TAMPA, Fla — A free health care event in Tampa on Saturday helped hundreds of people in need.
Pioneer Medical Foundation, a nonprofit, hosted its sixth annual community health fair.
What You Need To Know
Pioneer Medical Foundation hosted its sixth annual community health fair
The event aimed to help people who were uninsured and under insured get access to medical services
The fair also helped provide social services
There were about 40 booths and 400 people in attendance
There were about 40 booths and about 400 people in attendance, according to organizers.
“They’re going out of their way to help the homeless and they help people in need,” said David Poole, who attended.
The goal of the fair was to help people who are uninsured or under insured get access to health care.
According to the U.S. Census Bureau, in 2023 over 13% of Florida residents were uninsured.
“Access is not there. A lot of people can’t access health care, so this is why we’re bringing the health care to the people and bridging that gap,” said Ano Kashuma, Executive Director, Pioneer Medical Foundation.
At least 50 nurse practitioners, physicians and dentists volunteered their time and expertise to help hundreds of people.
Vision and mammogram screenings and teeth extractions were some of the medical services offered.
“A lot of the times we’re seeing that when people are coming to the E.R., they have chronic conditions that could have been prevented by a visit to your primary care doctor,” Kashuma said.
Along with medical services there were social services. There was access to showers, free clothing and bus passes. There were also giveaways.
Poole was there to try and win a free bike
“I hope they keep up the gratitude, the love, they’re showing for the homeless and keep doing what they’re doing,” Poole said.
Organizers said the health fair continues to grow year after year.
The foundation is also serving several counties on weekdays with a mobile medical unit van.
Some people think a proposed tax on California’s billionaires to make up for cuts in federal funding to hospitals and healthcare programs will drive money out of the state.
To Seema Kanani, a medical social worker for a major hospital system in Northern California, it is time to sound the alarm about the future of healthcare in the state.
“We need to do this now. We can’t wait 5-10 years,” she said. “We are at risk in the near future, actually, of having hospitals, ERs, and community clinics close down.”
She’s been a member of the healthcare justice union, the Service Employees International Union – United Healthcare Workers West (SEIU-UHW), for 19 years.
Her union is proposing a billionaire wealth tax to make up for massive federal healthcare spending cuts that are set to take place over the next decade, which will largely impact middle- and lower-income Californians.
“A lot of my patients will choose to kind of ration their diabetes medication or other medications they cannot afford because they have to choose between paying their electricity bill or getting their medication,” Kanani said.
The idea is to levy a one-time, 5% tax on the wealth, not income, of billionaires that live in California.
“There are over 200 billionaires just in California. So, it’s time for them to step up and do their part for the state that has given them so much,” she said. “This is not meant to be a long-term fix. That’s why it’s an emergency, one-time tax. It’s not a long-term tax.”
A December analysis from California’s non-partisan Legislative Analyst’s Office revealed the proposed billionaire tax would likely generate tens of billions of dollars for the state over several years. It also notes that state income tax revenues would likely decrease by hundreds of millions of dollars per year on an ongoing basis if the ultra-wealthy were to leave the state.
The latter is what San Jose Mayor Matt Mahan fears will happen if the idea comes to fruition.
“We will actually increasingly have to rely on middle-class and working families to fill that gap. That’s who will lose here. People who will benefit are the taxpayers of Texas and Arizona and Florida, who will now have more billionaires relocating to their state and sharing in the burden of paying for their public services and infrastructure,” Mahan said.
Mahan believes the concept would do more harm than good in the long-run for California.
“It’s an incredible risk. We are talking about putting at risk the driver of our economy, the job creation engine of California, for a one-time tax, to subsidize a system that is ripe with waste, fraud, and abuse,” he said. “Let’s get serious about tackling economic inequality by closing loopholes, not pushing capital out of state.”
He acknowledges there are bigger-picture solutions needed for addressing wealth inequality in the Bay Area, California, and the nation.
“Wealth inequality is a very real issue. It deserves serious solutions. I think there are a number of them out there that we ought to pursue. We make it far too easy for very wealthy individuals to avoid paying taxes on their accumulated assets. I’ve heard from folks who are quite wealthy who acknowledge that they can borrow against their assets and never pay taxes on them – they can pass them on, tax-free, to their heirs,” Mahan said. “There are very real ways that are pragmatic that we could, at a national level, close massive loopholes related to wealth accumulation that would level the playing field, generate additional public revenues, and really, create a more fair economy for everyone.”
From Kanani’s standpoint, this step is needed to help save California’s healthcare system, and it is not meant to be a silver bullet for solving wealth inequality.
“The life and the American Dream that California is known for is not going to exist if the healthcare collapse happens,” she said. “I would welcome anyone that has other ways to tackle this to suggest so.”
She’s hopeful the proposition will receive enough petition signatures and will be put to voters in November. It will need 874,641 signatures by June 24 to qualify for the November ballot, according to Ballotpedia.
When Kassidy Hooter learned in December how much her health insurance costs were going to rise this year, she went into panic mode.
The Shreveport, Louisiana, resident and mother of three knew she urgently needed care — Hooter is in the final trimester of a high-risk pregnancy. But the family could no longer afford their Affordable Care Act plan coverage now that a federal tax subsidy was lapsing on Dec. 31, 2025, meaning they would face thousands of dollars in additional out-of-pocket costs.
“We heavily considered that it might just be cheaper to give birth at home,” Hooter, 24, told CBS News. “Just because that’s an insane amount of debt to take on.”
In the end, Hooter decided to forgo insurance altogether.
Kassidy Hooter, seen here with her husband Morgan and their three children, faces sharply higher health costs after an Affordable Care Act tax credit expired in December of 2025.
Courtesy of Kassidy Hooter
A local medical center offered three months of financial aid that will carry her through her due date in February andinto late March. After that, she will have to bear any medical expenses on her own. Her plan now is to get her newborn on Medicaid, a government health plan for low-income Americans, as quickly as possible.
“I’m just hoping for the best,” she told CBS News.
Health insurance as “luxury”
Since its introduction in 2010, the ACA has been instrumental in cutting the share of uninsured Americans from approximately 15% to 8%, according to Nima Sheth, vice president of health justice at the National Partnership for Women and Families, a nonprofit advocacy group.
However, the number of people without health insurance is likely to surge if Congress fails to come up with a solution for the 22 million Americans who received an ACA tax credit, experts warn. The number of uninsured will rise by an average of 3.8 million each year from 2026 to 2034 without an extension of the credits, the Congressional Budget Office estimated in 2024.
Americans in most states have until Jan. 15 to enroll in an ACA marketplace plan, according to healthinsurance.org.
Without the tax credits, premiums for ACA enrollees who previously relied on the subsidies will increase by an average of 114%, estimates KFF, a nonprofit provider of health policy news and research.
“What we’re seeing here is a policy choice — is, in effect, turning insurance into a luxury item and medical debt into the default,” Michelle Sternthal, interim senior director of policy and strategy at health care advocacy group Community Catalyst, told CBS News.
The House of Representatives on Thursday approved a three-year extension of the expired ACA tax credits. The legislation faces an uphill climb in the Republican-led Senate, although lawmakers think it could provide a starting point for a compromise that would keep the credits alive in some form.
“It’s weighing extraordinarily heavily on me”
Plantation, Florida, resident Stacy Kanas, whose family also received an ACA tax credit, is now considering going without health insurance after realizing that her monthly premium to cover her and her husband would rise to $2,500 — more than double what she was paying last year to cover both of them plus her 20-year-old daughter.
“It’s weighing extraordinarily heavily on me,” Kanas, 59, told CBS News. “My husband had a major surgery about five years ago, and we don’t want to be uninsured.”
Although in decent health, the small business owner worries about what could happen if someone in her family falls seriously ill. “You’re one catastrophic event away from perhaps having a financial disaster,” she said.
Even people who keep their ACA coverage could end up skipping out on care to avoid out-of-pocket expenses, experts said.
“If you’re underinsured and you have high deductibles, the coverage that you’re getting is designed to dissuade getting care, including preventative care, so you’re going to delay your care until there are emergencies,” Sternthal said.
Robert Myers, a consultant based outside of St. Louis, Missouri, was on a silver ACA plan last year, but switched to a bronze plan after learning his premiums would rise to $400 a month, up from $17 in 2025.
Under his new plan, the 31-year-old does not have a monthly premium. However, Myers could owe much more in out-of-pocket costs due to $80 co-pays and an $8,000 deductible. As a result, he’s planning on scaling back on doctor’s visits, a trend experts say ends up driving more people to the emergency room for care.
“They’ll kind of go to the ER and get what they need fixed with a band aid, and then not get long-term care,” Sheth said.
This can have wider ripple effects because an increase in uncompensated hospital care can drive up costs for other patients, as facilities seek to recoup the costs, according to Sternthal, who supports an extension of the ACA tax credits.
“Every delay locks families into decisions that harm their health and their financial stability, but then also reverberates out into the business community, the local community,” she said.
As we begin a new year, we wanted to take a moment to look back on what we’ve accomplished together in 2025, and to look forward to all that we will accomplish together in 2026.
Thank you from the bottom of our hearts!
Because of MoveOn members like you, we took action when it mattered. We pushed back against harmful fascist agendas, fought to protect democracy, elected progressive leaders up and down the ballot, and helped ensure millions of voices were heard. None of that happens without people willing to stay involved, even when progress feels slow.
To capture just a snapshot of that work, we put together a short year in review highlighting some of the biggest wins moveOn members helped achieve in 2025.
If we’re going to win back congressional power with progressive candidates, we’re going to need your help.
We also know that staying engaged in this fight requires rest and here at MoveOn, we thrive on creativity and care. To start the year, we are sharing a few tokens of our appreciation for all of the change you helped drive in 2025. Check out some of our favorite stress relievers: a fun coloring book and a calendar to keep up the fight all year long.
Your AI doctor’s office is expanding. On Jan. 7, OpenAI announced that over the coming weeks, it will roll out ChatGPT Health, a dedicated tab for health that allows users to upload their medical records and connect apps like Apple Health, the personalized health testing platform Function, and MyFitnessPal.
According to the company, more than 40 million people ask ChatGPT a health care-related question every day, which amounts to more than 5% of all global messages on the platform—so, from a business perspective, leaning into health makes sense. But what about from a patient standpoint?
“I wasn’t shocked to hear this news,” says Dr. Danielle Bitterman, a radiation oncologist and clinical lead for data science and AI at Mass General Brigham Digital. “I do think that this speaks to an unmet need that people have regarding their health care. It’s difficult to get in to see a doctor, it’s nowadays hard to find medical information, and there is, unfortunately, some distrust in the medical system.”
We asked experts whether turning over your health data to an AI tool is a good idea.
What is ChatGPT Health?
The new feature will be a hub where people can upload their medical records, including lab results, visit summaries, and clinical history. That way, when you ask the bot questions, it will be “grounded in the information you’ve connected,” the company said in its announcement. OpenAI suggests asking questions like: “How’s my cholesterol trending?” “Can you summarize my latest bloodwork before my appointment?” “Give me a summary of my overall health.” Or: “I have my annual physical tomorrow. What should I talk to my doctor about?”
Users can also connect ChatGPT to Apple Health, so the AI tool has access to data like steps per day, sleep duration, and number of calories burned during a workout. Another new addition is the ability to sync with data from Function, a company that tests for more than 160 markers in blood, so that ChatGPT has access to lab results as well as clinicians’ health suggestions. Users can also connect MyFitnessPal for nutrition advice and recipes, and Weight Watchers for meal ideas and recipes geared toward those on GLP-1 medications.
OpenAI, which has a licensing and technology agreement that allows the company to access TIME’s archives, notes that Health is designed to support health care—not replace it—and is not intended to be used for diagnosis or treatment. The company says it spent two years working with more than 260 physicians across dozens of specialities to shape what the tool can do, as well as how it responds to users. That includes how urgently it encourages people to follow-up with their provider, the ability to communicate clearly without oversimplifying, and prioritizing safety when people are in mental distress.
Is it safe to upload your medical data?
OpenAI partnered with b.well, a data connectivity infrastructure company, to allow users to securely connect their medical records to the tool. The Health tab will have “enhanced privacy,” including a separate chat history and memory feature than other tabs, according to the announcement. OpenAI also said that “conversations in Health are not used to train our foundation models,” and Health information won’t flow into non-Health chats. Plus, users can “view or delete Health memories at any time.”
Still, some experts urge caution. “The most conservative approach is to assume that any information you upload into these tools, or any information that may be in applications you otherwise link to the tools, will no longer be private,” Bitterman says.
No federal regulatory body governs the health information provided to AI chatbots, and ChatGPT provides technology services that are not within the scope of HIPAA. “It’s a contractual agreement between the individual and OpenAI at that point,” says Bradley Malin, a professor of biomedical informatics at Vanderbilt University Medical Center. “If you are providing data directly to a technology company that is not providing any health care services, then it is buyer beware.” In the event that there was a data breach, ChatGPT users would have no specific rights under HIPAA, he adds, though it’s possible the Federal Trade Commission could step in on your behalf, or that you could sue the company directly. As medical information and AI start to intersect, the implications so far are murky.
“When you go to your health care provider and you have an interaction with them, there’s a professional agreement that they’re going to maintain this information in a confidential manner, but that’s not the case here,” Malin says. “You don’t know exactly what they are going to do with your data. They say that they’re going to protect it, but what exactly does that mean?”
When asked for comment on Jan. 8, OpenAI directed TIME to a post on X from chief information security officer Dane Stuckey. “Conversations and files in ChatGPT are encrypted by default at rest and in transit as part of our core security architecture,” he wrote. “For Health, we built on this foundation with additional, layered protections. This includes another layer of encryption…enhanced isolation, and data segmentation.” He added that the changes the company has made “give you maximum control over how your data is used and accessed.”
The question every user has to grapple with is “whether you trust OpenAI to keep to their word,” says Dr. Robert Wachter, chair of the department of medicine at the University of California, San Francisco, and author of A Giant Leap: How AI Is Transforming Healthcare and What That Means for Our Future.
Does he trust it? “I sort of do, in part because they have a really strong corporate interest in not screwing this up,” he says. “If they want to get into sensitive topics like health, their brand is going to be dependent on you feeling comfortable doing this, and the first time there’s a data breach, it’s like, ‘Take my data out of there—I’m not sharing it with you anymore.’”
Wachter says that if there was information in his records that could be detrimental if it leaked—like a past history of drug use, for example—he would be reluctant to upload it to ChatGPT. “I’d be a little careful,” he says. “Everybody’s going to be different on that, and over time, as people get more comfortable, if you think what you’re getting out of it is useful, I think people will be quite willing to share information.”
The risk of bad information
Beyond privacy concerns, there are known risks of using large-language-model-based chatbots for health information. Bitterman recently co-authored a study that found that models are designed to prioritize being helpful over medical accuracy—and to always supply an answer, especially one that the user is likely to respond to. In one experiment, for example, models that were trained to know that acetaminophen and Tylenol are the same drug still produced inaccurate information when asked why one was safer than the other.
“The threshold of balancing being helpful versus being accurate is more on the helpfulness side,” Bitterman says. “But in medicine we need to be more on the accurate side, even if it’s at the expense of being helpful.”
Plus, multiplestudiessuggest that if there’s missing information in your medical records, models are more likely to hallucinate, or produce incorrect or misleading results. According to a report on supporting AI in health care from the National Institute of Standards and Technology, the quality and thoroughness of the health data a user gives a chatbot directly determines the quality of the results the chatbot generates; poor or incomplete data leads to inaccurate, unreliable results. A few common traits help increase data quality, the report notes: correct, factual information that’s comprehensive, complete, and consistent, without any outdated or misleading insights.
In the U.S., “we get our health care from all different sites, and it’s fragmented over time, so most of our health care records are not complete,” Bitterman says. That increases the likelihood that you’ll see errors where it’s guessing what happened in areas where there are gaps, she says.
The best way to use ChatGPT Health
Overall, Wachter considers ChatGPT Health a step forward from the current iteration. People were already using the bot for health queries, and by providing it with more context via their medical records—like a history of diabetes or blood clots—he believes they’ll receive more useful responses.
“What you’ll get today, I think, is better than what you got before if all your background information is in there,” he says. “Knowing that context would be useful. But I think the tools themselves are going to have to get better over time and be a little bit more interactive than they are now.”
When Dr. Adam Rodman watched the ChatGPT Health introductory video, he was pleased with what he saw. “I thought it was pretty good,” says Rodman, a general internist at Beth Israel Deaconess Medical Center, where he leads the task force for integration of AI into the medical school curriculum, and an assistant professor at Harvard Medical School. “It really focused on using it to help understand your health better—not using it as a replacement, but as a way to enhance.” Since people were already using ChatGPT for things like analyzing lab results, the new feature will simply make doing so easier and more convenient, he says. “I think this more reflects what health care looks like in 2026 rather than any sort of super novel feature,” he says. “This is the reality of how health care is changing.”
When Rodman counsels his patients on how to best use AI tools, he tells them to avoid health management questions, like asking the bot to choose the best treatment program. “Don’t have it make autonomous medical decisions,” he says. But it’s fair game to ask if your doctor could be missing something, or to explore “low-risk” matters like diet and exercise plans, or interpreting sleep data.
One of Bitterman’s favorite usages is asking ChatGPT to help brainstorm questions ahead of a doctor appointment. Augmenting your existing care like that is a good idea, she says, with one clear bonus: “You don’t necessarily need to upload your medical records.”
It’s the first week of a new year for Congress, and each chamber is considering legislation with votes to watch on Thursday.Enhanced Health Care SubsidiesThe House of Representatives is voting on a bill to reinstate tax credits that expired last year and were central to the government shutdown.The bill aims to extend these subsidies for three years, helping those without insurance through their employers pay for coverage. Four Republicans: Rep. Brian Fitzpatrick (PA-1st), Rep. Ryan McKenzie (PA-7th), Rep. Rob Bresnahan (PA-8th), and Rep. Mike Lawler (NY-17th) joined Democrats to push the vote, which is expected to pass. Five more Republicans joined Democrats during a test vote on Wednesday.However, the Senate is not expected to consider this bill, as they are working on their own Affordable Care Act reform measure designed to pass both chambers.Venezuela War Powers ResolutionThe Senate is revisiting a war powers resolution that would prevent the president from using military force in Venezuela without congressional approval. This follows a recent military operation in Venezuela’s capital, which led to the arrest of President Nicolás Maduro and his wife, who are now in New York facing narcoterrorism charges. President Donald Trump has stated that the U.S. is running Venezuela and may deploy the military again if the remaining Maduro regime does not comply with U.S. demands.The same resolution failed a previous vote, as well as a measure to stop the Trump administration from bombing alleged drug boats in the Caribbean and Pacific that the White House says were connected to Venezuela. Past administrations arrested and charged such suspects. The Trump administration’s campaign has killed more than 100 people.Reactions To Greenland RhetoricThe White House’s suggestion to use military force to take over Greenland has been met with criticism on Capitol Hill. Democrats have long opposed this idea, and several Republicans have recently spoken out against it.Rep. Mike Johnson, House Speaker, said, “All this stuff about military action and all that, I don’t even think that’s a possibility.” Sen. Thom Tillis of North Carolina criticized the notion, saying, “Making insane comments about how it is our right to have territory owned by the kingdom of Denmark, folks, amateur hour is over.” Rep. Ryan Zinke of Montana noted, “In the case of Greenland, you have two things: one, not a present threat, and so they have a duly elected president. So, he doesn’t have the authority without Congress.”Rep. Don Bacon of Nebraska added, “It’s very… amateurish. I feel like we’ve got high school kids playing Risk.”Secretary of State Marco Rubio has also stated that the president wants to buy Greenland.Earlier this week, the White House Press Secretary Karoline Leavitt told Hearst Television: “President Trump has made it well known that acquiring Greenland is a national security priority of the United States, and it’s vital to deter our adversaries in the Arctic region. The President and his team are discussing a range of options to pursue this important foreign policy goal, and of course, utilizing the U.S. Military is always an option at the Commander in Chief’s disposal.”Keep watching for the latest from the Washington News Bureau:
WASHINGTON —
It’s the first week of a new year for Congress, and each chamber is considering legislation with votes to watch on Thursday.
Enhanced Health Care Subsidies
The House of Representatives is voting on a bill to reinstate tax credits that expired last year and were central to the government shutdown.
The bill aims to extend these subsidies for three years, helping those without insurance through their employers pay for coverage. Four Republicans: Rep. Brian Fitzpatrick (PA-1st), Rep. Ryan McKenzie (PA-7th), Rep. Rob Bresnahan (PA-8th), and Rep. Mike Lawler (NY-17th) joined Democrats to push the vote, which is expected to pass. Five more Republicans joined Democrats during a test vote on Wednesday.
However, the Senate is not expected to consider this bill, as they are working on their own Affordable Care Act reform measure designed to pass both chambers.
Venezuela War Powers Resolution
The Senate is revisiting a war powers resolution that would prevent the president from using military force in Venezuela without congressional approval. This follows a recent military operation in Venezuela’s capital, which led to the arrest of President Nicolás Maduro and his wife, who are now in New York facing narcoterrorism charges.
President Donald Trump has stated that the U.S. is running Venezuela and may deploy the military again if the remaining Maduro regime does not comply with U.S. demands.
The same resolution failed a previous vote, as well as a measure to stop the Trump administration from bombing alleged drug boats in the Caribbean and Pacific that the White House says were connected to Venezuela. Past administrations arrested and charged such suspects. The Trump administration’s campaign has killed more than 100 people.
Reactions To Greenland Rhetoric
The White House’s suggestion to use military force to take over Greenland has been met with criticism on Capitol Hill. Democrats have long opposed this idea, and several Republicans have recently spoken out against it.
Rep. Mike Johnson, House Speaker, said, “All this stuff about military action and all that, I don’t even think that’s a possibility.”
Sen. Thom Tillis of North Carolina criticized the notion, saying, “Making insane comments about how it is our right to have territory owned by the kingdom of Denmark, folks, amateur hour is over.”
Rep. Ryan Zinke of Montana noted, “In the case of Greenland, you have two things: one, not a present threat, and so they have a duly elected president. So, he doesn’t have the authority without Congress.”
Rep. Don Bacon of Nebraska added, “It’s very… amateurish. I feel like we’ve got high school kids playing Risk.”
Secretary of State Marco Rubio has also stated that the president wants to buy Greenland.
Earlier this week, the White House Press Secretary Karoline Leavitt told Hearst Television: “President Trump has made it well known that acquiring Greenland is a national security priority of the United States, and it’s vital to deter our adversaries in the Arctic region. The President and his team are discussing a range of options to pursue this important foreign policy goal, and of course, utilizing the U.S. Military is always an option at the Commander in Chief’s disposal.”
Keep watching for the latest from the Washington News Bureau:
In Utah, artificial intelligence can now renew some prescriptions. A Politico exclusive says the pilot program will “test how far patients and regulators are willing to trust AI in medicine.” Yasmin Khorram, economic policy reporter for Politico, joins CBS News to discuss her reporting.
Enhanced tax credits that have helped reduce the cost of health insurance for the vast majority of Affordable Care Act enrollees expired overnight as 2026 arrived, cementing higher health costs for millions of Americans at the start of the new year. Nicole Sganga reports.
From the passage of a massive bill that reduced federal funds for Medicaid to a comprehensive overhaul of a federal vaccine advisory panel, Congress and the Trump administration delivered major changes to America’s public health system in 2025.
Many of those changes are poised to reshape coverage, care delivery and public health policy in the new year as provisions take effect, healthcare premiums more than double, and new requirements begin to kick in.
Here’s a look at the biggest policy shifts set in motion last year that should be felt in the new year:
ACA Subsidies Will Sunset
Premium tax credits meant to further reduce the price of healthcare plans bought on the Affordable Care Act marketplace expired on Dec. 31 after Congress declined to address a looming “subsidy cliff.”
The credits increased financial assistance and expanded it to those with incomes above 400% of the federal poverty lines. Since the credits were first introduced in 2021, enrollment in the ACA marketplace increased to more than 24 million.
The Center on Budget and Policy Priorities projected that almost 22 million peoplewould see their healthcare costs “dramatically rise” or would lose their coverage altogether without the extension. The Urban Institute estimated that 7.3 million fewer Americans would receive subsidized coverage in 2026 and that 4.8 million more would be uninsured in 2026.
State Medicaid Expansion Incentives to End
The American Rescue Plan Act of 2021 offered a temporary financial incentive to encourage states to expand Medicaid coverage to more low-income Americans. The act used the 138% poverty level listed in the Affordable Care Act to offer states a two-year, 5% match to the Federal Medical Assistance Percentage, the amount the federal government shoulders, for Medicaid expansion expenditures.
But the incentive will largely end as it currently exists due to the legislation known as the “big, beautiful bill.” States wishing to qualify for the enhanced funding must have completely expanded their Medicaid programs by Jan. 1. States that have already expanded their programs will retain their existing FMAP levels, and those receiving the two-year bonus will continue to receive it until the period ends.
Removal of Tax Liability Caps
For ACA marketplace enrollees, their premium tax credits are determined based on what they estimate their income will be at the beginning of the year. If the prediction is incorrect and the income is higher than expected, they are expected to repay. The process of repayment to the IRS is known as reconciliation and was expected to be undertaken when enrollees filed their federal income tax returns.
Now, under a provision of the “big, beautiful bill,” marketplace enrollees will be expected to repay the full amount they owe. Also, the continuous special enrollment period for people whose incomes are below 150% of the federal poverty line will end. In addition, those enrolling in coverage during a special enrollment period based on their income and not tied to a qualifying life event will not be eligible for the credits beginning this year.
Change in Tax Credit Eligibility for Noncitizens
The “big, beautiful bill” also included changes to the eligibility requirements for people who are not citizens who wish to receive ACA marketplace premium credits.
Credits will be limited to green-card holders, Cuban or Haitian entrants, or Compact of Free Association migrants or citizens of the Marshall Islands, Palau or Micronesia. Previously eligible categories, like refugees, asylum-seekers and those granted temporary protected status, will no longer qualify.
The bill also ends a special rule known as the Medicaid waiting list loophole. The rule allowed people who are not citizens whose incomes are below 100% of the federal poverty line and who are ineligible for Medicaid coverage due to their status to receive the premium credits.
The changes are expected to take effect Jan. 1.
Caps on Federal Loans for Medical Students
The “big, beautiful bill” also caps the amount medical students can receive in Federal Direct Stafford Loans and Federal Direct PLUS Loans.
The changes will take effect on July 1.
Sign Up for U.S. News Healthcare of Tomorrow Bulletin
Your trusted source for critical insights and solutions-focused analysis.
Sign up to receive the latest updates from U.S. News & World Report and our trusted partners and sponsors. By clicking submit, you are agreeing to our Terms and Conditions & Privacy Policy.
More Vaccine Reviews
The Department of Health and Human Services is expected to continue its overhaul of vaccine recommendations in the new year, starting with the schedule of recommended vaccines for children. The proposed new schedule will recommend fewer shots to mimic those from other developed countries, specifically Denmark. CNN reported that the plan has not been finalized but was expected in late December before it was pushed to 2026.In addition, the Centers for Disease Control and Prevention’s vaccine advisory panel is set to meet three times in the new year: Feb. 25-26, June 24-25 and Oct. 21-22.
Maryland Rep. Glenn Ivey believes that Republicans will have to address the elimination of the Affordable Care Act tax subsidies with health care premiums rising.
Millions of Americans are entering the new year with far more expensive health insurance premiums. WTOP’s Sarah Jacobs reports Maryland Rep. Glenn Ivey predicts a health care fix early in the new year.
With the expiration of the Affordable Care Act tax subsidies, millions of Americans are entering the new year with far more expensive health insurance premiums.
Maryland Rep. Glenn Ivey said he believes this issue has fractured the Republican coalition in Congress.
“The health care fight that came out of the government shutdown has been a real sign,” said Ivey, a Democrat who represents Maryland’s 4th District. “I think there’s a lot of cracks, not only in the Trump administration, but the Republican caucuses in the Senate and the House”
In December, four Republicans broke from House Speaker Mike Johnson and signed a petition, led by Democrats, that would force a House vote on extending an enhanced pandemic-era subsidy for three years that lowers health insurance.
It came in the aftermath of House Republican leaders rushing to pass a health care bill that didn’t address the rising monthly premiums.
“I think that Republicans have dug a very deep hole for themselves with the way they’ve mishandled Americans health care, especially with respect to their refusal to extend the tax credits for the Affordable Care Act so that people can afford to continue to have insurance,” Ivey said.
Ivey expects that Democrats will force Republicans to address the elimination of the Affordable Care Act tax subsidies in the next 30 days.
“I think we’re going to force them to do something to address the elimination of the Obamacare tax credits so that people don’t see their premiums double and triple,” Ivey said.
Ivey is also predicting Democrats will retake the House in 2026 and possibly the Senate.
“Because he can’t be counted on to do it himself, the only way to keep him in check is to have counterweights to him and Republicans in Congress are not willing to do it,” he said. “It’s got to be Democrats that do it.”
Democrats forced a 43-day government shutdown over the issue. Moderate Republicans called for a solution to save their 2026 political aspirations. President Trump floated a way out, only to back off after conservative backlash.
In the end, no one’s efforts were enough to save the subsidies before their expiration date. A House vote expected in January could offer another chance, but success is far from guaranteed.
The change affects a diverse cross-section of Americans who don’t get their health insurance from an employer and don’t qualify for Medicaid or Medicare — a group that includes many self-employed workers, small business owners, farmers and ranchers.
It comes at the start of a high-stakes midterm election year, with affordability — including the cost of health care — topping the list of voters’ concerns.
“It really bothers me that the middle class has moved from a squeeze to a full suffocation, and they continue to just pile on and leave it up to us,” said 37-year-old single mom Katelin Provost, whose health care costs are set to jump. “I’m incredibly disappointed that there hasn’t been more action.”
Subsidies helped reduce costs since pandemic
The expired subsidies were first given to Affordable Care Act enrollees in 2021 as a temporary measure to help Americans get through the COVID-19 pandemic. Democrats in power at the time extended them, moving the expiration date to the start of 2026.
With the expanded subsidies, some lower-income enrollees received health care with no premiums, and high earners paid no more than 8.5% of their income. Eligibility for middle-class earners was also expanded.
On average, the more than 20 million subsidized enrollees in the Affordable Care Act program are seeing their premium costs rise by 114% in 2026, according to an analysis by the health care research nonprofit KFF.
Those surging prices come alongside an overall increase in health costs in the U.S., which are further driving up out-of-pocket costs in many plans.
Some enrollees, like Salt Lake City freelance filmmaker and adjunct professor Stan Clawson, have absorbed the extra expense. Clawson said he was paying just under $350 a month for his premiums last year, a number that will jump to nearly $500 a month this year. It’s a strain for the 49-year-old but one he’s willing to take on because he needs health insurance as someone who lives with paralysis from a spinal cord injury.
Others, like Provost, are dealing with steeper hikes. The social worker’s monthly premium payment is increasing from $85 a month to nearly $750.
Lori Hunt of Des Moines, Iowa, spoke with CBS News during the congressional stalemate in October and said she “couldn’t afford” health insurance without the subsidies.
“I’d have to cancel my insurance,” Hunt said, joking that her insurance would consist of “thoughts and prayers.”
Hunt survived breast cancer three years ago and was laid off from her job in 2025. Without the subsidies, she expected her ACA premium would jump to about $700 per month. “It would be more than my mortgage payment,” Hunt said.
Many expected to go without coverage
Health analysts have predicted the expiration of the subsidies will drive many of the 24 million total Affordable Care Act enrollees — especially younger and healthier Americans — to forgo health insurance coverage altogether.
Over time, that could make the program more expensive for the older, sicker population that remains.
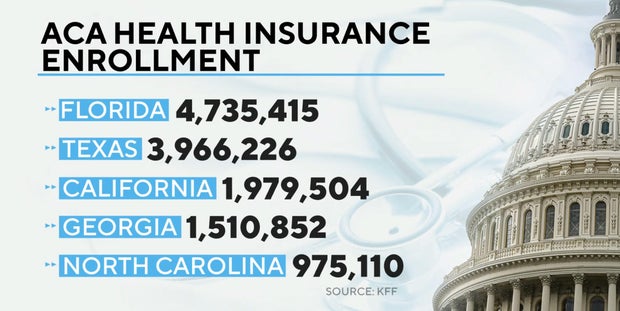
An analysis conducted last September by the Urban Institute and Commonwealth Fund projected the higher premiums from expiring subsidies would prompt some 4.8 million Americans to drop coverage in 2026.
The impact could be greatest in Florida, which has the largest number of ACA enrollees of any state — more than 4.7 million, according to KFF data. Texas is next, with more than 3.9 million, followed by California, Georgia and North Carolina.
KFF Data/CBS News
Kylie Barrios, a 30-year-old Florida resident, said she expected to be among those losing coverage.
“Our health insurance premium is effectively tripling from 2025 to 2026,” she told CBS News in December, saying it would rise from about $900 to $2,500.
Provost, the single mother, said she is holding out hope that Congress finds a way to revive the subsidies early in the year — but if not, she’ll drop herself off the insurance and keep it only for her 4-year-old daughter. She can’t afford to pay for both of their coverage at the current price.
But with the window to select and change plans still ongoing until Jan. 15 in most states, the final effect on enrollment is yet to be determined.
Last year, after Republicans cut more than $1 trillion in federal health care and food assistance with Mr. Trump’s big tax and spending cuts bill, Democrats repeatedly called for the subsidies to be extended. But while some Republicans in power acknowledged the issue needed to be addressed, they refused to put it to a vote until late in the year.
In December, the Senate rejected two partisan health care bills — a Democratic pitch to extend the subsidies for three more years and a Republican alternative that would instead provide Americans with health savings accounts.
In the House, four centrist Republicans broke with GOP leadership and joined forces with Democrats to force a vote that could come as soon as January on a three-year extension of the tax credits. But with the Senate already having rejected such a plan, it’s unclear whether it could get enough momentum to pass.
Meanwhile, Americans whose premiums are skyrocketing say lawmakers don’t understand what it’s really like to struggle to get by as health costs ratchet up with no relief.
Many say they want the subsidies restored alongside broader reforms to make health care more affordable for all Americans.
“Both Republicans and Democrats have been saying for years, oh, we need to fix it. Then do it,” said Chad Bruns, a 58-year-old Affordable Care Act enrollee in Wisconsin. “They need to get to the root cause, and no political party ever does that.”
Barrios, who said she has generally voted Republican, said she would like politicians to “act on those values that they … claim to protect.”
“The whole system feels as though it’s failed and isn’t advocating for me as a small business owner, as somebody who wants to become a mom and have a family,” she said.
First, why Germany is rearming, modernizing its military. Then, a look at life-saving drugs that cost millions per dose. And, Indiana Hoosiers: from outcast to undefeated.
But while every state applied for money from the Rural Health Transformation Program, it won’t be distributed equally. And critics worry that the funding might be pulled back if a state’s policies don’t match up with the administration’s.
Officials said the average award for 2026 is $200 million, and the fund puts a total of $50 billion into rural health programs over five years. States propose how to spend their awards, and the Centers for Medicare and Medicaid Services assigns project officers to support each state, said agency administrator Dr. Mehmet Oz.
“This fund was crafted as part of the One Big Beautiful Bill, signed only six months ago now into law, in order to push states to be creative,” Oz said in a call with reporters Monday.
Under the program, half of the money is equally distributed to each state. The other half is allocated based on a formula developed by CMS that considered rural population size, the financial health of a state’s medical facilities and health outcomes for a state’s population.
The formula also ties $12 billion of the five-year funding to whether states are implementing health policies prioritized by the Trump administration’s “Make America Healthy Again” initiative. Examples include requiring nutrition education for health care providers, having schools participate in the Presidential Fitness Test or banning the use of SNAP benefits for so-called junk foods, Oz said.
Several Republican-led states — including Arkansas, Iowa, Louisiana, Nebraska, Oklahoma and Texas — have already adopted rules banning the purchase of foods like candy and soda with SNAP benefits.
The money that the states get will be recalculated annually, Oz said, allowing the administration to “claw back” funds if, for example, state leaders don’t pass promised policies. Oz said the clawbacks are not punishments, but leverage governors can use to push policies by pointing to the potential loss of millions.
“I’ve already heard governors express that sentiment that this is not a threat, that this is actually an empowering element of the One Big Beautiful Bill,” he said.
Carrie Cochran-McClain, chief policy officer with the National Rural Health Association, said she’s heard from a number of Democratic-led states that refused to include such restrictions on SNAP benefits even though it could hurt their chance to get more money from the fund.
“It’s not where their state leadership is,” she said.
Experts say fund is inadequate in face of other cuts
Oz and other federal officials have touted the program as a 50% increase in Medicaid investments in rural health care. Rep. Don Bacon, a Republican from Nebraska who has been critical of many of the administration’s policies but voted for the budget bill that slashed Medicaid, pointed to the fund when recently questioned about how the cuts would hurt rural hospitals.
“That’s why we added a $50 billion rural hospital fund, to help any hospital that’s struggling,” Bacon said. “This money is meant to keep hospitals afloat.”
But experts say it won’t nearly offset the losses that struggling rural hospitals will face from the federal spending law’s $1.2 trillion cut from the federal budget over the next decade, primarily from Medicaid. Millions of people are also expected to lose Medicaid benefits.
Estimates suggest rural hospitals could lose around $137 billion over the next decade because of the budget measure. As many as 300 rural hospitals were at risk for closure because of the GOP’s spending package, according to an analysis by The Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill.
“When you put that up against the $50 billion for the Rural Health Transformation Fund, you know — that math does not add up,” Cochran-McClain said.
She also said there’s no guarantee that the funding will go to rural hospitals in need. For example, she noted, one state’s application included a proposal for healthier, locally sourced school lunch options in rural areas.
And even though innovation is a goal of the program, Cochran-McClain said it’s tough for rural hospitals to innovate when they were struggling to break even before Congress’ Medicaid cuts.
“We talk to rural providers every day that say, ‘I would really love to do x, y, z, but I’m concerned about, you know, meeting payroll at the end of the month,’” she said. “So when you’re in that kind of crisis mode, it is, I would argue, almost impossible to do true innovation.”
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Department of Science Education and the Robert Wood Johnson Foundation. The AP is solely responsible for all content.
[ad_2]
Devi Shastri and Margery A. Beck | The Associated Press
But while every state applied for money from the Rural Health Transformation Program, it won’t be distributed equally. And critics worry that the funding might be pulled back if a state’s policies don’t match up with the administration’s.
Officials said the average award for 2026 is $200 million, and the fund puts a total of $50 billion into rural health programs over five years. States propose how to spend their awards, and the Centers for Medicare and Medicaid Services assigns project officers to support each state, said agency administrator Dr. Mehmet Oz.
“This fund was crafted as part of the One Big Beautiful Bill, signed only six months ago now into law, in order to push states to be creative,” Oz said in a call with reporters Monday.
Under the program, half of the money is equally distributed to each state. The other half is allocated based on a formula developed by CMS that considered rural population size, the financial health of a state’s medical facilities and health outcomes for a state’s population.
The formula also ties $12 billion of the five-year funding to whether states are implementing health policies prioritized by the Trump administration’s “Make America Healthy Again” initiative. Examples include requiring nutrition education for health care providers, having schools participate in the Presidential Fitness Test or banning the use of SNAP benefits for so-called junk foods, Oz said.
Several Republican-led states — including Arkansas, Iowa, Louisiana, Nebraska, Oklahoma and Texas — have already adopted rules banning the purchase of foods like candy and soda with SNAP benefits.
The money that the states get will be recalculated annually, Oz said, allowing the administration to “claw back” funds if, for example, state leaders don’t pass promised policies. Oz said the clawbacks are not punishments, but leverage governors can use to push policies by pointing to the potential loss of millions.
“I’ve already heard governors express that sentiment that this is not a threat, that this is actually an empowering element of the One Big Beautiful Bill,” he said.
Carrie Cochran-McClain, chief policy officer with the National Rural Health Association, said she’s heard from a number of Democratic-led states that refused to include such restrictions on SNAP benefits even though it could hurt their chance to get more money from the fund.
“It’s not where their state leadership is,” she said.
Experts say fund is inadequate in face of other cuts
Oz and other federal officials have touted the program as a 50% increase in Medicaid investments in rural health care. Rep. Don Bacon, a Republican from Nebraska who has been critical of many of the administration’s policies but voted for the budget bill that slashed Medicaid, pointed to the fund when recently questioned about how the cuts would hurt rural hospitals.
“That’s why we added a $50 billion rural hospital fund, to help any hospital that’s struggling,” Bacon said. “This money is meant to keep hospitals afloat.”
But experts say it won’t nearly offset the losses that struggling rural hospitals will face from the federal spending law’s $1.2 trillion cut from the federal budget over the next decade, primarily from Medicaid. Millions of people are also expected to lose Medicaid benefits.
Estimates suggest rural hospitals could lose around $137 billion over the next decade because of the budget measure. As many as 300 rural hospitals were at risk for closure because of the GOP’s spending package, according to an analysis by The Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill.
“When you put that up against the $50 billion for the Rural Health Transformation Fund, you know — that math does not add up,” Cochran-McClain said.
She also said there’s no guarantee that the funding will go to rural hospitals in need. For example, she noted, one state’s application included a proposal for healthier, locally sourced school lunch options in rural areas.
And even though innovation is a goal of the program, Cochran-McClain said it’s tough for rural hospitals to innovate when they were struggling to break even before Congress’ Medicaid cuts.
“We talk to rural providers every day that say, ‘I would really love to do x, y, z, but I’m concerned about, you know, meeting payroll at the end of the month,’” she said. “So when you’re in that kind of crisis mode, it is, I would argue, almost impossible to do true innovation.”
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Department of Science Education and the Robert Wood Johnson Foundation. The AP is solely responsible for all content.
[ad_2]
Devi Shastri and Margery A. Beck | The Associated Press
At first, Everly Green’s parents didn’t understand why her doctors wanted genetic testing. Their daughter was behind on her milestones at 18 months, but was gradually making progress, and they expected that to continue.
Then, when she turned 2, the seizures started. She suddenly began to lose skills. Three months later, Everly needed a feeding tube. Now, at 8, she can only move her eyes, allowing her to communicate via a screen.
Everly, whose family lives in Fort Collins, has a rare mutation in a gene called FRRS1L, pronounced “frizzle,” which affects how cells in her brain communicate. Her parents, and other members of the tiny community of children with the condition, have worked with researchers and small-scale manufacturers to develop a treatment that could restore some of her ability to move — but only if they can raise $4 million to develop and test it.
Everly clearly understands what happens around her and loves school, where she learns in a mainstream classroom with support and has several best friends, said Chrissy Green, Everly’s mother. Still, she wants to do things she can’t, such as holding toys on her own or going on the occasional family trip with her brothers, Green said.
“These kids are in there, they want to play like other kids, they just can’t move,” she said.
Green is co-president of the foundation Finding Hope for FRRS1L, which is collecting funds for the next stage of drug development. Children with FRRS1L gene disorder, the foundation’s website says, “are trapped in a body they can’t move, however still retain high cognitive function, understanding, communication and awareness.”
Worldwide, only a few dozen children currently have a diagnosis of the same mutation in FRRS1L, meaning there’s little interest from drug companies. Families are on their own to fund research and, if all goes well, convince the U.S. Food and Drug Administration that the treatment is safe and effective enough to go on the market.
And, even if they succeed with the FDA, they’ll still face a battle with insurance companies that may not want to pay the steep price for a drug to correct a faulty gene. (Even though the families aren’t looking to make a profit, these types of treatments are expensive, and the company under contract to do the manufacturing isn’t doing it for free.)
Chrissy Green sits with her daughter Everly, 8, as her two boys Colton, 9, left, and Ryle, 4, play at their home in Fort Collins on Dec. 18, 2025. (Photo by RJ Sangosti/The Denver Post)
Normally, drug companies take on the financial risk of turning basic research that’s often publicly funded into treatments, with the hope of eventually making a profit. For gene therapies, that model can break down because of the small number of patients. Green’s FRRS1L foundation knows of about three dozen patients worldwide, though other children with unexplained seizures could have the mutation.
A drug that treats so few patients will never be profitable, so parents are largely on their own in trying to fund research and development, said Neil Hackett, a researcher who has worked with families on gene therapies and advised the FRRS1L foundation. Usually, they can’t do it unless they happen to have one or more business-savvy parents with the time and resources to run a foundation while caring for a child with complex needs, he said.
“They need specific expertise, which is not easy to find, and they need massive amounts of money,” he said.
Steve Green supports his daughter Everly’s head as the family plays with toys together at their home in Fort Collins on Dec. 18, 2025. (Photo by RJ Sangosti/The Denver Post)
When they first received Everly’s diagnosis, her doctor told the family to make the most of the time they had left, because medicine couldn’t offer anything to extend her life or reduce her symptoms, Green said. She didn’t initially question that, but focused on loving her daughter and trading tips for daily life with other families via Facebook.
Green connected with a mother in London who had a child the same age as Everly. Viviana Rodriguez was exploring whether researchers had found any evidence to suggest they could repurpose existing drugs to reduce FRRS1L symptoms.
Everly Green, 8, lies next to her mother, Chrissy Green, as she reads to her at their home in Fort Collins on Dec. 18, 2025. (Photo by RJ Sangosti/The Denver Post)
Through a “providential” series of events, one of Rodriguez’s contacts knew a doctor at the University of Texas Southwestern Medical Center who worked on gene therapies. That doctor had read a paper from a German researcher who bred mice with the FRSS1L mutation so he could study it. The German scientist had given the mice a gene therapy as part of his experiments, but his work wasn’t focused on the clinical applications, Green said.
Green and Rodriguez, along with a small group of other parents, formed the foundation to raise $400,000 for the UT Southwestern researchers to breed their own group of FRSS1L mice and give them a gene therapy in a study that was set up to show results. The mice that received the gene therapy had near-normal movement after it took effect, she said.
“We saw major recovery in the animals, so we’re really hopeful for our kids,” she said.
The next step was testing for toxic side effects, then finding a manufacturer who could do the complicated work of inserting the corrected gene into a harmless virus, Green said. If they can raise the necessary money and all goes as expected, children could receive their doses through a clinical trial starting in September, she said.
Colton Green, 9, pushes his sister Everly, 8, into the family’s living room at their home in Fort Collins on Dec. 18, 2025. (Photo by RJ Sangosti/The Denver Post)
Many treatments that look promising in mice don’t pan out in humans. Even if they do, foundations must navigate the complex process of getting permission from the FDA to sell the treatment, Hackett said. Then they face the separate battle of convincing insurance companies, or national health systems serving patients in other countries, that they should pay for it, he said.
Theoretically, a foundation could keep a treatment in reserve for patients diagnosed with the FRSS1L mutation in the future, but that likely isn’t feasible, Hackett said.
“At the end, I think you have to turn it over to a commercial entity, and I don’t think anyone knows what that looks like,” he said.
Green is hopeful, however, that the treatment she’s trying to fund will not only help children like Everly, but also ease the path for future gene therapies.
“All the diseases can kind of help each other move forward,” she said.
Chrissy Green lifts her daughter Everly, 8, out of bed at their home in Fort Collins on Dec. 18, 2025. (Photo by RJ Sangosti/The Denver Post)
BOSTON — More than a year after voters rejected a plan to legalize “magic” mushrooms, advocates have renewed the push on Beacon Hill for the use of psychedelic drugs again.
The Joint Committee on Public Health voted to advance bipartisan legislation that would decriminalize the drug for adults 21 and older for treatment of post-traumatic stress and other ailments for veterans, law enforcement officers or others who are “professionally diagnosed” with a “qualifying” condition.
This page requires Javascript.
Javascript is required for you to be able to read premium content. Please enable it in your browser settings.
BOSTON — Foreshadowing a legal challenge, Massachusetts Attorney General Campbell is joining a chorus of criticism over the Trump administration’s move to effectively ban gender-affirming care for minors at hospitals that depend on federal funding.
On Thursday, the U.S. Department of Health and Human Services and Centers for Medicare and Medicaid Services issued new regulations that would once finalized, restrict the use of puberty blockers, hormone therapy and surgical interventions for transgender children.
This page requires Javascript.
Javascript is required for you to be able to read premium content. Please enable it in your browser settings.
Congress has left for the year without reaching a health care deal, leaving Affordable Care Act subsidies that have helped lower insurance prices for roughly 22 million Americans to expire on Dec. 31 without taking action to address the surge in costs that is expected to follow.
As the end of the subsidies looms, families and individual Americans are bracing for immediate impacts. Monthly payments for millions of ACA marketplace enrollees are set to double or even triple without the tax credits that have made their premiums cheaper. The Congressional Budget Office has estimated that the lapse could leave roughly 4 million more Americans uninsured, with analysts warning of broader impacts over the coming years
The enhanced subsidies were introduced during the COVID-19 pandemic and extended by Democrats in 2022. For many lower-income Americans, they have resulted in free or nearly free coverage. For higher-earning recipients, they have dramatically reduced premiums. The lowered costs have contributed to a surge in enrollment, particularly among Americans in Republican-led Southern states, where coverage previously lagged.
Democrats have pushed for months to further extend the subsidies, making it a key demand in the spending standoff that shut down the government this fall. A group of Senate Democrats ultimately broke with the party to reopen the government on the condition that a vote on an extension measure would occur in December. But lawmakers have now left Washington without holding one.
Four swing-district House Republicans did defy party leadership and join a Democrat-led discharge petition to force a vote on a three-year extension in the chamber. Speaker Mike Johnson, who refused to bring the issue up for a vote before the holiday recess, will be required to do so after Congress reconvenes in the new year. The vote is expected the week of Jan. 5 when the House returns to session.
Even if the bill passes the House when it comes up for a vote next month, Senate Republicans are likely to block it, as they did in the case of a similar Democratic proposal earlier this month. But some lawmakers have expressed hope that it could help lawmakers move closer to passing a health care bill.
“I do believe if the bill comes to the floor, not only will it pass, but it’ll give the Senate the ability to come back with a bipartisan compromise and actually get something passed into law,” Rep. Mike Lawler of New York, one of the Republicans who signed on to the discharge petition, said Wednesday on NBC’s “Meet The Press Now.”
Republican Sen. Susan Collins of Maine told NBC News that the House passing the bill would “keep momentum going,” but declined to voice support for it.
“What we’re trying to do is to put together a bipartisan bill that would have reforms plus a two-year extension,” Collins said. “That is the best approach, in my opinion, and we’re making good progress.”
Appearing on ABC’s “This Week” with Jonathan Karl, House Minority Leader Hakeem Jeffries brushed off comments from Senate Majority Leader John Thune, who said a clean three-year extension would be dead on arrival in the Senate. Jeffries said Thune “is not serious about protecting the health care of the American people.”
“It will pass, with a bipartisan majority, and then that will put the pressure on John Thune and Senate Republicans to actually do the right thing by the American people: pass a straightforward extension of the Affordable Care Act tax credits so we can keep health care affordable for tens of millions of Americans who deserve to be able to go see a doctor when they need one,” Jeffries said.
Republican Sen. Rand Paul of Kentucky, meanwhile, said Sunday he remains opposed to extending the subsidies, instead promoting an alternative health care proposal centered on expanding Association Health Plans, which would allow consumers to band together to negotiate lower insurance premiums.
Paul, earlier this month, was the only Republican senator to vote against a GOP proposal to establish government-funded health savings accounts.
“We have health care in our country for poor people. It’s called Medicaid. All of the rest of the stuff has not worked,” Paul said in an interview with Jonathan Karl on ABC. “Obamacare has been a failure. President Obama said it would bring premiums down; premiums have gone through the roof. Every time we give more subsidies, the premiums go higher.”
A Republican proposal passed by the House on Wednesday, which does not include an extension of the subsidies, also appears unlikely to get traction in the Senate. “I would expect the vote count if it were just purely this wouldn’t be probably the same as it was last week,” Sen. Thom Tillis, a Republican of North Carolina, told NBC News, appearing to reference the failure of a separate GOP bill in the Senate.
In the meantime, subsidies are set to return to pre-pandemic levels before Congress returns, leaving millions to navigate sharp premium increases. And amid the anticipated price changes, the deadline for open enrollment on the ACA marketplace for the year is fast approaching on Jan. 15. Experts have suggested some options for Americans to consider as they look for ways to keep their coverage more affordable.
Each party has pointed fingers at the other for rising health care prices. On Wednesday, President Donald Trump delivered a 20-minute-long address in which he blamed Democrats for the high costs while claiming his administration’s policies offered relief. “It’s the Unaffordable Care Act,” he said. “The Democrats are responsible.”
Congressional Democrats, meanwhile, are placing blame on their Republican counterparts for failing to take action as the expiration date for the ACA subsidies approaches.
“Republicans still have a chance to lower costs on health care. But they still seem as determined not to as ever,” Democratic Sen. Elizabeth Warren of Massachusetts told Semafor.
Another deadline is also coming up in the new year: The short-term spending bill Congress passed in November, reopening the government, will only fund the government until Jan. 30, meaning it will once again shut down if lawmakers can’t reach a deal by that date.
Trump told a crowd of supporters at a rally in North Carolina on Friday that Democrats would again “close down the government,” accusing them of being “beholden” to insurance companies.
Senate Minority Leader Chuck Schumer, however, has insisted that Democrats will not link a spending bill to renewed subsidies in the new year.
Speaking to Punchbowl News,Schumer noted that the enhanced Obamacare subsidies will have expired by Jan. 30 and said Republicans have shown they are incapable of striking a bipartisan deal. He added that Democrats feel they have succeeded in making health care a top issue for voters next November.
“As of Jan. 1, that is a different time than before because the ACA [subsidies] expired,” Schumer said. “On the other hand, we’d like to get an appropriations bill done. That’s a Jan. 30 deadline … We’re trying to work with the Republicans to get it done.” “We’re working on appropriation bills to prevent another shutdown, now,” said Democrat Sen. Ben Ray Lujan of New Mexico, acknowledging the human stakes of legislative stalemate.“Let’s see what January brings. But people are hurting. Everything’s getting more expensive.”
Nancy Hunt arrived at an emergency room from a Genesis HealthCare nursing home in Pennsylvania in such dreadful shape, including maggots infesting her gangrened foot, that the hospital called an elder abuse hotline and then the police, her son alleged in a lawsuit.
Hunt died five days later. Her death certificate said the foot injury was a “significant” factor. Genesis denied wrongdoing but agreed to pay $3.5 million in a settlement Hunt’s son signed in August 2024.
Yet Genesis hasn’t paid most of that debt, court records show. It may never have to.
Once the nation’s largest nursing home chain, Genesis says it was spending $8 million a month defending and settling lawsuits over resident injuries and deaths in recent years. But the company is now poised to wipe the liability slate clean by seeking refuge in the most protective corner of the legal system for the nursing home industry: bankruptcy court.
The Genesis case, one of 11 large senior care bankruptcies this year, illustrates how health care companies can dodge public and financial accountability for alleged negligence through delays, confidentiality clauses, and bankruptcy maneuvers, a KFF Health News investigation found.
When it filed for bankruptcy in Dallas in July, Genesis estimated its total liability for nearly a thousand settled and pending lawsuits at $259 million. A KFF Health News review of the terms of 155 settlement agreements and corporate financial statements shows Genesis officials knew insolvency was possible yet included provisions in its settlement agreements allowing it to defer payment, often for a year or more.
As a result, Genesis paid nothing in 85 cases and only a portion in the other 70, according to civil court records and bankruptcy claims made available through people with access to them. It still owes $41 million of the $58 million it had agreed to pay in those cases, the records show.
“It just feels like they killed my mom and got away with it,” said Vanessa Betancourt, whose mother, Nellie Betancourt, a retired nurse, fractured her hip at a Genesis home in Albuquerque, New Mexico — an injury the medical examiner’s report said led to her death. Genesis agreed to a $650,000 settlement with Betancourt’s family in April under the condition it would not need to pay the first of seven installments for another year, according to the settlement document.
Gabe Betancourt holds an old photograph of his wife, Nellie, that he keeps in his wallet. (Adria Malcolm/KFF Health News/TNS)
Genesis HealthCare reached a $650,000 settlement with Nellie Betancourt’ s widower, Gabe Betancourt, and their daughter, Vanessa, in April after medical examiners said an injury Nellie sustained at a Genesis home in New Mexico led to her death. (Adria Malcolm/KFF Health News/TNS)
Genesis HealthCare reached a $650,000 settlement with Nellie Betancourt’s widower, Gabe Betancourt, and their daughter, Vanessa, in April after medical examiners said an injury Nellie sustained at a Genesis home in New Mexico led to her death. (Adria Malcolm/KFF Health News/TNS)
Nellie Betancourt, shown in a photo with her husband, Gabe, had planned a trip to Las Vegas before she fractured her hip at a Genesis HealthCare rehabilitation center— an injury the medical examiner’s report said led to her death.“ When she went into that place, I said,’ Well, she’ s going to be taken care of for a few more days and I’ ll take her home,’ “Gabe says. (Adria Malcolm/KFF Health News/TNS)
“It’ s almost two years now, ” Gabe Betancourt says of the death of his wife, Nellie.“ When you sleep with somebody for 67 years and you stretch your arm, she’s there. (Adria Malcolm/KFF Health News/TNS)
Nellie Betancourt, shown in a photo with her husband, Gabe, had planned a trip to Las Vegas before she fractured her hip at a Genesis HealthCare rehabilitation center— an injury the medical examiner’ s report said led to her death.“ When she went into that place, I said,‘ Well, she’ s going to be taken care of for a few more days and I’ll take her home,’ “Gabe says. (Adria Malcolm/KFF Health News/TNS)
Photographs of Nellie Betancourt and her family are displayed at Gabe Betancourt’s home in Albuquerque, New Mexico. (Adria Malcolm/KFF Health News/TNS)
1 of 7
Gabe Betancourt holds an old photograph of his wife, Nellie, that he keeps in his wallet. (Adria Malcolm/KFF Health News/TNS)
Genesis denied wrongdoing in all lawsuits and settlements. In a written statement, the company did not answer questions about individual personal injury cases. The statement said Genesis remained “focused on delivering high-quality, compassionate care to our patients and residents without disruption” during bankruptcy.
One lawsuit Genesis settled for nearly $1 million alleged nursing home managers ignored repeated warnings about a male resident’s behavior before he sexually assaulted a female Alzheimer’s patient, according to court records. In a case the company resolved for $500,000, a Genesis nursing home was accused of delaying the hospitalization of a resident who had vomited brown mucus. He died of a bowel obstruction. Genesis has paid nothing for either settlement, according to bankruptcy claims.
Creditors, including families of the deceased, are expected to salvage a fraction of what they were promised, if anything. On Dec. 10, the company’s owners were scheduled to seek approval by the U.S. Bankruptcy Court for the Northern District of Texas to sell its nursing homes and other assets to its largest investor, a private equity firm. In court papers, lawyers for residents and other creditors say the complex plan will prevent them from pursuing Genesis’ new ownership and other companies they blame for the company’s collapse.
John Anthony, a bankruptcy attorney representing 340 personal injury claims against Genesis, said, “They never had any intention to honor these deals.”
Low Ratings and Fines
During years of financial turmoil, Genesis has frequently struggled to provide top-notch care, federal records show. Using its five-star system, the Centers for Medicare & Medicaid Services rated 58% of homes affiliated with Genesis as below average or much below average. CMS has fined Genesis homes $10 million for violating federal health standards over the past three years.
In its Chapter 11 filing, Genesis said it cared for about 15,000 residents in 165 nursing homes and 10 assisted living facilities in 18 states. They are centered in Pennsylvania, West Virginia, New Mexico, New Hampshire, New Jersey, Maine, Alabama, Maryland, and North Carolina, according to the bankruptcy filing.
The company said it owed $709 million in secured debt to lenders and the IRS. Under bankruptcy rules, those debts, backed by Genesis collateral, take precedence over the $1.6 billion in unsecured debt Genesis said it owes. Unsecured creditors include a pension fund; contractors that provided health services and equipment; Pennsylvania, New Mexico, and West Virginia for unpaid provider taxes; and former residents and their families who sued.
Dangers in Memory Care
Sandia Ridge Center, a Genesis home in Albuquerque, was repeatedly faulted by health regulators for not preventing sexual misbehavior in its memory care unit. In November 2021, CMS cited the home for lacking enough nurses to prevent sexual abuse among residents. An inspection report the following August identified more inappropriate sexual contact. Police were called to investigate sexual assault allegations in February and March of 2023, police reports show; neither resulted in criminal charges.
Then in April 2023, a 61-year-old male resident with alcohol-related dementia sexually assaulted a female resident with Alzheimer’s in the dining room, according to a police report and an inspection report. When the resident screamed for him to stop and that he was hurting her, he responded “shut up bitch I know you like this,” according to a lawsuit brought on behalf of the woman, identified in court papers as R.S.
Sandia Ridge management had been aware of the male resident’s behavioral issues for months, according to employee depositions in the case. Police had investigated a prior sexual assault allegation against him the previous year without bringing charges. In one deposition, a former activities assistant testified he hit her and twice pushed her into a bathroom while announcing, “I want to have sex with you.” When she reported him to a senior Genesis manager, she said in the deposition, the manager put his finger over his lips and said, “Shhh.”
The activities worker testified that R.S. used to happily sing along with Elvis Presley songs. After the assault, the worker said, R.S. “don’t sing anymore.”
Inspectors cited the home for failing to protect R.S. The same report said the home didn’t provide a therapist for another female resident who was being sexually harassed. Medicare fined Sandia Ridge Center $91,247. Genesis denied liability but settled R.S.’ lawsuit for $925,000 in May, according to the bankruptcy claim.
“We just felt we have to hold them accountable,” R.S.’ daughter said in an interview, speaking on the condition that she and her mother not be identified, because of the nature of the assault. “Maybe I’m wrong, maybe I’m naive, but the only way to do that is to sue someone, right?”
Genesis has not paid any of the settlement, according to the family’s claim filing.
Growth and Debt
Genesis’ downfall can be traced to 2007, when affiliates of two private equity firms acquired the company in a $1.5 billion leveraged buyout, taking on substantial debt, according to its bankruptcy filing. Private equity also has been involved in other health care bankruptcies, including those of the HCR ManorCare nursing home chain, the prison health care contractor Corizon Health, and two for-profit hospital systems, Steward Health Care and Prospect Medical Holdings.
In 2011, Genesis raised $2.4 billion by transferring substantially all its nursing home buildings and other real estate to Welltower, a publicly traded real estate investment trust, according to Genesis’ bankruptcy filing. Genesis then rented the buildings back from Welltower, which made leasing costs a significant expense.
Genesis went on a nationwide buying spree. At its peak in 2016, it had grown to more than 500 nursing homes. In a court declaration, Louis Robichaux IV, a consultant overseeing Genesis’ bankruptcy restructuring, wrote that as the company expanded, it became harder to manage and “mired in corporate inefficiencies.” Robichaux wrote that Genesis’ financial woes were exacerbated by rapidly increasing labor costs and lawsuits, including some predating the covid pandemic.
But Genesis continued to teeter on the edge of insolvency. In audited financial statements for 2022 and 2023 submitted to a California oversight agency, management and auditors said rent and debt obligations raised “substantial doubt about the company’s ability to continue as a going concern.”
In a court filing, a committee appointed by the U.S. Trustee’s Office to represent the unsecured creditors in the bankruptcy accused Landau and Welltower of orchestrating a covert plan that allowed Welltower to keep getting its rents while Landau could run the company and “siphon value to himself.” The committee alleged their efforts forced the company into insolvency while “staffing levels and patient care declined precipitously.” Landau and Welltower did not respond to requests for comment.
Staff at a Genesis HealthCare nursing home delayed hospitalizing James Sanderson, seen here with daughter Erin Pearson, for a week after he showed symptoms of a bowel obstruction, according to a lawsuit. (Courtesy Erin S. Pearson/KFF Health News/TNS)
Drawn-Out Lawsuits
Erin Pearson sued Genesis over the death of her father, James Sanderson, a retired mining company executive who died in 2018 after spending less than a month at Bear Canyon Rehabilitation Center in Albuquerque. In the memory care unit, Sanderson fell repeatedly, suffered medication errors made by nursing home staff, and developed a bowel obstruction and sepsis, according to the lawsuit, filed in 2019. Pearson’s lawyers said he was not hospitalized until eight days after nurses noticed he was vomiting brown mucus.
After the judge rejected Genesis’ request to force Pearson into arbitration, Genesis appealed. It took 2½ years before an appeals court affirmed the original decision to let the case go forward in court, records show.
This past May, more than five years after suing, Pearson reached a $500,000 settlement, with the first payment required by November, according to a copy of the agreement. Nothing was paid, according to the bankruptcy claim.
“It was so drawn out and for so long,” Pearson said in an interview, calling Genesis’ bankruptcy “despicable.”
Genesis HealthCare settlements included periodic payment plans, like this one from a $600,000 settlement in February 2025, included in a court record, that allowed the company to delay paying for a year or more. (Jordan Rau/KFF Health News/TNS)
Payouts Postponed
Jennifer Foote, an Albuquerque attorney who represents clients in multiple lawsuits against Genesis, including Pearson’s, said the company frequently filed appeals. “They did not usually win them on these issues,” she said, “and our sense was that they were doing it as a delay tactic.”
Genesis started using installment payments around 2018, said Dusti Harvey, Foote’s law partner. “The payments wouldn’t start for several months out,” Harvey said. Foote said Genesis’ lawyers often wanted to time the payments to start the month the trial in the case was scheduled to occur.
Families had to wait even when comparatively small amounts of money were involved, settlement agreements show. Genesis’ settlement agreements also included a confidentiality clause prohibiting discussion of the incidents.
Genesis agreed to pay $42,000 in a November 2024 settlement, but the first payment was not due until nine months later. It was not paid, according to the bankruptcy claim.
A $250,000 settlement signed in October 2023 did not start paying out until the following September. When Genesis declared bankruptcy — 21 months after the case was resolved — it still owed $100,000, according to the family’s claim.
Genesis HealthCare still owes $112,500 from a $950,000 settlement over the death of Margarett Johnson after an accident in a Maryland nursing home, according to a bankruptcy claim. (Angela Swann/KFF Health News/TNS)
‘We Never Found Out the Truth’
Settling cases allowed Genesis to avoid the expense and publicity of a trial, at which details of how its nursing homes functioned might have been revealed. In October 2020, Margarett Johnson, a retired school bus driver, fell out of her wheelchair at a Genesis nursing home in Waldorf, Maryland, fracturing her jawbone, nose, and neck, according to a lawsuit brought by her family. Johnson was sent to a trauma center and placed on a ventilator. She died three months later, at age 76, from ventilator-associated pneumonia, the lawsuit said.
“It looked like she was hit by a truck,” Angelina Harley, one of her daughters, said in an interview. “I knew my mom was not going to come home. I knew the Lord was not going to punish her more.”
The company denied negligence and blamed the accident on Johnson’s jacket getting tangled in the wheel of her wheelchair, according to the lawsuit. Harley and her sister Angela Swann were dubious.
“We never found out the truth,” Harley said. “They wanted to settle out of court.”
The company denied liability but agreed to a $950,000 settlement in October 2024. It never paid the final $112,500 installment, according to a letter Johnson’s five children sent to the bankruptcy judge.
“If you settle out of court, you know doggone well you did something wrong,” Harley said.
Maddening Judges
By summer 2025, judges in some civil cases had run out of patience.
Alma Brown, a retired day care manager and accordion teacher living in a Genesis nursing home in Clovis, New Mexico, suffered falls, infections, bedsores, and other neglect that hastened her death in 2023, according to her estate’s lawsuit. In Santa Fe District Court, Judge Kathleen McGarry Ellenwood castigated Genesis after it failed to pay $2 million of the $3 million settlement to Brown’s estate or explain the delay.
Genesis “obviously benefited by not having to go to trial,” McGarry Ellenwood said in one hearing, according to a court transcript. “They assure me that they’re not trying to renege on their contract, but it certainly seems like they haven’t lived up to what the bargain was.”
Genesis declared bankruptcy the day McGarry Ellenwood announced she would impose more than $100,000 in fines, plus $10,000 more each day until the settlement was paid.
In Pennsylvania, Greg Hunt petitioned a judge to punish Genesis after it stopped payments of the $3.5 million settlement after the death of his mother, Nancy, the resident with the gangrenous foot. She had spent eight months in 2019 at Brandywine Hall, a Genesis facility in West Chester that was later sold and renamed.
In a filing with the Common Pleas Court of Montgomery County, Genesis admitted it was in arrears but asked the judge for more time, citing “unforeseen and exigent financial challenges.” Genesis said care for patients at its nursing homes would suffer if it had to pay immediately.
Unswayed, Judge Richard Haaz in June ordered Genesis to pay up, along with punitive interest. But the bankruptcy court stayed that order. Genesis still owes $1.4 million of the $2 million it was supposed to pay, according to Hunt’s claim. (The rest of the $3.5 million settlement is supposed to be paid by an insurer in January 2026.) Ian Norris, Hunt’s lawyer, declined to comment, citing confidentiality provisions in the settlement.
Court records indicate Genesis lawyers never disclosed in either case that it was preparing to declare bankruptcy.
Uptown Rehabilitation Center in Albuquerque, New Mexico, is one of 165 nursing homes Genesis HealthCare owns in the U.S.. (Adria Malcolm/KFF Health News/TNS)
‘Bankruptcy as a Tool’
In the first nine months of 2025, 10 other senior living companies with liabilities over $10 million entered Chapter 11 bankruptcy, according to Gibbins Advisors, a consulting firm.
Hamid Rafatjoo, a bankruptcy lawyer representing nursing homes who is not involved in the Genesis bankruptcy case, said filings may increase as the industry has become costlier to run and class action lawsuits have become a fixture.
“Nursing homes get sued all the time for everything,” Rafatjoo said. “A lot of operators wait too long to use bankruptcy as a tool.”
On Dec. 1, Genesis announced the results of its auction, saying it had elected to sell its assets to a private equity firm controlled by Landau. In a court filing, Anthony, the attorney for the personal injury claimants, alleged the auction was stacked in Landau’s favor despite an “objectively better and higher competing bid” from another private equity investor that would have provided more money to creditors. Genesis said in its statement that Landau’s group had increased its bid during the auction.
Sen. Elizabeth Warren, D-Mass., and two other senators last month asked the U.S. Trustee’s Office to intervene in the case, out of concern that “individuals who already own or control Genesis are trying to sell it to themselves, wiping away legal and other creditor debts in the process.” Lawyers representing those in charge of the auction did not respond to a request for comment.
Families of former Genesis residents said they fear the capacity to purge lawsuits through bankruptcy emboldens nursing home owners who provide deficient care.
“They can file bankruptcy again,” said Gabe Betancourt, whose wife, Nellie, died after her stay at Uptown Rehabilitation Center in Albuquerque. “And we’re the ones that will pay for it, with our memories, our lives.”
Millions of Americans are bracing for higher health costs in 2026, as subsidies that help them pay for health insurance under the Affordable Care Act are set to expire on December 31.
Experts warn that a failure in Congress to extend the tax credits could be financially devastating for individual policyholders, while also raising health care costs as a whole. Roughly 22 million Americans receive the ACA subsidies, which were created in 2021 to lower households’ monthly premiums.
New data from investment adviser SmartAsset projects how much people around the U.S. with an ACA plan would have paid on average for coverage in 2025 if they hadn’t received the enhanced subsidies. As the analysis shows, monthly premiums for the government health insurance would’ve been hundreds of dollars higher.
In Mississippi, where around 11% of residents are enrolled in an ACA plan, participants would have seen their average monthly premiums jump from $41 to $605, a 1,376% increase, SmartAsset found. In West Virginia, enrollees’ premiums would have risen an average of 1,058%.
A spokesperson for SmartAsset said the analysis captures 2025 costs, but noted the data amounts to a “close approximation” of how much more people with ACA coverage could expect to pay next year without the tax credits.
SmartAsset used public records from the Centers for Medicare and Medicaid Services’ 2025 Marketplace Open Enrollment Period to calculate the average cost of ACA plans.
The exact price hikes people could see next will depend on a range of factors, including their insurance plan, age, household income, health status and where they live, according to a spokesperson from KFF. The health policy group estimates that annual out-of-pocket premium costs will increase 114% on average for the 22 million ACA enrollees who rely on the subsidies.
What is the status of the ACA tax credits?
The tax credits are set to lapse at the end of the year. Democratic lawmakers have pushed for an extension but lack enough support in the Republican-led Congress. And while the House passed a health care bill this week that includes several policies favored by Republicans, it excludes an extension of the tax credits and faces hurdles in the Senate.
Both chambers of Congress have left Washington until early next year, making it all but certain that the tax credits will expire on December 31. But four GOP members this week signed a Democratic measure to force a vote on extending the subsidies for three years, teeing up a final vote early next year.
If Congress fails to solve the tax credit issue, some enrollees will qualify for a smaller subsidy, while others could lose eligibility completely, according to KFF.
With sharply higher ACA costs on the horizon, the Congressional Budget Office estimates that about 4 million people could drop their health insurance altogether. Experts say that could lead to higher costs for people with other types of health insurance because hospitals will have to provide more uncompensated care for those lacking coverage.
“Hospitals can only reconcile that by raising their prices for everybody,” Emma Wager, a senior policy analyst at KFF, told CBS News last week.