“I’m so sorry that I have to reschedule the first batch of Arena shows” scheduled for Feb. 27 through March 17, Manilow said on X. “But when I do come back, I will COME BACK!!!”
Canceled shows also include his March 11 concert at North Charleston Coliseum in Charleston, which was a makeup date for a concert canceled in January.
His condition has limited his endurance behind the mike, he said.
“Very depressing visit,” Manilow said about Friday’s trip to his surgeon. “I told him that I have been using the treadmill three times a day (I have) but that I still couldn’t sing more than three songs in a row before I had to stop.
“But I was sure that I would be able to do the Arena shows in a few weeks,” he said.
“’You won’t make it through,’” he said his surgeon replied, shaking his head and looking down.
“Well, I had a feeling he’d say that,” Manilow posted. “Deep down, I wanted to go back — but my body knew what my heart didn’t want to admit: I wasn’t ready.”
Joe Marusak has been a reporter for The Charlotte Observer since 1989 covering the people, municipalities and major news events of the region, and was a news bureau editor for the paper. He currently reports on breaking news. Support my work with a digital subscription
Brad Arnold, lead singer and founding member of the alternative rock band 3 Doors Down, has died after a lengthy cancer diagnosis. He was 47.Related video above: Remembering those we lost in 2026His death was announced in an Instagram post from the band’s account. “With his beloved wife Jennifer and his family by his side, he passed away peacefully, surrounded by loved ones, in his sleep after his courageous battle with cancer,” the post read.Arnold was diagnosed with stage 4 metastatic lung cancer in May of last year, which was also announced via the band’s Instagram account.”Brad helped redefine mainstream rock music, blending post-grunge accessibility with emotionally direct songwriting and lyrical themes that resonated with everyday listeners,” the post read.Arnold and the band saw peak popularity in the early 2000s, following their breakout hit single “Kryptonite,” from their debut album “The Better Life.””Those closest to him will remember not only his talent, but his warmth, humility, faith, and deep love for his family and friends,” the post read.
Brad Arnold, lead singer and founding member of the alternative rock band 3 Doors Down, has died after a lengthy cancer diagnosis. He was 47.
Related video above: Remembering those we lost in 2026
“With his beloved wife Jennifer and his family by his side, he passed away peacefully, surrounded by loved ones, in his sleep after his courageous battle with cancer,” the post read.
Arnold was diagnosed with stage 4 metastatic lung cancer in May of last year, which was also announced via the band’s Instagram account.
NBC
Brad Arnold of musical guest 3 Doors Down performs on “The Tonight Show w/ Jay Leno” on Oct. 27, 2000.
Slaven Vlasic
Singer Brad Arnold of 3 Doors Down performs at the 2023 FOX & Friends’ Summer Concert Series on May 26, 2023, in New York City.
“Brad helped redefine mainstream rock music, blending post-grunge accessibility with emotionally direct songwriting and lyrical themes that resonated with everyday listeners,” the post read.
Arnold and the band saw peak popularity in the early 2000s, following their breakout hit single “Kryptonite,” from their debut album “The Better Life.”
“Those closest to him will remember not only his talent, but his warmth, humility, faith, and deep love for his family and friends,” the post read.
Scott Legato
Brad Arnold of 3 Doors Down performs at Little Caesars Arena on Nov. 20, 2024, in Detroit, Michigan.
Barry Manilow gave fans an update on his health shortly after sharing his cancer diagnosis.
In an Instagram photo shared Friday, the 82-year-old singer was lying in a hospital bed in a green hospital gown with a smile on his face, captioning the post, “Better Today!”
Fans were happy to see the “Copacabana” singer was doing better, with many sending him love and positive wishes in the comments section.
“We love you Barry!! God is good! Can’t wait to see you again soon.”
Manilow gave his fans a health update, letting them know he is doing better.(Barry Manilow Instagram)
“I’ve loved you Barry for 50 years! My heart skipped a beat when I heard you were sick,” another said. “So glad to see you are doing well and recuperating.”
Manilow first shared that a cancerous spot had been found on his lungs in an Instagram post shared in late December.
He explained that after suffering “through six weeks of bronchitis followed by a relapse of another five weeks,” his doctors ordered more tests out of an abundance of caution and found something more serious.
“Even though I was over the bronchitis and back on stage at the Westgate Las Vegas, my wonderful doctor ordered an MRI just to make sure that everything was OK. The MRI discovered a cancerous spot on my left lung that needs to be removed. It’s pure luck (and a great doctor) that it was found so early. That’s the good news.”
Manilow first shared his cancer diagnosis last month.(Mat Hayward/Getty Images)
“The bad news is that now that the ‘Christmas A Gift of Love’ concerts are over, I’m going into surgery to have the spot removed,” he continued. “The doctors do not believe it has spread, and I’m taking tests to confirm the diagnosis. So, that’s it. No chemo. No radiation. Just chicken soup and ‘I Love Lucy’ reruns.”
He went on to apologize to all his fans who had already purchased tickets, telling them he was “looking forward to the January shows” as much as they were and that he “hate[s] having to move everything around.”
Manilow is known for hits such as “I Write the Songs” and “Can’t Smile Without You,” but he told NBC News in April 2024 he didn’t think his biggest hit, “Copacabana,” would become what it did. He explained he and his co-producer at the time, Ron Duarte, “never thought it would ever get played on the radio.”
Manilow didn’t think his hit song “Copacabana” would go on to become as big as it did.(Ann Limongello/Disney General Entertainment Content via Getty Images )
“But we took it to a disco, when there were discos, and we asked the DJ to play it,” Manilow said. “And everybody ran to the dance floor and started to dance like they were back in the 1940s. They were dipping the girls and all because, you know, it’s ‘Copa.’ And, I said to Ron, ‘We may be onto something with this one.’ And then, it turned out to be the most popular song in my catalog.”
Lori Bashian is an entertainment writer for Fox News Digital.
Barry Manilow, the singer-songwriter known for hits like “Copacabana,” announced Monday that he was recently diagnosed with lung cancer and will need to pause his current concert run in order to have surgery.
“As many of you know I recently went through six weeks of bronchitis followed by a relapse of another five weeks. Even though I was over the bronchitis and back on stage at the Westgate Las Vegas, my wonderful doctor ordered an MRI just to make sure that everything was OK,” Manilow, 82, said in a statement on Instagram. “The MRI discovered a cancerous spot on my left lung that needs to be removed.”
This is a developing story. Please check back for updates.
During the first three years of Augenstein’s lung cancer journey, he’s been happy to be able to share things he has been learning along the way.
WTOP’s Neal Augenstein was diagnosed with Stage 4 lung cancer in 2022. (WTOP/Neal Augenstein)
WTOP’s Neal Augenstein was diagnosed with Stage 4 lung cancer in 2022. (WTOP/Neal Augenstein)
In my first 25 years at WTOP, my reports about lung cancer were primarily stories about famous people who died from the deadliest and second-most common cancer in the U.S. — until I was diagnosed with Stage 4 lung cancer exactly three years ago.
Since then, most of my lung cancer stories have been about living.
Within six months of being diagnosed with Stage 4 non-small cell lung cancer just before Thanksgiving 2022, after great results with one-pill-a-day targeted therapy that shrank cancerous tumors and lymph nodes in both lungs, I became eligible for a robotic-assisted lung lobectomy.
Since then, I’ve had no evidence of disease, and have remained cancer-free since May 2023, while continuing to take my daily pill.
Giving thanks? Indeed.
During the first three years of my journey, I’ve been happy to be able to share things I’ve been learning along the way.
Biomarker testing involves testing biopsied lung tissue — often taken during a bronchoscopy — to try to learn the exact cell mutation that caused a patient’s cancer.
“The importance of testing is if they have that mutation, then the treatment is very different, and the patient outcomes are also much better,” thoracic medical oncologist Ram Subramanian with Inova Schar Cancer Institute in Fairfax County, Virginia, told me.
In my case, I was diagnosed with EGFR-positive lung cancer, which has several targeted treatments available, and generally limits the side effects of treatment compared to chemotherapy.
Despite having no evidence of cancer now, I (and my doctors) wouldn’t say that I’m “cured,” since I was originally diagnosed after cancer had spread from the original site in my left lung.
In 2025, life with lung cancer can be similar to life with other chronic diseases, including diabetes or heart disease.
The key is aggressive surveillance, which in my case involves low-dose CT scans every four months, as well as brain MRIs and liquid biopsies twice a year. If something suspicious were to show up on one of these scans, it would likely be early-stage, which could be removed with surgery or targeted by radiation.
“No evidence of intracranial metastasis” — good news in my twice-yearly brain MRI as part of aggressive surveillance, since I’ve been cancer-free for two years after dx of stage 4 #lungcancer. (Admit I had to ask whether gown ties in front or back) pic.twitter.com/uJSbaAH0gv
And, while the American Lung Association’s 2025 State of Lung Cancer report shows the five-year survival rate for lung cancer in the U.S. has risen to 29.7%, which represents a 26% improvement over the past five years, research continues to enable earlier detection, including the use of artificial intelligence.
Lung cancer patients in the D.C. region are lucky — there are a large number of clinical trials in Virginia, Maryland and the District, offering new options and hope for patients and their families.
Personally, while I’ve been lucky to not have any recurrences in my first three years living with cancer, I often discuss trials with my thoracic oncologist Amin Benyounes, who is the co-leader at the Inova Schar Cancer Institute’s Phase One Program.
Benyounes said many patients considering enrollment in a clinical trial worry about the unknown: “Will this make me feel worse, will it make me feel sick, could it hurt more than it would help? Will my kids or my partner have to bear the burden of me feeling sick?”
With clinical trials affording the possibilities for longer survival with fewer side effects, some patients ask, “What if I get my hopes up, and it doesn’t work?”
According to Benyounes: “My answer to that is usually, ‘We have to take things one step at a time.’”
That’s the same guidance he gave me when I began my cancer journey, three years ago.
Get breaking news and daily headlines delivered to your email inbox by signing up here.
New artificial intelligence technology is helping diagnose the U.S.’s most deadly cancer sooner, greatly improving the chances of lung cancer patients’ survival.
New artificial intelligence technology is helping diagnose the U.S.’s most deadly cancer sooner, greatly improving the chances of patients’ survival.
The key? Detecting tiny lung nodules when doctors aren’t screening for cancer, and automating and streamlining follow-up care. While most incidentally-discovered lung nodules turn out to be noncancerous, some become malignant over time.
The importance of catching lung cancer early is clear: The five-year survival rate for non-small cell lung cancer when detected in localized Stage 1 is 67%. However, most lung cancer is diagnosed after it has spread to other organs, when the five-year rate is 12%, according to the American Cancer Society.
Inova Schar Cancer Institute, based in Fairfax, Virginia, is one forward-thinking cancer center harnessing the power of AI to flag incidental lung nodules that often go unnoticed, during an emergency room CT scan or MRI for pneumonia or a broken bone. The Eon Lung Cancer Screening system uses computational linguistics and natural language processing to scan radiology reports.
The company says it identifies high-risk patients with 98.3% accuracy by analyzing imaging data and integrating with electronic health records in real time.
‘The patient is still in the ER, we call and tell them to come right to the clinic’
Amit “Bobby” Mahajan is the medical director of interventional pulmonology in the Inova Health System. (Disclosure: He is also the doctor who did my bronchoscopy in November 2022 and told me I had lung cancer. After four months of one-pill-a-day targeted therapy and a robotic-assisted lobectomy, I was declared cancer-free in May 2023 and have remained that way while continuing my daily pill.)
AI-powered technology is enabling Schar’s interventional pulmonologists and surgeons to get patients with found-by-accident nodules into cancer care months or years earlier. Mahajan heads the Incidental Pulmonary Nodule Clinic, as part of the Inova Saville Cancer Screening and Prevention Center.
“Whether it be an MRI, a chest CT, or abdominal CT, it takes that data, comprises it into a finding, and then makes a risk score of that being cancer,” said Mahajan, during a recent WTOP visit and demonstration of the Eon technology.
With the AI system scanning electronic health records as data is entered, “We’re able to call the patient and say, ‘Look, I know you just had a CT scan in the ER for your abdominal pain, but we also caught a lung nodule in the bottom of your lung that is suspicious,’” Mahajan said.
“For better or worse, we’ve had more than a handful of people who we’ve said, ‘We need to send you over to the clinic right now, because you came in for something that’s nothing to worry about, but we did find something that needs to be addressed today,’” he added.
Traditionally, reaching a cancer diagnosis for a patient with a persistent cough or other symptoms can take weeks and requires patients and doctors to coordinate follow-up scans and labs.
“From an AI perspective, the system will learn more from our CT scans and image reports every time it sees one, and starts picking out the word ‘spiculated,’ the word ‘nodule,’ and where it’s located,”‘ Mahajan said.
While benign nodules usually have smooth borders, a spiculated nodule’s edges appear irregular, or spiky, which often suggests the lesion is malignant.
“It takes that data to the very well known Brock Model for risk of lung cancer, and it will actually calculate the risk of cancer in those patients, and give us a percentage,” Mahajan said. “Anyone over 5%, we call, and get them into the clinic right away, most of the time in the same week.”
After being notified of an incidental nodule found in ER imaging, some patients prefer to check with their primary care physician.
“Totally reasonable,” Mahajan said.
Streamlining the follow-up process helps reduce the risk of patients “falling through the cracks.”
“We’ve biopsied them two days later, and gotten a diagnosis of cancer,” Mahajan said. “Luckily, most have been early stage disease and they’ve been resected afterward.”
With lung cancer, resection is a surgical procedure to remove lung tissue affected by cancer and is regarded as the most effective treatment for cancer that hasn’t spread to other organs.
“Our goal is to get a patient with a newly-diagnosed lung cancer evaluated as soon as possible, to get them into surgery,” Schar thoracic surgeon Melanie Subramanian said. “It’s not only better for treating the disease, but it also gives patients a peace of mind too, knowing that they have a treatment plan and a treatment team.”
The AI system creates guideline-based care plans, and sends alerts to doctors and nurse navigators, helping patients stay on schedule for future screenings.
‘It’s as close to an Xbox controller as you get’
Artificial intelligence is also enabling robotic bronchoscopy procedures.
“Previously, when we had to biopsy these small nodules in the lung, we had to use a handheld camera, to drive down as far as we could, but the lungs and airways get smaller and smaller the further out you go,” Mahajan said.
“Now, we have robotic platforms,” Mahajan added. “The patient is completely asleep, and we drive about a four millimeter camera down to these nodules, using a handheld controller that’s as close to an Xbox controller as you can get.”
And AI helps navigate through the airways: “There’s advanced imaging associated as well, and with the robotic platform, we can pretty much reach anything in the lung nowadays,” he said.
Inova Schar says 69% of lung cancers are now being detected at Stage 1 or 2, compared to only 34% without low-dose CT screening and proactive follow-up of incidental nodules.
Get breaking news and daily headlines delivered to your email inbox by signing up here.
Endurance athlete Kevin Humphrey was used to discomfort. He regularly participated in ultramarathons and other intense events. Swimming, biking and running dozens of miles at a time was standard for him. His two young sons also kept him active even when he wasn’t training. But in January 2024, a persistent back pain kept bothering him.
The pain “just would not go away,” Humphrey said. He couldn’t sleep on his back. At the same time, he started coughing. He was diagnosed with pneumonia, but his symptoms lingered even after treatment. A chest CT scan found “something going on” in his left lung. A biopsy of the organ came back inconclusive, Humphrey said, but he kept pushing for answers.
“I knew something was off. It just didn’t feel right,” Humphrey said.
Humphrey traveled from Michigan to Chicago to seek a second opinion at Northwestern Medicine in May 2024. A bronchoscopy found shocking results: There was a tumor in his lung that was crushing the left side of his windpipe, causing the coughing and pain.
“I was really in disbelief,” said Humphrey, who had never smoked and had no family history of lung cancer. “It wasn’t even on my radar as a possibility. It wasn’t even an option in my mind.”
Kevin Humphrey.
Kevin Humphrey
“A very concerning and dire situation”
Humphrey was diagnosed with Stage IV non-small cell adenocarcinoma, joining the growing number of young, non-smoking patients diagnosed with lung cancer. The rise may be driven by environmental or lifestyle factors, Dr. Jonathan Villena-Vargas, a thoracic surgeon at NewYork-Presbyterian and Weill Cornell Medicine, previously told CBS News. Villena-Vargas, who did not treat Humphrey, said there is no definitive reason for the increase.
Further tests found that the cancer had spread beyond Humphrey’s lung and had likely been growing for at least a year, Humphrey said. The disease typically has a 37% 5-year survival rate at that point, according to the Cleveland Clinic.
Humphrey’s tumor was “pretty advanced” and too large for surgery at first, said Dr. Daniel Dammrich, the Northwestern Medicine oncologist who treated him. But doctors were able to identify a “driver mutation” that was encouraging the cancer’s growth. These mutations are more common in young, non-smoking patients, Villena-Vargas said.
Identifying the mutation “really opened the door for some of our more nuanced, targeted therapies,” Dammrich said, and “turned a very concerning and dire situation into a much more optimistic one.”
Dammrich and Humphrey agreed on an aggressive plan that would combine targeted immunotherapy with chemotherapy, in the hopes that the medications would shrink the tumor enough for surgery. Humphrey began immunotherapy immediately, then had chemotherapy in summer 2024. By August, the cancer was operable.
Kevin Humphrey receives chemotherapy at Northwestern Medicine.
Kevin Humphrey
“The biggest question mark”
Removing the cancer meant taking out about half of Humphrey’s left lung. The athlete wasn’t sure what that would mean for his passion.
“You just had no idea. Can you run again, can you bike, can you do all these endurance sports that I’ve loved doing?” Humphrey said. “That was the biggest question mark going into surgery.”
Despite the unknowns, he focused on the future. Michigan’s Ironman 70.3 race — which included a 1-mile swim, 56.1-mile bike ride and a 13.2 mile run — was scheduled to take place a year and a day after his surgery. Humphrey decided to sign up, despite his fears.
Kevin Humphrey in the hospital.
Kevin Humphrey
Humphrey had surgery in mid-September. The operation removed most of the cancer, Dammrich said. Recovery was its own battle. Broken ribs and a “pretty big” incision made it difficult for Humphrey to do simple tasks like get out of bed or walk more than a few steps. Running was out of the question for months. But he kept putting one foot in front of the other until his strength and endurance began to slowly return. Even on the hardest days, the upcoming race kept him motivated.
“It was a great mental thing to put on the calendar and train for,” Humphrey said.
“Across the finish line”
On Sept. 14, Humphrey was one of over 1,600 athletes who took part in the Ironman. He finished in just under five and a half hours, coming in 411th place. The race was exhausting and emotional, Humphrey said.
“You’re replaying everything that’s happened over the past year and the whirlwind it’s been,” Humphrey said. “For me, when I got to the point of knowing ‘I’m going to finish this race’ and thinking about my young boys, my wife, the family and the community and support system we’ve had throughout the whole year, and how grateful I am to not only be here but to continue to do these types of races and events. I certainly did not think that was going to be the case when I received the diagnosis in May of ’24.”
Kevin Humphrey’s son gives him a high-five during the Ironman 70.3 Michigan.
Kevin Humphrey
Humphrey’s medical situation is also positive. He had a complete response to the treatment, and there is currently no evidence of disease in his body, Dammrich said. Regular CT scans and blood tests watch for any new tumor growth. Humphrey remains on immunotherapy with few side effects.
On Oct. 12, less than a month after the Ironman, Humphrey ran the Chicago marathon for the sixth time. Over 53,000 runners participated in the race. Humphrey placed 25,395th, finishing in about seven and a half hours. It was “40 or 45 minutes slower” than when he ran the same race in 2023, Humphrey said, but he was proud to have finished.
“My goal was just to get across the finish line, and that’s what we did,” Humphrey said. “I was just grateful for the ability to be out there and to run and be doing the things that I’ve loved doing for such a long time.”
Kevin Humphrey’s sons cheer him on during the Chicago marathon.
If you head down to the National Mall over the next two weeks, you’ll notice 60,000 white and American flags blanketing the lawn in front of the Capitol. It is an installation that hopes to hammer home the importance of early detection during Lung Cancer Awareness Month.
“Anyone with lungs can get lung cancer,” said Terri Ann DiJulio, a 20-year survivor of lung cancer who has received the diagnosis three times.
“I’m one of six people in my family to be diagnosed, and I’m the definition of early detection saves lives.”
Each of the 60,000 flags on the mall represents two deaths seen every year from lung cancer. That is more than colorectal and pancreatic cancers combined.
Another lung cancer survivor at the dedication of the Lungevity Foundation’s installation was WTOP’s own Neal Augenstein.
“I really didn’t think about it until I saw all of these flags, and it made me realize that it could have been me,” Augenstein said.
He received his stage four lung cancer diagnosis nearly three years ago on Nov. 22, 2022. He had cancerous tumors and cancerous lymph nodes in both lungs.
“Really, to be honest, I had thought I will never get lung cancer. I don’t smoke. I’m at no risk for it, but the fact is that I got lung cancer, I don’t know how,” he told WTOP.
Thanks to a one-pill-a-day targeted therapy and a robotic-assisted lobectomy Augenstein was declared cancer free just six months later.
The Lungevity Foundation hopes this mind-boggling number of flags and deaths is a reminder to any visitor about the importance of early detection even for people who do not have risk factors. Close to two-thirds of new diagnosis are among people with no or past tobacco use.
“If you catch lung cancer, for example, in stage one, you can have a greater than 90% chance of curing that cancer,” said Dr. Michael Gieske, director of lung cancer screening at St. Elizabeth Healthcare in northern Kentucky.
“Lung cancer, historically, has been a death sentence and we’re trying to change that narrative.”
Gieske described the screening as a non-invasive and quick CT scan.
“You’re in and out of the scanner within three minutes. It’s the highest yield test we have for the deadliest cancer that we have to deal with,” Gieske said.
According to the American Lung Association, nationally only about 18% of patients at high risk were screened.
The sea of flags is also a message to the federal government about the importance of continued research on the deadliest cancer in the U.S.
“I think there are multiple levels that we could do it. I think at the federal level, in terms of funding research and ensuring that we have awareness campaigns, public awareness campaigns, particularly to dispel a lot of the myths about lung cancer,” said Andrea Ferris, president and CEO of Lungevity.
And while the vast number of flags is still tragic, it is also a sign of hope for others that get the diagnosis.
“When my mother died from lung cancer in 2008, it would have been almost double the field. And so, thanks to advancements in research and now early detection, we had the opportunity to really change that,” Ferris said.
“My hope is that people look at these flags with hope. You know the fact that there are people now who’ve lived several years with the current lung cancer treatments,” Augenstein said.
“I’m doing great. My hope is that there’s a lot of people who feel empowered to get the good treatment and to look at the science and be really good patients and live a long life with lung cancer.”
The installation will be on the National Mall for the next two weeks. Lungevity will also host a lung health resource fair there this weekend.
Get breaking news and daily headlines delivered to your email inbox by signing up here.
Leslie Stoll developed a blood clot that led to a pulmonary embolism after she broke her leg in 2014. The embolism was treated, but another occurred when Stoll had surgery on her foot years later. After the treatment, she was referred to a hematologist who could prescribe blood thinners and monitor the clot.
At an appointment in 2024, the hematologist recommended a CT scan. It showed a small anomaly in her lungs. Stoll wasn’t worried: She was an athlete and former boxer who had never smoked. Her lung function felt normal.
“I tried to reassure him that it was nothing, and it was probably something that was damaged from my pulmonary embolism, and he didn’t think I was very good at diagnosing myself,” Stoll told CBS News. “He was like, ‘Well, it probably is nothing, but let’s schedule a PET scan, just to check.’”
Stoll scheduled the test, but still doubted there was anything wrong, even telling the exam tech that she believed she was just going through the motions. Shortly after the scan, results saying that “malignancy could not be ruled out” were uploaded to an online patient portal. Then Stoll’s doctor called and asked her to come in the next day. Stoll’s doctor recommended a lung biopsy.
Leslie Stoll runs a race at Disney World in 2023, one year before her diagnosis.
Leslie Stoll
The biopsy revealed that Stoll had Stage One lung cancer, becoming one of the small but rising number of people diagnosed with the disease despite never smoking.
“I was just shocked at the fact that it could happen to me, disappointed that it could happen to me,” Stoll said. “I would love to have gone through life thinking I was immune to cancer, that it couldn’t get me. This was a big awakening that I might check ‘very healthy’ on my doctor’s forms when I go in every year, but all of a sudden I was not very healthy.”
Lung cancer in “never-smokers”
Dr. Jonathan Villena-Vargas, a thoracic surgeon at NewYork-Presbyterian and Weill Cornell Medicine, told CBS News in February that non-smokers with lung cancer are more common than people might expect. “Never-smokers” account for about 20% of the 250,000 new lung cancer diagnoses each year, said Villena-Vargas, who was not involved in Stoll’s care.
Dr. Lucas Delasos, an oncologist at the Cleveland Clinic who did not treat Stoll, said women, particularly those of Asian descent, are more likely to be diagnosed with lung cancer despite never smoking.
Younger non-smoking patients are also more likely to have mutations that drive the disease’s growth, Delasos said. Identifying those mutations allows for more personalized treatment.
Some of the increase in diagnoses may come from an increased awareness, Delasos said. A spot that might have been ignored or missed by earlier technology is now more likely to be tested and diagnosed, he said. Researchers are also studying environmental factors, like radon gas or other hazardous materials.
Leslie Stoll at Northwestern Medicine.
Leslie Stoll
“Too young to not be aggressive”
Stoll was referred to Dr. Andrew Arndt, a thoracic surgeon at Northwestern Medicine. He encouraged her to treat the cancer with a robotic surgery that would remove a section of her right lung’s lower lobe.
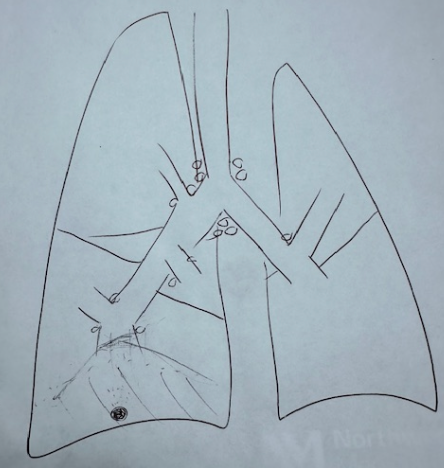
Stoll worried the operation would impact her ability to exercise or take part in daily life. To reassure her, Arndt sketched her lung and drew what the minimally invasive operation would entail.
“He said I was too young to ignore this, I was too young to not be aggressive with it,” Stoll said. She agreed to the surgery.
Dr. Andrew Arndt’s sketch of Leslie Stoll’s lung.
Leslie Stoll
During the procedure, Arndt biopsied Stoll’s lymph nodes to confirm the cancer hadn’t spread. The tests were negative, meaning Stoll didn’t have to undergo chemotherapy or radiation treatment.
Further tests found that she had no evidence of cancer after the surgery, Arndt said.
“I was able to get my life back”
Recovery felt harder than surgery, Stoll said. Before, she had easily been able to run for miles at a time. The day after the operation, Stoll “could barely walk down the hall.” Being unable to exercise as usual felt like the cancer “took away some of my personality,” Stoll said.
As the days ticked by, Stoll slowly improved. She went from trudging down the hall to taking long walks in her neighborhood. Hills became less of a struggle. When she was cleared for full activity, she celebrated with a “very slow” run. Nine months after the surgery, she climbed Phoenix’s Camelback Mountain, a difficult trek that can take up to three hours.
“I was just determined to take some action to get back to my old self as soon as possible,” Stoll said.
Leslie Stoll hiking Camelback Mountain.
Leslie Stoll
Now, about six months after her surgery, Stoll is back to her regular life. She works out and walks her dog twice a day. Arndt’s drawing of her lung sits on her mantle as a reminder of what she went through. She has regular scans to make sure the cancer has not returned. Stoll said she is careful to attend all of her follow-up appointments, aware that those precautions were key to diagnosing her cancer early.
“I was able to stop my cancer from taking control of my life, and I was able to get my life back,” Stoll said. “If I had never gone to that follow-up appointment, then I might still have cancer growing inside me.”
Frederick Health Medical Group is outpacing national averages by detecting nearly 40% of lung cancers at Stage 1 with 3D imaging and robotic bronchoscopy.
An ion robotic bronchoscopy system used by Frederick Health.(Courtesy Frederick Health)
An ion robotic bronchoscopy system used by Frederick Health.(Courtesy Frederick Health)
Most lung cancer in the U.S. is diagnosed at Stage 4, after the leading cause of cancer deaths has spread to other parts of the body. However, a Maryland health system is outpacing national averages by detecting nearly 40% of lung cancers at Stage 1.
Frederick Health Medical Group, in Frederick, Maryland, identifies lung cancer early by investigating tiny clues, which enables patients to get to cancer specialists earlier in the process, according to a doctor with the group.
“Lung cancer is a scary thing because it does not cause symptoms until it’s too late,” said Dr. Maurice Smith, thoracic surgeon and medical director for chest surgery with Frederick Health Medical Group.
With new 3D imaging, robotic bronchoscopy and a comprehensive multidisciplinary approach, Frederick Health is diagnosing nearly 40% of lung cancers at Stage 1, surpassing the national average of 27%.
“We’re able to get to these abnormalities in the lung before they get too big,” Smith said.
Doctors and researchers have long known that early diagnosis of lung cancer improves the success of available treatments, and the patient’s quality of life.
With more and more younger patients being diagnosed with lung cancer, advocacy groups have called for earlier screening with low-dose CT scans. Currently, the U.S. Preventive Services Task Force guidelines is limited to adults aged 50 to 80, who have smoked a pack of cigarettes a day for 20 years.
“That’s for patients who are high risk,” Smith said. “The government pays for it for 50 through 80. You don’t necessarily have an abnormality, but you’re trying to screen to see if you do.”
And only approximately 20% of Americans who are eligible for screening get it done on an annual basis.
Most of the lung cancer cases discovered by Frederick Health came when doctors weren’t looking for cancer.
Smith said that of the 130 lung cancers diagnosed at Frederick Health recently, 60% were identified after a CT scan for another reason, and only 40% were discovered during lung cancer screening.
According to the American Cancer Society, the five-year survival rate for non-small cell lung cancer discovered in Stage 1 is 67%. For Stage 4, in which lung cancer has spread to other organs, the five-year survival rate is 12%, although it continues to improve significantly with recent trends in targeted therapies.
Early diagnosis, even though ‘it didn’t blare lung cancer’
Smith said Frederick Health isn’t getting more people in for CT lung cancer screening, but rather capitalizing on CT scans that are done in the emergency room or a physician’s office to deal with everything from a cough to a sprain.
“If you go to the ER department, for the most part you’re going to walk out of there with a CT scan,” Smith said. “The disconnect has been that those CT scans in the ER, those CT scans in the community, were not being followed up on, because it wasn’t flagged as suspicious, because it was a smaller nodule.”
But that’s changed with implementation of ION robotic technology, manufactured by Intuitive, along with advanced 3D imaging.
“We’re able to go after lesions as small as an apple seed,” Smith said.
Now, if a CT scan done in the ER or the office of a Frederick Health provider discovers a nodule that was previously considered too small for concern, a report is automatically forwarded to the center’s incidental pulmonary nodules clinic, which contacts the patient and primary care provider to coordinate follow-up.
It’s cancer: Now what?
New robotic bronchoscopy technology gives surgeons and interventional pulmonologists a way to perform minimally invasive biopsies of lung nodules.
“The traditional bronchoscopy is about the size of your thumb, so it can only navigate to a certain point within your airway,” Smith said. “With our new robotic bronchoscopy, it’s very thin and flexible, so it’s able to reach any point in the lung from the outside.”
During the staging process to determine whether lung cancer has spread, a patient would typically undergo three procedures: a bronchoscopy to retrieve a biopsy, another bronchoscopy after diagnosis to look for spread to lymph nodes in the center of the chest, and finally a lobectomy, or other surgery to remove an early-stage tumor.
“So now, from that first appointment, we are usually getting patients a biopsy within two to three weeks,” Smith said. “From beginning to end, to diagnosis, we’re about three to four weeks, which we’re very excited about.”
Get breaking news and daily headlines delivered to your email inbox by signing up here.
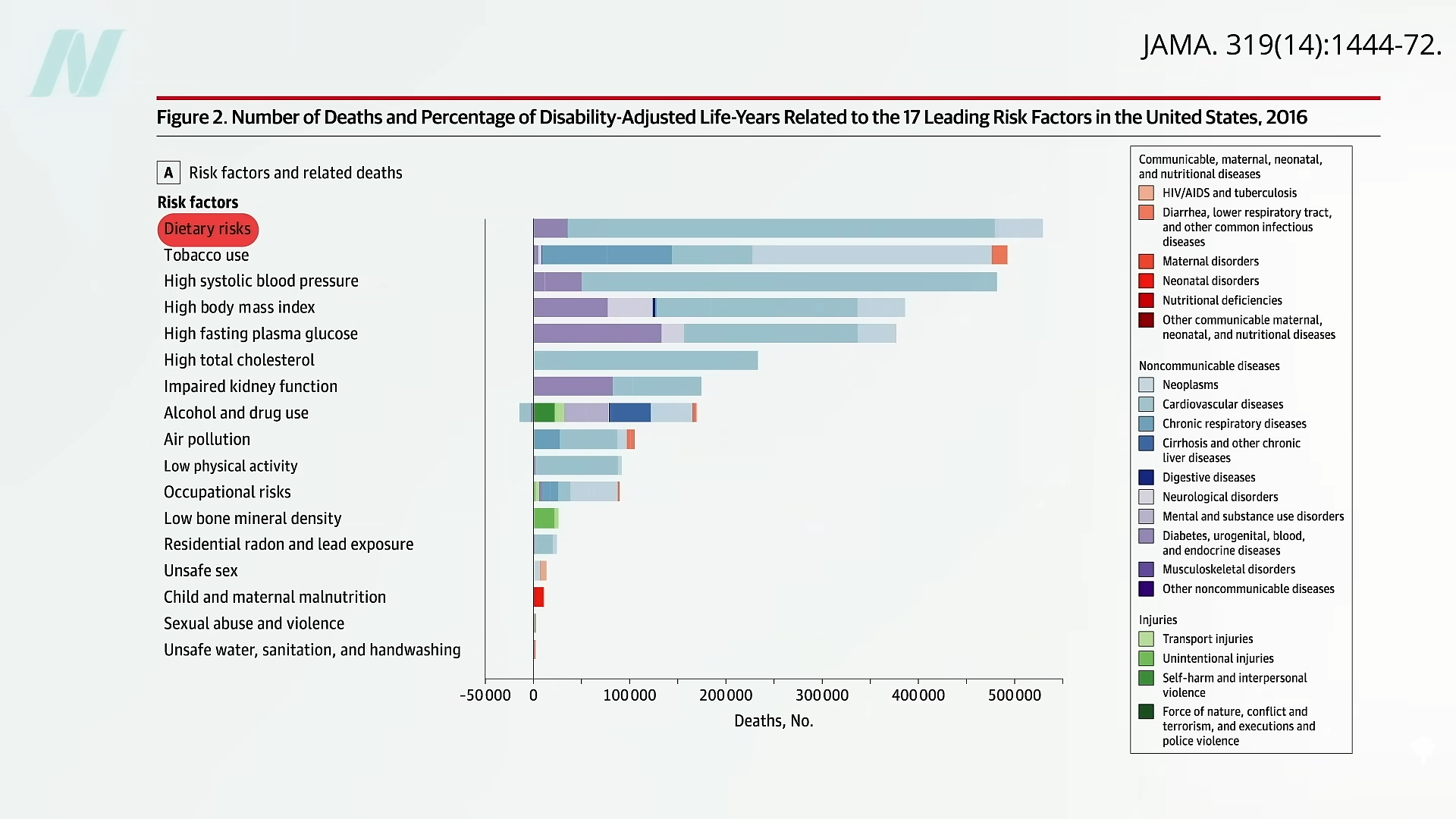
The leading risk factor for death in the United States is the American diet.
About a decade ago, the American Heart Association (AHA) expressed concern that its “2020 target of improving cardiovascular health by 20% by 2020 will not be reached if current trends continue.” By 2006, most people were already not smoking and had nearly achieved their goal for exercise. But when it came to healthy diet score, only about 1 percent got a 4 or 5 out of its diet quality score of 0 to 5, as you can see below and at 0:35 in my video, Friday Favorites: The Scientific Consensus on a Healthy Diet. And that’s with such “ideal” criteria as drinking less than four and a half cups of soda a week.
In the last decade, the AHA saw a bump in the prevalence of the ideal healthy diet score to about 1 percent of Americans reaching those kinds of basic criteria, but, given its “aggressive” goal of reaching a “20% target” by 2020, it hoped to turn that 1 percent into about 1.2 percent. (Really, as you can see here and at 1:01 in my video.)
So, how’d we do? According to the 2019 update, it seems we’ve slipped down to as low as one in a thousand, and American teens scored a big fat zero. No wonder, perhaps, that “for all mortality-based metrics, the US rank declined…to 27th or 28th among 34 OECD [industrialized] countries. Citizens living in countries with a substantially lower gross domestic product and health expenditure per capita…have lower mortality rates than those in the United States.” Slovenia, for example, beat the United States, ranking 24th in life expectancy. More recently, the United States’s life expectancy slipped further, down to 43rd in the world, although the United States spent the most ($3.0 trillion) on health care…”
What is the leading risk factor for death in the United States? As seen below and at 2:04 in my video, it is the standard American diet. Those trillions in health care spending aren’t addressing the root cause of disease, disability, and death.
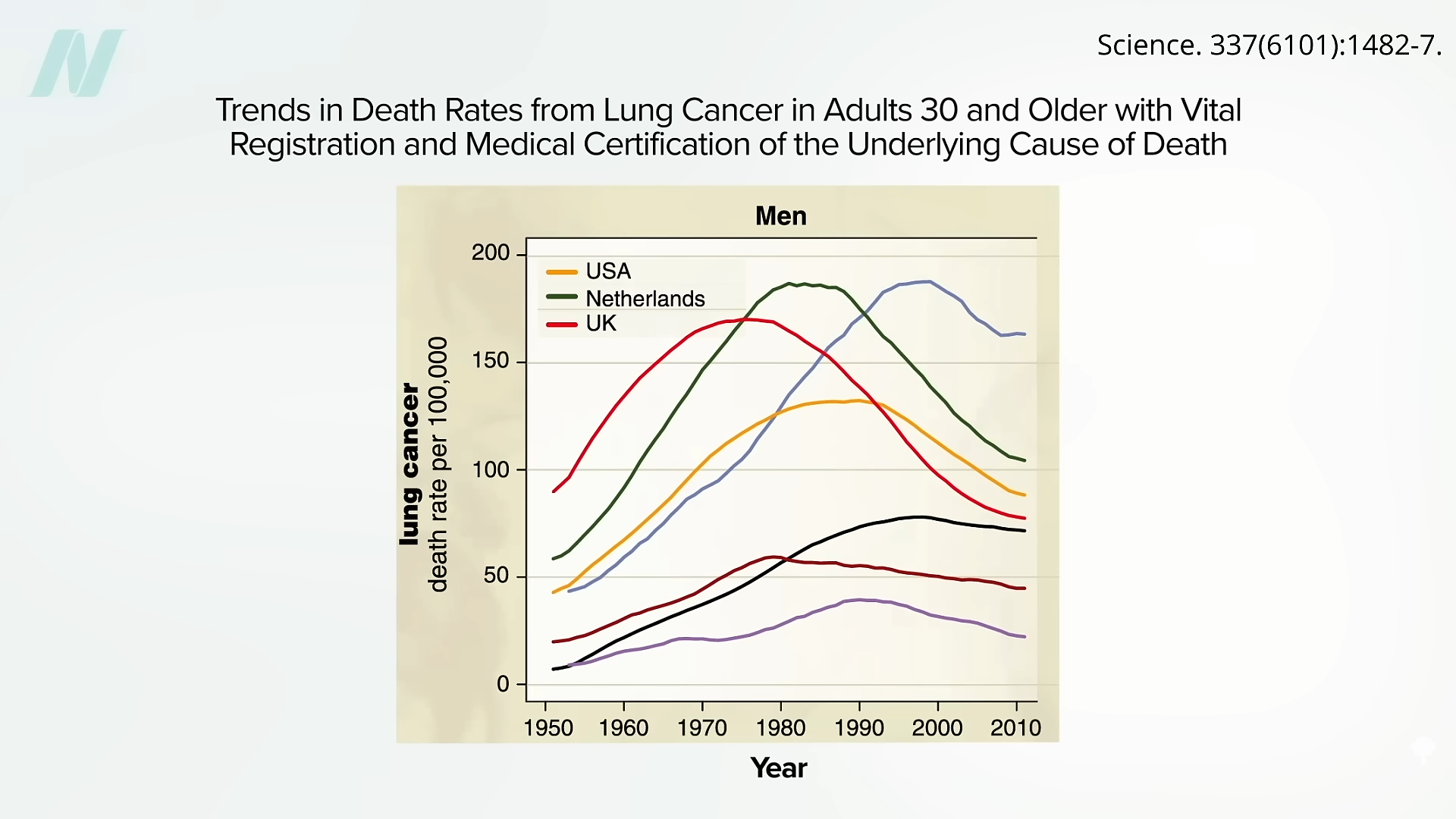
Here are some of the lung cancer death curves, below and at 2:08 in my video:
It took decades to finally turn the corner, but it’s so nice to finally see those drops. When will we see the same with diet?
“Approximately 80% of chronic disease and premature death could be prevented by not smoking, being physically active, and adhering to a healthful dietary pattern.” What exactly is meant by “healthy diet”? “Unfortunately, media messages surrounding nutrition are often inconsistent, confusing, and do not enable the public to make positive changes in health behaviors….Certainly, there is pressure within today’s competitive journalism market for sensationalism. There may even be a disincentive to present the facts in the context of the total body of information consumers need to act on dietary recommendations.” And there’s an incentive to sell more magazines and newspapers. The paper I’m quoting was written in 1997, before the lure of clickbait headlines. In fact, about three-quarters of a century ago, it was noted: “It is unfortunate that the subject of nutrition seems to have a special appeal to the credulous, the social zealot and, in the commercial field, the unscrupulous….The combination is one calculated to strike despair in the hearts of the sober, objective scientist.”
Indeed, the most important health care problem we face may be “our poor lifestyle choices based on misinformation.” It is like the climate change deniers: “Analogous to outspoken cynics denying climate change and influencing public opinion, healthy lifestyle and dietary advice are overshadowed by critics, diet books, the food industry, and misguided information in the media.” Maybe we need an entity like the Intergovernmental Panel on Climate Change (IPCC)—but for nutrition.
These days, “no single expert, regardless of academic stature or reputation, has the prominence to overcome the obstacles created by confusing media messages and deliver the fundamental principles of healthy living effectively to the public.”
What if there were “a global coalition consisting of a variety of nutrition experts, who collectively represent the views held by the majority of scientists, physicians, and health practitioners” that could “serve as the guiding resource of sound nutrition information for improved health and prevention of disease”?
Enter the True Health Initiative, which “was conceived for that very purpose.” A nonprofit coalition of hundreds of experts from dozens of countries has agreed to a consensus statement on the fundamentals of healthy living. See www.truehealthinitiative.org.
Spoiler alert: The healthiest diet is one generally comprised mostly of minimally processed plants.
Women with breast cancer should include the “liberal culinary use of cruciferous vegetables.”
Both the Women’s Intervention Nutrition Study and the Women’s Health Initiative study showed that women randomized to a lower-fat diet enjoyed improved breast cancer survival. However, in the Women’s Healthy Eating and Living Study, women with breast cancer were also randomized to drop their fat intake down to 15 to 20 percent of calories, yet there was no difference in breast cancer relapse or death after seven years.
Any time there’s an unexpected result, you must question whether the participants actually followed through with study instructions. For instance, if you randomized people to stop smoking and they ended up with the same lung cancer rates as those in the group who weren’t instructed to quit, one likely explanation is that the group told to stop smoking didn’t actually stop. In the Women’s Healthy Eating and Living Study, both the dietary intervention group and the control group started out at about 30 percent of calories from fat. Then, the diet group was told to lower their fat intake to 15 to 20 percent of calories. By the end of the study, they had in fact gone from 28.5 percent fat to 28.9 percent fat, as you can see below and at 1:16 in my video The Food That Can Downregulate a Metastatic Cancer Gene. They didn’t even reduce their fat intake. No wonder they didn’t experience any breast cancer benefit.
When you put together all the trials on the effect of lower-fat diets on breast cancer survival, even including that flawed study, you see a reduced risk of breast cancer relapse and a reduced risk of death. In conclusion, going on a low-fat diet after a breast cancer diagnosis “can improve breast cancer survival by reducing the risk of recurrence.” We may now know why: by targeting metastasis-initiating cancer cells through the fat receptor CD36.
We know that the cancer-spreading receptor is upregulated by saturated fat. Is there anything in our diet that can downregulate it? Broccoli.
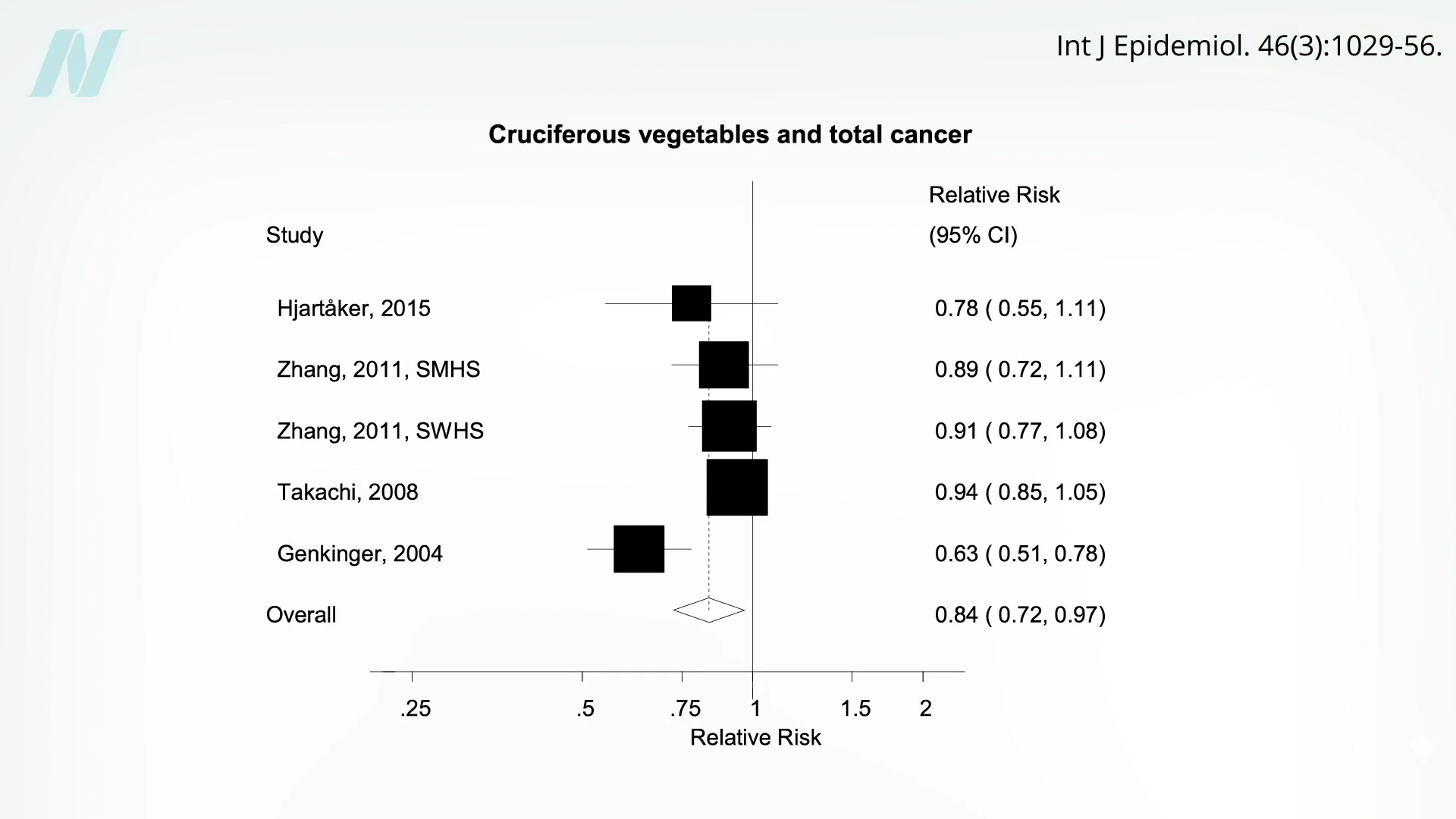
Broccoli appears to decrease CD36 expression by as much as 35 percent (in mice). Of all fruits and vegetables, cruciferous vegetables like broccoli were the only ones associated with significantly less total risk of cancer and not just getting cancer in the first place, as you can see here and at 2:19 in my video.
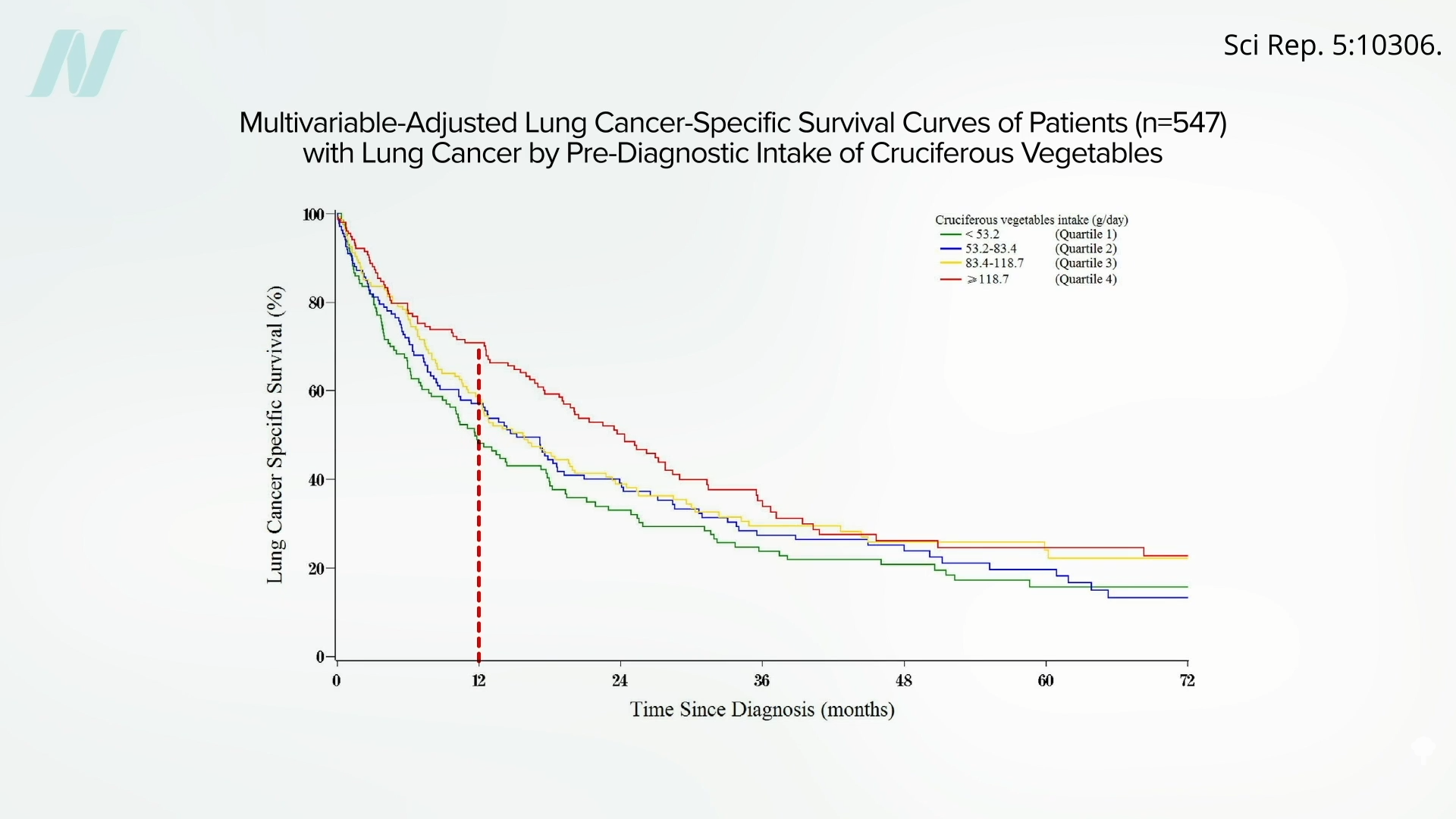
Those with bladder cancer who eat broccoli also appear to live longer than those who don’t, and those with lung cancer who eat more cruciferous veggies appear to survive longer, too.
For example, as you can see below and at 2:45 in my video, one year out, about 75 percent of lung cancer patients eating more than one serving of cruciferous vegetables a day were still alive (the top line in red), whereas, by then, most who had been getting less than half a serving a day had already died from their cancer (the bottom line in green).
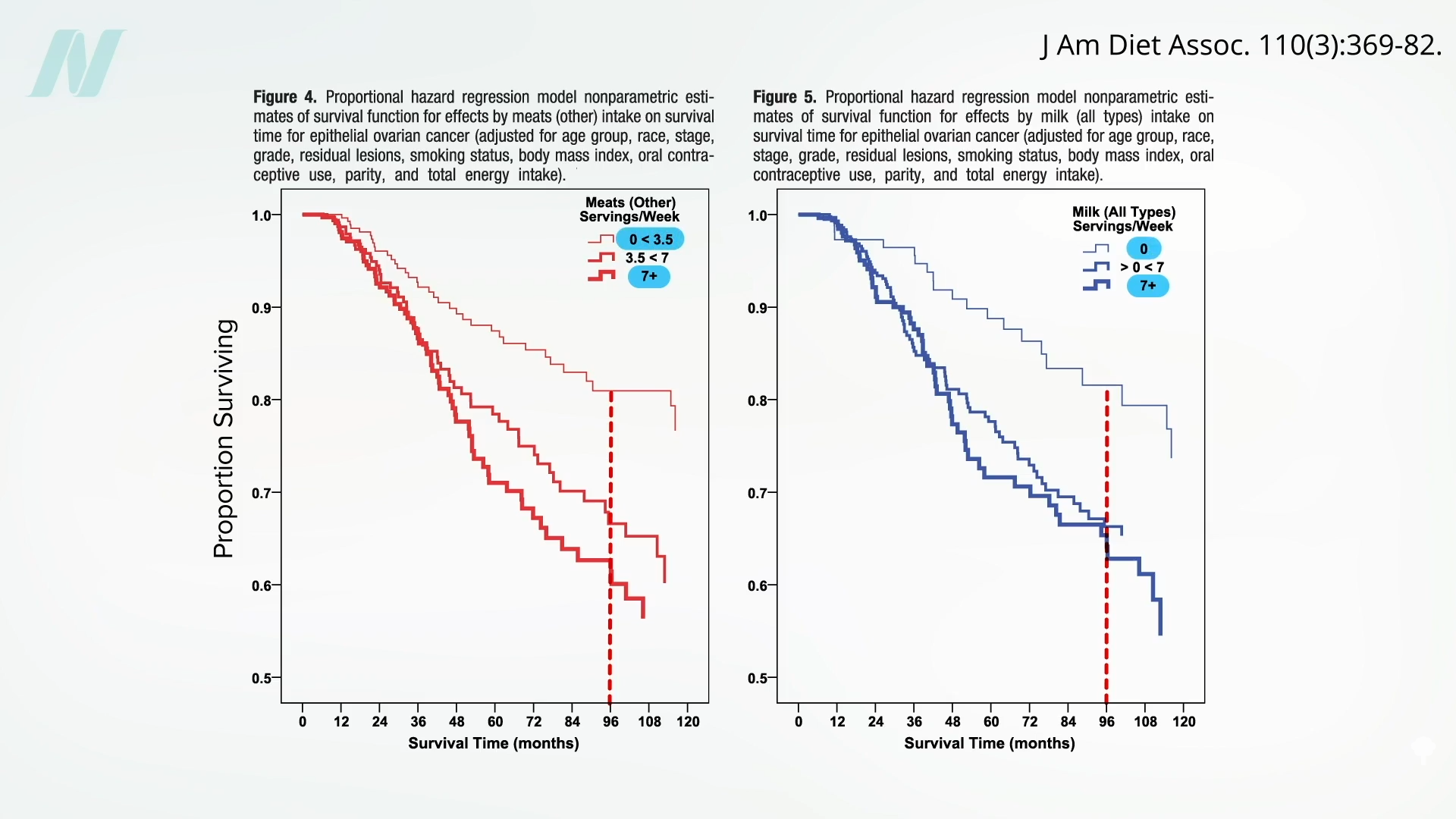
Ovarian cancer, too. Intake of cruciferous vegetables “significantly favored survival,” whereas “a survival disadvantage was shown for meats.” Milk also appeared to double the risk of dying. Below and at 3:21 in my video are the survival graphs. Eight years out, about 40 percent of ovarian cancer patients who averaged meat or milk every day were deceased (the boldest line, on the bottom), compared to only about 20 percent who had meat or milk only a few times a week at most (the faintest line, on the top).
Now, it could be that the fat and cholesterol in meat increased circulating estrogen levels, or it could be because of meat’s growth hormones or all its carcinogens. And galactose, the sugar naturally found in milk, may be directly toxic to the ovary. Dairy has all its hormones, too. However, the lowering of risk with broccoli and the increasing of risk with meat and dairy are also consistent with the CD36 mechanism of cancer spread.
Researchers put it to the test in patients with advanced pancreatic cancer who were given pulverized broccoli sprouts or a placebo. The average death rate was lower in the broccoli sprout group compared to the placebo group. After a month, 18 percent of the placebo group had died, but none in the broccoli group. By three months, another 25 percent of the placebo group had died, but still not a single death in the broccoli group. And by six months, 43 percent of the remaining patients in the placebo group were deceased, along with the first 25 percent of the broccoli group. Unfortunately, even though the capsules for both groups looked the same, “true blinding was not possible,” and the patients knew which group they were in “because the pulverized broccoli sprouts could be easily distinguished from the methylcellulose [placebo] through their characteristic smell and taste.” So, we can’t discount the placebo effect. What’s more, the study participants weren’t properly randomized “because many of the patients refused to participate unless they were placed into the [active] treatment group.” That’s understandable, but it makes for a less rigorous result. A little broccoli can’t hurt, though, and it may help. It’s the lack of downsides of broccoli consumption that leads to “Advising Women Undergoing Treatment for Breast Cancer” to include the “liberal culinary use of cruciferous vegetables,” for example.
It’s the same for reducing saturated fat. The title of an editorial in a journal of the National Cancer Institute asked: “Is It Time to Give Breast Cancer Patients a Prescription for a Low-Fat Diet?” “Although counseling women to consume a healthy diet after breast cancer diagnosis is certainly warranted for general health, the existing data still fall a bit short of proving this will help reduce the risk of breast cancer recurrence and mortality.” But what do we have to lose? After all, it’s still certainly warranted for general health.
For the last five years, Vicky Ni has been battling lung cancer — a diagnosis that came out of the blue in 2019 after she went to a doctor for pain in her shoulder.
“He was taking X-rays of my neck, and it was only by chance that the bottom corner of the X-ray showed a raised diaphragm,” Ni said. “I was stunned beyond words.”
The 54-year-old lawyer and mother of two is now part of a medical mystery: lung cancer in nonsmoking, Asian American women had been rising for more than a decade before Ni received her diagnosis.
“I assumed that I would get chemo and beat it. It was only later when I met with an oncologist that I learned that I was stage 4 and therefore incurable,” Ni said.
Of the Asian women diagnosed with lung cancer, 57% are nonsmokers, according to a study by leading California medical centers. For all others, only 15% of the women diagnosed had no history of smoking.
Ni says she doesn’t believe she was exposed to any cancer-causing chemicals and didn’t grow up in an area with a lot of air pollution. As a nonsmoker, she wasn’t eligible to be screened for lung cancer.
“Currently, screening guidelines drive what’s covered under insurance,” said epidemiologist Scarlett Gomez.
Gomez and epidemiologist Iona Cheng of the University of California San Francisco were awarded a $12.5 million grant from the National Cancer Institute.
“Some of the factors we’re looking at include certainly exposure to second-hand smoke, high exposure to cooking oil fumes is an established risk factor,” Gomez said, adding that recent cellular studies suggest that a particular genetic mutation may predispose people to being more vulnerable to air pollution.
At New York University’s Perlmutter Cancer Center, Dr. Elaine Shum is randomly screening 1,000 Asian women for free.
“We are definitely going to need a much larger study to really provide the evidence to try to change the guidelines one day, so that other populations can be offered low-dose CT scans by insurance companies,” Shum said.
Potentially changing the guidelines for earlier detection won’t affect the outcome for Ni and her husband David. “Like any cancer, it affects the whole family,” David said.
But it could offer hope to spare other families that same pain in the future.
Less than a month after arriving at KPIX 5 as the 5pm co-anchor and night-side reporter, Elizabeth Cook was in San Francisco’s Mission District covering a chaotic Occupy march when a protester shoved her and her cameraman. With only moments to spare, the team got to safety and filed their report for the 11 pm news.
Might animal protein-induced increases in the cancer-promoting growth hormone IGF-1 help promote brain artery integrity?
In 2014, a study on stroke risk and dietary protein found that greater intake was associated with lower stroke risk and, further, that the animal protein appeared particularly protective. Might that help explain why, as shown in the graph below and at 0:31 in my video Vegetarians and Stroke Risk Factors: Animal Protein?, vegetarians were recently found to have a higher stroke rate than meat eaters?
Animal protein consumption increases the levels of a cancer-promoting growth hormone in the body known as IGF-1, insulin-like growth factor 1, which “accelerates the progression of precancerous changes to invasive lesions.” High blood concentrations are associated with increased risks of breast, colorectal, lung, and prostate cancers, potentially explaining the association between dairy milk intake and prostate cancer risk, for example. However, there are also IGF-1 receptors on blood vessels, so perhaps IGF-1 promotes cancer and brain artery integrity.
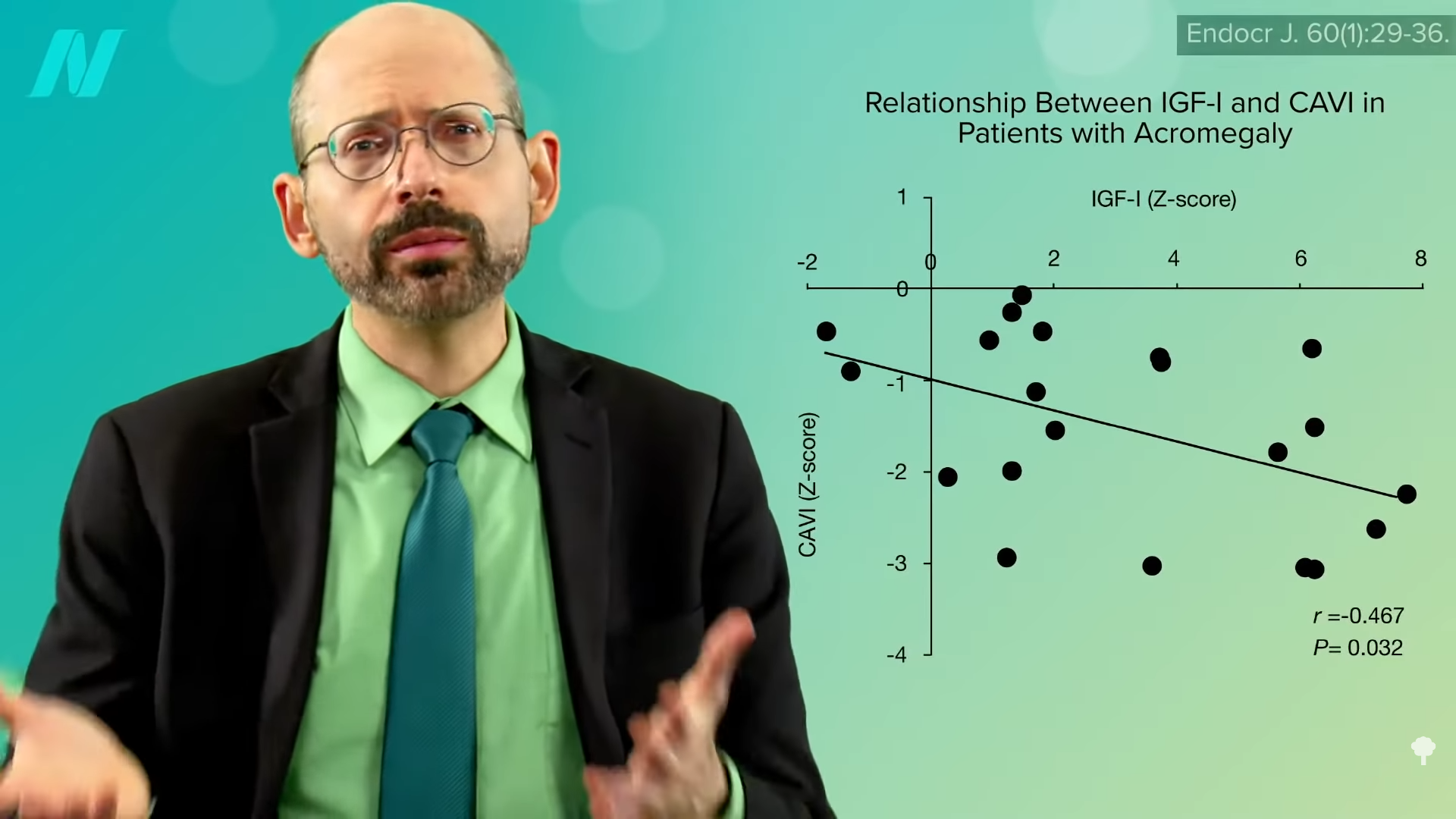
People who have strokes appear to have lower blood levels of IGF-1, but it could just be a consequence of the stroke rather than the cause. There weren’t any prospective studies over time until 2017 when researchers found that, indeed, higher IGF-1 levels were linked to a lower risk of stroke—but is it cause and effect? In mice, the answer seems to be yes, and in a petri dish, IGF-1 appears to boost the production of elastin, a stretchy protein that helps keep our arteries elastic. As you can see in the graph below and at 1:41 in my video, higher IGF-1 levels are associated with less artery stiffness, but people with acromegaly, like Andre the Giant, those with excessive levels of growth hormones like IGF-1, do not appear to have lower stroke rates, and a more recent study of dietary protein intake and risk of stroke that looked at a dozen studies of more than half a million people (compared to only seven studies with a quarter million in the previous analysis), found no association between dietary protein intake and the risk of stroke. If anything, dietary plant protein intake may decrease the risk of stroke.
However, those with high blood pressure who have low IGF-1 levels do appear to be at increased risk of developing atherosclerosis, which is the thickening of the artery walls leading up to the brain, but no such association was found in people with normal blood pressure. So, there may be “a cautionary lesson for vegans” here. Yes, a whole food, plant-based diet “can down-regulate IGF-1 activity” and may slow the human aging process, not to mention reduce the risk of some of the common cancers that plague the Western world. But, “perhaps the ‘take-home’ lesson should be that people who undertake to down-regulate IGF-1 activity [by cutting down on animal protein intake] as a pro-longevity measure should take particular care to control their blood pressure and preserve their cerebrovascular health [the health of the arteries in their brain] – in particular, they should keep salt intake relatively low while insuring an ample intake of potassium” to keep their blood pressures down. So, that means avoiding processed foods and avoiding added salt, and, in terms of potassium-rich foods, eating beans, sweet potatoes, and dark-green leafy vegetables.
Might this explain the higher stroke risk found among vegetarians? No—because dairy and egg whites are animal proteins, too. Only vegans have lower IGF-1 levels in both men and women, so low levels of IGF-1 can’t explain why higher rates of stroke were found in vegetarians. Then what is it? I think the best explanation for the mystery is something called homocysteine, which I cover next.
Beyond eating a plant-based diet, how else can we lower our blood pressure? Check out the chapter of hypertension in my book How Not to Die at your local public library.
This is the eighth video in a 12-part series on vegetarians’ stroke risk. If you missed any of the previous ones, check out the related posts below.
Coming up, we turn to what I think is actually going on:
Susan Wojcicki, the former YouTube chief executive officer and longtime Google executive, has died, her husband said. She was 56.
“My beloved wife of 26 years and mother to our five children left us today after 2 years of living with non small cell lung cancer,” Dennis Troper said in a social media post late Friday.
“Susan was not just my best friend and partner in life, but a brilliant mind, a loving mother, and a dear friend to many,” Troper said.
No other details of her death were immediately provided.
Wojcicki, who played a key role in Google’s creation, stepped down as YouTube’s CEO in 2023 after spending nine years running the video-sharing service that reshaped entertainment, culture and politics.
Shortly after Google co-founders Larry Page and Sergey Brin incorporated their search engine into a business in 1998, Wojcicki rented the garage of her Menlo Park, California, home to them for $1,700 a month.
Wojcicki and Troper’s 19-year-old son, Marco Troper, died in February at the UC Berkeley campus where he resided as a freshman student.
Here is a review of reviews on the health effects of tea, coffee, milk, wine, and soda.
If you’ve watched my videos or read my books, you’ve heard me say, time and again, the best available balance of evidence. What does that mean? When making decisions as life-or-death important as what to feed ourselves and our families, it matters less what a single study says, but rather what the totality of peer-reviewed science has to say.
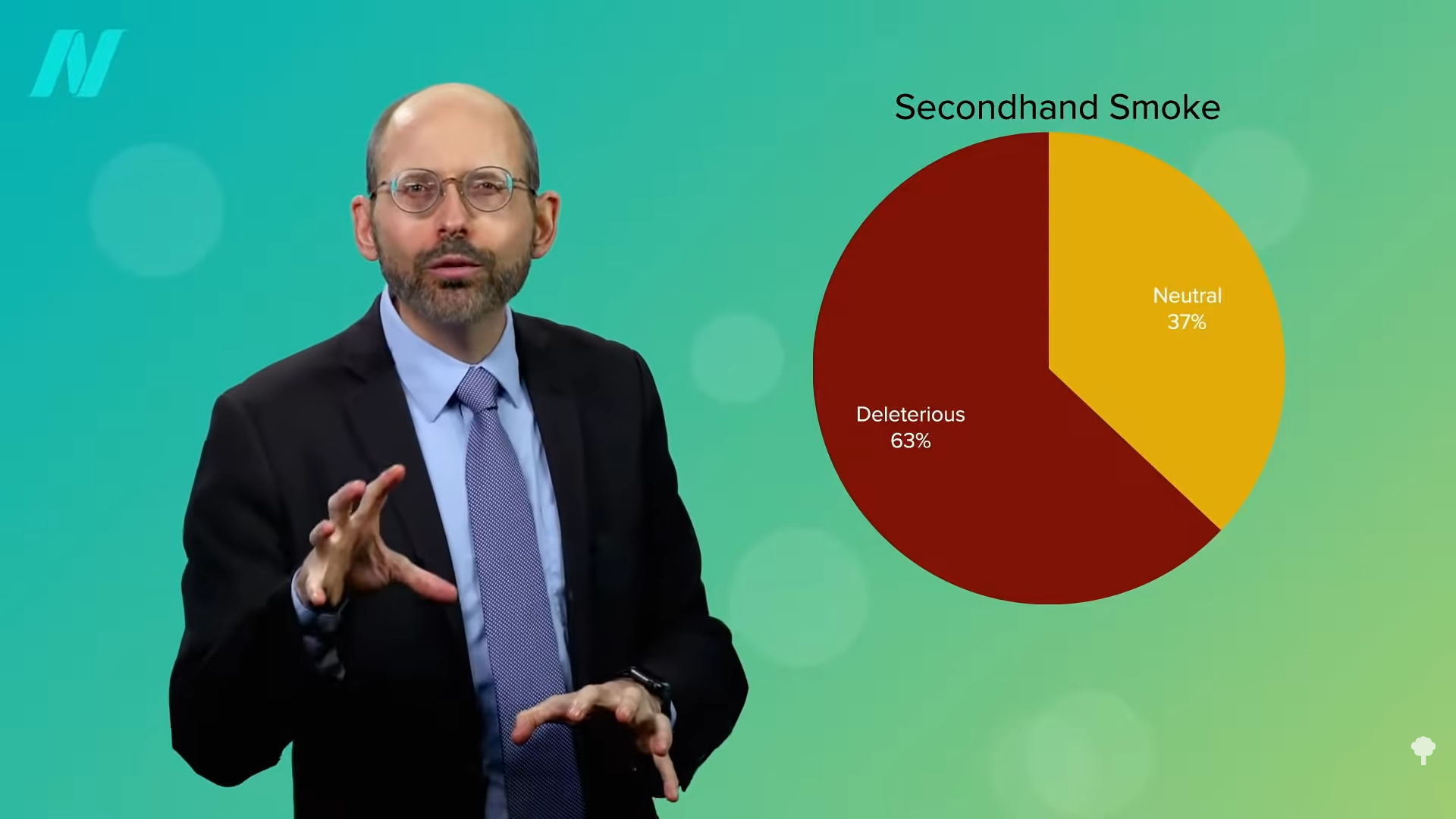
Individual studies can lead to headlines like “Study Finds No Link Between Secondhand Smoke and Cancer,” but to know if there is a link between secondhand smoke and lung cancer, it would be better to look at a review or meta-analysis that compiles multiple studies. The problem is that some reviews say one thing—for instance, “breathing other people’s tobacco smoke is a cause of lung cancer”—and other reviews say another—such as, the effects of secondhand smoke are insignificant and further such talk may “foster irrational fears.” And, while we’re at it, you can indulge in “active smoking of some 4-5 cigarettes per day” without really worrying about it, so light up!
Why do review articles on the health effects of secondhand smoke reach such different conclusions? As you can imagine, about 90 percent of reviews written by researchers affiliated with the tobacco industry said it was not harmful, whereas you get the opposite number with independent reviews, as you can see below and at 1:18 in my video Friday Favorites: What Are the Best Beverages?. Reviews written by the tobacco industry–affiliated researchers had 88 times the odds of concluding that secondhand smoke was harmless. It was all part of “a deliberate strategy to use scientific consultants to discredit the science…” In other words, “the strategic and long run antidote to the passive smoking issue…is developing and widely publicizing clear-cut, credible, medical evidence that passive smoking [secondhand smoke] is not harmful to the non-smoker’s health.”
Can’t we just stick to the independent reviews? The problem is that industry-funded researchers have all sorts of sneaky ways to get out of declaring conflicts of interest, so it can be hard to follow the money. For instance, it was found that “77% failed to disclose the sources of funding” for their research. But, even without knowing who funded what, the majority of reviews still concluded that secondhand smoke was harmful. So, just as a single study may not be as helpful as looking at a compilation of studies on a topic, a single review may not be as useful as a compilation of reviews. In that case, looking at a review of reviews can give us a better sense of where the best available balance of evidence may lie. When it comes to secondhand smoke, it’s probably best not to inhale, as you can see in the graph below and at 2:30 in my video.
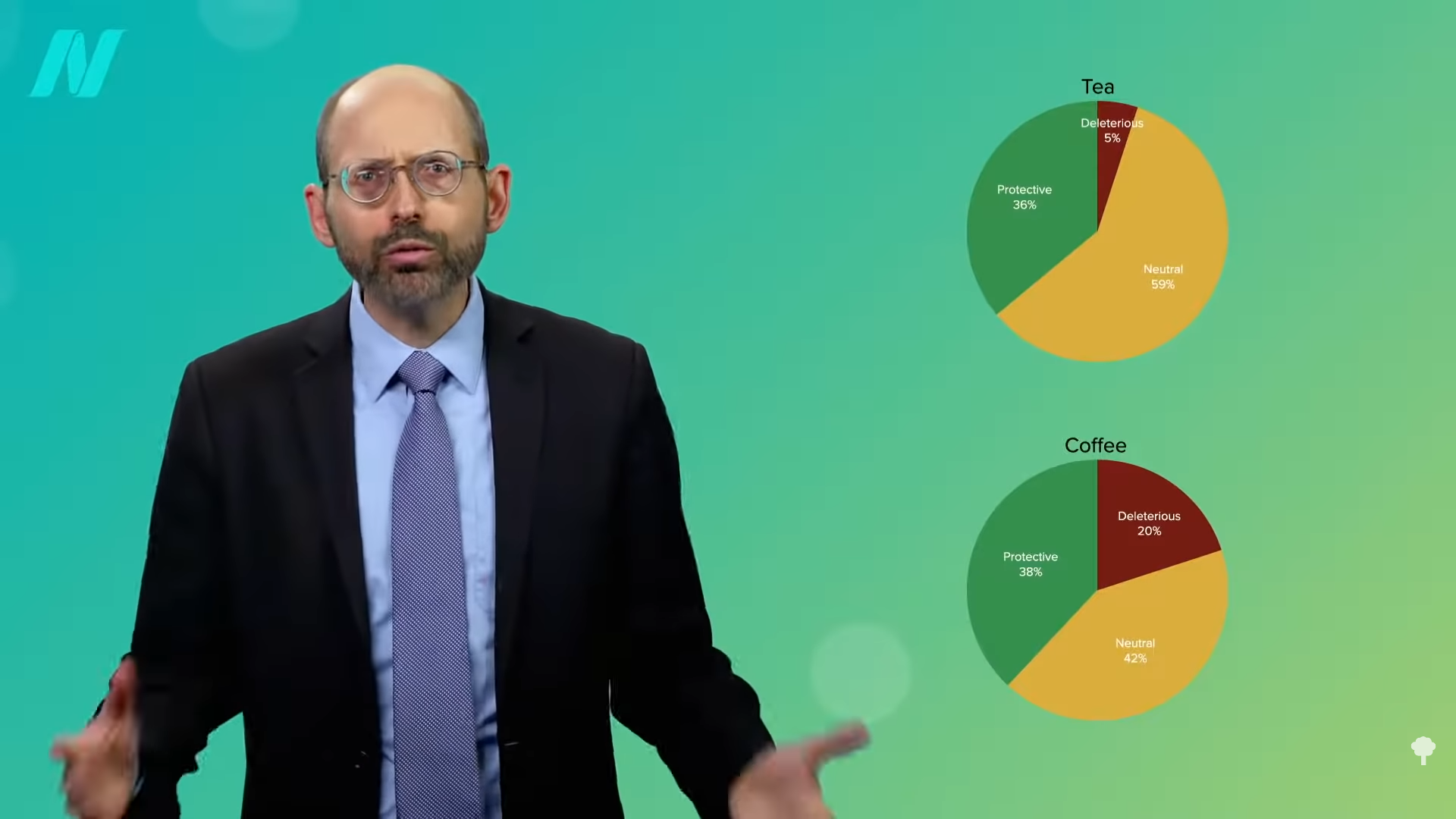
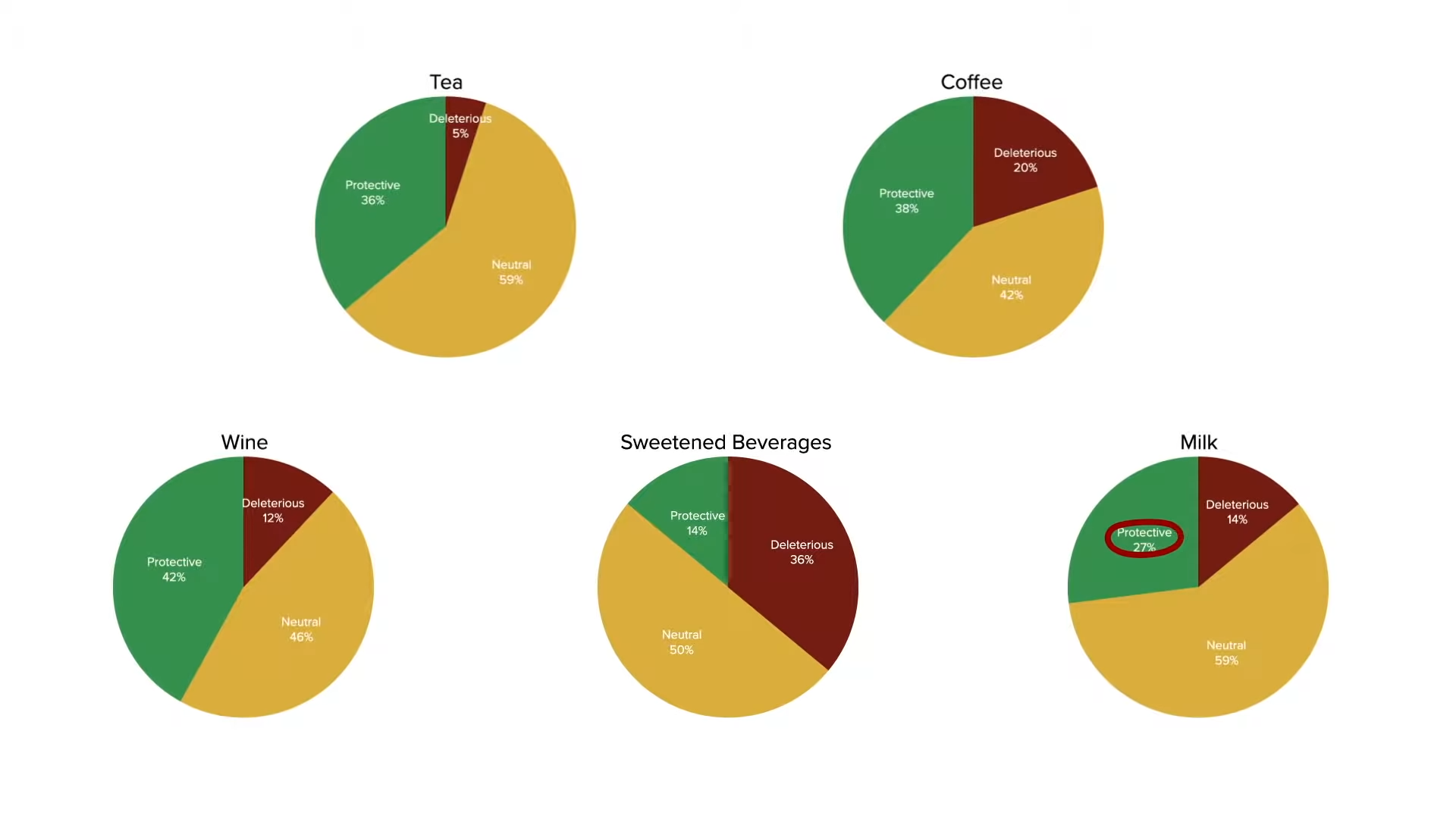
Wouldn’t it be cool if there were reviews of reviews for different foods and drinks? Voila! Enter “Associations Between Food and Beverage Groups and Major Diet-Related Chronic Diseases: An Exhaustive Review of Pooled/Meta-Analyses and Systematic Reviews.” Let’s start with the drinks. As you can see below and at 2:51 in my video, the findings were classified into three categories: protective, neutral, or deleterious.
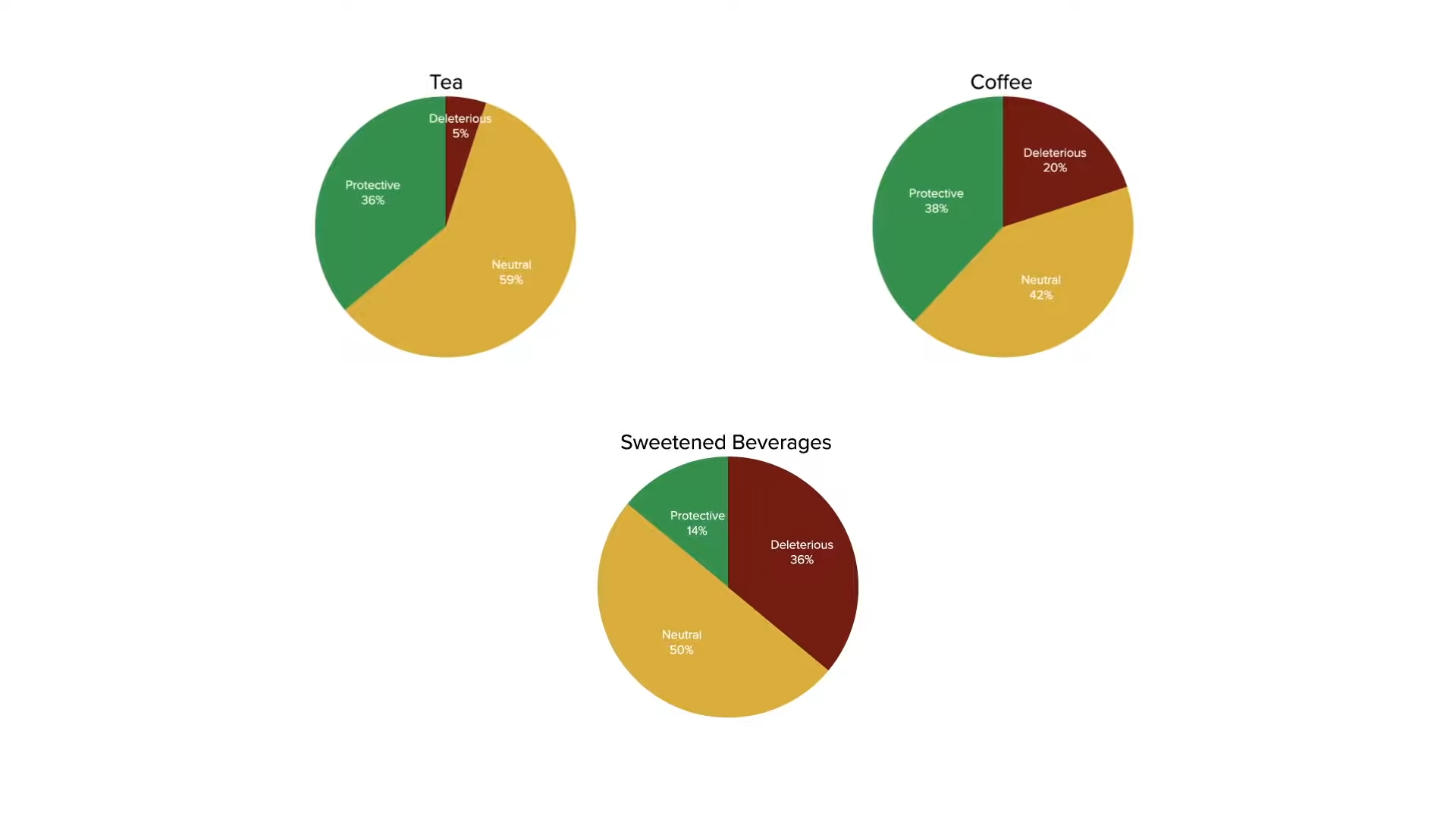
First up: tea versus coffee. As you can see in the graph below and at 2:58, most reviews found both beverages to be protective for whichever condition they were studying, but you can see how this supports my recommendation for tea over coffee. Every cup of coffee is a lost opportunity to drink a cup of green tea, which is even healthier.
It’s no surprise that soda sinks to the bottom, as you can see below and at 3:20 in my video, but 14 percent of reviews mentioned the protective effects of drinking soda. What?! Well, most were references to papers like “High Intake of Added Sugar Among Norwegian Children and Adolescents,” a cross-sectional study that found that eighth-grade girls who drank more soda were thinner than girls who drank less. Okay, but that was just a snapshot in time. What do you think is more likely? That the heavier girls were heavier because they drank less soda, or that they drank less sugary soda because they were heavier? Soda abstention may therefore be a consequence of obesity, rather than a cause, yet it gets marked down as having a protective association.
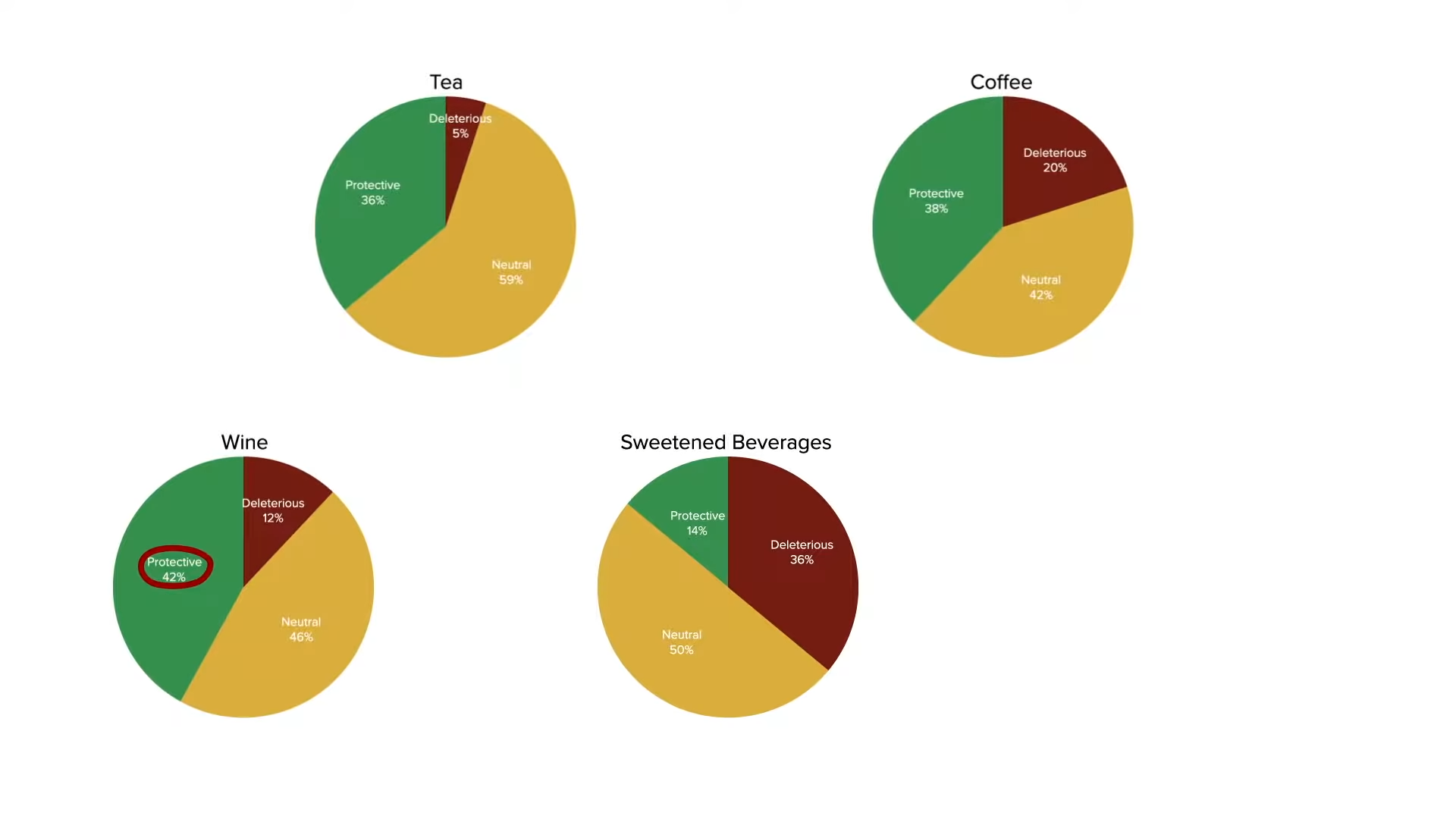
Study design flaws may also account for wine numbers, as seen below and at 4:07 in my video. This review of reviews was published in 2014, before the revolution in our understanding of “alcohol’s evaporating health benefits,” suggesting that the “presumed health benefits from ‘moderate’ alcohol use [may have] finally collapsed”—thanks in part to a systematic error of misclassifying former drinkers as if they were lifelong abstainers, as I revealed in a deep dive in a video series on the subject.
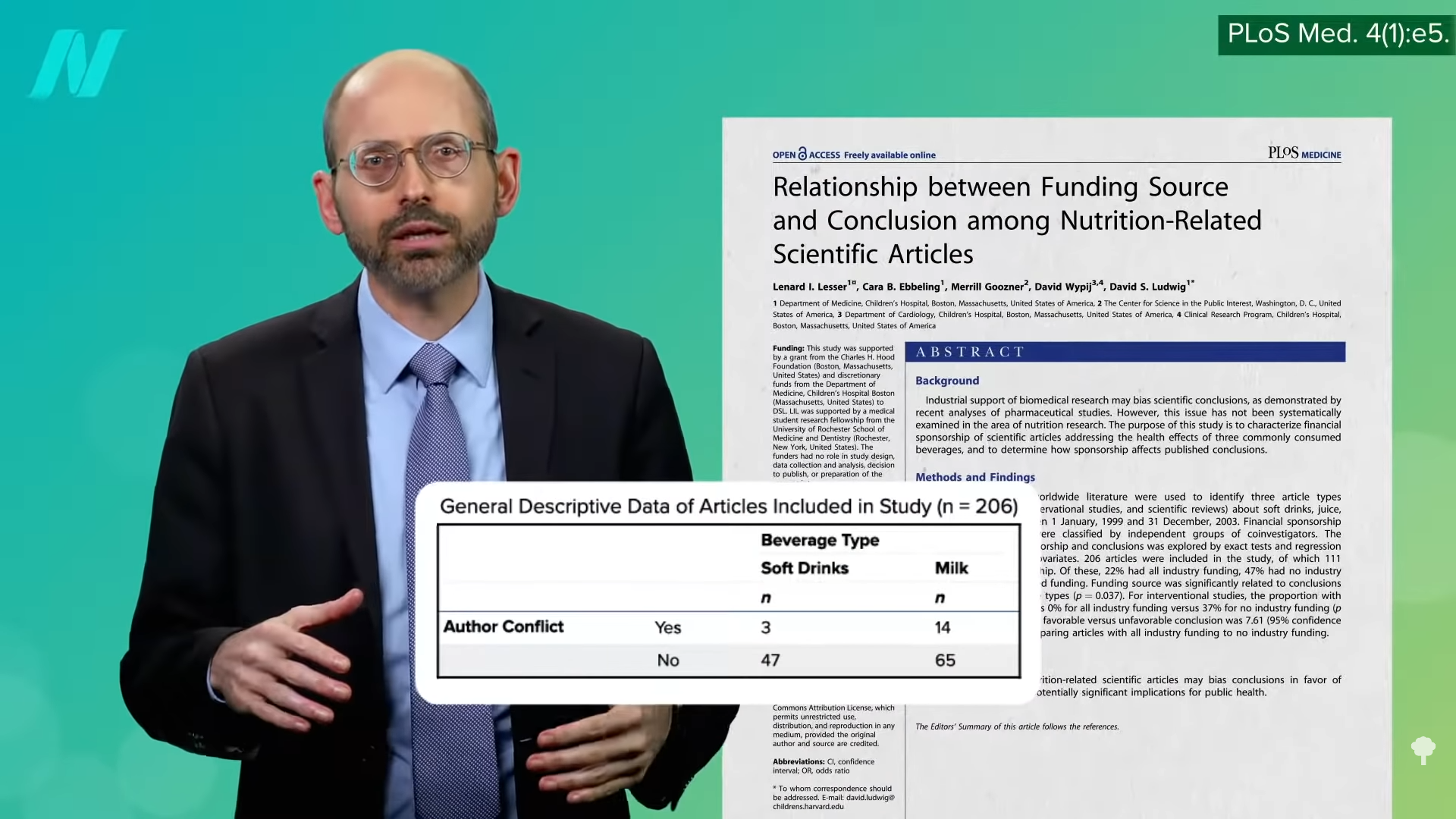
Sometimes there are unexplainable associations. For example, one of the soft drink studies found that increased soda consumption was associated with a lower risk of certain types of esophageal cancers. Don’t tell me. Was the study funded by Coca-Cola? Indeed. Does that help explain the positive milk studies, as you can see in the graph below and at 5:02 in my video? Were they all just funded by the National Dairy Council?
As shown below and at 5:06, even more conflicts of interest have been found among milk studies than soda studies, with industry-funded studies of all such beverages “approximately four to eight times more likely to be favorable to the financial interests of the [study] sponsors than articles without industry-related funding.”
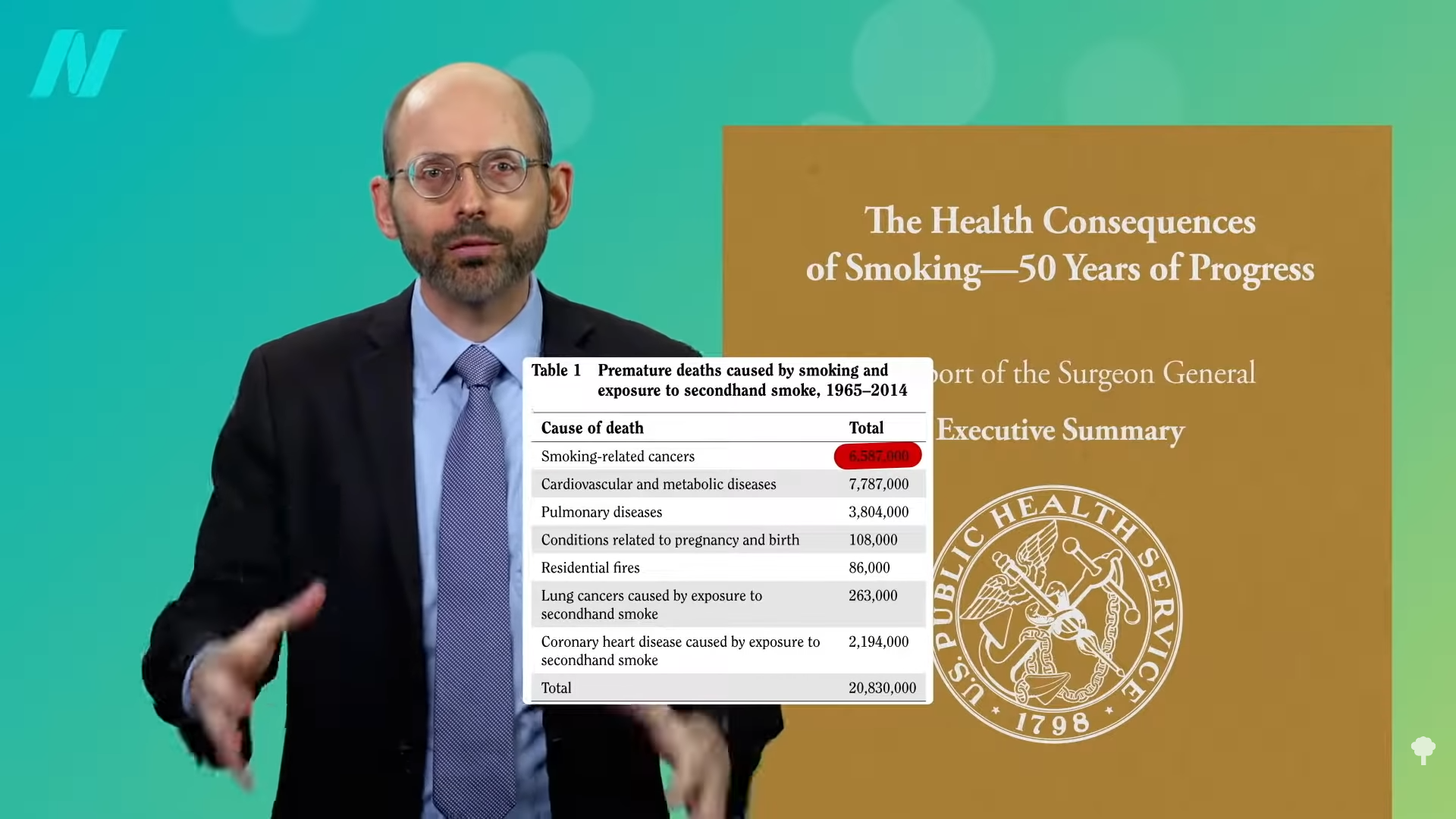
Funding bias aside, though, there could be legitimate reasons for the protective effects associated with milk consumption. After all, those who drink more milk may drink less soda, which is even worse, so they may come out ahead. It may be more than just relative benefits, though. The soda-cancer link seems a little tenuous and not just because of the study’s financial connection to The Coca-Cola Company. It’s hard to imagine a biologically plausible mechanism, whereas even something as universally condemned as tobacco isn’t universally bad. As I’ve explored before, more than 50 studies have consistently found a protective association between nicotine and Parkinson’s disease. Even secondhand smoke may be protective. Of course, you’d still want to avoid it. Passive secondhand smoke may decrease the risk of Parkinson’s, but it increases the risk of stroke, an even deadlier brain disease, not to mention lung cancer and heart disease, which has killed off millions of Americans since the first Surgeon General’s report was released, as you can see below and at 6:20 in my video.
Thankfully, by eating certain vegetables, we may be able to get some of the benefits without the risks, and the same may be true of dairy. As I’ve described before, the consumption of milk is associated with an increased risk of prostate cancer, leading to recommendations suggesting that men may want to cut down or minimize their intake, but milk consumption is also associated with decreased colorectal cancer risk. This appears to be a calcium effect. Thankfully, we may be able to get the best of both worlds by eating high-calcium plant foods, such as greens and beans.
What does our review-of-reviews study conclude about such plant-based foods, in comparison to animal-based foods? We’ll find out next.
Stay tuned for the exhaustive review of meta-analyses and systematic reviews on major diet-related chronic diseases found for food groups in What Are the Best Foods?.
In Kathy Griffin’s life, there are no sacred cows. Since starting her career in the 1980s, the two-time Emmy and Grammy Award-winning comedian has fearlessly taken on celebrities, Hollywood, her family, herself and (perhaps, most famously) fellow reality TV star-turned-President Donald Trump…
In a twist of irony, a powerful drug that battles lung cancer might be delivered safer via inhalation versus surgery, injection, and other invasive methods, a new study suggests.
Researchers associated with Columbia University observed rat models and determined that a new inhalable lung cancer treatment is capable of delivering localized immunotherapy to difficult-to-treat tumors.
Lately researchers have been looking for a safe and non-invasive alternative to current approaches to tackling cancerous tumors that require direct injection of immunomodulators into the tumors. But when cancer is found in the lungs, it is typically hard to reach and treat with drugs by direct injection.
Researchers believe that a potent drug that fights cancer might be better delivered via inhalation in order to battle lung cancer. The study was published recently in Nature Nanotechnology and online Jan. 11, showing how nanobubbles containing a powerful drug could be administered via inhalation to provide a safer delivery route.
Medscapereports that researchers demonstrated that nanobubbles can deliver potent immunotherapy directly to tough-to-treat lung cancer tumors via inhalation. Researchers suspect that exosomes, also known as extracellular vesicles (EVs), could be the key to the next step in lung cancer treatment.
“Exosomes work like text messages between cells , sending and receiving information,” said lead researcher Ke Cheng, PhD, professor of biomedical engineering at Columbia, who has been working with stem cells and exosomes for over 15 years. “The significance of this study is that exosomes can bring mRNA-based treatment to lung cancer cells locally, unlike systemic chemotherapy that can have side effects throughout the body. And inhalation is totally noninvasive. You don’t need a nurse to use an IV needle to pierce your skin.”
The study could help move research forward by allowing for the therapeutic uses of exosomes, inhalable treatments for lung conditions, and the safe delivery of powerful interleukin-12 (IL-12) immunotherapy.
Researchers have known about IL-12’s abilities to fight cancer for decades, but early human trials lead to serious side effects and several deaths. Researchers are now trying new delivery methods that target tumor cells without affecting healthy tissue. The research team’s new approach involves inserting mRNA for IL-12 into exosomes.
“One of the advantages of exosomes is that they are naturally secreted by the body or cultured cells,” he noted. “They have low toxicity and have multiple ways of getting their message into cells.”
The scientists borrowed an approach that captured public attention during the pandemic: Using messenger RNA, which directs cells to make proteins for tasks — including boosting immune response.
In the study, researchers developed inhalable extracellular vesicles loaded with IL-12 mRNA to battle lung cancer and bolster systemic immunity in mice with tumors. IL-12 mRNA was loaded into human embryonic kidney cell-derived exosomes (HEK-Exo) through electroporation, yielding IL-12 mRNA-loaded exosomes (IL-12-Exo).
When inhaled by mice with lung tumors, IL-12-Exo outperformed IL-12 mRNA-loaded liposomes (IL-12-Lipo)n and minimized systemic toxicity. These inhaled IL-12-Exo promoted
immune activation, systemic immunity, and immune memory, culminating in lung tumor suppression and heightened resistance against tumor recurrences.
Lung Cancer and Smoking
Human trials could launch within five years, and help put an end to the devastation that lung cancer causes each year.
Lung cancer is the leading cause of cancer death overall and among both men and women. (The second leading cause of cancer death is prostate for men and breast for women.) In 2021, 134,592 people died from lung cancer, or 22% of all cancer deaths. In the United States, cigarette smoking is linked to about 80% to 90% of lung cancer deaths.
However, even the Lung Cancer Society notes that while it is not risk-free as it involves combustion, cannabis smoke is not as carcinogenic as tobacco smoke. NORML explains this very well: THC and CBD, the two most popular cannabis active ingredients, are non-carcinogenic and demonstrate anticancer properties in vivo and in vitro. Nicotine—in stark contrast—promotes the development of cancer cells and their blood supply. In addition, cannabinoids stimulate other biological activities and responses that may mitigate the carcinogenic effects of smoke.
People who smoke cigarettes are 15 to 30 times more likely to develop lung cancer or die from lung cancer than people who do not smoke. Even smoking a few cigarettes a day or on occasion increases the risk of lung cancer.
Even if you don’t smoke anything, or only vape, you’re still not off the hook, depending on how hazardous areas are that you live in.
People also get lung cancer from radon, and they usually have no control over the undetectable radioactive gas caused by the natural decay of traces in uranium in rocks and the soil. The U.S. Environmental Protection Agency (EPA) estimates that radon causes about 21,000 lung cancer deaths each year.
One of the most important reasons for the recent improvements in lung cancer treatments is biomarker testing — testing to determine the exact kind of cancer a patient has, in order to enable the most personalized treatment possible.
This page contains a video which is being blocked by your ad blocker. In order to view the video you must disable your ad blocker.
‘Close doesn’t count:’ Biomarker testing crucial for modern lung cancer treatment
One of the most important reasons for the recent improvements in lung cancer treatments is biomarker testing — testing to determine the exact kind of cancer a patient has, in order to enable the most personalized treatment possible.
For many patients, a lung cancer diagnosis comes as a surprise. Lung cancer remains the most deadly form of cancer, according to the National Cancer Institute.
Yet, in the past two decades, Dr. Stephen Liu, director of Thoracic Oncology and Developmental Therapeutics at Georgetown University’s Lombardi Cancer Center, said knowing as much as possible about a patient’s specific cancer can greatly affect treatment’s effectiveness.
“Within lung cancer, there are dozens of different types of cancer,” Liu said. “And we now have personalized treatments that are tailored to those types of cancers.”
Lung cancer biomarker testing, which is also known as tumor testing, genetic mutation testing, next-generation sequencing (NGS) or genomic testing, looks for changes in the DNA of tumor cells.
“And it is absolutely essential in choosing the right therapy,” said Liu, since a growing number of mutations have targeted therapies available.”
“These tend to be oral medications, taken once or twice a day, and while they have their share of side effects, they’re generally and consistently, much better tolerated than chemotherapy,” which affects both cancerous and healthy tissue.
Liu, who co-hosts the “Lung Cancer Considered” podcast that is produced by the International Association for the Study of Lung Cancer (IASLC), said the effectiveness of targeted therapy is dramatic.
“More effective than chemotherapy, we can see immediate responses, sometimes within days, but only if we get it right” through biomarker testing, Liu said. “Close doesn’t count. We need to match this perfectly.”
Often, biomarker testing doesn’t begin until after a patient has been diagnosed with lung cancer, which coincides with CT scans and brain MRIs, to determine whether the newly diagnosed cancer had already spread.
Liu said it is important for an oncology team to gather all test results before beginning treatment.
“It’s very common for there to be this urgency to begin therapy — completely understandable,” said Liu. “You get the sense that this cancer has some momentum, and you want to start treatment, yesterday.”
While waiting for test results can be frustrating for a newly-diagnosed patient, Liu said biomarker testing is important.
“I’m not looking for the fastest treatment,” Liu said. “We’re looking for the right treatment.”
Despite the importance of biomarker testing, Liu said surveys show a surprising number of doctors, even oncologists, aren’t aware of its value.
“I think we’ve moved past this paternalistic era, where the doctor knows everything,” Liu said. “In oncology, even within the world of lung cancer, things move at a pace we’ve never seen before.”
Still, given the dramatic improvements in the effectiveness and relatively gentle side effects of targeted therapy, and its reliance on biomarker testing, Liu hopes patients will feel empowered to ensure they’re tested.
“There’s no harm at all in asking your doctor, ‘What biomarker tests were done, and what were the results of those tests?’” Liu said. “I will tell you, if a doctor is threatened by someone asking a question, I think you really need to reconsider that relationship.”
Get breaking news and daily headlines delivered to your email inbox by signing up here.
Anthony Stumbo’s heart sank after the doctor shared his mother’s chest X-ray.
“I remember that drive home, bringing her back home, and we basically cried,” said the internal medicine physician, who had started practicing in eastern Kentucky near his childhood home shortly before his mother began feeling ill. “Nobody wants to get told they’ve got inoperable lung cancer. I cried because I knew what this meant for her.”
Now Stumbo, whose mother died the following year, in 1997, is among a group of Kentucky clinicians and researchers determined to rewrite the script for other families by promoting training and boosting awareness about early detection in the state with the highest lung cancer death rate. For the past decade, Kentucky researchers have promoted lung cancer screening, first recommended by the U.S. Preventive Services Task Force in 2013. These days the Bluegrass State screens more residents who are at high risk of developing lung cancer than any state except Massachusetts — 10.6% of eligible residents in 2022, more than double the national rate of 4.5% — according to the most recent American Lung Association analysis.
Anthony Stumbo is among a group of Kentucky clinicians and researchers working to improve outcomes for lung cancer patients and their families by increasing screening rates and thereby catching tumors earlier, when they’re more treatable.
Veronica Turner for KFF Health News
The effort has been driven by a research initiative called the Kentucky LEADS (Lung Cancer Education, Awareness, Detection, and Survivorship) Collaborative, which in 2014 launched to improve screening and prevention, to identify more tumors earlier, when survival odds are far better. The group has worked with clinicians and hospital administrators statewide to boost screening rates both in urban areas and regions far removed from academic medical centers, such as rural Appalachia. But, a decade into the program, the researchers face an ongoing challenge as they encourage more people to get tested, namely the fear and stigma that swirl around smoking and lung cancer.
Lung cancer kills more Americans than any other malignancy, and the death rates are worst in a swath of states including Kentucky and its neighbors Tennessee and West Virginia, and stretching south to Mississippi and Louisiana, according to data from the Centers for Disease Control and Prevention.
It’s a bit early to see the impact on lung cancer deaths because people may still live for years with a malignancy, LEADS researchers said. Plus, treatment improvements and other factors may also help reduce death rates along with increased screening. Still, data already shows that more cancers in Kentucky are being detected before they become advanced, and thus more difficult to treat, they said. Of total lung cancer cases statewide, the percentage of advanced cases — defined as cancers that had spread to the lymph nodes or beyond — hovered near 81% between 2000 and 2014, according to Kentucky Cancer Registry data. By 2020, that number had declined to 72%, according to the most recent data available.
“We are changing the story of families. And there is hope where there has not been hope before,” said Jennifer Knight, a LEADS principal investigator.
Older adults in their 60s and 70s can hold a particularly bleak view of their mortality odds, given what their loved ones experienced before screening became available, said Ashley Shemwell, a nurse navigator for the lung cancer screening program at Owensboro Health, a nonprofit health system that serves Kentucky and Indiana.
“A lot of them will say, ‘It doesn’t matter if I get lung cancer or not because it’s going to kill me. So I don’t want to know,’” said Shemwell. “With that generation, they saw a lot of lung cancers and a lot of deaths. And it was terrible deaths because they were stage 4 lung cancers.” But she reminds them that lung cancer is much more treatable if caught before it spreads.
The collaborative works with several partners, including the University of Kentucky, the University of Louisville, and GO2 for Lung Cancer, and has received grant funding from the Bristol Myers Squibb Foundation. Leaders have provided training and other support to 10 hospital-based screening programs, including a stipend to pay for resources such as educational materials or a nurse navigator, Knight said. In 2022, state lawmakers established a statewide lung cancer screening program based in part on the group’s work.
Jacob Sands, a lung cancer physician at Boston’s Dana-Farber Cancer Institute, credits the LEADS collaborative with encouraging patients to return for annual screening and follow-up testing for any suspicious nodules. “What the Kentucky LEADS program is doing is fantastic, and that is how you really move the needle in implementing lung screening on a larger scale,” said Sands, who isn’t affiliated with the Kentucky program and serves as a volunteer spokesperson for the American Lung Association.
In 2014, Kentucky expanded Medicaid, increasing the number of lower-income people who qualified for lung cancer screening and any related treatment. Adults 50 to 80 years old are advised to get a CT scan every year if they have accumulated at least 20 pack years and still smoke or have quit within the past 15 years, according to the latest task force recommendation, which widened the pool of eligible adults. (To calculate pack years, multiply the packs of cigarettes smoked daily by years of smoking.) The lung association offers an online quiz, called “Saved By The Scan,” to figure out likely eligibility for insurance coverage.
Half of U.S. patients aren’t diagnosed until their cancer has spread beyond the lungs and lymph nodes to elsewhere in the body. By then, the five-year survival rate is 8.2%.
But regular screening boosts those odds. When a CT scan detects lung cancer early, patients have an 81% chance of living at least 20 years, according to data published in November in the journal Radiology.
Some adults, like Lisa Ayers, didn’t realize lung cancer screening was an option. Her family doctor recommended a CT scan last year after she reported breathing difficulties. Ayers, who lives in Ohio near the Kentucky border, got screened at UK King’s Daughters, a hospital in far eastern Kentucky. The scan didn’t take much time, and she didn’t have to undress, the 57-year-old said. “It took me longer to park,” she quipped.
She was diagnosed with a lung carcinoid tumor, a type of neuroendocrine cancer that can grow in various parts of the body. Her cancer was considered too risky for surgery, Ayers said. A biopsy showed the cancer was slow-growing, and her doctors said they would monitor it closely.
Ayers, a lifelong smoker, recalled her doctor said that her type of cancer isn’t typically linked to smoking. But she quit anyway, feeling like she’d been given a second chance to avoid developing a smoking-related cancer. “It was a big wake-up call for me.”
Adults with a smoking history often report being treated poorly by medical professionals, said Jamie Studts, a health psychologist and a LEADS principal investigator, who has been involved with the research from the start. The goal is to avoid stigmatizing people and instead to build rapport, meeting them where they are that day, he said.
“If someone tells us that they’re not ready to quit smoking but they want to have lung cancer screening, awesome; we’d love to help,” Studts said. “You know what? You actually develop a relationship with an individual by accepting, ‘No.’”
Nationally, screening rates vary widely. Massachusetts reaches 11.9% of eligible residents, while California ranks last, screening just 0.7%, according to the lung association analysis.
That data likely doesn’t capture all California screenings, as it may not include CT scans done through large managed care organizations, said Raquel Arias, a Los Angeles-based associate director of state partnerships at the American Cancer Society. She cited other 2022 data for California, looking at lung cancer screening for eligible Medicare fee-for-service patients, which found a screening rate of 1%-2% in that population.
But, Arias said, the state’s effort is “nowhere near what it needs to be.”
The low smoking rate in California, along with its image as a healthy state, “seems to have come with the unintended consequence of further stigmatizing people who smoke,” said Arias, citing one of the findings from a 2022 report looking at lung cancer screening barriers. For instance, eligible patients may be reluctant to share prior smoking habits with their health provider, she said.
Meanwhile, Kentucky screening efforts progress, scan by scan.
At Appalachian Regional Healthcare, 3,071 patients were screened in 2023, compared with 372 in 2017. “We’re just scratching the surface of the potential lives that we can have an effect on,” said Stumbo, a lung cancer screening champion at the health system, which includes 14 hospitals, most located in eastern Kentucky.
The doctor hasn’t shed his own grief about what his family missed after his mother died at age 51, long before annual screening was recommended. “Knowing that my children were born, and never knowing their grandmother,” he said, “just how sad is that?”
KFF Health News, formerly known as Kaiser Health News (KHN), is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.