[ad_1]
How can you get a perfect diet score?
How do you rate the quality of people’s diets? Well, “what could be more nutrient-dense than a vegetarian diet?” Indeed, if you compare the quality of vegetarian diets with non-vegetarian diets, the more plant-based diets do tend to win out, and the higher diet quality in vegetarian diets may help explain greater improvements in health outcomes. However, vegetarians appear to have a higher intake of refined grains, eating more foods like white rice and white bread that have been stripped of much of their nutrition. So, just because you’re eating a vegetarian diet doesn’t mean you’re necessarily eating as healthfully as possible.
Those familiar with the science know the primary health importance of eating whole plant foods. So, how about a scoring system that simply adds up how many cups of fruits, vegetables, whole grains, beans, chickpeas, split peas, and lentils, and how many ounces of nuts and seeds per 1,000 calories (with or without counting white potatoes)? Looking only at the total intake of whole plant foods doesn’t mean you aren’t also stuffing donuts into your mouth. So, you could imagine proportional intake measures, based on calories or weight, to determine the proportion of your diet that’s whole plant foods. In that case, you’d get docked points if you eat things like animal-derived foods—meat, dairy, or eggs—or added sugars and fats.
My favorite proportional intake measure is McCarty’s “phytochemical index,” which I’ve profiled previously. I love it because of its sheer simplicity, “defined as the percent of dietary calories derived from foods rich in phytochemicals.” It assigns a score from 0 to 100, based on the percentage of your calories that are derived from foods rich in phytochemicals, which are biologically active substances naturally found in plants that may be contributing to many of the health benefits obtained from eating whole plant foods. “Monitoring phytochemical intake in the clinical setting could have great utility” in helping people optimize their diet for optimal health and disease prevention. However, quantifying phytochemicals in foods or tissue samples is impractical, laborious, and expensive. But this concept of a phytochemical index score could be a simple alternative method to monitor phytochemical intake.
Theoretically, a whole food, plant-based or vegan diet that excluded refined grains, white potatoes, hard liquors, added oils, and added sugars could achieve a perfect score of 100. Lamentably, most Americans’ diets today might be lucky to score just 20. What’s going on? In 1998, our shopping baskets were filled with about 20% whole plant foods; more recently, that has actually shrunk, as you can see below and at 2:49 in my video Plant-Based Eating Score Put to the Test.
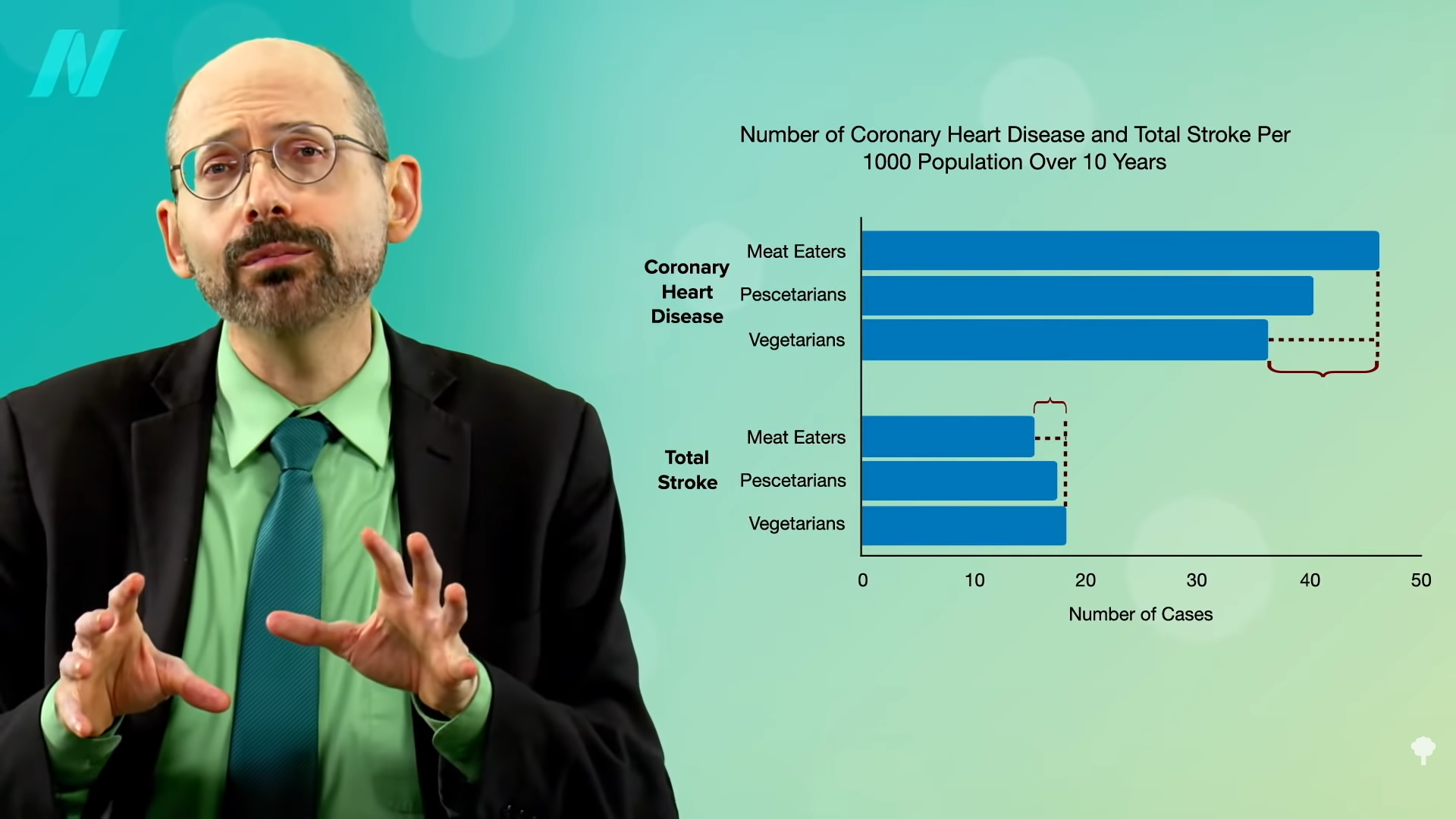
Wouldn’t it be interesting if researchers used this phytochemical index to try to correlate it with health outcomes? That’s exactly what they did. We know that studies have demonstrated that vegetarian diets have a protective association with weight and body mass index. For instance, a meta-analysis of five dozen studies has shown that vegetarians had significantly lower weight and BMI compared with non-vegetarians. And even more studies show that high intakes of fruits, vegetables, whole grains, and legumes may be protective regardless of meat consumption. So, researchers wanted to use an index that gave points for whole plant foods. They used the phytochemical index and, as you may recall from an earlier video, tracked people’s weight over a few years, using a scale of 0 to 100 to simply reflect what percentage of a person’s diet is whole plant foods. And even though the healthiest-eating tier only averaged a score of about 40, which meant the bulk of their diet was still made up of processed foods and animal products, just making whole plant foods a substantial portion of the diet may help prevent weight gain and decrease body fat. So, it’s not all or nothing. Any steps we can take to increase our whole plant food intake may be beneficial.
Many more studies have since been performed, with most pointing in the same direction for a variety of health outcomes—indicating, for instance, higher healthy plant intake is associated with about a third of the odds of abdominal obesity and significantly lower odds of high triglycerides. So, the index may be “a useful dietary target for weight loss,” where there is less focus on calorie intake and more on increasing consumption of these high-nutrient, lower-calorie foods over time. Other studies also suggest the same is true for childhood obesity.
Even at the same weight, with the same amount of belly fat, those eating plant-based diets tend to have higher insulin sensitivity, meaning the insulin they make works better in their body, perhaps thanks to the compounds in plants that alleviate inflammation and quench free radicals. Indeed, the odds of hyperinsulinemia—an indicator of insulin resistance—were progressively lower with greater plant consumption. No wonder researchers found 91% lower odds of prediabetes for people getting more than half their calories from healthy plant foods.
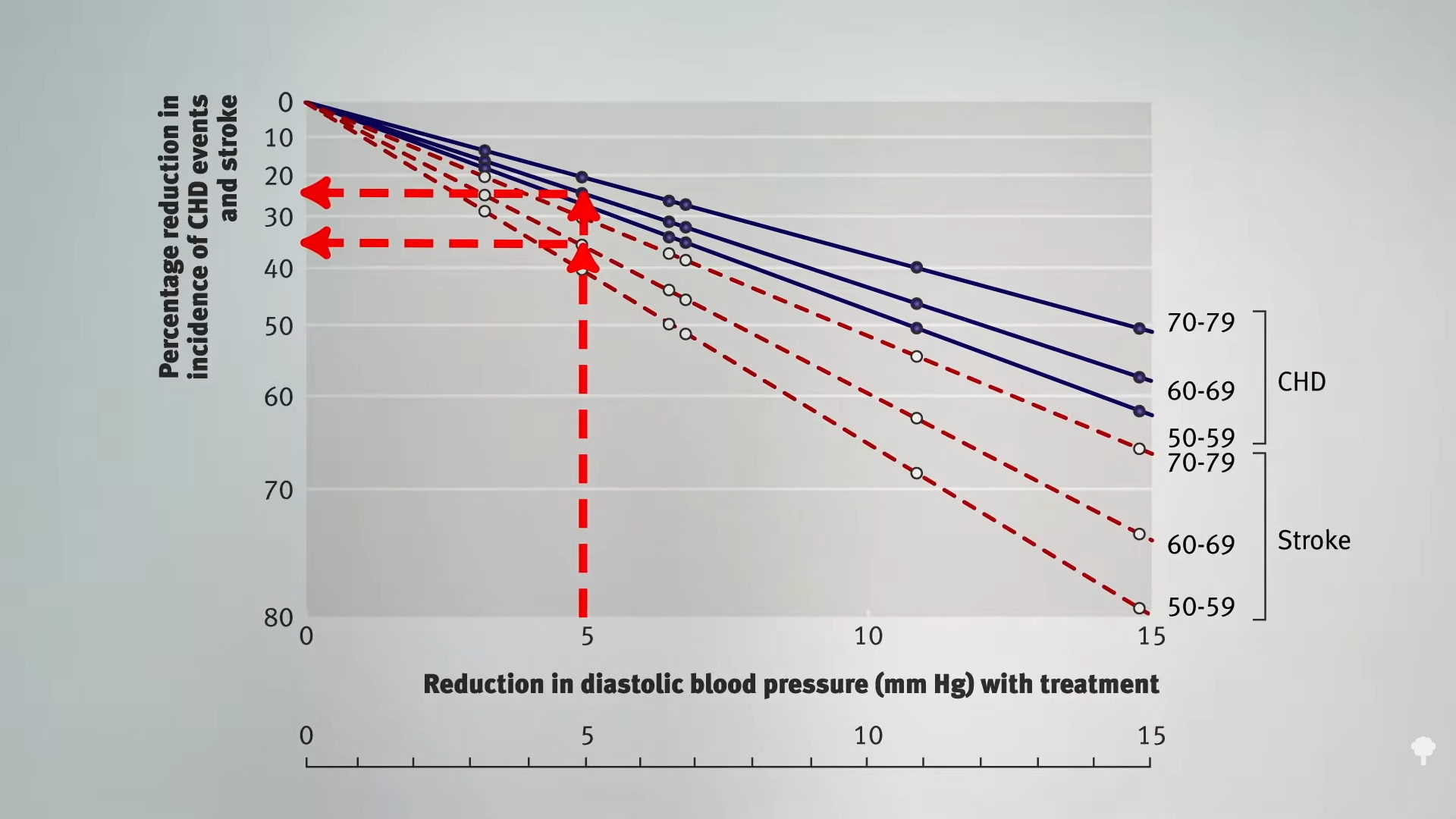
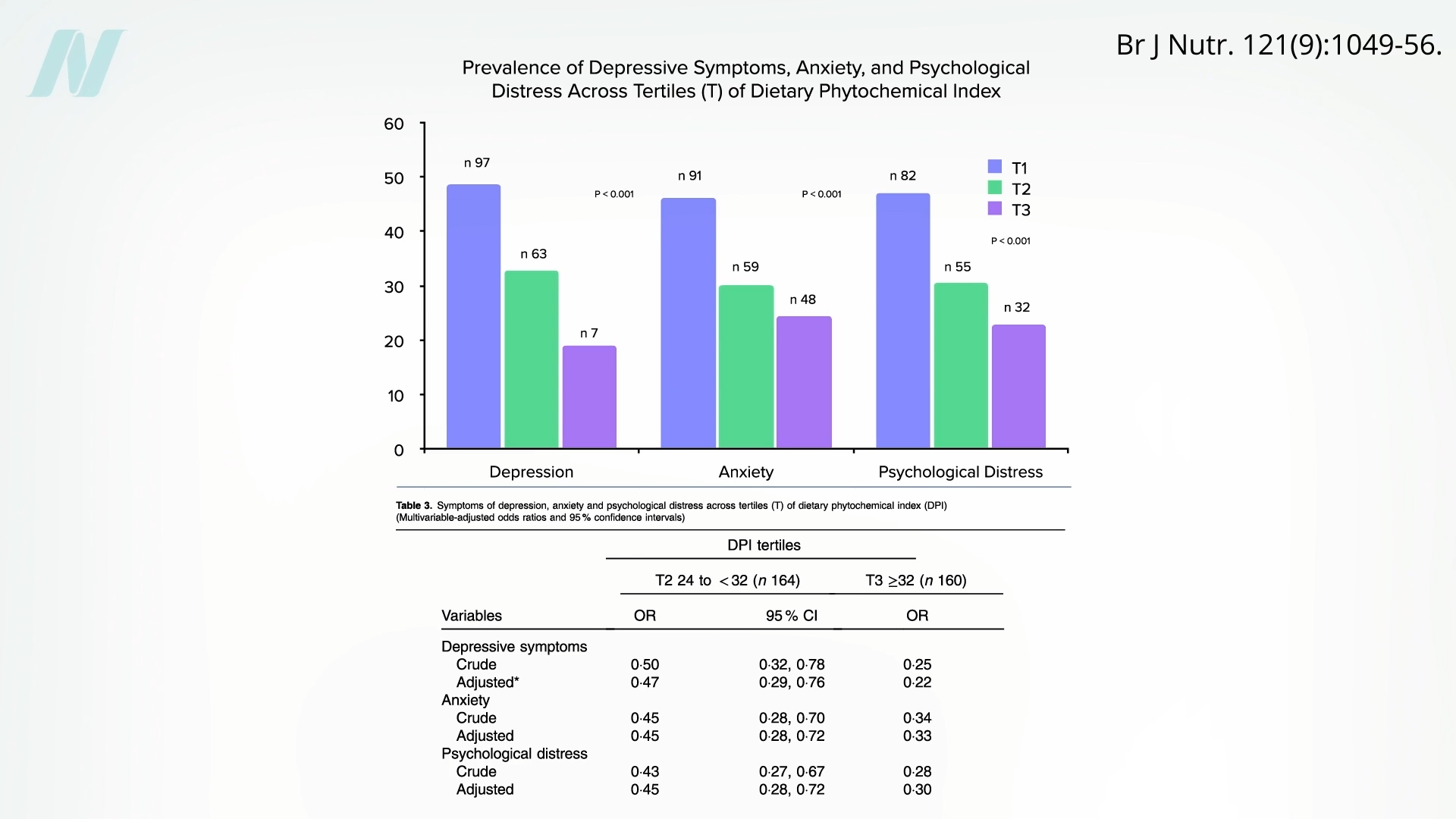
They also found significantly lower odds of metabolic syndrome and high blood pressure. There were only about half the odds of being diagnosed with hypertension over a three-year period among those eating more healthy plants. Even mental health may be impacted—about 80% less depression, 2/3 less anxiety, and 70% less psychological distress, as you can see below and at 5:15 in my video.
Is there a link between the dietary phytochemical index and benign breast diseases, such as fibrocystic diseases, fatty necrosis, ductal ectasia, and all sorts of benign tumors? Yes—70% lower odds were observed in those with the highest scores. But what about breast cancer? A higher intake of healthy plant foods was indeed associated with a lower risk of breast cancer, even after controlling for a long list of other factors. And not just by a little bit. Eating twice the proportion of plants compared to the standard American diet was linked to more than 90% lower odds of breast cancer.
Doctor’s Note
You can learn more about the phytochemical index in Calculate Your Healthy Eating Score.
If you’re worried about protein, check out Flashback Friday: Do Vegetarians Get Enough Protein?
It doesn’t have to be all or nothing, though. Do Flexitarians Live Longer?
For more on plant-based junk, check out Friday Favorites: Is Vegan Food Always Healthy?.
[ad_2]
Michael Greger M.D. FACLM
Source link