed the first time. It wasn’t until I got the 3D that detected my breast cancer. Had I gone on and thought it was clear, I may not have been sitting here talking to you today.”
AV: For those that are looking for resources or someone to talk to, what can EmpowHer and Him be for that person?
DM: “I’m frontline, and what better person to be frontline than the person who’s actually going through it? I get calls every week of a new diagnosis, and I have to put a lot of hats on. I have to speak, because the one thing people want to know is, ‘What’s your suggestion?’ Do what’s gonna be best for you. Don’t just run with the first thing and then say, this is what I’m gonna do without checking deeper into it. The other thing is for resources. When you’re going through treatment, you’re not gonna feel good. I had to go through 18 rounds. You’re tired, you’re sad, you go into depression. So you have to battle with all of those things. There are several support groups that are out there, including with us.
“I found myself telling people to just start journaling. Do what makes you feel good to get you through that. Ask for help. It’s not a death sentence. Just because we’re diagnosed with breast cancer doesn’t mean that that’s our end. It’s actually a beginning. And it was a beginning for me, because I was on one side of the Richter scale as an advocate, to now I’m a surviving advocate, and my goal is to put this out there as much as possible and really help bring about this awareness with me.”
AV: What does it mean for you to be on the front line and to see what the organization has grown into?
DM: “I’m proud of myself. And a lot of times people say, ‘Oh, you shouldn’t brag.’ No, I am. I’m proud of myself, I’m proud of my friends, I’m proud of my family, because while I was a survivor of the disease, they were survivors of me, because they were there with me. I’m proud when that person comes to me and says, ‘Man, that event that you had opened up some doors. I’m gonna get tested.’ ‘I didn’t know that, because I’m a male…’ or ‘I didn’t know that just by changing your diet to this, that and the third could help…’ ‘I didn’t know how to do an exam.’
“My first scare, believe it or not, was when I was eight years old, so by the time I was diagnosed, that was my fifth surgery. So it’s here. Unfortunately they say that there’s no cure, but there are some things that we can change. We just have to take care of ourselves, love one another, keep down the stress, and survive this game.”
Please note: This blog contains descriptions of sexual assault.
“Recent reports of medical students performing pelvic exams for training purposes on anesthetized women without their consent”—or their knowledge—“have produced a firestorm of controversy and calls for greater regulation.” However, that “burst of public outcry” was in the mid-1990s. California was the first state to make the practice illegal, but the “early gains quickly petered out.”
As I discuss in my videoEnding the Hidden Practice of Pelvic Exams on Unconscious Women Without Their Consent, “This practice, common since the late 1800s, was largely unchallenged until a 2003 study reported that 90 percent of medical students who completed obstetrics and gynecology (ob-gyn) rotations at four Philadelphia-area medical schools performed pelvic exams on anesthetized women for educational purposes.” (A subsequent study found the percentage to be lower than that in other areas of the country.) The bottom line? “Pelvic Exams Done on Anesthetized Women Without Consent: Still Happening.” How can this continue into 2025? Medical ethicists have called such practices “immoral and indefensible.” “At the end of the day, this is a practice that should come to an abrupt and immediate halt.” Some schools vowed they’d end the practice, but, unfortunately, these early victories quickly stalled. At the same time, a handful of schools revamped their policies, an equal number of hospitals and medical schools publicly dug in, defending the practice.
The Association of Professors of Gynecology and Obstetrics wrote: “As medical educators, we must balance our obligation to develop the next generation of physicians with women’s freedom to decide from whom they receive treatment and what aspects of their care are performed by learners.” “Some especially blunt teaching faculty contend that ‘public’ patients”—those without health insurance—“owe it to the facility and society to participate since they receive free or subsidized care.” Regulations to curb this practice are said to be “placing inappropriate and unnecessary barriers in the way of medical students who need to learn fundamental medical skills” and therefore “should be resisted.” Unsurprisingly, medical students still perform pelvic exams on anesthetized women.
Professional medical societies have given lip service to the concept of asking for explicit consent, but despite the recommendations, “evidence…suggests that the practice is alive and well.” And the “unauthorized use of women is not a localized phenomenon confined to a handful of errant medical schools,” a few bad med school apples, but an international problem.
Even with the emergence of the #MeToo movement and even after Larry Nasser, the infamous USA gymnastics doctor, was sentenced to 40 to 175 years in prison for touching women’s genitalia without their consent, “there are still women who are being used as teaching subjects for these exams without their permission, without their consent.”
A 2020 update from Yale’s Center for Bioethics was entitled: “A Pot Ignored Boils On: Sustained Calls for Explicit Consent of Intimate Medical Exams.” It reads, “Over the last 30 years, several parties—both within and external to medicine—have increasingly voiced opposition to these exams. Arguments from medical associations, legal scholars, ethicists, nurses, and some physicians have not compelled meaningful institutional change.” Yes, there is the lip service paid by medical associations recommending bans on pelvic exams without consent, but those statements are “advisory and incomplete. Associations simply do not have the capacity to compel systemic change, as evidenced by institutions’ inaction.” In response to the medical profession’s inability to police itself, many states have passed legislation to protect patients from this practice.
But, of course, if you are anesthetized, how would you even know if medical students are lining up or not? “Teaching hospitals take patients who are in the worst position to know what’s occurring—they are unconscious—and use them in ways that leave no physical signs and are often undocumented in the patients’ medical records.” So, when the media loses interest, as it has decade after decade, “what incentive is there for teaching faculty or hospitals to voluntarily change?” Perhaps, “when physicians start being threatened with litigation, they’ll start obtaining informed consent.” As one commentator wrote, “Hospital administrators who allow medical students in their facilities to perform pelvic examinations on unconsenting anesthetized women ought to consult with their legal counsel concerning the definition of rape in their jurisdiction.”
“The solution is simple: Just ask.” Ask women for permission. It’s their body, their choice. “But recent experience has shown that meaningful and complete hospital-by-hospital change is unlikely to come until a hospital or doctor pays a substantial award [in some lawsuit] for this error in ethical judgment. We believe that day is coming soon, lest that ignored pot finally boil over.
“Some defend it as harmless and say asking for consent would make it more likely that patients would say no, denying students a crucial part of their training.” When I first wrote about this practice more than 20 years ago in my book Heart Failure about my time in medical school, I talked about how I had gotten the same comments from my classmates: “A well-then-how-are-we-going-to-learn response. To even present such a question is to lose a bit of one’s humanity. The answer, of course, is we should learn from women who give their consent! And to do that—God forbid—we might actually have to first establish a relationship with the patient, a trust—talk to them even. We may have to treat them like human beings.”
It’s unconscionable that medical students are legally allowed to practice pelvic exams on anesthetized women without their consent. Even if you live in one of the states where this practice is technically illegal, how do you know the law will be respected once you’re unconscious? Maybe medical students should wear bodycams.
There used to be a lot of jokes about the terrible nature of doctors’ handwriting, until much of the process of seeing a physician was digitized, improving things no end for both doctors and patients. But consulting a medical expert still involves a whole lot of note-taking, and that’s an increasing burden for many healthcare workers, from physicians to clerical staff. A new report says things are changing yet again, however, and a new generation of digital tools is improving the way health care workers make notes. The new innovations are powered by AI, and even if your business has nothing to do with practicing medicine, there are lessons here for your company.
The study, led by a research group from the Yale School of Medicine, cited previous reports that showed over half of a clinician’s typical workday gets consumed dealing with electronic health records, leaving just a quarter of the day for direct time with patients. Documentation time has been trending upwards too, which has been linked to burnout, depleted efforts at work and more staff thinking of quitting, industry news site MedicalXPress reports.
But when medical professionals used what’s described as an ambient AI scribe platform — a system that unobtrusively takes part in a patient consultation, capturing the audio of the conversation and then transcribing it via specialized AI models into notes for the clinician to review later — things were very different.
Between the nearly 200 participants in the investigation, most of them attending physicians, the proportion of doctors reporting feelings that qualified as burnout fell from nearly 52 percent at the start to just under 39 percent after 30 days.
An Inc.com Featured Presentation
That’s a dramatic downward shift. The study measured how the AI tool, which the researchers pointedly did not identify, was helping, and showed it was lowering the cognitive burden of the physicians, easing up the amount of time eaten up by working on documentation, decreasing the effort the professionals felt they had to deliver at work, and lowering their mental demands. The time needed per week in “after hours” moments to complete documentation also fell by nearly one hour, reducing pressure still further. Overall the report suggests this leads to doctors having more energy to give the proper attention to patients’ concerns, and frees them up for more urgent care access.
This is, of course, just one single use case for AI tools. And it’s easy to see how having a reliable automatic note-taking system could dramatically change the working day of a typical frontline health care worker. Freeing up time needed to write things down would easily translate into more face-time with patients, and as long as the overall pressure on a typical physician to achieve a certain workload doesn’t go up because of this extra time, then the risk of burnout would be reduced.
How does this impact your company, though?
It’s a giant thumbs-up for the benefits of AI technology. In this case, as the Yale report says, it’s specialized tools “that can produce professional appearing text,” which are “taught to listen, instantaneously transcribe, assimilate, and assemble a document, with fine-tuning by human training.”
The study shows that in the right setting, using exactly the right tools, AI can achieve some of the big promises that AI evangelists make. Instead of threatening to take over people’s jobs, AI proponents argue that it can take on mundane tasks on behalf of a worker, thus freeing up staff to do more frontline, more productive tasks. The Yale report, for example, says AI scribes allowed doctors “more time for meaningful work and professional well-being.”
This means that for your office, tools other than an AI scribe may prove useful and could genuinely reduce workloads and burnout risks for your staff. Choosing AI tools in a careful, considered way is important, however, and upskilling and training staff on the correct use of the technology is likely a key for this process to work properly. Many reports say organizations are failing to do this when they roll out AI systems.
Please note: This blog contains descriptions of sexual assault.
From Heart Failure, a book I wrote about my time at Tufts University School of Medicine: “I am all gloved up, fifth in line. At Tufts, medical students—particularly male students—practice pelvic exams on anesthetized women without their consent and without their knowledge. Women come in for surgery and, once they’re asleep, we all gather around; line forms to the left…We learn more than examination skills. Taking advantage of the woman’s vulnerability—as she lay naked on a table unconscious—we learn that patients are tools to exploit for our education.”
Using female patients to teach pelvic exams without their consent or knowledge remains “a dirty little secret about medical schools.” It is an “age-old” practice that continues to this day in med schools around the world. It’s been referred to as “the ‘vending machine’ model of pelvic exams, in which medical students line up to take their turn…” “Only it’s not a vending machine; it’s a woman’s vagina.”
It’s been called “an outrageous assault upon the dignity and autonomy of the patient…The practice shows a lack of respect for these patients as persons, revealing a moral insensitivity and a misuse of power.” Indeed, “it is yet another example of the way in which physicians abuse their power and have shown themselves unwilling to police themselves in matters of ethics, especially with regard to female patients.” Said a residency-program director at the Johns Hopkins University School of Medicine, “I don’t think any of us even think about it. It’s just so standard as to how you train medical students.”
What happened when this practice came to light in New Zealand? The chair of the New Zealand Medical Association got on television and said: “‘Until recently it wasn’t an issue…I’m very sorry that women feel they’ve been assaulted and violated in this way. That was never our intention.’ He had no idea then, asked the [TV] presenter, that women might object? ‘All I can say is that there have been no objections…’ ‘Could the reason be,’ asked the interviewer logically, “that it’s very hard for an anesthetized woman to know what’s going on?’”
The practice has been defended publicly by many medical schools and hospitals, contending “this touching is entirely appropriate and clearly falls well within the patient’s ‘implied consent’ to carry out the operation.” After all, “patients are aware they are entering a teaching hospital and therefore know that trainees will be actively participating in their care.” However, “researchers have found that many patients do not know when they have interacted with medical students, or even whether they are in a teaching hospital.” How can this be? “Deliberate lies and deception.”
“A survey of medical students found that 100% of them had been introduced to patients as ‘doctor’ by members of the clinical team,” and, as they go through training, there is, as a journal article is titled, an “Erosion in Medical Students’ Attitudes About Telling Patients They Are Students.” “Additionally, as medical students complete their clinical years of training, their sense of responsibility to inform patients that they are students is found to decrease,” especially if there is an opportunity to perform an invasive procedure. That may be why medical students seem to develop a “don’t ask, don’t tell” policy when it comes to seeking consent for pelvic examinations on anesthetized patients. More than a third of 1,600 medical students surveyed across the country strongly disagreed with the statement “Hospitals should obtain explicit permission for student involvement in pelvic exams,” as seen below and at 4:03 of my video Medical Students Practice Pelvic Exams on Anesthetized Women Without Their Consent.
After all, doctors “argue that performing a pelvic examination is no more intimate than placing one’s hands inside an abdomen during general surgery or attempting to intubate a patient” and assert that sticking your fingers in a woman’s vagina is “just as intimate” as an ophthalmologist looking into the back of your eye; any claim to the contrary is just “another attempt to justify the obsession with political correctness.” Said one medical school professor, “Personally, I would prefer to see a new generation of well-trained doctors…rather than a nation of women whose vaginas are protected from battery by medical students.”
The national survey concluded: “Patients admitted to teaching hospitals do not, however, by the mere act of admission relinquish their rights as human beings to have ultimate control over their own body and to be involved in decisions concerning their health care.”
Is it possible that women just don’t care? Studies show that up to 100% of women asked said they would want to know that vaginal exams were being performed by medical students. Since patients care deeply about being asked, why can’t we at least ask their permission? “We can’t ask women,” the medical school faculty replied. “If we do, they might say no.”
What is the dirty little secret of drugs for lifestyle diseases?
Drug companies go out of their way—in direct-to-consumer ads, for example—to “present pharmaceutical drugs as a preferred solution to cholesterol management while downplaying lifestyle change.” You see this echoed in the medical literature, as in this editorial in the Journal of the American Medical Association: “Despite decades of exhortation for improvement, the high prevalence of poor lifestyle behaviors leading to elevated cardiovascular disease risk factors persists, with myocardial infarction [heart attack] and stroke remaining the leading causes of death in the United States. Clearly, many more adults could benefit from…statins for primary prevention.” Do we really need to put more people on drugs? A reply was published in the British Medical Journal: “Once again, doctors are implored to ‘get real’—stop hoping that efforts to help their patients and communities adopt healthy lifestyle habits will succeed, and start prescribing more statins. This is a self-fulfilling prophecy. Note that the author of these comments [the pro-statin editorial] disclosed receipt of funding from 11 drug companies, at least four of which produce or are developing new classes of cholesterol-lowering agents,” which make billions of dollars a year in annual sales.
Every time the cholesterol guidelines expand the number of people eligible for statins, they’re decried as a “big kiss to big pharma.” This is understandable, since the majority of guideline panel members “had industry ties,” financial conflicts of interest. But these days, all the major statins are off-patent, so there are inexpensive generic versions. For example, the safest, most effective statin is generic Lipitor, sold as atorvastatin for as little as a few dollars a month. So, nowadays, the cholesterol guidelines are not necessarily “part of an industry plot.”
“The US way of life is the problem, not the guidelines…” The reason so many people are candidates for cholesterol- and blood-pressure-lowering medications is that so many people are taking such terrible care of themselves. The bottom line is that “individuals must take more responsibility for their own health behaviors.” What if you are unwilling or unable to improve your diet and make lifestyle changes to bring down that risk? If your ten-year risk of having a heart attack is 7.5 percent or more and going to stay that way, then the benefits of taking a statin drug likely outweigh the risk. That’s really for you to decide, though. It’s your body, your choice.
“Whether or not the overall benefit-harm balance justifies the use of a medication for an individual patient cannot be determined by a guidelines committee, a health care system, or even the attending physician. Instead, it is the individual patient who has a fundamental right to decide whether or not taking a drug is worthwhile.” This was recognized by some of medicine’s “historical luminaries such as Hippocrates,” but “only in recent decades has the medical profession begun to shift from a paternalistic ‘doctor knows best’ stance towards one explicitly endorsing patient-centered, evidence-based, shared decision-making.” One of the problems with communicating statin evidence to support this shared decision-making is that most doctors “have a poor understanding of concepts of risk and probability and…increasing exposure to statistics in undergraduate and postgraduate education hasn’t made much difference.” But that understanding is critical for preventive medicine. When doctors offer a cholesterol-lowering drug, “they’re doing something quite different from treating a patient who has sought help because she is sick. They’re not so much doctors as life insurance salespeople, peddling deferred benefits in exchange for a small (but certainly not negligible) ongoing inconvenience and cost. In this new kind of medicine, not understanding risk is the equivalent of not knowing about the circulation of the blood or basic anatomy. So, let’s dive in and see exactly what’s at stake.
If you follow the asterisk I’ve circled after the “36%” in the ad, you can see how they came up with that. I’ve included it here and at 3:56 in my video. In a large clinical study, 3 percent of patients not taking the statin had a heart attack within a certain amount of time, compared to 2 percent of patients who did take the drug. So, the drug dropped heart attack risk from 3 percent to 2 percent; that’s about a one-third drop, hence the 36 percent reduced relative risk statistic. But another way to look at going from 3 percent to 2 percent is that the absolute risk only dropped by 1 percent. So, in effect, “your chance to avoid a nonfatal heart attack during the next 2 years is about 97% without treatment, but you can increase it to about 98% by taking a Crestor [a statin] every day.” Another way to say that is that you’d have to treat 100 people with the drug to prevent a single heart attack. That statistic may shock a lot of people.
If you ask patients what they’ve been led to believe, they don’t think the chance of avoiding a heart attack within a few years on statins is 1 in 100, but 1 in 2. “On average, it was believed that most patients (53.1%) using statins would avoid a heart attack after statin treatment for 5 years.” Most patients, not just 1 percent of patients. And this “disparity between actual and expected effect could be viewed as a dilemma. On the one hand, it is not ethically acceptable for caregivers to deliberately support and maintain illusive treatment expectations by patients.” We cannot mislead people into thinking a drug works better than it really does, but on the other hand, how else are we going to get people to take their pills?
When asked, people want an absolute risk reduction of at least about 30 percent to take a cholesterol-lowering drug every day, whereas the actual absolute risk reduction is only about 1 percent. So, the dirty little secret is that, if patients knew the truth about how little these drugs actually worked, almost no one would agree to take them. Doctors are either not educating their patients or actively misinforming them. Given that the majority of patients expect a much larger benefit from statins than they’d get, “there is a tension between the patient’s right to know about benefiting from a preventive drug and the likely reduction in uptake [willingness to take the drugs] if they are so informed,” and learn the truth. This sounds terribly paternalistic, but hundreds of thousands of lives may be at stake.
If patients were fully informed, people would die. About 20 million Americans are on statins. Even if the drugs saved 1 in 100, that could mean hundreds of thousands of lives lost if everyone stopped taking their statins. “It is ironic that informing patients about statins would increase the very outcomes they were designed to prevent.”
Do you know more about basic nutrition than most doctors?
“A poor diet now outranks smoking as the leading cause of death globally and in the United States, according to the latest data.” The top killer of Americans is the American diet, as you can see below and at 0:23 in my video How Much Do Doctors Actually Know About Nutrition?.
If diet is humanity’s number one killer, then, obviously, nutrition is the number one subject taught in medical school, right? Sadly, “medical students around the world [are] poorly trained in nutrition.” It isn’t that medical students aren’t interested in learning about it. In fact, “interest in nutrition was ‘uniformly high’ among medical students,” but medical schools just aren’t teaching it. “Without a solid foundation of clinical nutrition knowledge and skills, physicians worldwide are generally not equipped to even begin to have an informed nutrition conversation with their patients….”
How bad is it? One study, “Assessing the clinical nutrition knowledge of medical doctors,” found the majority of participants got 70 percent of the questions wrong—and they were multiple choice questions, so they should have gotten about a fifth of them right just by chance. “Wrong answers in the…knowledge test were not limited to difficult or demanding questions” either. For example, less than half of the doctors were able to guess how many calories are in fat, carbohydrates, and protein; only one in ten knew the recommended protein intake; and only about one in three knew what a healthy body mass index (BMI) was. We’re talking about really basic nutrition knowledge.
Even worse, not only did the majority of medical doctors get a failing grade, but 30 percent of those who failed had “a high self-perception of their CN [clinical nutrition] expertise.” They weren’t only clueless about nutrition; they were clueless that they were clueless about nutrition, a particularly bad combination given that doctors are “trusted and influential sources” of healthy eating advice. “For those consumers who get information from their personal healthcare professional, 78% indicate making a change in their eating habits as a result of those conversations.” So, if the doctor got everything they know from some article in a magazine while waiting in the grocery store checkout aisle, that’s what the patients will be following.
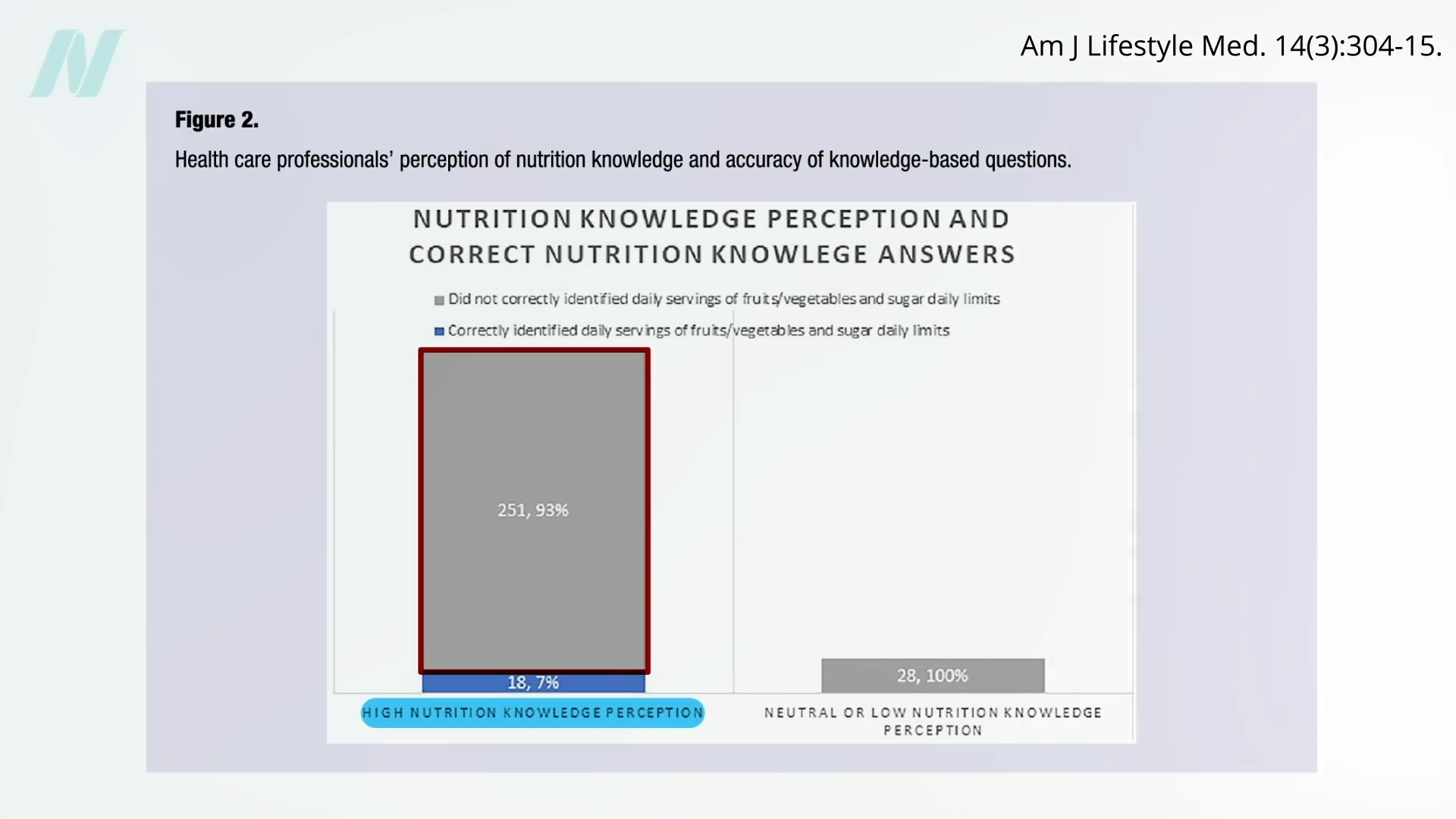
Of doctors surveyed, “only 25% correctly identified the American Heart Association recommended number of fruit and vegetable servings per day, and fewer still (20%) were aware of the recommended daily added sugar limit for adults.” So how are they going to counsel their patients? And get ready for this: Of the doctors who perceived themselves as having high nutrition knowledge, 93 percent couldn’t answer those two basic multiple-choice questions, as seen here and at 2:39 in my video.
“Physicians with no genuine expertise in, say, neurosurgery [brain surgery] are neither likely to broadcast detailed opinions on that topic nor to have their ‘expert’ opinions solicited by the media. Most topical domains in medicine enjoy such respect: we defer expert opinion and commentary to actual experts. Not so nutrition, where the common knowledge that physicians are generally ill-trained in this area is conjoined to routine invitations to physicians for their expert opinions on the matter. All too many are willing to provide theirs, absent any basis for actual expertise…” Or worse, they’re “often made on the basis of native bias and personal preference, at times directly tethered to personal gain—such as diet book sales—and so arises yet another ethical challenge.” That’s one of the reasons all the proceeds I receive from my books are donated directly to charity. I don’t want even the appearance of any conflicts of interest.
“In a culture that routinely fails to distinguish expertise from mere opinion or personal anecdote, we physicians should be doing all we can to establish relevant barriers to entry for expert opinion in this [diet and nutrition], as in all other matters of genuine medical significance.” I mean, we aren’t talking celebrity gossip. Lives are at stake. “Entire industries are devoted to marketing messages that may conspire directly against well-informed medical advice in this area.”
“Medical education must be brought up to date. For physicians to be ill-trained in the very area most impactful on the rate of premature death at the population level is an absurd anachronism….The mission of medicine is to protect, defend, and advance the human condition. That mission cannot be fulfilled if the diet is neglected.”
A possible starting place? “Physicians and health care organizations can collectively begin to emphasize their seriousness about nutrition in health care by practicing what they (theoretically) preach. Is it appropriate to serve pizza and soft drinks at a resident conference while bemoaning the high prevalence of obesity and encouraging patients to eat healthier? A similarly poor example exists in medical conferences, including national meetings, where some morning sessions are accompanied by foods such as donuts and sausage.”
Kira Stoops lives in Bozeman, Montana—a beautiful mountain town where it sometimes feels like everyone regularly goes on 50-mile runs. Stoops, however, can’t walk around her own block on most days. To stand for more than a few minutes, she needs a wheeled walker. She reacts so badly to most foods that her diet consists of just 12 ingredients. Her “brain fog” usually lifts for a mere two hours in the morning, during which she can sometimes work or, more rarely, see friends. Stoops has myalgic encephalomyelitis, or chronic fatigue syndrome (ME/CFS). “I’m considered a moderate patient on the mild side,” she told me.
ME/CFS involves a panoply of debilitating symptoms that affect many organ systems and that get worse with exertion. The Institute of Medicine estimates that it affects 836,000 to 2.5 million people in the U.S. alone, but is so misunderstood and stigmatized that about 90 percent of people who have it have never been diagnosed. At best, most medical professionals know nothing about ME/CFS; at worst, they tell patients that their symptoms are psychosomatic, anxiety-induced, or simply signs of laziness. While ME/CFS patients, their caregivers, and the few doctors who treat them have spent years fighting for medical legitimacy, the coronavirus pandemic has now forced the issue.
A wide variety of infections can cause ME/CFS, and SARS-CoV-2, the coronavirus that causes COVID-19, is no different: Many cases of long COVID are effectivelyME/CFS by another name. The exact number is hard to define, but past studies have shown that 5 to 27 percent of people infected by variouspathogens, including Epstein-Barr virus and the original SARS, develop ME/CFS. Even if that proportion is 10 times lower for SARS-CoV-2, the number of Americans with ME/CFS would still have doubled in the past three years. “We’re adding an immense volume of patients to an already dysfunctional and overburdened system,” Beth Pollack, a scientist at MIT who studies complex chronic illnesses, told me.
The U.S. has so few doctors who truly understand the disease and know how to treat it that when they convened in 2018 to create a formal coalition, there were only about a dozen, and the youngest was 60. Currently, the coalition’s website lists just 21 names, of whom at least three have retired and one is dead, Linda Tannenbaum, the CEO and president of the Open Medicine Foundation, told me. These specialists are concentrated on the coasts; none work in the Midwest. American ME/CFS patients may outnumber the population of 15 individual states, but ME/CFS specialists couldn’t fill a Major League Baseball roster. Stoops, who is 39, was formally diagnosed with ME/CFS only four years ago, and began receiving proper care from two of those specialists—Lucinda Bateman of the Bateman Horne Center and David Kaufman from the Center for Complex Diseases. Bateman told me that even before the pandemic, she could see fewer than 10 percent of the patients who asked for a consultation. “When I got into those practices, it was like I got into Harvard,” Stoops told me.
ME/CFS specialists, already overwhelmed with demand for their services, now have to decide how to best use and spread their knowledge, at a time when more patients and doctors than ever could benefit from it. Kaufman recently discharged many of the more stable ME/CFS patients in his care—Stoops among them—so that he could start seeing COVID long-haulers who “were just making the circuit of doctors and getting nowhere,” he told me. “I can’t clone myself, and this was the only other way to” make room for new patients.
Bateman, meanwhile, is feverishly focused on educating other clinicians. The hallmark symptom of ME/CFS—post-exertional malaise, or PEM—means even light physical or mental exertion can trigger major crashes that exacerbate every other symptom. Doctors who are unfamiliar with PEM, including many now running long-COVID clinics, can unwittingly hurt their patients by encouraging them to exercise. Bateman is racing to spread that message, and better ways of treating patients, but that means she’ll have to reduce her clinic hours.
These agonizing decisions mean that many existing ME/CFS patients are losing access to the best care they had found so far—what for Stoops meant “the difference between being stuck at home, miserable and in pain, and actually going out once or twice a day, seeing other humans, and breathing fresh air,” she told me. But painful trade-offs might be necessary to finally drag American medicine to a place where it can treat these kinds of complex, oft-neglected conditions. Kaufman is 75 and Bateman is 64. Although both of them told me they’re not retiring anytime soon, they also won’t be practicing forever. To make full use of their expertise and create more doctors like them, the medical profession must face up to decades spent dismissing illnesses such as ME/CFS—an overdue reckoning incited by long COVID. “It’s a disaster possibly wrapped up in a blessing,” Stoops told me. “The system is cracking and needs to crack.”
Many ME/CFS specialists have a deep knowledge of the disease because they’ve experienced it firsthand. Jennifer Curtin, one of the youngest doctors in the field, has two family members with the disease, and had it herself for nine years. She improved enough to make it through medical school and residency training, which showed her that ME/CFS “just isn’t taught,” she told me. Most curricula don’t include it; most textbooks don’t mention it.
Even if doctors learn about ME/CFS, America’s health-care system makes it almost impossible for them to actually help patients. The insurance model pushes physicians toward shorter visits; 15 minutes might feel luxurious. “My average visit length is an hour, which doesn’t include the time I spend going over the patient’s 500 to 1,700 pages of records beforehand,” Curtin said. “It’s not a very scalable kind of care.” (She works with Kaufman at the Center for Complex Diseases, which bills patients directly.) This also explains why the cohort of ME/CFS clinicians is aging out, with little young blood to refresh them. “Hospital systems want physicians to see lots of patients and they want them to follow the rules,” Kaufman said. “There’s less motivation for moving into areas of medicine that are more unknown and challenging.”
ME/CFS is certainly challenging, not least because it’s just “one face of a many-sided problem,” Jaime Seltzer, the director of scientific and medical outreach at the advocacy group MEAction, told me. The condition’s root causes can also lead to several distinct but interlocking illnesses, including mast cell activation syndrome, Ehlers-Danlos syndrome, fibromyalgia, dysautonomia (usually manifesting as POTS), and several autoimmune and gastrointestinal disorders. “I’m still amazed at how often patients come in with Complaint No. 1, and then I find five to seven of the other things,” Kaufman said. These syndromes collectively afflict many organ systems, which can baffle doctors who’ve specialized in just one. Many of them disproportionately affect women, and are subject to medicine’s long-standing tendency to minimize or psychologize women’s pain, Pollack told me: An average woman with Ehlers-Danlos syndrome typically spends 16 years getting a diagnosis, while a man needs only four.
People with long COVID might have many of these conditions and not know about any—because their doctors don’t either. Like ME/CFS, they rarely feature in medical training, and it’s hard to “teach someone about all of them when they’ve never heard of any of them,” Seltzer said. Specialists like Bateman and Kaufman matter because they understand not just ME/CFS but also the connected puzzle pieces. They can look at a patient’s full array of symptoms and prioritize the ones that are most urgent or foundational. They know how to test for conditions that can be invisible to standard medical techniques: “None of my tests came back abnormal until I saw an ME/CFS doctor, and then all my tests came back abnormal,” said Hannah Davis of the Patient-Led Research Collaborative, who has had long COVID since March 2020.
ME/CFS specialists also know how to help, in ways that are directly applicable to cases of long COVID with overlapping symptoms. ME/CFS has no cure but can be managed, often through “simple, inexpensive interventions that can be done through primary care,” Bateman told me. Over-the-counter antihistamines can help patients with inflammatory problems such as mast cell activation syndrome. Low doses of naltrexone, commonly used for addiction disorders, can help those with intense pain. A simple but rarely administered test can show if patients have orthostatic intolerance—a blood-flow problem that worsens other symptoms when people stand or sit upright. Most important, teaching patients about pacing—carefully sensing and managing your energy levels—can prevent debilitating crashes. “We don’t go to an ME/CFS clinic and walk out in remission,” Stoops told me. “You go to become stabilized. The ship has 1,000 holes, and doctors can patch one before the next explodes, keeping the whole thing afloat.”
That’s why the prospect of losing specialists is so galling. Stoops understands why her doctors might choose to focus on education or newly diagnosed COVID long-haulers, but ME/CFS patients are “just so lost already, and to lose what little we have is a really big deal,” she said. Kaufman has offered to refer her to generalist physicians or talk to primary-care doctors on her behalf. But it won’t be the same: “Having one appointment with him is like six to eight appointments with other practitioners,” she said. He educates her about ME/CFS; with other doctors, it’s often the other way round. “I’m going to have to work much harder to receive a similar level of care.”
At least, she will for now. The ME/CFS specialists who are shifting their focus are hoping that they can use this moment of crisis to create more resources for everyone with these diseases. In a few years, Bateman hopes, “there will be 100 times more clinicians who are prepared to manage patients, and many more people with ME/CFS who have access to care.”
For someone who is diagnosed with ME/CFS today, the landscape already looks very different than it did just a decade ago. In 2015, the Institute of Medicine published a landmark report redefining the diagnostic criteria for the disease. In 2017, the CDC stopped recommending exercise therapy as a treatment. In 2021, Bateman and 20 other clinicians published a comprehensive guide to the condition in the journal of the Mayo Clinic. For any mainstream disease, such events—a report, a guideline revision, a review article—would be mundane. For ME/CFS, they felt momentous. And yet, “the current state of things is simply intolerable,” Julie Rehmeyer, a journalist with ME/CFS, told me. Solving the gargantuan challenge posed by complex chronic diseases demands seismic shifts in research funding, medical training, and public attitudes. “Achieving shifts like that takes something big,” Rehmeyer said. “Long COVID is big.”
COVID long-haulers have proved beyond any reasonable doubt that acute viral infections can leave people chronically ill. Many health-care workers, political-decision makers, and influencers either know someone with long COVID or have it themselves. Even if they still don’t know about ME/CFS, their heightened awareness of post-viral illnesses is already making a difference. Mary Dimmock’s son developed ME/CFS in 2011, and before the pandemic, one doctor in 10 might take him seriously. “Now it’s the flip: Only one doctor out of 10 will be a real jerk,” Dimmock told me. “I attribute that to long COVID.”
But being believed is the very least that ME/CFS patients deserve. They need therapeutics that target the root causes of the disease, which will require a clear understanding of those causes, which will require coordinated, well-funded research—three things ME/CFS has historically lacked. But here, too, “long COVID is going to be a catalyst,” Amy Proal, the president of the Polybio Research Foundation, told me. She is leading the Long Covid Research Initiative—a group of scientists, including ME/CFS researchers, that will use state-of-the-art techniques to see exactly how the new coronavirus causes long COVID, and rapidly push potential treatments through clinical trials. The National Institutes of Health has also committed $1.15 billion to long-COVID research, and while some advocates are concerned about how that money will be spent, Rehmeyer notes that the amount is still almost 80 times greater than the paltry $15 million spent on ME/CFS every year—less than any other disease in the NIH’s portfolio, relative to its societal burden. “Even if 90 percent is wasted, we’d be doing a lot better,” she said.
While they wait for better treatments, patients also need the medical community to heed the lessons that they and their clinicians have learned. For example, the American Academy for Family Physicians website still wrongly recommends exercise therapy and links ME/CFS to childhood abuse. “That group of doctors is very important to these patients,” Dimmock said, “so what does that say to them about what this disease is all about?”
Despite all evidence to the contrary, many clinicians and researchers still don’t see ME/CFS as a legitimate illness and are quick to dismiss any connection between it and long COVID. To ensure that both groups of patients get the best possible treatments, instead of advice that might harm them, ME/CFS specialists are working to disseminate their hard-won knowledge. Bateman and her colleagues have been creating educational resources for cliniciansand patients, continuing-medical-education courses, and an online lecture series. Jennifer Curtin has spent two years mapping all the decisions she makes when seeing a new patient, and is converting those into a tool that other clinicians can use. As part of her new start-up, called RTHM, she’s also trying to develop better ways of testing for ME/CFS and its related syndromes, of visualizing the hefty electronic health records that chronically ill patients accumulate, and of tracking the treatments they try and their effects. “There are a lot of things that need to be fixed for this kind of care to be scalable,” Curtin told me.
Had such shifts already occurred, the medical profession might have had more to offer COVID long-haulers beyond bewilderment and dismissal. But if the profession starts listening to the ME/CFS community now, it will stand the best chance of helping people being disabled by COVID, and of steeling itself against future epidemics. Pathogens have been chronically disabling people for the longest time, and more pandemics are inevitable. The current one could and should be the last whose long-haulers are greeted with disbelief.
New centers that cater to ME/CFS patients are already emerging. RTHM is currently focused on COVID long-haulers but will take on some of David Kaufman’s former patients in November, and will open its waiting list to the broader ME/CFS community in December. (It is currently licensed to practice in just five states but expects to expand soon.) David Putrino, who leads a long-COVID rehabilitation clinic in Mount Sinai, is trying to raise funds for a new clinic that will treat both long COVID and ME/CFS. He credits ME/CFS patients with opening his eyes to the connection between long COVID and their condition.
Every ME/CFS patient I’ve talked with predicted long COVID’s arrival well before most doctors or even epidemiologists started catching up. They know more about complex chronic illnesses than many of the people now treating long COVID do. Despite having a condition that saps their energy, many have spent the past few years helping long-haulers navigate what for them was well-trodden terrain: “I did barely anything but work in 2020,” Seltzer told me. Against the odds, they’ve survived. But the pandemic has created a catalytic opportunity for the odds to finally be tilted in their favor, “so that neither patients nor doctors of any complex chronic illness have to be heroes anymore,” Rehmeyer said.