If you’re still skeptical about the power of red light therapy, I get it. I was hesitant, too, before I used Bon Charge’s Red Light Face Mask for one month. During the 30-day experiment, my skin completely transformed to reveal a brighter, more even complexion—and it was easily the best thing I’ve done for my skin years.
Tag: longevity
-
50+ Unbeatable Black Friday Deals To Save On All Your Favorite Well-Being Essentials
Support your well-being one can’t-miss sale at a time.
-
Prostate Cancer and Mushrooms | NutritionFacts.org
What can reishi mushrooms, shiitake mushroom extracts, and whole, powdered white mushrooms do for cancer patients?
“A regular intake of mushrooms can make us healthier, fitter, and happier, and help us live longer,” but what is the evidence for all that? “Mushrooms are widely cited for their medicinal qualities, yet very few human intervention studies have been done using contemporary guidelines.”
There is a compound called lentinan, extracted from shiitake mushrooms. To get about an ounce, you have to distill around 400 pounds of shiitakes, about 2,000 cups of mushrooms. Researchers injected the compound into cancer patients to see what happens. The pooled response from a dozen small clinical trials found that the objective response rate was significantly improved when lentinan was added to chemotherapy regimens for lung cancer. “Objective response rate” means, for example, tumor shrinkage, but what we really care about is survival and quality of life. Does it actually make cancer patients live any longer or any better? Well, those in the lentinan group suffered less chemo-related toxicity to their gut and bone marrow, so that alone might be reason enough to use it. But what about improving survival?
I was excited to see that lentinan may significantly improve survival rates for a type of leukemia. Indeed, researchers found that adding lentinan to the standards of care increased average survival, reduced cachexia (cancer-associated muscle wasting), and improved cage-side health. Wait, what? This was improved survival for brown Norwegian rats, so that the so-called clinical benefit only applies if you’re a rat or a veterinarian.
A compilation of 17 actual human clinical studies did find improvements in one-year survival in advanced cancer patients but no significant difference in the likelihood of living out to two years. Even the compilations of studies that purport that lentinan offers a significant advantage in terms of survival are just talking about statistical significance. As you can see below and at 2:15 in my video White Button Mushrooms for Prostate Cancer, it’s hard to even tell these survival curves apart.
Lentinan improved survival by an average of 25 days. Now, 25 days is 25 days, but we “should evaluate assertions made by companies about the miraculous properties of medicinal mushrooms very critically.”
Lentinan has to be injected intravenously. What about mushroom extract supplements you can just take yourself? Researchers have noted that shiitake mushroom extract is available online for the treatment of prostate cancer for approximately $300 a month, so it’s got to be good, right? Men who regularly eat mushrooms do seem to be at lower risk for getting prostate cancer—and apparently not just because they eat less meat or consume more fruits and vegetables in general. So, why not give a shiitake mushroom extract a try? Because it doesn’t work. On its own, it is “ineffective in the treatment of clinical prostate cancer.” Researchers wrote that “the results demonstrate that claims for CAM [complementary and alternative medicine], particularly for herbal and food supplement remedies, can be easily and quickly tested.” Put something to the test? What a concept! Maybe it should be required before individuals spend large amounts of money on unproven treatments, or, in this case, a disproven treatment.
What about God’s mushroom (also known as the mushroom of life) or reishi mushrooms? “Conclusions: No significant anticancer effects were observed”—not even a single partial response. Are we overthinking it? Plain white button mushroom extracts can kill off prostate cancer cells, at least in a petri dish, but so could the fancy God’s mushroom, but that didn’t end up working in people. You don’t know if plain white button mushrooms work on real people until you put them to the test.
What I like about this study is that the researchers didn’t use a proprietary extract. They just used regular whole mushrooms, dried and powdered, the equivalent of a half cup to a cup and a half of fresh white button mushrooms a day, in other words, a totally doable amount. The researchers gave them to men with “biochemically recurrent prostate cancer”—the men had already gotten a prostatectomy or radiation in an attempt to cut or burn out all the cancer, but it returned and started growing, as evidenced by a rise in PSA levels, an indicator of prostate cancer progression.
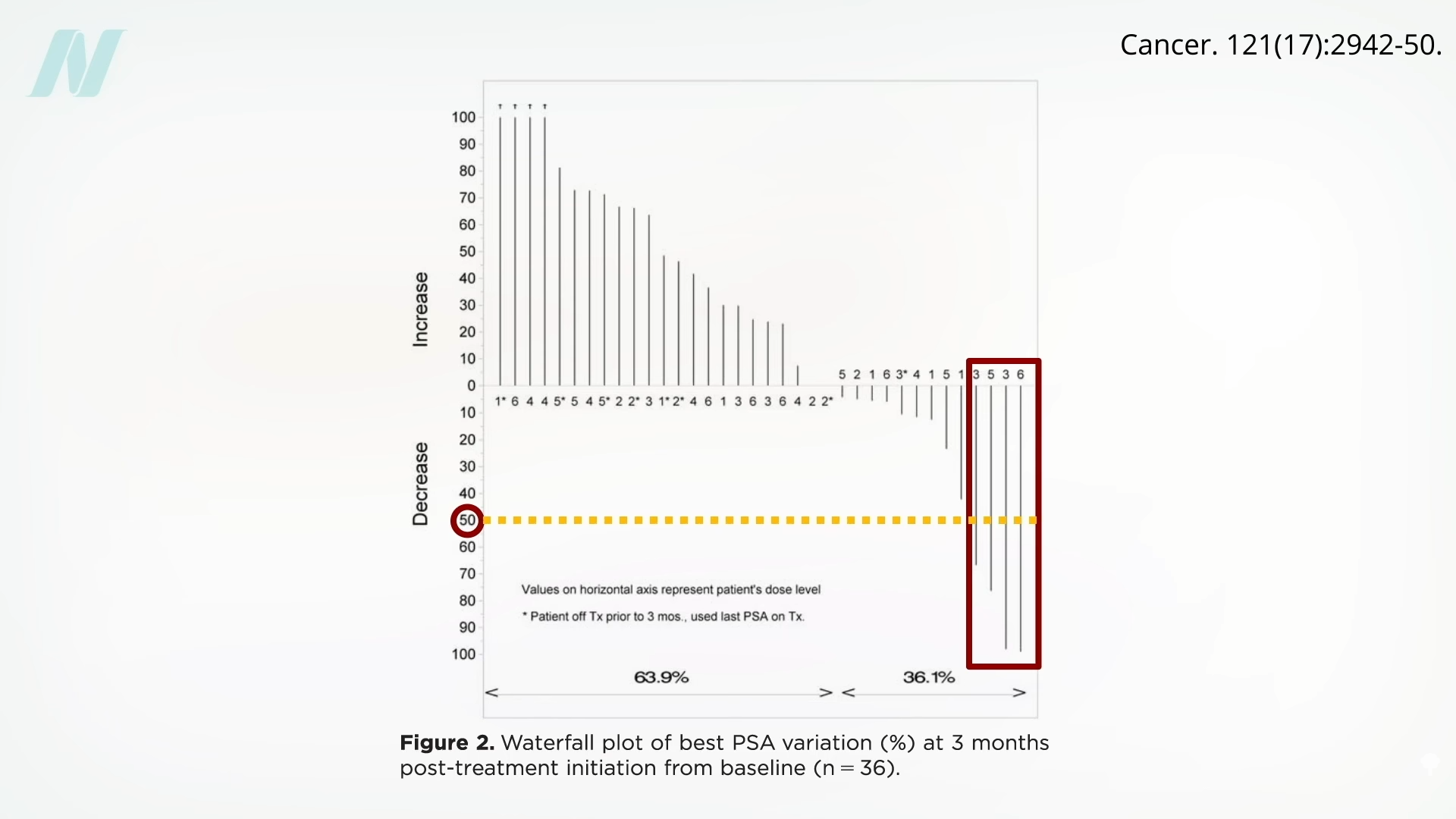
Of the 26 patients who had gotten the button mushroom powder, 4 appeared to respond, meaning they got a drop in PSA levels by more than 50% after starting the mushrooms, as you can see here and at 4:31 in my video.
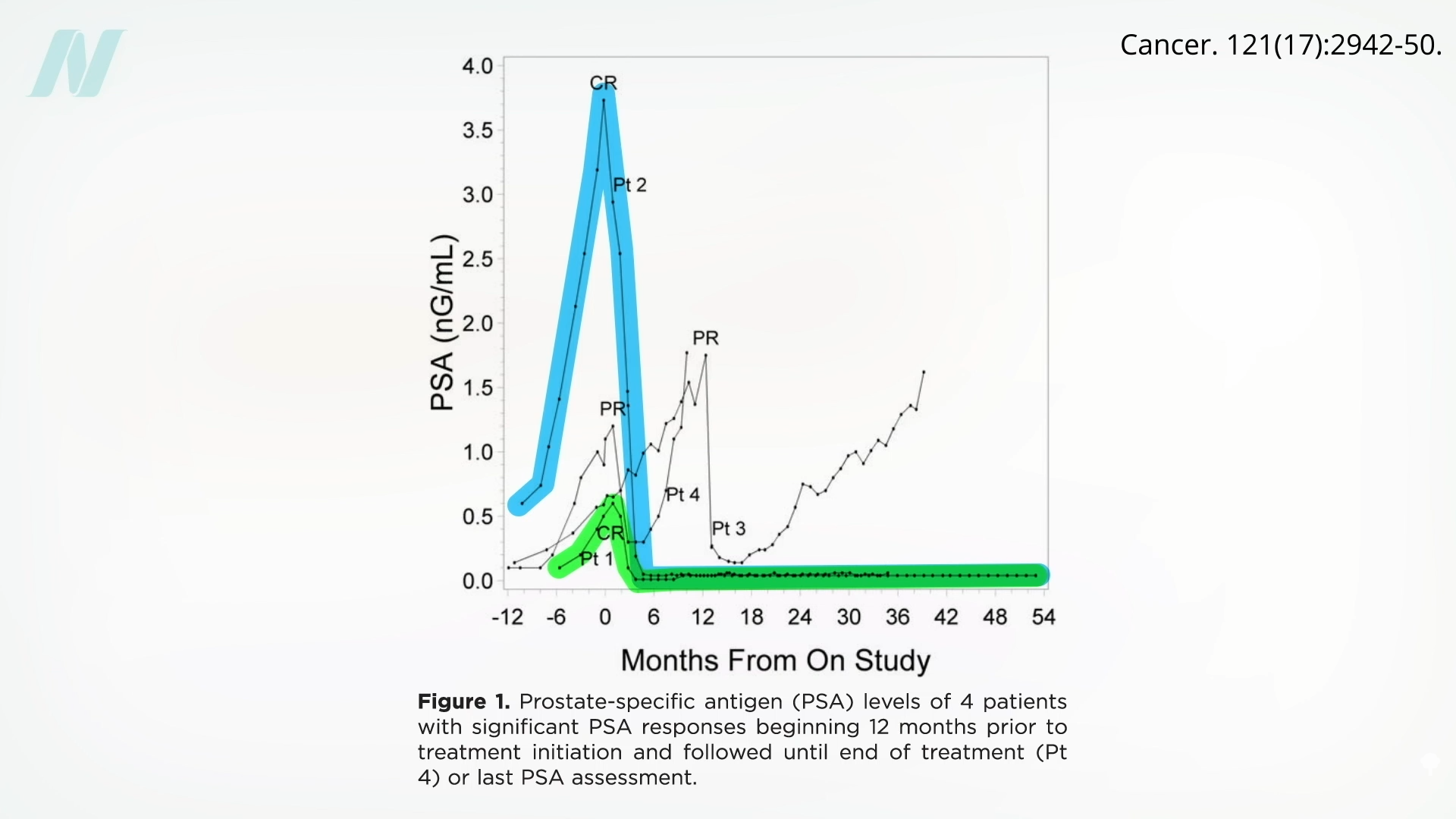
In the next graphic, below and at 4:22, you can see where the four men who responded started out in the months leading up to starting the mushrooms. Patient 2 (“Pt 2”) was my favorite. He had an exponential increase in PSA levels for a year, then he started some plain white mushrooms, and boom! His PSA level dropped to zero and stayed down. A similar response was seen with Patient 1. Patient 4 had a partial response, before his cancer took off again, and Patient 3 appeared to have a delayed partial response.
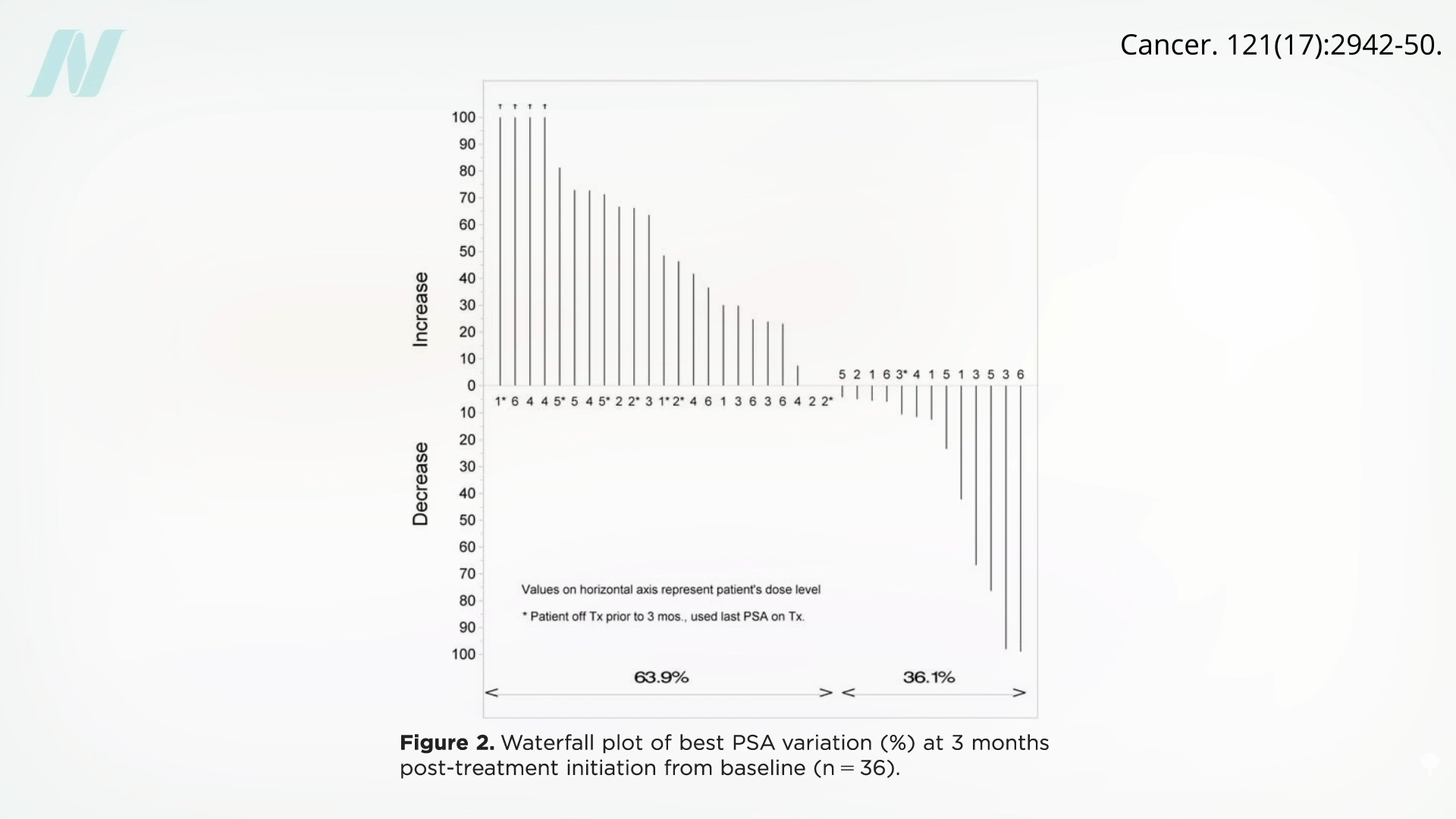
Now, in the majority of cases, PSA levels continued to rise, not dipping at all. But even if there is only a 1-in-18 chance you’ll be like Patients 1 and 2, seen below and at 5:12, you may get a prolonged, complete response that continues.
We aren’t talking about weighing the risks of some toxic chemotherapy for the small chance of benefit, but just eating some inexpensive, easy, tasty plain white mushrooms every day. Yes, the study didn’t have a control group, so it may have just been a coincidence, but rising PSAs in post-prostatectomy patients are almost always indicators of cancer progression. And, what’s the downside of adding white button mushrooms to your diet?
In these two patients, their PSA levels became undetectable, suggesting that the cancer disappeared altogether. They had already gone through surgery, had gotten their primary tumor removed, along with their entire prostate, and had already gone through radiation to try to clean up any cancer that remained, and yet the cancer appeared to be surging back—until, that is, they started a little plain mushroom powder.
Doctor’s Note
If you missed the previous blog, check out Medicinal Mushrooms for Cancer Survival.
Also check out Friday Favorites: Mushrooms for Prostate Cancer and Cancer Survival.
For more on mushrooms, see Breast Cancer vs. Mushrooms and Is It Safe to Eat Raw Mushrooms?.
For more videos on prostate cancer, check the related posts below.
Michael Greger M.D. FACLM
Source link -
The Era of Startup Outrage-Bait Marketing Is Upon Us
If the goal was to spark a reaction among the denizens of the biggest city in the U.S., then a recent advertising campaign that implores new parents to “pick your baby” has been a remarkable success.
Recently, ads for Nucleus Genomics, a New York City-based startup that offers what it calls IVF “for longevity,” began appearing in subway stations across the city. Images of ethnically diverse, healthy, and happy babies appeared above the words “IQ is 50% genetic,” and “height is 80% genetic” on banner ads hanging at Broadway-Lafayette station in Lower Manhattan. Other ads tell parents to “have your best baby” and to “have a healthier baby.” The campaign also points the public to a website: Pickyourbaby.com. (A Nucleus spokesperson told Inc that NYC’s Metropolitan Transportation Authority initially rejected the ads, requiring tweaks to copy and images before approval.)
Nucleus was founded in 2021 by Kian Sadeghi, who describes the company’s mission as “IVF for genetic optimization.” The company offers “advanced embryo testing” that allows parents to lower their children’s chance of disease, it claims. So far, Nucleus has raised $32 million from a variety of investors, including Alexis Ohanian’s Seven Seven Six and Founders Fund.
The reaction to Nucleus’s campaign has been mostly critical. Social media users accused the company of promoting a sci-fi-tinted version of eugenics—the pseudoscience that promotes racial purity through selective breeding.
However, Sadeghi has a different perspective. He tells Inc. the campaign was meant to cultivate a deeper understanding of genetics for prospective parents. “Some of the reasons why people get scared about genetics and the randomness of genetics is because they don’t understand it,” Sadeghi says.
The startups standing out by rage-baiting
Nucleus’ subway campaign is just one example of how tech startups are intentionally rage-baiting the public to promote their businesses. The recent glut of AI startups has led several new firms to lean into the strategy to distinguish themselves from the competition.
Earlier this year, another slate of ads run by the AI chatbot company Friend was defaced across the city by various detractors. The ads were sparse and featured a definition of the word “friend” alongside its flagship product, a necklace that listens to users and responds via a corresponding app. Its critics accused the company of promoting “AI sycophancy,” the kind of behavior that has led some users into codependent and sometimes delusional relationships with chatbots.
Another AI startup, Cluely, raised eyebrows earlier this year after its founders introduced the app by saying it lets users “cheat on everything.” (Cluely has since pivoted to a note-taking product, but still promotes its “cheating on everything” ethos.) In August, the company purchased a billboard in Times Square. But instead of putting up a high-production-value ad, it ran simple black-on-white text with the tone of a meme, from the POV of the founder Roy Lee: “hi i’m roy im 21 this was very expensive pls buy my thing.” One advertising industry website called the stunt “brutally honest.” And Artisan AI, a company that builds agentic AI for sales, sparked a high-profile reprimand from Senator Bernie Sanders in October over its “stop hiring humans” campaign.
Nucleus’ says it drew inspiration for its campaign from another recent ad blitz: Levi’s campaign with actress Sydney Sweeney featured the tagline “Sydney has great jeans.” The ads sparked an uproar about genetics, race, and societal beauty standards. However, the company’s presentation of ethnically diverse babies seems to be directly responding to the backlash against the Levi’s campaign for promoting white beauty standards. Signs taped around specific downtown neighborhoods offer a riff on the Levi’s slogan: “these babies have great genes,” they read. Before the launch of the Nucleus campaign, Sadeghi told Inc, “We expect it to incite conversation. We expect it to incite curiosity, and we expect people to start engaging.”
But does rage-bait marketing work?
A spokesperson for the firm lauded the campaign in an email on Friday, writing: “Nucleus’ campaign has driven +150% surge in sales across its products and 8M impressions over social media this week, despite being met with negative backlash.”
While it’s unclear whether or not it always works for brands that intentionally incite public anger, research indicates that people are inclined to engage with content online when it defies or challenges their personal views.
Nucleus’s metrics make for further promotional fodder, but it’s also spotlighted the company’s legal troubles. In October, Nucleus was sued by another IVF company, Genomic Prediction, for allegedly stealing trade secrets. So far, Nucleus has prevailed. Genomic Prediction’s request for injunctive relief was denied in federal district court last week, lawyers for Nucleus noted in a blog post. Sadeghi didn’t respond to Inc’s request for comment on the lawsuit, but he briefly took to X to address the outrage over the company’s ad campaign and to briefly remark on the legal victory. “To the mob trying to cancel Nucleus,” he wrote on Sunday. “Keep tweeting. Stay mad. We’ll keep building and serving patients. P.S. We won the injunction.”
The final deadline for the 2026 Inc. Regionals Awards is Friday, December 12, at 11:59 p.m. PT. Apply now.
Sam Blum
Source link -
Antonei Csoka: Aging Is Not Something We Have to Accept as Inevitable
SHARYL ATTKISSON: Leading the charge are visionary scientists whose work is transforming theory into tangible advances.Visionary scientist David Sinclair has popularized supplements that boost levels of a crucial coenzyme, potentially delaying age-related decline.
At the Buck Institute for Research on Aging, researcher Eric Verdin explores how metabolic shifts can extend healthy years.
Maria Blasco of Spain’s National Cancer Research Center focuses on telomeres, a piece of DNA at the end of animal chromosomes protecting them from degradation.
Nir Barzilai, director of the Institute for Aging Research at Albert Einstein College of Medicine, is leading a study testing the diabetes drug metformin as an anti-aging agent.
And Vadim Gladyshev at Harvard is investigating rejuvenation by reprogramming or “resetting” cells without turning them cancerous.
As researchers work to crack the code on aging and how to slow or stop it, there’s a philosophical and scientific divide: Is aging a natural, programmed part of life, or a treatable condition akin to a disease that can be “cured”?
ANTONEI CSOKA: I see aging as a kind of great challenge to humanity. It’s not something that we have to accept as inevitable.
SHARYL ATTKISSON: Antonei Csoka is an associate professor at Howard University who studies the cell and molecular biology of aging.
Do you see it as an illness, a disease, a common process that could be reversed?
ANTONEI CSOKA: Great question. So I actually call it a meta-disease, in the sense that it is the cause behind almost every other disease. So it’s like the molecular damage, the DNA mutations, the telomere loss, even the epigenetic changes accumulate over lifespan and lead to these diverse diseases. But they’re all really being caused by aging. So it’s like the generative mechanism behind all of them. It’s the cause and the diseases are the effect.
SHARYL ATTKISSON: Whatever the theory, advances are arriving at breakneck speed. And there’s been an explosion in the practice of medicine surrounding aging and longevity.
Csoka says he hopes we’re on the cusp of virtual immortality.
Do you think in your lifetime we’ll be seeing people live to what age, you know, more people living to 120?
ANTONEI CSOKA: I think it’s quite possible. Yeah. I think we’re actually in an incredibly unique time. Like maybe a time that only happens once in human history. And that time is where the people alive today could determine whether they live a very long time, you know, potentially like, you know, extreme long old age, you know, a thousand years, for example.
SHARYL ATTKISSON: You think that’s possible that people can live a thousand years?
ANTONEI CSOKA: Yeah, I do. Yeah. I don’t think there’s any like, biological law that, that denies that possibility. But in the past, you know, people dreamed of, of immortality and the fountain of youth and so on, but it was basically impossible. Like the, the science didn’t exist. And in the future, I think it will be solved. Like it will be, you know, say a hundred years from now, the aging will be fully understood and potentially fully reversible. So we’re kind of in a very unique, very unique sliver of time.
Antonei Csoka, Full Measure
Source link -
The Hidden Effects Of Long COVID On Your Gut, Brain & Energy
A few months ago, I got my routine lab work back, and one number stopped me in my tracks. My neuroinflammation marker was off the charts. Which made no sense. I felt great. I was training regularly, sleeping well, and eating clean. But my doctor, Frank Lipman, M.D., told me it could be a lingering sign of Long COVID, even though I hadn’t had symptoms in months.
-
Ultra-Processed Foods May Harm Every Major Organ, Says 100+ Studies
But this research also highlights something hopeful. Even in a landscape dominated by UPFs, shifting back toward whole and minimally processed foods—slowly, consistently, and in ways that feel doable—can meaningfully support your health. These foods deliver the fiber, antioxidants, and nutrients your body relies on to regulate appetite, stabilize blood sugar, calm inflammation, and fuel long-term well-being.
-
Study Finds Link Between ADHD & Alzheimer’s Disease
Scientists have previously hypothesized that attention-deficit/hyperactivity disorder (ADHD) may be a risk factor for cognitive decline and Alzheimer’s disease (AD). However, the lack of studies investigating age-related cognitive decline in individuals with ADHD later in life has prevented a distinct association between ADHD and cognitive decline—until now.
-
23 Longevity Gifts That Prove Biohacking Isn't Just For The Boys
Biohacking isn’t just for the boys.
-
Plant-Based Hospital Menus | NutritionFacts.org
The American Medical Association passed a resolution encouraging hospitals to offer healthy plant-based food options.
“Globally, 11 million deaths annually are attributable to dietary factors, placing poor diet ahead of any other risk factor for death in the world.” Given that diet is our leading killer, you’d think that nutrition education would be emphasized during medical school and training, but there is a deficiency. A systematic review found that, “despite the centrality of nutrition to a healthy lifestyle, graduating medical students are not supported through their education to provide high-quality, effective nutrition care to patients…”
It could start in undergrad. What’s more important? Learning about humanity’s leading killer or organic chemistry?
In medical school, students may average only 19 hours of nutrition out of thousands of hours of instruction, and they aren’t even being taught what’s most useful. How many cases of scurvy and beriberi, diseases of dietary deficiency, will they encounter in clinical practice? In contrast, how many of their future patients will be suffering from dietary excesses—obesity, diabetes, hypertension, and heart disease? Those are probably a little more common than scurvy or beriberi. “Nevertheless, fully 95% of cardiologists [surveyed] believe that their role includes personally providing patients with at least basic nutrition information,” yet not even one in ten feels they have an “expert” grasp on the subject.
If you look at the clinical guidelines for what we should do for our patients with regard to our number one killer, atherosclerotic cardiovascular disease, all treatment begins with a healthy lifestyle, as shown below and at 1:50 in my video Hospitals with 100-Percent Plant-Based Menus.
“Yet, how can clinicians put these guidelines into practice without adequate training in nutrition?”
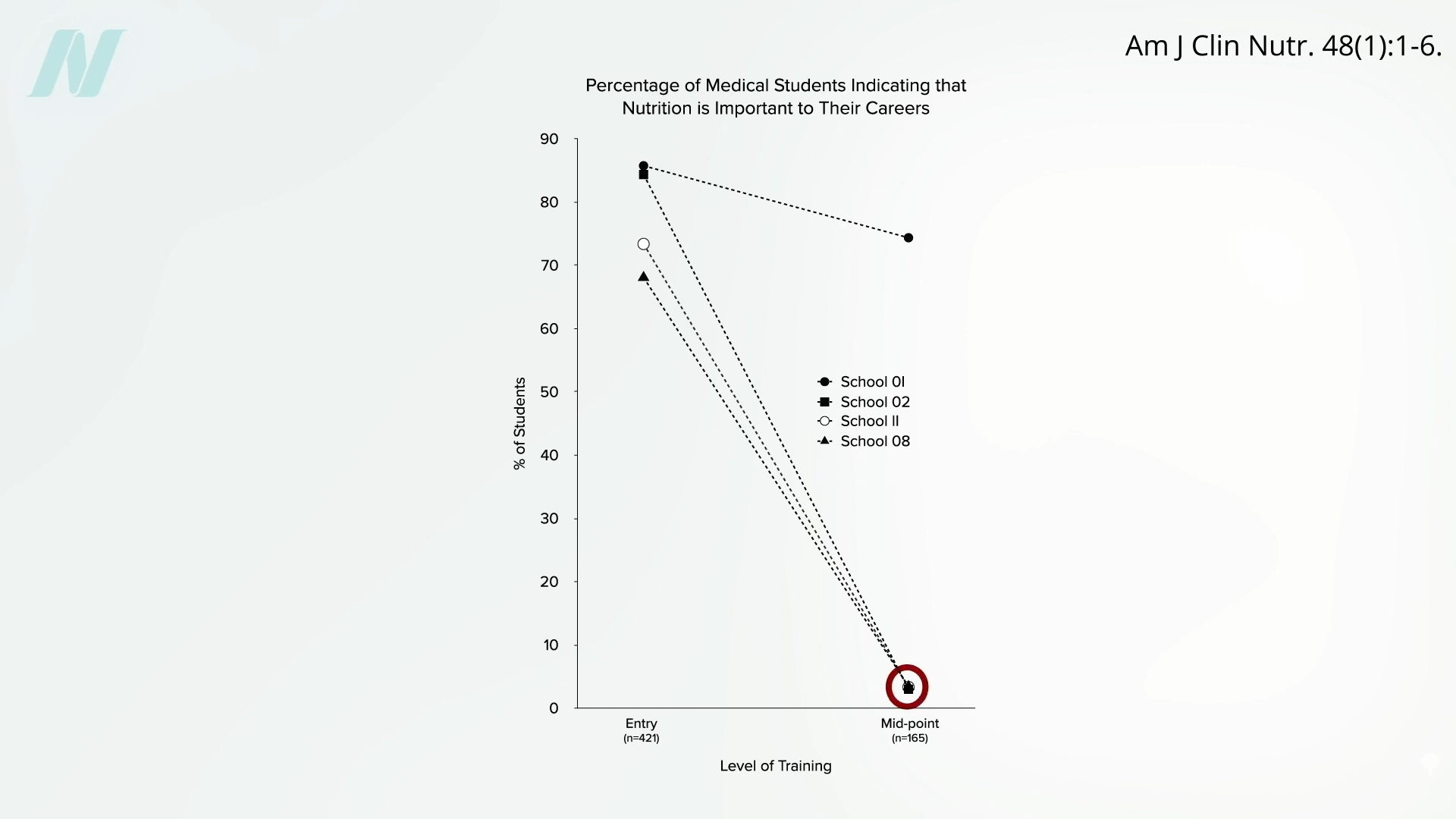
Less than half of medical schools report teaching any nutrition in clinical practice. In fact, they may be effectively teaching anti-nutrition, as “students typically begin medical school with a greater appreciation for the role of nutrition in health than when they leave.” Below and at 2:36 in my video is a figure entitled “Percentage of Medical Students Indicating that Nutrition is Important to Their Careers.” Upon entry to different medical schools, about three-quarters on average felt that nutrition is important to their careers. Smart bunch. Then, after two years of instruction, they were asked the same question, and the numbers plummeted. In fact, at most schools, it fell to 0%. Instead of being educated, they got de-educated. They had the notion that nutrition is important washed right out of their brains. “Thus, preclinical teaching”— the first two years of medical school—“engenders a loss of a sense of the relevance of the applied discipline of nutrition.”
Following medical school, during residency, nutrition education is “minimal or, more typically, absent.” “Major updates” were released in 2018 for residency and fellowship training requirements, and there were zero requirements for nutrition. “So you could have an internal medicine graduate who comes out of a terrific program and has learned nothing—literally nothing—about nutrition.”
“Why is diet not routinely addressed in both medical education and practice already, and what should be done about that?” One of the “reasons for the medical silence in nutrition” is that, “sadly…nutrition takes a back seat…because there are few financial incentives to support it.” What can we do about that? The Food Law and Policy Clinic at Harvard Law School identified a dozen different policy levers at all stages of medical education and the kinds of policy recommendations there could be for the decision-makers, as you can see here and at 3:48 in my video.
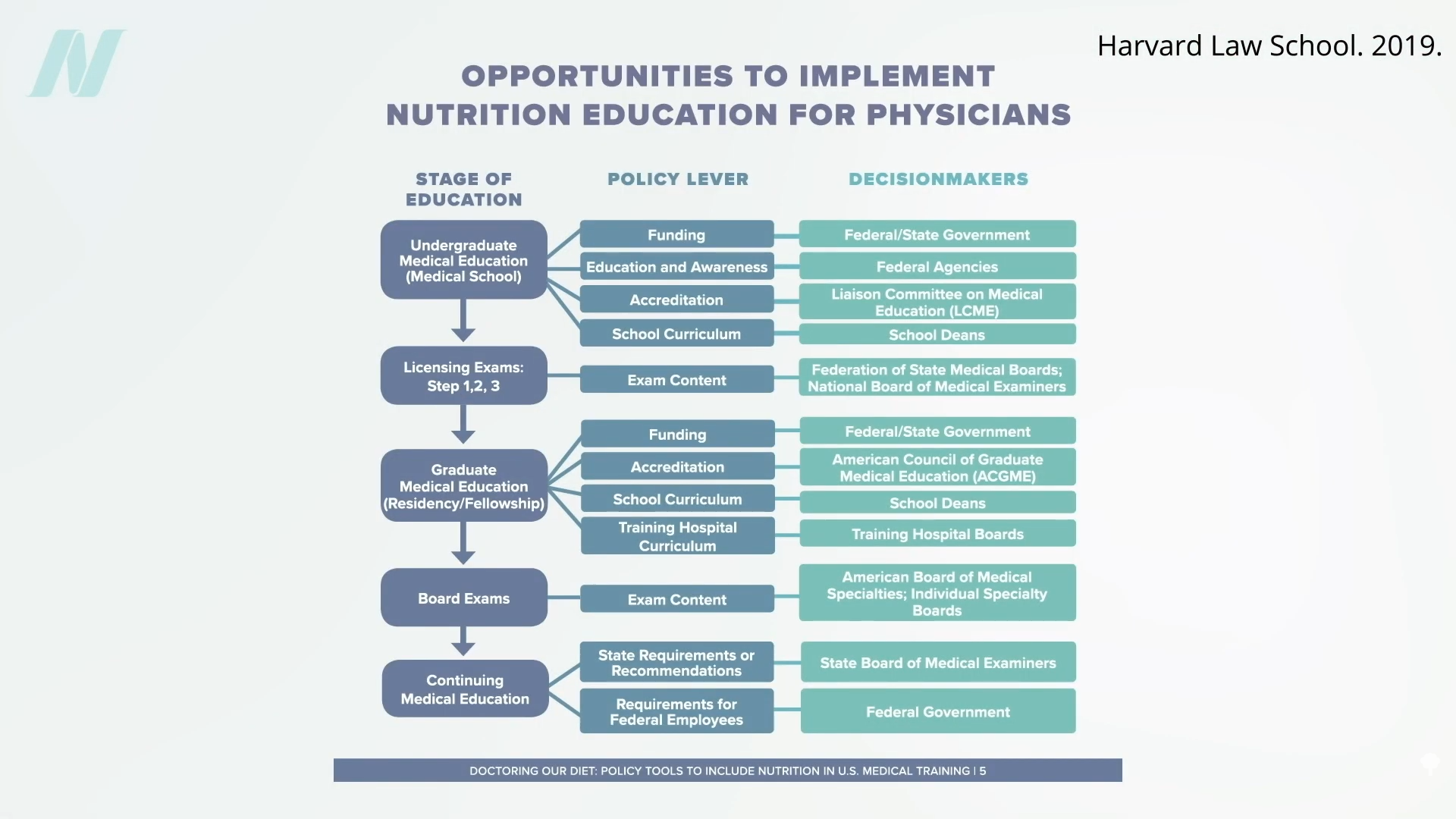
For instance, the government could require doctors working for Veterans Affairs (VA) to get at least some courses in nutrition, or we could put questions about nutrition on the board exams so schools would be pressured to teach it. As we are now, even patients who have just had a heart attack aren’t changing their diet. Doctors may not be telling them to do so, and hospitals may be actively undermining their future with the food they serve.
The good news is that the American Medical Association (AMA) has passed a resolution encouraging hospitals to offer healthy food options. What a concept! “Our AMA hereby calls on [U.S.] Health Care Facilities to improve the health of patients, staff, and visitors by: (a) providing a variety of healthy food, including plant-based meals, and meals that are low in saturated and trans fat, sodium, and added sugars; (b) eliminating processed meats from menus; and (c) providing and promoting healthy beverages.” Nice!
“Similarly, in 2018, the State of California mandated the availability of plant-based meals for hospital patients,” and there are hospitals in Gainesville (FL), the Bronx, Manhattan, Denver, and Tampa (FL) that “all provide 100% plant-based meals to their patients on a separate menu and provide educational materials to inpatients to improve education on the role of diet, especially plant-based diets, in chronic illness.”
Let’s check out some of their menu offerings: How about some lentil Bolognese? Or a cauliflower scramble with baked hash browns for breakfast, mushroom ragu for lunch, and, for supper, white bean stew, salad, and fruit for dessert. (This is the first time a hospital menu has ever made me hungry!)
The key to these transformations was “having a physician advocate and increasing education of staff and patients on the benefits of eating more plant-based foods.” A single clinician can spark change in a whole system, because science is on their side. “Doctors have a unique position in society” to influence policy at all levels; it’s about time we used it.
For more on the ingrained ignorance of basic clinical nutrition in medicine, see the related posts below.
Michael Greger M.D. FACLM
Source link -
Inside Peter Attia, M.D.’s Exercise & Bloodwork Routine
When it comes to living longer and better, few voices carry as much weight as Peter Attia, M.D. The longevity medicine expert and author of Outlive: The Science of Art & Longevity has spent years translating complex research into actionable strategies for extending both lifespan and healthspan.
-
The #1 Food Category Linked To Colon Cancer In Women Under 50
Cancer cases in young adults have surged nearly 80% worldwide over the past three decades. And while population growth accounts for some of that increase, the trend is undeniable: more people in their 20s, 30s, and 40s are developing diseases we once thought of as problems for our parents’ and grandparents’ generations.
-
The Best Years of Your Life Are Probably Still Ahead
Laura Carstensen’s favorite lecture of the year is the one when she tells undergrads at Stanford University that—contrary to what they’ve probably been told and believe—these are not the best years of their lives. Those come much, much later.
“I look out at a sea of 100 students sitting in a classroom, and I love the look on their faces. It’s just such relief,” says Carstensen, a professor of psychology and founding director of the Stanford Center on Longevity. “I can visibly see it, because not only are the late teens and 20s the worst time in our lives—with the highest rates of loneliness, anxiety, and depression—but people are constantly telling [young people] that they’re the best years.”
Carstensen’s research consistently suggests that starting in people’s mid-20s, they begin experiencing fewer negative emotions. That doesn’t mean they have more frequent or intense positive emotions; rather, their emotional balance improves as they age.
As part of TIME’s series interviewing leaders in the longevity field, we caught up with Carstensen to talk about what drives these changes—and the surprising type of friendship she wishes more people would prioritize.
This interview has been condensed and edited for clarity.
Your research seems to suggest that older age is something to look forward to, not dread. Is that how you see it?
Yes, and in many ways, it’s the best time in life. Emotionally speaking, it’s the best time in life. Now let me be clear: There’s a lot not to like about aging; physically, it sucks. It’s not a good story, but the emotional one is. There’s not a perfect stage in life—there’s always trade-offs. When you’re young and miserable, you’re also at your physical peak, and that’s wonderful. Having a limitless future is exciting, too.
Older people don’t have that, but they do have a sense of focus and what matters in their life. There’s this juxtaposition of physical vitality and emotional richness, and they’re occurring in different stages in different ways.
So what happens to emotional well-being as we get older?
People have a better emotional experience. They’re more satisfied with their relationships and more at peace with themselves, and as we get older, we stop caring so much about these trivial matters that can drive us crazy at earlier stages of life. Plus, in terms of cognitive processing, we tend to literally see, hear, and remember positive information more than negative information.
Read More: 4 Ways to Get Happier As You Age
Older people aren’t happier—we don’t see changes so much in happiness across the life course. But we do see a significant reduction in anger and sadness and fear and anxiety. That’s why we say emotional balance improves with age. It’s different than saying, ‘I’m happier.’ Your emotional life becomes richer, and you’re more likely to see an old friend and smile and get a tear in your eye at the same time. I think that’s because we know life doesn’t go on forever. It’s not happy-go-lucky, but there’s something sweetly poignant about it.
As time becomes more valuable, we use it in better ways.
When do these changes happen?
We’ve done a major longitudinal study looking at this, and it looks like the 20s are the worst. Then you begin to see some reduction in negative emotion, and it’s really going down by your 40s and 50s. The 60s and 70s are the peak of life, emotionally speaking. It doesn’t get worse significantly as you get older than that, but that’s where it kind of levels off—so the major bang-for-the-buck change is between 40 and 60.
What are some of your other interesting takeaways about older age?
Another reliable finding has to do with what we call prosocial behavior: basically giving to and doing things for other people. Older people are more likely to engage in prosocial behavior and also feel better when they do, so they’re giving more and they’re getting a bigger bang for their buck. It’s a very rewarding experience. Because of these findings, occasionally I’ll be having a really bad day and I’ll think, ‘Boy, I’ve got to go help somebody.’
Are there other surprising insights about aging that you wish more people knew about?
One is how much older people like younger people. There are lots of myths about generational conflict, but older people think young people are the bee’s knees. For the first time in human history, because we’re living longer, we now have this kind of even distribution of age in the population, and I think that’s exciting—the idea that we can come together and address big and little challenges with groups of people where we’re combining the skill and the strength and the ambition of youth with the prosociality and experience and emotional balance of older people. That inspires me—thinking about what we can do together.
What is the Stanford Center for Longevity’s ‘New Map of Life’ initiative?
There’s a lot of concern about aging societies: that older people are going to reduce productivity, they’ll be a burden, and on and on. There’s very little evidence for this, first of all; a lot of it’s just mythology. But there is a truth to the idea that there’s a mismatch between the way we live our lives, the social policies and structures that guide us through life, and the length of our lives.
The premise of The New Map of Life—and, really, of our Center on Longevity—is that current generations are born into worlds that were literally built by and for young people, from the knowledge that’s housed in the medical-school libraries to the depth of the stairs that we climb every day. The presumed user is a young person, and we really think that’s why there’s so many problems related to aging.
Read More: 4 Science-Backed Habits That Could Help You Live Longer
What we’re trying to do is start a global conversation about new ways of living, and to think seriously about the policies and institutions. What should education look like when we live to be 100 and work until we’re 80? How should families think about the definition of family, which has long been thought of as the nuclear family? Now most families have at least three or even four generations alive at the same time. Who’s responsible to whom, and when do we give financially to our children? Should it be waiting until you die? Well, if you’re going to die at 100, your kids have to wait until they’re 80 to get the family farm.
That’s a lot to figure out. Are you seeing this conversation start to spread?
I think we are right on the cusp of really rewriting the life script, yes. I do believe that people have recognized—really, for the first time—that century-long lives are becoming increasingly common, and 90-year lives are very common. What are the implications of that for financial security, for education, for the nature of family, and for politics?
Every aspect of our life will change as a function of longevity. And we need to think of ways we can make those changes good for people. How can we use longer lives to improve quality of life at all ages?
Are there already specific ideas on how to accomplish all this?
There are. The financial security industry, for example, is thinking of new products that can help people prepare for longer lives. A real struggle people are having today is, how do you save enough to retire? And then let’s say you did all the right things and you’ve saved millions of dollars and you’re 65 or 70 and you’re retiring. There’s very little guidance on how to decumulate that, how to spend down that money. There are new products being developed that are helping people do that, so that’s exciting.
We also work and talk with people in the transportation world—automating cars is going to make travel much, much better for people of all ages. A lot is percolating, and one of the things we hope to do more of at the center is to pull that together and be a repository for information about best practices, new ideas, and new ways of being.
I want to ask you about one other area you’re passionate about: intergenerational friendships.
This intergenerational opportunity is one that we don’t think about enough, and it’s really exciting. We know that we’re really age-segregated in our world, so young people don’t have old people who are their friends. We have relatives, so we interact across generations within families, but not very much outside of our family. If you look at somebody who’s over 65 and ask them, out of all the people in their social network, they have fewer than one friend who’s under 25.
Read More: Unlocking the Secrets to Living to 100
What’s interesting to me is those friendships—the opportunities and the mutual benefits. Being friends with people of different generations is really quite extraordinary, and we’re not taking advantage of it.
How could we do a better job of that?
We’re just starting to study this in our laboratory. We think one way to forge these connections is by having people at different ages work together on something to solve—let’s say there’s a community challenge of some sort, whether it’s having enough food distributed, building a community center, or something where people come together to work on a project together. That’s why we form strong bonds.
In the past, a lot of intergenerational efforts have been friendly visiting programs, and those have never been successful. They’re usually patronizing to old people. I think it’s key to approach it differently and say, ‘I’m so lucky because I live in an intergenerational world.’
This article is part of TIME Longevity, an editorial platform dedicated to exploring how and why people are living longer and what this means for individuals, institutions, and the future of society. For other articles on this topic, click here.
Angela Haupt
Source link -
This Vitamin Slashes The Risk Of A Second Heart Attack By 50%
In the United States, someone has a heart attack nearly every 40 seconds1
-
Struggling To Sleep? Science Says This Is Better Than Any Sleep Aid
Time to hit the hay.
-
The #1 Science-Backed Habit To Slow Brain Aging, Study Finds
Take control over how fast your brain ages.
-
8 Ways to Stay Healthy As You Age
Most people might not have heard of the Framingham Heart Study. But the massive public-health research effort, now in its 77th year of conducting in-depth analysis of more than 15,000 people, is the source of many insights we now have into healthier aging. It inspired the first checklist for assessing heart disease risk, and our current understanding of how to reduce cardiovascular disease can be traced directly to its findings.
While the Framingham Heart Study started off solely focused on heart health, following a large subset of the inhabitants of a former mill town on the outskirts of Boston throughout their lives, it is now providing information about the brain, liver, and many other organs.
As part of TIME’s series interviewing leaders in the longevity field, we spoke to epidemiologist Dr. Donald Lloyd-Jones, the current head of the study and a professor at Boston University Chobanian & Avedisian School of Medicine, about the study and what it tells us about aging well.
This interview has been condensed and edited for clarity.
What is the Framingham Heart Study?
It’s the longest-running community-based study in the world. Its origins lie in finding the root causes of cardiovascular diseases, especially heart attacks and strokes. In 1948, the people who designed the study enrolled about a third of the population of the town of Framingham, Massachusetts, which is about 20 miles west of Boston. They really wanted to understand what was causing the emerging epidemic of heart disease after World War II.
It was already the leading cause of death, but it was quite clear that it was on the rise, and it wasn’t well-understood why that was happening. There were some very good hypotheses implying that diet and cigarette smoking might be linked, but it had never really been shown systematically or consistently.
They started to understand that it would be valuable to have families involved in this study—that heart disease is not just a man’s disease, and that there might be some familial component. They hadn’t even discovered DNA yet. This is decades before thinking about genetics.
Read More: How Tracking Your Health Metrics Can Help You Live Longer
They saw all of the participants every two years and did a full physical examination, collected blood, measured height and weight, things like that. They asked, What were they doing? What were their health habits? Really deep data collection for what was available at the time.
By the early 1960s, they had a strong signal that, in fact, blood cholesterol levels were tightly linked to risk for cardiovascular disease. Blood pressure was especially tightly linked to risks for cardiovascular disease and smoking. Pretty quickly thereafter, they could see that body weight was related, that sedentary lifestyle was related, certain aspects of diet were related.
So Framingham is really the study that put what we now consider the traditional risk factors for cardiovascular disease on the map.
What happened next?
They enrolled another 5,000-plus individuals who were the offspring of the original participants and the spouses of those offspring. So we’re starting to get the genetic linkages, but also the environmental linkages—the shared environment between spouses. It was decades before we understood these things were important, but there were inklings, and they were smart enough to listen to those signals. So the offspring cohorts get examined about every four years, in addition to the first cohort being examined still every two years. That goes on through the 1970s and 80s and 90s.
We start to understand more about not just total cholesterol, but the subcomponents of cholesterol. We start to understand more that it’s actually your systolic blood pressure that’s more dangerous for you than your diastolic blood pressure. Certain types of dietary factors, certain types of physical activity were better.
Fast forward another few decades: in 2002, Framingham enrolled the third generation of related individuals. Along the way, the town of Framingham was actually changing pretty dramatically. Originally, back in 1948, Framingham was a town largely made up of people from European ancestry. It was a mill town, so there was a broad stratification socioeconomically, but it was pretty homogeneous in terms of race and ethnicity—almost exclusively white. But by the 90s and 2000s, there were lots of people of Asian heritage; a lot of Brazilian people settled in Framingham, so it became a much more diverse community.
Read More: Unlocking the Secrets to Living to 100
In total, we’re following six different groups of people, all of whom are related to Framingham in some way. And now there’s the technology to fully sequence someone’s DNA, and understand modifications to that DNA, called epigenetics. We can collect data on what their cells are actually transcribing. We can collect data on proteomics, metabolomics, microbiomics, and there are new technologies to help us look inside the body non-invasively, so we can see disease developing in the cardiovascular system, in the brain and the kidneys.
There has been a huge explosion in the ways we can characterize people. And Framingham has really been a leader all along in understanding the process of aging in every organ system in the body. Yes, we are still the Framingham Heart Study, but we have just as much activity going on in brain health across the life course, and lots of activity looking at bone health, kidney health, lung health, liver health—you name it—because these people are so well studied across their entire life course.
What kinds of things can people do to reduce the risk of diseases of aging?
The American Heart Association has kind of a nice way to package this all together, called Life’s Essential Eight. It’s a platform in which people can measure their cardiovascular health status today. It’s also linked to really positive health outcomes over time, and it’s influenced by evidence from the Framingham Heart Study.
The eight components are not going to surprise you, but they’re all actionable. They’re all modifiable, and they’re all things that people can do today to improve their cardiovascular health, which has been shown to reduce their risk for Alzheimer’s disease, all forms of cardiovascular disease, even cancer, arthritis—all the things that we worry about as chronic diseases of aging. If you focus on your cardiovascular health, you’ll have benefits for all these things simultaneously.
Read More: Want to Live Longer? First Find Out How Old You Really Are
So what are the eight components? They are a healthy diet, participating in physical activity, avoiding all forms of nicotine exposure (combustible cigarettes, but also other forms of nicotine exposure, because they’re toxic, too), healthy sleep, healthy weight, healthy blood pressure, healthy blood sugar, and healthy blood lipids.
No surprises, but here is what this is about: How can we optimize your health today, so that we extend not only your lifespan, but your healthspan—meaning not just the years in your life, but the life in your years?
Can we make the date that you get sick much later—much closer to the time you’re going to die—so that you have more healthy years, not just more years, period?
We don’t seem to necessarily be doing what the science suggests, as a society. Why is that?
The truth is, although we’ve known that for 60 years, we’re still terrible at implementing it in public-health policies and in clinical practice. It’s a pretty simple message, but we don’t design our society, our environment, our neighborhoods, or our food supply to optimize those things.
It is possible to take this information and make a change. Great story: In the early 70s, Finland had the highest coronary heart disease death rates in the world, by a fair amount. They took information from Framingham and they said, You know what, let’s design a study where we take a county with particularly high coronary disease death rates and we just make some public-health changes. We’re going to implement smoking policy changes. We’re going to help people quit. We’re going to stop subsidizing meat, and we’re going to start subsidizing fruits and vegetables in our food supply.
Read More: Scientists Say These Daily Routines Can Slow Cognitive Decline
Immediately, the rates of coronary heart disease started to fall, and the strategies were soon applied across the country. By 30 years later, there was an 84% decline in coronary disease death rates, and suddenly Finland has the lowest coronary disease death rates in the world—so going from last to first.
In the U.S., we saw about a 70% decline in death rates from heart disease between 1968 and 2010, because we’ve gotten better clinically, and we’ve done some things with public health.
Unfortunately, I think while we were making really, really great progress, the obesity epidemic has started to really kick in on the burden of cardiovascular diseases. Because obesity will drive higher blood pressure, higher blood sugar, more adverse cholesterol levels—all sorts of things—that sort of becomes a perfect storm. Since 2011, we’ve now seen leveling off of those improvements in death rates and maybe even some reversal, which is unfortunate. We understand everything we need to know about preventing cardiovascular disease. As we actually implement that, we’ll expand healthy aging.
What does the future hold for the Framingham Heart Study?
Well, you may have heard that funding for science is a little difficult these days. But my hope would be that we would continue to represent the town of Framingham. I think there could be real value also for enrolling our fourth and our fifth generation.
The more we’ve studied the life course of all these chronic diseases, the more we’ve understood that every time we get a diagnosis, the horse is already partly out of the barn, if not all the way. So we need to get much, much earlier in the life course with prevention.
Read More: Your Brain Reveals a Lot About Your Age
I’ll leave you something hopeful. In another community-based study—a kind of descendant of the Framingham Heart Study—when they looked at how long people lived without cardiovascular disease, they found that lifestyle wins. Even people with high-risk genes, if they have a good lifestyle, they on average live 12 years longer than people with good genes but poor lifestyle habits. What’s more, they live 19 years longer on average without cardiovascular disease.
They not only extended their lifespan; they extended their healthspan substantially.
Genetics are not destiny. We can actually bend that curve, and people can do better if they can pursue these healthy lifestyle options. So much of this is actually in our control. But we need help: We need help from our food supply. We need help from good public-health policies so we are not exposed to indoor air that is contaminated by cigarette smoke. We need safe streets to go out and do physical activity. We need to actually be able to afford to buy fruits and vegetables.
A lot of this is policy that sets the stage. But there’s a lot in our control as well.
This article is part of TIME Longevity, an editorial platform dedicated to exploring how and why people are living longer and what this means for individuals, institutions, and the future of society. For other articles on this topic, click here.
Veronique Greenwood
Source link -
Treat the Cause | NutritionFacts.org
Treat the underlying cause of chronic lifestyle diseases.
It’s been said that more than 2,000 years ago, Hippocrates declared, “Let food be thy medicine and medicine be thy food.” In actuality, it appears that he never actually said those words, but there’s “no doubt about the relevance of food…and its role in health and disease states” in his writings. Regardless, 2,000 years ago, disease was thought to arise from a bad sense of “humors,” as you can see here and at 0:32 in my video Lifestyle and Disease Prevention: Your DNA Is Not Your Destiny.
Now, we have science, and there is “an overwhelming body of clinical and epidemiological evidence illustrating the dramatic impact of a healthy lifestyle on reducing all-cause mortality”—meaning death from all causes put together—“and preventing chronic diseases such as coronary heart disease, stroke, diabetes, and cancer.” But don’t those diseases just run in our family? What if we just have bad genes?
According to the esteemed former chair of nutrition at Harvard, for most of the diseases that have contributed “importantly” to mortality in Western peoples, we’ve long known that non-genetic factors often account for at least 80% to 90% of risk. We know this because rates of the leading killers, like major cancers and cardiovascular diseases, vary up to 100-fold around the world, and, “when groups migrate from low- to high-risk countries, their disease rates almost always change to those of the new environment.” Modifiable behavioral factors have been identified, “including specific aspects of diet, overweight, inactivity, and smoking that account for over 70% of stroke and colon cancer, over 80% of coronary heart disease, and over 90% of adult-onset [type 2] diabetes”—diseases that can largely be prevented by our own actions.
If most of the power is in our own hands, why do we allocate massively more resources to treatment than prevention? And speaking of prevention, “even preventive strategies are heavily biased towards pharmacology rather than supporting improvements in diet and lifestyle that could be more cost-effective. For example, treatment of [high] serum cholesterol with statins alone could cost approximately 30 billion dollars per year in the United States and would have only a modest impact on coronary heart disease incidence. The inherent problem is that most pharmacologic strategies don’t address the underlying causes of ill health in Western countries, which are not drug deficiencies.”
Ironically, the chronic diseases that are most amenable to lifestyle treatment are the same ones most profitably treated by drugs. Why? If you don’t change your diet, you have to pop the pills every day for the rest of your life. So, the cash-cow drugs are the very drugs we need the least. “Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy, physicians often do not follow these recommendations.” “By ignoring the root causes of disease and neglecting to prioritize lifestyle measures for prevention, the medical community is placing people at harm.”
“Traditional medical care relies primarily on the application of pharmacologic and surgical interventions after the development of illness,” whereas lifestyle medicine relies primarily on “the use of optimal nutrition (a whole foods, plant-based diet) and exercise in the prevention, arrest, and reversal of chronic conditions leading to premature disability and death. It looks in a holistic way at the underlying causes of illness.”
Dr. Adriane Fugh-Berman, director of PharmedOut, a wonderful organization I’m proud to support, wrote a great editorial entitled “Doctors Must Not Be Lapdogs to Drug Firms.” “The illusion that the relationship between medicine and the drug industry is collegial, professional, and personal is carefully maintained by the drug industry, which actually views all transactions with physicians in finely calculated financial terms…The drug industry is happy to play the generous and genial uncle until physicians want to discuss subjects that are off limits, such as the benefits of diet or exercise, or the relationship between medicine and pharmaceutical companies…Let us not be a lapdog to Big Pharma. Rather than sitting contentedly in our master’s lap, let us turn around and bite something tender.”
Doctor’s Note
The organization I mentioned, PharmedOut, is a project of Georgetown University Medical Center.
For more on Lifestyle Medicine, see related videos below.
Michael Greger M.D. FACLM
Source link -
9 Early Signs Of Dementia That Are Often Overlooked By Loved Ones
No. 5 may surprise you.