(CNN) — When was the last time you had your blood sugar checked? It might be worth looking into, a new study says.
Forty-four percent of people age 15 and older living with diabetes are undiagnosed, so they don’t know they have it, according to data analysis published Monday in the journal The Lancet Diabetes & Endocrinology.
The study looked at data from 204 countries and territories from 2000 to 2023 in a systematic review of published literature and surveys. The findings at the global level are for people age 15 and older.
“The majority of people with diabetes that we report on in the study have type 2 diabetes,” said Lauryn Stafford , the lead author of the study.
Around 1 in 9 adults live with diabetes worldwide, according to the International Diabetes Foundation. In the United States, 11.6% of Americans have diabetes, according to 2021 data from the American Diabetes Association.
“We found that 56% of people with diabetes are aware that they have the condition,” said Stafford, a researcher for the Institute for Health Metrics and Evaluation. “Globally, there’s a lot of variation geographically, and also by age. So, generally, higher-income countries were doing better at diagnosing people than low- and middle-income countries.”
Younger people don’t know they have diabetes
People under 35 years were much less likely to be diagnosed if they had diabetes than people in middle age or older. Just “20% of young adults with diabetes were aware of their condition,” Stafford said.
Routine screenings aren’t promoted as much for young adults as for older adults. Many larger organizations, like the American Diabetes Association, suggest annual routine screenings for adults 35 and older.
“You can survive with elevated glucose levels for many, many years,” Stafford said. “People end up getting diagnosed with diabetes only at the point where they have complications,” which are more common in older adults.
Depending on how long a person has had diabetes before it’s discovered, the health impacts may vary.
“Diagnosing diabetes early is important because it allows for timely management to prevent or delay long-term complications such as heart disease, kidney failure, nerve damage, and vision loss,” said Rita Kalyani, chief scientific and medical officer at the American Diabetes Association. She was not involved in the study.
Around one-third of adults are diagnosed with diabetes later than their earliest symptom, according to a 2018 study.
What symptoms should you look for?
“Symptoms of diabetes include increased thirst or hunger, frequent urination, blurry vision, unexpected weight loss, and fatigue. However, in the early stages, most people with diabetes are asymptomatic, which highlights the importance of screening and diagnosis,” said Kalyani, a professor of medicine in the division of endocrinology, diabetes and metabolism at Johns Hopkins University.
If you experience any of these symptoms or have a history of diabetes in your family, experts recommend you get a glucose screening.
Globally, in 2023, about 40% of people with treated diabetes were getting optimal results and lowering their blood sugar, said Stafford. That’s why it’s important that future efforts focus on ensuring that more people receive and follow proper treatment post-diagnosis.
That only 4 in 10 patients were seeing optimal results was surprising, as several well-established treatments, including insulin, Metformin and other drugs like GLP-1s, are available.
People with diabetes likely also have other health issues, such as hypertension or chronic kidney disease, which can make treatment complex, Stafford added.
Can you prevent diabetes?
It depends.
While there is no known way to prevent type 1 diabetes, there are many ways to prevent the more common form of type 2 diabetes.
Reducing the amount of red and processed meats you eat can help lower your risk of type 2 diabetes, as previously reported by CNN. You could do this with a Mediterranean diet or by introducing more plant-based foods to your meals.
In addition, limit the amount of ultraprocessed foods you eat, adding more whole foods, like fruits and nuts, instead.
Incorporating physical activity into your regular routine can also decrease your risk of developing not only diabetes but also other chronic diseases. Fast walking for at least 15 minutes a day is just one form of exercise you can do.
“I think, ultimately, if we can also focus more on the risk factors for developing diabetes — preventing people from needing to be diagnosed in the first place — that is also critical,” Stafford said.
A sweeping review published in The Lancet Regional Health—Europe has drawn a direct line between mental health disorders and cardiovascular disease (CVD), showing that individuals living with psychiatric conditions face not only a higher risk of heart problems but also a shorter life expectancy. The paper, authored by researchers from Emory University, the University of Copenhagen, the University of Leeds, and others, concludes that people with depression, schizophrenia, bipolar disorder, post-traumatic stress disorder (PTSD), and anxiety live 10 to 20 years less on average, mainly due to heart disease.
A Bidirectional Threat
The analysis shows that the connection between mental health and cardiovascular disease is not one-directional. The stress of a heart attack or stroke can trigger psychiatric disorders, while psychiatric conditions themselves set the stage for heart disease. The risks are striking as depression raises cardiovascular risk by 72 percent, schizophrenia by 95 percent, bipolar disorder by 57 percent, PTSD by 61 percent, and anxiety disorders by 41 percent. “It is important to understand that stress, anxiety, and depression can affect your heart, just like other physical factors,” the paper noted, offering guidance for how doctors might begin crucial conversations with patients.
A Widespread Burden
One in four people will experience a mental health disorder in their lifetime, yet many go untreated and often receive poor cardiovascular care. “Despite having more interactions with the healthcare system, they undergo fewer physical checkups and screenings and receive fewer diagnoses and treatments for CVD and its risk factors,” the authors reported. According to 2023 U.S. survey data cited in the study, more than half of those who met the criteria for a mental health disorder had not received any treatment, with even lower rates among non-White populations.
Shared Risk Factors
Researchers identified a cluster of overlapping drivers—poverty, trauma, social disadvantage, substance use, and poor access to health care—that amplify the dual risks of mental illness and cardiovascular disease. Lifestyle behaviors such as smoking, poor diet, physical inactivity, and disrupted sleep patterns are also more common among people with psychiatric conditions. The biological picture is equally troubling. Dysregulation of the stress response system, inflammation, and autonomic nervous system dysfunction are all pathways through which psychiatric disorders may accelerate cardiovascular decline.
Breaking the Cycle
The study calls for a fundamental shift in medical practice. “For the best care, an integrated approach is needed to address the complex needs of this vulnerable population,” the authors wrote. “Such approach should offer enhanced support and interdisciplinary care encompassing mental, cardiovascular, and behavioral health, as well as consideration of the social needs and barriers to care.” Among the interventions reviewed, exercise emerged as one of the most effective treatments, improving both mood and heart health. Evidence shows that physical activity can deliver improvements on par with or greater than medication or psychotherapy for depression. Mind-body practices like yoga and mindfulness, while requiring more evaluation, also show promise for improving outcomes across both mental and cardiovascular health.
A Call to Integrate Care
The authors stressed that progress depends on healthcare systems breaking down the wall between physical and mental health. For decades, treatment has been siloed, with psychiatrists focusing on the mind and cardiologists on the body. That separation, the study finds, has left millions vulnerable. The authors argue for expanded insurance coverage, investment in housing and employment stability, and the inclusion of psychiatric patients in cardiovascular research. Above all, they call for integrated care models that recognize the tight link between mental and cardiovascular health.
“Closing the disparity gap for individuals with mental health disorders would be consistent with the World Health Organization 2025 targets of reducing the global burden of CVD,” the researchers concluded. “Reducing these disparities would also uphold the rights of people with mental health disorders to achieve the highest possible level of health and to fully participate in society and the workforce.”
Related
[ad_2]
Stacy M. Brown, NNPA Newswire Senior National Correspondent and NNPA
Doctors may soon have a new way to treat high blood pressure, even among people for whom medicines haven’t worked well in the past.Baxdrostat, an experimental medicine made by AstraZeneca, showed promise in treating people with uncontrolled or resistant high blood pressure in a recent trial. If the medicine gets approved by regulatory authorities, it will be one of the first new approaches to treating high blood pressure in decades, researchers say.Scientists presented the trial results Saturday at the European Society of Cardiology Congress 2025 in Madrid and simultaneously published them in the New England Journal of Medicine.For the study, researchers enrolled 800 adults who still had high blood pressure after taking two or more medications for at least four weeks. To qualify for the study, patients’ systolic blood pressure had to be between 140 and 170.Blood pressure is measured in millimeters of mercury, which is abbreviated as mm Hg. The measurement has an upper number, or systolic reading, and a lower number, a diastolic reading. Systolic pressure measures the force of blood as it pumps out of the heart into the arteries; diastolic is the pressure created as the heart rests between beats.Normal blood pressure is less than 120/80 mm Hg, and elevated blood pressure is considered to be from 120 to 129/80 mm Hg. At 130/80 mmHg or higher, according to new U.S. guidelines, a person’s medical provider will want them to take a blood pressure medication if lifestyle changes — including eating healthier, reducing salt in the diet and exercising more — don’t work first.The researchers on the new trial placed the participants into three groups. One received 1 milligram of baxdrostat, another got 2 mg, and another got a placebo, which does nothing. Participants took their dose in addition to medicines they were already taking.At 12 weeks, about 4 in 10 patients taking baxdrostat reached healthy blood pressure levels, compared with less than 2 in 10 who got a placebo.Specifically, participants who got 1 or 2 mg of baxdrostat daily saw their systolic blood pressure – the upper number in the reading – fall around 9 to 10 mm Hg more than those taking a placebo. This reduction, studies show, is large enough to cut cardiovascular risk.When blood pressure is high, the force of the blood pushes against the walls of their blood vessels, making the heart less efficient: Both the vessels and the heart must work harder, and it’s more difficult to get blood to essential organs and cells. Without treatment, high blood pressure will eventually damage the arteries, raising the risk of conditions like a heart attack, stroke, coronary disease, vascular dementia and cognitive problems.Heart disease is the No. 1 killer in the world. Lowering blood pressure is the most modifiable way to avoid such a death.Nearly half of all adults in the U.S. have higher than normal blood pressure, and 1 in 10 people have what doctors call resistant hypertension: Despite being on three or more medications, they are not meeting the goal for blood pressure control.When a patient has high blood pressure, doctors may need to try a variety of medications to see what works best.Adding baxdrostat to the list of options could be a big help for patients, according to Dr. Stacey E. Rosen, volunteer president of the American Heart Association, who was not involved with the new research.“What’s interesting about this medication is that they can really be a wonderful partner, so to speak, with some of the more classically recommended anti-hypertensive medications,” said Rosen, who is also a senior vice president of women’s health and executive director of the Katz Institute for Women’s Health of Northwell Health in New York City.Medication options now on the market control blood pressure in a variety of ways. Some, such as vasodilators, relax and widen arteries and veins to allow blood to get through easier and increase flow. Diuretics primarily work by removing excess fluid and salt from the body by increasing urine production. Centrally acting alpha agonists help prevent the nervous system from responding to stress. ACE inhibitors keep the body from producing angiotensin II, a hormone that makes blood vessels constrict. ARBs, or angiotensin II receptor blockers, help reduce the production of aldosterone, a hormone that promotes salt and water retention. Calcium channel blockers can keep calcium away from the cells of the heart and arteries so they don’t have to work as hard.Each can have different side effects, including dizziness, rapid or slower heart rate, exhaustion, upset stomach and swelling in the legs.Baxdrostat’s side effects, the study showed, were mild overall. The most common problem was abnormalities in potassium and sodium levels, but this was rare.Baxdrostat takes a new approach to managing high blood pressure. It focuses on blocking aldosterone, a hormone created by the adrenal glands that helps kidneys regulate salt and maintain the body’s water balance. Some people produce too much aldosterone, leading their body to retain too much water and salt, pushing up blood pressure.“We’ve also known for a while now that most of us eat too much salt and in doing that, it raises blood pressure. But we’re also increasingly recognizing that aldosterone may have a direct impact on causing damage to the blood vessels, to the heart, to the kidneys,” said Dr. Jenifer Brown, one of the lead investigators and co-author of the published study.Brown said she often sees cardiology patients at Brigham and Women’s who may have had a heart event, so she needs to be aggressive in getting their blood pressure under control to prevent another. Some patients may have trouble tolerating other blood pressure medications. For others, the standard medicines just don’t work well. Baxdrostat could be a good complement, she said.“We really have had the same tools as clinicians for many years,” Brown said. “I would be excited to have an option like this.”In an editorial accompanying the publication, Dr. Tomasz Guzik, a cardiovascular scientist at the University of Edinburgh, and Dr. Maciej Tomaszewski, a cardiovascular expert at the University of Manchester, write that next steps should be to figure out which patients would best respond to this new medicine and provide longer-term data. If the medication works long-term, they wrote, it could become a “central piller of therapy for difficult-to-control hypertension.”AstraZeneca said it plans to submit its data to regulatory agencies before the end of 2025.
Doctors may soon have a new way to treat high blood pressure, even among people for whom medicines haven’t worked well in the past.
Baxdrostat, an experimental medicine made by AstraZeneca, showed promise in treating people with uncontrolled or resistant high blood pressure in a recent trial. If the medicine gets approved by regulatory authorities, it will be one of the first new approaches to treating high blood pressure in decades, researchers say.
Scientists presented the trial results Saturday at the European Society of Cardiology Congress 2025 in Madrid and simultaneously published them in the New England Journal of Medicine.
For the study, researchers enrolled 800 adults who still had high blood pressure after taking two or more medications for at least four weeks. To qualify for the study, patients’ systolic blood pressure had to be between 140 and 170.
Blood pressure is measured in millimeters of mercury, which is abbreviated as mm Hg. The measurement has an upper number, or systolic reading, and a lower number, a diastolic reading. Systolic pressure measures the force of blood as it pumps out of the heart into the arteries; diastolic is the pressure created as the heart rests between beats.
Normal blood pressure is less than 120/80 mm Hg, and elevated blood pressure is considered to be from 120 to 129/80 mm Hg. At 130/80 mmHg or higher, according to new U.S. guidelines, a person’s medical provider will want them to take a blood pressure medication if lifestyle changes — including eating healthier, reducing salt in the diet and exercising more — don’t work first.
The researchers on the new trial placed the participants into three groups. One received 1 milligram of baxdrostat, another got 2 mg, and another got a placebo, which does nothing. Participants took their dose in addition to medicines they were already taking.
At 12 weeks, about 4 in 10 patients taking baxdrostat reached healthy blood pressure levels, compared with less than 2 in 10 who got a placebo.
Specifically, participants who got 1 or 2 mg of baxdrostat daily saw their systolic blood pressure – the upper number in the reading – fall around 9 to 10 mm Hg more than those taking a placebo. This reduction, studies show, is large enough to cut cardiovascular risk.
When blood pressure is high, the force of the blood pushes against the walls of their blood vessels, making the heart less efficient: Both the vessels and the heart must work harder, and it’s more difficult to get blood to essential organs and cells. Without treatment, high blood pressure will eventually damage the arteries, raising the risk of conditions like a heart attack, stroke, coronary disease, vascular dementia and cognitive problems.
Heart disease is the No. 1 killer in the world. Lowering blood pressure is the most modifiable way to avoid such a death.
Nearly half of all adults in the U.S. have higher than normal blood pressure, and 1 in 10 people have what doctors call resistant hypertension: Despite being on three or more medications, they are not meeting the goal for blood pressure control.
When a patient has high blood pressure, doctors may need to try a variety of medications to see what works best.
Adding baxdrostat to the list of options could be a big help for patients, according to Dr. Stacey E. Rosen, volunteer president of the American Heart Association, who was not involved with the new research.
“What’s interesting about this medication is that they can really be a wonderful partner, so to speak, with some of the more classically recommended anti-hypertensive medications,” said Rosen, who is also a senior vice president of women’s health and executive director of the Katz Institute for Women’s Health of Northwell Health in New York City.
Medication options now on the market control blood pressure in a variety of ways. Some, such as vasodilators, relax and widen arteries and veins to allow blood to get through easier and increase flow. Diuretics primarily work by removing excess fluid and salt from the body by increasing urine production. Centrally acting alpha agonists help prevent the nervous system from responding to stress. ACE inhibitors keep the body from producing angiotensin II, a hormone that makes blood vessels constrict. ARBs, or angiotensin II receptor blockers, help reduce the production of aldosterone, a hormone that promotes salt and water retention. Calcium channel blockers can keep calcium away from the cells of the heart and arteries so they don’t have to work as hard.
Each can have different side effects, including dizziness, rapid or slower heart rate, exhaustion, upset stomach and swelling in the legs.
Baxdrostat’s side effects, the study showed, were mild overall. The most common problem was abnormalities in potassium and sodium levels, but this was rare.
Baxdrostat takes a new approach to managing high blood pressure. It focuses on blocking aldosterone, a hormone created by the adrenal glands that helps kidneys regulate salt and maintain the body’s water balance. Some people produce too much aldosterone, leading their body to retain too much water and salt, pushing up blood pressure.
“We’ve also known for a while now that most of us eat too much salt and in doing that, it raises blood pressure. But we’re also increasingly recognizing that aldosterone may have a direct impact on causing damage to the blood vessels, to the heart, to the kidneys,” said Dr. Jenifer Brown, one of the lead investigators and co-author of the published study.
Brown said she often sees cardiology patients at Brigham and Women’s who may have had a heart event, so she needs to be aggressive in getting their blood pressure under control to prevent another. Some patients may have trouble tolerating other blood pressure medications. For others, the standard medicines just don’t work well. Baxdrostat could be a good complement, she said.
“We really have had the same tools as clinicians for many years,” Brown said. “I would be excited to have an option like this.”
In an editorial accompanying the publication, Dr. Tomasz Guzik, a cardiovascular scientist at the University of Edinburgh, and Dr. Maciej Tomaszewski, a cardiovascular expert at the University of Manchester, write that next steps should be to figure out which patients would best respond to this new medicine and provide longer-term data. If the medication works long-term, they wrote, it could become a “central piller of therapy for difficult-to-control hypertension.”
AstraZeneca said it plans to submit its data to regulatory agencies before the end of 2025.
WASHINGTON — A divided Supreme Court said Thursday the Trump administration may cancel hundreds of health research grants that involve diversity, equity and inclusion or gender identity.
The justices granted an emergency appeal from President Trump’s lawyers and set aside a Boston’s judge order that blocked the canceling of $783 million in research grants.
The justices split 5-4. Chief Justice John G. Roberts Jr. joined the court’s three liberals in dissent and said the district judge had not overstepped his authority.
The court’s conservative majority has repeatedly sided with the administration and against federal judges in disputes over spending and staffing at federal agencies.
In the latest case, the majority agreed that Trump and his appointees may decide on how to spend health research funds allocated by Congress.
Upon taking office in January, Trump issued an executive order “ending radical and wasteful government DEI programs and preferencing.”
A few weeks later, the acting director of the National Institutes of Health said the agency would no longer fund “low-value and off-mission research programs, including but not limited to studies based on diversity, equity, and inclusion (DEI) and gender identity.”
More than 1,700 grants were canceled.
Trump’s lawyers told the court the NIH had terminated grants to study “Buddhism and HIV stigma in Thailand”; “intersectional, multilevel and multidimensional structural racism for English- and Spanish-speaking populations”; and “anti-racist healing in nature to protect telomeres of transitional age BIPOC [Black, Indigenous, and People of Color] for health equity.”
California Atty. Gen. Rob Bonta and his counterparts from 15 Democrat-led states had sued to halt what they called an “unprecedented disruption to ongoing research.” They were joined by groups of researchers and public health advocates.
The state attorneys said their public universities were using grant money for “projects investigating heart disease, HIV/AIDS, Alzheimer’s disease, alcohol and substance abuse, mental-health issues, and countless other health conditions.”
They said the NIH had terminated a grant for a University of California study examining how inflammation, insulin resistance and physical activity affect Alzheimer’s disease in Black women, a group with higher rates and a more aggressive profile of the disease.
Also terminated, they said, was a University of Hawaii study that aimed to identify genetic and biological risk factors for colorectal cancer among Native Hawaiians, a population with increased incidence and mortality rates of that disease.
In June, the Democratic state attorneys won a ruling from U.S. District Judge William G. Young, a Reagan appointee. He said the sudden halt to research grants violated a federal procedural law because it was “arbitrary” and poorly explained.
He said Trump had required agencies “to focus on eradicating anything that it labels as Diversity, Equity and Inclusion (“DEI”), an undefined enemy.” He said he had tried and failed to get a clear definition of DEI and what it entailed.
When the 1st Circuit Court refused to lift the judge’s order, Trump’s Solicitor Gen. D. John Sauer appealed to the Supreme Court in late July.
The solicitor general argued that Trump’s order rescinded an executive order from President Biden in 2021 that mandated “an ambitious whole-of-government equity agenda” and instructed federal agencies to “allocate resources to address the historic failure to invest sufficiently, justly, and equally in underserved communities.”
He said the new administration decided these DEI-related grants “do nothing to expand our knowledge of living systems, provide low returns on investment, and ultimately do not enhance health, lengthen life, or reduce illness.”
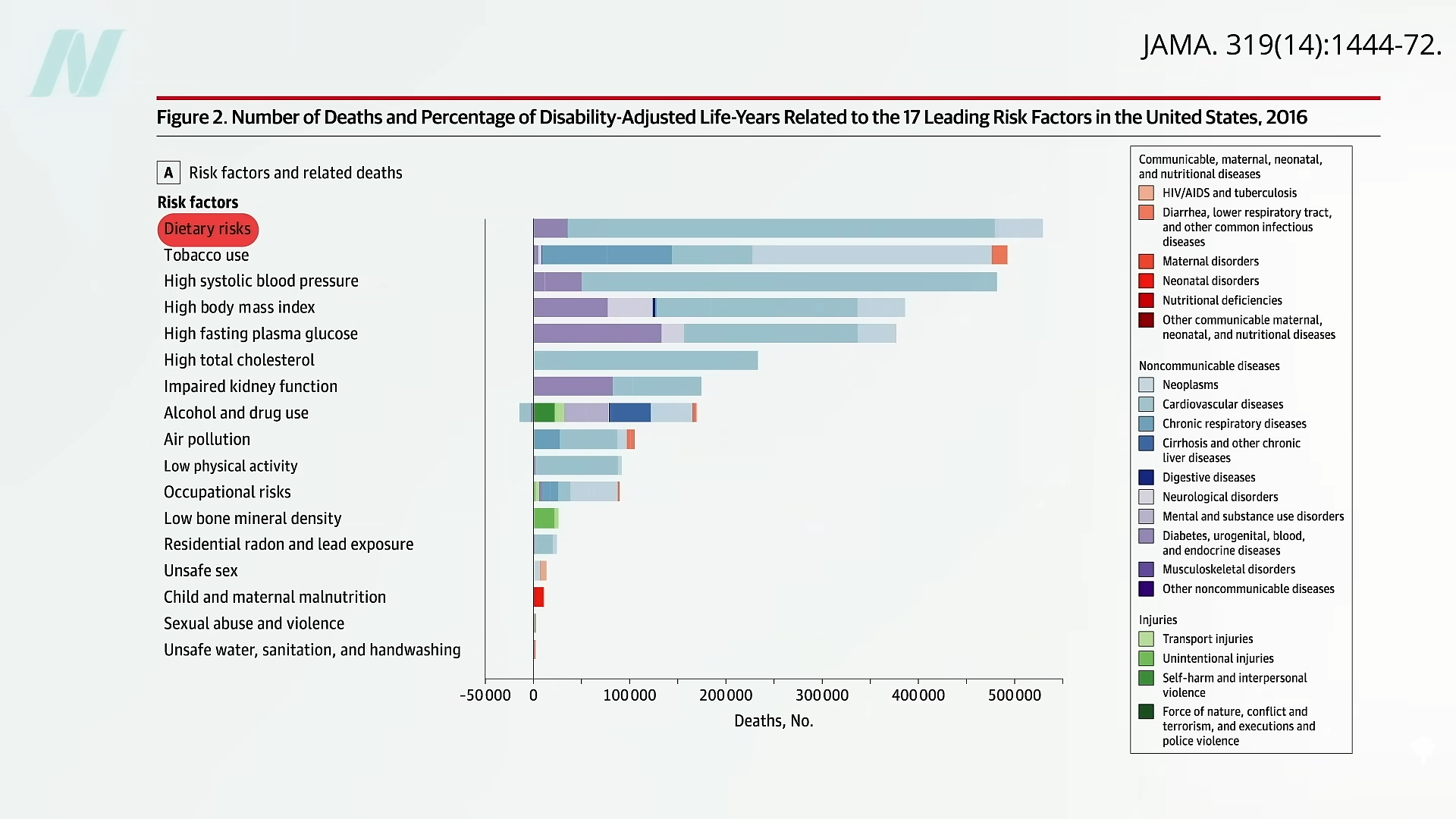
The leading risk factor for death in the United States is the American diet.
About a decade ago, the American Heart Association (AHA) expressed concern that its “2020 target of improving cardiovascular health by 20% by 2020 will not be reached if current trends continue.” By 2006, most people were already not smoking and had nearly achieved their goal for exercise. But when it came to healthy diet score, only about 1 percent got a 4 or 5 out of its diet quality score of 0 to 5, as you can see below and at 0:35 in my video, Friday Favorites: The Scientific Consensus on a Healthy Diet. And that’s with such “ideal” criteria as drinking less than four and a half cups of soda a week.
In the last decade, the AHA saw a bump in the prevalence of the ideal healthy diet score to about 1 percent of Americans reaching those kinds of basic criteria, but, given its “aggressive” goal of reaching a “20% target” by 2020, it hoped to turn that 1 percent into about 1.2 percent. (Really, as you can see here and at 1:01 in my video.)
So, how’d we do? According to the 2019 update, it seems we’ve slipped down to as low as one in a thousand, and American teens scored a big fat zero. No wonder, perhaps, that “for all mortality-based metrics, the US rank declined…to 27th or 28th among 34 OECD [industrialized] countries. Citizens living in countries with a substantially lower gross domestic product and health expenditure per capita…have lower mortality rates than those in the United States.” Slovenia, for example, beat the United States, ranking 24th in life expectancy. More recently, the United States’s life expectancy slipped further, down to 43rd in the world, although the United States spent the most ($3.0 trillion) on health care…”
What is the leading risk factor for death in the United States? As seen below and at 2:04 in my video, it is the standard American diet. Those trillions in health care spending aren’t addressing the root cause of disease, disability, and death.
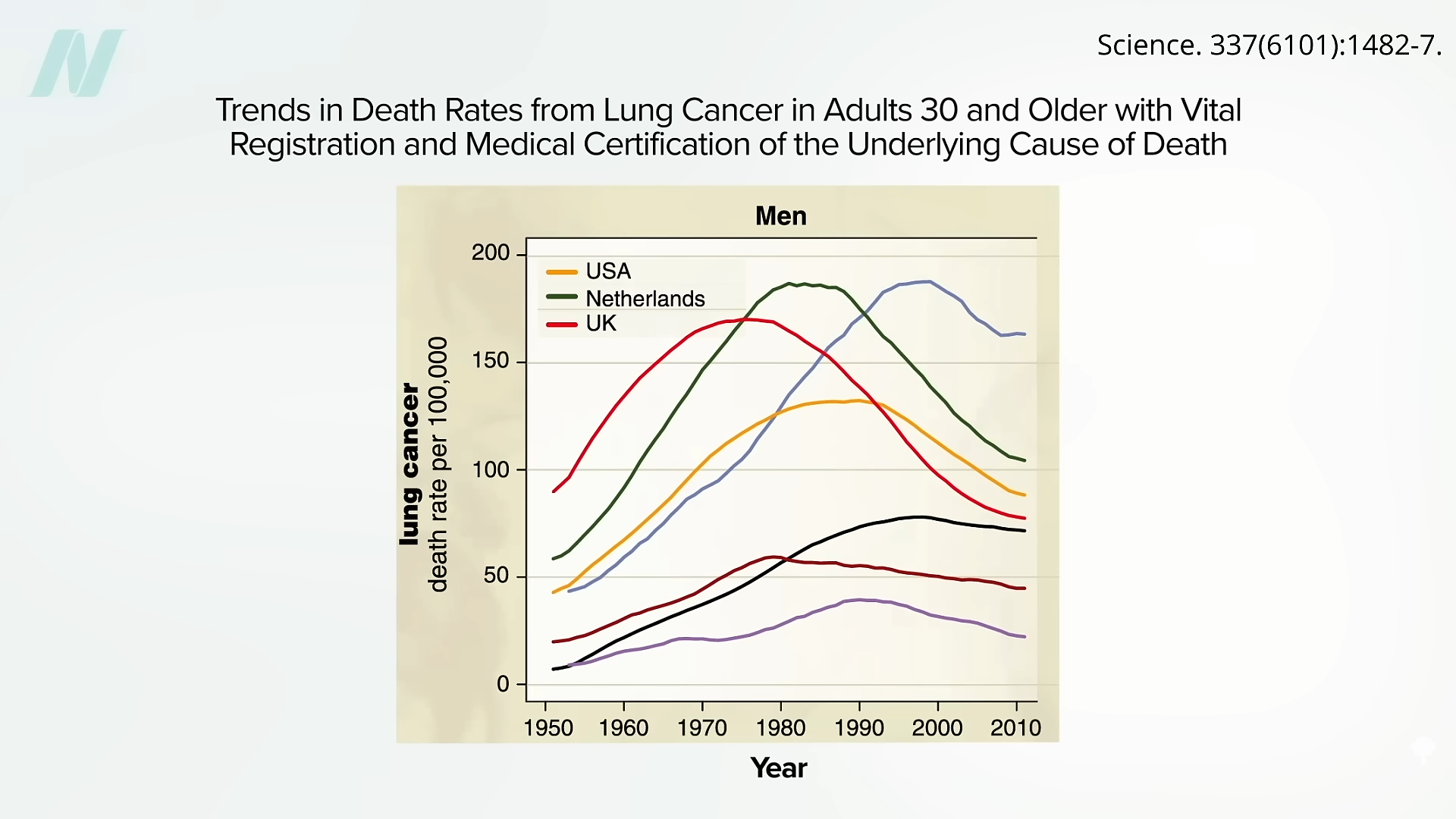
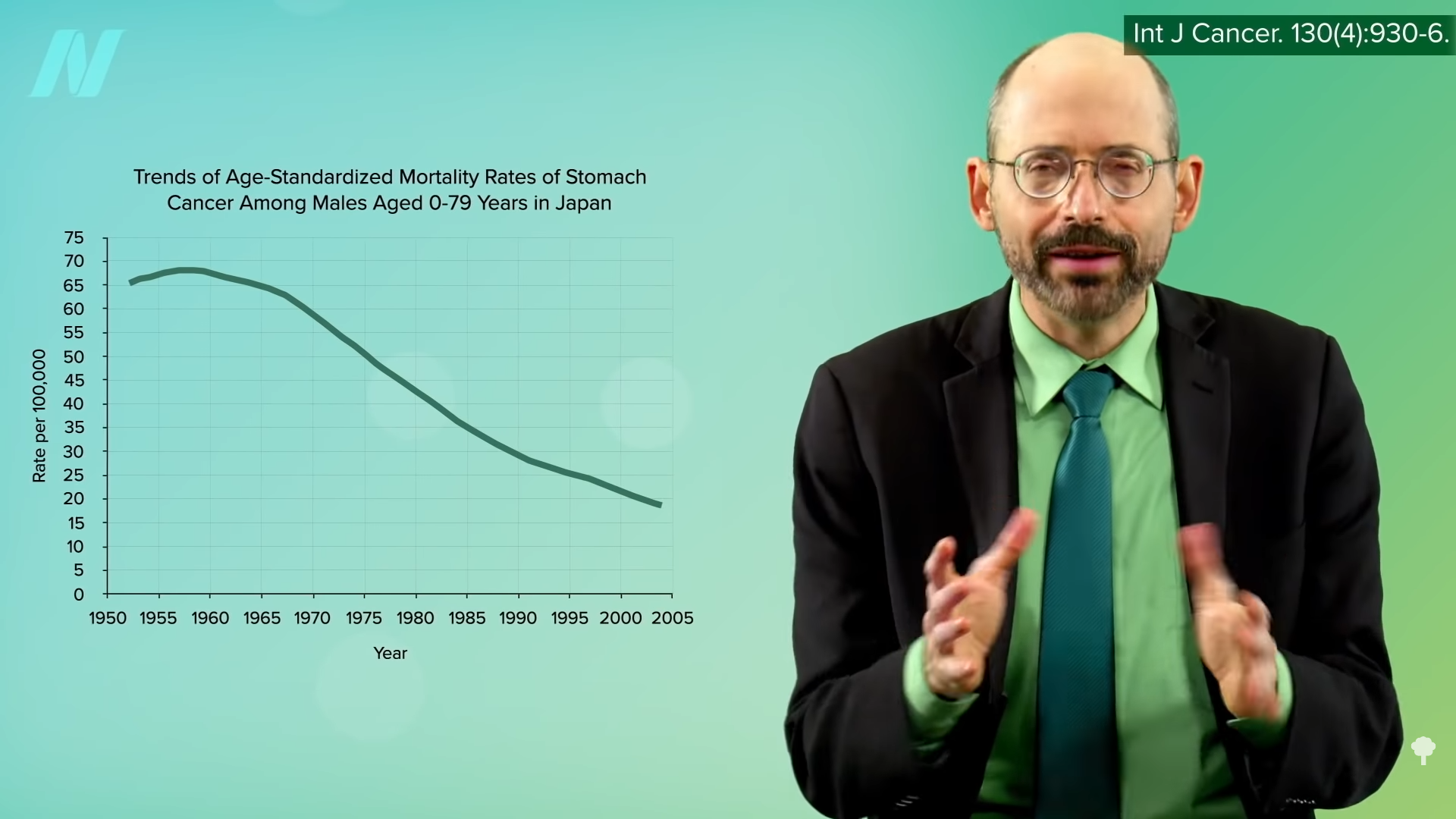
Here are some of the lung cancer death curves, below and at 2:08 in my video:
It took decades to finally turn the corner, but it’s so nice to finally see those drops. When will we see the same with diet?
“Approximately 80% of chronic disease and premature death could be prevented by not smoking, being physically active, and adhering to a healthful dietary pattern.” What exactly is meant by “healthy diet”? “Unfortunately, media messages surrounding nutrition are often inconsistent, confusing, and do not enable the public to make positive changes in health behaviors….Certainly, there is pressure within today’s competitive journalism market for sensationalism. There may even be a disincentive to present the facts in the context of the total body of information consumers need to act on dietary recommendations.” And there’s an incentive to sell more magazines and newspapers. The paper I’m quoting was written in 1997, before the lure of clickbait headlines. In fact, about three-quarters of a century ago, it was noted: “It is unfortunate that the subject of nutrition seems to have a special appeal to the credulous, the social zealot and, in the commercial field, the unscrupulous….The combination is one calculated to strike despair in the hearts of the sober, objective scientist.”
Indeed, the most important health care problem we face may be “our poor lifestyle choices based on misinformation.” It is like the climate change deniers: “Analogous to outspoken cynics denying climate change and influencing public opinion, healthy lifestyle and dietary advice are overshadowed by critics, diet books, the food industry, and misguided information in the media.” Maybe we need an entity like the Intergovernmental Panel on Climate Change (IPCC)—but for nutrition.
These days, “no single expert, regardless of academic stature or reputation, has the prominence to overcome the obstacles created by confusing media messages and deliver the fundamental principles of healthy living effectively to the public.”
What if there were “a global coalition consisting of a variety of nutrition experts, who collectively represent the views held by the majority of scientists, physicians, and health practitioners” that could “serve as the guiding resource of sound nutrition information for improved health and prevention of disease”?
Enter the True Health Initiative, which “was conceived for that very purpose.” A nonprofit coalition of hundreds of experts from dozens of countries has agreed to a consensus statement on the fundamentals of healthy living. See www.truehealthinitiative.org.
Spoiler alert: The healthiest diet is one generally comprised mostly of minimally processed plants.
There is a reason the U.S. Centers for Disease Control and Prevention prohibits not only smoking but also scented or fragranced products in its buildings.
In a recent review entitled “Damaging Effects of Household Cleaning Products on the Lungs,” researchers noted: “Adverse respiratory effects of cleaning products were first observed in populations experiencing high levels of exposure at the workplace, such as cleaners and health-care workers, with a primary focus on asthma.” Occupational use of disinfectants has also been linked to a higher risk of developing chronic obstructive pulmonary disease, such as emphysema.
As I discuss in my video Friday Favorites: The Effects of Cleaning Products and Air Fresheners on Lung Function, we now know that, in addition to workplace exposures, “exposure to household cleaning products has also emerged as a risk factor for respiratory disorders in childhood,” as well potentially being “an important risk factor for adult asthma.” Common household cleaning spray use accounts for as many as one in seven adult asthma cases. The thought is that inhaling chemical irritants may cause injury to the airways, leading to oxidative stress and inflammation. What can we do about it?
Well, it may be limited to sprays. Researchers found that cleaning products that were not sprayed were not associated with asthma. It’s also possible that environmentally friendly cleaning products “may represent a safer alternative,” though they may still present some risk.
Ideally, safer cleaning products should be available. Unfortunately, the research suggesting harm has “seldom been heeded by manufacturers, vendors, and commercial cleaning companies.” I wonder how much of that is because “most of the workers exposed to cleaning products are women”—both occupationally and, perhaps, domestically.
One of the problems may be the fragrance chemicals. One in three Americans surveyed “reported health problems, such as migraine headaches and respiratory difficulties, when exposed to fragranced products.” And, for about half of them, the problems were so bad they actually lost work over it, either “workdays or a job due to fragranced product exposure in the workplace.”
“Results from this study reveal that over one-third of Americans suffer adverse health effects, such as respiratory difficulties and migraine headaches, from exposure to fragranced products. Of those individuals, half reported that the effects can be disabling. Yet over 99% of Americans are exposed to fragranced products at least once a week, from their own or others’ use.”
The effect on asthmatics may be even worse, affecting closer to two-thirds of Americans. One compound that may be of particular concern is called 1,4-dichlorobenzene, also known as para-dichlorobenzene, which is found in many air fresheners, toilet bowl deodorants, and mothballs. It breaks down in the body into a compound called 2,5-dichlorophenol, which we pee out, giving researchers a reliable measure of our dichlorobenzene exposure. Not only may it make respiratory problems worse for those already suffering from compromised airways, but exposure to dichlorobenzene “at [blood] levels found in the U.S. general population, may result in reduced pulmonary [lung] function” in people who start out with normal breathing. What’s worse, higher exposures “were associated with greater prevalence of CVD [cardiovascular disease] and all cancers combined,” another reason to avoid it. We’d better read labels, right?
Surprisingly, “no law in the US requires the disclosure of all ingredients in fragranced consumer products.” In fact, for laundry supplies, cleaning products, and air fresheners, manufacturers “do not need to list the presence of a ‘fragrance’ on either the label or MSDS,” the material safety data sheet. We won’t know until we smell it.
I support the U.S. Centers for Disease Control and Prevention’s ban. Not only is “the use of tobacco products (including cigarettes, cigars, pipes, smokeless tobacco, or other tobacco products)…prohibited at all times,” but “scented or fragranced products are prohibited at all times in all interior space owned, rented, or leased by CDC.” I wish rideshare services like Uber and Lyft would have a similar policy. I’d even be happy with just a fragrance-free option. About one in five of more than a thousand Americans surveyed said they “would enter a business but then leave as quickly as possible if they smelled air fresheners or some fragranced product,” so it’s in the best interest of businesses, too. “Over 50% of the population would prefer that workplaces, health care facilities and professionals, hotels, and airplanes were fragrance-free.”
Randomized controlled trials show that lowering saturated fat intake can lead to improved breast cancer survival.
The leading cause of cancer-related death is metastasis. Cancer kills because cancer spreads. The five-year survival rate for women with localized breast cancer is nearly 99 percent, for example, but that falls to only 27 percent in women with metastasized cancer. Yet, “our ability to effectively treat metastatic disease has not changed significantly in the past few decades…” The desperation is evident when there are such papers as “Targeting Metastasis with Snake Toxins: Molecular Mechanisms.”
We have built-in defenses, natural killer cells that roam the body, killing off budding tumors. But, as I’ve discussed, there’s a fat receptor called CD36 that appears to be essential for cancer cells to spread, and these cancer cells respond to dietary fat intake, but not all fat.
Palmitic acid is a saturated fat made from palm oil that can be found in junk food, but it is most concentrated in meat and dairy. This may explain why, when looking at breast cancer mortality and dietary fat, “there was no difference in risk of breast-cancer-specific death…for women in the highest versus the lowest category of total fat intake,” but there’s about a 50 percent greater likelihood of dying of breast cancer with higher intake of saturated fat. Researchers conclude: “These meta-analyses have shown that saturated fat intake negatively impacts breast cancer survival.”
This may also explain why “intake of high-fat dairy, but not low-fat dairy, was related to a higher risk of mortality after breast cancer diagnosis.” If a protein in dairy, like casein, was the problem, skim milk might be even worse, but that wasn’t the case. It’s the saturated butterfat, perhaps because it triggered that cancer-spreading mechanism induced by CD36. Women who consumed one or more daily servings of high-fat dairy had about a 50 percent higher risk of dying from breast cancer.
We see the same with dairy and its relationship to prostate cancer survival. Researchers found that “drinking high-fat milk increased the risk of dying from prostate cancer by as much as 600% in patients with localized prostate cancer. Low-fat milk was not associated with such an increase in risk.” So, it seems to be the animal fat, rather than the animal protein, and these findings are consistent with analyses from the Health Professionals Follow-up Study (HPFS) and the Physicians’ Health Study (PHS), conducted by Harvard researchers.
There is even more evidence that the fat receptor CD36 is involved. The “risk of colorectal cancer for meat consumption” increased from a doubling to an octupling—that is, the odds of getting cancer multiplied eightfold for those who carry a specific type of CD36 gene. So, “Is It Time to Give Breast Cancer Patients a Prescription for a Low-Fat Diet?” A cancer diagnosis is often referred to as a ‘teachable moment’ when patients are motivated to make changes to their lifestyle, and so provision of evidence-based guidelines is essential.”
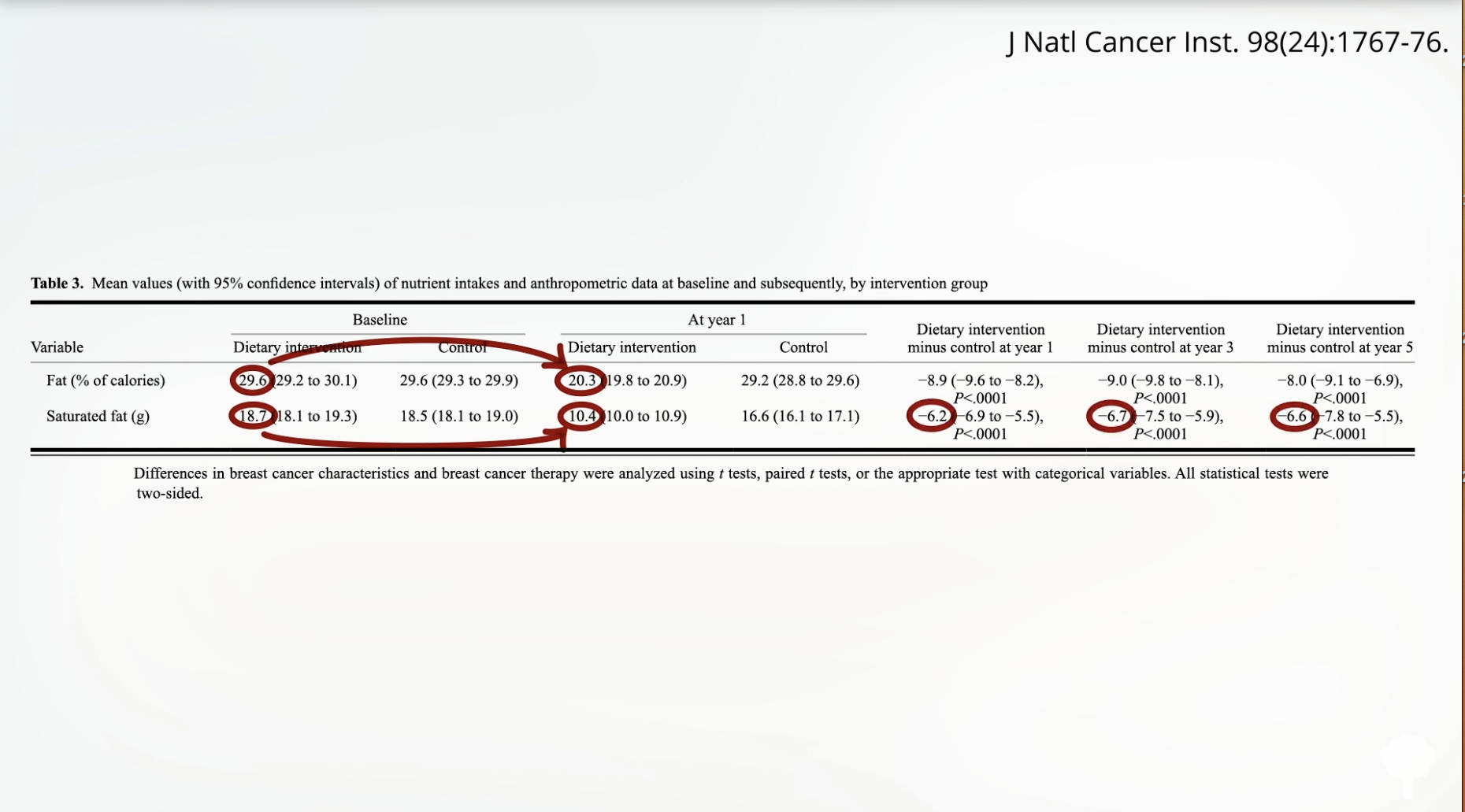
In a randomized, prospective, multicenter clinical trial, researchers set out “to test the effect of a dietary intervention designed to reduce fat intake in women with resected, early-stage breast cancer,” meaning the women had had their breast cancer surgically removed. As shown below and at 4:02 in my video, the study participants in the dietary intervention group dropped their fat intake from about 30 percent of calories down to 20 percent, reduced their saturated fat intake by about 40 percent, and maintained it for five years. “After approximately 5 years of follow-up, women in the dietary intervention group had a 24% lower risk of relapse”—a 24-percent lower risk of the cancer coming back—“than those in the control group.”
That was the WINS study, the Women’s Intervention Nutrition Study. Then there was the Women’s Health Initiative study, where, again, women were randomized to lower their fat intake down to 20 percent of calories, and, again, “those randomized to a low-fat dietary pattern had increased breast cancer overall survival. Meaning: A dietary change may be able to influence breast cancer outcome.” What’s more, not only was their breast cancer survival significantly greater, but the women also experienced a reduction in heart disease and a reduction in diabetes.
Is the apparent protection of plant-based diets for thyroid health due to the exclusion of animal foods, the benefits of plant foods, or both?
Several autoimmune diseases affect the thyroid gland, and Graves’ disease and Hashimoto’s thyroiditis are the most common. Graves’ disease results in hyperthyroidism, an overactive thyroid gland. Though slaughter plants are supposed to remove animals’ thyroid glands as they “shall not be used for human food,” should some neck meat slip in, you can suffer a similar syndrome called Hamburger thyrotoxicosis. That isn’t from your body making too much thyroid hormone, though. Rather, it’s from your body eating too much thyroid hormone. Graves’ disease is much more common, and meat-free diets may be able to help with both diseases, as plant-based diets may be associated with a low prevalence of autoimmune disease in general, as observed, for example, in rural sub-Saharan Africa. Maybe it’s because plants are packed with “high amounts of antioxidants, possible protective factors against autoimmune disease,” or because they’re packed with anti-inflammatory compounds. After all, “consuming whole, plant-based foods is synonymous with an anti-inflammatory diet.” But you don’t know until you put it to the test.
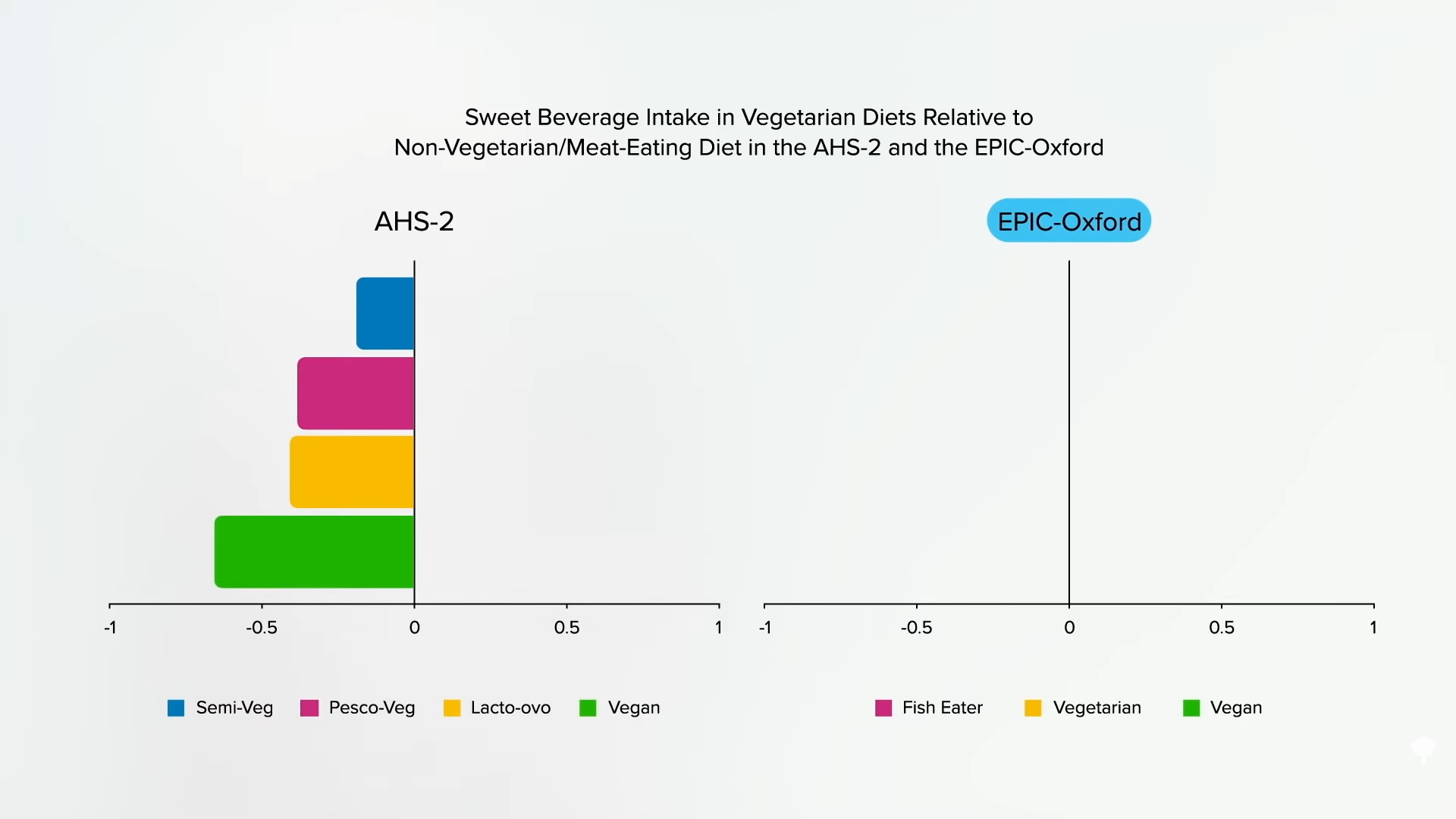
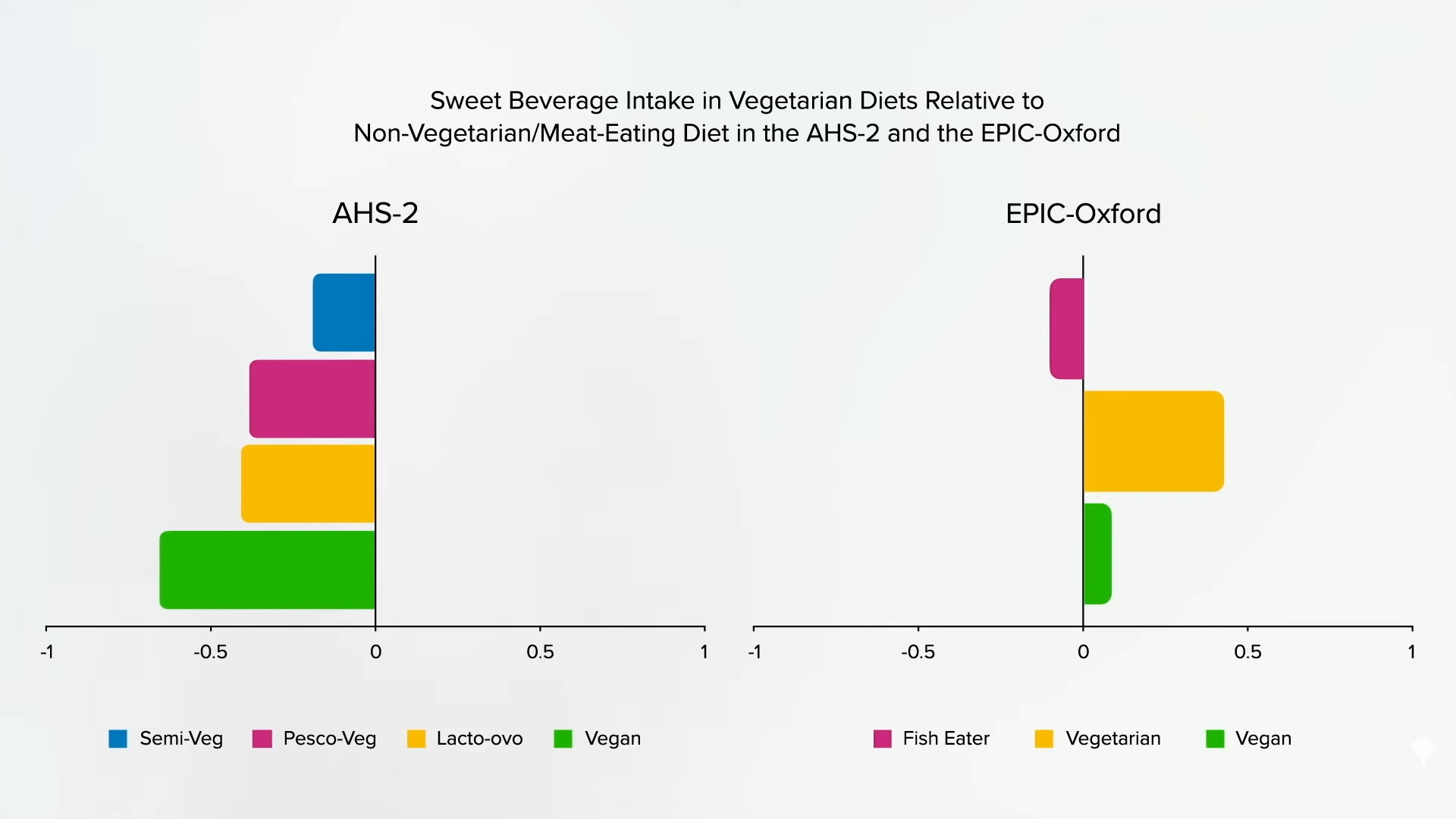
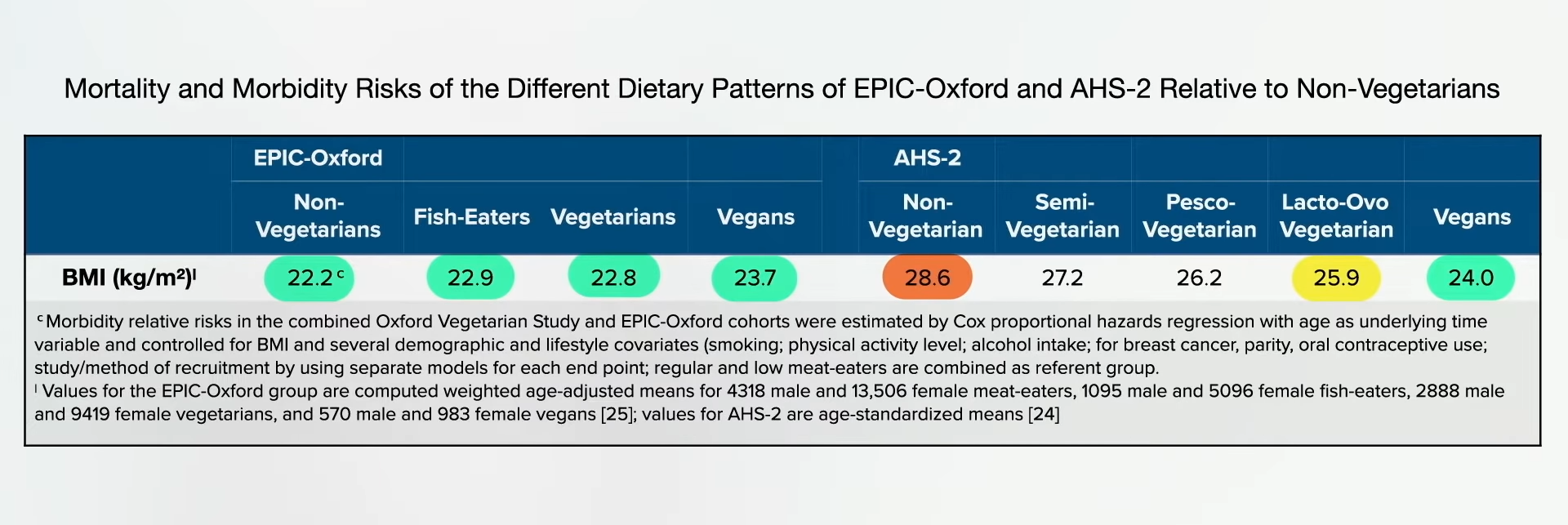
It turns out that the “exclusion of all animal foods was associated with half the prevalence of hyperthyroidism compared with omnivorous diets. Lacto-ovo [dairy-and-egg] and pesco [fish] vegetarian diets were associated with intermediate protection.” But, for those eating strictly plant-based, there is a 52 percent lower odds of hyperthyroidism.
As I discuss in my video The Best Diet for Hypothyroidism and Hyperthyroidism, this apparent protection “may be due to the exclusion of animal foods, the [beneficial] effects of plant foods, or both. Animal foods like meat, eggs, and dairy products may contain high oestrogen concentrations, which have been linked to autoimmunity in cell and animal studies.” Or it could be because the decrease in animal protein by excluding animal foods may downregulate IGF-1, which is not just a cancer-promoting growth hormone, but may play a role in autoimmune diseases. The protection could also come from the goodness in plants that may “protect cells against autoimmune processes,” like the polyphenol phytochemicals, such as flavonoids found in plant foods. Maybe it’s because environmental toxins build up in the food chain. For example, fish contaminated with industrial pollutants, like PCBs, are associated with an increased frequency of thyroid disorders.
But what about the other autoimmune thyroid disease, Hashimoto’s thyroiditis, which, assuming you’re getting enough iodine, is the primary cause of hypothyroidism, an underactive thyroid gland? Graves’ disease wasn’t the only autoimmune disorder that was rare or virtually unknown among those living in rural sub-Saharan Africa, eating near-vegan diets. They also appeared to have less Hashimoto’s.
There is evidence that those with Hashimoto’s have compromised antioxidant status, but we don’t know if it’s cause or effect. But if you look at the dietary factors associated with blood levels of autoimmune anti-thyroid antibodies, animal fats seem to be associated with higher levels, whereas vegetables and other plant foods are associated with lower levels. So, again, anti-inflammatory diets may be useful. It’s no surprise, as Hashimoto’s is an inflammatory disease—that’s what thyroiditis means: inflammation of the thyroid gland.
Another possibility is the reduction in intake of methionine, an amino acid concentrated in animal protein, thought to be one reason why “regular consumption of whole-food vegan diets is likely to have a favourable influence on longevity through decreasing the risk of cancer, coronary [heart] disease, and diabetes.” Methionine restriction improves thyroid function in mice, but it has yet to be put to the test for Hashimoto’s in humans.
If you compare the poop of patients with Hashimoto’s to controls, the condition appears to be related to a clear reduction in the concentration of Prevotella species. Prevotella are good fiber-eating bugs known to enhance anti-inflammatory activities. Decreased Prevotella levels are also something you see in other autoimmune conditions, such as multiple sclerosis and type 1 diabetes. How do you get more Prevotella? Eat more plants. If a vegetarian goes on a diet of meat, eggs, and dairy, within as few as four days, their levels can drop. So, one would expect those eating plant-based diets to have less Hashimoto’s, but in a previous video, I expressed concern about insufficient iodine intake, which could also lead to hypothyroidism. So, which is it? Let’s find out.
“In conclusion, a vegan diet tended to be associated with lower, not higher, risk of hypothyroid disease.” Why “tended”? The associated protection against hypothyroidism incidence and prevalence studies did not reach statistical significance. It wasn’t just because they were slimmer either. The lower risk existed even after controlling for body weight. So, researchers think it might be because animal products may induce inflammation. The question I have is: If someone who already has Hashimoto’s, what happens if they change their diet? That’s exactly what I’ll explore next.
Why is the incidence of side effects from statins so low in clinical trials while appearing to be so high in the real world?
“There is now overwhelming evidence to support reducing LDL-C (low-density lipoprotein cholesterol)”—so-called bad cholesterol—to reduce atherosclerotic cardiovascular disease (CVD),” the number one killer of men and women. So, why is adherence to cholesterol-lowering statin drug therapy such “a major challenge worldwide”? Researchers found “that the majority of studies reported that at least 40%, and as much as 80%, of patients did not comply fully with statin treatment recommendations.” Three-quarters of patients may flat out stop taking them, and almost 90 percent may discontinue treatment altogether.
When asked why they stopped taking the pills, most “former statin users or discontinuers…cited muscle pain, a side effect, as the primary reason…” “SAMSs”—statin-associated muscle symptoms—“are by far the most prevalent and important adverse event, with up to 72% of all statin adverse events being muscle-related.” Taking coenzyme Q10 supplements as a treatment for statin-associated muscle symptoms was a good idea in theory, but they don’t appear to help. Normally, side-effect symptoms go away when you stop the drug but can sometimes linger for a year or more. There is “growing evidence that statin intolerance is predominantly psychosocial, not pharmacological.” Really? It may be mostly just in people’s heads?
“Statins have developed a bad reputation with the public, a phenomenon driven largely by proliferation on the Internet of bizarre and unscientific but seemingly persuasive criticism of these drugs.” “Does Googling lead to statin intolerance?” But people have stopped taking statins for decades before there even was an Internet. What kinds of data have doctors suggested that patients are falsely “misattribut[ing] normal aches and pains to be statin side effects”?
Well, if you take people who claim to have statin-related muscle pain and randomize them back and forth between statins and an identical-looking placebo in three-week blocks, they can’t tell whether they’re getting the real drug or the sugar pill. The problem with that study, though, is that it may take months not only to develop statin-induced muscle pain, but months before it goes away, so no wonder three weeks on and three weeks off may not be long enough for the participants to discern which is which.
However, these data are more convincing: Ten thousand people were randomized to a statin or a sugar pill for a few years, but so many more people were dying in the sugar pill group that the study had to be stopped prematurely. So then everyone was offered the statin, and the researchers noted that there was “no excess of reports of muscle-related AEs” (adverse effects) among patients assigned to the statin over those assigned to the placebo. But when the placebo phase was over and the people knew they were on a statin, they went on to report more muscle side effects than those who knew they weren’t taking the statin. “These analyses illustrate the so-called nocebo effect,” which is akin to the opposite of the placebo effect.
Placebo effects are positive consequences falsely attributed to a treatment, whereas nocebo effects are negative consequences falsely attributed to a treatment, as was evidently seen here. There was an excess rate of muscle-related adverse effects reported only when patients and their doctors were aware that statin therapy was being used, and not when its use was concealed. The researchers hope “these results will help assure both physicians and patients that most AEs associated with statins are not causally related to use of the drug and should help counter…exaggerated claims about statin-related side effects.”
These are the kinds of results from “placebo-controlled randomised trials [that] have shown definitively that almost all of the symptomatic adverse events that are attributed to statin therapy in routine practice are not actually caused by it (ie, they represent misattribution.)” Now, “only a few patients will believe that their SAMS are of psychogenic origin” and just in their head, but their denial may have “deadly consequences.” Indeed, “discontinuing statin treatment may be a life-threatening mistake.”
Below and at 4:46 in my video How Common Are Muscle Side Effects from Statins?, you can see the mortality of those who stopped their statins after having a possible adverse reaction compared to those who stuck with them. This translates into about “1 excess death for every 83 patients who discontinued treatment” within a four-year period. So, when there are media reports about statin side effects and people stop taking them, this could “result in thousands of fatal and disabling heart attacks and strokes, which would otherwise have been avoided. Seldom in the history of modern therapeutics have the substantial proven benefits of a treatment been compromised to such an extent by serious misrepresentations of the evidence for its safety.” But is it a misrepresentation to suggest “that statin therapy causes side-effects in up to one fifth of patients”? That is what is seen in clinical practice; between 10 to 25 percent of patients placed on statins complain of muscle problems. However, because we don’t see anywhere near those kinds of numbers in controlled trials, patients are accused of being confused. Why is the incidence of side effects from statins so low in clinical trials while appearing to be so high in the real world?
Take this meta-analysis of clinical trials, for example: It found muscle problems not in 1 in 5 patients, but only 1 in 2,000. Should everyone over a certain age be on statins? Not surprisingly, every one of those trials was funded by statin manufacturers themselves. So, for example, “how could the statin RCTs [randomized controlled trials] miss detecting mild statin-related muscle adverse side effects such as myalgia [muscle pain]? By not asking. A review of 44 statin RCTs reveals that only 1 directly asked about muscle-related adverse effects.” So, are the vast majority of side effects just being missed in all these trials, or are the vast majority of side effects seen in clinical practice just a figment of patients’ imagination? The bottom line is we don’t know, but there is certainly an urgent need to figure it out.
Is it possible to reverse type 1 diabetes if caught early enough?
TheInternational Journal of Disease Reversal and Prevention has already had its share of miraculous disease reversals with a plant-based diet. For instance, one patient began following a whole food, plant-based diet after having two heart attacks in two months. Within months, he experienced no more chest pain, controlled his cholesterol, blood pressure, and blood sugars, and also lost 50 pounds as a nice bonus. Yet, the numbers “do not capture the patient’s transformation from feeling like a ‘dead man walking’ to being in command of his health with a new future and life.”
I’ve previously discussed cases of reversing the autoimmune inflammatory disease psoriasis and also talked about lupus nephritis (kidney inflammation). What about type 1 diabetes, an autoimmune disease we didn’t think we could do anything about? In contrast to type 2 diabetes, which is a lifestyle disease that can be prevented and reversed with a healthy enough diet and lifestyle, type 1 diabetes is an autoimmune disease in which our body attacks our pancreas, killing off our insulin-producing cells and condemning us to a life of insulin injections—unless, perhaps, it’s caught early enough. If a healthy enough diet is started early enough, might we be able to reverse the course of type 1 diabetes by blunting that autoimmune inflammation?
As I discuss in my video Type 1 Diabetes Treatment: A Plant-Based Diet, we know that patients with type 1 diabetes “may be able to reduce insulin requirements and achieve better glycemic [blood sugar] control” with healthier diets. For example, children and teens were randomized to a nutritional intervention in which they increased the whole plant food density of their diet—meaning they ate more whole grains, whole fruits, vegetables, legumes (beans, split peas, chickpeas, and lentils), nuts, and seeds. Researchers found that the more whole plant foods, the better the blood sugar control.
The fact that more whole fruits were associated “with better glycemic [blood sugar] control has important clinical implications for nutrition education” in those with type 1 diabetes. We should be “educating them on the benefits of fruit intake, and allaying erroneous concerns that fruit may adversely affect blood sugar.”
The case series in the IJDRP, however, went beyond proposing better control of just their high blood sugars, the symptom of diabetes, but better control of the disease itself, suggesting the anti-inflammatory effects of whole healthy plant foods “may slow or prevent further destruction of the beta cells”—the insulin-producing cells of the pancreas—“if dietary intervention is initiated early enough.” Where did this concept come from?
A young patient. Immediately following diagnosis of type 1 diabetes at age three, a patient began a vegetable-rich diet and, three years later, “has not yet required insulin therapy…and has experienced a steady decline in autoantibody levels,” which are markers of insulin cell destruction. Another child, who also started eating a healthier diet, but not until several months after diagnosis, maintains a low dose of insulin with good control. And, even if their insulin-producing cells have been utterly destroyed, individuals with type 1 diabetes can still enjoy “dramatically reduced insulin requirements,” reduced inflammation, and reduced cardiovascular risk, which is their number one cause of death over the age of 30. People with type 1 diabetes have 11 to 14 times the risk of death from cardiovascular disease compared to the general population, and it’s already the top killer among the public, so it’s closer to 11 to 14 times more important for those with type 1 diabetes to be on the only diet and lifestyle program ever proven to reverse heart disease in the majority of patients—one centered around whole plant foods. The fact it may also help control the disease itself is just sugar-free icing on the cake.
All this exciting new research was presented in the first issue of The International Journal of Disease Reversal and Prevention. As a bonus, there’s a companion publication called the Disease Reversal and Prevention Digest. These are for the lay public and are developed with the belief I wholeheartedly share that “everyone has a right to understand the science that could impact their health.” You can go behind the scenes and hear directly from the author of the lupus series, read interviews from luminaries like Dean Ornish, see practical tips from dietitians on making the transition towards a healthier diet, and enjoy recipes.
The second issue includes more practical tips, such as how to eat plant-based on a budget, and gives updates on what Dr. Klaper is doing to educate medical students, what Audrey Sanchez from Balanced is doing to help change school lunches, and how Dr. Ostfeld got healthy foods served in a hospital. (What a concept!) And what magazine would be complete without an article to improve your sex life?
The journal is free, downloadable at IJDRP.org, and its companion digest, available at diseasereversaldigest.com, carries a subscription fee. I am a proud subscriber.
Want to learn more about preventing type 1 diabetes in the first place? See the related posts below.
JUST eight years after euthanasia was legalised in Canada, some doctors there say the result is “horrendous” as more and more people are driven to it by a failing health-care system.
Assisted deaths have risen at an alarming rate, while the criteria to be given a lethal injection has been relaxed.
3
Alicia Duncan, left, with her late mother Donna, who was helped to take her own lifeCredit: Supplied
3
Pro-assisted dying supporters at WestminsterCredit: EPA
Now experts warn it would be disastrous to allow a system like Canada’s Medical Assistance In Death (Maid) in the UK, after the families of some of those who opted for it revealed they did so because they could not access medical help.
Professor Leonie Herx, a Canadian palliative medicine consultant based in Calgary, Alberta, described the outcome as “horrific from a medical perspective”.
In 2017, the first full year the legislation was in place, one per cent of deaths in Canada were from euthanasia.
By 2022, it was four per cent, as 13,241 people opted for Maid.
Supporters insist the bill is strictly to help the terminally ill.
Ms Leadbeater said: “I believe that, with the right safeguards in place, people who are already dying and are mentally competent should be given the choice of a shorter, less painful death on their own terms and without placing family and loved ones at risk of prosecution.
“It will not undermine calls for improvements to palliative care. Nor will it conflict with the rights of people with disabilities to be treated equally and have the respect and support they are right to campaign for in order to live fulfilling lives.”
But this is very similar to how Canada’s law was introduced — and now the rules there have softened and the numbers resorting to euthanasia have soared.
My parents held hands as they passed away by assisted dying – we supported ‘beautiful’ decision, it wasn’t a surprise
When Maid was introduced in Canada in 2016, it was limited to the terminally ill.
But following a legal challenge in 2021 it was made available to those whose death was NOT “reasonably foreseeable”.
A further change due to come into force in March 2027 will open up the service to people whose sole medical condition is MENTAL illness.
Doctors in Canada have approved assisted dying after just ZOOM calls, and some politicians want to extend the practice to CHILDREN old enough to make an “informed” choice.
Requests for Maid are now much more frequently approved in Canada than in 2019, when eight per cent of requests were denied.
In 2022, that figure fell to 3.5 per cent, a Health Canada report says.
I believe that, with the right safeguards in place, people who are already dying and are mentally competent should be given the choice of a shorter, less painful death on their own terms and without placing family and loved ones at risk of prosecution
Kim Leadbeater
The report adds that 17 per cent of those who applied cited “isolation or loneliness”, while nearly 36 per cent believed they were a “burden on family, friends or care-givers”.
The number of Canadians ending their lives via Maid — usually given in the form of an injection administered by a physician — has outpaced other nations with similar laws.
And its legislation has grown far looser than those of other countries offering assisted dying, such as Belgium and the Netherlands.
One expert claimed that what has happened in Canada could happen in the UK because both countries have a struggling health system and an ageing population.
Canadian-born Alexander Raikin, a researcher at the Ethics And Public Policy Centre in Washington DC, said: “Euthanasia in Canada was meant to be rare and last resort, but it isn’t. It has become routine.
“Assisted deaths have seen dram-atic rates of growth in all the places that have legalised it, like the Netherlands, Switzerland and Oregon in the US, but in Canada that rate has been quite unprecedented. The similarities between Canada and the UK . . . suggest the UK is likely to follow Canada’s route.
“I don’t think it is a coincidence that this massive surge happens at the same time our health system is collapsing. It should ring alarm bells in Britain.”
In an interview with the Sun on Sunday, Canadian Alicia Duncan told, from her home in Mission, British Columbia, how her “active and happy” mother was given a fast-track death in 2021. She opted for it because she could not get the healthcare she needed.
Alicia, 41, an interior designer, now warns the UK about the perils of following Canada’s lead.
Her mum Donna, a psychiatric nurse, suffered a brain injury in a minor car crash but despite not facing immediate death, and receiving treatment for mental health symptoms, the 61-year-old’s Maid request was granted.
Despite protests by her daughter and long-serving GP, she was helped to take her own life just 48 hours later.
Alica said: “People in Britain should be very worried about this.
3
Now, in the UK, a bill to legalise the early ending of life has been introduced in Parliament by Labour MP Kim Leadbeater
“It won’t stop at terminal illness alone. The UK needs to look at what happened in Canada.
“People think, ‘This will never happen to me’. I never thought my mother, who was active and happy, would have chosen to end her life because of a mental illness, and been helped to do so.
“I would say to Britain, you need to be cautious because once you decide to open this door you don’t get to choose who walks through.
“The moment you legalise euthanasia it starts as a crack then it becomes a wide-open chasm and there is nothing you can do to stop it.”
Since their mother’s death, Alicia and her sister Christie have been denied key details about the circumstances and believe safe-guards to protect vulnerable people were not followed properly.
She added: “I am so angry. People are choosing to die because they can’t access healthcare in a timely manner.
The moment you legalise euthanasia it starts as a crack then it becomes a wide-open chasm and there is nothing you can do to stop it
Alicia Duncan
“My mum was waiting to see a specialist for 18 months and her appointment was the week after she died.
“It’s easier to die in Canada than to access healthcare.”
Ms Carr — who has rare genetic condition arthrogryposis multiplex congenita, which affects her joints and muscles, and uses a wheelchair, warned: “These laws will put lives like mine, marginalised lives, at risk and those risks will be fatal.
“All because of the dangerous assumption some of us are better off dead. Let’s be aware, maybe it’s going to be like Canada, and that is terrifying.”
This week in Canada, a 51-year old gran from Nova Scotia told how doctors offered her Maid while she was in hospital about to undergo a mastectomy for breast cancer.
These laws will put lives like mine, marginalised lives, at risk and those risks will be fatal
Liz Carr
Before she went in for what she hoped was life-saving surgery, the doctor sat her down and asked: “Did you know about Medical Assistance In Dying?”
She was then asked again before undergoing a second mastectomy nine months later, and a third time while in the recovery room after that procedure.
Around three quarters of Brits support assisted dying, a survey this year from advocacy group Dying With Dignity found, while just 14 per cent of us oppose it.
“If I decide my own life is not worth living, please may I ask for help to die.”
But the Archbishop of Canterbury, Justin Welby, said of the bill: “This approach is both dangerous and sets us in a direction even more dangerous.
All I’m asking is that we be given the dignity of choice. If I decide my own life is not worth living, please may I ask for help to die
Esther Rantzen
“In every place where it’s been done, it has led to a slippery slope.
“The right to end your life could too easily, all too accidentally, turn into a duty to do so.”
‘BRITS, BE WARNED OF PERIL’
By Prof Leonie Herx, Professor of Palliative Medicine at the University of Calgary
IN Canada, a doctor-administered lethal injection has become the solution to almost any suffering, which is horrific from a medical perspective.
Any adult with a disability or chronic illness can get an “assisted death”.
There is no requirement to receive any treatment for even a reversible condition and sometimes it is the only “intervention” provided.
I have seen a person’s worst day become their last.
We are seeing people getting Maid for poverty, social isolation or deprivation.
It is routinely offered to any potentially eligible person as they access a care home, at time of surgery or during hospital admission for a health crisis.
It has altered the practice of medicine here and is leading to the premature death of many vulnerable people.
It has become something it never started as, something no Canadian could have imagined.
The UK should take warning.
Keep medicine invested in helping people restore their health and live well.
HAMDEN, Conn. (AP) — Hip-hop artist Fatman Scoop, who collapsed onstage while performing in Connecticut last month, died of heart disease, the state medical examiner’s office has determined.
The official cause of death for the performer, born Isaac Freeman III, was hypertensive and atherosclerotic cardiovascular disease, a spokesperson for the Connecticut medical examiner’s office said Wednesday.
Fatman Scoop, 56, collapsed while performing in Hamden on Aug. 30 and was taken to a hospital.
His family said later on Instagram that “the world lost a radiant soul, a beacon on stage and in life.”
A New York City-born rapper and hype man, Fatman Scoop was known for his single “Be Faithful,” which topped charts in Europe in the early 2000s, and for his contributions to hits by Missy Elliott, Mariah Carey and others.
His family cherished him as “the laughter in our lives, a constant source of support, unwavering strength and courage,” his relatives said.
“His music made us dance and embrace life with positivity,” his family members said. “His joy was infectious and the generosity he extended to all will be deeply missed but never forgotten.”
__________
This story has been corrected to note that Fatman Scoop was 56, not 53.
Those on a healthy plant-based diet who have elevated homocysteine levels despite taking sufficient vitamin B12 may want to consider taking a gram a day of contaminant-free creatine.
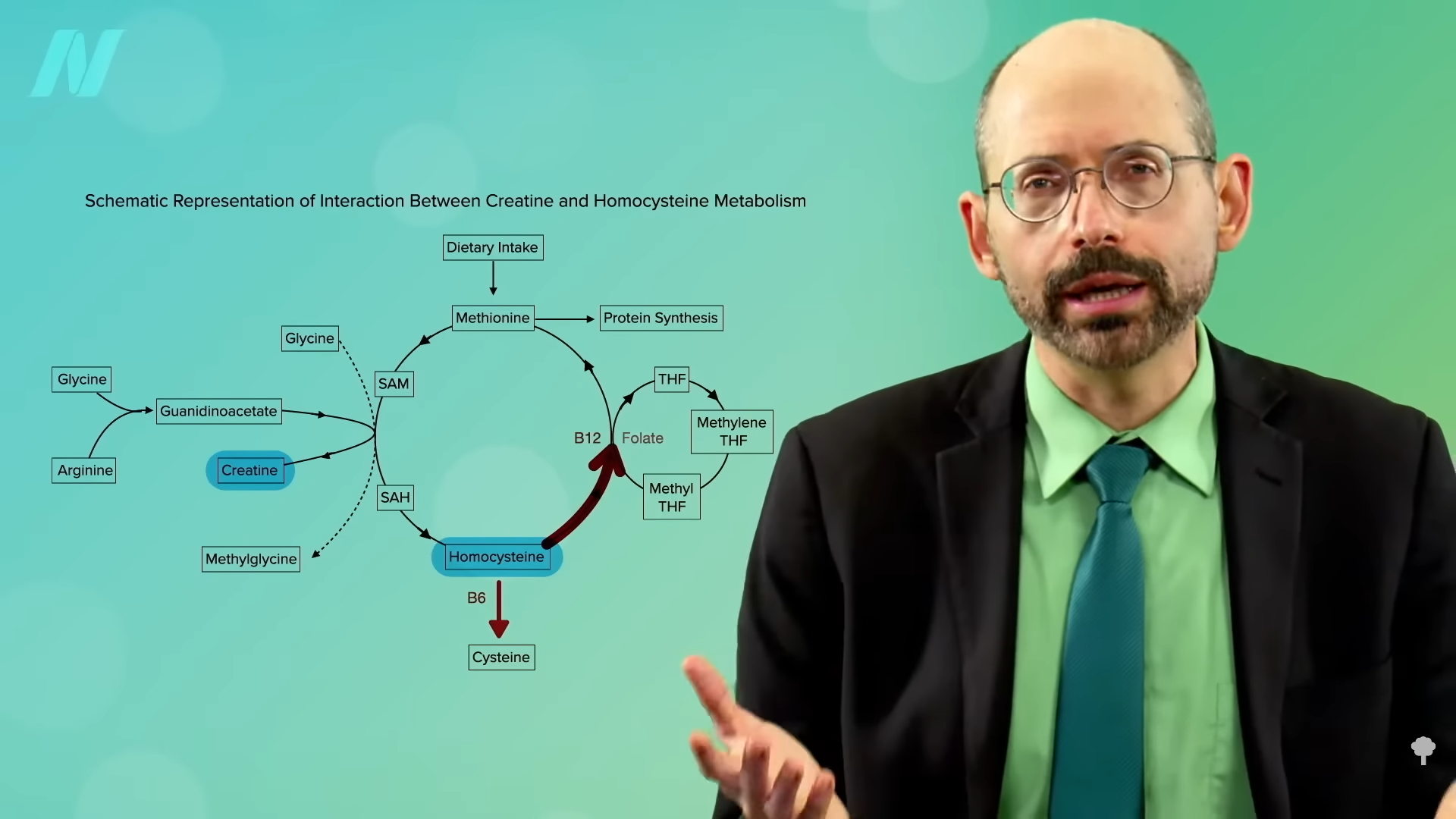
The average blood levels of homocysteine in men are about 1.5 points higher than in women, which may be one of the reasons men tend to be at higher risk for cardiovascular disease. Women don’t need to make as much creatine as men since they tend to have less muscle mass. That may help explain “the ‘gender gap’ in homocysteine levels.” If you remember from my previous video and as seen below and at 0:36 in The Efficacy and Safety of Creatine for High Homocysteine, in the process of making creatine, our body produces homocysteine as a by-product. So, for people with stubbornly high homocysteine levels that don’t respond sufficiently to B vitamins, “creatine supplementation may represent a practical strategy for decreasing plasma homocysteine levels”—that is, lowering the level of homocysteine into the normal range.
It seemed to work in rats. What about humans? Well, it worked in one study, but it didn’t seem to work in another. It didn’t work in yet another either. And, in another study, homocysteine levels were even driven up. So, this suggestion that taking creatine supplements would lower homocysteine was called into question.
However, all those studies were done with non-vegetarians, so they were already effectively supplementing with creatine every day in the form of muscle meat. In that way, researchers were testing higher versus lower supplementation. Those eating strictly plant-based make all their creatine from scratch, so they may be more sensitive to an added creatine source. There weren’t any studies on creatine supplementation in vegans to lower homocysteine until now.
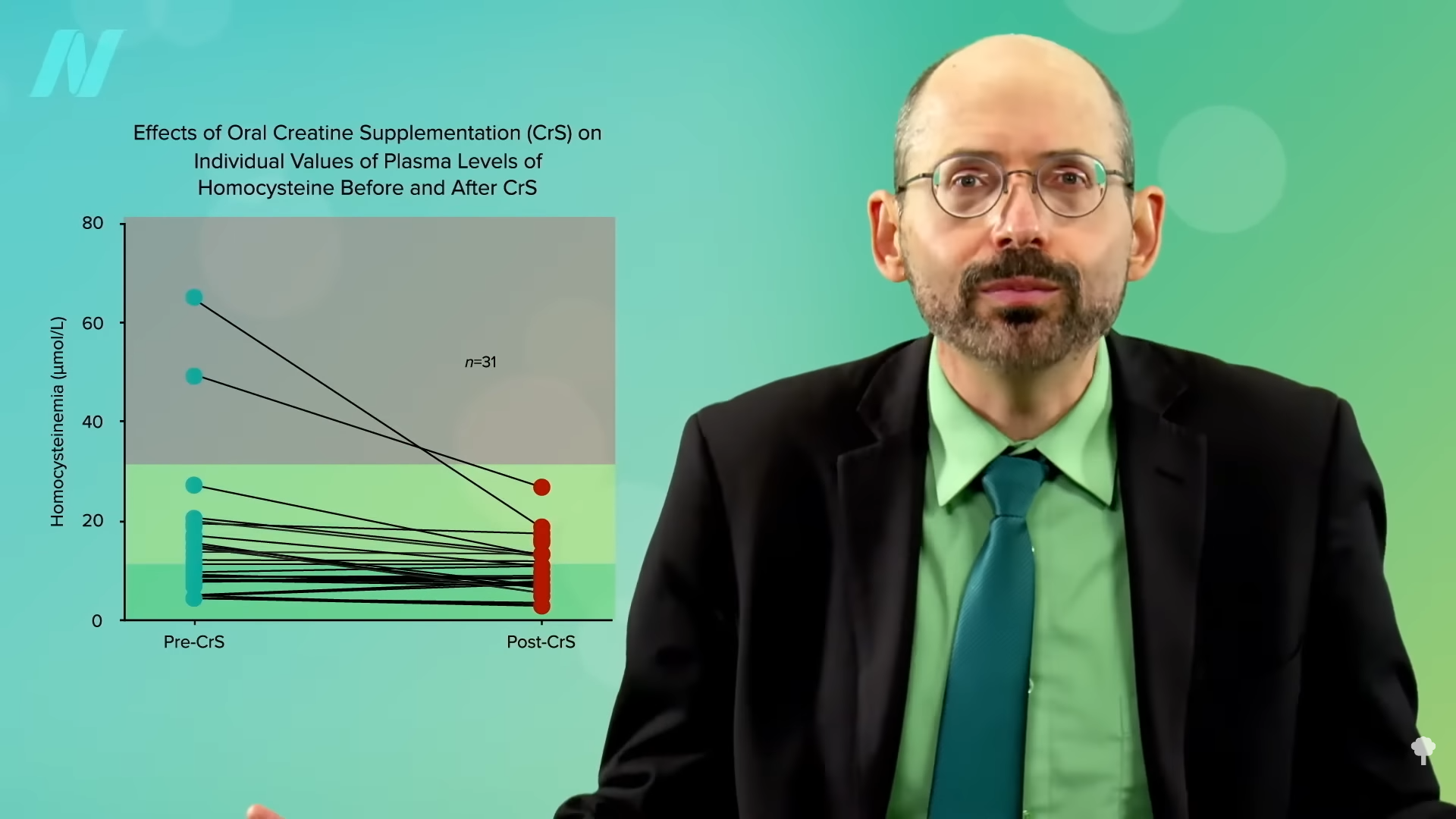
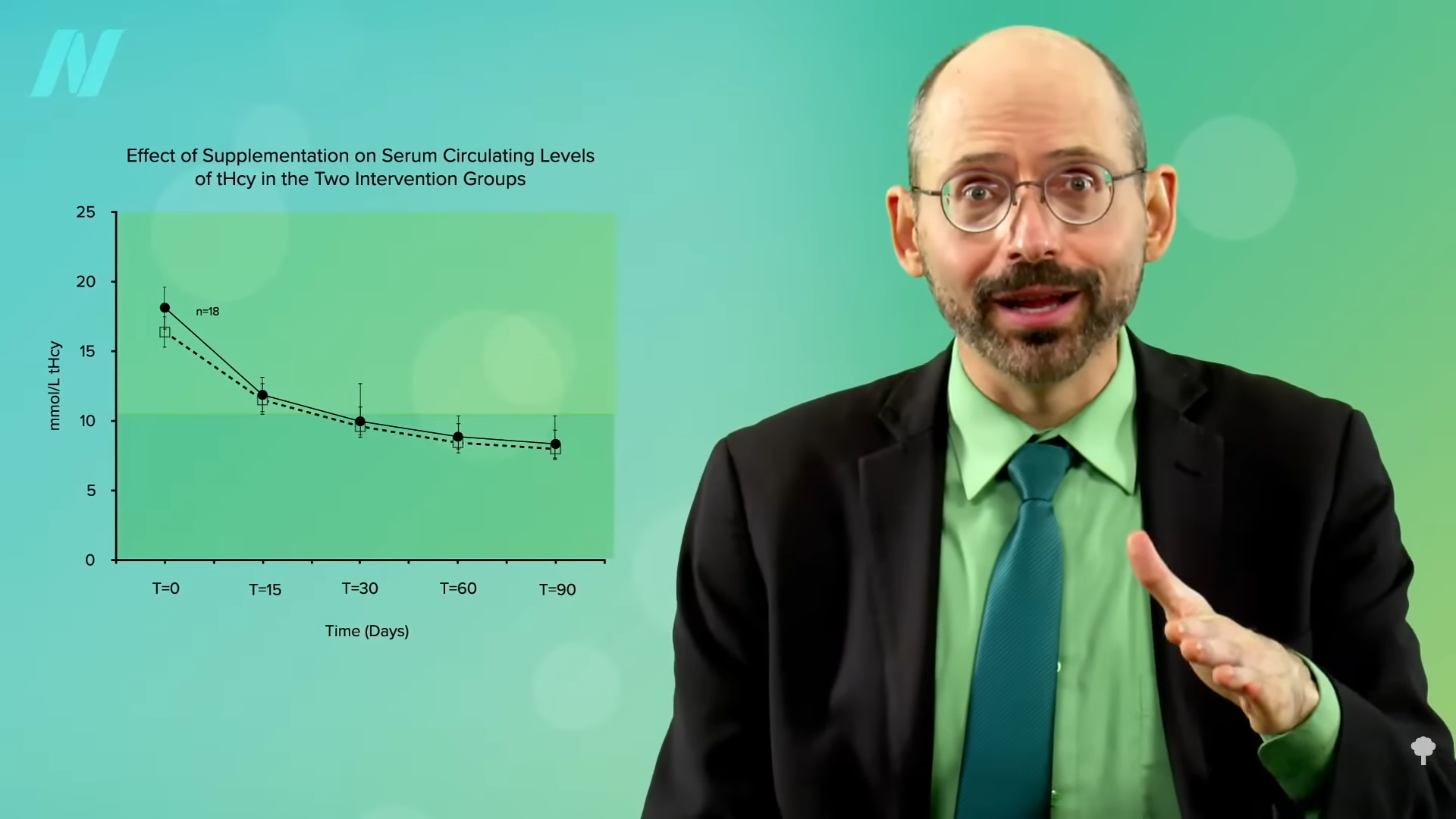
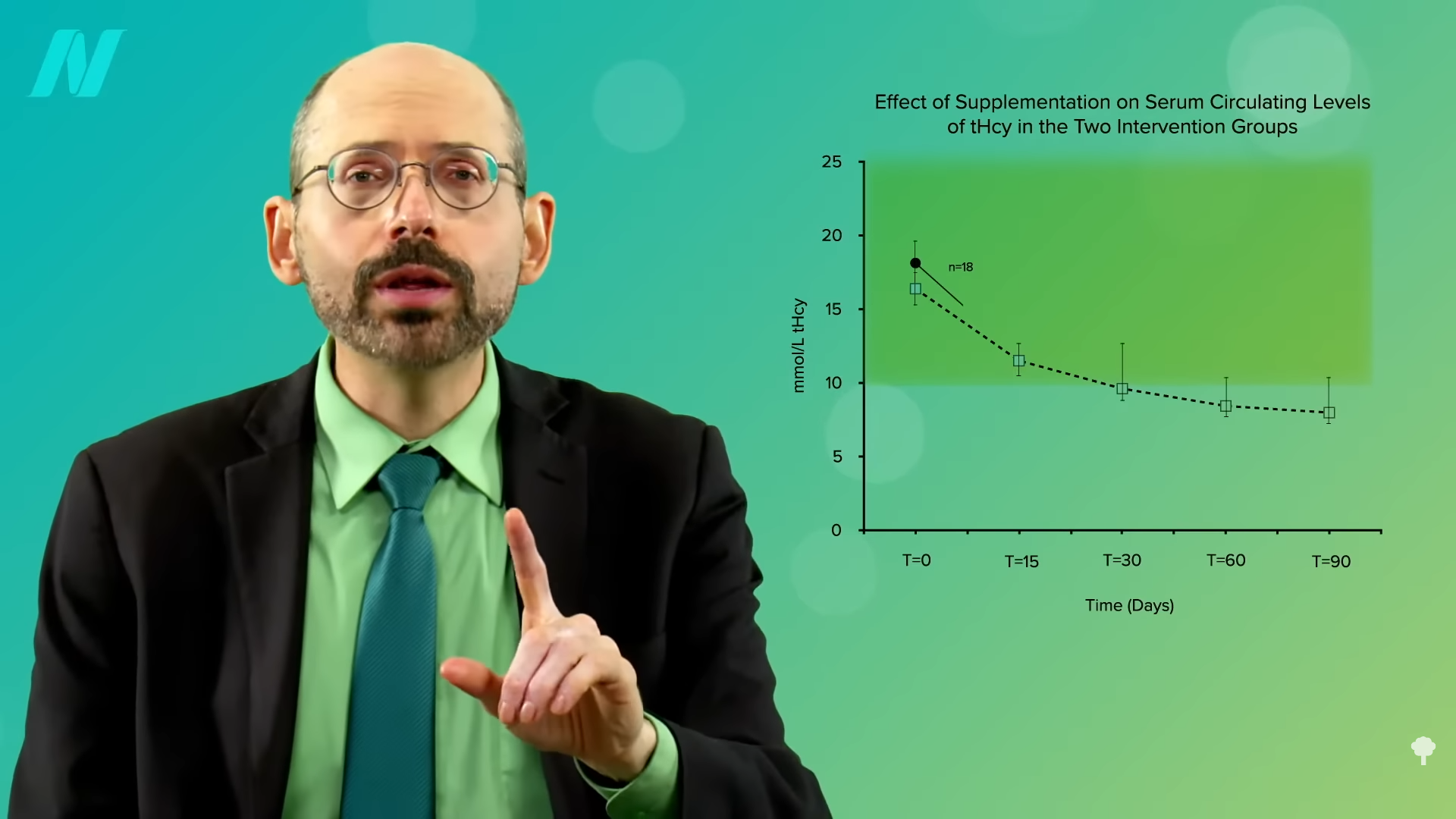
Researchers took vegans who were not supplementing their diets with vitamin B12, so some of their homocysteine levels were through the roof. A few were as high as 50 when the ideal is more like under 10, for example. After taking some creatine for a few weeks, all of their homocysteine levels normalized. You can see the before and after in the graph below and at 2:04 in my video.
Now, they didn’t normalize, as that would have been a level under 10, but that’s presumably because they weren’t taking any B12. Give vegetarians and vegans vitamin B12 supplements, either dosing daily or once a week, and their levels normalize in a matter of months, as you can see below and at 2:20 in my video. However, the fact that you could bring down homocysteine levels with creatine alone, even without any B12, suggests—to me at least—that if your homocysteine is elevated (above 10) on a plant-based diet despite taking B12 supplements and eating greens and beans to get enough folate, it might be worth experimenting with supplementing with a gram of creatine a day for a few weeks to see if your homocysteine comes down.
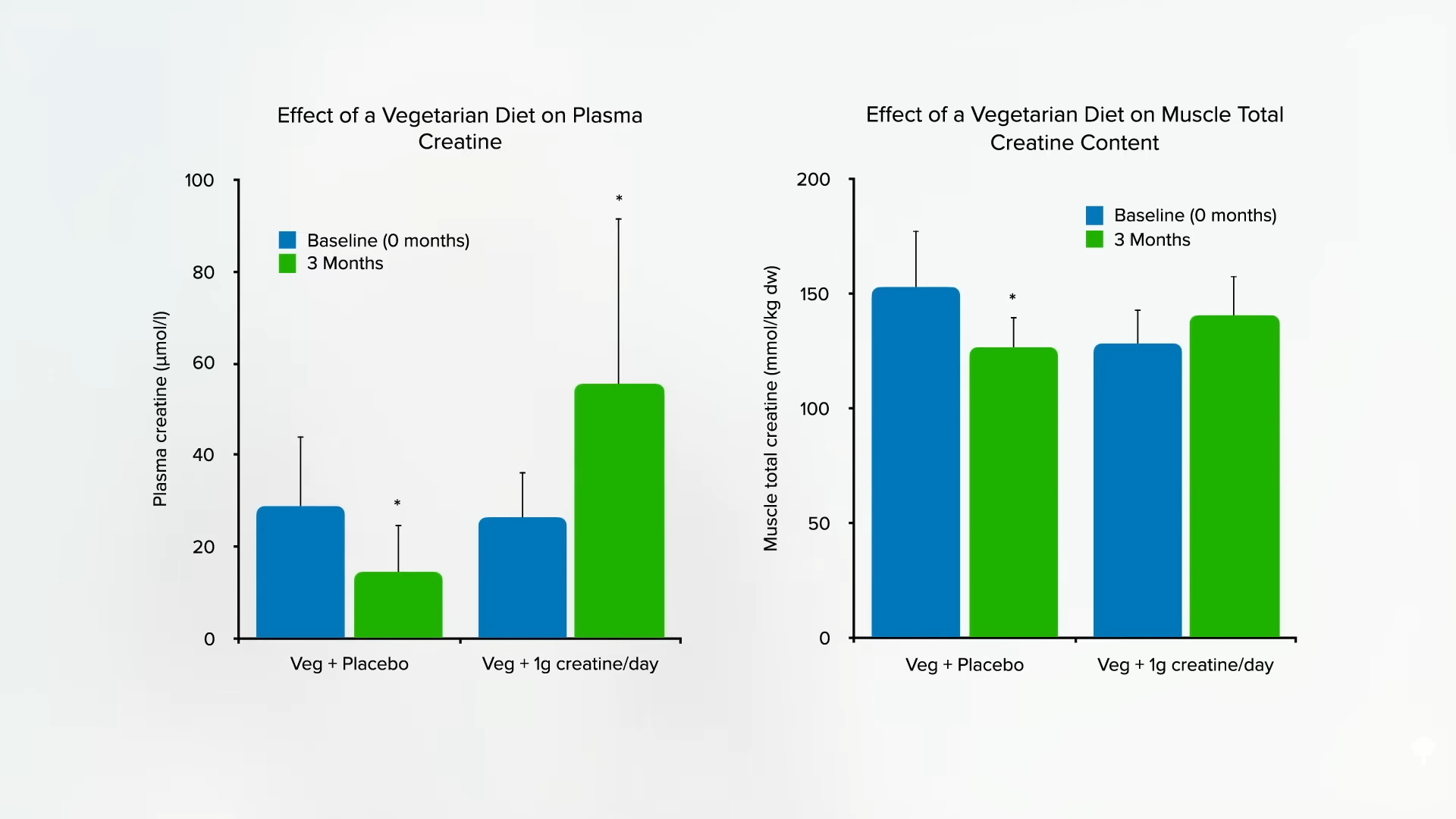
Why just a single gram? That’s approximately how much non-vegetarians do not have to make themselves; it’s the amount that erased vegetarian discrepancies in blood and muscle, as you can see in the graph below and at 3:01 in my video, and how much has been shown to be safe in the longer term.
How safe is it? We can take a bit of comfort in the fact that it’s “one of the world’s best-selling dietary supplements,” with literally billions of servings taken, and the only consistently reported side effect has been weight gain, presumed to be from water retention. The only serious side effects appear to be among those with pre-existing kidney diseases taking whopping doses closer to 20 grams a day. A concern was raised that creatine could potentially form a carcinogen known as N-nitrososarcosine when it hit the acid bath of the stomach, but, when it actually put to the test, researchers found this does not appear to be a problem.
Bottom line: Doses of supplemental creatine up to 3 grams a day are “unlikely to pose any risk,” provided “high purity creatine” is used. However, as we all know, dietary supplements in the United States “are not regulated by the US Food and Drug Administration and may contain contaminants or variable quantities of the desired supplement” and may not even contain what’s on the label. We’re talking about “contaminants…that may be generated during the industrial production.” When researchers looked at 33 samples of creatine supplements made in the United States and Europe, they found that they all actually contained creatine, which is nice, but about half exceeded the maximum level recommended by food safety authorities for at least one contaminant. The researchers recommend that “consumers give their preference to products obtained by producers that ensure the highest quality control and certify the maximum amount of contaminants present in their products.” Easier said than done.
Because of the potential risks, I don’t think people should take creatine supplements willy-nilly, but the potential benefits may exceed the potential risks if, again, you’re on a healthy plant-based diet and taking B12, and your homocysteine levels are still not under 10. In that case, I would suggest giving a gram a day of creatine a trying to see if it brings it down.
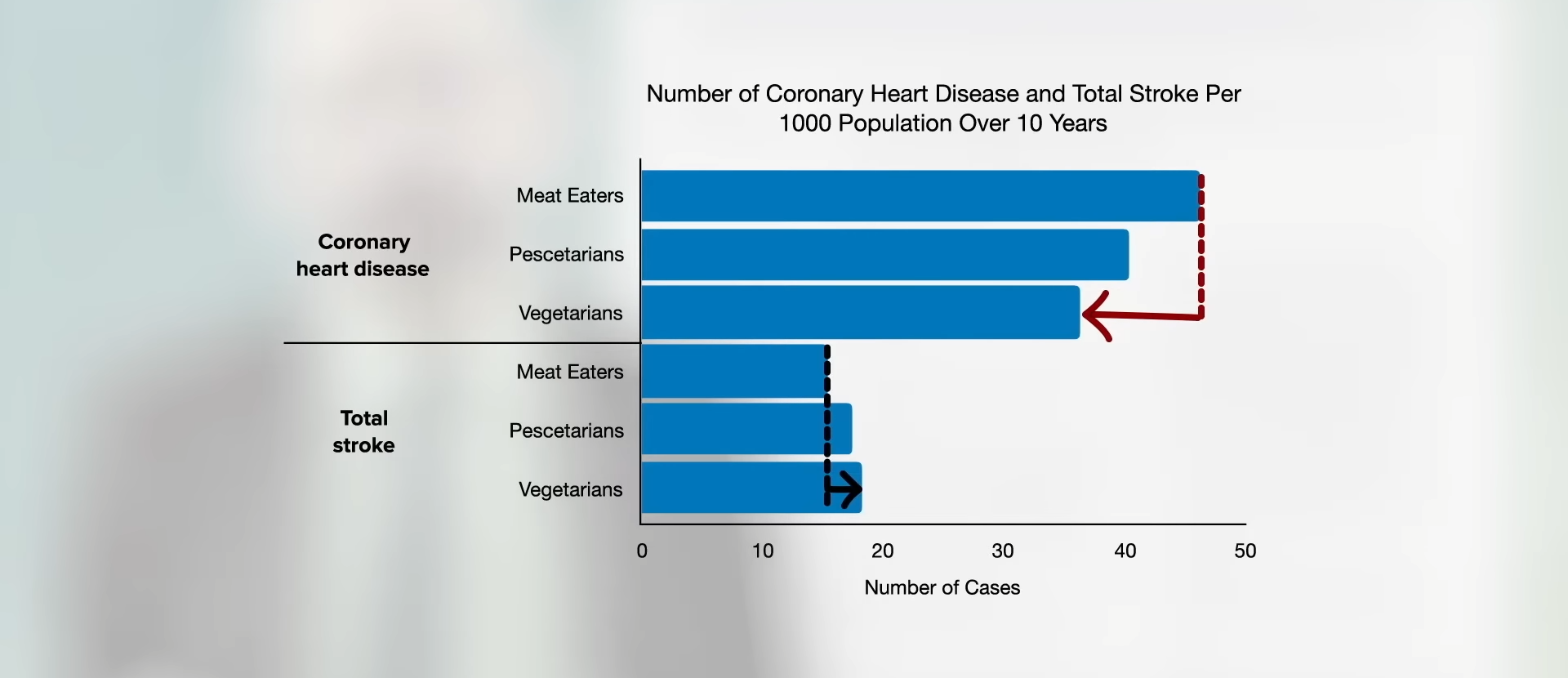
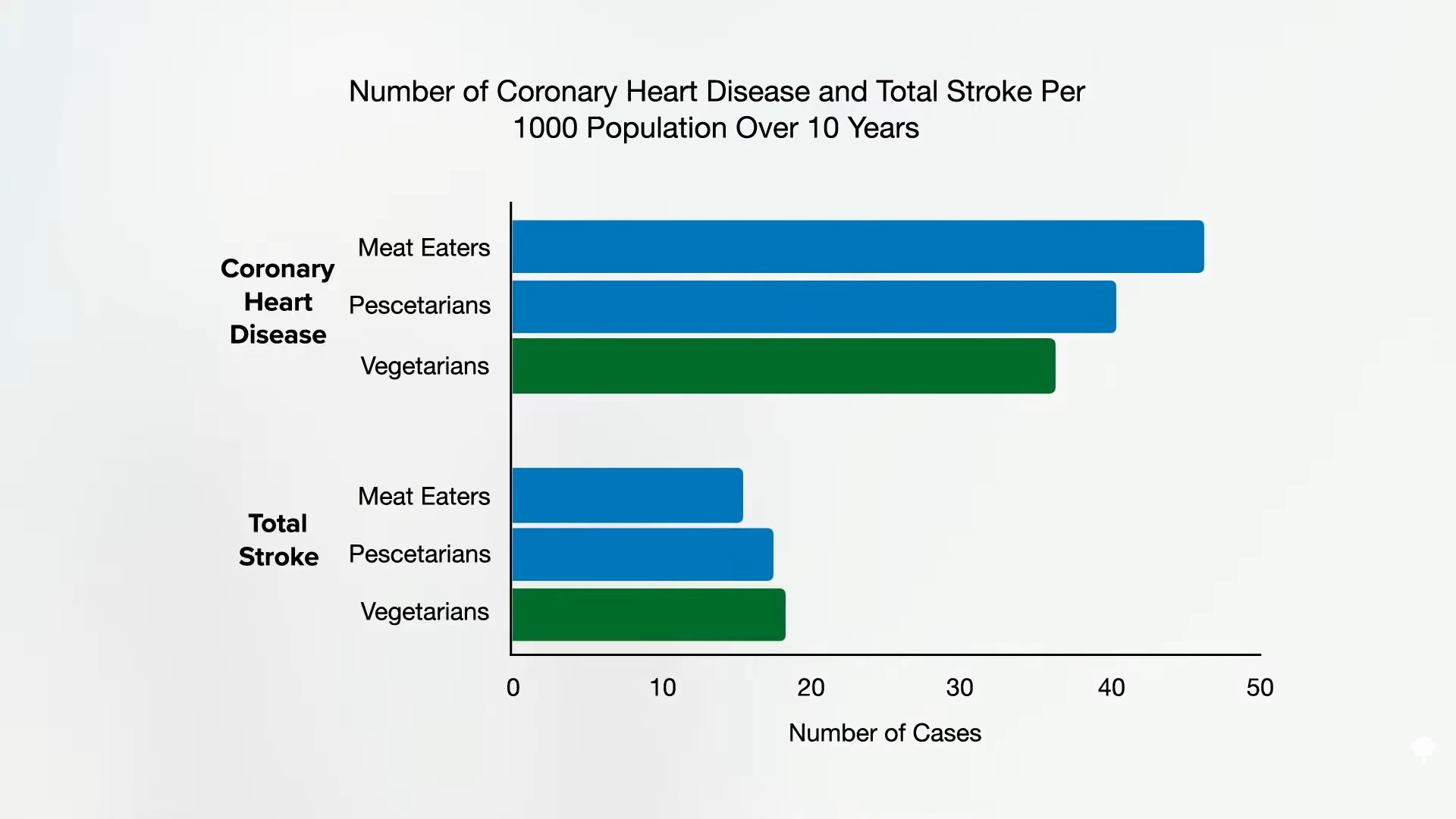
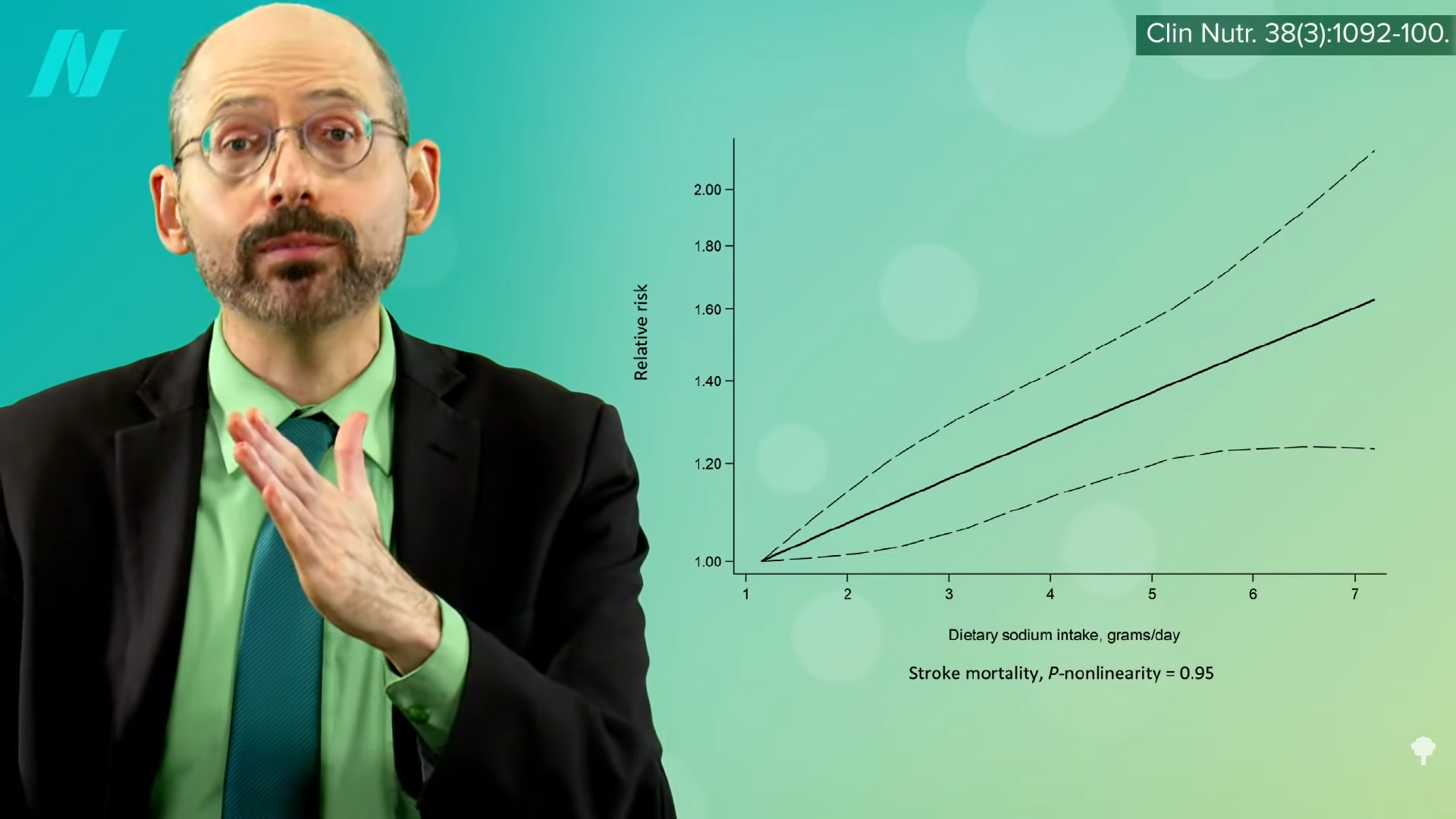
The reason I did this whole video series goes back to “Risks of Ischaemic Heart Disease and Stroke in Meat Eaters, Fish Eaters, and Vegetarians Over 18 Years of Follow-Up: Results from the Prospective EPIC-Oxford Study,” which found that, although the overall cardiovascular risk is lower in vegetarians and vegans combined, they appeared to be at slightly higher stroke risk, as you can see in the graph below and at 5:06 in my video.
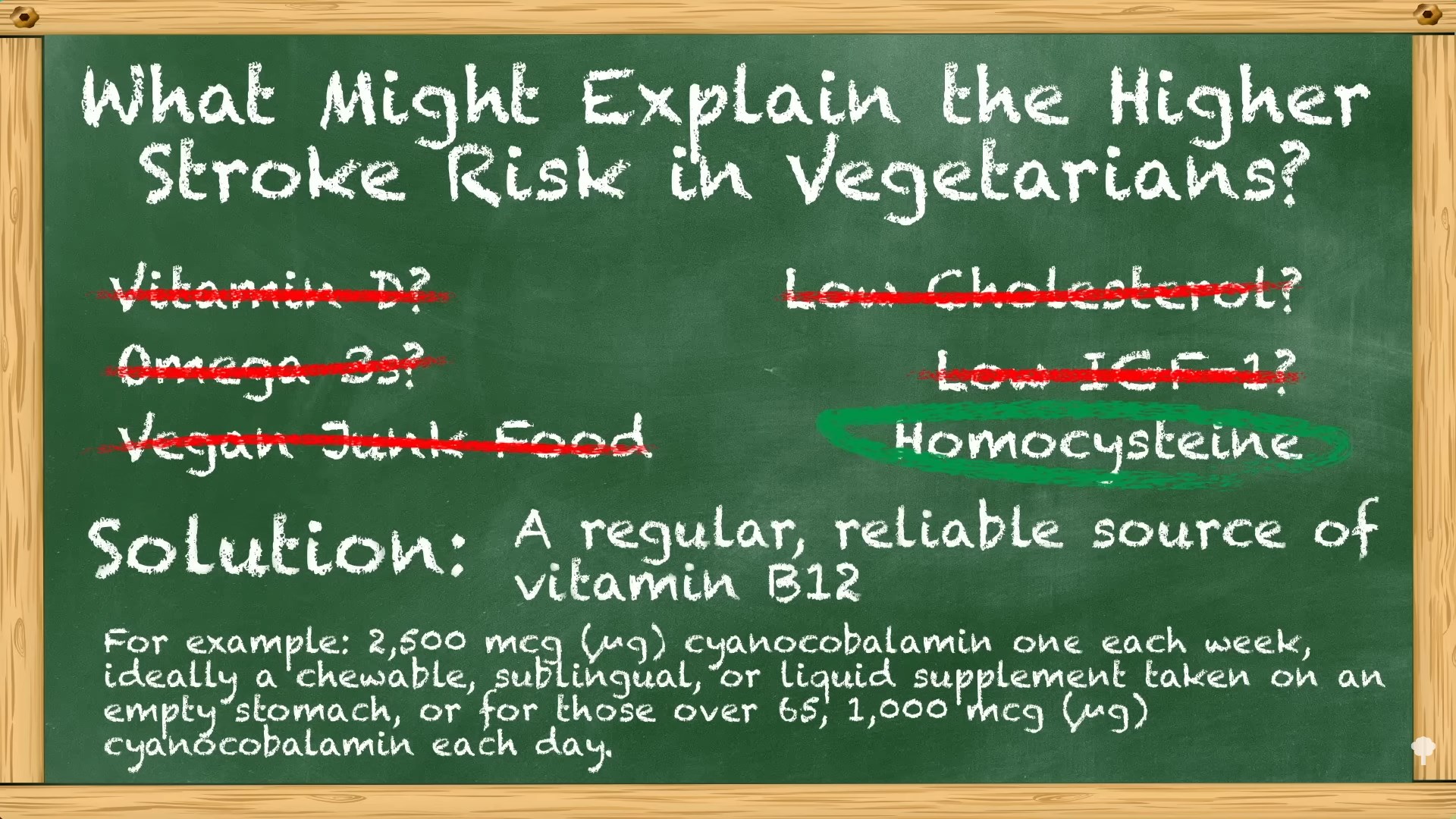
I went through a list of potential causes, as you can see at 5:11 and below, and arrived at elevated homocysteine. What’s the solution? A regular, reliable source of vitamin B12. The cheapest, easiest method that I personally use is one 2,500 mcg chewable tablet of cyanocobalamin, the most stable source of B12, once a week. (In fact, you can just use 2,000 mcg once a week.) And, again, a backup plan for those doing that but still having elevated homocysteine is an empirical trial of a single gram a day of creatine supplementation, which was shown to improve at least capillary blood flow in those who started out with high homocysteine levels.
In sum, plant-based diets appear to “markedly reduce risk” for multiple leading killer diseases—heart disease, type 2 diabetes, and many common types of cancer—but “an increased risk for stroke may represent an ‘Achilles heel.’ Nonetheless, vegans have the potential to achieve a truly exceptional ‘healthspan’ if they face this problem forthrightly by restricting salt intake and taking other practical measures that promote cerebrovascular [brain artery] health…Nonetheless, these considerations do not justify nutritional nihilism. On balance, low-fat vegan diets offer such versatile protection for long-term health that they remain highly recommendable. Most likely, the optimal strategy is to adopt such a [plant-based] diet, along with additional measures—appropriate food choices, exercising training, judicious supplementation [of vitamin B12]—that will mitigate the associated stroke risk.” And try not to huff whipped cream charging canister gas. Leave the “whippets” alone.
This concludes my series on stroke risk. If you missed any of the other videos, see the related posts below.
I’m assuming that nearly everyone taking their B12 will have normal homocysteine levels, so these last two videos are just for the rare person who doesn’t. However, those on a healthy plant-based diet with elevated homocysteine levels despite taking sufficient vitamin B12 should consider taking a gram a day of contaminant-free creatine, which should be about a quarter teaspoon.
Where do you get contaminant-free creatine? Since regulations are so lax, you can’t rely on supplement manufacturers no matter what they say, so I would recommend going directly to the chemical suppliers that sell it to laboratories and guarantee a certain purity. Here are some examples (in alphabetical order) of some of the largest companies where you can get unadulterated creatine: Alfa Aesar, Fisher Scientific, Sigma-Aldrich, and TCI America.
What are the consequences of having to make your creatine rather than relying on dietary sources?
“Almost universally, research findings show a poor vitamin B12 status among vegetarians” because they aren’t taking vitamin B12 supplements like they should, which results in an elevation in homocysteine levels. This may explain why vegetarians were recently found to have higher rates of stroke, as you can see in the graph below and at 0:30 in my video Should Vegetarians Take Creatine to Normalize Homocysteine?.
Of course, plant-based eating is just one of many ways to become deficient in vitamin B12. Even nitrous oxide (laughing gas) can do it in as little as two days, thanks to the recreational use of whipped cream canister gas. (I just learned about “whippits”!)
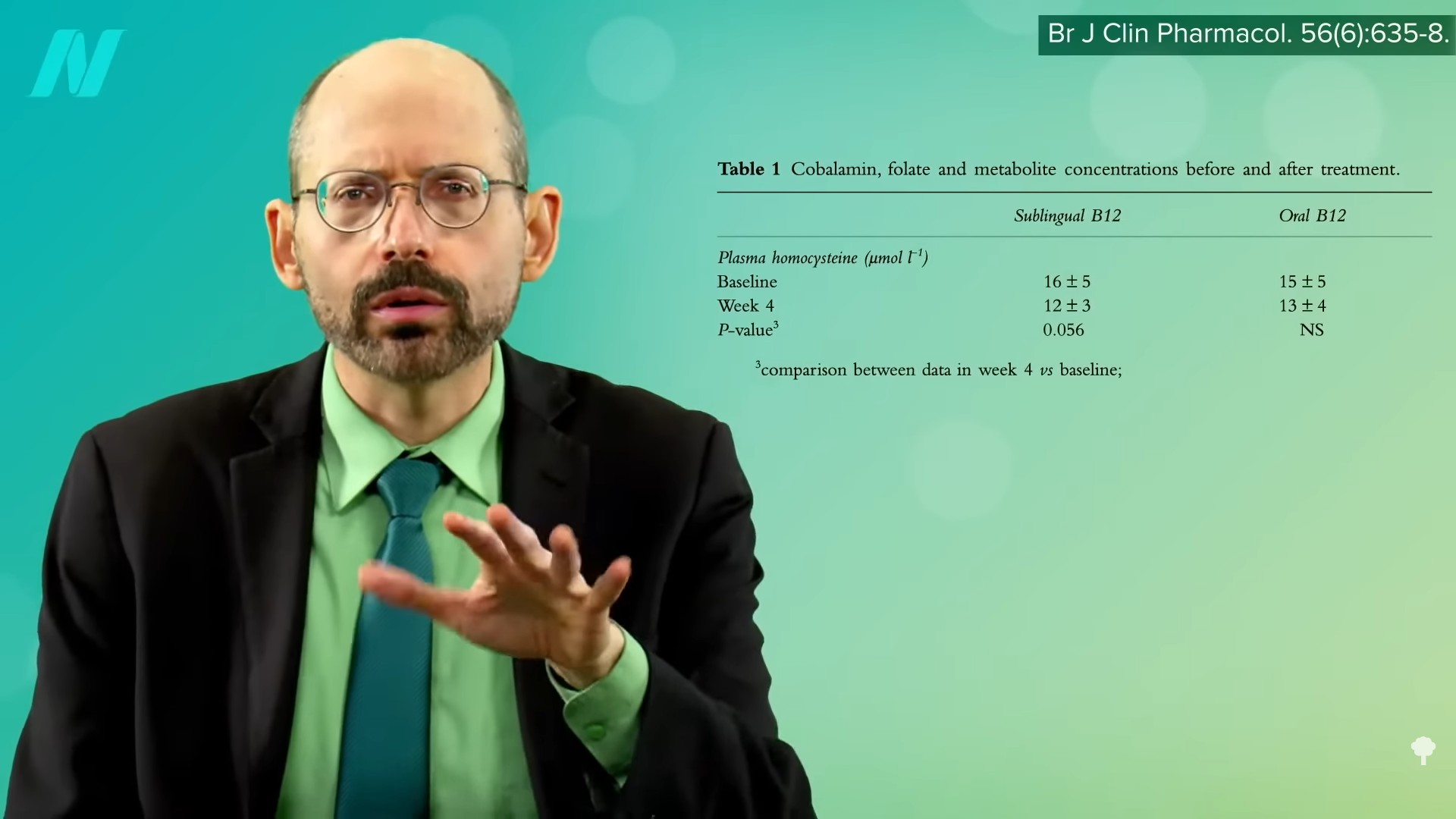
When researchers gave vegetarians and vegans as little as 50 daily micrograms of cyanocobalamin, which is the recommended and most stable form of vitamin B12 supplement, their homocysteine levels, which had started up in the elevated zone, normalized right down into the safe zone under 10 mmol/L within only one to two months. Just 2,000 micrograms of cyanocobalamin once a week gave the same beautiful result, as you can see in the graph below and at 1:15 in my video.
Not always, though. In another study, even 500 daily micrograms, taken as either a sublingual chewable or swallowable regular B12 supplement, didn’t normalize homocysteine within a month, as shown below and at 1:24. Now, presumably, if the participants had kept it up, their levels would have continued to fall as they did in the 50-daily-microgram study.
If you’re plant-based and have been taking your B12, but your homocysteine level is still too high (above 10 mmol/L), is there anything else you can do? Well, inadequate folate intake can also increase homocysteine, but folate comes from the same root as foliage. It’s found in beans and leaves, concentrated in greens. If you’re eating beans and greens, taking your B12, and your homocysteine level is still too high, I’d suggest taking 1 gram of creatine a day as an experiment, then getting your homocysteine levels retested in a month to see if it helped.
Creatine is a compound formed naturally in the human body that is primarily involved with energy production in our muscles and brain. It’s also formed naturally in the bodies of many other animals. So, when we eat their muscles, we can also take in some of the creatine in their bodies through our diet. We only need about 2 grams of creatine a day, so those who eat meat may get about 1 gram from their diet and their body makes the rest from scratch. There are rare birth defects where you’re born without the ability to make it, in which case, you have to get it from your diet. Otherwise, our bodies can make as much as we need to maintain normal concentrations in our muscles.
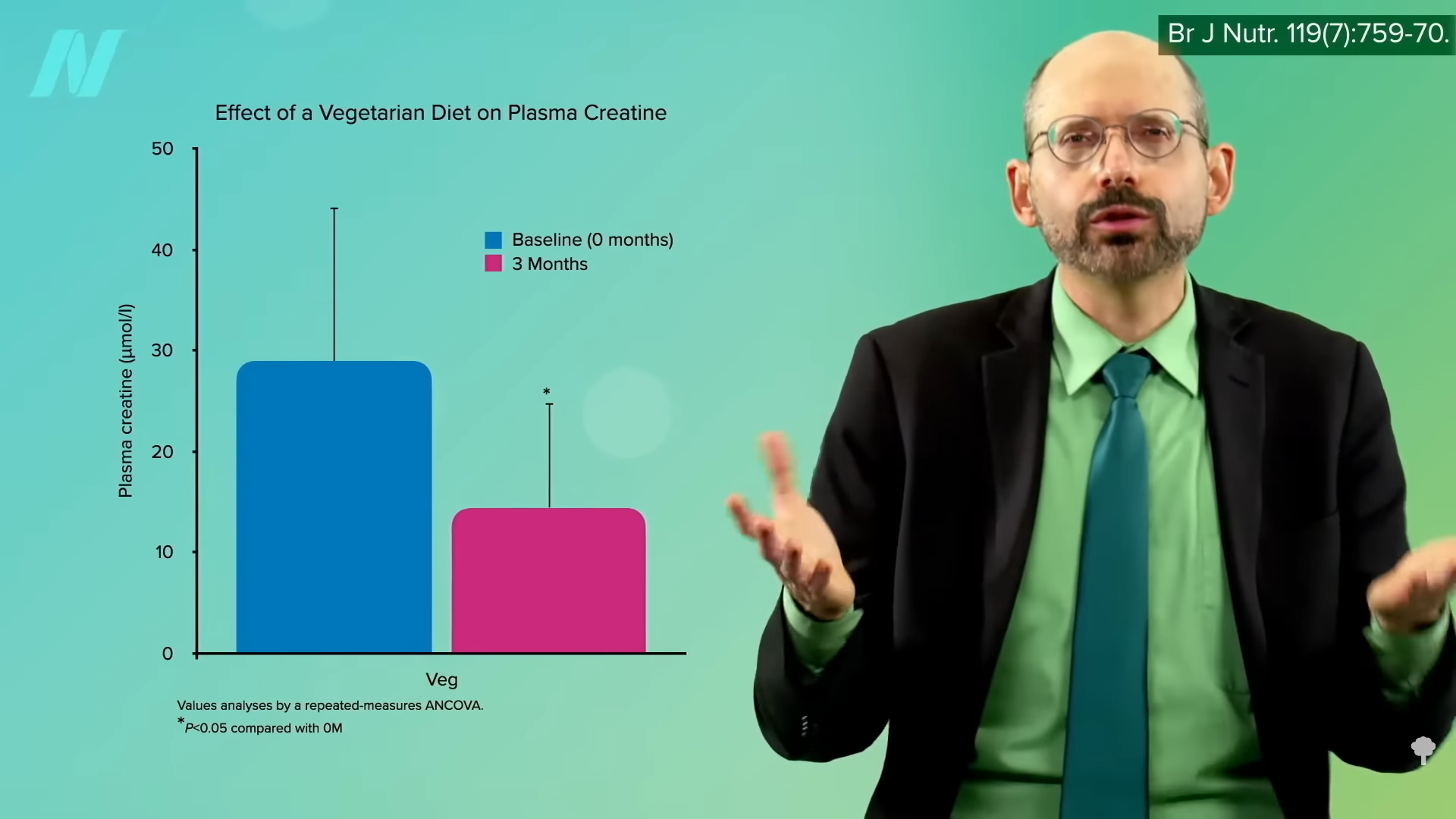
As you can see in the graph below and at 2:54 in my video, when you cut out meat, the amount of creatine floating around in your bloodstream goes down.
However, the amount in your brain remains the same, as shown in the graph below and at 2:57. This shows that dietary creatinine doesn’t influence the levels of brain creatine, because our brain makes all the creatine we need. The level in vegetarian muscles is lower, but that doesn’t seem to affect exercise performance, as both vegetarians and meat eaters respond to creatine supplementation with similar increases in muscle power output. If vegetarian muscle creatine were insufficient, then presumably an even bigger boost would be seen. So, all that seems to happen when we eat meat is that our body doesn’t have to make as much. What does all of this have to do with homocysteine?
As you can see below and at 3:36 in my video, in the process of making creatine, our body produces homocysteine as a waste product. Now, normally this isn’t a problem because our body has two ways to detoxify it: by using vitamin B6 or a combination of vitamin B12 and folate. Vitamin B6 is found in both plant and animal foods, and it’s rare to be deficient. But, vitamin B12 is mainly found in animal foods, so its level can be too low in those eating plant-based who don’t also supplement or eat B12-fortified foods. And, as I mentioned, folate is concentrated in plant foods, so it can be low in those who don’t regularly eat greens, beans, or folic-acid-fortified grains. Without that escape valve, homocysteine levels can get too high. However, if you’re eating a healthy plant-based diet and taking your B12 supplement, your homocysteine levels should be fine.
What if they aren’t? We might predict that if we started taking creatine supplements, our level of homocysteine might go down since we won’t have to make so much of it from scratch, producing homocysteine as a by-product, but you don’t know until you put it to the test. I’ll cover that next.
This whole creatine angle was new to me. I had long worried about homocysteine levels being too high among those getting inadequate B12 intake, but I didn’t realize there was another potential mechanism for bringing it down other than with vitamin B. Let’s see if it pans out in my final video of the series: The Efficacy and Safety of Creatine for High Homocysteine.
Many doctors mistakenly rely on serum B12 levels in the blood to test for vitamin B12 deficiency.
There were two cases of young, strictly vegetarian individuals with no known vascular risk factors. One suffered a stroke, and the other had multiple strokes. Why? Most probably because they weren’t taking vitamin B12 supplements, which leads to high homocysteine levels, which can attack our arteries.
So, those eating plant-based who fail to supplement with B12 may increase their risk of both heart disease and stroke. However, as you can see in the graph below and at 0:47 in my videoHow to Test for Functional Vitamin B12 Deficiency, vegetarians have so many heart disease risk factor benefits that they are still at lower risk overall, but this may help explain why vegetarians were found to have more stroke. This disparity would presumably disappear with adequate B12 supplementation, and the benefit of lower heart disease risk would grow even larger.
Compared with non-vegetarians, vegetarians enjoy myriad other advantages, such as better cholesterol, blood pressure, blood sugars, and obesity rates. But, what about that stroke study? Even among studies that have shown benefits, “the effect was not as pronounced as expected, which may be a result of poor vitamin B12 status due to a vegetarian diet. Vitamin B12 deficiency may negate the cardiovascular disease prevention benefits of vegetarian diets. To further reduce the risk of cardiovascular disease, vegetarians should be advised to use vitamin B12 supplements.”
How can you determine your B12 status? By the time you’re symptomatic with B12 deficiency, it’s too late. And, initially, the symptoms can be so subtle that you might even miss them. What’s more, you develop metabolic vitamin B12 deficiency well before you develop a clinical deficiency, so there’s “a missed opportunity to prevent dementia and stroke” when you have enough B12 to avoid deficiency symptoms, but not enough to keep your homocysteine in check. “Underdiagnosis of this condition results largely from a failure to understand that a normal serum [blood level] B12 may not reflect an adequate functional B12 status.” The levels of B12 in our blood do not always represent the levels of B12 in our cells. We can have severe functional deficiency of B12 even though our blood levels are normal or even high.
“Most physicians tend to assume that if the serum B12 is ‘normal,’ there is no problem,” but, within the lower range of normal, 30 percent of patients could have metabolic B12 deficiency, with high homocysteine levels.
Directly measuring levels of methylmalonic acid (MMA) or homocysteine is a “more accurate reflection of vitamin B12 functional statuses.” Methylmalonic acid can be checked with a simple urine test; you’re looking for less than a value of 4 micrograms per milligram of creatinine. “Elevated MMA is a specific marker of vitamin B12 deficiency while Hcy [homocysteine] rises in both vitamin B12 and folate deficiencies.” So, “metabolic B12 deficiency is strictly defined by elevation of MMA levels or by elevation of Hcy in folate-replete individuals,” that is, in those getting enough folate. Even without eating beans and greens, which are packed with folate, folic acid is added to the flour supply by law, so, these days, high homocysteine levels may be mostly a B12 problem. Ideally, you’re looking for a homocysteine level in your blood down in the single digits.
Measured this way, “the prevalence of subclinical functional vitamin B12 deficiency is dramatically higher than previously assumed…” We’re talking about 10 to 40 percent of the general population, more than 40 percent of vegetarians, and the majority of vegans who aren’t scrupulous about getting their B12. Some suggest that those on plant-based diets should check their vitamin B12 status every year, but you shouldn’t need to if you’re adequately supplementing.
There are rare cases of vitamin B12 deficiency that can’t be picked up on any test, so it’s better to just make sure you’re getting enough.
Not taking vitamin B12 supplements or regularly eating B12-fortified foods may explain the higher stroke risk found among vegetarians.
Leonardo da Vinci had a stroke. Might his vegetarian diet have been to blame? “His stroke…may have been related to an increase in homocysteine level because of the long duration of his vegetarian diet.” A suboptimal intake of vitamin B12 is common in those eating plant-based diets (unless they take B12 supplements or regularly eat B12-fortified foods) and can lead to an increased level of homocysteine in the blood, which “is accepted as an important risk factor for stroke.”
“Accepted” may be overstating it as there is still “a great controversy” surrounding the connection between homocysteine and stroke risk. But, as you can see in the graph below and at 0:57 in my video Vegetarians and Stroke Risk Factors: Vitamin B12 and Homocysteine?, those with higher homocysteine levels do seem to have more atherosclerosis in the carotid arteries that lead up to the brain, compared to those with single-digit homocysteine levels, and they also seem to be at higher risk for clotting ischemic strokes in observational studies and, more recently, bleeding hemorrhagic strokes, as well as increased risk of dying from cardiovascular disease and all causes put together.
Even more convincing are the genetic data. About 10 percent of the population has a gene that increases homocysteine levels by about 2 points, and they appear to have significantly higher odds of having a stroke. Most convincing would be randomized, double-blind, placebo-controlled trials to prove that lowering homocysteine with B vitamins can lower strokes, and, indeed, that appears to be the case for clotting strokes: Strokes with homocysteine-lowering interventions were more than five times as likely to reduce stroke compared with placebo.
Ironically, one of the arguments against the role of homocysteine in strokes is that, “assuming that vegetarians have lower vitamin B12 concentrations than meat-eaters and that low vitamin B12 concentrations cause ischaemic stroke, then the incidence of stroke should be increased among vegetarians…but this is not the case.” However, it has never been studied until now.
As you can see in the graph below and at 2:16 in my video, the EPIC-Oxford study researchers found that vegetarians do appear to be at higher risk.
And no wonder, as about a quarter of the vegetarians and nearly three-quarters of the vegans studied were vitamin B12-depleted or B12-deficient, as you can see below and at 2:23, and that resulted in extraordinarily high homocysteine levels.
Why was there so much B12 deficiency? Because only a small minority were taking a dedicated B12 supplement. And, unlike in the United States, B12 fortification of organic foods isn’t allowed in the United Kingdom. So, while U.S. soymilk and other products may be fortified with B12, UK products may not. We don’t see the same problem among U.S. vegans in the Adventist study, presumably because of the B12 fortification of commonly eaten foods in the United States. It may be no coincidence that the only study I was able to find that showed a significantly lower stroke mortality risk among vegetarians was an Adventist study.
Start eating strictly plant-based without B12-fortified foods or supplements, and B12 deficiency can develop. However, that was only for those not eating sufficient foods fortified with B12. Those eating plant-based who weren’t careful about getting a regular reliable source of B12 had lower B12 levels and, consequently, higher homocysteine levels, as you can see below and at 3:27 in my video.
The only way to prove vitamin B12 deficiency is a risk factor for cardiovascular disease in vegetarians is to put it to the test. When researchers measured the amount of atherosclerosis in the carotid arteries, the main arteries supplying the brain, “no significant difference” was found between vegetarians and nonvegetarians. They both looked just as bad even though vegetarians tend to have better risk factors, such as lower cholesterol and blood pressure. The researchers suggest that B12 deficiency plays a role, but how do they know? Some measures of artery function weren’t any better either. Again, they surmised that vitamin B12 deficiency was overwhelming the natural plant-based benefits. “The beneficial effects of vegetarian diets on lipids and blood glucose [cholesterol and blood sugars] need to be advocated, and efforts to correct vitamin B12 deficiency in vegetarian diets can never be overestimated.”
Sometimes vegetarians did even worse. Worse artery wall thickness and worse artery wall function, “raising concern, for the first time, about the vascular health of vegetarians”—more than a decade before the new stroke study. Yes, their B12 was low, and, yes, their homocysteine was high, “suggest[ing] that vitamin B12 deficiency in vegetarians might have adverse effects on their vascular health.” What we need, though, is an interventional study, where participants are given B12 to see if that fixes it, and here we go. The title of this double-blind, placebo-controlled, randomized crossover study gives it away: “Vitamin B-12 Supplementation Improves Arterial Function in Vegetarians with Subnormal Vitamin B-12 Status.” So, compromised vitamin B12 status among those eating more plant-based diets due to not taking B12 supplements or regularly eating vitamin B12-fortified foods may explain the higher stroke risk found among vegetarians.
Unfortunately, many vegetarians resist taking vitamin B12 supplements due to “misconceptions,” like “hold[ing] on to the old myth that deficiency of this vitamin is rare and occurs only in a small proportion of vegans.” “A common mistake is to think that the presence of dairy products and eggs in the diet, as in LOV [a lacto-ovo vegetarian diet], can still ensure a proper intake [of B12]…despite excluding animal flesh.”
Now that we may have nailed the cause, maybe “future studies with vegetarians should focus on identifying ways to convince vegetarians to take vitamin B12 supplements to prevent a deficiency routinely.”
I have updated my recommendation for B12 supplementation. I now suggest at least 2,000 mcg (µg) of cyanocobalamin once weekly, ideally as a chewable, sublingual, or liquid supplement taken on an empty stomach, or at least 50 mcg daily of supplemental cyanocobalamin. (You needn’t worry about taking too much.) You can also have servings of B12-fortified foods three times a day (at each meal), each containing at least 190% of the Daily Value listed on the nutrition facts label. (Based on the new labeling mandate that started on January 1, 2020, the target is 4.5 mcg three times a day.) Please note, though, that those older than the age of 65 have only one option: to take 1,000 micrograms a day.
Might animal protein-induced increases in the cancer-promoting growth hormone IGF-1 help promote brain artery integrity?
In 2014, a study on stroke risk and dietary protein found that greater intake was associated with lower stroke risk and, further, that the animal protein appeared particularly protective. Might that help explain why, as shown in the graph below and at 0:31 in my video Vegetarians and Stroke Risk Factors: Animal Protein?, vegetarians were recently found to have a higher stroke rate than meat eaters?
Animal protein consumption increases the levels of a cancer-promoting growth hormone in the body known as IGF-1, insulin-like growth factor 1, which “accelerates the progression of precancerous changes to invasive lesions.” High blood concentrations are associated with increased risks of breast, colorectal, lung, and prostate cancers, potentially explaining the association between dairy milk intake and prostate cancer risk, for example. However, there are also IGF-1 receptors on blood vessels, so perhaps IGF-1 promotes cancer and brain artery integrity.
People who have strokes appear to have lower blood levels of IGF-1, but it could just be a consequence of the stroke rather than the cause. There weren’t any prospective studies over time until 2017 when researchers found that, indeed, higher IGF-1 levels were linked to a lower risk of stroke—but is it cause and effect? In mice, the answer seems to be yes, and in a petri dish, IGF-1 appears to boost the production of elastin, a stretchy protein that helps keep our arteries elastic. As you can see in the graph below and at 1:41 in my video, higher IGF-1 levels are associated with less artery stiffness, but people with acromegaly, like Andre the Giant, those with excessive levels of growth hormones like IGF-1, do not appear to have lower stroke rates, and a more recent study of dietary protein intake and risk of stroke that looked at a dozen studies of more than half a million people (compared to only seven studies with a quarter million in the previous analysis), found no association between dietary protein intake and the risk of stroke. If anything, dietary plant protein intake may decrease the risk of stroke.
However, those with high blood pressure who have low IGF-1 levels do appear to be at increased risk of developing atherosclerosis, which is the thickening of the artery walls leading up to the brain, but no such association was found in people with normal blood pressure. So, there may be “a cautionary lesson for vegans” here. Yes, a whole food, plant-based diet “can down-regulate IGF-1 activity” and may slow the human aging process, not to mention reduce the risk of some of the common cancers that plague the Western world. But, “perhaps the ‘take-home’ lesson should be that people who undertake to down-regulate IGF-1 activity [by cutting down on animal protein intake] as a pro-longevity measure should take particular care to control their blood pressure and preserve their cerebrovascular health [the health of the arteries in their brain] – in particular, they should keep salt intake relatively low while insuring an ample intake of potassium” to keep their blood pressures down. So, that means avoiding processed foods and avoiding added salt, and, in terms of potassium-rich foods, eating beans, sweet potatoes, and dark-green leafy vegetables.
Might this explain the higher stroke risk found among vegetarians? No—because dairy and egg whites are animal proteins, too. Only vegans have lower IGF-1 levels in both men and women, so low levels of IGF-1 can’t explain why higher rates of stroke were found in vegetarians. Then what is it? I think the best explanation for the mystery is something called homocysteine, which I cover next.
Beyond eating a plant-based diet, how else can we lower our blood pressure? Check out the chapter of hypertension in my book How Not to Die at your local public library.
This is the eighth video in a 12-part series on vegetarians’ stroke risk. If you missed any of the previous ones, check out the related posts below.
Coming up, we turn to what I think is actually going on:
Stroke had been a leading cause of death in Japan, but the mortality rate decreased sharply as they moved away from their traditional diets and started eating more like those in the West. Did the consumption of all that extra meat and dairy have a protective effect? After all, their intake of animal fat and animal protein was going up at the same time their stroke rates were going down, as shown below and at 0:35 in my video.
Commented a noted Loma Linda cardiology professor, “Protection from stroke by eating animal foods? Surely not!…Many vegetarians, like myself, have almost come to expect the data to indicate that they have an advantage, whatever the disease that is being considered. Thus, it is disquieting to find evidence in a quite different direction for at least one subtype of stroke.”
Can dietary saturated fat, like that found in meat and dairy, be beneficial in preventing stroke risk? There appeared to be a protective association—but only in East Asian populations, as you can see below and at 1:11 in my video.
High dietary saturated fat was found to be associated with a lower risk of stroke in Japanese but not in non-Japanese. So, what was it about the traditional Japanese diet that the westernization of their eating habits made things better when it came to stroke risk? Well, at the same time, their meat and dairy intake was going up, and their salt intake was going down, as you can see below and at 1:40.
The traditional Japanese diet was packed with salt. They had some of the highest salt intakes in the world, about a dozen spoonsful of salt a day. Before refrigeration became widely available, they ate all sorts of salted, pickled, and fermented foods from soy sauce to salted fish. In the areas with twice the salt intake, they had twice the stroke mortality, but when the salt intake dropped, so did the stroke death rates, because when the salt consumption went down, their blood pressure went down, too. High blood pressure is perhaps “the single most important potentially modifiable risk factor for stroke,” so it’s no big mystery why the westernization of the Japanese diet led to a drop in stroke risk.
When they abandoned their more traditional diets, their obesity rates went up and so did their diabetes and coronary artery disease, but, as they gave up the insanely high salt intake, their insanely high stroke rates correspondingly fell.
Stomach cancer is closely associated with excess salt intake. When you look at their stomach cancer rates, they came down beautifully as they westernized their diets away from salt-preserved foods, as you can see in the graph below and at 2:50 in my video.
But, of course, as they started eating more animal foods like dairy, their rates of fatal prostate cancer, for example, shot through the roof. Compared to Japan, the United States has 7 times more deaths from prostate cancer, 5 times more deadly breast cancer, 3 times more colon cancer and lymphoma mortality, and 6 to 12 times the death rate from heart disease, as you can see in the graph below and at 3:15 in my video. Yes, Japanese stroke and stomach cancer rates were higher, but they were also eating up to a quarter cup of salt a day.
That would seem to be the most likely explanation, rather than some protective role of animal fat. And, indeed, it was eventually acknowledged in the official Japanese guidelines for the prevention of cardiovascular disease: “Refrain from the consumption of large amounts of fatty meat, animal fat, eggs, and processed foods…”
Now, one of the Harvard cohorts found a protective association between hemorrhagic strokes and both saturated fat and trans fat, prompting a “sigh of relief…heard throughout the cattle-producing Midwestern states,” even though the researchers concluded that, of course, we all have to cut down on animal fat and trans fat for the heart disease benefit. Looking at another major Harvard cohort, however, they found no such protective association for any kind of stroke, and when they put all the studies together, zero protection was found across the board, as you can see below and at 4:07 in my video.
Observational studies have found that higher LDL cholesterol seems to be associated with a lower risk of hemorrhagic stroke, raising the possibility that cholesterol may be “a double-edged sword,” by decreasing the risk of ischemic stroke but increasing the risk of hemorrhagic stroke. But low cholesterol levels in the aged “may be a surrogate for nutritional deficiencies…or a sign of debilitating diseases,” or perhaps the individuals were on a combination of cholesterol-lowering drugs and blood thinners, and that’s why we tend to see more brain bleeds in those with low cholesterol. You don’t know until you put it to the test.
Researchers put together about two dozen randomized controlled trials and found that the lower your cholesterol, the better when it comes to overall stroke risk, with “no significant increase in hemorrhagic stroke risk with lower achieved low-density lipoprotein [LDL] cholesterol levels.”
The genetic data appear mixed, with some suggesting a lifetime of elevated LDL would give you a higher hemorrhagic stroke risk, while other data suggest more of that double-edged sword effect. However, with lower cholesterol, “any possible excess of hemorrhagic [bleeding] stroke is greatly outweighed by the protective effect against ischaemic stroke,” the much more common clotting type of stroke, not to mention heart disease. It may be on the order of 18 fewer clotting strokes for every 1 extra bleeding stroke with cholesterol-lowering.
Does this explain the increased stroke risk found among vegetarians? Hemorrhagic stroke is the type of stroke that appeared higher in vegetarians, but the cholesterol levels in vegans were even lower, and, if anything, vegans trended towards a higher clotting stroke risk, so it doesn’t make sense. If there is some protective factor in animal foods, it is to be hoped that a diet can be found that still protects against the killer number one, heart disease, without increasing the risk of the killer number five, stroke. But, first, we have to figure out what that factor is, and the hunt continues.
Aren’t there studies suggesting that saturated fat isn’t as bad as we used to think? Check out:
Just like the traditional Japanese diet had a lot going for it despite having high sodium as the fatal flaw, what might be the Achilles’ heel of plant-based diets when it comes to stroke risk?
This is the seventh video in this stroke series. See the related posts below for the others.
Just because you’re eating a vegetarian or vegan diet doesn’t mean you’re eating healthfully.
“Plant-Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults”: This study of a diverse sample of 12,000 Americans found that “progressively increasing the intake of plant foods by reducing the intake of animal foods is associated with benefits on cardiovascular health and mortality.” Still, regarding plant-based diets for cardiovascular disease prevention, “all plant foods are not created equal.” As you can see in the graph below and at 0:40 in my video Vegetarians and Stroke Risk Factors: Vegan Junk Food?, a British study found higher stroke risk in vegetarians. Were they just eating a lot of vegan junk food?
“Any diet devoid of animal food sources can be claimed to be a vegetarian [or vegan] diet; thus, it is important to determine” what is being eaten. One of the first things I look at when I’m trying to see how serious a population is about healthy eating is something that is undeniably, uncontroversially bad: soda, aka liquid candy. Anyone drinking straight sugar water doesn’t have health on top of mind.
A large study was conducted of plant-based eaters in the United States, where people tend to cut down on meat for health reasons far more than for ethics, as you can see in the graph below and at 1:20 in my video.
Researchers found that flexitarians drink fewer sugary beverages than regular meat eaters, as do pescatarians, vegetarians, and vegans, as you can see below and at 1:30.
However, in the study from the United Kingdom where the increased stroke risk in vegetarians was found and where people are more likely to go veg or vegan for ethical reasons, researchers found that pescatarians drink less soda, but the vegetarians and vegans drink more, as shown in the graph below and at 1:44.
I’m not saying that’s why they had more strokes; it might just give us an idea of how healthfully they were eating. In the UK study, the vegetarian and vegan men and women ate about the same amounts of desserts, cookies, and chocolate, as you can see in the graph below and at 1:53.
They also consumed about the same total sugar, as shown below and at 2:02.
In the U.S. study, the average non-vegetarian is nearly obese, the vegetarians are a little overweight, and the vegans were the only ideal weight group. In this analysis of the UK study, however, everyone was about the same weight. The meat eaters were lighter than the vegans, as you can see below, and at 2:19 in my video. The EPIC-Oxford study seems to have attracted a particularly “health-conscious” group of meat eaters weighing substantially less than the general population.
Let’s look at some specific stroke-related nutrients. Dietary fiber appears to be beneficial for the prevention of cardiovascular disease, including stroke, and it seems the more, the better, as you can see in the graph below and at 2:43 in my video.
Based on studies of nearly half a million men and women, there doesn’t seem to be any upper threshold of benefit—so, again, “the more, the better.” At more than 25 grams of soluble fiber and 47 grams of insoluble dietary fiber, you can start seeing a significant drop in associated stroke risk. So, one could consider these values “as the minimal recommendable daily intake of soluble and insoluble fiber…to prevent stroke at a population level.” That’s what you see in people eating diets centered around minimally processed plant foods. Dean Ornish, M.D., got up around there with his whole food, plant-based diet. It might not be as much as we were designed to eat, based on the analyses of fossilized feces, but that’s about where we might expect significantly lower stroke risk, as shown below and at 3:25 in my video.
How much were the UK vegetarians getting? 22.1 grams. Now, in the UK, they measure fiber a little differently, so it may be closer to 30 grams, but that’s still not the optimal level for stroke prevention. It’s so little fiber that the vegetarians and vegans only beat out the meat eaters by about one or two bowel movements a week, as you can see below and at 3:48 in my video, suggesting the non-meat eaters were eating lots of processed foods.
The vegetarians were only eating about half a serving more of fruits and vegetables. Intake is thought to reduce stroke risk in part because of their potassium content, but the UK vegetarians at higher stroke risk were eating so few greens and beans that they couldn’t even match the meat eaters. The vegetarians (and the meat eaters) weren’t even reaching the recommended minimum daily potassium intake of 4,700 mg a day.
What about sodium? “The vast majority of the available evidence indicates that elevated salt intake is associated with higher stroke risk…” There is practically a straight-line increase in the risk of dying from a stroke, the more salt you eat, as you can see in the graph below and at 4:29 in my video.
Even just lowering sodium intake by a tiny fraction every year could prevent tens of thousands of fatal strokes. “Reducing Sodium Intake to Prevent Stroke: Time for Action, Not Hesitation” was the title of the paper, but the UK vegetarians and vegans appeared to be hesitating, as did the other dietary groups. “All groups exceeded the advised less than 2400 mg daily sodium intake”—and that didn’t even account for salt added to the table! The American Heart Association recommends less than 1,500 mg a day. So, they were all eating a lot of processed foods. It’s no wonder the vegetarians’ blood pressures were only one or two points lower. High blood pressure is perhaps “the single most important potentially modifiable risk factor for stroke.”
What evidence do I have that the vegetarians’ and vegans’ stroke risk would go down if they ate more healthfully? Well, in rural Africa, where they were able to nail the fiber intake that our bodies were designed to get by eating so many whole, healthy plant foods—including fruits, vegetables, grains, greens, beans, and protein almost entirely from plant sources—not only was heart disease, our number one killer, “almost non-existent,” but so was stroke. It only surged up from nowhere “with the introduction of salt and refined foods” to their diet.
“It is notable that stroke and senile dementia appear to be virtually absent in Kitava, an Oceanic culture [near Australia] whose quasi-vegan traditional diet is very low in salt and very rich in potassium.” They ate fish a few times a week, but the other 95 percent or so of their diet was made up of vegetables, fruits, corn, and beans. They had an apparent absence of stroke, even despite their ridiculously high rates of smoking, 76 percent of men and 80 percent of women. We evolved by eating as little as less than an eighth of a teaspoon of salt a day, and our daily potassium consumption is thought to have been as high as 10,000 mg or so. We went from an unsalted, whole-food diet to eating salty, processed foods depleted of potassium whether we eat meat or not.
Caldwell Esselstyn at the Cleveland Clinic tried putting about 200 patients with established cardiovascular disease on a whole food, plant-based diet. Of the 177 who stuck with the diet, only a single patient went on to have a stroke in the subsequent few years, compared to a hundred-fold greater rate of adverse events, including multiple strokes and deaths in those who strayed from the diet. “This is not vegetarianism,” Esselstyn explains. Vegetarians can eat a lot of less-than-ideal foods, “such as milk, cream, butter, cheese, ice cream, and eggs. This new paradigm is exclusively plant-based nutrition.”
This entire train of thought—that the reason typical vegetarians don’t have better stroke statistics is because they’re not eating particularly stellar diets—may explain why they don’t have significantly lower stroke rates. However, it still doesn’t explain why they may have higher stroke rates. Even if they’re eating similarly crappy, salty, processed diets, at least they aren’t eating meat, which we know increases stroke risk. There must be something about vegetarian diets that so increases stroke risk that it offsets their inherent advantages. We’ll continue our hunt for the answer next.
From a medical standpoint, labels like vegan and vegetarian just tell me what you don’t eat. It’s like identifying yourself as a “No-Twinkie-tarian.” You don’t eat Twinkies? Great, but what’s the rest of your diet like?
What are the healthiest foods? Check out my Daily Dozen.
To catch up on the rest of this series, see related posts below.
Does eating fish or taking fish oil supplements reduce stroke risk?
In my last video, we started to explore what might explain the higher stroke risk in vegetarians found in the EPIC-Oxford study. As you can see below and at 0:25 in my video Vegetarians and Stroke Risk Factors: Omega-3s?, vegetarians have a lower risk of heart disease and cardiovascular disease overall, but a higher risk of stroke. We looked into vitamin D levels as a potential mechanism, but that didn’t seem to be the reason. What about long-chain omega-3s, the fish fats like EPA and DHA?
Not surprisingly, their levels are found to be “markedly lower in vegetarians and particularly in vegans than in meat-eaters.” They’re about 30 percent lower in vegetarians and more than half as low in vegans, as you can see below and at 0:45 in my video.
According to “the most extensive systematic assessment of effects of omega-3 fats on cardiovascular health to date,” combining 28 randomized controlled trials, stroke has no benefit. There is evidence that taking fish oil “does not reduce heart disease, stroke or death,” or overall mortality, either. This may be because, on the one hand, the omega-3s may be helping, but the mercury in fish may be making things worse. “Balancing the benefits with the contaminant risks of fish consumption has represented a challenge for regulatory agencies and public health professionals.”
For example, dietary exposure to polychlorinated biphenyls (PCBs) may be associated with an increased risk of stroke. In one study, for instance, “neither fish nor intake of PCBs was related to stroke risk. However, with adjustment for fish intake,” that is, at the same fish intake, “dietary PCBs were associated with an increased risk of total stroke,” so the PCB pollutants may be masking the fish benefit. If we had a time machine and could go back before the Industrial Revolution and find fish in an unpolluted state, we might find that it is protective against stroke. Still, looking at the EPIC-Oxford study data, if fish were protective, then we might expect that the pescatarians (those who eat fish but no other meat) would have lower numbers of strokes since they would have the fish benefit without the risk from other meat. But, no. That isn’t the reality. So, it doesn’t seem to be the omega-3s either.
Let’s take a closer look at what the vegetarians are eating.
When it comes to plant-based diets for cardiovascular disease prevention, all plant foods are not created equal. There are two types of vegetarians—those who do it for their health, and those who do it for ethical reasons, like global warming or animals—and the latter tend to eat different diets. Health vegans tend to eat more fruits and fewer sweets, for instance, and you don’t tend to see them chomping down on vegan donuts, as shown below and at 2:41 in my video.
“Concerns about health and costs were primary motivations for [meat] reduction” in the United States. A middle-class American family is four times more likely to reduce meat for health reasons compared to environmental or animal welfare concerns, as you can see in the graph below and at 2:55 in my video.
But in the United Kingdom, where the EPIC-Oxford stroke study was done, ethics was the number one reason given for becoming vegetarian or vegan, as you can see in below and at 3:05 in my video.
We know that “plant-based diets, diets that emphasize higher intakes of plant foods and lower intakes of animal foods, are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality”—a lower risk of dying from all causes put together—“in a general US adult population.” But, that’s only for healthy plant foods. Eating a lot of Wonder Bread, soda, and apple pie isn’t going to do you any favors. “For all types of plant-based diets, however, it is crucial that the choice of plant foods is given careful consideration.” We should choose whole fruits and whole grains over refined grains and avoid trans fats and added sugars. Could it be that the veggie Brits were just eating more chips? We’ll find out next.
Another strikeout trying to explain the increased risk. Could it be that the vegetarians were eating particularly unhealthy diets? Labels like vegetarian or vegan just tell me what is not being eaten. You can be vegetarian and consume a lot of unhealthy fare, like french fries, potato chips, and soda. That’s why, as a physician, I prefer the term whole food, plant-based nutrition. That tells me what you do eat. You eat vegetables and follow a diet centered around the healthiest foods out there.
If you missed the first four videos in this series, see: