Why might healthy lifestyle choices wipe out 90% of our risk for having a heart attack, while drugs may only reduce risk by 20% to 30%?
On the standard American diet, atherosclerosis—hardening of the arteries, the number one killer of men and women—has been found to start in our teens. Investigators collected about 3,000 sets of coronary arteries and aortas (the aorta is the main artery in the body) from victims of accidents, homicides, and suicides who were 15 to 34 years old and found that the fatty streaks in arteries can begin forming in our teens, which turn into atherosclerotic plaques in our 20s that get worse in our 30s and can then become deadly. In the heart, atherosclerosis can cause a heart attack. In the brain, it can cause a stroke. See the progression below and at 0:35 in my video Can Cholesterol Get Too Low?.
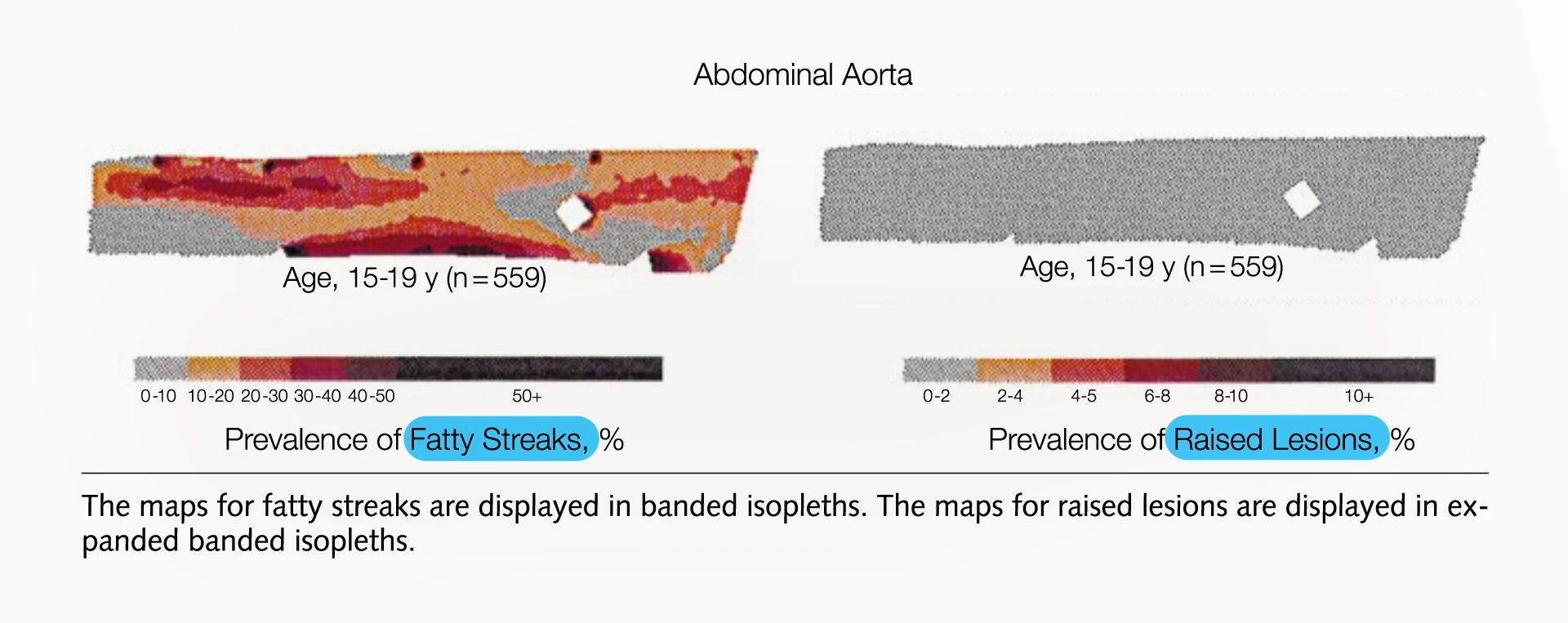
How common is this? All of the teens they looked at—100% of them—already had fatty streaks building up inside their arteries. By their early 30s, most already had those streaks blossoming into atherosclerotic plaques that bulged into their arteries. From ages 15 through 19, their aortas had fatty streaks building up throughout them, but no plaques yet, on average, as seen below and at 1:15 in my video.
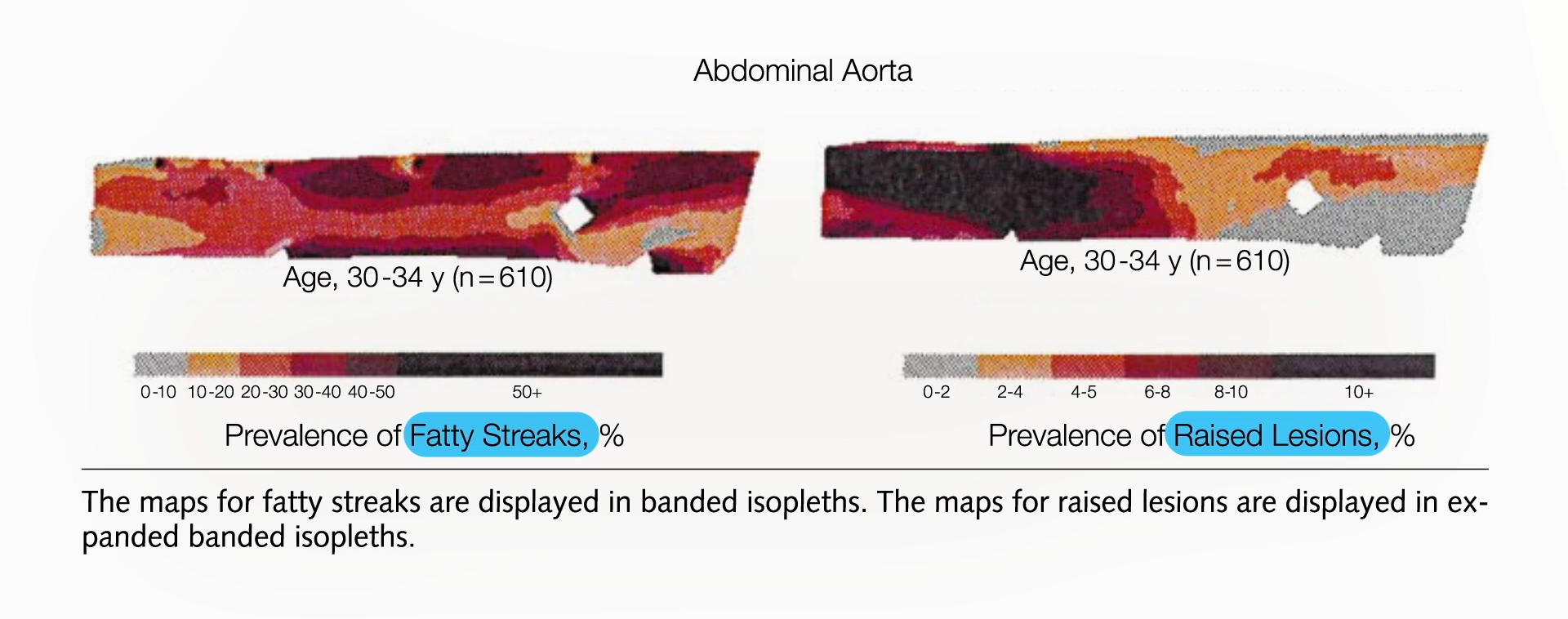
The plaques started appearing in their abdominal aorta in their early 20s and worsened by their late 20s, by which time fatty streaks had infiltrated throughout. By their early 30s, their arteries were in bad shape, as seen below and at 1:25 in my video.
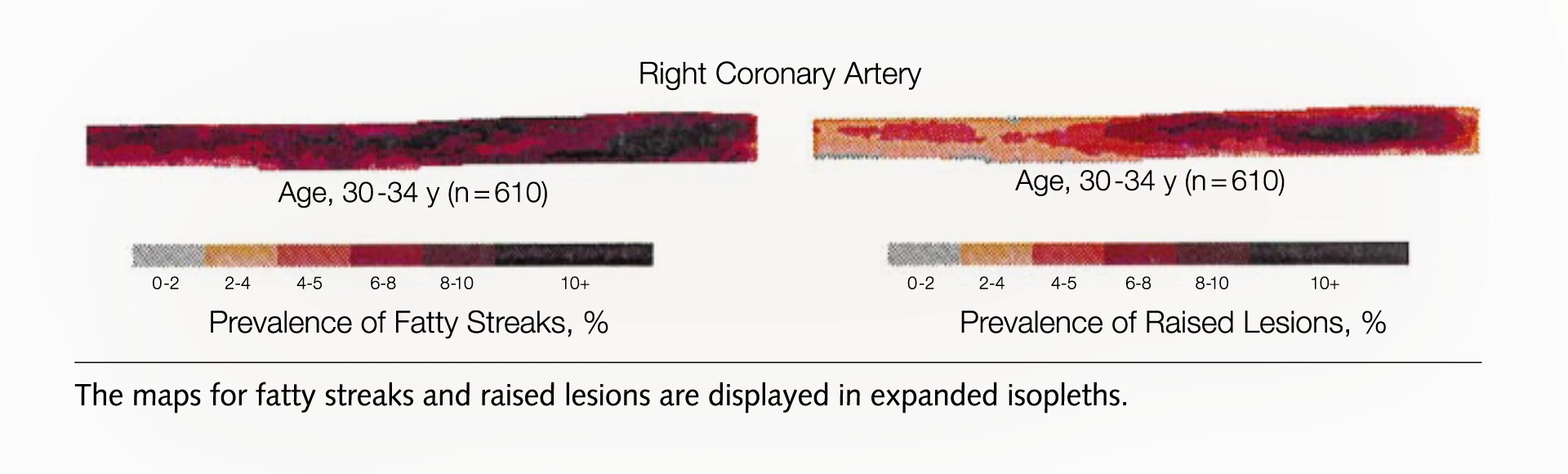
But that’s just the abdominal aorta, the main artery running through the torso that splits off into our legs. What about the coronary arteries that feed the heart?
Researchers found the same pattern: fatty streaks in teens, early signs of plaque in early 20s that progress with age, and by the early 30s, most people already had plaques in their coronary arteries, as seen below and at 1:47 in my video.
That’s why we shouldn’t wait until heart disease becomes symptomatic to treat it. If it starts in our youth, we should start treating it when we’re youths. If you knew you had a cancerous tumor, you wouldn’t want to wait until it grew to a certain size to treat it. If you had diabetes, you wouldn’t want to wait until you started going blind before you did something about it. So, how do you treat atherosclerosis? You lower LDL cholesterol through a diet low in saturated fat and cholesterol—a diet that’s low in eggs, meat, dairy, and junk.
If we want to stop this epidemic, we have to “alter our lifestyle accordingly, beginning in infancy or early childhood. Is such a radical proposal totally impractical?” (Eating more healthfully? Radical?!) It would take serious dedication to change our behavior, but atherosclerosis is our number one cause of death. In the case of cigarettes, we did pretty well, slashing smoking rates and dropping lung cancer rates. And, yes, healthy eating is safe. According to the Academy of Nutrition and Dietetics, the largest and oldest association of nutrition professionals in the world, even strictly plant-based diets are appropriate for all stages of life, starting from pregnancy. (NutritionFacts.org is among the websites recommended by the Academy for more information.)
The title of an important study published in the Journal of the American College of Cardiology declares: “Curing Atherosclerosis Should Be the Next Major Cardiovascular Prevention Goal.” What evidence do we have that a lifelong suppression of LDL will do it? There is a genetic mutation of a gene called PCSK9 that about 1 in 50 African Americans are lucky to be born with because it gives them about a 40% lower LDL cholesterol level their whole lives. Indeed, they were found to have dramatically lower rates of coronary heart disease—an 88% drop in risk compared to those without the genetic mutation, despite otherwise terrible cardiovascular risk factors on average. Most had high blood pressure and were overweight, almost a third smoked, and nearly 20% had diabetes, but that highlights how a lifelong history of low LDL cholesterol levels can substantially reduce the risk of coronary heart disease, even when there are multiple risk factors.
This near-90% drop in events like heart attacks or sudden death occurred at an average LDL level of 100 mg/dL, compared to 138 mg/dL in those without the genetic mutation. This means LDL can drop below even 100 mg/dL. Why does a drop in LDL cholesterol by about 40 mg/dL from a lucky genetic mutation lower the risk of coronary heart disease by nearly 90%, while the same reduction with statin drugs lowers it by only about 20%? The most probable explanation? Duration. When it comes to lowering LDL cholesterol, it’s not only about how low it is, but how long it’s been low.
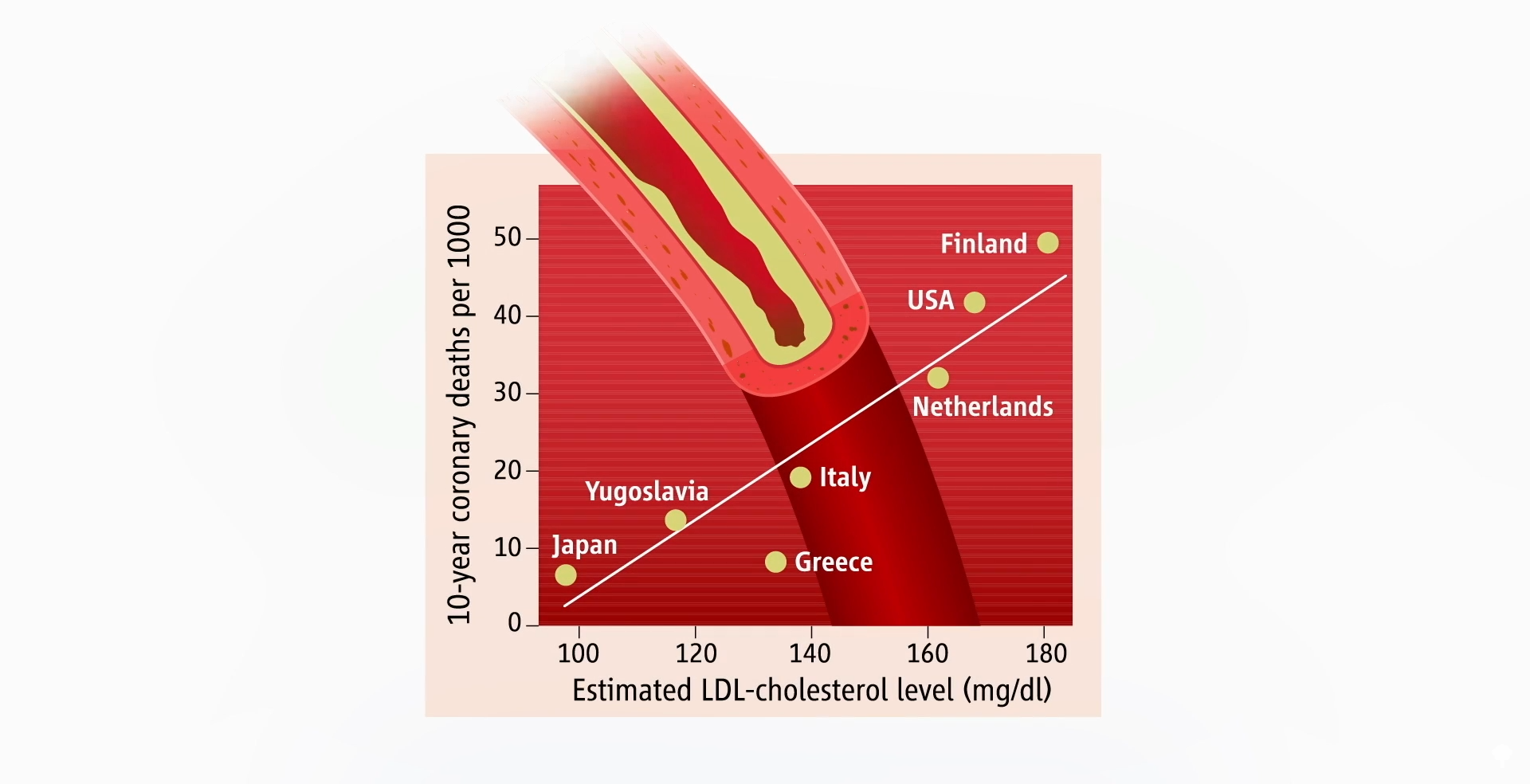
That’s why healthy lifestyle choices may wipe out about 90% of our risk for having a heart attack, while drugs may reduce it by only 20% to 30%. If you’re getting treated with drugs later in life, you may have to get your LDL under 70 mg/dL to halt the progression of coronary atherosclerosis. But if we start making healthier choices earlier, it may be enough to lower LDL cholesterol just to 100 mg/dL, which should be achievable for most of us. That’s consistent with country-by-country data that suggested death from heart disease would bottom out at a population average of about 100 mg/dL, as seen below and at 5:21 in my video.
But that’s only if you can keep your LDL cholesterol down your whole life.
If you’re relying on medication later in life to halt disease progression, you may need to get your LDL below 70 mg/dL, and if you’re trying to use drugs to reverse a lifetime of bad food choices, you may not get to zero coronary heart disease events until your LDL drops to about 55 mg/dL. If your heart disease is so bad that you’ve already had a heart attack but you’re trying not to die from another one, ideally, you might want to push your LDL down to about 30 mg/dL. Once you get that low, not only would you likely prevent any new atherosclerotic plaques, but you’d also help stabilize the plaques you already have so they’re less likely to burst open and kill you.
Is it even safe to have cholesterol levels that low, though? In other words, can LDL cholesterol ever be too low? We’ll find out next.
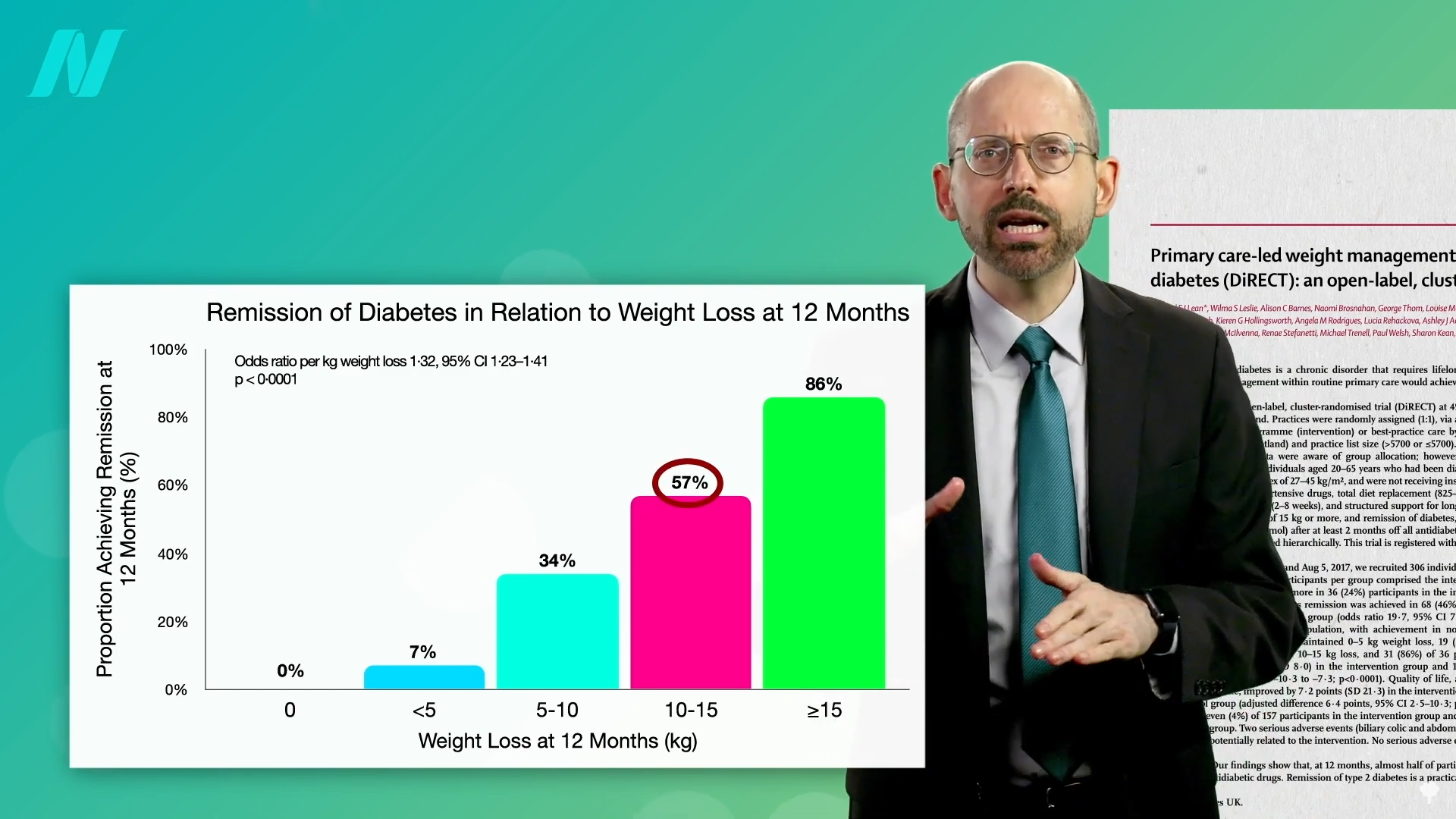
By losing 15% of their body weight, nearly 90% of those who have had type 2 diabetes for less than four years may achieve remission.
Currently, more than half a billion adults have diabetes, and about a 50% increase is expected in another generation. I’ve got tons of videos on the best diets for diabetes, but what about no diet at all?
More than a century ago, fasting was said to cure diabetes, quickly halting its progression and eliminating all signs of the disease within days or weeks. Even so, starvation is guaranteed to lead to the complete disappearance of you if kept up long enough. What’s the point of fasting away the pounds if they’re just going to return as soon as you restart the diet that created them in the first place? Might it be useful to kickstart a healthier diet? Let’s see what the science says.
Type 2 diabetes has long been recognized as a disease of excess, once thought to afflict only “the idle rich…anyone whose environment and self-support does not require of him some sustained vigorous bodily exertion every day, and whose earnings or income permit him, and whose inclination tempts him, to eat regularly more than he needs.” Diabetes is preventable, so might it also be treatable? If we’re dying from overeating, maybe we can be saved by undereating. Remarkably, this idea was proposed about 2,000 years ago in an Ayurvedic text:
“Poor diabetic people’s medicine He should live like a saint (Munni); He should walk for 800–900 miles. Or he shall dig a pond; Or he shall live only on cow dung and cow urine.”
That reminds me of the Rollo diet for diabetes proposed in 1797, which was composed of rancid meat. That was on top of the ipecac-like drugs he used to induce severe sickness and vomiting. Anything that makes people sick has only “a temporary effect in relieving diabetes” because it reduces the amount of food eaten. His diet plan—which included congealed blood for lunch and spoiled meat for dinner—certainly had that effect.
Similar benefits were seen in people with diabetes during the siege of Paris in the Franco‐Prussian War, leading to the advice to mangez le moins possible, which translates to “eat as little as possible.” This was formalized into the Allen starvation treatment, considered to be “the greatest advance in the treatment of diabetes prior to the discovery of insulin.” Before insulin, there was “The Allen Era.”
Dr. Allen noted that there are clinical reports of even severe diabetes cases clearing up after the onset of a “wasting condition” like tuberculosis or cancer, so he decided to put it to the test. He found that even in the most severe type of diabetes, he could clear sugar from people’s urine within ten days. Of course, that’s the easy part; it’s harder to maintain once they start eating again. To manage patients’ diabetes, he stuck to two principles: Keep them underweight and restrict the fat in their diet. A person with severe diabetes can be symptom-free for days or weeks, but eating butter or olive oil can make the disease come raging back.
As I’ve said before, diabetes is a disease of fat toxicity. Infuse fat into people’s veins through an IV, and, by using a high-tech type of MRI scanner, you can show in real time the buildup of fat in muscle cells within hours, accompanied by an increase in insulin resistance. The same thing happens when you put people on a high-fat diet for three days. It can even happen in just one day. Even a single meal can increase insulin resistance within six hours. Acute dietary fat intake rapidly increases insulin resistance. Why do we care? Insulin resistance in our muscles, in the context of too many calories, can lead to a buildup of liver fat, followed by fat accumulation in the pancreas, and eventually full-blown diabetes. “Type 2 diabetes can now be understood as a state of excess fat in the liver and pancreas, and remains reversible for at least 10 years in most individuals.”
When people are put on a very low-calorie diet—700 calories a day—fat can get pulled out of their muscle cells, accompanied by a corresponding boost in insulin sensitivity, as shown below and at 4:43 in my video Fasting to Reverse Diabetes.
The fat buildup in the liver has then been shown to decrease substantially, and if the diet is continued, the excess fat in the pancreas also reduces. If caught early enough, reversing type 2 diabetes is possible, which would mean sustained healthy blood sugar levels on a healthy diet.
With the loss of 15% of body weight, nearly 90% of individuals who have had type 2 diabetes for less than four years can achieve non-diabetic blood sugar levels, whereas it may only be reversible in 50% of those who’ve lived with the disease for longer than eight years. That’s better than bariatric surgery, where those losing even more weight had lower remission rates of 62% and 26%, respectively. Your forks are better than surgeons’ knives. Indeed, most people who have had their type 2 diabetes diagnosis for an average of three years can reverse their disease after losing about 30 pounds, as you can see below and at 5:37 in my video.
Of course, an extended bout of physician-supervised, water-only fasting could also get you there, but you would have to maintain that weight loss. One of the things that has been said with “certainty” is that if you regain the weight, you regain your diabetes.
To bring it full circle, “the initial euphoria about ‘medicine’s greatest miracle’”—the discovery of insulin in 1921—“soon gave way to the realisation” that, while it was literally life-saving for people with type 1 diabetes, insulin alone wasn’t enough to prevent such complications as blindness, kidney failure, stroke, and amputations in people with type 2 diabetes. That’s why one of the most renowned pioneers in diabetes care, Elliott Joslin, “argued that self-discipline on diet and exercise, as it was in the days prior to the availability of the drug [insulin], should be central to the management of diabetes….”
The American Medical Association passed a resolution encouraging hospitals to offer healthy plant-based food options.
“Globally, 11 million deaths annually are attributable to dietary factors, placing poor diet ahead of any other risk factor for death in the world.” Given that diet is our leading killer, you’d think that nutrition education would be emphasized during medical school and training, but there is a deficiency. A systematic review found that, “despite the centrality of nutrition to a healthy lifestyle, graduating medical students are not supported through their education to provide high-quality, effective nutrition care to patients…”
It could start in undergrad. What’s more important? Learning about humanity’s leading killer or organic chemistry?
In medical school, students may average only 19 hours of nutrition out of thousands of hours of instruction, and they aren’t even being taught what’s most useful. How many cases of scurvy and beriberi, diseases of dietary deficiency, will they encounter in clinical practice? In contrast, how many of their future patients will be suffering from dietary excesses—obesity, diabetes, hypertension, and heart disease? Those are probably a little more common than scurvy or beriberi. “Nevertheless, fully 95% of cardiologists [surveyed] believe that their role includes personally providing patients with at least basic nutrition information,” yet not even one in ten feels they have an “expert” grasp on the subject.
If you look at the clinical guidelines for what we should do for our patients with regard to our number one killer, atherosclerotic cardiovascular disease, all treatment begins with a healthy lifestyle, as shown below and at 1:50 in my video Hospitals with 100-Percent Plant-Based Menus.
“Yet, how can clinicians put these guidelines into practice without adequate training in nutrition?”
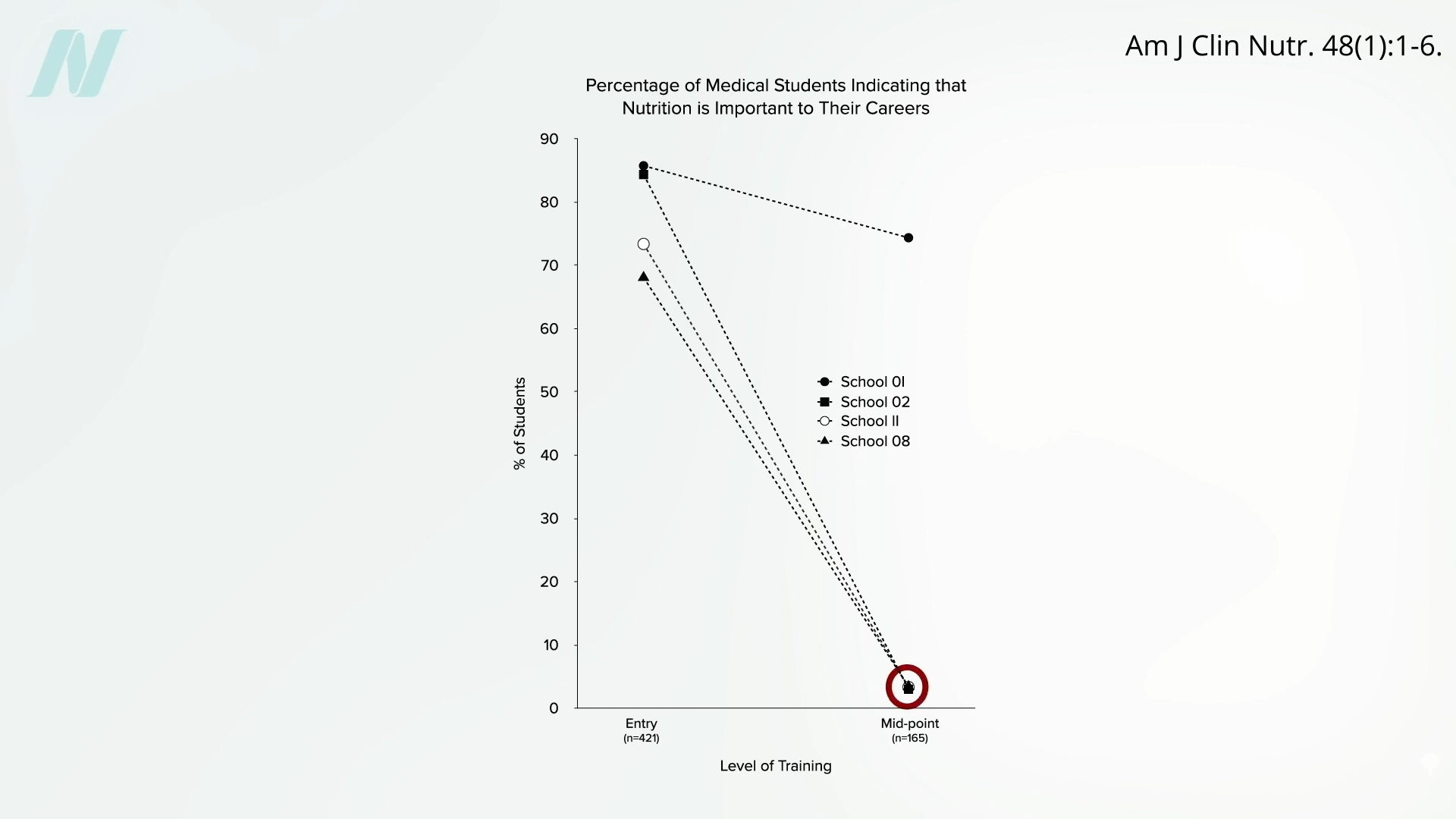
Less than half of medical schools report teaching any nutrition in clinical practice. In fact, they may be effectively teaching anti-nutrition, as “students typically begin medical school with a greater appreciation for the role of nutrition in health than when they leave.” Below and at 2:36 in my video is a figure entitled “Percentage of Medical Students Indicating that Nutrition is Important to Their Careers.” Upon entry to different medical schools, about three-quarters on average felt that nutrition is important to their careers. Smart bunch. Then, after two years of instruction, they were asked the same question, and the numbers plummeted. In fact, at most schools, it fell to 0%. Instead of being educated, they got de-educated. They had the notion that nutrition is important washed right out of their brains. “Thus, preclinical teaching”— the first two years of medical school—“engenders a loss of a sense of the relevance of the applied discipline of nutrition.”
Following medical school, during residency, nutrition education is “minimal or, more typically, absent.” “Major updates” were released in 2018 for residency and fellowship training requirements, and there were zero requirements for nutrition. “So you could have an internal medicine graduate who comes out of a terrific program and has learned nothing—literally nothing—about nutrition.”
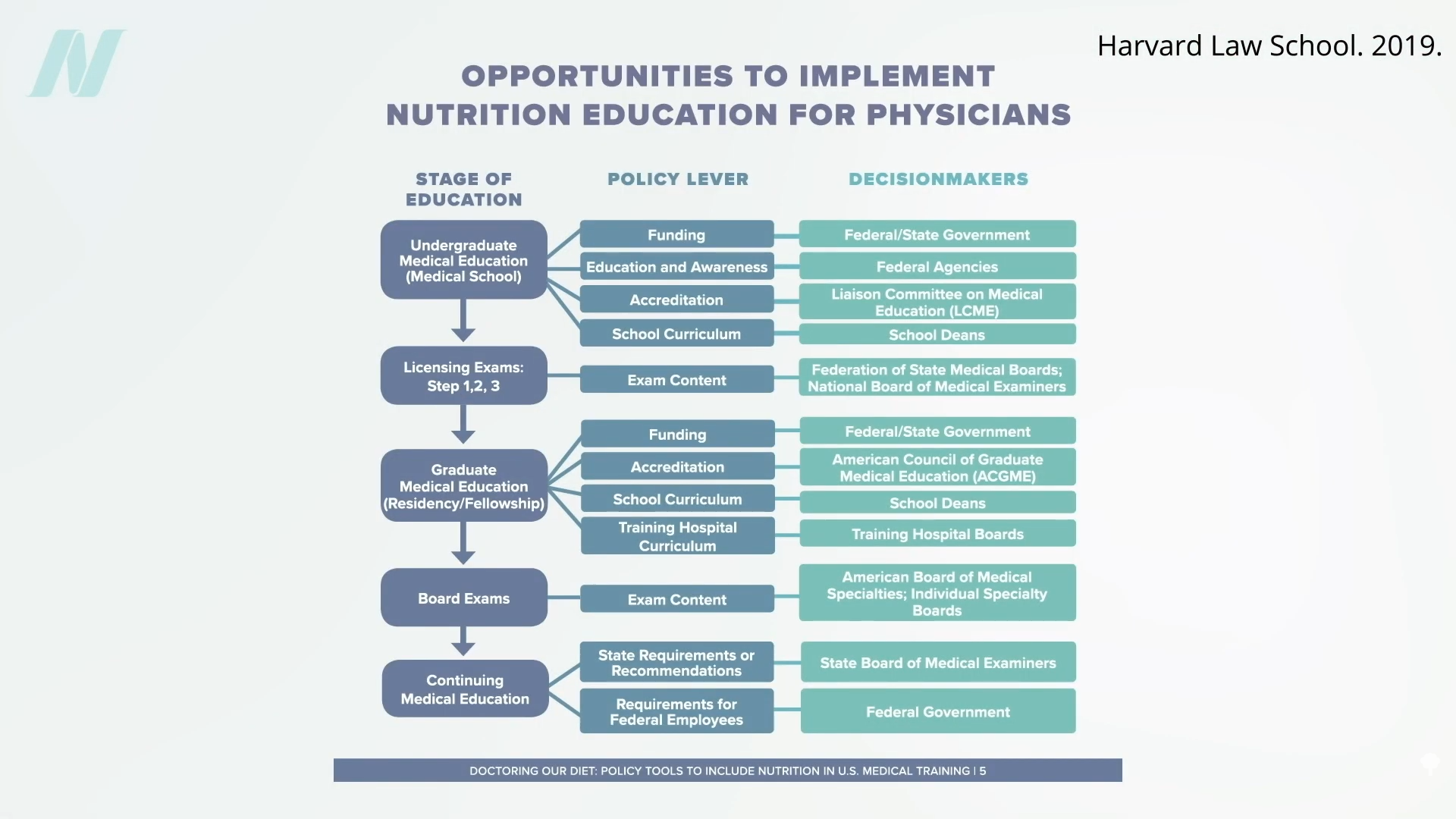
“Why is diet not routinely addressed in both medical education and practice already, and what should be done about that?” One of the “reasons for the medical silence in nutrition” is that, “sadly…nutrition takes a back seat…because there are few financial incentives to support it.” What can we do about that? The Food Law and Policy Clinic at Harvard Law School identified a dozen different policy levers at all stages of medical education and the kinds of policy recommendations there could be for the decision-makers, as you can see here and at 3:48 in my video.
For instance, the government could require doctors working for Veterans Affairs (VA) to get at least some courses in nutrition, or we could put questions about nutrition on the board exams so schools would be pressured to teach it. As we are now, even patients who have just had a heart attack aren’t changing their diet. Doctors may not be telling them to do so, and hospitals may be actively undermining their future with the food they serve.
The good news is that the American Medical Association (AMA) has passed a resolution encouraging hospitals to offer healthy food options. What a concept! “Our AMA hereby calls on [U.S.] Health Care Facilities to improve the health of patients, staff, and visitors by: (a) providing a variety of healthy food, including plant-based meals, and meals that are low in saturated and trans fat, sodium, and added sugars; (b) eliminating processed meats from menus; and (c) providing and promoting healthy beverages.” Nice!
“Similarly, in 2018, the State of California mandated the availability of plant-based meals for hospital patients,” and there are hospitals in Gainesville (FL), the Bronx, Manhattan, Denver, and Tampa (FL) that “all provide 100% plant-based meals to their patients on a separate menu and provide educational materials to inpatients to improve education on the role of diet, especially plant-based diets, in chronic illness.”
Let’s check out some of their menu offerings: How about some lentil Bolognese? Or a cauliflower scramble with baked hash browns for breakfast, mushroom ragu for lunch, and, for supper, white bean stew, salad, and fruit for dessert. (This is the first time a hospital menu has ever made me hungry!)
The key to these transformations was “having a physician advocate and increasing education of staff and patients on the benefits of eating more plant-based foods.” A single clinician can spark change in a whole system, because science is on their side. “Doctors have a unique position in society” to influence policy at all levels; it’s about time we used it.
For more on the ingrained ignorance of basic clinical nutrition in medicine, see the related posts below.
Treat the underlying cause of chronic lifestyle diseases.
It’s been said that more than 2,000 years ago, Hippocrates declared, “Let food be thy medicine and medicine be thy food.” In actuality, it appears that he never actually said those words, but there’s “no doubt about the relevance of food…and its role in health and disease states” in his writings. Regardless, 2,000 years ago, disease was thought to arise from a bad sense of “humors,” as you can see here and at 0:32 in my video Lifestyle and Disease Prevention: Your DNA Is Not Your Destiny.
Now, we have science, and there is “an overwhelming body of clinical and epidemiological evidence illustrating the dramatic impact of a healthy lifestyle on reducing all-cause mortality”—meaning death from all causes put together—“and preventing chronic diseases such as coronary heart disease, stroke, diabetes, and cancer.” But don’t those diseases just run in our family? What if we just have bad genes?
According to the esteemed former chair of nutrition at Harvard, for most of the diseases that have contributed “importantly” to mortality in Western peoples, we’ve long known that non-genetic factors often account for at least 80% to 90% of risk. We know this because rates of the leading killers, like major cancers and cardiovascular diseases, vary up to 100-fold around the world, and, “when groups migrate from low- to high-risk countries, their disease rates almost always change to those of the new environment.” Modifiable behavioral factors have been identified, “including specific aspects of diet, overweight, inactivity, and smoking that account for over 70% of stroke and colon cancer, over 80% of coronary heart disease, and over 90% of adult-onset [type 2] diabetes”—diseases that can largely be prevented by our own actions.
If most of the power is in our own hands, why do we allocate massively more resources to treatment than prevention? And speaking of prevention, “even preventive strategies are heavily biased towards pharmacology rather than supporting improvements in diet and lifestyle that could be more cost-effective. For example, treatment of [high] serum cholesterol with statins alone could cost approximately 30 billion dollars per year in the United States and would have only a modest impact on coronary heart disease incidence. The inherent problem is that most pharmacologic strategies don’t address the underlying causes of ill health in Western countries, which are not drug deficiencies.”
Ironically, the chronic diseases that are most amenable to lifestyle treatment are the same ones most profitably treated by drugs. Why? If you don’t change your diet, you have to pop the pills every day for the rest of your life. So, the cash-cow drugs are the very drugs we need the least. “Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy, physicians often do not follow these recommendations.” “By ignoring the root causes of disease and neglecting to prioritize lifestyle measures for prevention, the medical community is placing people at harm.”
“Traditional medical care relies primarily on the application of pharmacologic and surgical interventions after the development of illness,” whereas lifestyle medicine relies primarily on “the use of optimal nutrition (a whole foods, plant-based diet) and exercise in the prevention, arrest, and reversal of chronic conditions leading to premature disability and death. It looks in a holistic way at the underlying causes of illness.”
Dr. Adriane Fugh-Berman, director of PharmedOut, a wonderful organization I’m proud to support, wrote a great editorial entitled “Doctors Must Not Be Lapdogs to Drug Firms.” “The illusion that the relationship between medicine and the drug industry is collegial, professional, and personal is carefully maintained by the drug industry, which actually views all transactions with physicians in finely calculated financial terms…The drug industry is happy to play the generous and genial uncle until physicians want to discuss subjects that are off limits, such as the benefits of diet or exercise, or the relationship between medicine and pharmaceutical companies…Let us not be a lapdog to Big Pharma. Rather than sitting contentedly in our master’s lap, let us turn around and bite something tender.”
Doctor’s Note
The organization I mentioned, PharmedOut, is a project of Georgetown University Medical Center.
For more on Lifestyle Medicine, see related videos below.
What is the dirty little secret of drugs for lifestyle diseases?
Drug companies go out of their way—in direct-to-consumer ads, for example—to “present pharmaceutical drugs as a preferred solution to cholesterol management while downplaying lifestyle change.” You see this echoed in the medical literature, as in this editorial in the Journal of the American Medical Association: “Despite decades of exhortation for improvement, the high prevalence of poor lifestyle behaviors leading to elevated cardiovascular disease risk factors persists, with myocardial infarction [heart attack] and stroke remaining the leading causes of death in the United States. Clearly, many more adults could benefit from…statins for primary prevention.” Do we really need to put more people on drugs? A reply was published in the British Medical Journal: “Once again, doctors are implored to ‘get real’—stop hoping that efforts to help their patients and communities adopt healthy lifestyle habits will succeed, and start prescribing more statins. This is a self-fulfilling prophecy. Note that the author of these comments [the pro-statin editorial] disclosed receipt of funding from 11 drug companies, at least four of which produce or are developing new classes of cholesterol-lowering agents,” which make billions of dollars a year in annual sales.
Every time the cholesterol guidelines expand the number of people eligible for statins, they’re decried as a “big kiss to big pharma.” This is understandable, since the majority of guideline panel members “had industry ties,” financial conflicts of interest. But these days, all the major statins are off-patent, so there are inexpensive generic versions. For example, the safest, most effective statin is generic Lipitor, sold as atorvastatin for as little as a few dollars a month. So, nowadays, the cholesterol guidelines are not necessarily “part of an industry plot.”
“The US way of life is the problem, not the guidelines…” The reason so many people are candidates for cholesterol- and blood-pressure-lowering medications is that so many people are taking such terrible care of themselves. The bottom line is that “individuals must take more responsibility for their own health behaviors.” What if you are unwilling or unable to improve your diet and make lifestyle changes to bring down that risk? If your ten-year risk of having a heart attack is 7.5 percent or more and going to stay that way, then the benefits of taking a statin drug likely outweigh the risk. That’s really for you to decide, though. It’s your body, your choice.
“Whether or not the overall benefit-harm balance justifies the use of a medication for an individual patient cannot be determined by a guidelines committee, a health care system, or even the attending physician. Instead, it is the individual patient who has a fundamental right to decide whether or not taking a drug is worthwhile.” This was recognized by some of medicine’s “historical luminaries such as Hippocrates,” but “only in recent decades has the medical profession begun to shift from a paternalistic ‘doctor knows best’ stance towards one explicitly endorsing patient-centered, evidence-based, shared decision-making.” One of the problems with communicating statin evidence to support this shared decision-making is that most doctors “have a poor understanding of concepts of risk and probability and…increasing exposure to statistics in undergraduate and postgraduate education hasn’t made much difference.” But that understanding is critical for preventive medicine. When doctors offer a cholesterol-lowering drug, “they’re doing something quite different from treating a patient who has sought help because she is sick. They’re not so much doctors as life insurance salespeople, peddling deferred benefits in exchange for a small (but certainly not negligible) ongoing inconvenience and cost. In this new kind of medicine, not understanding risk is the equivalent of not knowing about the circulation of the blood or basic anatomy. So, let’s dive in and see exactly what’s at stake.
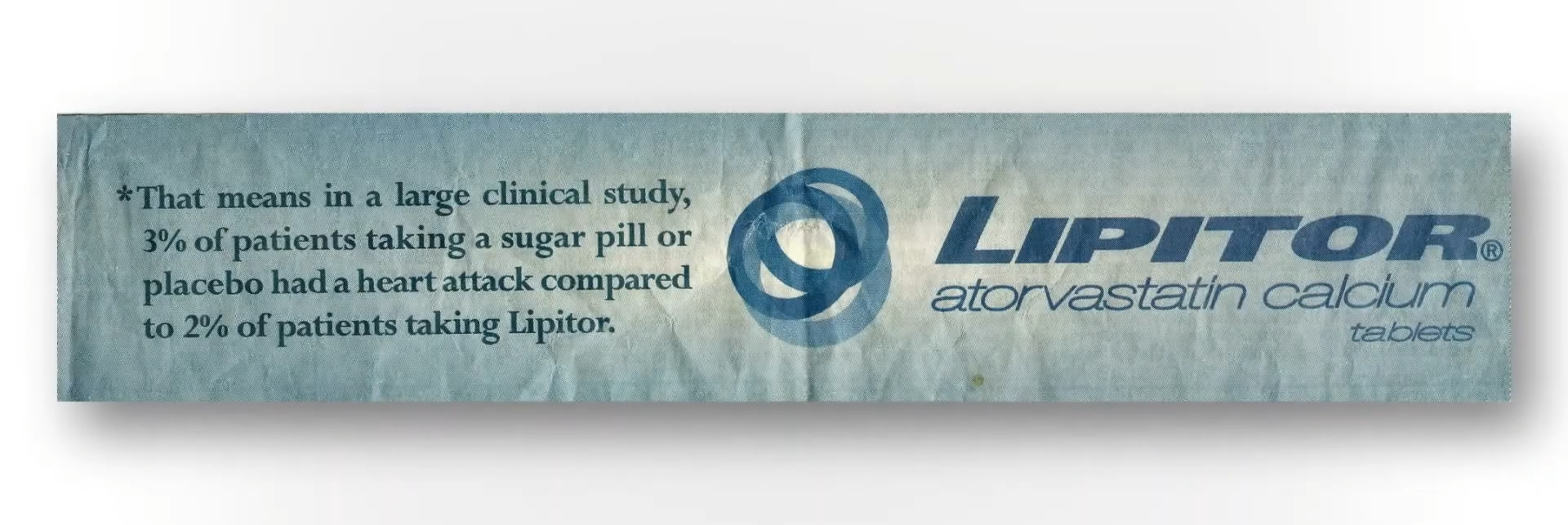
If you follow the asterisk I’ve circled after the “36%” in the ad, you can see how they came up with that. I’ve included it here and at 3:56 in my video. In a large clinical study, 3 percent of patients not taking the statin had a heart attack within a certain amount of time, compared to 2 percent of patients who did take the drug. So, the drug dropped heart attack risk from 3 percent to 2 percent; that’s about a one-third drop, hence the 36 percent reduced relative risk statistic. But another way to look at going from 3 percent to 2 percent is that the absolute risk only dropped by 1 percent. So, in effect, “your chance to avoid a nonfatal heart attack during the next 2 years is about 97% without treatment, but you can increase it to about 98% by taking a Crestor [a statin] every day.” Another way to say that is that you’d have to treat 100 people with the drug to prevent a single heart attack. That statistic may shock a lot of people.
If you ask patients what they’ve been led to believe, they don’t think the chance of avoiding a heart attack within a few years on statins is 1 in 100, but 1 in 2. “On average, it was believed that most patients (53.1%) using statins would avoid a heart attack after statin treatment for 5 years.” Most patients, not just 1 percent of patients. And this “disparity between actual and expected effect could be viewed as a dilemma. On the one hand, it is not ethically acceptable for caregivers to deliberately support and maintain illusive treatment expectations by patients.” We cannot mislead people into thinking a drug works better than it really does, but on the other hand, how else are we going to get people to take their pills?
When asked, people want an absolute risk reduction of at least about 30 percent to take a cholesterol-lowering drug every day, whereas the actual absolute risk reduction is only about 1 percent. So, the dirty little secret is that, if patients knew the truth about how little these drugs actually worked, almost no one would agree to take them. Doctors are either not educating their patients or actively misinforming them. Given that the majority of patients expect a much larger benefit from statins than they’d get, “there is a tension between the patient’s right to know about benefiting from a preventive drug and the likely reduction in uptake [willingness to take the drugs] if they are so informed,” and learn the truth. This sounds terribly paternalistic, but hundreds of thousands of lives may be at stake.
If patients were fully informed, people would die. About 20 million Americans are on statins. Even if the drugs saved 1 in 100, that could mean hundreds of thousands of lives lost if everyone stopped taking their statins. “It is ironic that informing patients about statins would increase the very outcomes they were designed to prevent.”
How can you calculate your own personal heart disease risk to help you determine if you should start on a cholesterol-lowering statin drug?
The muscle-related side effects from cholesterol-lowering statins “are often severe enough for patients to stop taking the drug. Of course, these side effects could be coincidental or psychosomatic and have nothing to do with the drug,” given that many clinical trials show such side effects are rare. “It is also possible that previous clinical trials”—funded by the drug companies themselves—“under-recorded the side effects of statins.” The bottom line is that there’s an urgent need to establish the true incidence of statin side effects.
“What proportion of symptomatic side effects in patients taking statins are genuinely caused by the drug?” That’s the title of a journal article that reports that, even in trials funded by Big Pharma, “only a small minority of symptoms reported on statins are genuinely due to the statins,” and those taking statins are significantly more likely to develop type 2 diabetes than those randomized to placebo sugar pills. Why? We’re still not exactly sure, but statins may have the double-whammy effect of impairing insulin secretion from the pancreas while also diminishing insulin’s effectiveness by increasing insulin resistance.
Even short-term use of statins may “approximately double the odds of developing diabetes and diabetic complications.” As shown below and at 1:49 in my video Who Should Take Statins?, fewer people develop diabetes and diabetic complications off statins over a period of about five years than those who do develop diabetes while on statins. “Of more concern, this increased risk persisted for at least 5 years after statin use stopped.”
“In view of the overwhelming benefit of statins in the reduction of cardiovascular events,” the number one killer of men and women, any increase in risk of diabetes, our seventh leading cause of death, would be outweighed by any cardiovascular benefits, right? That’s a false dichotomy. We don’t have to choose between heart disease and diabetes. We can treat the cause of both with the same diet and lifestyle changes. The diet that can not only stop heart disease, but also reverse it, is the same one that can reverse type 2 diabetes. But what if, for whatever reason, you refuse to change your diet and lifestyle? In that case, what are the risks and benefits of starting statins? Don’t expect to get the full scoop from your doctor, as most seemed clueless about statins’ causal link with diabetes, so only a small fraction even bring it up with their patients.
“Overall, in patients for whom statin treatment is recommended by current guidelines, the benefits greatly outweigh the risks.” But that’s for you to decide. Before we quantify exactly what the risks and benefits are, what exactly are the recommendations of current guidelines?
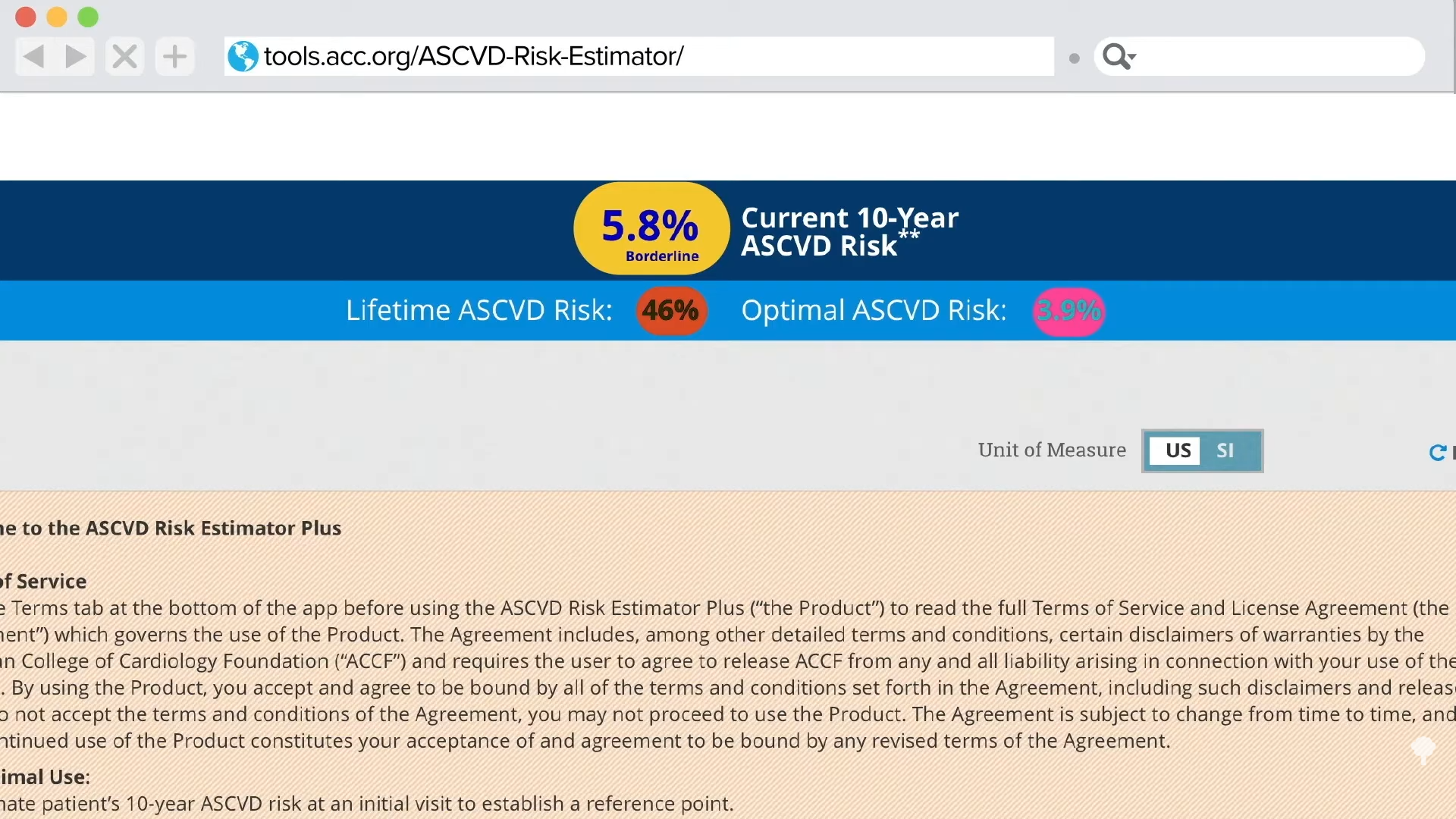
How should you decide if a statin is right for you? “If you have a history of heart disease or stroke, taking a statin medication is recommended, without considering your cholesterol levels.” Period. Full stop. No discussion needed. “If you do not yet have any known cardiovascular disease,” then the decision should be based on calculating your own personal risk. If you know your cholesterol and blood pressure numbers, it’s easy to do that online with the American College of Cardiology risk estimator or the Framingham risk profiler.
My favorite is the American College of Cardiology’s estimator because it gives you your current ten-year risk and also your lifetime risk. So, for a person with a 5.8 percent risk of having a heart attack or stroke within the next decade, if they don’t clean up their act, that lifetime risk jumps to 46 percent, nearly a flip of the coin. If they improved their cholesterol and blood pressure, though, they could reduce that risk by more than tenfold, down to 3.9 percent, as shown below and at 4:11 in my video.
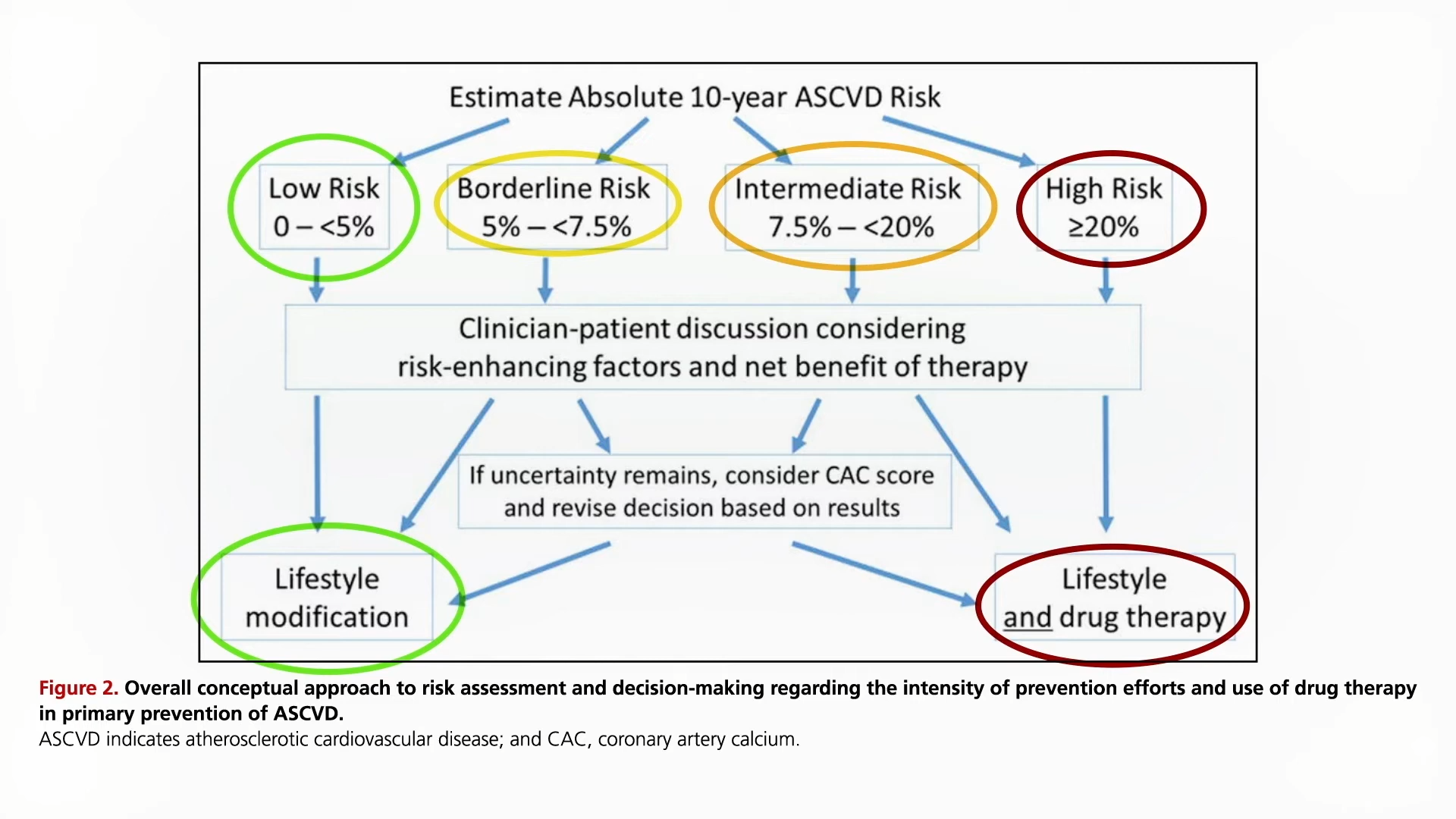
Since the statin decision is based on your ten-year risk, what do you do with that number? As you can see here and at 4:48 in my video, under the current guidelines, if your ten-year risk is under 5 percent, then, unless there are extenuating circumstances, you should just stick to diet, exercise, and smoking cessation to bring down your numbers. In contrast, if your ten-year risk hits 20 percent, then the recommendation is to add a statin drug on top of making lifestyle modifications. Unless there are risk-enhancing factors, the tendency is to stick with lifestyle changes if risk is less than 7.5 percent and to move towards adding drugs if above 7.5 percent.
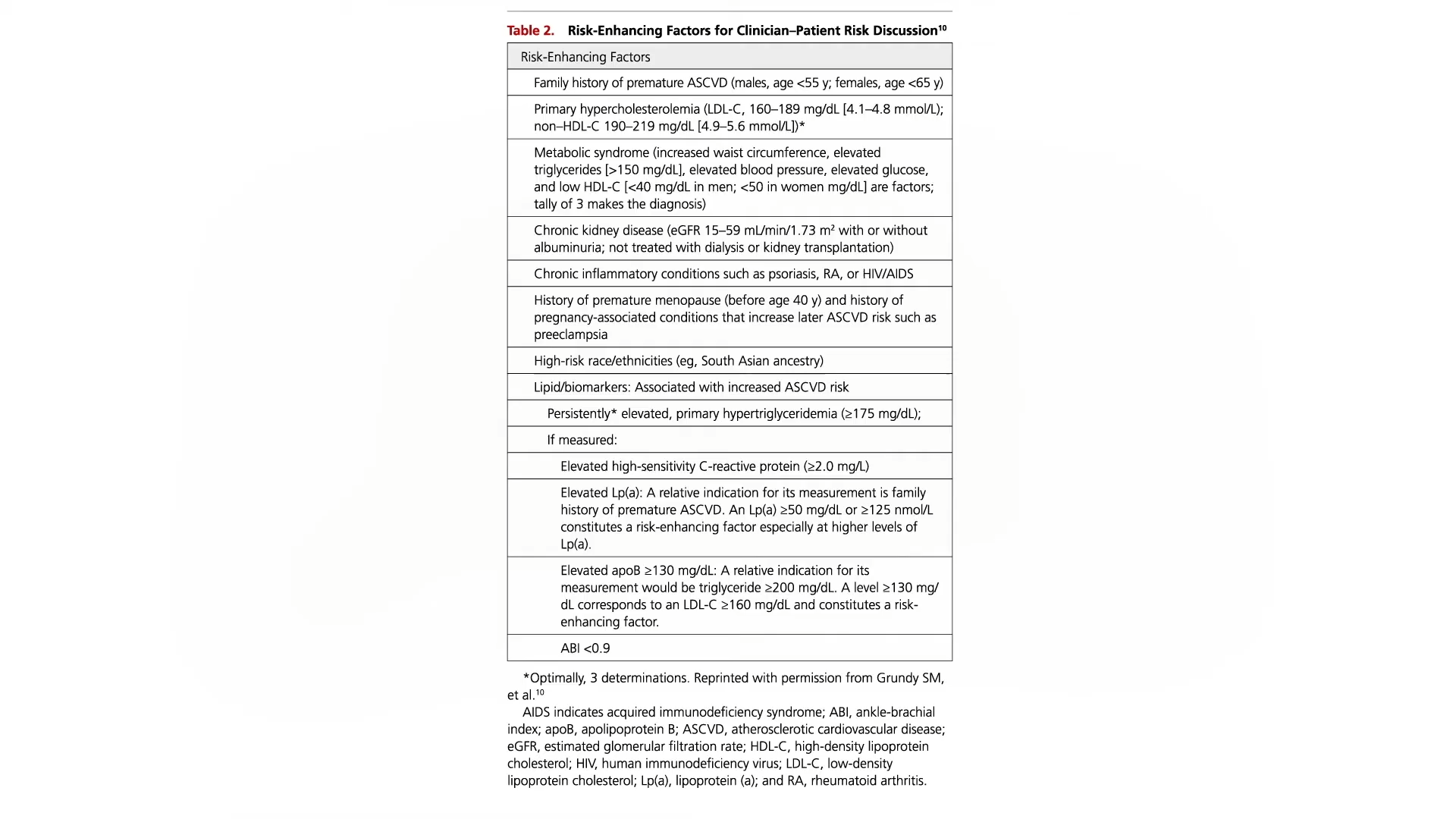
Risk-enhancing factors that your doctor should take into account when helping you make the decision include a bad family history, really high LDL cholesterol, metabolic syndrome, chronic kidney or inflammatory conditions, or persistently high triglycerides, C-reactive protein, or LP(a). You can see the whole list here and at 4:54 in my video.
If you’re still uncertain, guidelines suggest you consider getting a coronary artery calcium (CAC) score, but even though the radiation exposure from that test is relatively low these days, the U.S. Preventive Services Task Force has explicitly concluded that the current evidence is insufficient to conclude that the benefits outweigh the harms.
Do you know more about basic nutrition than most doctors?
“A poor diet now outranks smoking as the leading cause of death globally and in the United States, according to the latest data.” The top killer of Americans is the American diet, as you can see below and at 0:23 in my video How Much Do Doctors Actually Know About Nutrition?.
If diet is humanity’s number one killer, then, obviously, nutrition is the number one subject taught in medical school, right? Sadly, “medical students around the world [are] poorly trained in nutrition.” It isn’t that medical students aren’t interested in learning about it. In fact, “interest in nutrition was ‘uniformly high’ among medical students,” but medical schools just aren’t teaching it. “Without a solid foundation of clinical nutrition knowledge and skills, physicians worldwide are generally not equipped to even begin to have an informed nutrition conversation with their patients….”
How bad is it? One study, “Assessing the clinical nutrition knowledge of medical doctors,” found the majority of participants got 70 percent of the questions wrong—and they were multiple choice questions, so they should have gotten about a fifth of them right just by chance. “Wrong answers in the…knowledge test were not limited to difficult or demanding questions” either. For example, less than half of the doctors were able to guess how many calories are in fat, carbohydrates, and protein; only one in ten knew the recommended protein intake; and only about one in three knew what a healthy body mass index (BMI) was. We’re talking about really basic nutrition knowledge.
Even worse, not only did the majority of medical doctors get a failing grade, but 30 percent of those who failed had “a high self-perception of their CN [clinical nutrition] expertise.” They weren’t only clueless about nutrition; they were clueless that they were clueless about nutrition, a particularly bad combination given that doctors are “trusted and influential sources” of healthy eating advice. “For those consumers who get information from their personal healthcare professional, 78% indicate making a change in their eating habits as a result of those conversations.” So, if the doctor got everything they know from some article in a magazine while waiting in the grocery store checkout aisle, that’s what the patients will be following.
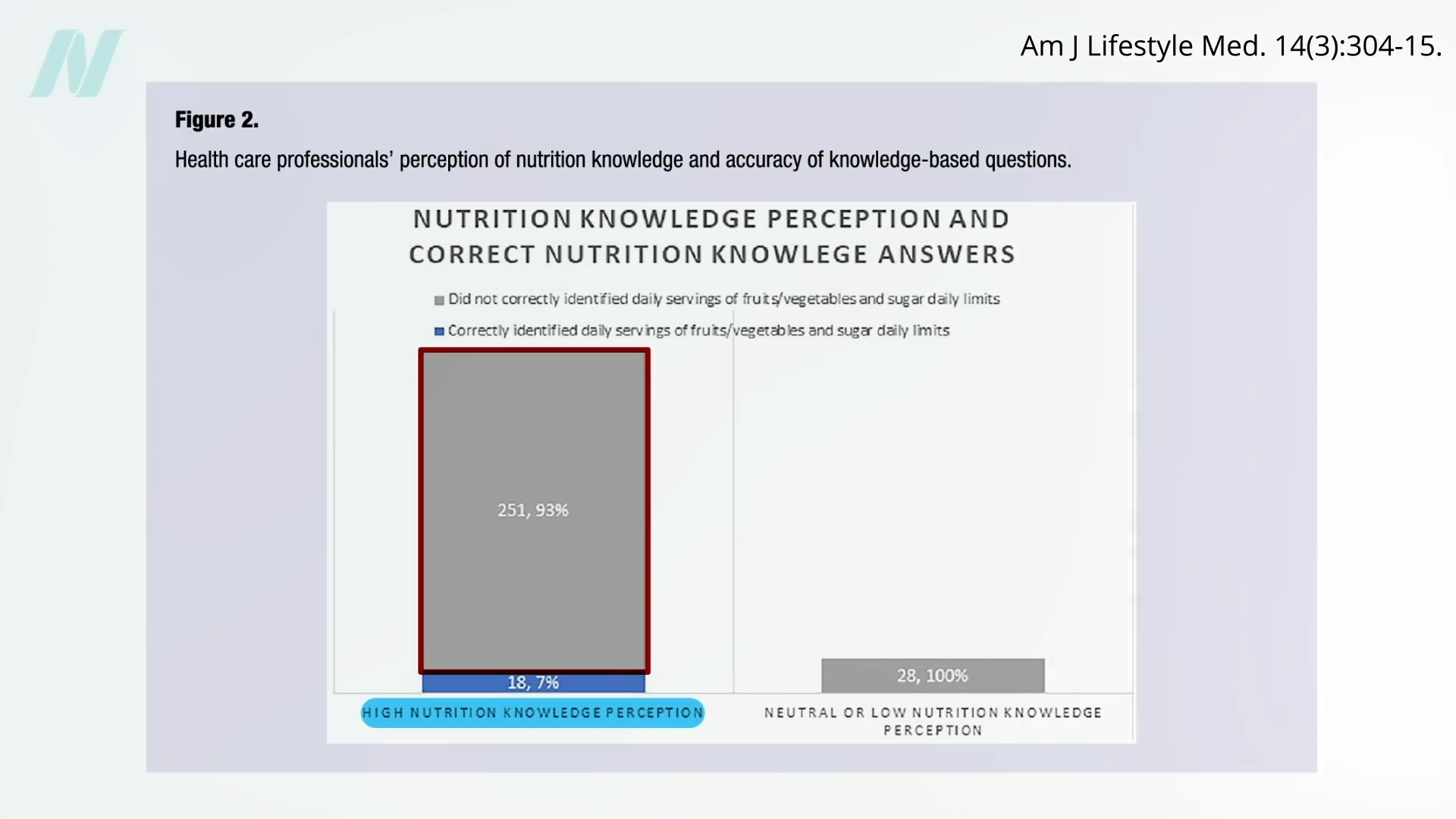
Of doctors surveyed, “only 25% correctly identified the American Heart Association recommended number of fruit and vegetable servings per day, and fewer still (20%) were aware of the recommended daily added sugar limit for adults.” So how are they going to counsel their patients? And get ready for this: Of the doctors who perceived themselves as having high nutrition knowledge, 93 percent couldn’t answer those two basic multiple-choice questions, as seen here and at 2:39 in my video.
“Physicians with no genuine expertise in, say, neurosurgery [brain surgery] are neither likely to broadcast detailed opinions on that topic nor to have their ‘expert’ opinions solicited by the media. Most topical domains in medicine enjoy such respect: we defer expert opinion and commentary to actual experts. Not so nutrition, where the common knowledge that physicians are generally ill-trained in this area is conjoined to routine invitations to physicians for their expert opinions on the matter. All too many are willing to provide theirs, absent any basis for actual expertise…” Or worse, they’re “often made on the basis of native bias and personal preference, at times directly tethered to personal gain—such as diet book sales—and so arises yet another ethical challenge.” That’s one of the reasons all the proceeds I receive from my books are donated directly to charity. I don’t want even the appearance of any conflicts of interest.
“In a culture that routinely fails to distinguish expertise from mere opinion or personal anecdote, we physicians should be doing all we can to establish relevant barriers to entry for expert opinion in this [diet and nutrition], as in all other matters of genuine medical significance.” I mean, we aren’t talking celebrity gossip. Lives are at stake. “Entire industries are devoted to marketing messages that may conspire directly against well-informed medical advice in this area.”
“Medical education must be brought up to date. For physicians to be ill-trained in the very area most impactful on the rate of premature death at the population level is an absurd anachronism….The mission of medicine is to protect, defend, and advance the human condition. That mission cannot be fulfilled if the diet is neglected.”
A possible starting place? “Physicians and health care organizations can collectively begin to emphasize their seriousness about nutrition in health care by practicing what they (theoretically) preach. Is it appropriate to serve pizza and soft drinks at a resident conference while bemoaning the high prevalence of obesity and encouraging patients to eat healthier? A similarly poor example exists in medical conferences, including national meetings, where some morning sessions are accompanied by foods such as donuts and sausage.”
Chef-prepared, plant-forward meals are tailored for early-stage Alzheimer’s patients
Meals are based on the “Ornish lifestyle” to promote brain health and slow disease progression
Program includes 14 culturally relevant, vegetarian meals, expanding to 28 soon
EmblemHealth, a health insurer with locations on Long Island, is partnering with physician-researcher Dr. Dean Ornish and chef-led meal service CookUnity to provide medically tailored meals as part of a new Alzheimer’s program, according to a news release about the initiative.
Based in Williamsburg, Brooklyn, CookUnity, which serves Long Island, said it is providing medically tailored meals for participants in the program for those with early-stage Alzheimer’s disease. Backed by emerging research, the meals are delivered to participants’ homes and are designed to slow the onset and progression of the disease.
“Lifestyle and diet play a critical role in how we live and how we age,” Dr. Dan Knecht, chief medical officer at EmblemHealth, said in the news release.
“Yet access to healthy, affordable, and delicious meals remains a major challenge for many,” Knecht said. “That’s why our collaboration with CookUnity is so unique and exciting. Their local chefs are helping us bring high-quality, plant-forward meals to participants in our Alzheimer’s program, making it easier to support health through food.”
The program – it’s in a pilot phase, currently – comes at a time when Alzheimer’s affects more than 426,000 New Yorkers, according to the New York State Office for the Aging. More than 7 million are living with Alzheimer’s across the United States, according to Alzheimer’s Association. And, experts say, there are limited treatment options.
“For this program to succeed, the food must be both culturally relevant and delicious,” Knecht said. “This program isn’t just about science; it’s about dignity and joy. Meals that reflect our members’ heritage and taste preferences aren’t just nourishing, but they’re healing.”
Participants can choose from over a dozen chef-prepared, ready-to-eat meals from CookUnity, developed to meet the specific nutritional needs of those with Alzheimer’s while maintaining restaurant-quality flavor.
“Our chefs view this program as a testament to their ever-evolving expertise and to the belief that food is medicine,” Bruno Didier, head of CookUnity Business, said in the news release.
“It’s often said that we are what we eat, and we believe the right recipes can empower better health,” Didier added. “This collaboration reflects our mission to deliver nourishing, chef-crafted meals – and deepens our commitment to scaling medically tailored solutions.”
CookUnity’s veteran chefs – Emily Peck, Einat Admony, Ivy Stark and Lena Elkousy – worked with EmblemHealth’s clinical team and CookUnity’s in-house nutritionist to create a nourishing and flavorful custom menu based on the principles of the “Ornish lifestyle,” according to the news release.
“When my team first learned about this meal program, we couldn’t contain our enthusiasm,” Admony said in the news release.
“This initiative not only offers us a platform to showcase our culinary skills, but it also encourages us to think creatively through the lens of health by eliminating excess salt and unhealthy fats while using more nutritious alternatives,” Admony said. “It’s an exciting challenge that allows us to redefine our dishes while promoting better health.”
The program currently offers 14 vegetarian meals, with plans to double to 28 soon. Each meal is designed to meet strict clinical nutritional guidelines and features diverse global flavors – from Middle Eastern Moroccan vegetable stew to Italian mushroom Stroganoff – designed to satisfy varied palates and encourage long-term adherence.
Participants in the program are screened by EmblemHealth’s provider group, Advantage Care Physicians, to implement a comprehensive lifestyle medicine program aimed at enhancing brain health and providing crucial support for caregivers, according to EmblemHealth.
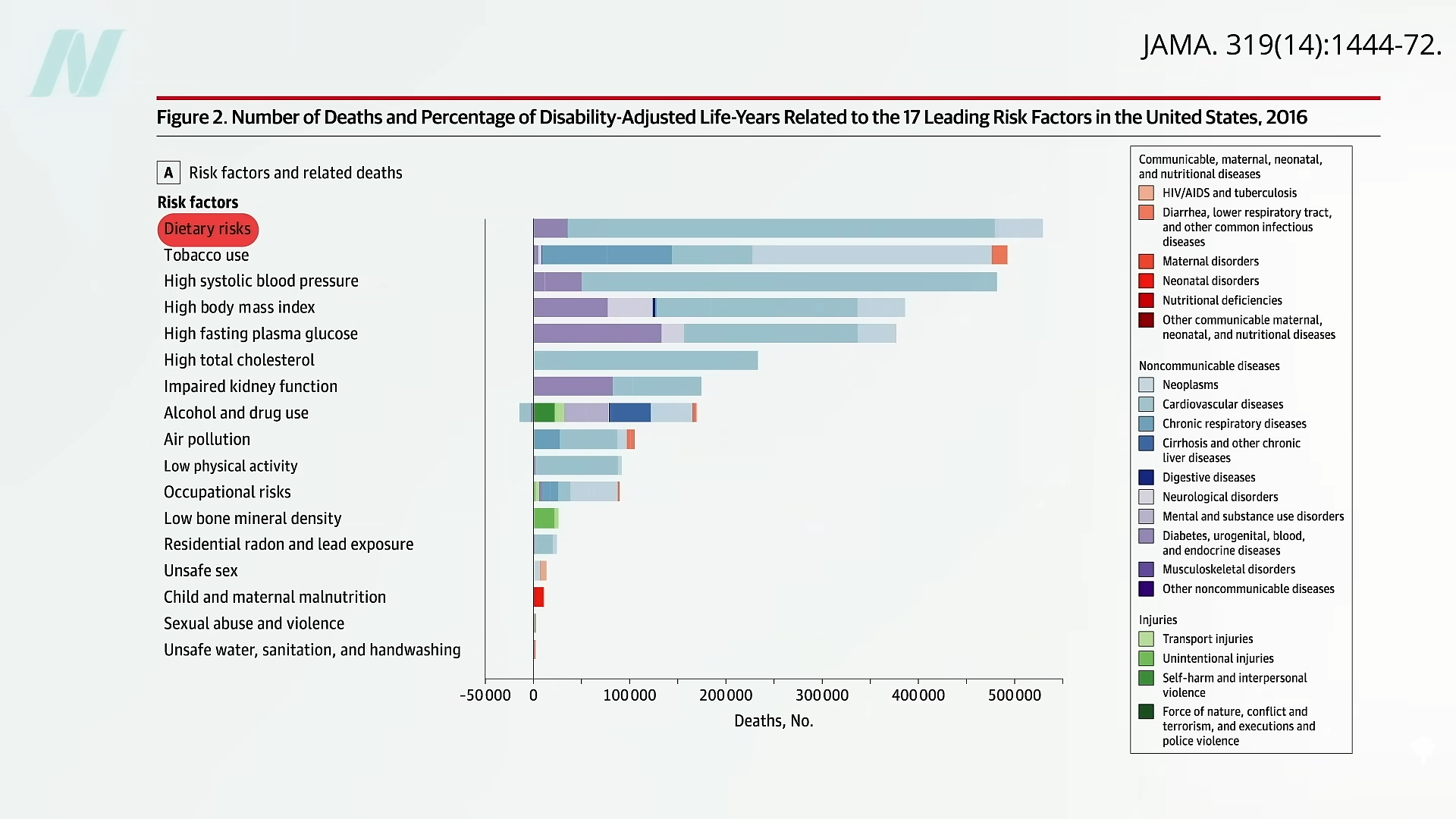
The leading risk factor for death in the United States is the American diet.
About a decade ago, the American Heart Association (AHA) expressed concern that its “2020 target of improving cardiovascular health by 20% by 2020 will not be reached if current trends continue.” By 2006, most people were already not smoking and had nearly achieved their goal for exercise. But when it came to healthy diet score, only about 1 percent got a 4 or 5 out of its diet quality score of 0 to 5, as you can see below and at 0:35 in my video, Friday Favorites: The Scientific Consensus on a Healthy Diet. And that’s with such “ideal” criteria as drinking less than four and a half cups of soda a week.
In the last decade, the AHA saw a bump in the prevalence of the ideal healthy diet score to about 1 percent of Americans reaching those kinds of basic criteria, but, given its “aggressive” goal of reaching a “20% target” by 2020, it hoped to turn that 1 percent into about 1.2 percent. (Really, as you can see here and at 1:01 in my video.)
So, how’d we do? According to the 2019 update, it seems we’ve slipped down to as low as one in a thousand, and American teens scored a big fat zero. No wonder, perhaps, that “for all mortality-based metrics, the US rank declined…to 27th or 28th among 34 OECD [industrialized] countries. Citizens living in countries with a substantially lower gross domestic product and health expenditure per capita…have lower mortality rates than those in the United States.” Slovenia, for example, beat the United States, ranking 24th in life expectancy. More recently, the United States’s life expectancy slipped further, down to 43rd in the world, although the United States spent the most ($3.0 trillion) on health care…”
What is the leading risk factor for death in the United States? As seen below and at 2:04 in my video, it is the standard American diet. Those trillions in health care spending aren’t addressing the root cause of disease, disability, and death.
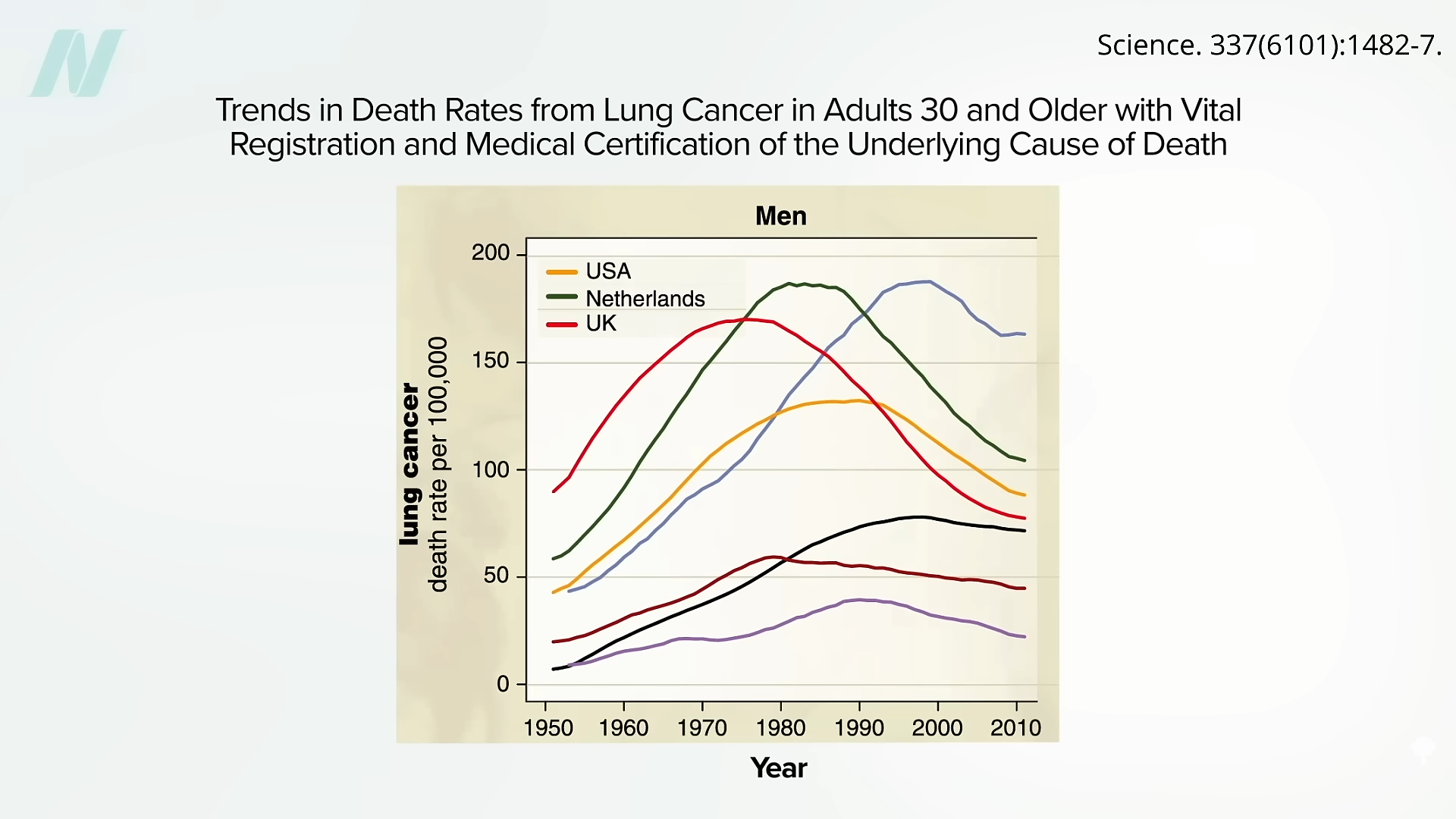
Here are some of the lung cancer death curves, below and at 2:08 in my video:
It took decades to finally turn the corner, but it’s so nice to finally see those drops. When will we see the same with diet?
“Approximately 80% of chronic disease and premature death could be prevented by not smoking, being physically active, and adhering to a healthful dietary pattern.” What exactly is meant by “healthy diet”? “Unfortunately, media messages surrounding nutrition are often inconsistent, confusing, and do not enable the public to make positive changes in health behaviors….Certainly, there is pressure within today’s competitive journalism market for sensationalism. There may even be a disincentive to present the facts in the context of the total body of information consumers need to act on dietary recommendations.” And there’s an incentive to sell more magazines and newspapers. The paper I’m quoting was written in 1997, before the lure of clickbait headlines. In fact, about three-quarters of a century ago, it was noted: “It is unfortunate that the subject of nutrition seems to have a special appeal to the credulous, the social zealot and, in the commercial field, the unscrupulous….The combination is one calculated to strike despair in the hearts of the sober, objective scientist.”
Indeed, the most important health care problem we face may be “our poor lifestyle choices based on misinformation.” It is like the climate change deniers: “Analogous to outspoken cynics denying climate change and influencing public opinion, healthy lifestyle and dietary advice are overshadowed by critics, diet books, the food industry, and misguided information in the media.” Maybe we need an entity like the Intergovernmental Panel on Climate Change (IPCC)—but for nutrition.
These days, “no single expert, regardless of academic stature or reputation, has the prominence to overcome the obstacles created by confusing media messages and deliver the fundamental principles of healthy living effectively to the public.”
What if there were “a global coalition consisting of a variety of nutrition experts, who collectively represent the views held by the majority of scientists, physicians, and health practitioners” that could “serve as the guiding resource of sound nutrition information for improved health and prevention of disease”?
Enter the True Health Initiative, which “was conceived for that very purpose.” A nonprofit coalition of hundreds of experts from dozens of countries has agreed to a consensus statement on the fundamentals of healthy living. See www.truehealthinitiative.org.
Spoiler alert: The healthiest diet is one generally comprised mostly of minimally processed plants.
What if the very hormone designed to help you survive is actually the reason you’re struggling to thrive?
My mother relentlessly saved and sacrificed so that she could enjoy her life in retirement. But two years into retirement, she was diagnosed with early onset Alzheimer’s.
Here’s what I’ve learned since becoming a Functional Diagnostic Nutrition Practitioner: she didn’t just “get” Alzheimer’s two years after retirement. It was building and building for years before that. She was making it worse with lifestyle choices: the over-exercising that women in their 40s and 50s often do, eating trans fats during the low-fat craze of the 80s and 90s.
Had I known what I know now, her outcome might have been different.
This is why I’m passionate about functional health. This is why thousands of practitioners are learning to identify and address the root causes of dysfunction before they become disease. If we can reach people in that gray space (when things are out of balance but before they become diagnosable conditions), we can change their trajectory. We can save lives.
As functional health practitioners, we see it every day: clients who’ve tried everything, followed every protocol, cleaned up their diet, and taken all the right supplements, yet they’re still stuck in that frustrating place of “I’m okay, but I’m not great.”
The missing piece? Understanding cortisol and its profound impact on every system in the body.
If you’ve ever wondered why some clients get amazing results while others plateau, or why you yourself might be experiencing symptoms that doctors dismiss as “normal aging,” this deep dive into cortisol will change everything.
What Is Wellness, Really?
Before we dive into cortisol, let’s get clear on what we’re actually working toward. At FDN, we don’t believe in “fine” or “okay.” We believe in abundant vitality.
Picture this as a spectrum:
The Right Side (The Medical Model): Symptoms → Sickness → Disease → Death
The Middle (Neutral Health): No symptoms, but no energy either. This is the “I’m fine, I guess” zone where most people live.
The Left Side (True Wellness): High energy, optimal function, metabolic fire, abundant vitality, joy for life.
Here’s the thing: neutral health equals a neutral life. When you’re operating from “I’m okay, I don’t have any complaints,” you’re not building empires, writing books, raising joyful kids, or showing up as your best self in relationships.
Good health, abundant vitality, is your birthright. It’s not just for the lucky few.
The Body’s Incredible Healing Power (And What’s Limiting It)
Your body is a self-healing machine. You know this because when you get a cut, it heals. When you break a bone, it mends. When you catch a cold, you recover.
But this healing ability isn’t infinite. If it were, we’d never age or die.
So what’s the difference between what your body can heal and what it can’t?
It’s a savings versus spending problem.
Think of your body as having a bank account called “Vital Reserve.” This is your innate intelligence: your body’s natural ability to function at 100% and fix imbalances before they become problems.
Where do you spend this precious currency? On your environment.
This has always been the case. Our paleolithic ancestors spent their Vital Reserve on not knowing if food would be available, dealing with harsh weather, avoiding predators, and navigating tribal conflicts.
Today? We spend it on mental-emotional stress, environmental toxins, and poor lifestyle habits that are constantly draining our account.
The main spender of Vital Reserve is stress.
The Modern Stress Problem: It’s Not What You Think
When most people think of stress, they picture this: work deadlines, traffic, relationship conflicts, financial pressure. And yes, these mental-emotional stressors are huge.
But there are two other categories most people completely miss:
Physical Stressors:
Sitting too long
Blue light exposure from screens
Too much coffee
Not exercising enough (or exercising too much)
Needing wine to fall asleep
Poor sleep quality
Environmental Stressors:
Depleted soils
EMF exposure
Chemicals in food, water, and air
Toxins our paleolithic ancestors never encountered
Plus, there’s the existential stress of modern life: What’s my purpose? How do I make my life meaningful when I’ll likely be forgotten in 100 years?
All of these are constantly withdrawing from your Vital Reserve account.
Meet Cortisol: Your Body’s “Energy on Credit” System
Cortisol is your primary stress hormone, and it’s actually designed to help you survive. When your environment throws stressors at you, cortisol says, “We need to put internal spending on hold and take all available resources to deal with this external threat.”
Cortisol breaks the body down for quick energy. We call this “catabolic.”
Why would your body have a mechanism for breaking itself down? Because sometimes you need energy RIGHT NOW. When your boss says, “This project is actually due in 30 minutes,” you can’t drive to the store, buy food, cook it, eat it, digest it, and then produce energy. You need quick fuel immediately.
So cortisol reaches for easy-to-break-down tissues like cartilage, tendons, connective tissue, and muscle, converting them to blood sugar.
Here’s the kicker: Cortisol is also a natural painkiller and anti-inflammatory. It masks the damage it’s doing, which is why it makes you feel amazing in the moment: clear thinking, quick reactions, pain-free movement.
Think of cortisol as your body’s credit card. You’re borrowing energy now and promising to pay it back later through rest, recovery, and healing.
When “Energy on Credit” Becomes a Problem
Throughout history, humans dealt with stress that was intense but occasional and short-lived. A wild animal attack, a natural disaster, a tribal conflict: these were serious but temporary.
Take a moment to think about this: Does this describe the stress in your life?
For most of us, stress is intense, constant, and never-ending. We wake up stressed, work stressed, drive home stressed, and lie in bed stressed about tomorrow’s stress.
This creates what we call “catabolic debt”: you’re constantly running up charges on your cortisol credit card without ever paying it back.
Chronic stress is not within our biological design.
Consider this: Anthropological studies show paleolithic humans worked only 15-20 hours per week. How many of you work only 15-20 hours per week? (And remember, “work” includes housework, childcare, and all the other responsibilities that don’t stop when you leave the office.)
They lived in close communities with cooperative resource sharing and had each other’s backs. Think about your own life: Do you know your neighbors? If you do, would they really have your back if things got serious?
Most of us are duplicating resources instead of sharing them. We’re all figuring out our own childcare, making our own meals, maintaining our own everything. There’s no interdependence, no shared load.
The cost of modern life is enormous:
70-80% of doctor visits are for stress-related illnesses
People with high anxiety are 4-5 times more likely to die from heart attack or stroke
Stress contributes to 50% of all illnesses
The Stress Response Curve: Your Roadmap to Understanding Where You Are
This is where it gets really interesting. Understanding this curve will change how you see your health (and your clients’ health) forever.
We all start in the green zone: Homeostasis. When you experience occasional stressors, cortisol and adrenaline spike, you handle the situation, then return to baseline to rest and repair.
But when stress becomes chronic, you move into the orange zone: Acute Stress. You’re constantly producing cortisol and adrenaline, never returning to homeostasis.
Here’s the thing: on your way up this curve, you feel AMAZING. Remember when you could pull all-nighters and still ace exams? When you could eat junk food without consequences? When you had laser focus for 12-16 hours straight?
That’s the acute phase. You’re running on cortisol, and it feels like superpowers.
Then you hit Peak Production. Your body says, “We’ve put way too much on the cortisol credit card. We have to cut back.”
Now you fall into the Compensatory Phase. Your cortisol numbers might look normal to a doctor, but the distribution is all wrong. Maybe you have too much in the morning and crash by afternoon, or you spike at night and can’t sleep.
Plus, you have a relativity problem. You’re used to feeling like Superman from the acute phase, so normal cortisol levels feel terrible by comparison.
Continue down this path, and you reach the Exhaustive Phase. Like a phone on low battery mode, everything still works but at 30% capacity and not for long. You’re devoting everything to just getting through the day.
The Hidden Cost: What Happens to Your Body’s Core Systems
At FDN, we focus on six foundational systems that chronic stress systematically shuts down. We call them the H-I-D-D-E-N systems, and understanding what happens to each one under chronic stress is crucial for practitioners:
H – Hormones DHEA is your anabolic hormone: the one responsible for building you back up after cortisol breaks you down. This is how you pay off your cortisol credit card. But when stress is constant, DHEA steps back and says, “I’ll come back when it’s safe to focus internally, but right now we need to keep spending on the environment.” DHEA becomes chronically low, which means your healing potential becomes chronically low.
Then sex hormones get the message: “We don’t have enough resources to fund fertility right now.” Sex hormones plummet, taking motivation and joy for life with them. This is when you get to that neutral state where you’re thinking, “I have dreams I want to pursue, but it’s just too much effort. I’ll just watch Netflix instead.”
I – Immune Your immune system is expensive to run. Under chronic stress, it says, “I cost a ton of money, so I’m going to operate at 30% capacity and not for very long.” Now you’re getting sick often, it takes forever to heal, you can’t shake that cough, and if anyone around you is sick, you know you’re going down.
D – Digestion Digestion costs a lot of energy to function properly. When you’re spending everything on stress, digestion goes into low-power mode. Now you’re only digesting at 30% capacity. Even if you’re eating the cleanest diet in the world, you can’t use it. You’re not getting the building blocks to repair or the nutrients your body needs to power metabolic functions at full capacity.
D – Detoxification Detoxification is another huge system that’s expensive to run. When your body’s bank account is overdrawn from cortisol debt, detox says, “I don’t have enough money to find these toxins, bind them up, and effectively remove them. So I’ll put them in storage instead.” Your body shoves toxins into fat cells, brain tissue, and bones, creating a toxic backlog that makes you feel slow, gives you acne, throws off digestion, and impairs hormone production.
E – Energy Production Your mitochondria can’t function optimally when all resources are diverted to stress response. This leads to that “tired but wired” feeling where you’re exhausted but can’t actually rest.
N – Nervous System Sleep, mood, and cognitive function all suffer. This is where we see the brain fog, insomnia, anxiety, and depression that so many people struggle with.
The fundamental principle of FDN: These systems don’t operate in isolation. You can’t just say, “Oh, you have classic hormone symptoms, so let’s run a hormone test.” You miss immunity, digestion, detoxification: all the other systems contributing to what we call “Metabolic Chaos.”
This is why the “take this supplement for that symptom” approach rarely works long-term. You’re not dealing with isolated problems: you’re dealing with systemic dysfunction where multiple systems are compromised simultaneously.
Real-Life Case Studies: The Stress Curve in Action
Let’s look at three real clients to see how this plays out. As FDN practitioners, we use what we call “clinical correlation,” which means we never look at lab numbers in isolation. We always consider how someone feels alongside their test results.
Case Study 1: Adam – The Acute Phase Crash
Profile: 35-year-old male, broker at a mid-size investment firm, former athlete still crushing CrossFit workouts
Symptoms: Weight gain, trouble concentrating, loss of muscle mass despite rigorous workouts, headaches
Doctor’s Assessment: “Your results are unremarkable. This is normal aging.”
Lab Results:
Cortisol sum: 9 (acute phase)
Four-point pattern: Way too high in morning, drops low at noon, crashes severely in afternoon, bounces back up at night
The Reality: How do we know Adam isn’t on the left side of the stress curve going up into acute phase? His symptoms tell us everything. If he were on the way up, he’d feel amazing and wouldn’t be in our office. Instead, he’s on the right side coming down from peak production.
His cortisol pattern explains everything: sky-high morning cortisol makes him feel wired and anxious, the afternoon crash leaves him unable to concentrate (not ideal for an investment broker), and the nighttime spike disrupts his sleep.
Even though his DHEA looks “normal,” when we compare it to his cortisol level of 9, he’s clearly catabolic dominant. He’s breaking down faster than he’s building up, which explains why his intense CrossFit sessions aren’t building muscle: they’re just adding more stress to an already overloaded system.
The Reality: Caitlyn’s cortisol sum looks normal, but the distribution is completely dysfunctional. She can barely drag herself out of bed in the morning, crashes hard in the afternoon (imagine trying to accurately record legal proceedings when your cortisol is plummeting), and lies awake at night because her cortisol spikes just when it should be lowest.
She also has a relativity problem. When she was in the acute phase, she felt like Superman. Now that she’s in compensatory with “normal” cortisol levels, she feels terrible by comparison. Her DHEA is low, confirming she’s still in catabolic debt despite the lower cortisol numbers.
Case Study 3: Maggie – The Exhaustive Phase Crisis
Profile: 43-year-old chef at a popular five-star restaurant, diagnosed with hypothyroid
Symptoms: Weight gain in hips and belly, trouble keeping up at work, depression, irregular menstrual cycle
Lifestyle: Working 60+ hours per week, consistently sleeping only 5 hours per night
Medical Status: Seeing a counselor, considering antidepressant medication
Lab Results:
Cortisol sum: 3.1 (exhaustive phase)
Four-point pattern: Way too low in morning, drops low at noon, slight bounce in afternoon, drops again at night
DHEA: Very low
Clinical correlation: Still catabolic dominant despite low cortisol
The Reality: Maggie’s body is operating like a phone on low battery mode: everything still works, but at 30% capacity and not for long. Her thyroid has downregulated because there’s literally not enough energy in the system to maintain normal function.
The depression isn’t just psychological: it’s physiological. Her body can’t afford to fund optimal brain function. Even though her cortisol is very low and her DHEA is very low, she’s still cortisol dominant and in catabolic debt.
This is why understanding the stress curve is so crucial. Three people, three different phases, three different approaches needed.
The Path Forward: Why Understanding Cortisol Changes Everything
Here’s why this matters for you as a health practitioner:
1. It explains why some clients plateau. If you’re not addressing the stress component, you’ll hit a ceiling on healing no matter how perfect the diet or supplement protocol.
2. It validates your clients’ experiences. When someone says, “I used to be able to handle so much more,” or “I don’t feel like myself anymore,” you now understand the physiology behind it.
3. It gives you a roadmap for intervention. Different phases require different approaches. Someone in the acute phase needs different support than someone in the exhaustive phase.
4. It highlights the importance of comprehensive testing. A single cortisol measurement tells you almost nothing. You need the full pattern plus clinical correlation.
The FDN Approach: Test, Don’t Guess
At FDN, we don’t just talk about stress: we measure it. We use what we call “clinical correlation,” which means we never look at lab numbers in isolation. We always consider how someone feels alongside their test results.
We look at:
Four-point cortisol patterns throughout the day (not just a single measurement)
DHEA levels and the cortisol-to-DHEA ratio
How stress is affecting all the H-I-D-D-E-N systems
The complete picture of metabolic chaos
Progress tracking with tools like the Metabolic Chaos Scorecard
Then we address it systematically through our DRESS protocol:
D – Diet: Personalized nutrition based on lab findings, not generic “healthy eating” advice
R – Rest: Sleep optimization and recovery strategies tailored to your stress phase
E – Exercise: Right-sized movement for your current capacity (over-exercise is just as harmful as under-exercise)
S – Stress Reduction: Targeted techniques for your specific stressors: mental/emotional, physical, environmental, and lifestyle factors
S – Supplementation: Targeted support based on actual lab results, not guesswork
This isn’t about generic protocols. It’s about understanding exactly where someone is on the stress curve and what their body needs to heal.
Key Takeaways for Health Practitioners
Cortisol isn’t the enemy. A lot of people talk about cortisol as if it’s the villain—commercials make it sound like cortisol just makes you “old and fat.” That’s not what cortisol does. Cortisol is a vital hormone for navigating stress. The problem is chronic stress disrupting its natural rhythm.
Understanding the stress curve is diagnostic gold. It explains why clients feel the way they do and gives you a framework for intervention. Different phases require different approaches.
Clinical correlation is everything. You can’t just look at lab numbers in isolation. A cortisol sum of 5 might be “normal” to a doctor, but if your client feels terrible and the distribution is dysregulated, that tells you the real story.
You can’t ignore stress and expect lasting results. No matter how perfect your diet protocol or how targeted your supplements, chronic stress will cap healing potential. There’s a ceiling you’ll never break through if you don’t address the stress component.
The body’s systems are interconnected. You can’t just “fix hormones” without addressing how stress is affecting immunity, digestion, detoxification, and all the other H-I-D-D-E-N systems. This is why comprehensive testing and systematic protocols are crucial.
Metabolic Chaos requires a systematic approach. When multiple systems are compromised simultaneously, you need a framework like DRESS that addresses all aspects of healing, not just isolated symptoms.
Your Next Steps
If you’re ready to master functional lab testing and learn how to identify and address cortisol dysregulation in your practice, FDN provides the training, community, and ongoing support you need.
Because here’s the truth: your clients deserve more than “fine.” They deserve abundant vitality. And you deserve the confidence that comes from knowing exactly how to help them achieve it.
When you understand cortisol (really understand it), you hold the key to unlocking transformation for every client who walks through your door.
Ready to become the practitioner who always knows what to do next?
The answer lies in data-driven functional health. The answer lies in understanding that robust health isn’t just about the absence of symptoms: it’s about the presence of vitality.
And it starts with the hormone you can’t ignore: cortisol.
Want to learn more about becoming a Functional Diagnostic Nutrition Practitioner?
Discover how our comprehensive training program gives you the tools to master cortisol testing, interpretation, and protocols that get results. Because when you know how to test, you never have to guess. View an indepth case study here.
Switching to a plant-based diet has been shown to achieve far better outcomes than those reported on conventional treatments for both active and quiescent stages of Crohn’s disease (CD) and ulcerative colitis.
Important to our understanding and the prevention of the global increase of inflammatory bowel disease (IBD), we know that “dietary fiber reduces risk, whereas dietary fat, animal protein, and sugar increase it.” “Despite the recognition of westernization of lifestyle as a major driver of the growing incidence of IBD, no countermeasures against such lifestyle changes have been recommended, except that patients with Crohn’s disease should not smoke.”
We know that “consuming whole, plant-based foods is synonymous with an anti-inflammatory diet.” Lists of foods with inflammatory effects and anti-inflammatory effects are shown here and at 0:50 in my video, The Best Diet for Crohn’s Disease.
How about putting a plant-based diet to the test?
Cutting down on red and processed meats didn’t work, but what about cutting down on all meat? A 25-year-old man “with newly diagnosed CD…failed to enter clinical remission despite standard medical therapy. After switching to a diet based exclusively on grains, legumes [beans, split peas, chickpeas, and lentils], vegetables, and fruits, he entered clinical remission without need for medication and showed no signs of CD on follow-up colonoscopy.”
It’s worth delving into some of the details. The conventional treatment he was started on is infliximab, sold as REMICADE®, which can cause a stroke and may increase our chances of getting lymphoma or other cancers. (It also costs $35,000 a year.) It may not even work in 35 to 40 percent of patients, and that seemed to be the case with the 25-year-old man. So, his dose was increased after 37 weeks, but he was still suffering after two years on the drug. Then he completely eliminated animal products and processed foods from his diet and finally experienced a complete resolution of his symptoms.
“Prior to this, his diet had been the typical American diet, consisting of meat, dairy products, refined grains, processed foods, and modest amounts of vegetables and fruits. Having experienced complete clinical remission for the first time since his Crohn’s disease diagnosis, the patient decided to switch to a whole food, plant-based diet permanently, severely reducing his intake of processed foods and limiting animal products to one serving, or less, per week.” Whenever his diet slipped, his symptoms started coming back, but he could always eliminate them by eating healthier again. After six months adhering to these diet and lifestyle changes, including stress relief and exercise, a follow-up “demonstrated complete mucosal healing [of the gut lining] with no visible evidence of Crohn’s disease.”
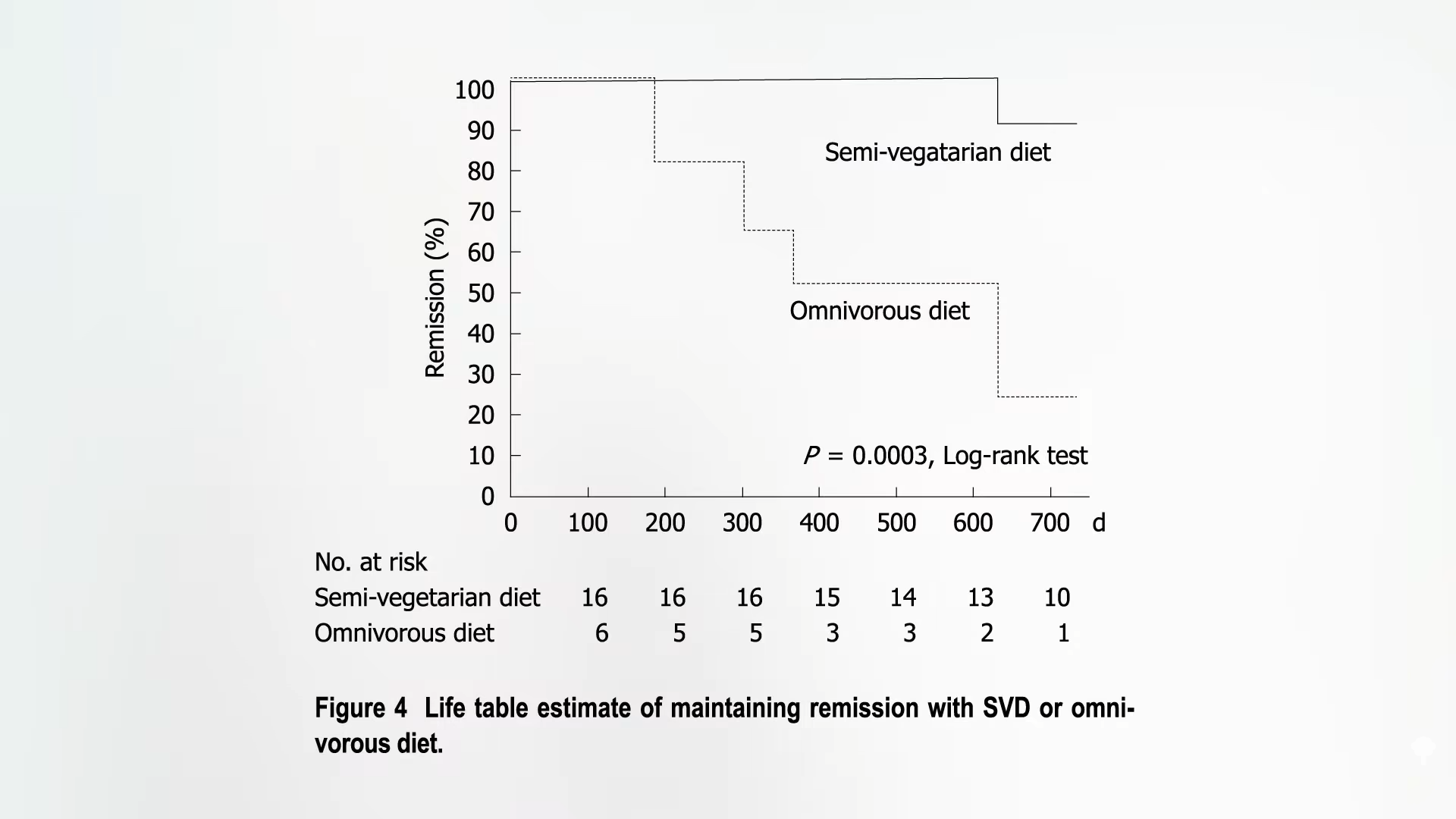
We know that “a diet consisting of whole grains, legumes, fruits, and vegetables has been shown to be helpful in the prevention and treatment of heart disease, obesity, diabetes, hypertension, gallbladder disease, rheumatoid arthritis, and many cancers. Although further research is required, this case report suggests that Crohn’s disease might be added to this list of conditions.” That further research has already been done! About 20 patients with Crohn’s disease were placed on a semi-vegetarian diet—no more than half a serving of fish once a week and half a serving of meat once every two weeks—and they achieved a 100 percent remission rate at one year and 90 percent at two years.
Some strayed from the diet, though. What happened to them? As you can see below and at 3:32 in my video, after one year, half had relapsed, and, at year two, only 20 percent had remained in remission. But those who stuck with the semi-veg diet had remarkable success. It was a small study with no formal control group, but it represents the best-reported result in Crohn’s relapse prevention published in the medical literature to date.
Nowadays, Crohn’s patients are often treated with so-called biologic drugs, expensive injected antibodies that suppress the immune system. They have effectively induced and maintained remission in Crohn’s disease, but not in everybody. The current remission rate in Crohn’s with early use of REMICADE® is 64 percent. So, 30 to 40 percent of patients “are likely to experience a disabling disease course even after their first treatment.” What about adding a plant-based diet? Remission rates jumped up to 100 percent for those who didn’t have to drop out due to drug side effects. Even after excluding milder cases, researchers found that 100 percent of those with serious, even “severe/fulminant disease, achieved remission.”
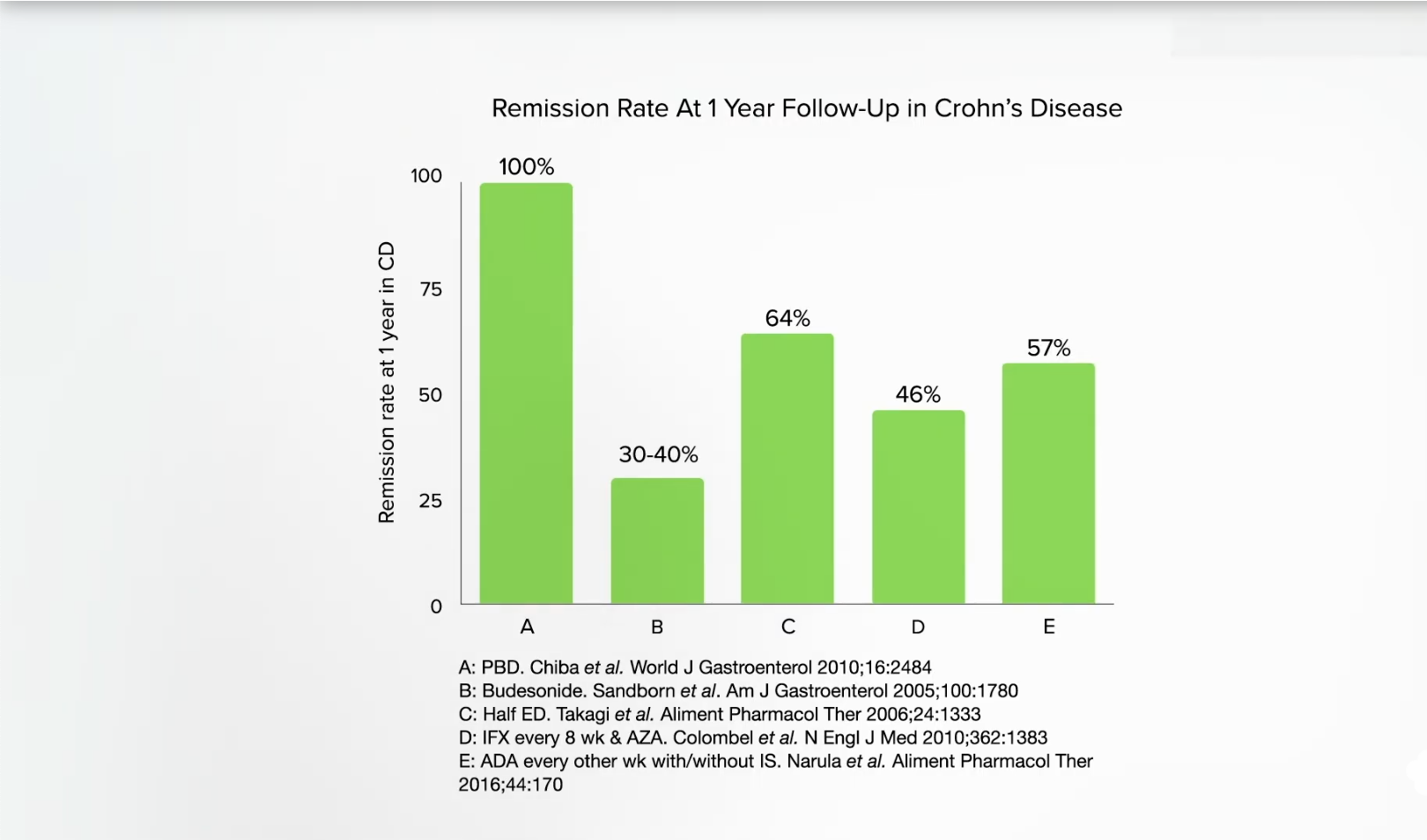
If we look at gold standard systematic reviews, they conclude that the effects of dietary interventions on inflammatory bowel diseases—Crohn’s disease and ulcerative colitis—are uncertain. However, this is because only randomized controlled trials were considered. That’s totally understandable, as that is the most rigorous study design. “Nevertheless, people with IBD deserve advice based on the ‘best available evidence’ rather than no advice at all…” And switching to a plant-based diet has been shown to achieve “far better outcomes” than those reported on conventional treatments in both active and quiescent stages in Crohn’s disease and ulcerative colitis. For example, below and at 5:37 in my video, you can see one-year remission rates in Crohn’s disease (100 percent) compared to budesonide, an immunosuppressant corticosteroid drug (30 to 40 percent), a half elemental diet, such as at-home tube feedings (64 percent), the $35,000-a-year drug REMICADE® (46 percent), or the $75,000-a-year drug Humira (57 percent).
Safer, cheaper, and more effective. That’s why some researchers have made the “recommendation of plant-based diets for inflammatory bowel disease.”
It would seem clear that treatment based on addressing the cause of the disease is optimal. Spreading the word about healthier diets could help halt the scourge of inflammatory bowel disease, but how will people hear about this amazing research without some kind of public education campaign? That’s what NutritionFacts.org is all about.
Is it possible to reverse type 1 diabetes if caught early enough?
TheInternational Journal of Disease Reversal and Prevention has already had its share of miraculous disease reversals with a plant-based diet. For instance, one patient began following a whole food, plant-based diet after having two heart attacks in two months. Within months, he experienced no more chest pain, controlled his cholesterol, blood pressure, and blood sugars, and also lost 50 pounds as a nice bonus. Yet, the numbers “do not capture the patient’s transformation from feeling like a ‘dead man walking’ to being in command of his health with a new future and life.”
I’ve previously discussed cases of reversing the autoimmune inflammatory disease psoriasis and also talked about lupus nephritis (kidney inflammation). What about type 1 diabetes, an autoimmune disease we didn’t think we could do anything about? In contrast to type 2 diabetes, which is a lifestyle disease that can be prevented and reversed with a healthy enough diet and lifestyle, type 1 diabetes is an autoimmune disease in which our body attacks our pancreas, killing off our insulin-producing cells and condemning us to a life of insulin injections—unless, perhaps, it’s caught early enough. If a healthy enough diet is started early enough, might we be able to reverse the course of type 1 diabetes by blunting that autoimmune inflammation?
As I discuss in my video Type 1 Diabetes Treatment: A Plant-Based Diet, we know that patients with type 1 diabetes “may be able to reduce insulin requirements and achieve better glycemic [blood sugar] control” with healthier diets. For example, children and teens were randomized to a nutritional intervention in which they increased the whole plant food density of their diet—meaning they ate more whole grains, whole fruits, vegetables, legumes (beans, split peas, chickpeas, and lentils), nuts, and seeds. Researchers found that the more whole plant foods, the better the blood sugar control.
The fact that more whole fruits were associated “with better glycemic [blood sugar] control has important clinical implications for nutrition education” in those with type 1 diabetes. We should be “educating them on the benefits of fruit intake, and allaying erroneous concerns that fruit may adversely affect blood sugar.”
The case series in the IJDRP, however, went beyond proposing better control of just their high blood sugars, the symptom of diabetes, but better control of the disease itself, suggesting the anti-inflammatory effects of whole healthy plant foods “may slow or prevent further destruction of the beta cells”—the insulin-producing cells of the pancreas—“if dietary intervention is initiated early enough.” Where did this concept come from?
A young patient. Immediately following diagnosis of type 1 diabetes at age three, a patient began a vegetable-rich diet and, three years later, “has not yet required insulin therapy…and has experienced a steady decline in autoantibody levels,” which are markers of insulin cell destruction. Another child, who also started eating a healthier diet, but not until several months after diagnosis, maintains a low dose of insulin with good control. And, even if their insulin-producing cells have been utterly destroyed, individuals with type 1 diabetes can still enjoy “dramatically reduced insulin requirements,” reduced inflammation, and reduced cardiovascular risk, which is their number one cause of death over the age of 30. People with type 1 diabetes have 11 to 14 times the risk of death from cardiovascular disease compared to the general population, and it’s already the top killer among the public, so it’s closer to 11 to 14 times more important for those with type 1 diabetes to be on the only diet and lifestyle program ever proven to reverse heart disease in the majority of patients—one centered around whole plant foods. The fact it may also help control the disease itself is just sugar-free icing on the cake.
All this exciting new research was presented in the first issue of The International Journal of Disease Reversal and Prevention. As a bonus, there’s a companion publication called the Disease Reversal and Prevention Digest. These are for the lay public and are developed with the belief I wholeheartedly share that “everyone has a right to understand the science that could impact their health.” You can go behind the scenes and hear directly from the author of the lupus series, read interviews from luminaries like Dean Ornish, see practical tips from dietitians on making the transition towards a healthier diet, and enjoy recipes.
The second issue includes more practical tips, such as how to eat plant-based on a budget, and gives updates on what Dr. Klaper is doing to educate medical students, what Audrey Sanchez from Balanced is doing to help change school lunches, and how Dr. Ostfeld got healthy foods served in a hospital. (What a concept!) And what magazine would be complete without an article to improve your sex life?
The journal is free, downloadable at IJDRP.org, and its companion digest, available at diseasereversaldigest.com, carries a subscription fee. I am a proud subscriber.
Want to learn more about preventing type 1 diabetes in the first place? See the related posts below.
Green smoothies are put to the test for the autoimmune disease lupus.
There are dozens and dozens of journals I try to stay on top of every month, and one I always anticipate is TheInternational Journal of Disease Reversal and Prevention, a peer-reviewed medical “journal created to document the science of nutrition and lifestyle to prevent, suspend and reverse disease,” with an editor-in-chief no less prestigious than Dr. Kim Williams, past president of the American College of Cardiology. I was honored to join its editorial advisory board, along with so many of my heroes. The best part? It’s free. Go to IJDRP.org and put in your email to subscribe at no cost, and you’ll be alerted when new issues are out, which you can download in full in PDF form. (Did I mention it’s free?)
When it comes to chronic lifestyle diseases, wrote Dr. Williams, “Instead of preventing chronic lifestyle diseases, we [doctors] manage. Never cure, just mitigate. Why? Because of finance, culture, habit, and tradition.” There are many of us, though, who “envision a world where trillions of dollars are not spent on medical care that should never have been necessary, but rather on infrastructure, environment, education, and advancing science. For this reason, comes TheInternational Journal of Disease Reversal and Prevention (IJDRP).” After all, wrote the journal’s co-founder, “Without data, you’re just another person with an opinion.”
To give you a taste of the journal: How about pitting plants against one of the most inflammatory diseases out there—lupus, an autoimmune disease in which your body can start attacking your DNA? Kidney inflammation is a common consequence, and even with our armamentarium of immunosuppressant drugs and steroids, lupus-induced kidney inflammation can lead to end-stage renal disease, which means dialysis, and even death. That is, unless you pack your diet with some of the most anti-inflammatory foods out there and your kidney function improves so much you no longer need dialysis or a kidney transplant. Another similar case was presented with a resolution in symptoms and normal kidney function, unless the patient deviated from the diet and his symptoms then reappeared.
As I discuss in my video Anti-Inflammatory Diet for Lupus, even just cutting out animal products can make a difference. Researchers randomized people to remove meat, eggs, and dairy from their diets without significantly increasing fruit and vegetable intake and found that doing just that can lower C-reactive protein levels by nearly a third within eight weeks, as you can see below and at 2:21 in my video. (Our C-reactive protein level is a sensitive indicator of whole-body inflammation.)
But with lupus, the researchers didn’t mess around. Each day, the study subjects were to eat a pound of leafy greens and cruciferous vegetables like kale, fruits like berries, and lots of chia or flax, and drink a gallon of water. We’re talking about a green smoothie diet to extinguish lupus flares. (Note, though, that if your kidneys are already compromised, this should be done under physician supervision so they can monitor your electrolytes like potassium and make sure you don’t get overloaded with fluid.) Bottom line? With such remarkable improvements due to dietary changes alone, the hope is that researchers will take up the mantle and formally put it to the test.
Reversals of autoimmune inflammatory skin disease can be particularly striking visually. A woman with a 35-year history of psoriasis that had been unsuccessfully managed for 19 years with drugs suffered from other autoimmune conditions, including Sjogren’s syndrome. She was put on an extraordinarily healthy diet packed with greens and other vegetables, fruits, nuts, seeds, avocados, and some whole grains, and boom! Within one year, she went from 40 percent of her entire body surface area inflamed and affected down to 0 percent, completely clear, and, as a bonus, her Sjogren’s symptoms resolved, too, while helping to normalize her weight and cholesterol. You can see before and after photos below and at 3:39 in my video.
I think I only have one other video on lupus: Fighting Lupus with Turmeric: Good as Gold. It’s not for lack of trying, though. There just hasn’t been much research out there.
In the world of healthcare, lifestyle medicine is gaining momentum. Here, the focus is less about disease and more about taking control of health through lifestyle choices.
DR. IRIS GRANECK: Lifestyle medicine has ‘become a very big component of the preventive medicine training.’ Courtesy of Stony Brook Medicine
“Lifestyle medicine is a medical approach that uses evidence-based behavioral interventions to prevent, treat, manage and reverse chronic disease,” Dr. Iris Graneck, who chairs Stony Brook Medicine’s Department of Family, Population & Preventive Medicine. She spoke about the field on a webinar hosted by Stony Brook Medicine earlier in February.
Lifestyle medicine “is going to hopefully become part of all primary care specialties in the future because the current system of just treating chronic diseases is kind of a treadmill that is leading to more and more costs in medicine, and more and more diseases,” Dr. Raja Jaber, the medical director of Stony Brook Medicine’s lifestyle medicine programs, said on the webinar.
There are six pillars to lifestyle medicine. They include a whole-food, plant-predominant eating pattern; physical activity; restorative sleep; stress management; avoidance of risky substances; and positive social connections.
The area of lifestyle medicine is gaining traction at a time of an epidemic of chronic diseases that include diabetes, high blood pressure, obesity and more.
Lifestyle medicine has “become a very big component of the preventive medicine training,” Graneck said.
The specialty is taught at Stony Brook University’s Renaissance School of Medicine, Hofstra University’s Zucker School of Medicine and NYU Long Island School of Medicine.
By adopting the pillars of lifestyle medicine, it is possible to reverse many chronic diseases, leading to improved health, experts say. Even in medical practices that don’t have a dedicated lifestyle medicine practice, it’s not uncommon to find physicians who impart elements of lifestyle medicine to their patients.
It’s easy to see why, given the factors that lead to poor health.
“If we look at one of the biggest areas like risk for premature death or early death and … some of the contributors to that, and individual behaviors actually contributes 40% to the risk of early death,” Graneck said. “Social economic and environmental factors can contribute 20%, genetics 30%.”
These factors not only lead to poor health but are also costly to us as a nation.
DR. RAJA JABER: ‘We can prevent up to 90% of diabetes, 80% of heart diseases and stroke and 40% of cancers.’ Courtesy of Stony Brook Medicine
Currently, “our general medical costs in the country are $4.1 trillion,” Jaber said. “That’s how much we spend on healthcare costs, and 90% of these healthcare costs go to treating chronic diseases.”
But by following the principles of lifestyle medicine – eating a mostly plant-based diet, exercising 150 minutes a week, sleeping well, connecting with others, and more – experts say populations become healthier.
“If we were to do that, then we can prevent up to 90% of diabetes, 80% of heart diseases and stroke and 40% of cancers,” Jaber said.
Lifestyle medicine got a big lift in December. That’s when New York City’s Mayor Eric Adams announced that the American College of Lifestyle Medicine in St. Louis, MO, is investing $44 million to provide every New York City healthcare practitioner free introductory training in nutrition and lifestyle medicine. The training is extended to hospitals in the city, including Northwell Health.
That focus is good news, especially regarding counseling patients on nutrition. According to PubMed.gov, 71% of U.S. medical schools do not reach the minimum benchmark of 25 hours of nutrition education set by the National Academy of Sciences.
But empowering people to eat more healthfully can lead to healthier populations.
“One of the most powerful aspects of lifestyle medicine is that patients become more engaged, active participants in their own self-care, disease prevention and management, and overall well-being,” Dr. Cindy Geyer, a board member of the American College of Lifestyle Medicine, said in a statement. “The end results include better health outcomes for patients and a fulfilling collaborative model of practice for physicians and other health practitioners.”
For example, according to PubMed.gov, lifestyle intervention reduced the incidence of Type 2 diabetes by 58%, compared with the drug Metformin, which reduced it by 31%.
True, the premise around the pillars may not seem revolutionary. Everyone knows they should eat well, exercise and get a good night’s sleep, for example. Yet, putting those concepts into practice can seem monumental.
That’s why the support of a lifestyle medicine practitioner “can be really powerful,” said Dr. Penny Stern, who 15 months ago began practicing lifestyle medicine at Northwell Health’s Center for Wellness and Integrative Medicine in Roslyn. There, new patients complete a “very thick intake form,” so Stern can hone in on the support they want.
“The importance of lifestyle behaviors on health is a cornerstone of primary care education,” said Dr. Gladys Ayala, professor of the Department of Medicine at NYU Long Island School of Medicine.
“Our curriculum not only teaches our learners about the importance of lifestyle factors on health; we also help students to acquire key communication skills that engender trust and understanding and that motivate patients to partner with us on their care,” Ayala said. “Motivational interviewing techniques are used to discuss diet, physical activity, tobacco use, alcohol use, illicit drug use, high risk sexual behavior, stress management, sleep hygiene, socialization, and medication adherence, to name a few.”
One could point to modern living as to how we’ve moved away from the pillars of health.
For example, “we’ve totally turned into a sedentary world,” Stern said. “We used to walk a lot, now we drive everywhere.”
In addition, people eat more processed foods in the United States than they did two decades ago. That consumption is linked to the higher risk of chronic disease, according to a 2021 study by NYU School of Global Public Health.
JOSEPHINE CONNOLLY-SCHOONEN: ‘Most people do know the basics of nutrition like broccoli is healthy and French fries aren’t healthy, but there’s so much food in the marketplace that is un-clear.’ Courtesy of Stony Brook Medicine
“Most people do know the basics of nutrition, like broccoli is healthy and French fries aren’t healthy, but there’s so much food in the marketplace that is unclear,” said Josephine Connolly-Schoonen, director of Stony Brook’s Medicine Nutrition Division, Department of Family, Population & Preventive Medicine, on the Stony Brook webinar. “A lot of foods are by big food industry, [which] created synthetic foods and are then marketed in a way that makes it very confusing for people to understand whether they’re contributing to health or not.”
Even our modern-day sleep habits have disrupted our health.
Prior to the invention of electrical light, “we went to sleep when it was dark, and got up when the sun rose – suddenly we are up till all hours. We run ourselves into the ground, watching TV or staying up to see the end of a movie,“ Stern said.
Stern tells patients to try an experiment – going to sleep when first feeling tired. “That’s when you’re meant to go to sleep.” Sleep is “the time when we rejuvenate and produce growth hormone, so you can restore, and repair,” she said. A poor night’s sleep leads to suppressed immune systems, accidents, poor relationships, low concentration and depression and other unfavorable outcomes, she said.
Social connections, too, are important to good health. When there is community, and a person doesn’t show up, others will reach out to find out why, Stern said. Even time spent with pets is beneficial. “People thrive when they have connections,” she said.
But, as Graneck pointed out, “changing behavior is not an easy thing.”
To offer support, Stony Brook Medicine offers a host of services and developed a lifestyle medicine website. The website includes information on each of the pillars and links to internal and external resources to specialists, coaches, programs, classes and more.
DR. PENNY STERN: Sleep is ‘the time when we rejuvenate and produce growth hormone, so you can restore, and repair.’ Courtesy of Northwell Health
Northwell’s Center for Wellness and Integrative Medicine also offers an abundance of resources including yoga, acupuncture, health and wellness coaching and other services. Where appropriate, Stern will refer patients to medical experts, including for nutrition counseling, or in the instances of sleep apnea to a sleep specialist, and others depending on the patient’s need.
Yes, there will always be a need for such experts as cardiologists, orthopedists and other specialists, but when it comes to helping people embrace the pillars of health, lifestyle medicine “can be so transformative,” Stern said.
By adopting these pillars, “we can prolong our life by 10 years,” Jaber said.
People can have “not only a longer life, but free of disease, and that’s what we want. We don’t want to have a longer life where we are in and out of hospitals or in a nursing home. We want to live and live very healthily.”