[ad_1]
More than half of irritable bowel syndrome (IBS) sufferers appear to have a form of atypical food allergy.
A chronic gastrointestinal disorder, irritable bowel syndrome affects about one in ten people. You may have heard about low-FODMAP diets, but they don’t appear to work any better than the standard advice to avoid things like coffee or spicy and fatty foods. In fact, you can hardly tell which is which, as shown below and at 0:27 in my video Friday Favorites: Fasting for Irritable Bowel Syndrome.
Most IBS patients, however, do seem to react to specific foods, such as eggs, wheat, dairy, or soy sauce, but when they’re tested with skin prick tests for typical food allergies, they may come up negative. We want to know what happens inside their gut when they eat those things, though, not what happens on their skin. Enter confocal laser endomicroscopy.
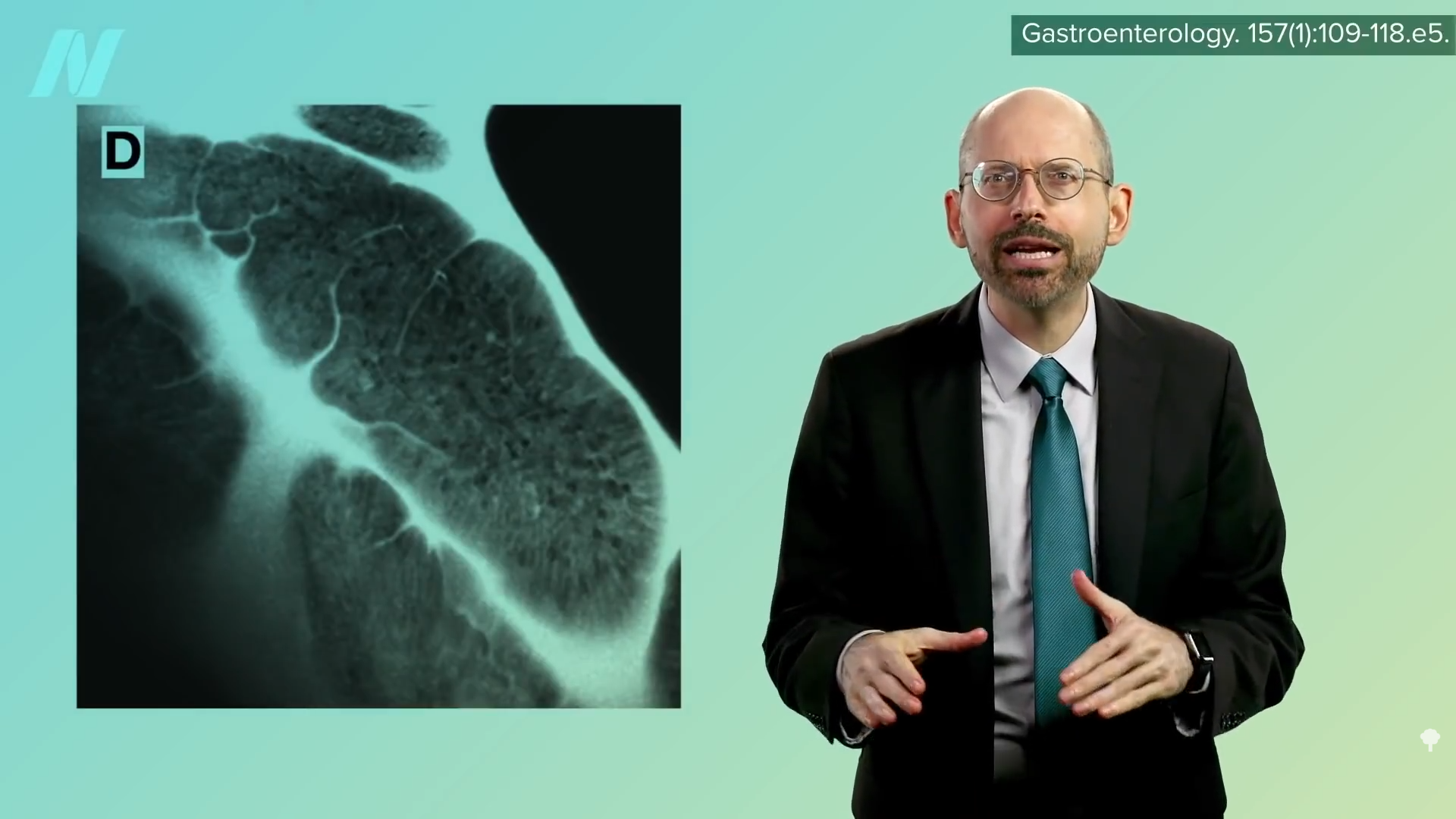
You can snake a microscope down the throat, into the gut, and watch in real-time as the gut wall becomes inflamed and leaky after foods are dripped in. Isn’t that fascinating? You can actually see cracks forming within minutes, as shown below and at 1:03 in my video. This had never been tested on a large group of IBS patients, though, until now.
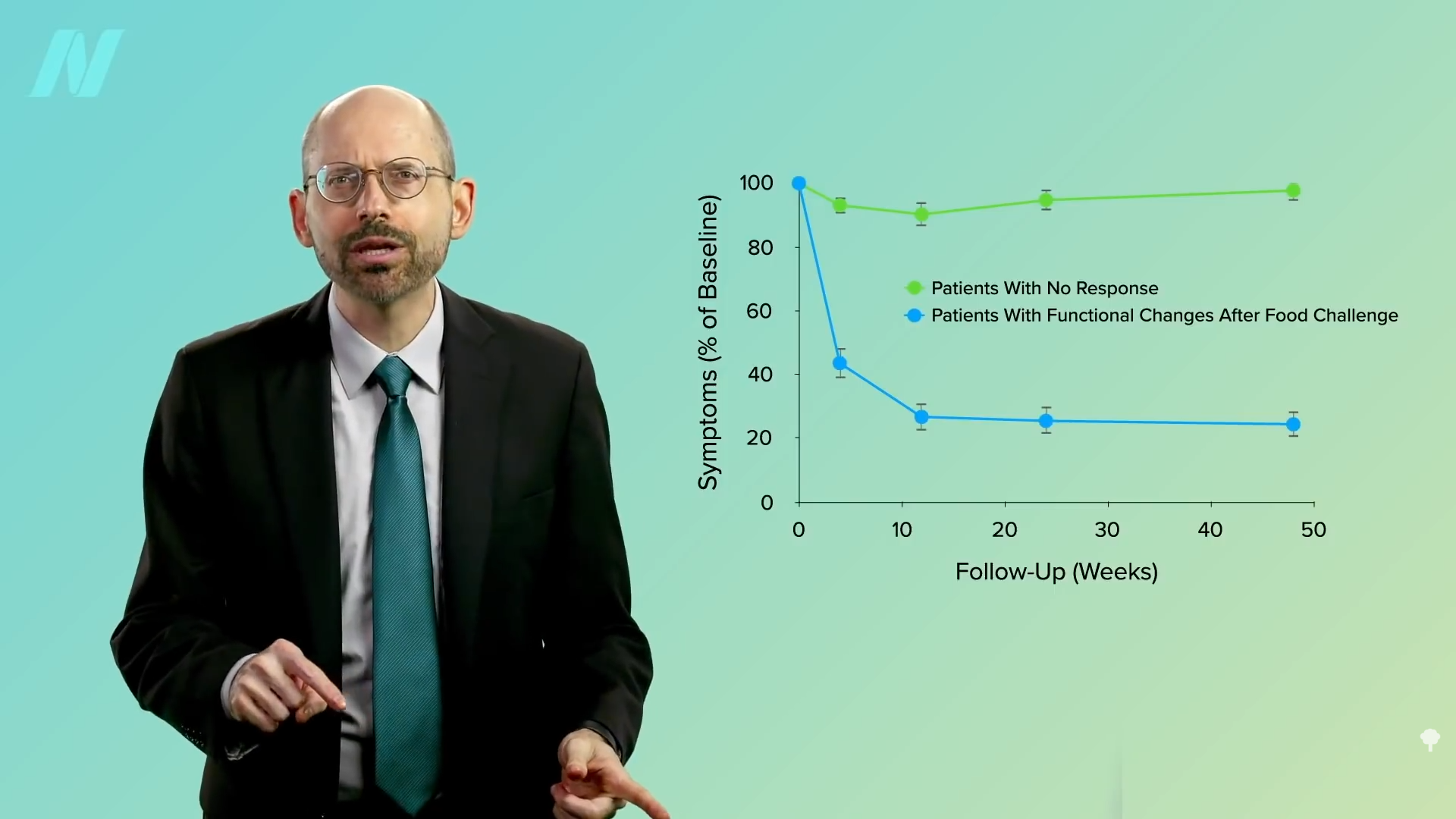
Using this new technology, researchers found that more than half of IBS sufferers have this kind of reaction to various foods—“an atypical food allergy” that flies under the radar of traditional allergy tests. As you can see below and at 1:28 in my video, when you exclude those foods from the diet, there is a significant alleviation of symptoms.
However, outside a research setting, there’s no way to know which foods are the culprit without trying an exclusion diet, and there’s no greater exclusion diet than excluding everything. A 25-year-old woman had complained of abdominal pain, bloating, and diarrhea for a year, and drugs didn’t seem to help. But, after fasting for ten days, her symptoms improved considerably and appeared to stay that way at least 18 months later. It wasn’t just subjective improvement either. Biopsies were taken that showed the inflammation had gone down, her bowel irritability was measured directly, and expanding balloons and electrodes were inserted in her rectum to measure changes in her sensitivity to pressure and electrical stimulation. Fasting seemed to reboot her gut in a way, but just because it worked for her doesn’t mean it works for others. Case reports are most useful when they inspire researchers to put them to the test.
“Despite research efforts to develop a cure for IBS, medical treatment for this condition is still unsatisfactory.” We can try to suppress the symptoms with drugs, but what do we do when even that doesn’t work? In a study of 84 IBS patients, 58 of whom failed basic treatment (consisting of pharmacotherapy and brief psychotherapy), 36 of the 58 who were still suffering underwent ten days of fasting, whereas the other 22 stuck with the basic treatment. The findings? Those in the fasting group experienced significant improvements in abdominal pain, bloating, diarrhea, loss of appetite, nausea, anxiety, and interference with life in general, which were significantly better than those of the control group. The researchers concluded that fasting therapy “could be useful for treating moderate to severe patients with IBS.”
Unfortunately, patient allocation was neither blinded nor randomized in the study, so the comparison to the control group doesn’t mean much. They were also given vitamins B1 and C via IV, which seems typical of Japanese fasting trials, even though one would not expect vitamin-deficiency syndromes—beriberi or scurvy—to present within just ten days of fasting. The study participants were also isolated; might that make the psychotherapy work better? It’s hard to tease out just the fasting effects.
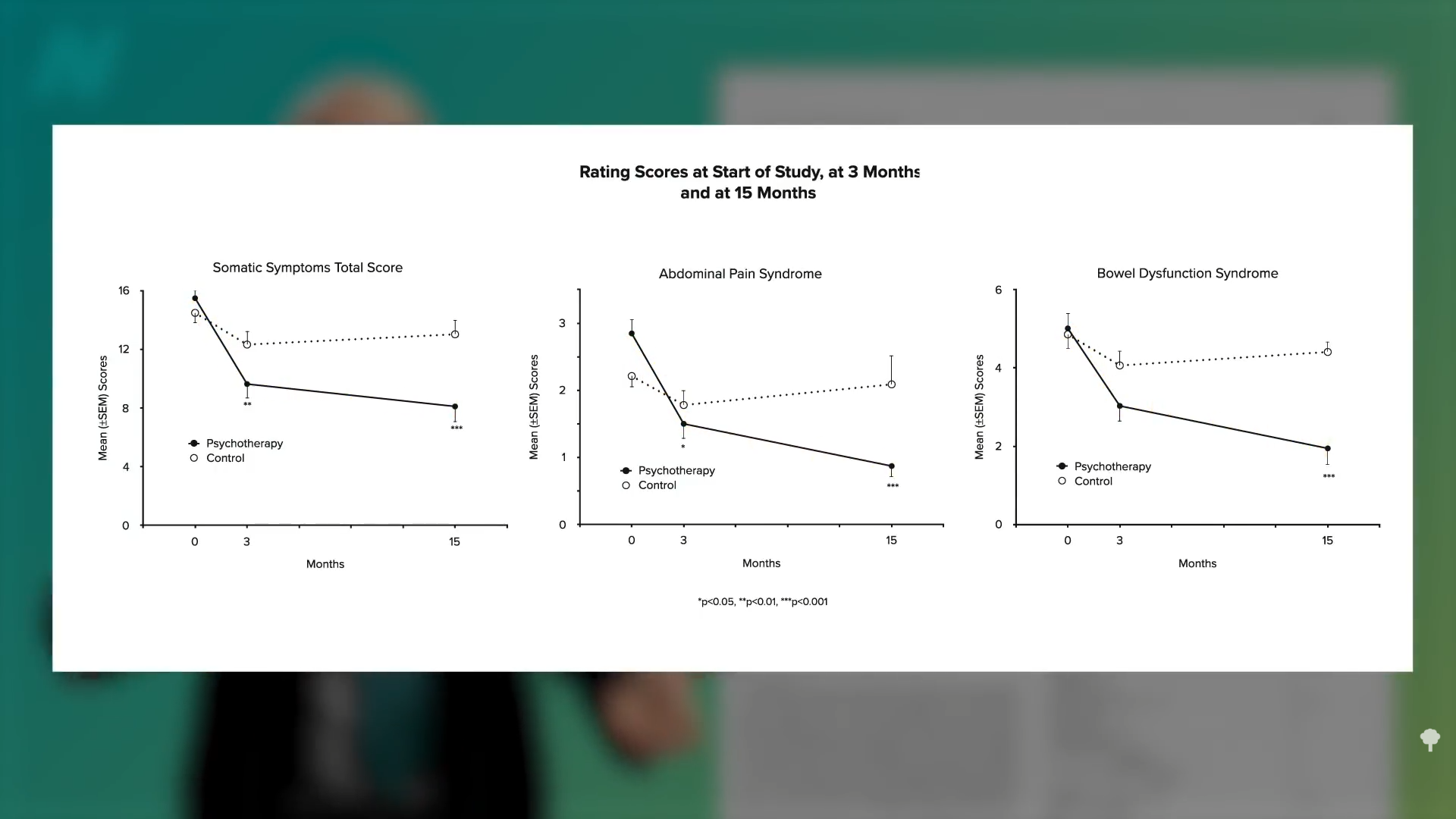
Psychotherapy alone can provide lasting benefits. Researchers randomized 101 outpatients with irritable bowel syndrome to medical treatment or medical treatment with three months of psychotherapy. After three months, the psychotherapy group did better, and the difference was even more pronounced a year later, a year after the psychotherapy ended. Better at three months, and even better at 15 months, as you can see here and at 3:58 in my video.
Psychological approaches appear to work about as well as antidepressant drugs for IBS, but the placebo response for IBS is on the order of 40%, whether psychological interventions, drugs, or alternative medicine approaches. So, doing essentially nothing—taking a sugar pill—improves symptoms 40% of the time. In that case, I figure one might as well choose a therapy that’s cheap, safe, simple, and free of side effects, which extended fasting is most certainly not. But, if all else fails, it may be worth exploring fasting under close physician supervision.
All my fasting videos are available in a digital download here.
Check the videos on the topic that are already on the site here.
For more on IBS, see related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link