[ad_1]
Elevated levels of pro-inflammatory, aging-associated oxylipins can be normalized by eating ground flaxseed.
I previously explored the “Potent Antihypertensive Effect of Dietary Flaxseed in Hypertensive Patients” study in my video Flaxseeds for Hypertension. That was a double-blind, randomized, placebo-controlled trial where researchers disguised ground flaxseed in baked goods versus flax-free placebo muffins and saw an extraordinary drop in high blood pressure. As you can imagine, the flaxseed industry was overjoyed, praising the “impressive” findings, as was I. After all, high blood pressure is “the single largest risk factor” for death in the world. Yes, we give people medications, lots and lots of medications, but most people don’t take them. Nine out of ten people take less than 80 percent of their prescribed blood pressure pills.
It’s not difficult to understand why. “Patients are asked to follow an inconvenient and potentially costly regimen, which will likely have a detrimental effect on health-related quality of life, to treat a mostly asymptomatic condition that commonly does not cause problems for many years.” So, they may feel worse instead of better, due to the side effects. Then, some think the answer is to give them even more drugs to counteract the effects of the first drugs, like giving men Viagra to counteract the erectile dysfunction caused by their blood pressure pills.
How about using a dietary strategy instead, especially if it can be just as effective? And, indeed, the drop in blood pressure the researchers saw in the flaxseed study “was greater than the average decrease observed with the standard dose of anti-hypertensive medications.” Flaxseeds are cheaper, too, compared to even single medications, and most patients are on multiple drugs. Plus, flaxseeds have good side effects beyond their anti-hypertensive actions. Taking tablespoons of flaxseed a day is a lot of fiber for people living off of cheeseburgers and milkshakes their whole lives, and your gut bacteria may need a little time to adjust to the new bounty. So, those who start with low-fiber diets may want to take it a little slow with the flaxseeds at first.
Not all studies have shown significant blood pressure–lowering effects, though. There have been more than a dozen trials by now, involving more than a thousand subjects. And, yes, when you put them all together, overall, there were “significant reductions in both SBP and DBP”—systolic blood pressure (the upper number) and diastolic blood pressure (the lower number)—“following supplementation with various flaxseed products.” But none was as dramatic as what the researchers had found in that six-month trial. The longer trials tended to show better results, and some of the trials just used flaxseed oil or some kind of flaxseed extract. We think this is because the whole is greater than the sum of its parts. “Each of the components of interest within flaxseed, ALA, lignans, fiber, and peptides”—the omega-3s, the cancer-fighting lignans, all the soluble fiber, and the plant proteins, for instance—“all contribute towards BP reduction.” Okay, but how? Why? What is the mechanism?
Some common blood-pressure medications like Norvasc or Procardia work in part by reducing the ability of the heart to contract or by slowing down the heart. So, might it be that’s how flaxseeds work, too? But, no. In my video Benefits of Flaxseeds for Inflammation, I profile the “Dietary Flaxseed Reduces Central Aortic Blood Pressure Without Cardiac Involvement but Through Changes in Plasma Oxylipins” study. What are oxylipins?
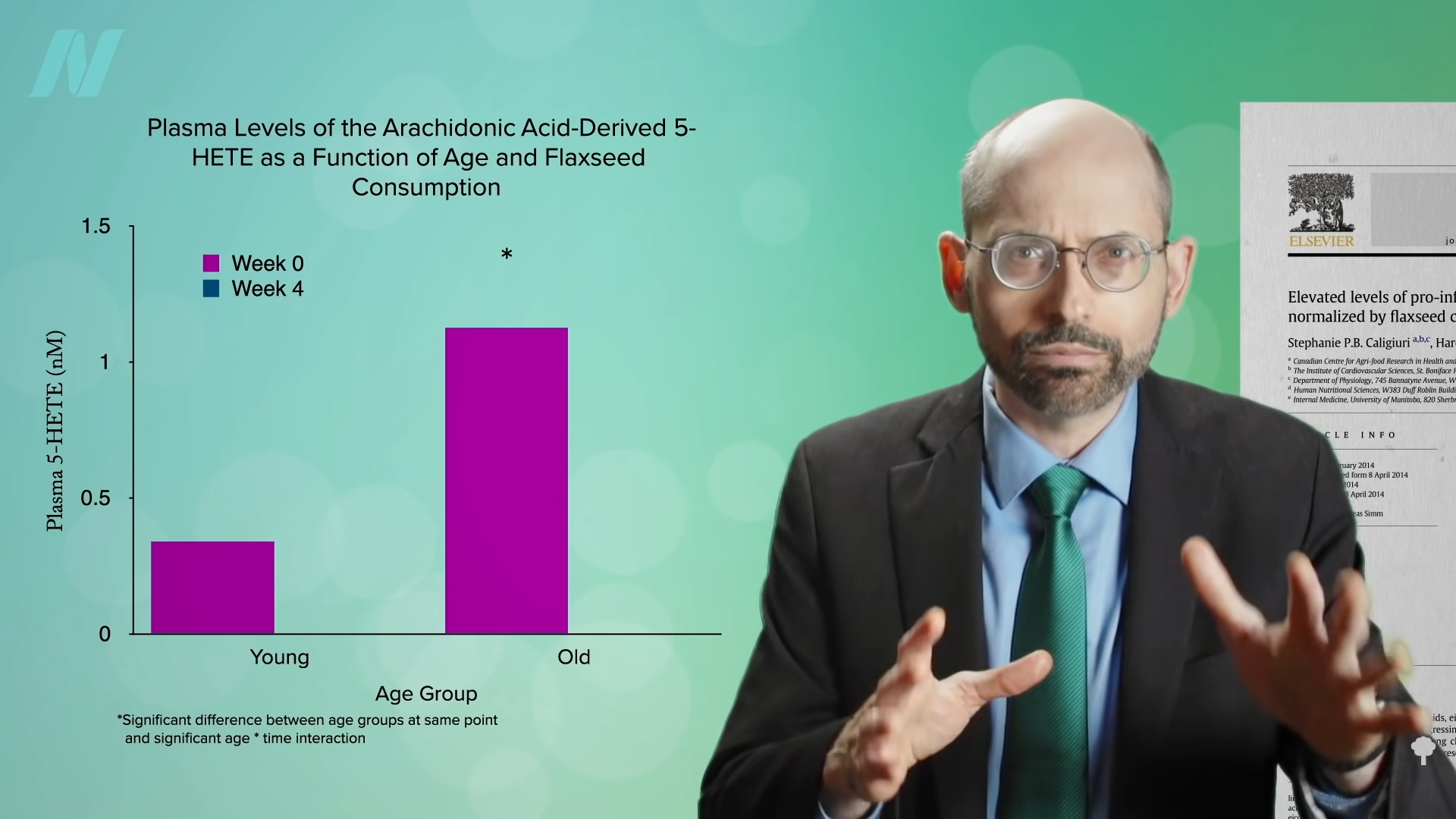
“Oxylipins are a group of fatty acid metabolites” involved in inflammation and, as a result, have been implicated in many pro-inflammatory conditions, including aging and cardiovascular disease. “The best-characterized oxylipins about cardiovascular disease are derived from the w-6 fatty acid arachidonic acid,” a long-chain omega-6 fatty acid. These are found preformed in animal products, particularly chicken and eggs, and can be made inside the body from junky oils rich in omega-6, such as cottonseed oil, as noted below and at 3:49 in my video. But, as this study is titled, “Elevated levels of pro-inflammatory oxylipins in older subjects are normalized by flaxseed consumption.”
That’s how we think flaxseed consumption reduces blood pressure in patients with hypertension: by inhibiting the enzyme that makes these pro-inflammatory oxylipins. I’ll spare you from acronym overload, but eating flaxseeds inhibits the activity of the enzyme that makes these pro-inflammatory oxylipins, called leukotoxin diols, which in turn may lower blood pressure. “Identifying the biological mechanism adds confidence to the antihypertensive actions of dietary flaxseed,” but that’s not all oxylipins do. Oxylipins may also play a role in the aging process. However, we may be able to “beneficially disrupt these biological changes associated with inflammation and aging” with a nutritional intervention like flaxseed. Older adults around age 50 have higher levels of this arachidonic acid–derived oxylipin compared to younger adults around age 20, as you can see in the graph below and at 4:56 in my video. “These elevated concentrations of pro-inflammatory oxylipins in the older age group…may…explain the higher levels of inflammation in older versus younger individuals.” As we get older, we’re more likely to be stricken with inflammatory conditions like arthritis. So, this “elevation of pro-inflammatory oxylipins…may predispose individuals to chronic disease conditions.”
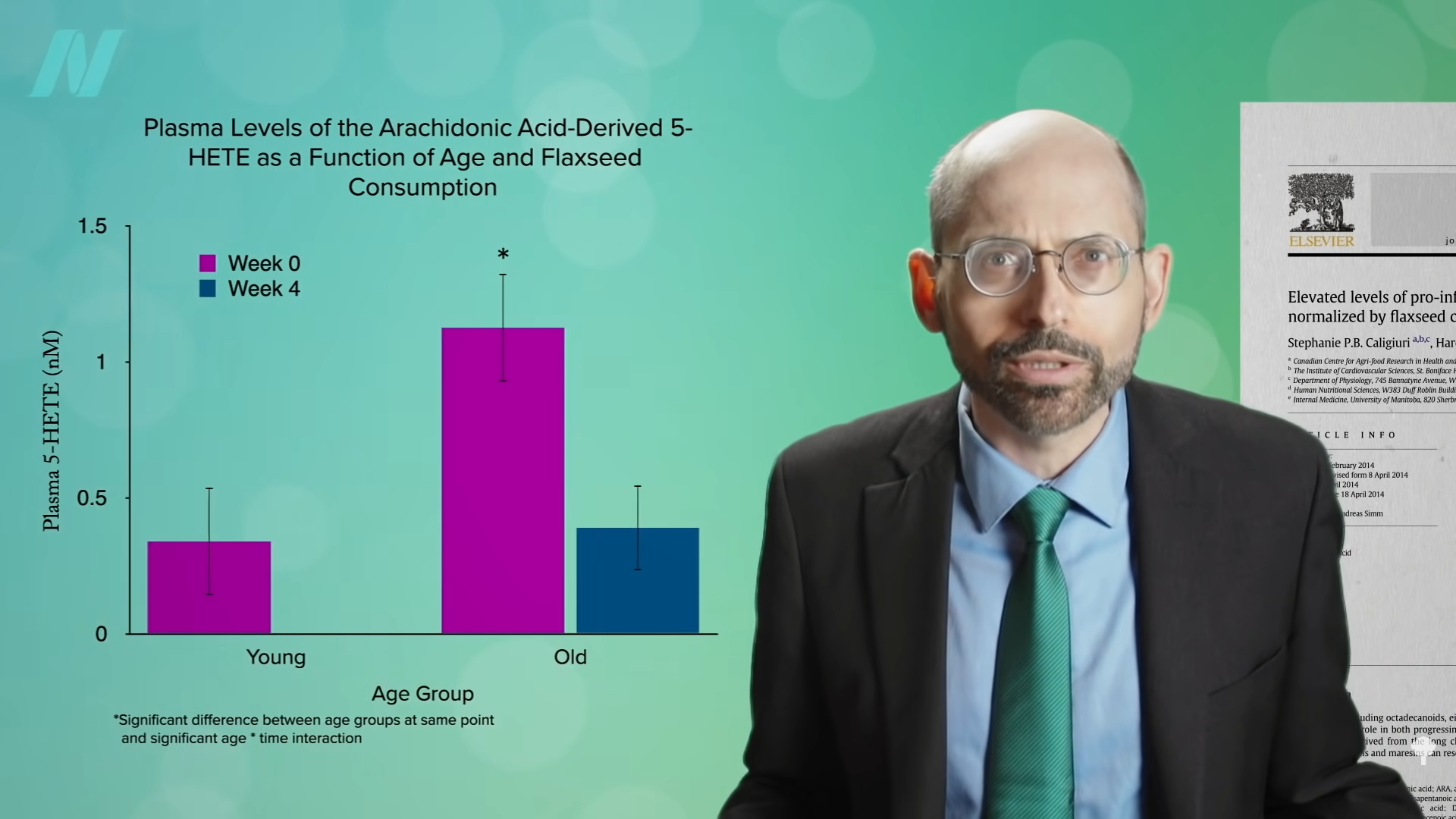
What if you took those older adults and gave them muffins, like the ones with ground flaxseed? That’s just what a group of researchers did. Four weeks later, the subjects’ levels dropped down to like 20-year-olds’ levels, as seen in the graph below and at 5:32 in my video, “demonstrating that a potential therapeutic strategy to correct the deleterious pro-inflammatory oxylipin profile is via a dietary supplementation with flaxseed.”
What about flax and cancer? See the related posts below.
I also have a video on diabetes: Flaxseeds vs. Diabetes.
If you’re interested in weight loss, see Benefits of Flaxseed Meal for Weight Loss.
What about the cyanide content of flax? I answered that in Friday Favorites: How Well Does Cooking Destroy the Cyanide in Flaxseeds and Should We Be Concerned About It?.
What else can help fight inflammation? Check out in related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link





 Even compared to spinach? As you can see in the graph below and at 3:14 in my
Even compared to spinach? As you can see in the graph below and at 3:14 in my 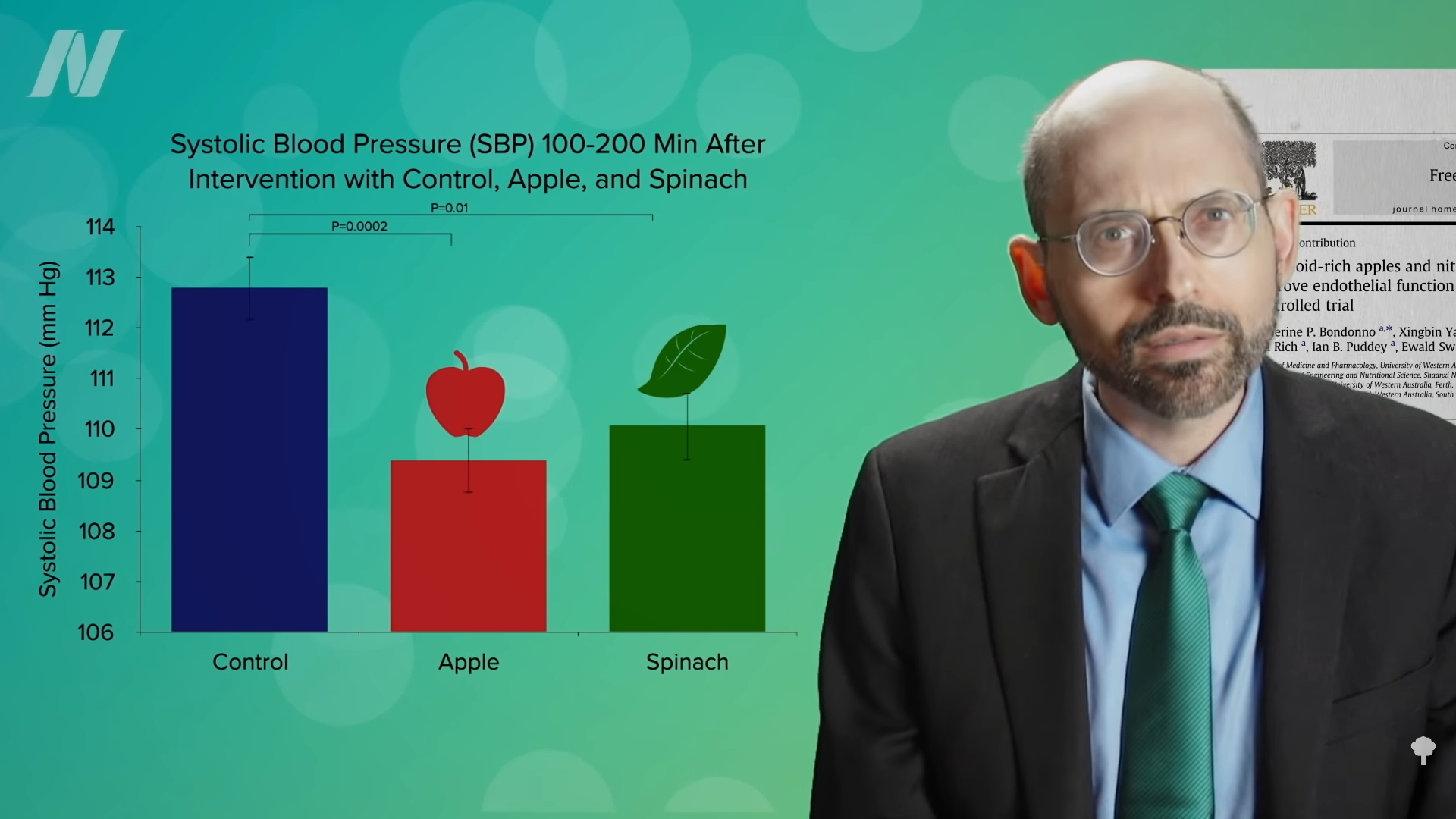 What’s nice about these results is that we’re talking about whole foods, not some supplement or extract. So, easily, “this could be translated into a natural and low-cost method of reducing the cardiovascular risk profile of the general population.”
What’s nice about these results is that we’re talking about whole foods, not some supplement or extract. So, easily, “this could be translated into a natural and low-cost method of reducing the cardiovascular risk profile of the general population.”