[ad_1]
[ad_2]
AggregatedNews
Source link

[ad_1]
[ad_2]
AggregatedNews
Source link

[ad_1]
Rather than being some kind of disorder or a failure of willpower, weight gain is largely a normal response by normal people to an abnormal situation.
It’s been said that “Nothing in biology makes sense except in the light of evolution.” The known genetic contribution to obesity may be small, but, in a certain sense, you could argue that it’s all in our genes. The excess consumption of available calories may be hardwired into our DNA. We were born to eat.
Throughout human history and beyond, we existed in survival mode—in unpredictable scarcity. We’ve been programmed with a powerful drive to eat as much as we can while we can and just store the rest for later. Food availability could never be taken for granted, so those who ate more at the moment and were best able to store more fat for the future might better survive subsequent shortages to pass along their genes. So, generation after generation, millennia after millennia, those with lesser appetites may have died out, while those who gorged may have selectively lived long enough to pass along their genetic predisposition to eat and store more calories. That may be how we evolved into such voracious calorie-conserving machines. Now that we’re no longer living in such lean times, though, we’re no longer so lean ourselves.
What I just described is the “thrifty gene” concept proposed in 1962. As I discuss in my video The Thrifty Gene Theory: Survival of the Fattest, it suggests that obesity is the result of a “‘mismatch’ between the environment in which humans evolved and our modern environment”—like being a polar bear in a jungle. All that fur and fat may have given polar bears an edge in the Arctic but would be decidedly disadvantageous in the Congo. Similarly, a propensity to pack on the pounds may have been a plus in prehistoric times but can turn into a liability when our scarcity-sculpted biology is plopped down into the land of plenty. So, it’s not gluttony or sloth. Obesity may simply be “a normal response to an abnormal environment.”
Much of our physiology is finely tuned to stay within a narrow range of upper and lower limits. If we get too hot, we sweat; if we get too cold, we shiver. Our body has mechanisms to keep us in balance. In contrast, our bodies have had little reason to develop an upper limit to the accumulation of body fat. In the beginning, there may have been evolutionary pressures to keep lithe and nimble in the face of predation, but thanks to things like weapons and fire, we haven’t had to outrun as many saber-toothed tigers for about two million years or so. This may have left our genes with the one-sided selection pressures to binge on every morsel in sight and stockpile as many calories as possible in our bodies.
What was once adaptive is now a problem—or at least so says the thrifty gene hypothesis that originated more than half a century ago. It “provides a simple and elegant explanation for the modern obesity epidemic and was quickly embraced by scientists and lay people alike.” Although the researcher, James Neel, later distanced himself from the original proposal, the basic premise, despite remaining mostly theoretical, is still “largely accepted” by the scientific community, and the implications are profound.
In 2013, the American Medical Association voted to classify obesity as a disease (going against the advice of its own Council on Science and Public Health). Not that it necessarily matters what we call it, but disease implies dysfunction. Bariatric drugs and surgery are not correcting an anomaly in human physiology. Our bodies are just doing what they were designed to do in the face of excess calories. Rather than being some sort of disorder, weight gain is largely “a normal response by normal people to an abnormal environment.” As you can see below and at 4:12 in my video, more than 70 percent of Americans are now overweight. It’s normal.
“A body gaining weight when excess calories are available for consumption is behaving normally. Efforts to curtail such weight gain with drugs [or surgery] are not efforts to correct an anomaly in human physiology, but rather to deconstruct and reconstruct its normal operations at the core.”
If weight gain is largely a normal response by normal people to an abnormal situation, what exactly is that abnormal situation? Calorie-Rich-And-Processed Foods. (I’ll let you work out the acronym.) That’s the topic we’ll turn to next.
This is the third in an 11-video series on the history of the obesity epidemic. If you missed the first two, see The Role of Diet vs. Exercise in the Obesity Epidemic and The Role of Genes in the Obesity Epidemic.
There are eight more coming up. See the related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
The “fat gene” accounts for less than 1 percent of the differences in size between people.
To date, about a hundred genetic markers have been linked to obesity, but when you put them all together, overall, they account for less than 3 percent of the difference in body mass index (BMI) between people. You may have heard about the “fat gene,” called FTO, short for FaT mass and Obesity-associated). It’s the gene most strongly linked to obesity, but it explains less than 1 percent of the difference in BMI between people, a mere 0.34 percent.
As I discuss in my video The Role of Genes in the Obesity Epidemic, FTO codes for a brain protein that appears to affect our appetite. Are you one of the billion people who carry the FTO susceptibility genes? It doesn’t matter because it only appears to result in a difference in intake of a few hundred extra calories a year. The energy imbalance that led to the obesity epidemic is on the order of hundreds of calories a day, and that’s the gene known so far to have the most effect. The chances of accurately predicting obesity risk based on FTO status is “only slightly better than tossing a coin.” In other words, no, those genes don’t make you look fat.
When it comes to obesity, the power of our genes is nothing compared to the power of our fork. Even the small influence the FTO gene does have appears to be weaker among those who are physically active and may be abolished completely in those eating healthier diets. FTO only appears to affect those eating diets higher in saturated fat, which is predominantly found in meat, dairy, and junk food. Those eating more healthfully appear to be at no greater risk of weight gain, even if they inherited the “fat gene” from both of their parents.
Physiologically, FTO gene status does not appear to affect our ability to lose weight. Psychologically, knowing we’re at increased genetic risk for obesity may motivate some people to eat and live more healthfully, but it may cause others to fatalistically throw their hands up in the air and resign themselves to thinking that it just runs in their family, as you can see in the graph below and at 2:11 in my video. Obesity does tend to run in families, but so do lousy diets.
Comparing the weight of biological versus adopted children can help tease out the contributions of lifestyles versus genetics. Children growing up with two overweight biological parents were found to be 27 percent more likely to be overweight themselves, whereas adopted children placed in a home with two overweight parents were 21 percent more likely to be overweight. So, genetics do play a role, but this suggests that it’s more the children’s environment than their DNA.
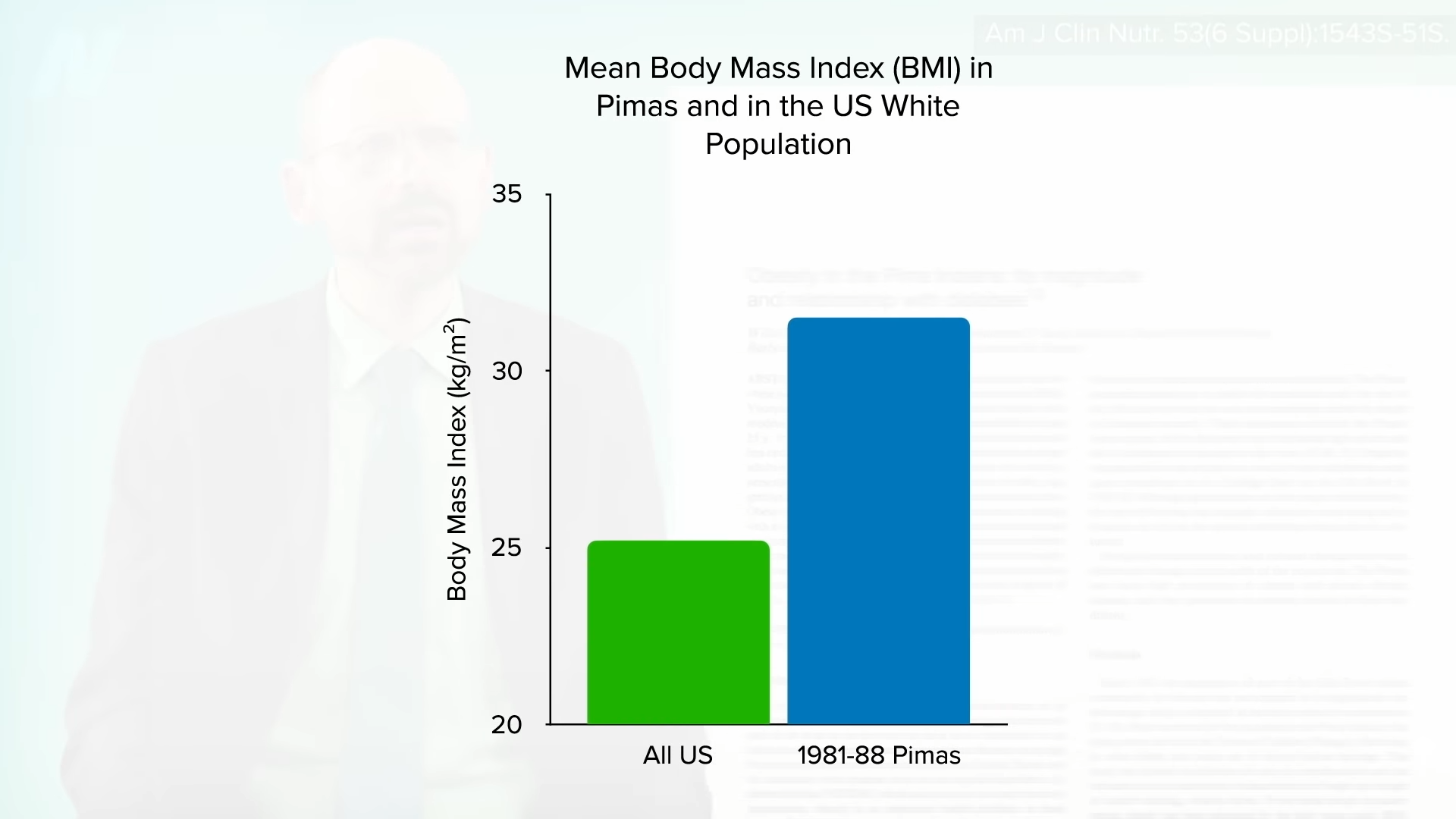
One of the most dramatic examples of the power of diet over DNA comes from the Pima Indians of Arizona. As you can see in the graph below and at 3:05 in my video, they not only have among the highest rates of obesity, but they also have the highest rates of diabetes in the world. This has been ascribed to their relatively fuel-efficient genetic makeup. Their propensity to store calories may have served them well in times of scarcity when they were living off of corn, beans, and squash, but when the area became “settled,” their source of water, the Gila River, was diverted upstream. Those who survived the ensuing famine had to abandon their traditional diet to live off of government food programs and chronic disease rates skyrocketed. Same genes, but different diet, different result.
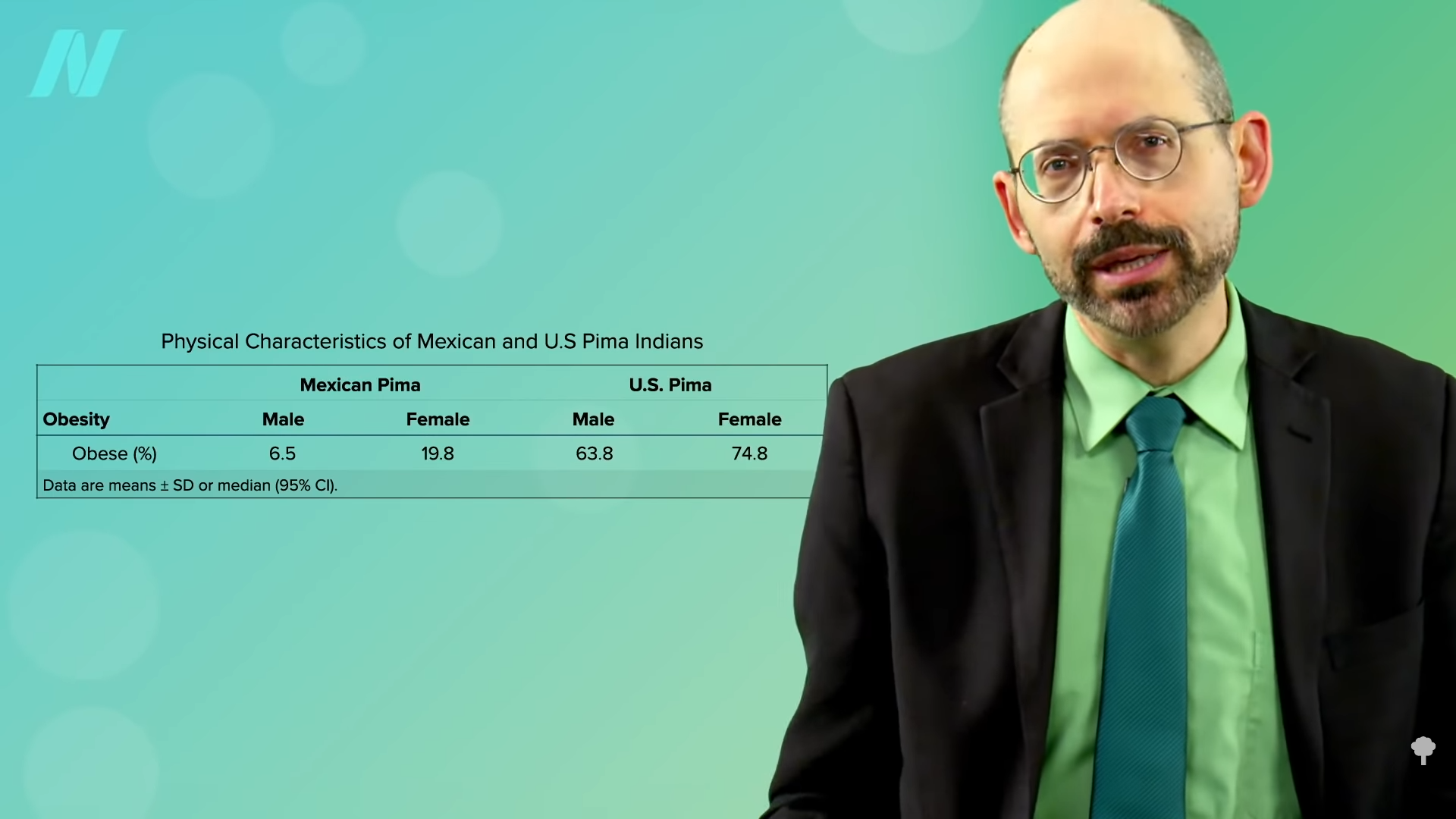
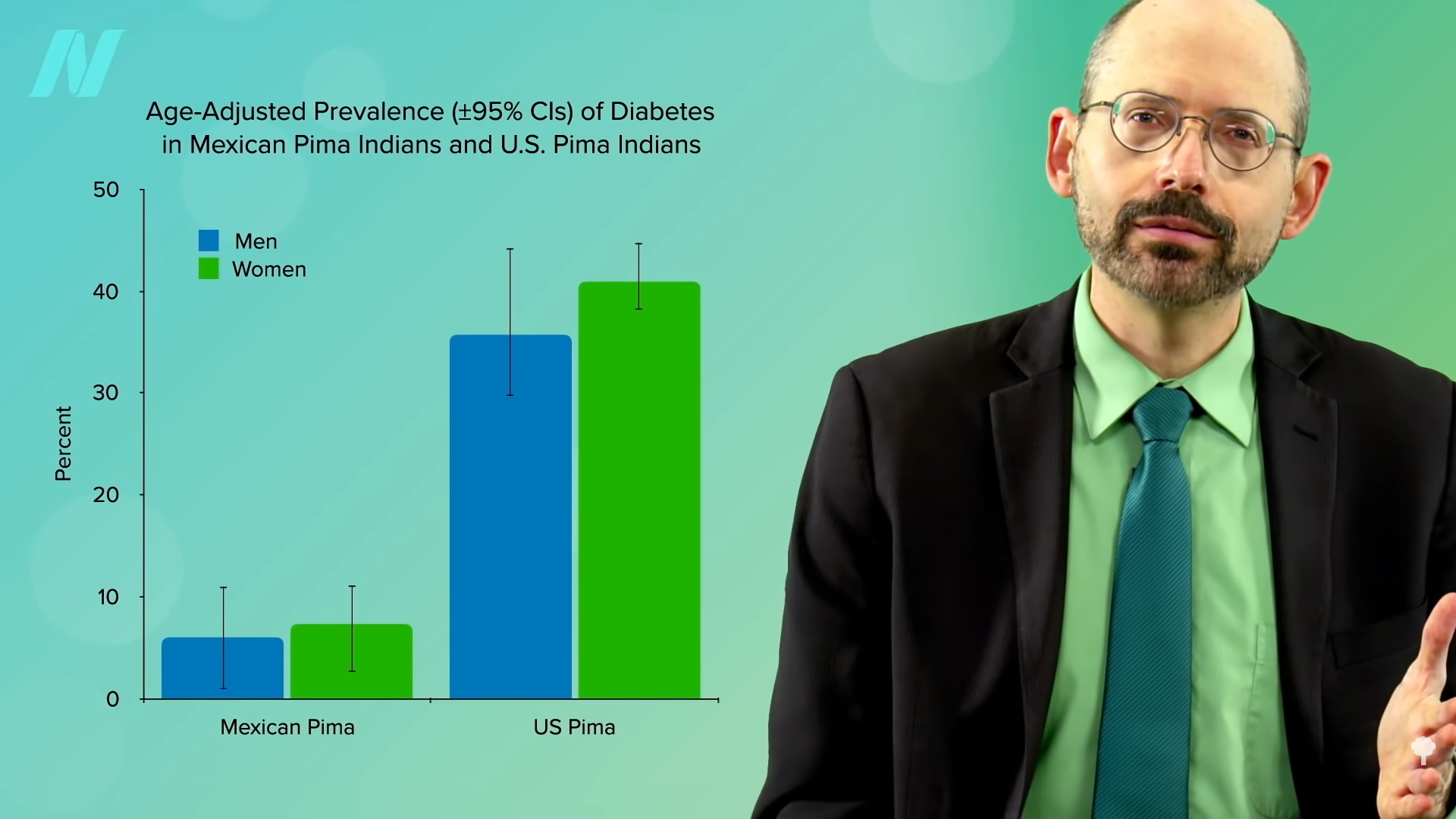
In fact, a natural experiment was set up. The Pima living over the border in Mexico come from the same genetic pool but were able to maintain more of their traditional lifestyle, sticking with their main staples of beans, wheat flour tortillas, and potatoes. Same genes, but seven times less obesity and about four times less diabetes. You can see those graphs below and at 3:58 and 4:02 in my video. Genes may load the gun, but diet pulls the trigger.
Of course, it’s not our genes! Our genes didn’t suddenly change 40 years ago. At the same time, though, in a certain sense, it could be thought of as all in our genes. That’s the topic of my next video The Thrifty Gene Theory: Survival of the Fattest.
This is the second in an 11-video series on the obesity epidemic. If you missed the first one, check out The Role of Diet vs. Exercise in the Obesity Epidemic.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
The future of weight loss is fast approaching. At a recent scientific conference, drug companies showed off a variety of next-generation drugs for both obesity and type 2 diabetes. Some of these treatments might help people lose even more weight than current forerunners like Novo Nordisk’s semaglutide—the active ingredient in popular drugs Ozempic and Wegovy—while others may come with fewer side effects or be easier to take.
Semaglutide is a drug that mimics GLP-1, one of several hormones that help regulate our sense of hunger and blood sugar. In clinical trials, semaglutide has proven to be much more effective at treating obesity than diet and exercise alone. Previously only approved for type 2 diabetes as Ozempic, semaglutide was approved for obesity in 2021 under the name Wegovy. However, it’s already started to be overshadowed by the arrival of Eli Lilly’s tirzepatide, which combines GLP-1 with another incretin hormone called GIP. Tirzepatide was approved by the Food and Drug Administration in 2021 for type 2 diabetes under the brand name Mounjaro; in November 2023, it was approved to treat obesity as Zepbound.
Newer treatments in the works are poised to compete with and possibly surpass both of these drugs. The American Diabetes Association held its annual conference over the past weekend, and the emergence of these future medications was a big aspect of the event. Companies presented preliminary data on over two dozen GLP-1 related drugs, all in various stages of development.
“We’ve heard about Ozempic and Mounjaro and so on, but now we’re seeing lots and lots of different drug candidates in the pipeline, from very early-stage preclinical all the way through late-stage clinical,” Marlon Pragnell, ADA’s vice president of research and science, told NBC News. “It’s very exciting to see so much right now.”
Altimmune’s pemvidutide, for instance, combines GLP-1 with glucagon, another hormone key to keeping our blood sugar level stable. In Phase II trial data presented this weekend, pemvidutide was found to help people lose over 15% of their baseline weight within 48 weeks, a bit ahead of the pace seen with semaglutide (15% weight loss over 68 weeks). A dual GLP-1/GIP candidate developed by scientists in China, called HRS9531 for now, was found to cause up to 16% weight loss within 24 weeks. Eli Lilly also presented new data on its second-generation drug retatrutide, which combines GLP-1, GIP, and glucagon, finding it improved insulin’s ability to control blood sugar in people with type 2 diabetes. In previous research, retatrutide was found to cause up to 24% weight loss, the highest mark seen yet with these drugs.
It’s not certain that these or other GLP-1 drugs in development will truly outmatch semaglutide and tirzepatide in terms of weight loss, but they may still have other benefits over them. Pemvidutide was found to cause less lean body mass loss, for instance, possibly due to the addition of glucagon (exercise naturally raises glucagon levels, so the drug could be mimicking some of the positive effects of exercise). Some experts are skeptical that lean body mass loss is a major concern with these drugs. However, it may be important to prevent this in individuals who are more vulnerable to muscle or bone loss, such as older adults.
It will take years for these newer drugs to reach the public, assuming they continue to succeed in larger trials. Their arrival may not only help people who don’t respond to existing treatments, though, but could also drive down the overall high costs of these medications (without insurance coverage, which is often denied, a month’s supply of semaglutide can reach over $1,000 per month).
“Over the past few years, we have seen the substantial impact of new research working to solve the dual health crisis we are facing, obesity and diabetes,” said Robert Gabbay, chief scientific and medical officer for the ADA, in a statement from the ADA. “The studies we are seeing presented at this year’s annual meeting show great promise to fuel new solutions and treatment options for patients across the globe living with type 2 diabetes and obesity.”
[ad_2]
Ed Cara
Source link

[ad_1]
WASHINGTON, June 18, 2024 (Newswire.com)
–
A recently published article in Experimental Biology and Medicine (249:3, 2024) entitled “Topical naltrexone increases aquaporin 5 production in the lacrimal gland and restores tear production in diabetic rats” highlights factors underlying sustained dry eye in diabetes. The study, led by Dr. Pat McLaughlin and Dr. Ian Zagon, and their graduate student David Diaz, at Pennsylvania State University College of Medicine in Hershey, along with Dr. Joseph W. Sassani, an ophthalmologist at the Pennsylvania State Hershey Medical Center, reports that blockade of the Opioid Growth Factor – Opioid Growth Factor Receptor pathway using formulations of naltrexone is effective at reversing dry eye and stabilizing corneal surface sensitivity in preclinical diabetic animal models.
Diabetes and pre-diabetes are a global epidemic and are accompanied by complications of the visual system. In addition to retinopathy and keratopathy, diabetes is often associated with low tear production (i.e., dry eye) and corneal surface irregularities. Due to the multiple causes of dry eye, how these symptoms occur is not well understood. Chronic dry eye has been described as a dysfunction in the lacrimal functional unit that includes the cornea, lacrimal glands, conjunctiva, and eyelids; tissues that function to create, maintain, and clear tears from the eyes. Previous studies by these researchers have shown that animal models of diabetes develop dry eye within weeks of becoming hyperglycemic. Simultaneously an innate pathway, the Opioid Growth Factor (OGF) – OGF Receptor (OGFr) axis, that regulates cellular homeostasis becomes dysregulated and there is an overproduction of OGF, an inhibitory peptide that reduces cellular proliferation. Blockade of the interaction between peptide and receptor using topical applications of the FDA-approved opioid antagonist naltrexone reverses dry eye symptoms in 5 days and restores tear fluid volumes to normal baseline.
The mechanism related to this relatively fast reversal of dry eye following OGFr blockade is the focus of the current paper and continues their pioneering studies of the dysregulation of the OGF-OGFr axis and corneal surface complications. Hyperglycemic male and female rats showing characteristic type 1 diabetic ocular surface complications including dry eye and decreased corneal sensitivity received topical naltrexone treatment in one eye for 10 days. Within 5 days, normal tear volume was measured, dry eye was reversed, and corneal sensitivity was restored. Treatment with naltrexone resulted in no significant morphological changes in the lacrimal or meibomian glands, however, there was an increase in conjunctiva goblet cells that produce beneficial mucin. Topical naltrexone treatment also increased the presence of aquaporin-5, an aqueous protein marker for secretory function in the lacrimal gland.
The results in this paper extend knowledge about the role of receptor blockade of the OGF-OGFr pathway by naltrexone, demonstrating that the mechanism behind short-term topical application to reverse dry eye is not related to direct morphological changes in the lacrimal glands. Rather it is due to the amounts of aqueous protein and mucin secretions which in turn are related to sensory fibers that reside on the surface of the cornea. Dr. McLaughlin stated that “these data are provocative and direct our research toward sensory nerve density and function in the cornea in order to better understand the mechanisms of dry eye and its relationship to the OGF-OGFr pathway.”
Dr. Goodman, Editor-in-Chief for Experimental Biology and Medicine, said: “McLaughlin and Zagon initially identified and characterized the OGF-OGFr axis. With clinical colleagues, they have studied its dysregulation in diabetes and have patented treatments for treatment of dry eye and delayed skin repair. Their important findings warrant clinical studies to determine the efficacy of receptor blockade by naltrexone for treatment of dry eye in persons with diabetes.”
Experimental Biology and Medicine is a global journal dedicated to the publication of multidisciplinary and interdisciplinary research in the biomedical sciences. The journal was first established in 1903. Experimental Biology and Medicine is the journal of the Society of Experimental Biology and Medicine. To learn about the benefits of society membership, visit www.sebm.org. If you are interested in publishing in the journal, please visit https://www.ebm-journal.org.
For further information, please contact bzimmer@sebm.org.
Source: Experimental Biology and Medicine
[ad_2]

[ad_1]
How do healthier plant-based diets compare to unhealthy plant foods and animal foods when it comes to diabetes risk?
In my video on flexitarians, I discuss how the benefits of eating a plant-based diet are not all-or-nothing. “Simple advice to increase the consumption of plant-derived foods with compensatory [parallel] reductions in the consumption of foods from animal sources confers a survival advantage”— a live-longer advantage. The researchers call it a “pro-vegetarian” eating pattern, one that’s moving in the direction of vegetarianism, “a more gradual and gentle approach.”
If you’re dealing with a serious disease, though, like diabetes, completely “avoiding some problem foods is easier than attempting to moderate their intake. Clinicians would never tell an alcoholic to try to simply cut down on alcohol. Avoiding alcohol entirely is more effective and, in fact, easier for a problem drinker…Paradoxically, asking patients to make a large change may be more effective than making a slow transition. Diet studies show that recommending more significant changes increases the chances that patients can accomplish [them]. It may help to replace the common advice, ‘all things in moderation’ with ‘big changes beget big results.’ Success breeds success. After a few days or weeks of major dietary changes, patients are likely to see improvements in weight and blood glucose [sugar] levels—improvements that reinforce the dietary changes that elicited them. Furthermore, they may enjoy other health benefits of a plant-based diet” that may give them further motivation.
As you can see below and at 1:43 in my video Friday Favorites: Is Vegan Food Always Healthy?, those who choose to eat plant-based for their health say it’s mostly for “general wellness or general disease prevention” or to improve their energy levels or immune function, for example.
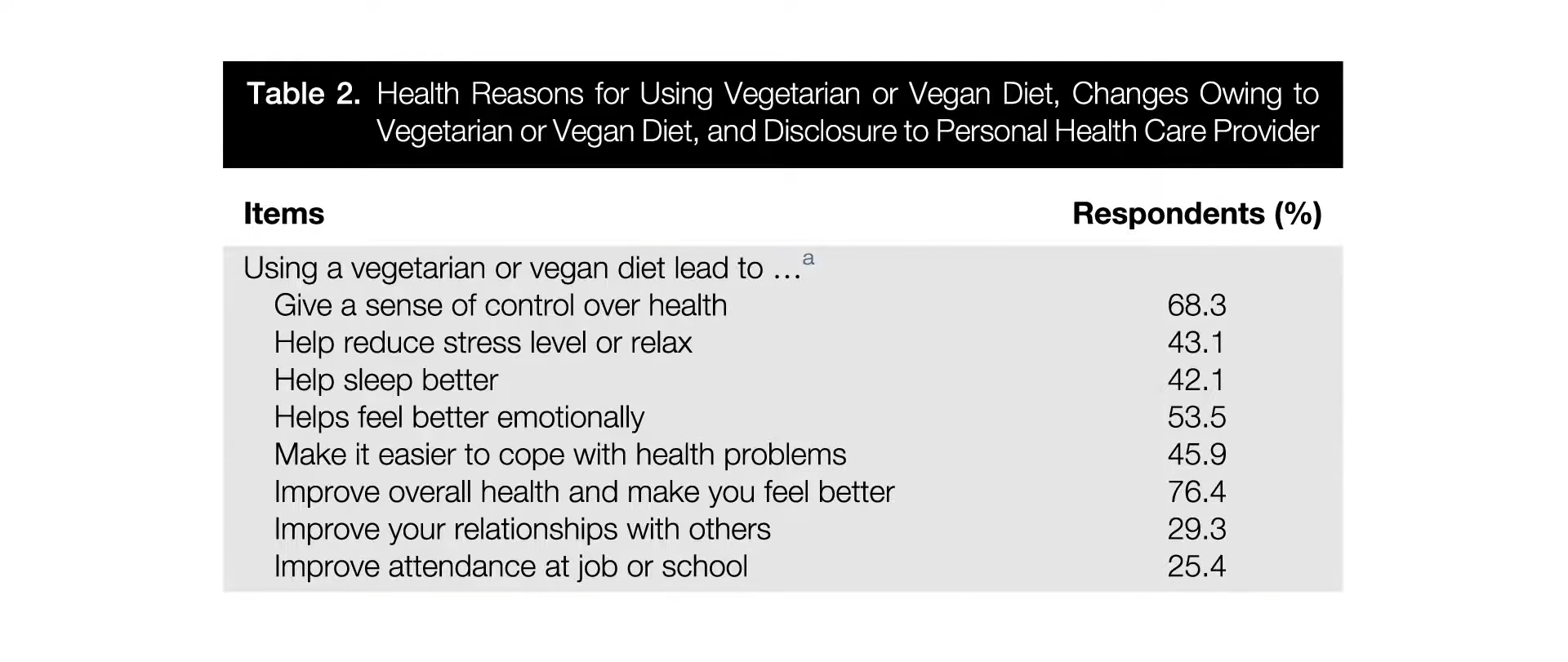
They felt it gives them a sense of control over their health, helps them feel better emotionally, improves their overall health, makes them feel better, and more, as shown below and at 1:48. Most felt it was very important for maintaining their health and well-being.
For the minority who used it for a specific health problem, mostly high cholesterol or weight loss, followed by high blood pressure and diabetes, most reported they felt it helped a great deal, as you can see below and at 2:14. 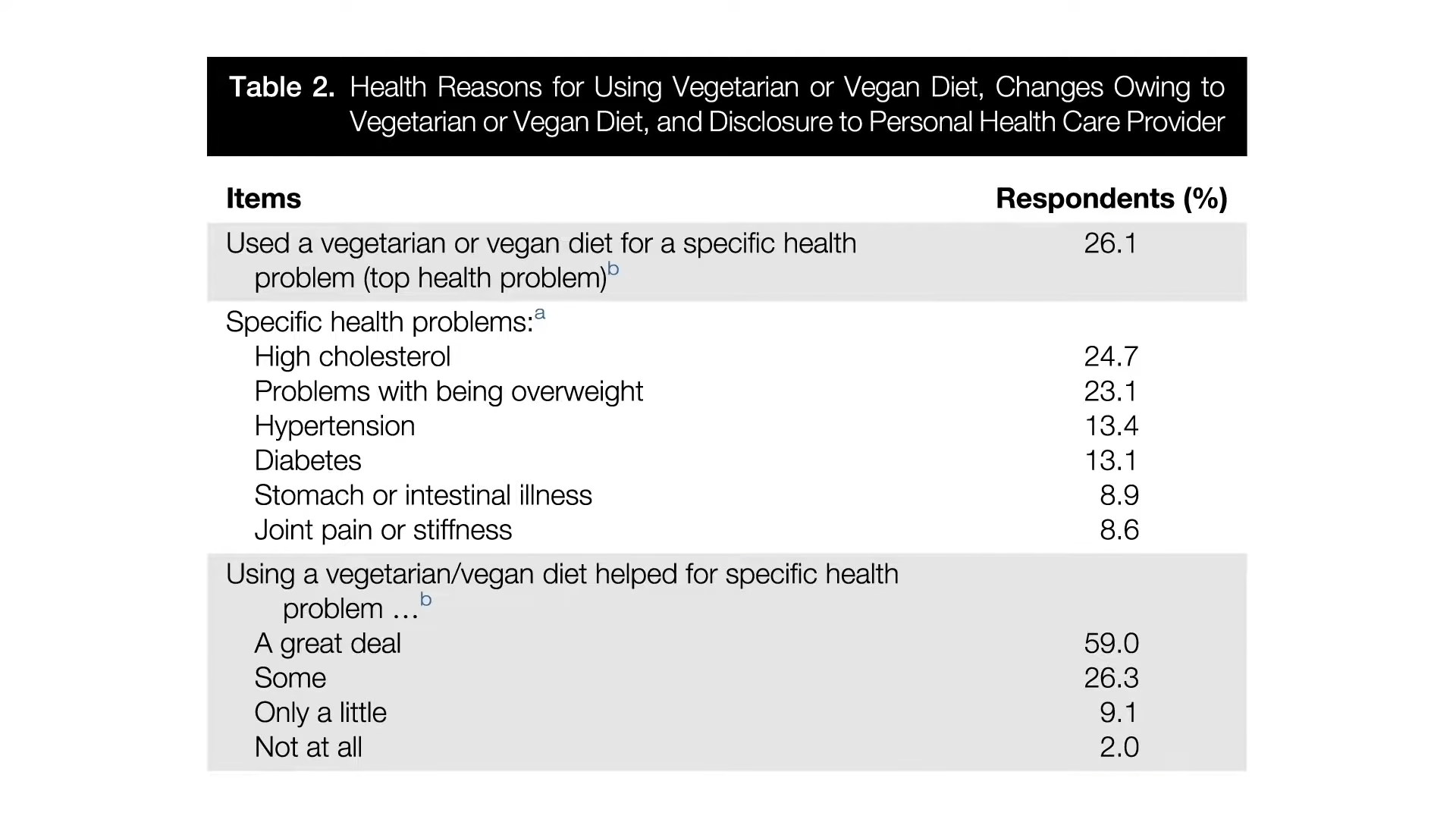
Some choose plant-based diets for other reasons, such as animal welfare or global warming, and it looks like “ethical vegans” are more likely to eat sugary and fatty foods, like vegan donuts, compared to those eating plant-based because of religious or health concerns, as you can see below and at 2:26 in my video.
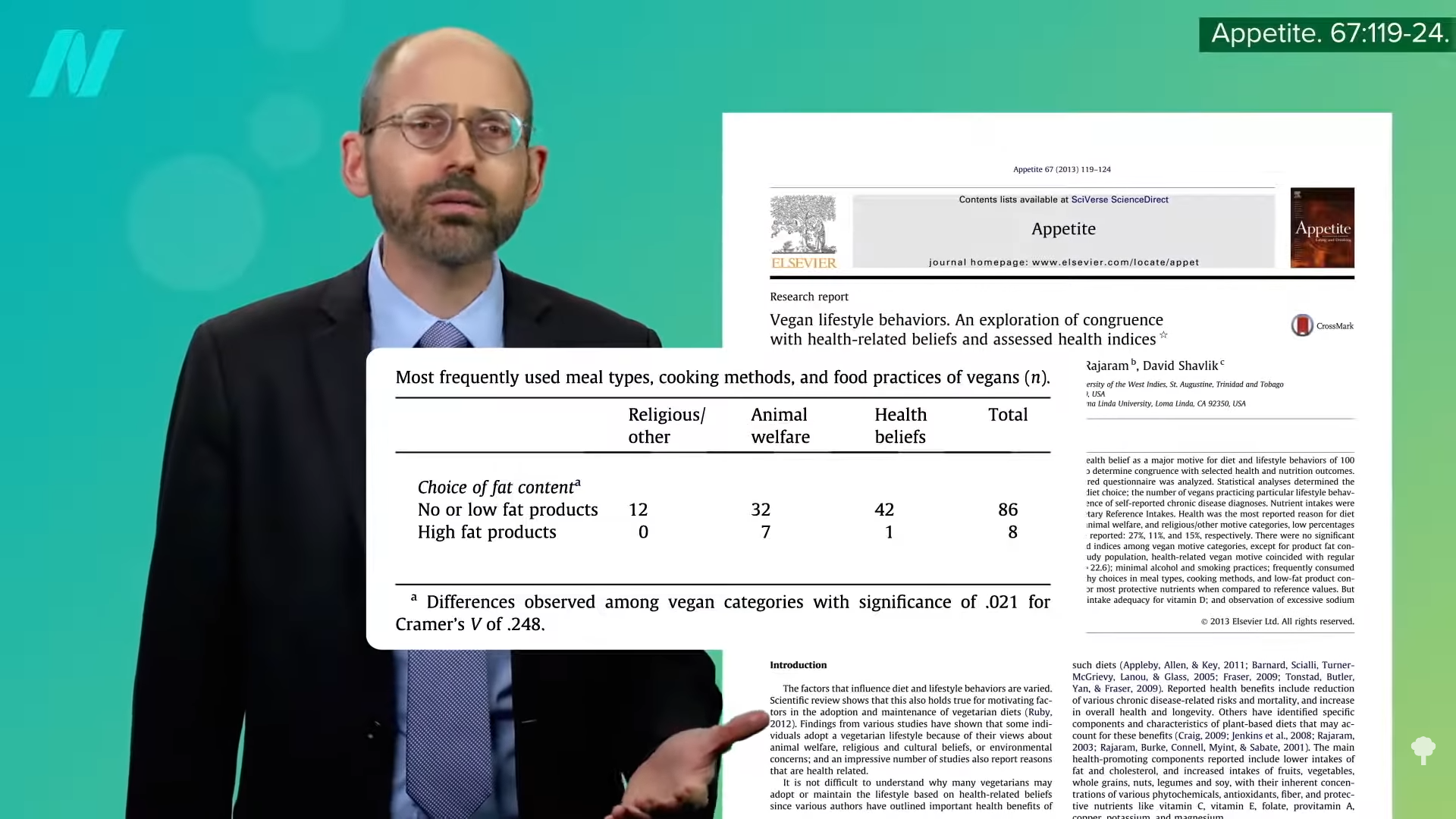
The veganest vegan could make an egg- and dairy-free cake, covered with frosting, marshmallow fluff, and chocolate syrup, topped with Oreos, and served with a side of Doritos. Or, they may want fruit for dessert, but in the form of Pop-Tarts and Krispy Kreme pies. Vegan, yes. Healthy, no.
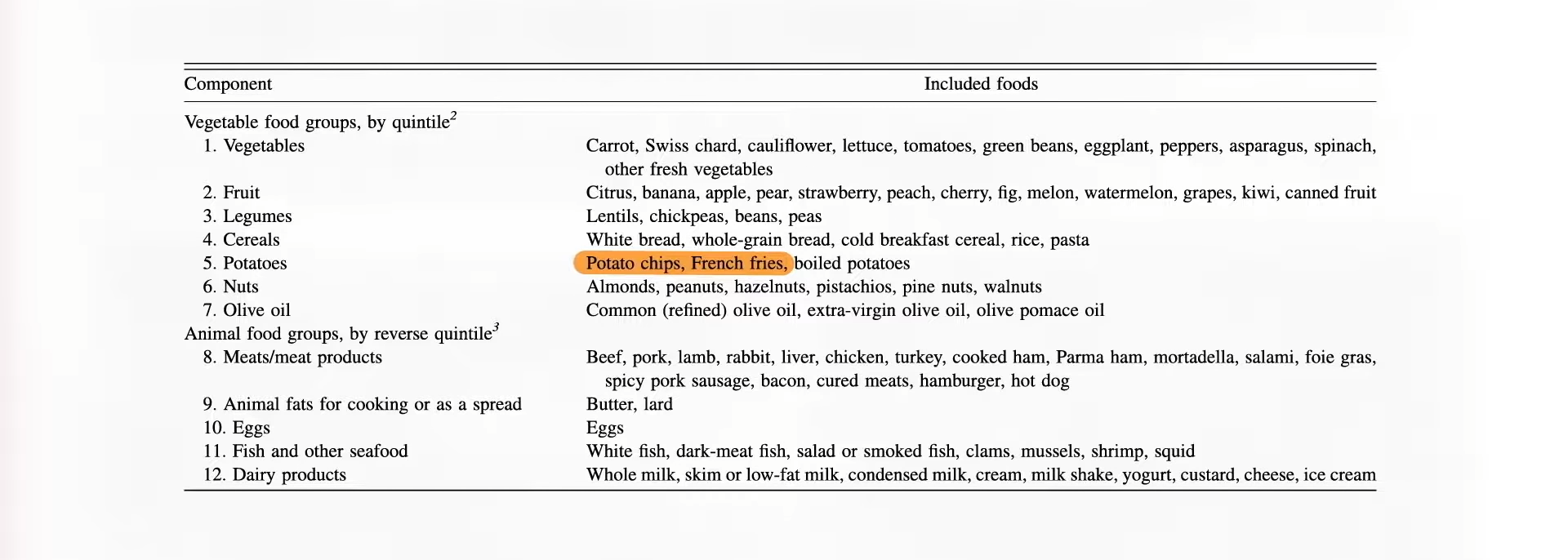
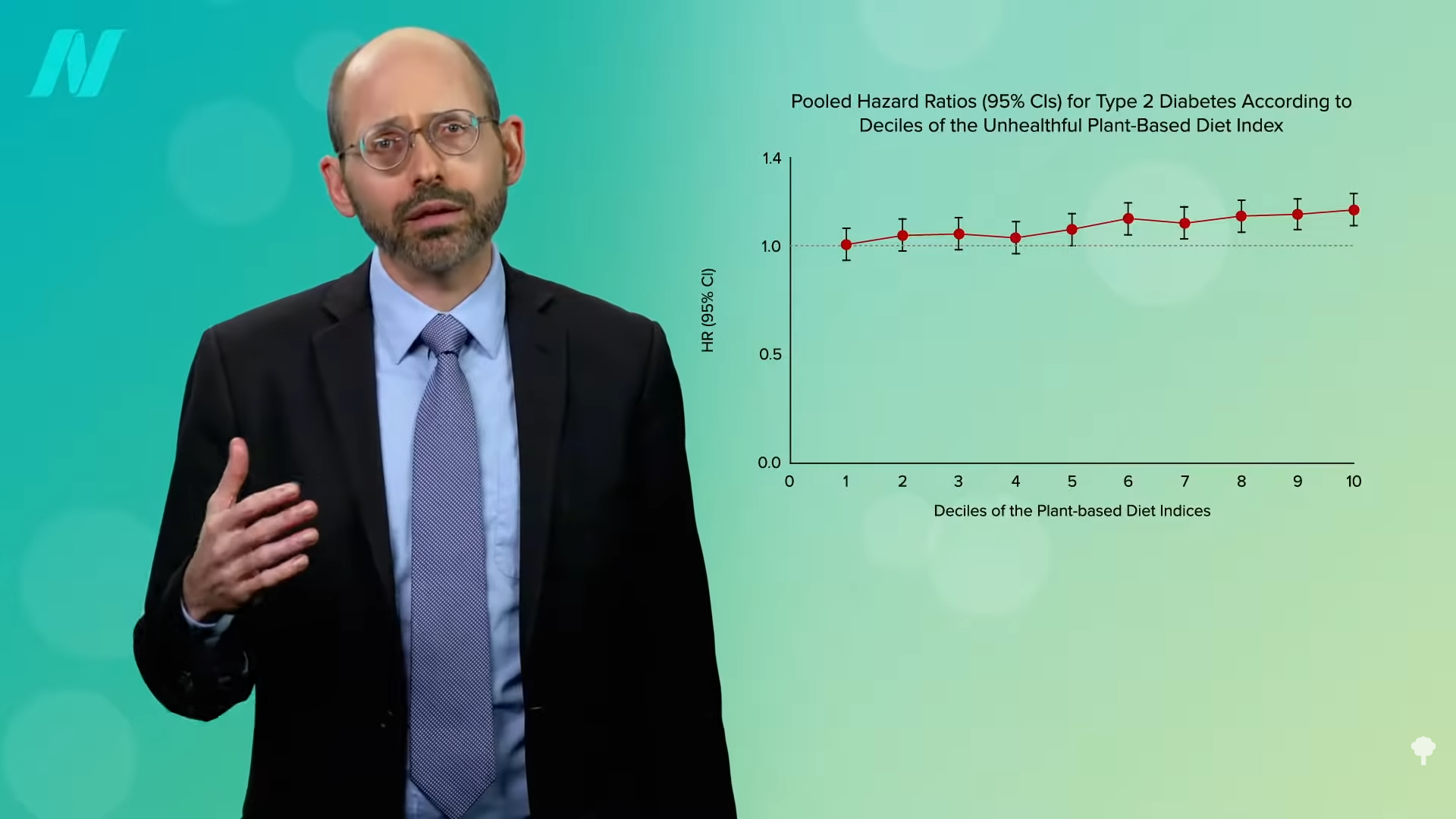
“Plant-based diets have been recommended to reduce the risk of type 2 diabetes (T2D). However, not all plant foods are necessarily beneficial.” In the pro-vegetarian scoring system I mentioned above, you get points for eating potato chips and French fries because they are technically plant-based, as you can see below and at 3:07 in my video, but Harvard researchers wanted to examine the association of not only an overall plant-based diet, but healthy and unhealthy versions. So, they created the same kind of pro-vegetarian scoring system, but it was weighted towards any sort of plant-based foods and against animal foods; then, they created a healthful plant-based diet index, where at least some whole plant foods took precedence and Coca-Cola and other sweetened beverages were no longer considered plants. Lastly, they created an unhealthful plant-based diet index by assigning positive scores to processed plant-based junk and negative scores for healthier plant foods and animal foods.
Their findings? As you can see below and at 3:51 in my video, a more plant-based diet, in general, was good for reducing diabetes risk, but eating especially healthy plant-based foods did better, nearly cutting risk in half, while those eating more unhealthy plant foods did worse, as shown in the graph below and at 4:03.
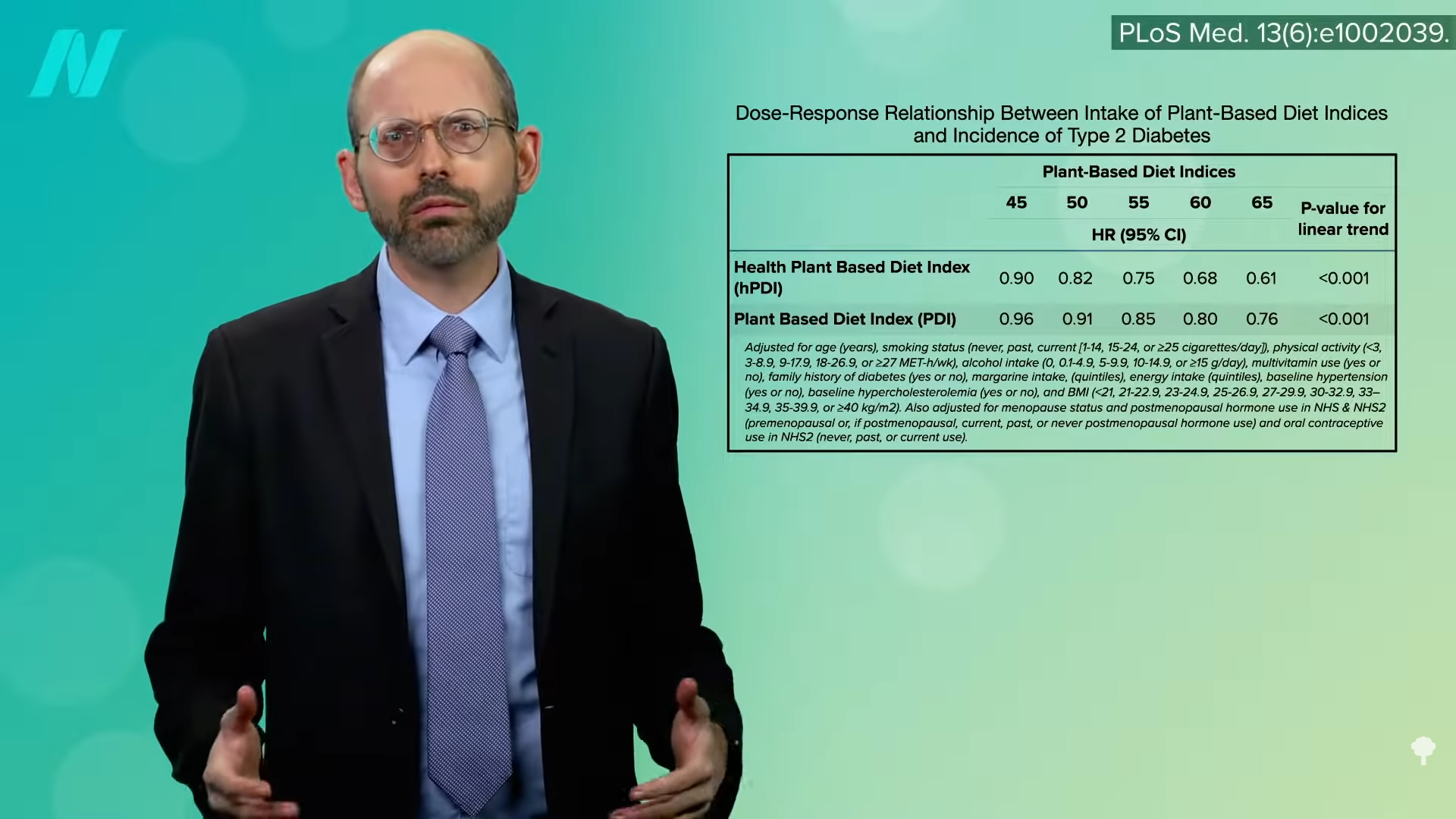
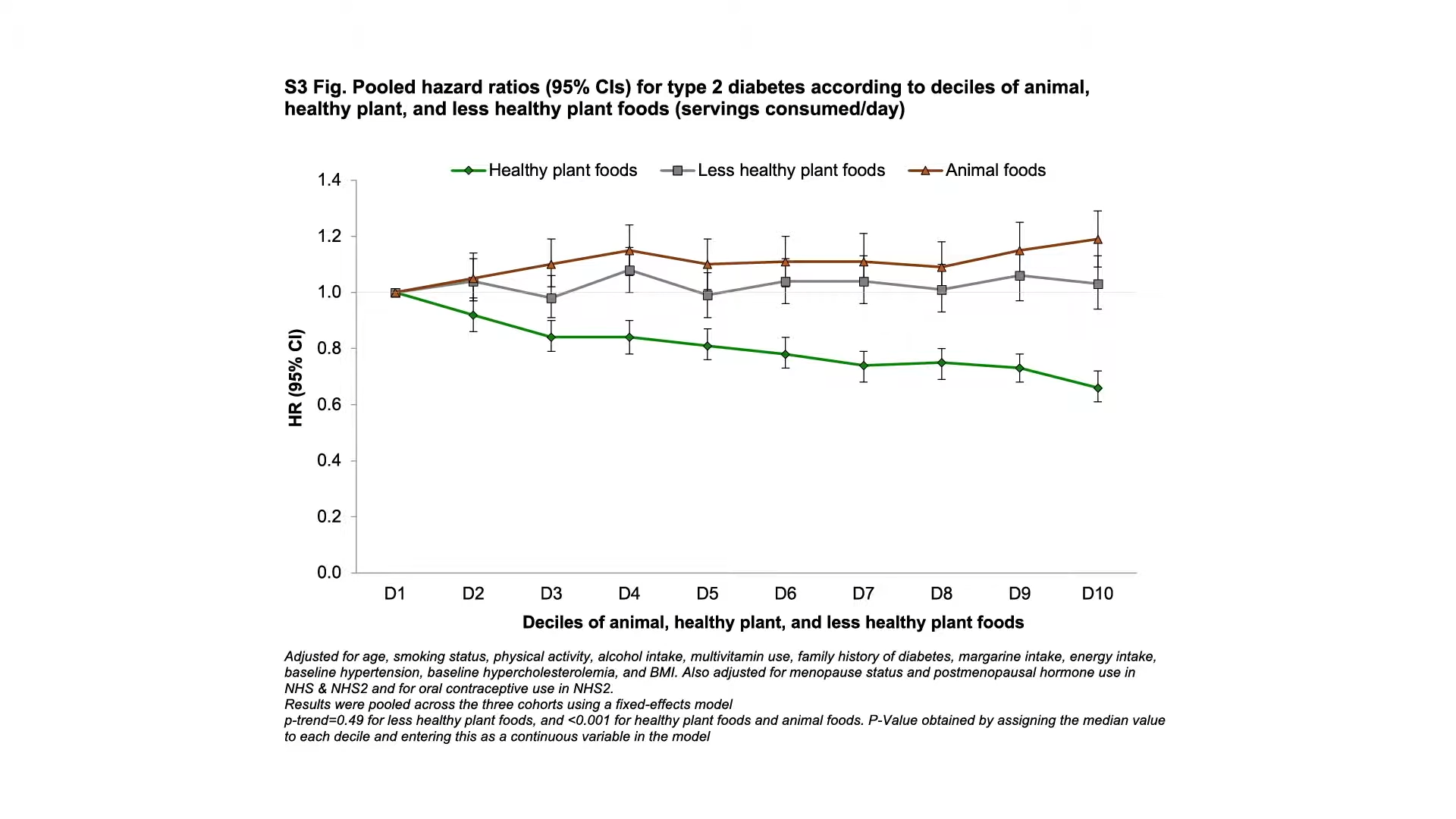
Now, is that because they were also eating more animal foods? People often eat burgers with their fries, so the researchers separated the effects of healthy plant foods, less healthy plant foods, and animal foods on diabetes risk. And, they found that healthy plant foods were protectively associated, animal foods were detrimentally associated, and less healthy plant foods were more neutral when it came to diabetes risk. Below and at 4:32 in my video, you can see the graph that shows higher diabetes risk with more and more animal foods, no protection whatsoever with junky plant foods, and lower and lower diabetes risk associated with more and more healthy whole plant foods in the diet. So, they concluded that, yes, “plant-based diets…are associated with substantially lower risk of developing T2D.” However, it may not be enough to just lower the intake of animal foods; consumption of less healthy plant foods may need to decrease, too.
 As a physician, labels like vegetarian and vegan just tell me what you don’t eat, but there are a lot of unhealthy vegetarian fare like French fries, potato chips, and soda pop. That’s why I prefer the term whole food and plant-based nutrition. That tells me what you do eat—a diet centered around the healthiest foods out there.
As a physician, labels like vegetarian and vegan just tell me what you don’t eat, but there are a lot of unhealthy vegetarian fare like French fries, potato chips, and soda pop. That’s why I prefer the term whole food and plant-based nutrition. That tells me what you do eat—a diet centered around the healthiest foods out there.
The video I mentioned is Do Flexitarians Live Longer?.
You may also be interested in some of my past popular videos and blogs on plant-based diets. Check related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
What can shift workers do to moderate the adverse effects of circadian rhythm disruption?
Shift workers may have higher rates of death from heart disease, stroke, diabetes, dementia, and cardiovascular disease, as well as higher rates of death from cancer. Graveyard shift, indeed! But, is it just because they’re eating out of vending machines or not getting enough sleep? Highly controlled studies have recently attempted to tease out these other factors by putting people on the same diets with the same sleep—but at the wrong time of day. Redistributing eating to the nighttime resulted in elevated cholesterol and increases in blood pressure and inflammation. No wonder shift workers are at higher risk. Shifting meals to the night in a simulated night-shift protocol effectively turned about one-third of the subjects prediabetic in just ten days. Our bodies just weren’t designed to handle food at night, as I discuss in my video The Metabolic Harms of Night Shifts and Irregular Meals.
Just as avoiding bright light at night can prevent circadian misalignment, so can avoiding night eating. We may have no control over the lighting at our workplace, but we can try to minimize overnight food intake, which has been shown to help limit the negative metabolic consequences of shift work. When we finally do get home in the morning, though, we may disproportionately crave unhealthy foods. In one experiment, 81 percent of participants in a night-shift scenario chose high-fat foods, such as croissants, out of a breakfast buffet, compared to just 43 percent of the same subjects during a control period on a normal schedule.
Shiftwork may also leave people too fatigued to exercise. But, even at the same physical activity levels, chronodisruption can affect energy expenditure. Researchers found that we burn 12 to 16 percent fewer calories while sleeping during the daytime compared to nighttime. Just a single improperly-timed snack can affect how much fat we burn every day. Study subjects eating a specified snack at 10:00 am burned about 6 more grams of fat from their body than on the days they ate the same snack at 11:00 pm. That’s only about a pat and a half of butter’s worth of fat, but it was the identical snack, just given at a different time. The late snack group also suffered about a 9 percent bump in their LDL cholesterol within just two weeks.
Even just sleeping in on the weekends may mess up our metabolism. “Social jetlag is a measure of the discrepancy in sleep timing between our work days and free days.” From a circadian rhythm standpoint, if we go to bed late and sleep in on the weekends, it’s as if we flew a few time zones west on Friday evening, then flew back Monday morning. Travel-induced jet lag goes away in a few days, but what might the consequences be of constantly shifting our sleep schedule every week over our entire working career? Interventional studies have yet put it to the test, but population studies suggest that those who have at least an hour of social jet lag a week (which may describe more than two-thirds of people) have twice the odds of being overweight.
If sleep regularity is important, what about meal regularity? “The importance of eating regularly was highlighted early by Hippocrates (460–377 BC) and later by Florence Nightingale,” but it wasn’t put to the test until the 21st century. A few population studies had suggested that those eating meals irregularly were at a metabolic disadvantage, but the first interventional studies weren’t published until 2004. Subjects were randomized to eat their regular diets divided into six regular eating occasions a day or three to nine daily occasions in an irregular manner. Researchers found that an irregular eating pattern can cause a drop in insulin sensitivity and a rise in cholesterol levels, as well as reduce the calorie burn immediately after meals in both lean and obese individuals. The study participants ended up eating more, though, on the irregular meals, so it’s difficult to disentangle the circadian effects. The fact that overweight individuals may overeat on an irregular pattern may be telling in and of itself, but it would be nice to see such a study repeated using identical diets to see if irregularity itself has metabolic effects.
Just such a study was published in 2016: During two periods, people were randomized to eat identical foods in a regular or irregular meal pattern. As you can see in the graph below and at 4:47 in my video, during the irregular period, people had impaired glucose tolerance, meaning higher blood sugar responses to the same food.
They also had lower diet-induced thermogenesis, meaning the burning of fewer calories to process each meal, as seen in the graph below and at 4:55 in my video.
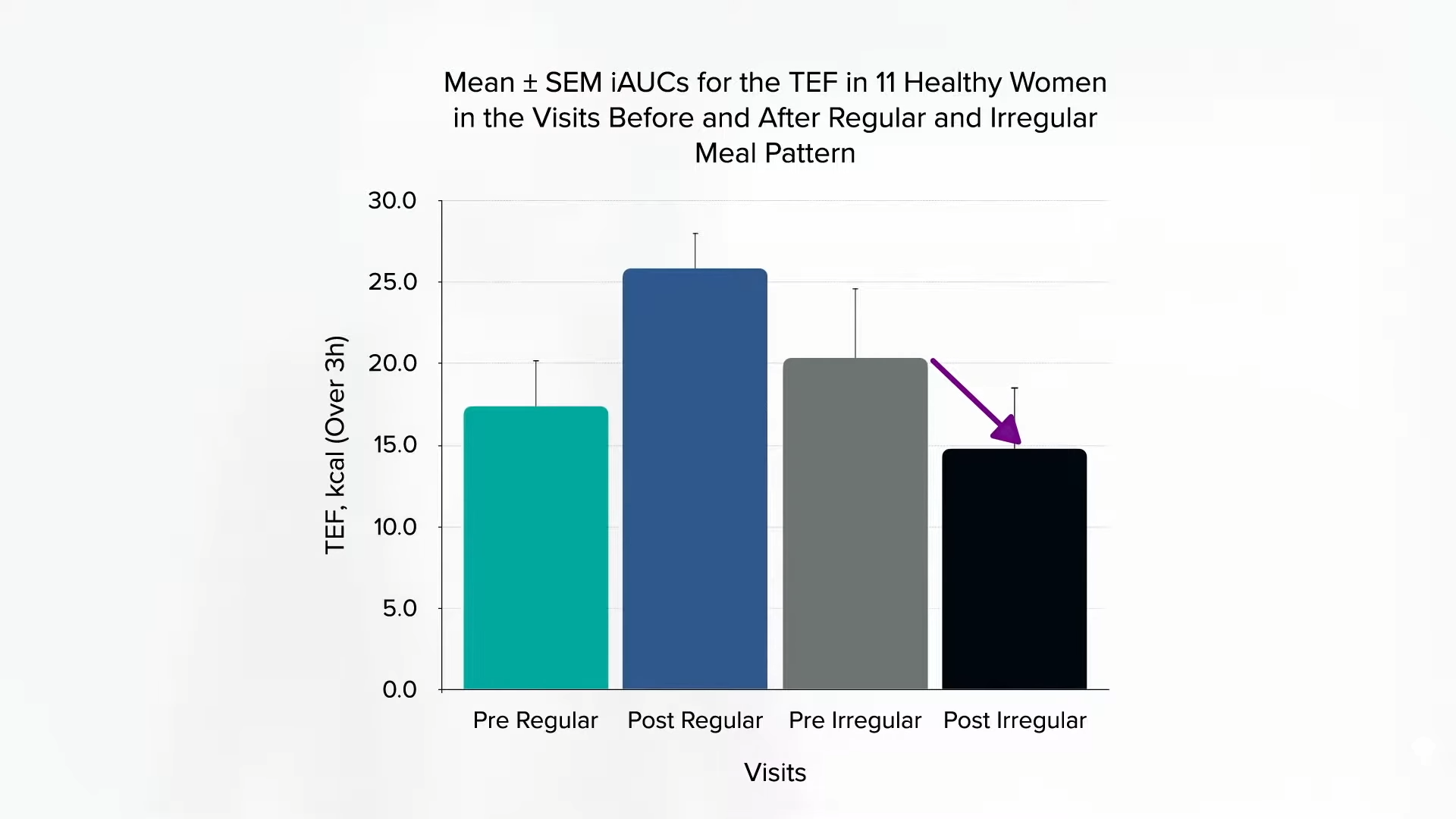
The difference in thermogenesis only came out to be about ten calories per meal, though, and there was no difference in weight changes over the two-week periods. However, diet-induced thermogenesis can act as “a satiety signal.” The extra work put into processing a meal can help slake one’s appetite. And, indeed, “lower hunger and higher fullness ratings” during the regular meal period could potentially translate into better weight control over the long term.
The series on chronobiology is winding down with just two videos left in this series: Shedding Light on Shedding Weight and Friday Favorites: Why People Gain Weight in the Fall.
If you missed any of the other videos, see the related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
More than 200 people with diabetes were injured after technology defect caused their insulin pump to unexpectedly shut down, according to the Food and Drug Administration.
The software glitch has prompted the recall of more than 85,000 versions of a mobile app, called t:connect and developed by Tandem Diabetes Care, the FDA noted on Wednesday.
The Apple iOS-based software recall involves Version 2.7 of the mobile app, which works with the t:slim X2 insulin pump with Control-IQ technology. The issue can cause the app to continuously crash and restart, draining the pump’s battery.
A shutdown of the pump suspends the delivery of insulin, which can result in hyperglycemia or even ketoacidosis, a potentially life-threatening condition that can require hospitalization or intervention by a medical professional. Tandem urged patients and physicians who use the device to update the app to version 2.7.1 or later as soon as possible.
As of April 15, there have been 224 reported injuries and no reports of death, according to the notice posted by the FDA.
Roughly 38 million people in the U.S. have diabetes, according to the Centers for Disease Control and Prevention. Diabetes can cause health complications including blindness, kidney failure, heart disease, stroke, and loss of toes, feet or legs.
[ad_2]

[ad_1]
Ancient types of wheat, like kamut, are put to the test for inflammation, blood sugar, and cholesterol control.
The number one killer in the United States and around the world is what we eat. As you can see in the graph below and at 0:15 in my video Friday Favorites: Are Ancient Grains Healthier?, our diet kills millions more than tobacco. What are the five most important things we can do to improve our diets, based on the single most comprehensive global study of the health impact of nutrition? Eat less salt, eat more nuts, eat more non-starchy vegetables, eat more fruit, and, finally, eat more whole grains.
Any particular type of whole grains? What about so-called ancient grains? Are they any better than modern varieties? For instance, what about kamut, described as “mummy wheat” and supposedly unearthed from an Egyptian tomb?
After WWII, the wheat industry selected particularly high-yielding varieties for pasta and bread. Over the past few years, though, some of the more ancient grains—“defined as those species that have remained unchanged over the last hundred years” despite agricultural revolutions—have been reintroduced to the market.
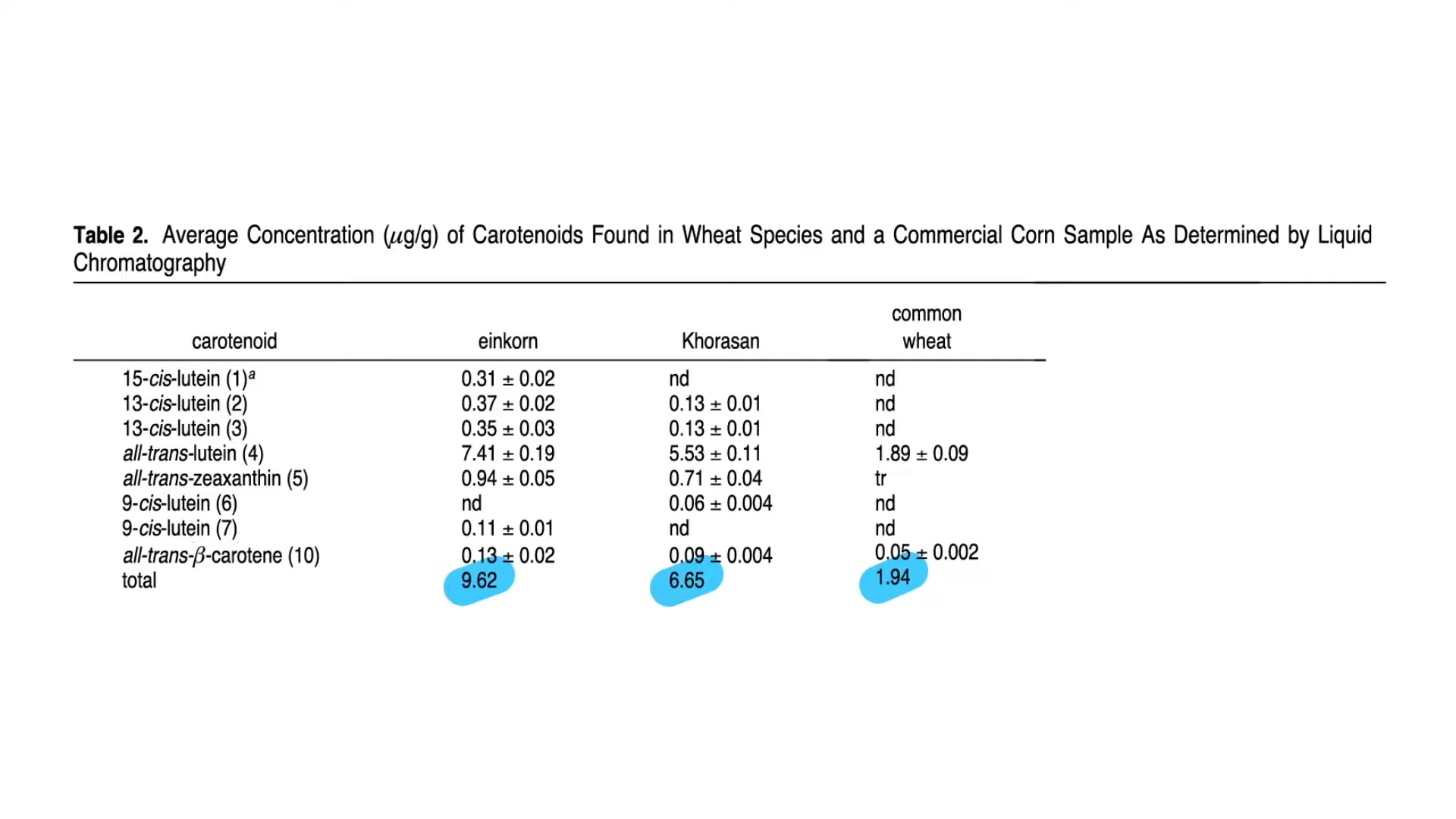
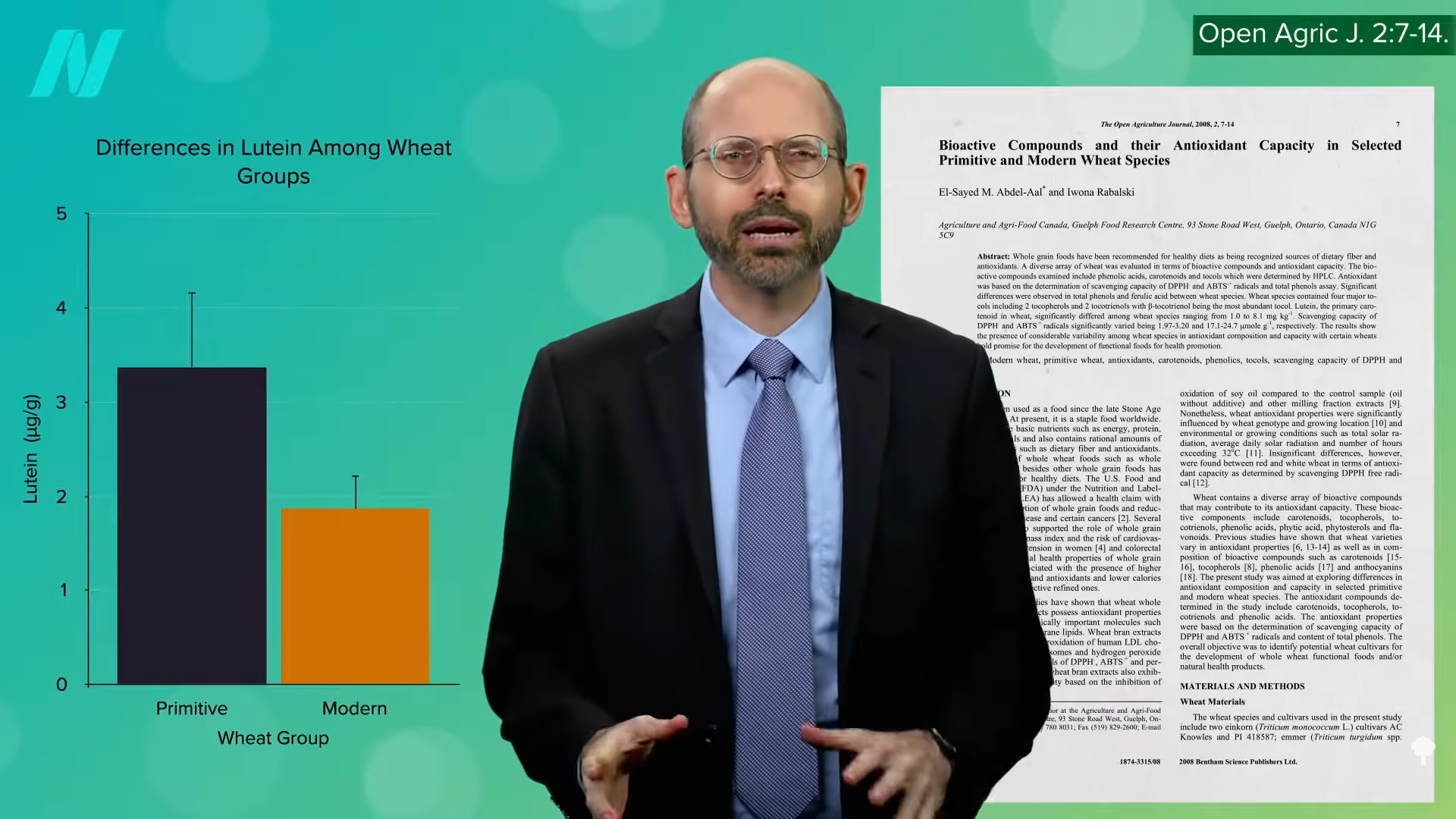
As you can see below and at 1:13 in my video, nutritionally, kamut and einkorn wheat, which is the oldest wheat, have more eyesight-improving yellow carotenoid pigments, such as lutein and zeaxanthin, compared to modern bread and pastry wheat, because the pigments have been bred out of the bread intentionally. People want their white bread white, but modern pasta flour (durum wheat) maintains much of that yellow nutritional hue.
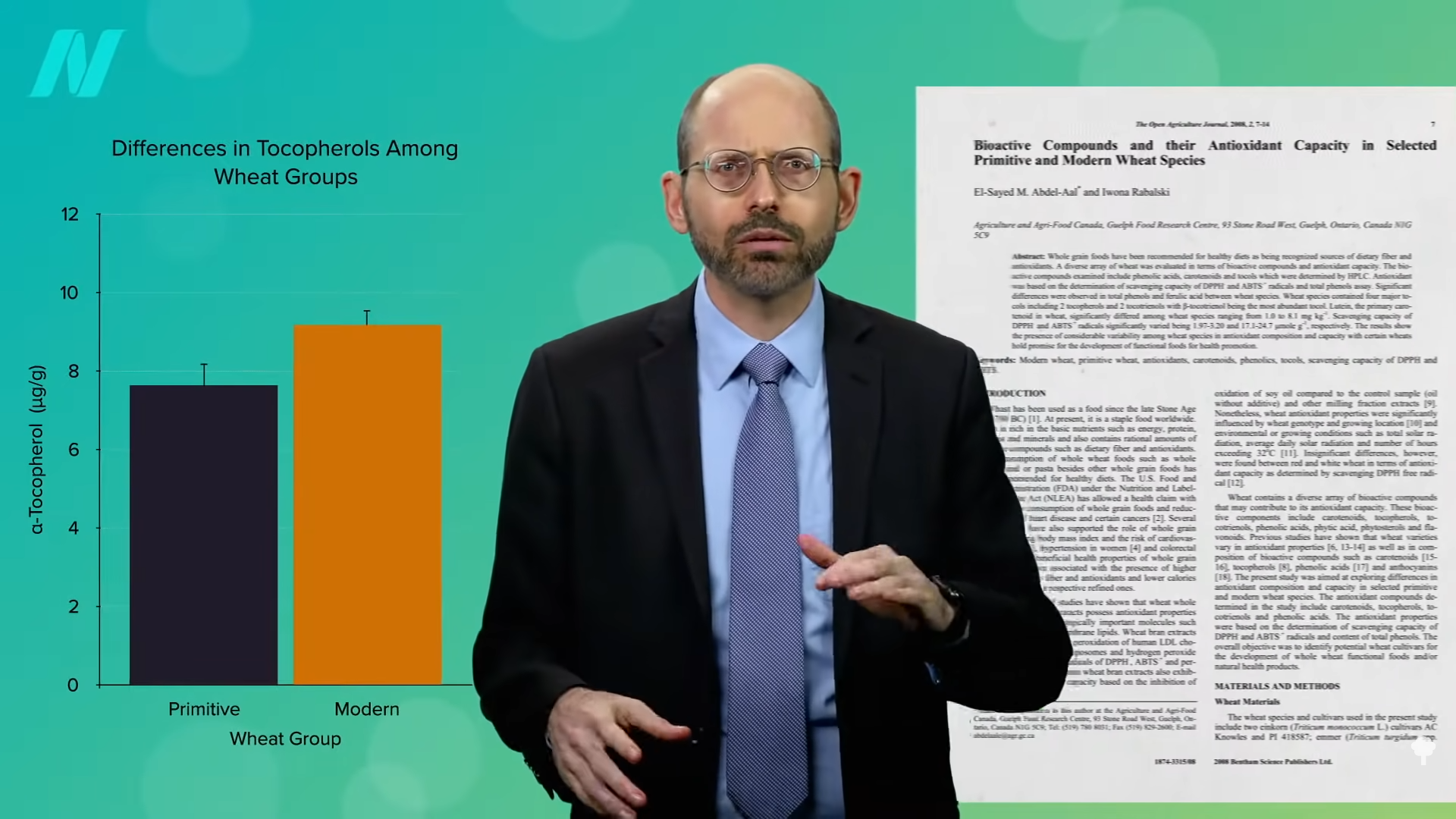
 As you can see in the graph below and at 1:41 in my video, modern wheat may have less lutein, but it tends to have more vitamin E, as seen in the graph below and at 1:45. Based on straight vitamin and mineral concentrations, it’s pretty much a wash. Both modern and primitive kinds of wheat have a lot of each, but primitive wheats do have more antioxidant capacity, likely due to their greater polyphenol content, as you can see in the graph below and at 2:00 in my video. To know if that makes any difference, though, we have to put it to the test.
As you can see in the graph below and at 1:41 in my video, modern wheat may have less lutein, but it tends to have more vitamin E, as seen in the graph below and at 1:45. Based on straight vitamin and mineral concentrations, it’s pretty much a wash. Both modern and primitive kinds of wheat have a lot of each, but primitive wheats do have more antioxidant capacity, likely due to their greater polyphenol content, as you can see in the graph below and at 2:00 in my video. To know if that makes any difference, though, we have to put it to the test.
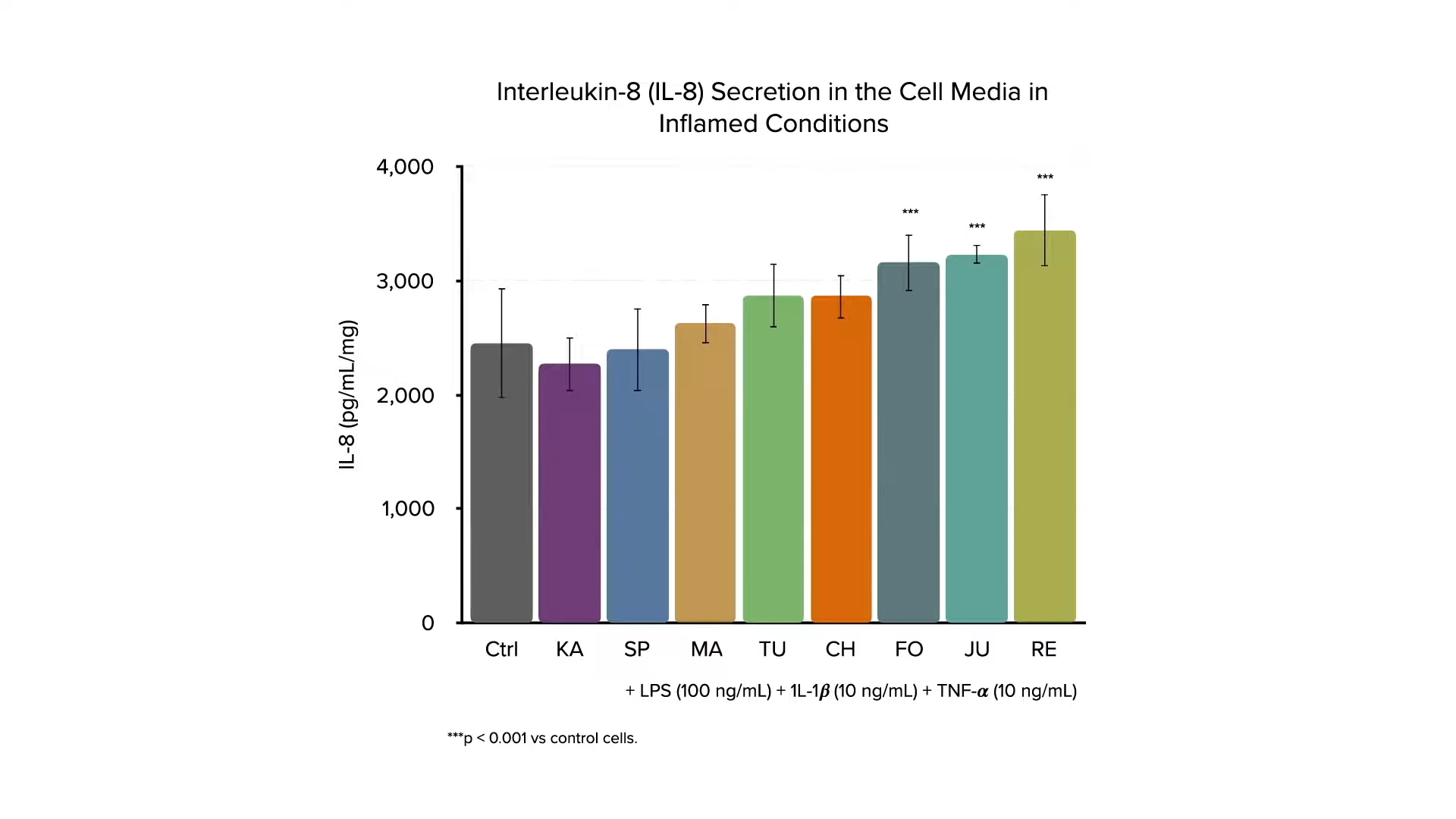
If you expose human liver cells to digested bread made out of ancient grains (kamut and spelt), heritage kinds of wheat, or modern strains, then expose the cells to an inflammatory stimulus, the modern wheat strains seem less able to suppress the inflammation, as you can see in the graphs below and at 2:09 in my video. The investigators conclude that even though these different grains seem to be very similar nutritionally, they appear to exert different effects on human cells, “confirming the potential health benefits of ancient grains.” 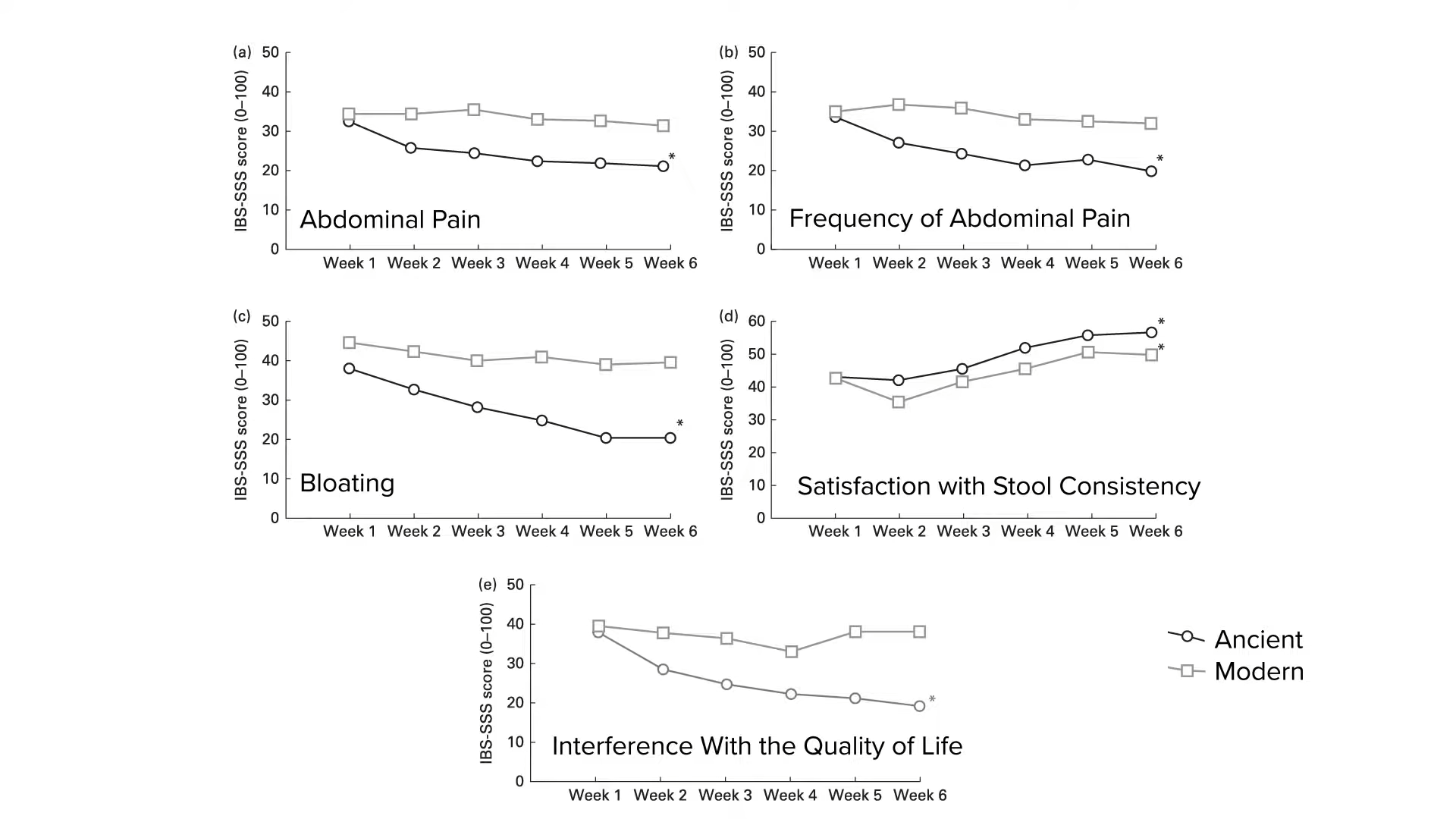 That was in a petri dish, though. What about people? If ancient kinds of wheat are better at suppressing inflammation, what if you took people with irritable bowel syndrome (IBS) and randomized them to receive six weeks of wheat products made out of modern wheat or ancient wheat—in this case, kamut? Same amount of wheat, just different types. If there is no difference between the wheats, there’d be no difference in people’s symptoms, right? But, when study participants in the control group were switched to the ancient wheat kamut, they experienced less abdominal pain, less frequent pain, less bloating, more satisfaction with stool consistency, and less interference with their quality of life, compared to the modern wheat. So, after switching to the ancient wheat, they had “a significant global improvement in the extent and severity of symptoms related to IBS…”
That was in a petri dish, though. What about people? If ancient kinds of wheat are better at suppressing inflammation, what if you took people with irritable bowel syndrome (IBS) and randomized them to receive six weeks of wheat products made out of modern wheat or ancient wheat—in this case, kamut? Same amount of wheat, just different types. If there is no difference between the wheats, there’d be no difference in people’s symptoms, right? But, when study participants in the control group were switched to the ancient wheat kamut, they experienced less abdominal pain, less frequent pain, less bloating, more satisfaction with stool consistency, and less interference with their quality of life, compared to the modern wheat. So, after switching to the ancient wheat, they had “a significant global improvement in the extent and severity of symptoms related to IBS…”
What about liver inflammation? The liver function of those with nonalcoholic fatty liver disease randomized to eat kamut improved, compared to those eating the same amount of regular wheat, suggesting kamut is superior, as you can see below and at 3:47 in my video.

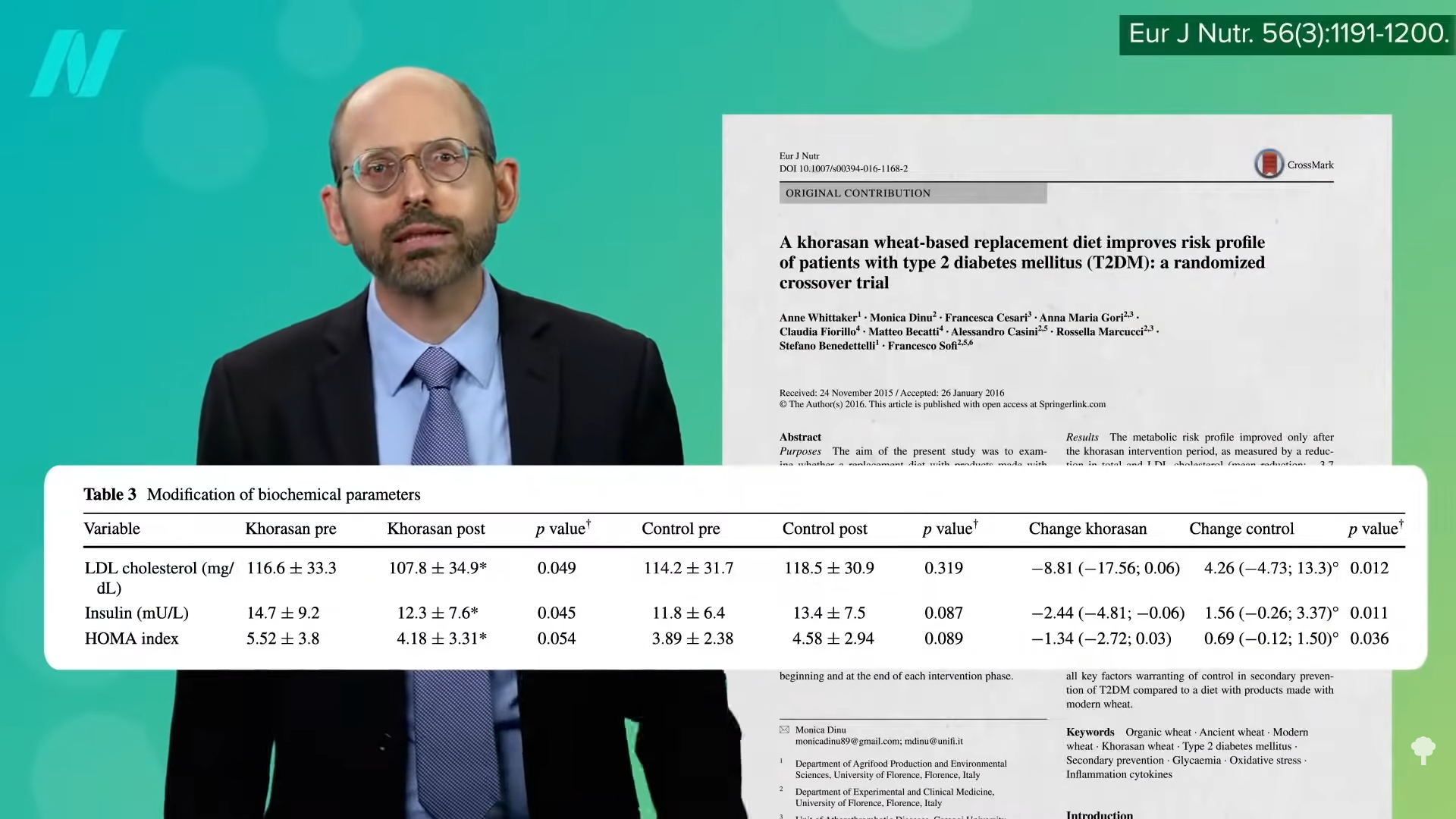
People with diabetes, had better cholesterol and better insulin sensitivity on the same ancient grain, as shown below and at 3:57.
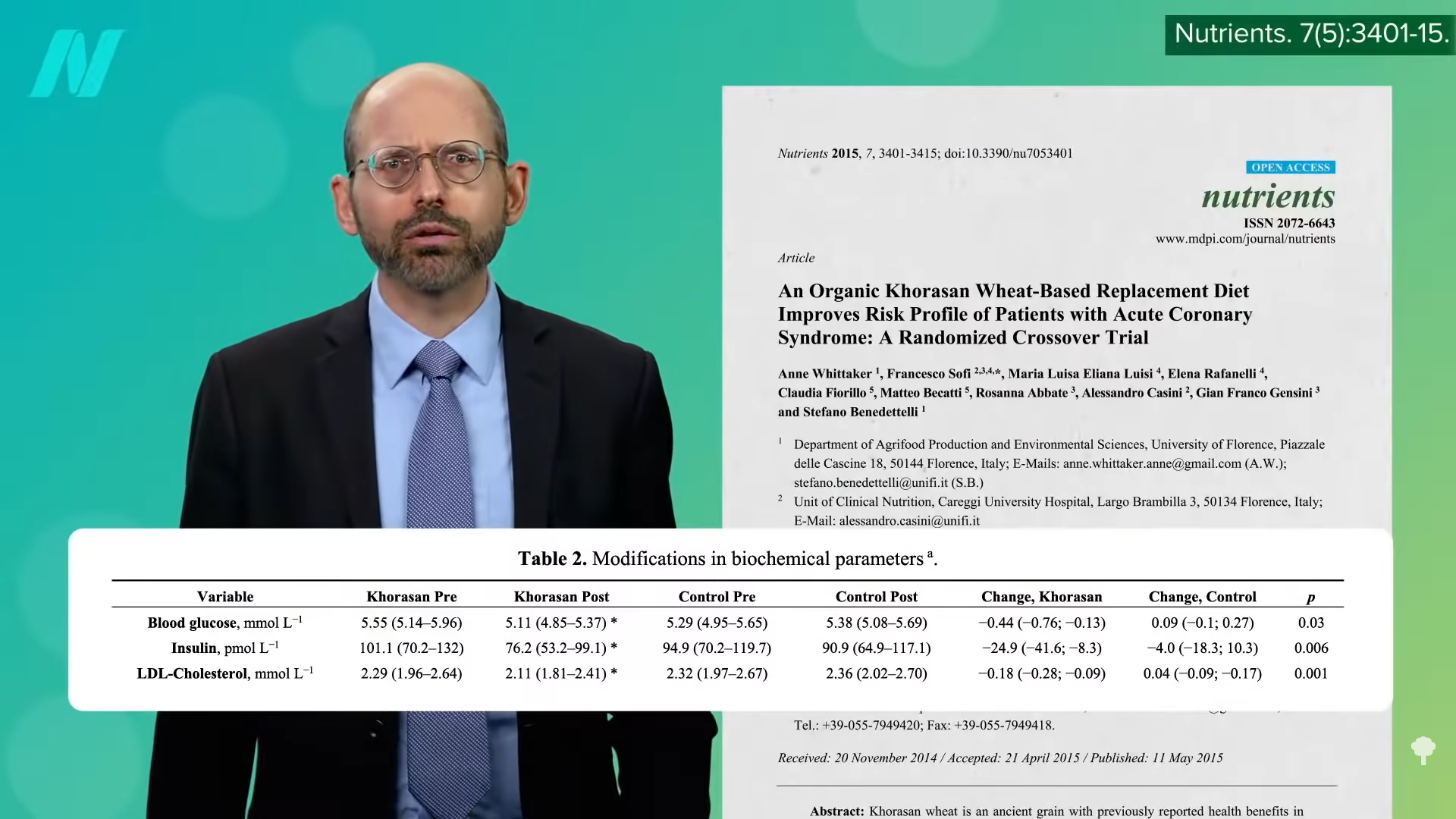
And those with heart disease? They had better blood sugar control and better cholesterol, as shown below and at 4:03.
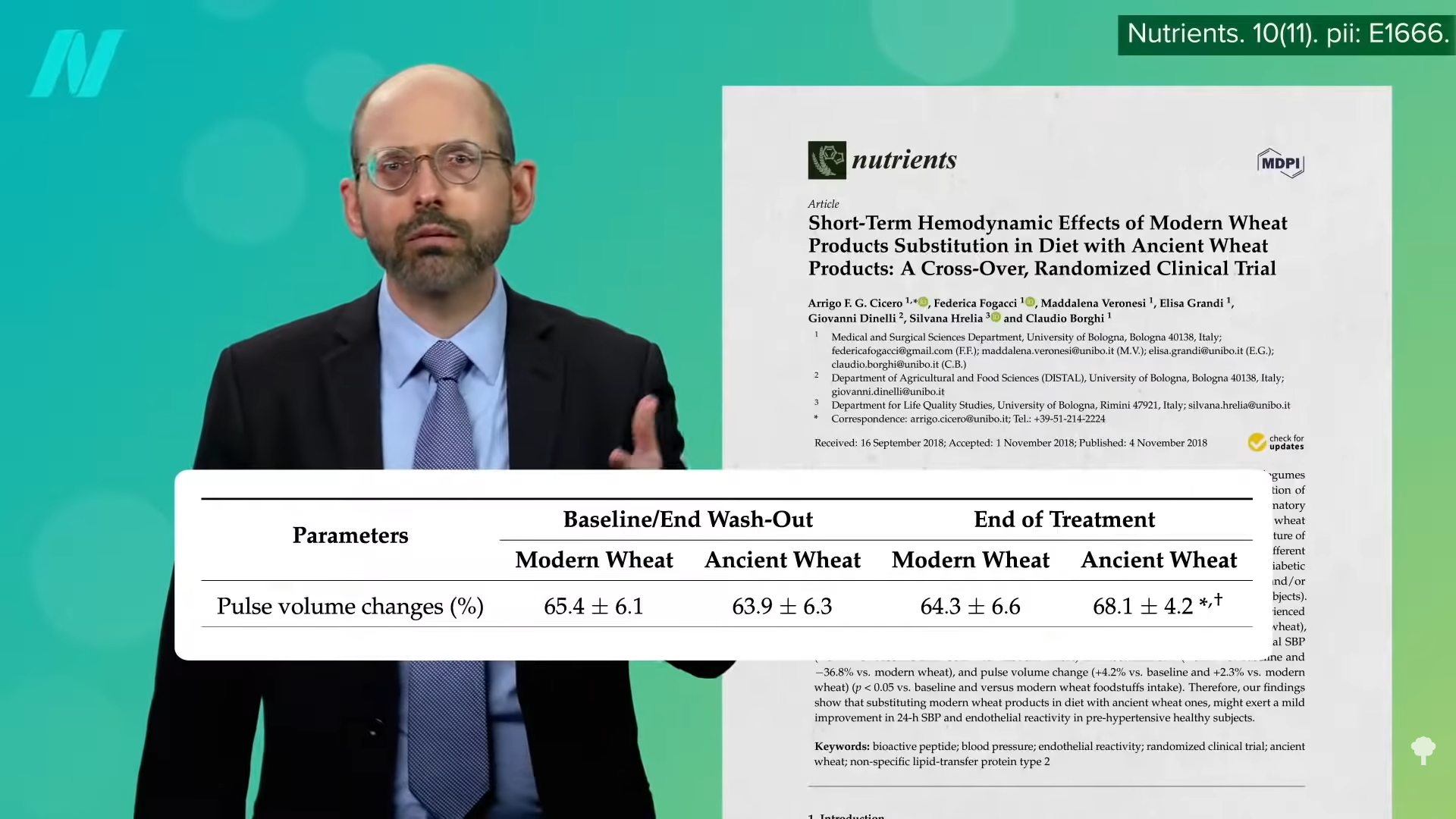
And, people without overt heart disease had better artery function, as you can see below and at 4:06 in my video.
The bottom line is that findings derived from human studies suggest that ancient wheat products are more anti-inflammatory and may improve things like blood sugar control and cholesterol. “Given that the overall number of human interventional trials conducted to date are numerically insufficient, it is not possible to definitively conclude that ancient wheat varieties are superior to all commercial, modern wheat counterparts in reducing chronic disease risk.” However, the best available data do suggest they’re better for us.
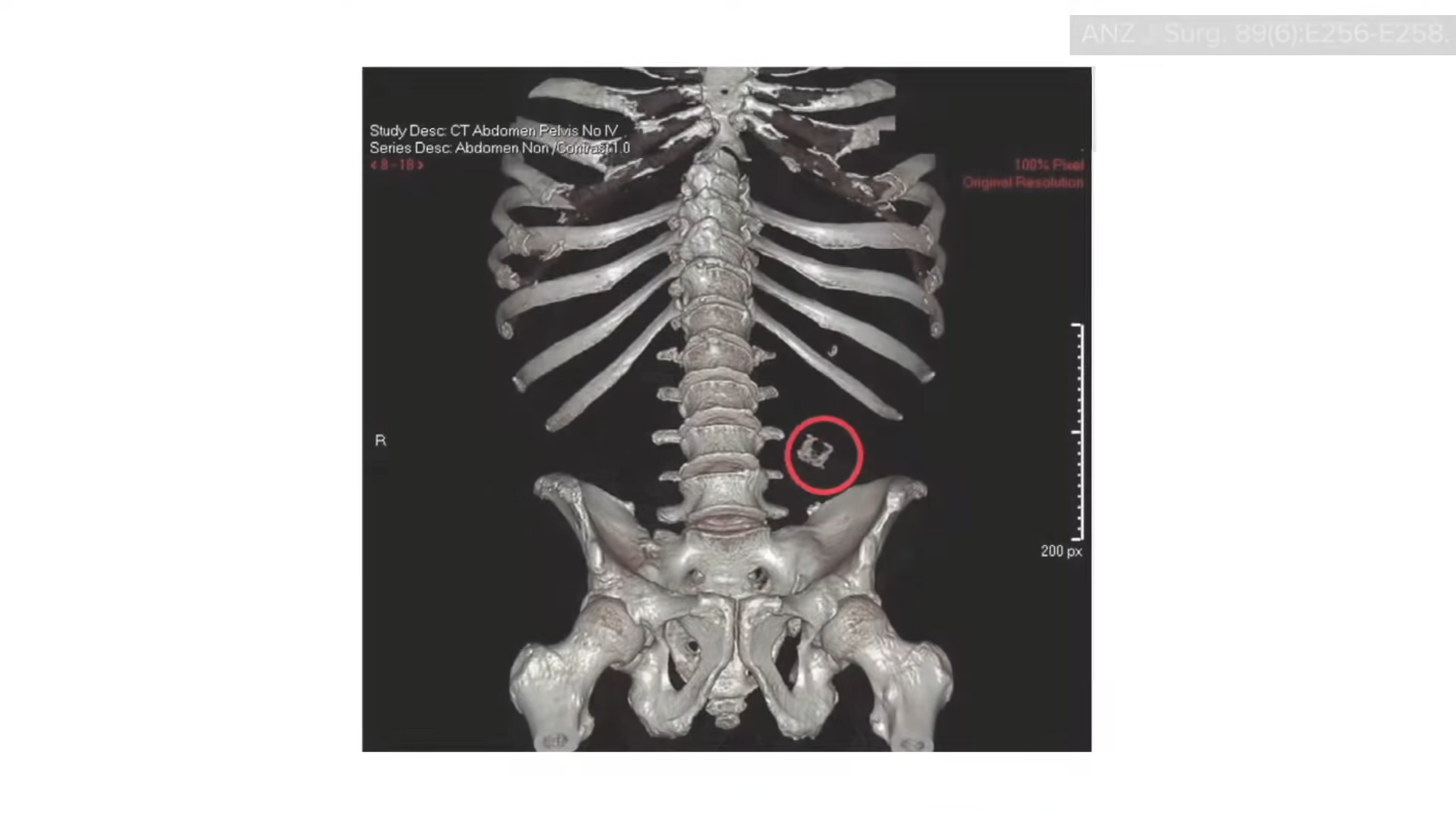
Regardless of what type of wheat you may eat, a word to the wise: Don’t eat the plastic bread-bag clip. A 45-year-old man presented with bloody stools, and his CT scan showed the offending piece of plastic from his bag of bread, as you can see below and at 4:53 in my video. When the patient was questioned, he “admitted to habitually eating quickly without chewing properly.”
Whole grains—ideally intact ones and ancient and modern varieties alike—are an integral part of my Daily Dozen checklist, the healthiest of healthy things I encourage everyone to try to fit into their daily routines.
Whole grains are especially good for our microbiome. Learn more in the related posts below. What about gluten? Also, see the related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
The same meal eaten at the wrong time of day can double blood sugar.
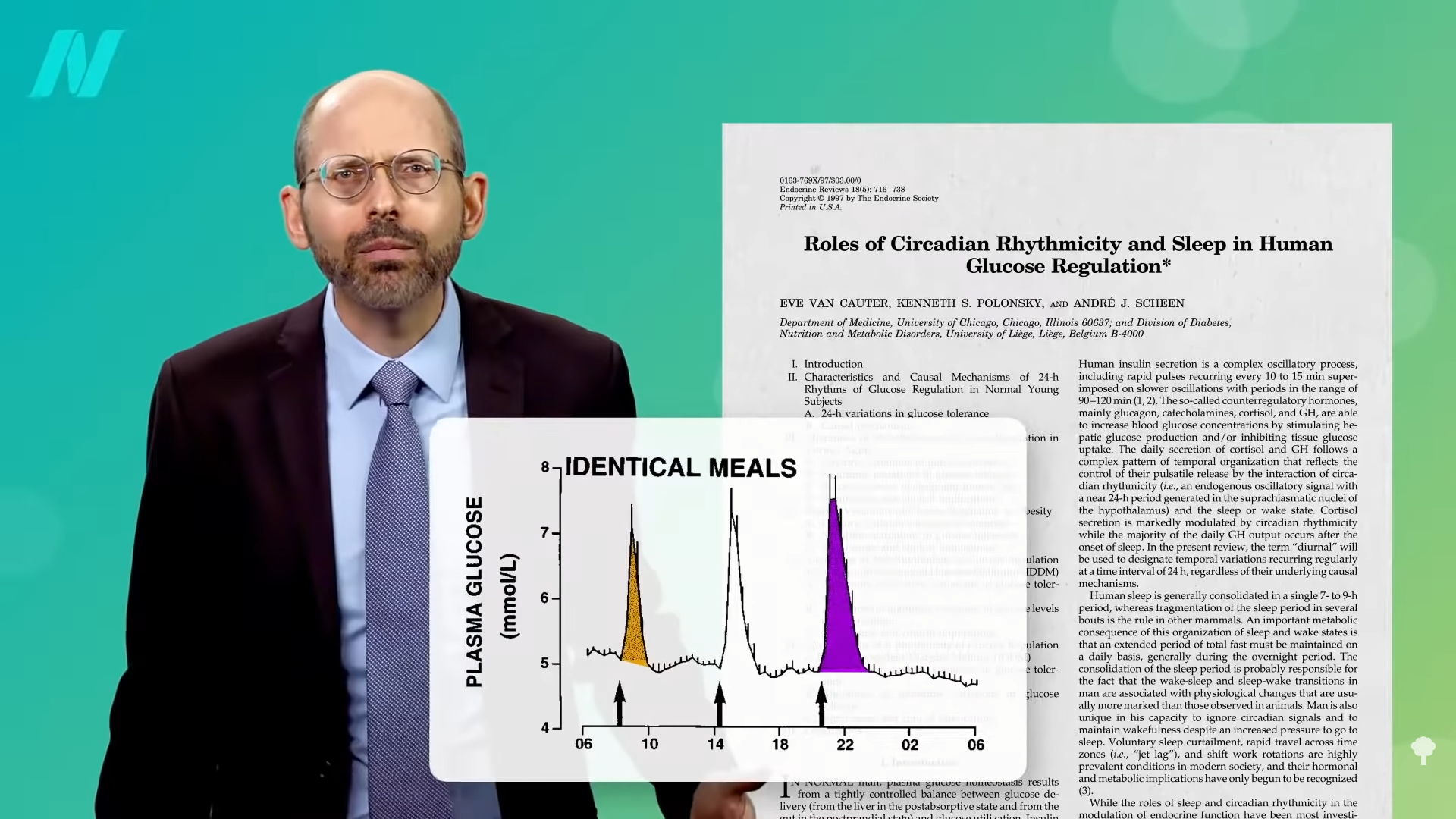
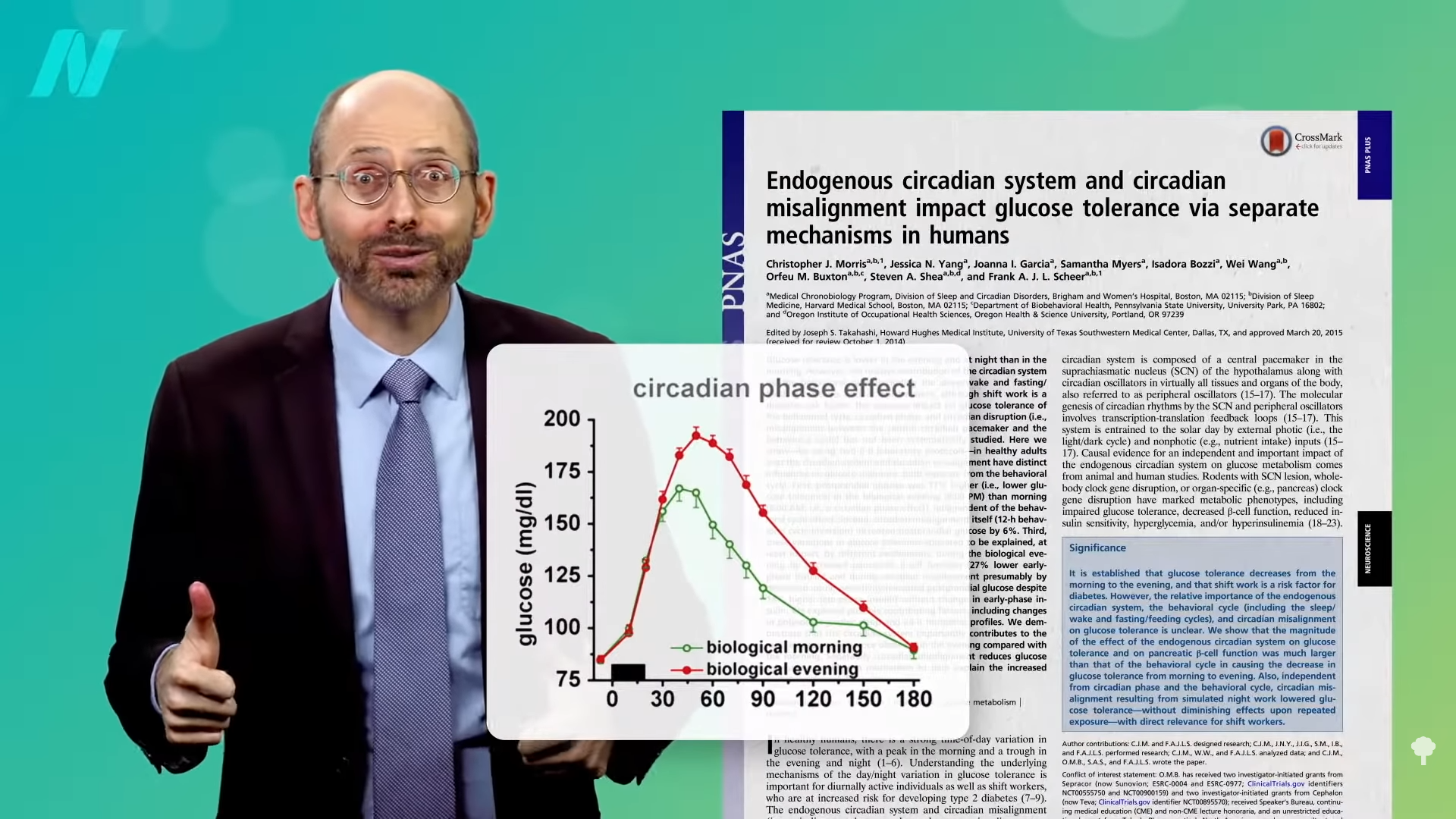
We’ve known for more than half a century that our glucose tolerance—the ability of our body to keep our blood sugars under control—declines as the day goes on. As you can see in the graph below and at 0:25 in my video How Circadian Rhythms Affect Blood Sugar Levels, if you hook yourself up to an IV and drip sugar water into your vein at a steady pace throughout the day, your blood sugars will start to go up at about 8:00 pm, even though you haven’t eaten anything and the infusion rate didn’t change.
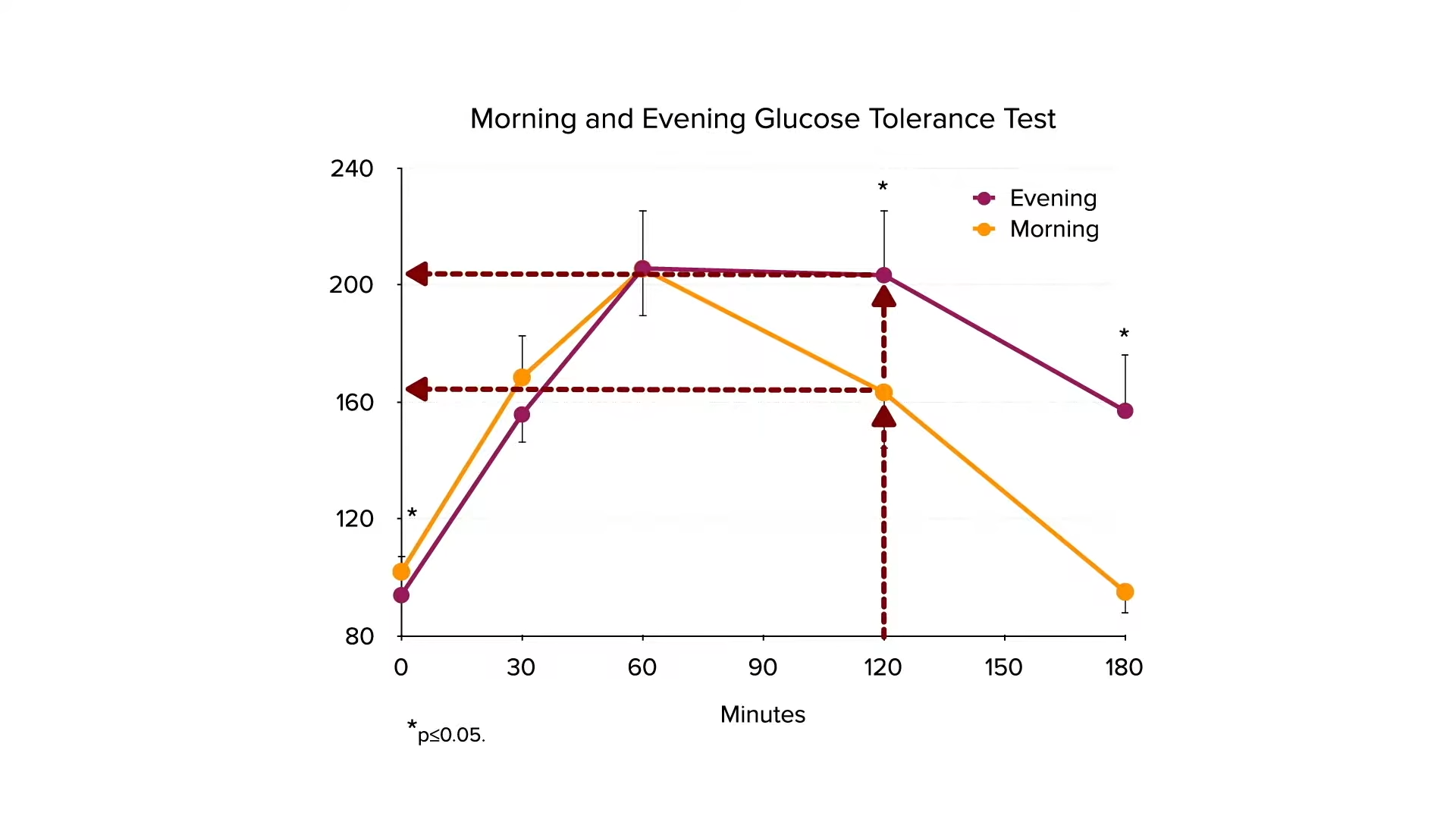
The same amount of sugar is going into your system every minute, but your ability to handle it deteriorates in the evening before bouncing right back in the morning. A meal eaten at 8:00 pm can cause twice the blood sugar response as an identical meal eaten at 8:00 am, as shown in the graph below and at 0:51 in my video. It’s as if you ate twice as much. Your body just isn’t expecting you to be eating when it’s dark outside. Our species may have only discovered how to use fire about a quarter million years ago. We just weren’t built for 24-hour diners.
One of the tests for diabetes is called the glucose tolerance test, which sees how fast our body can clear sugar from our bloodstream. You swig down a cup of water with about four and a half tablespoons of regular corn syrup mixed in, then have your blood sugar measured two hours later. By that point, your blood sugar should be under 140 mg/dL. Between 140 and 199 is considered to be a sign of prediabetes, and 200 and up is a sign of full-blown diabetes, as you can see in the graph below and at 1:37 in my video.
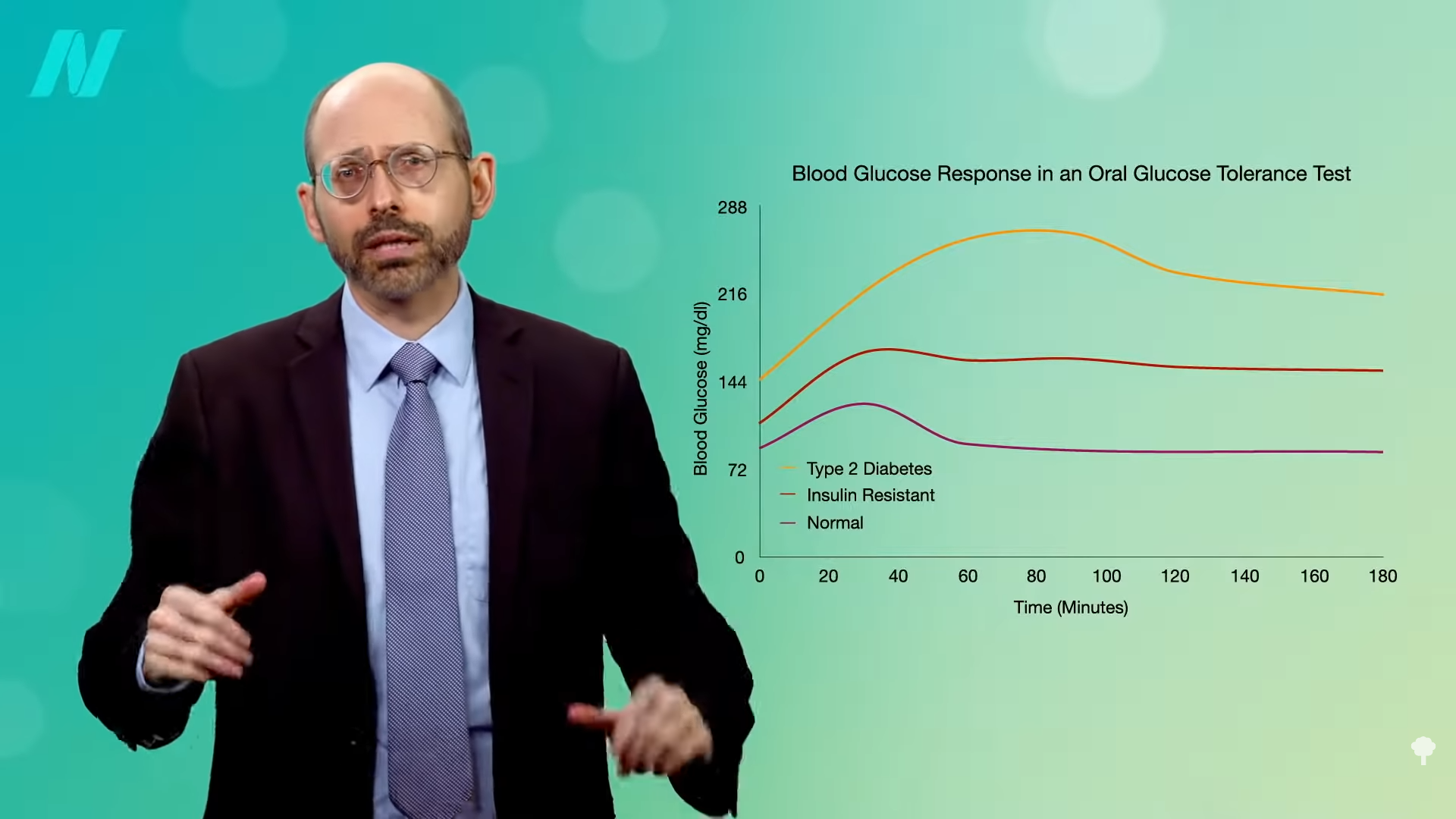
The circadian rhythm of glucose tolerance is so powerful that a person can test normal in the morning but as a prediabetic later in the day. Prediabetics who average 163 mg/dL at 7:00 am may test out as frank diabetics at over 200 mg/dL at 7:00 pm, as you can see in the graph below and at 1:53 in my video.
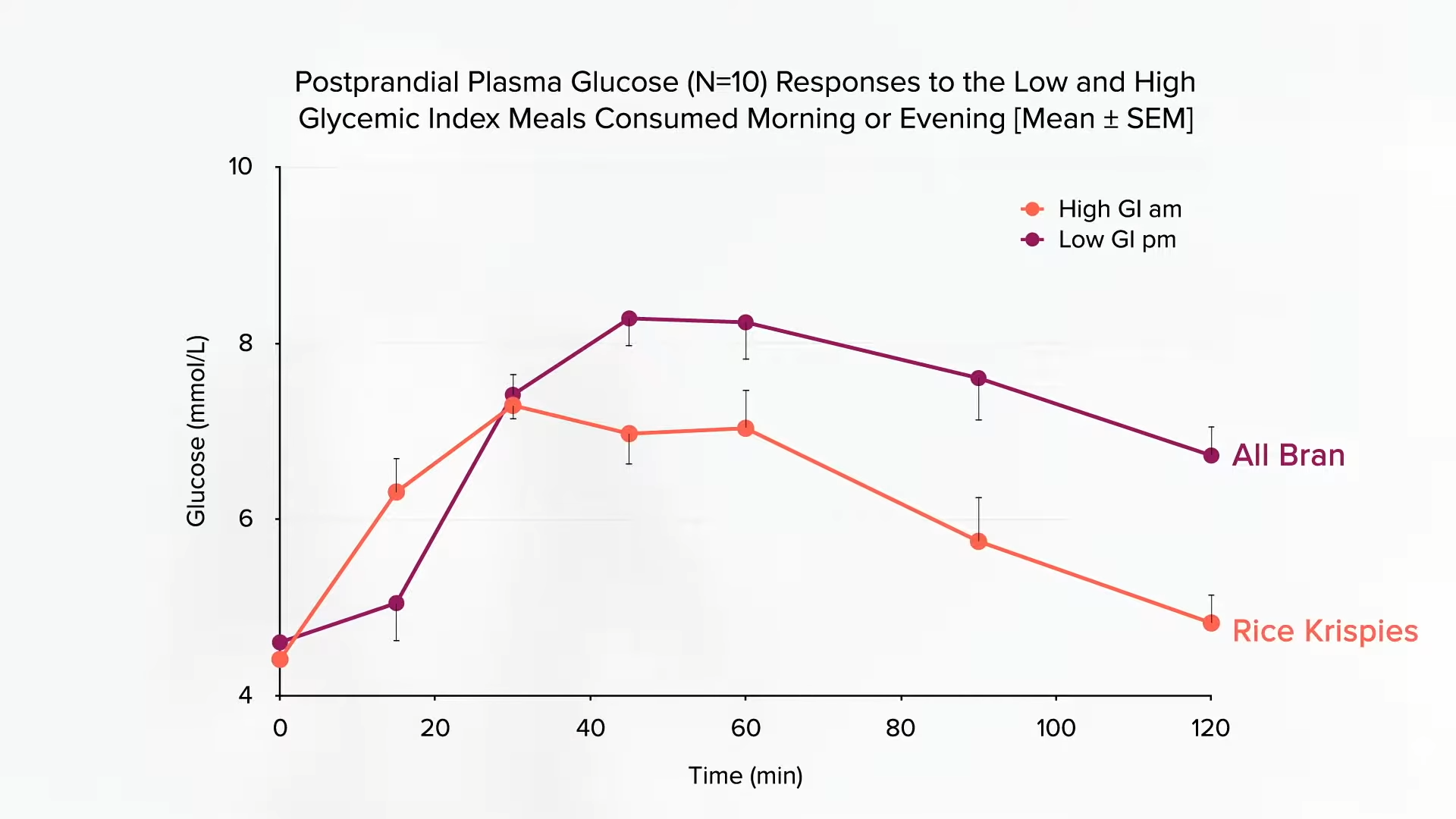
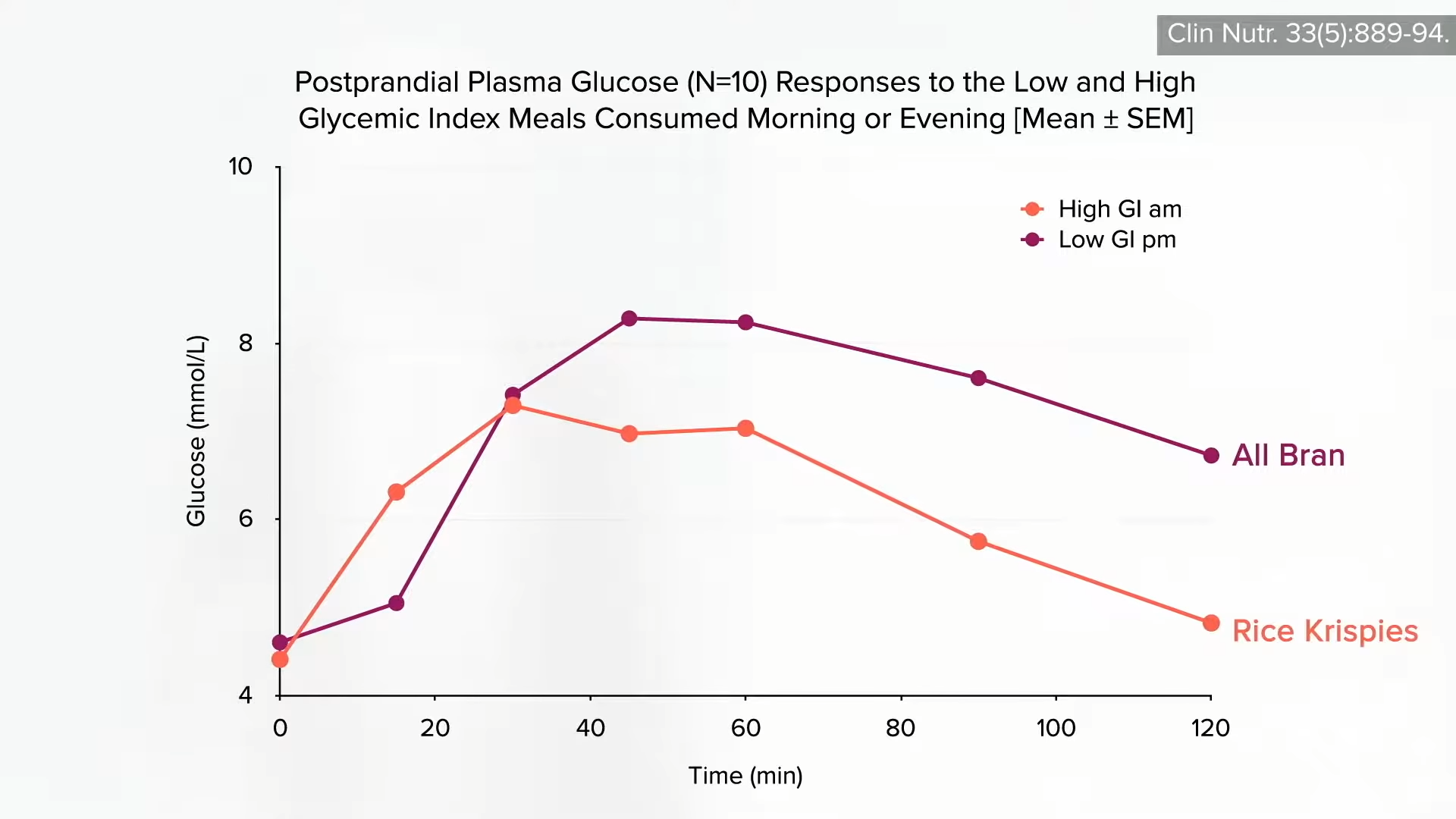
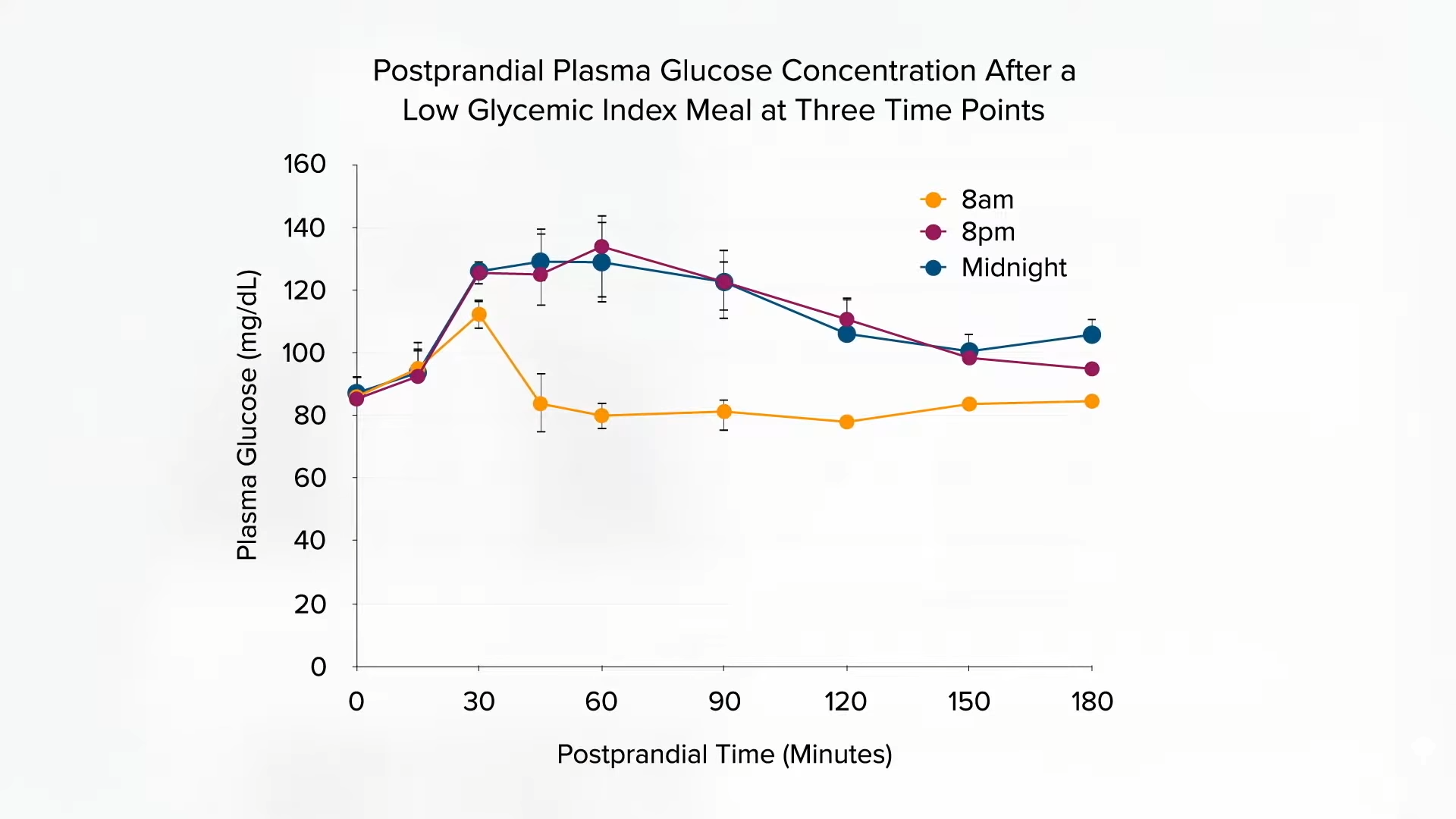
Choosing lower glycemic foods may help promote weight loss, but timing is critical. Due to this circadian pattern in glucose tolerance, a low-glycemic food at night can cause a higher blood sugar spike than a high-glycemic food eaten in the morning, as you can see below and at 2:05 in my video.
We’re so metabolically crippled at night that researchers found that eating a bowl of All Bran cereal at 8:00 pm caused as high a blood sugar spike as eating Rice Krispies at 8:00 am, as you can see in the graph below and at 2:23 in my video.
High glycemic foods at night would seem to represent the worst of both worlds. So, if you’re going to eat refined grains and sugary junk, it might be less detrimental in the morning, as you can see in the graph below and at 2:32 in my video.
The drop in glucose tolerance over the day could therefore help explain the weight-loss benefits of frontloading calories towards the beginning of the day. Even just taking lunch earlier versus later may make a difference, as you can see in the graph below and at 2:48 in my video.
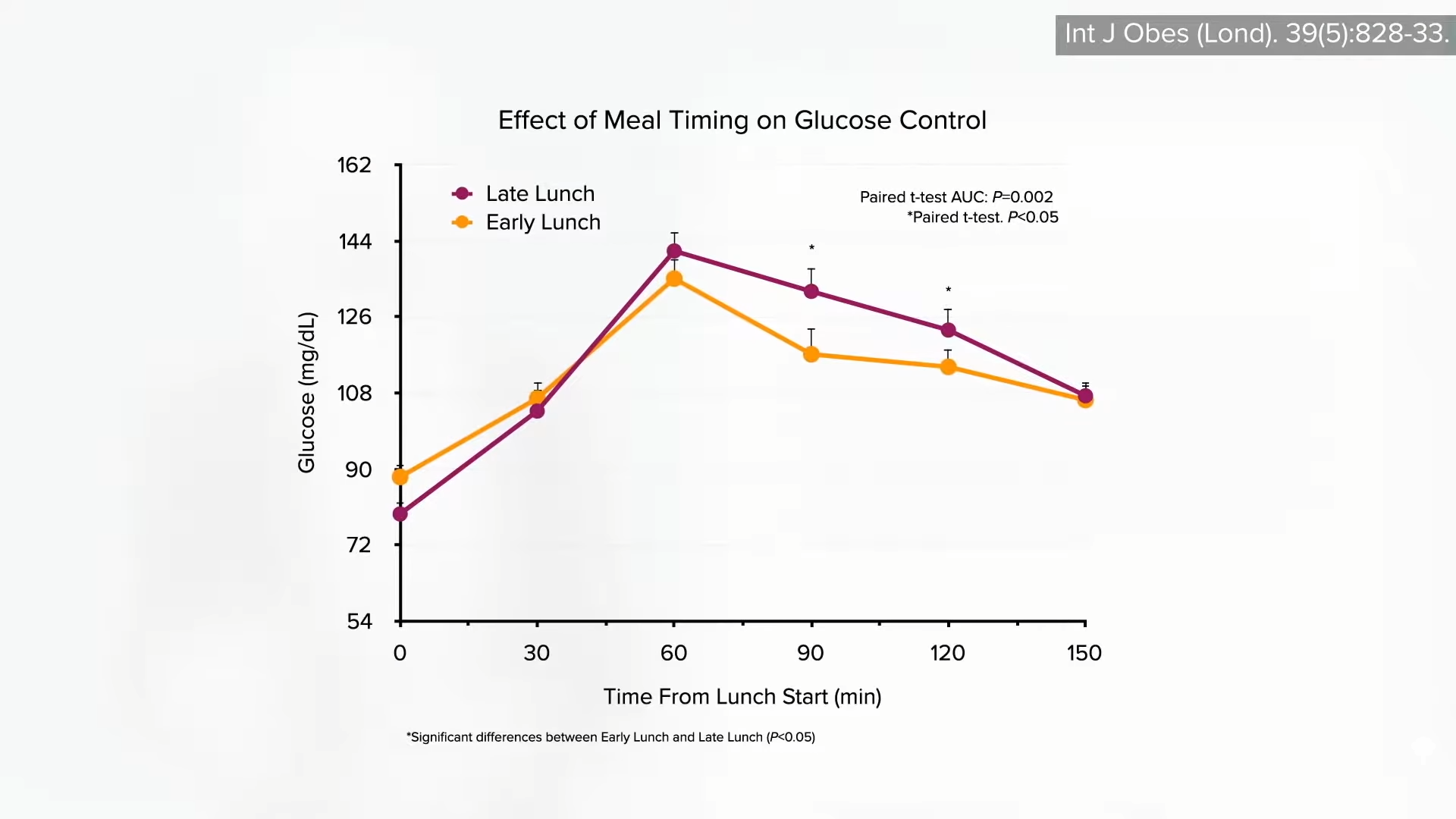
People randomized to eat a large lunch at 4:30 pm suffered a 46 percent greater blood sugar response compared to an identical meal eaten just a few hours earlier at 1:00 pm. A meal at 7:00 am can cause 37 percent lower blood sugars than an identical meal at 1:00 pm, as you can see below, and at 3:04 in my video.
Now, there doesn’t seem to be any difference between a meal at 8:00 pm and the same meal at midnight; they both seem to be too late, as you can see below, and at 3:15 in my video.
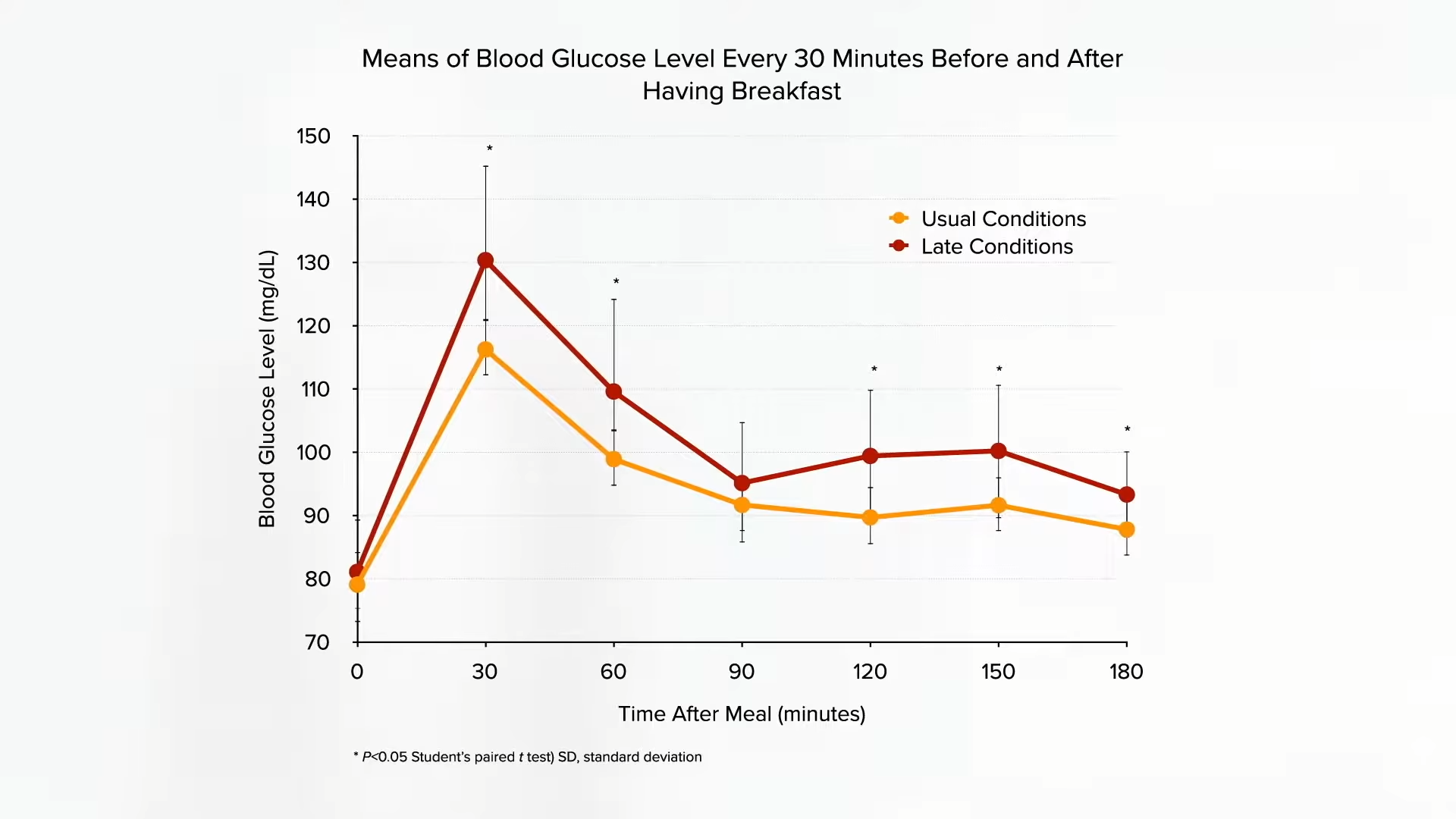
But, eating that late, at midnight or even 11:00 pm, can so disrupt your circadian rhythm that it can mess up your metabolism the next morning, resulting in significantly higher blood sugars after breakfast, compared to eating the same dinner at 6:00 pm the evening before, as shown in the graph below and at 3:32 in my video.
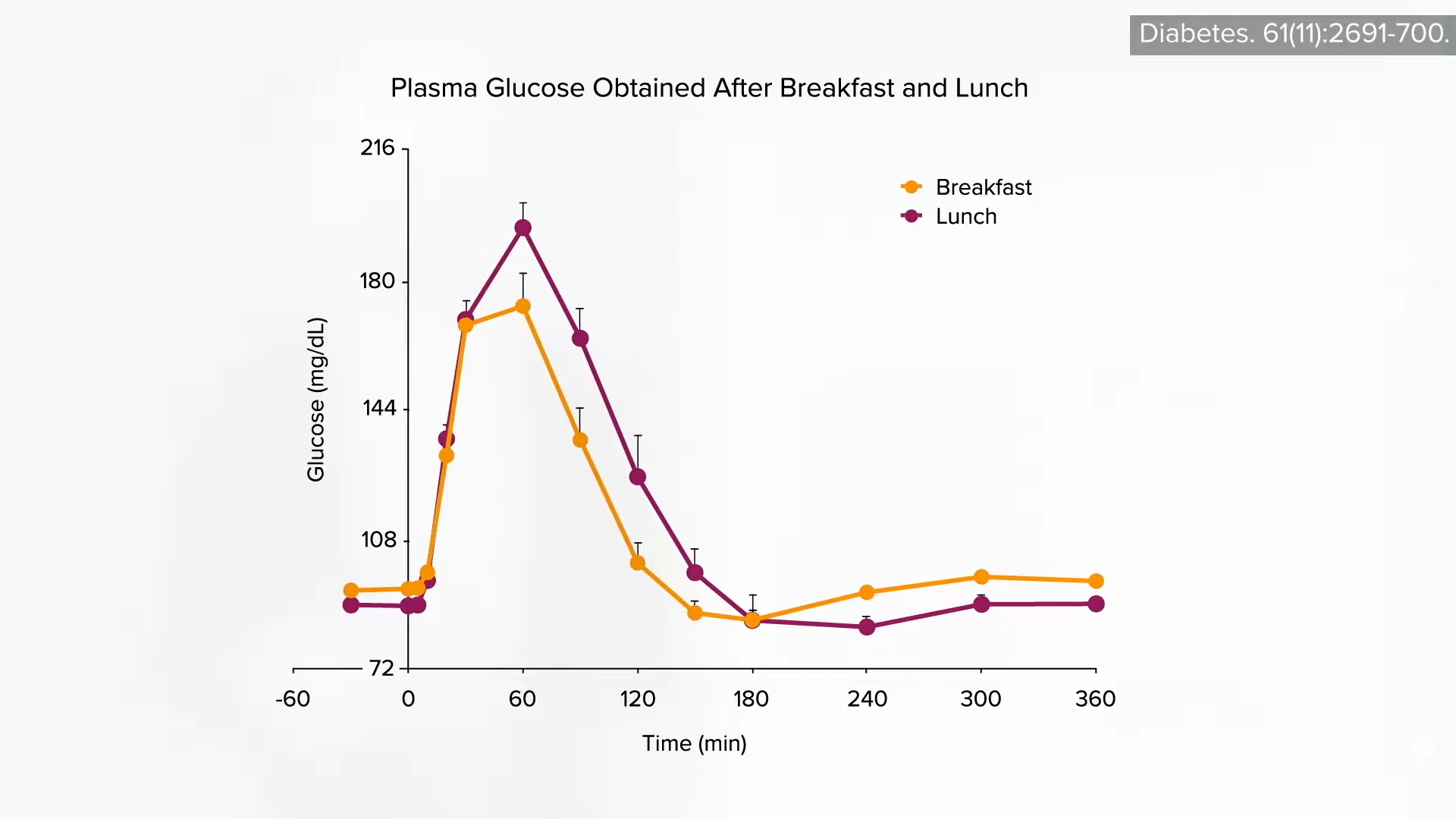
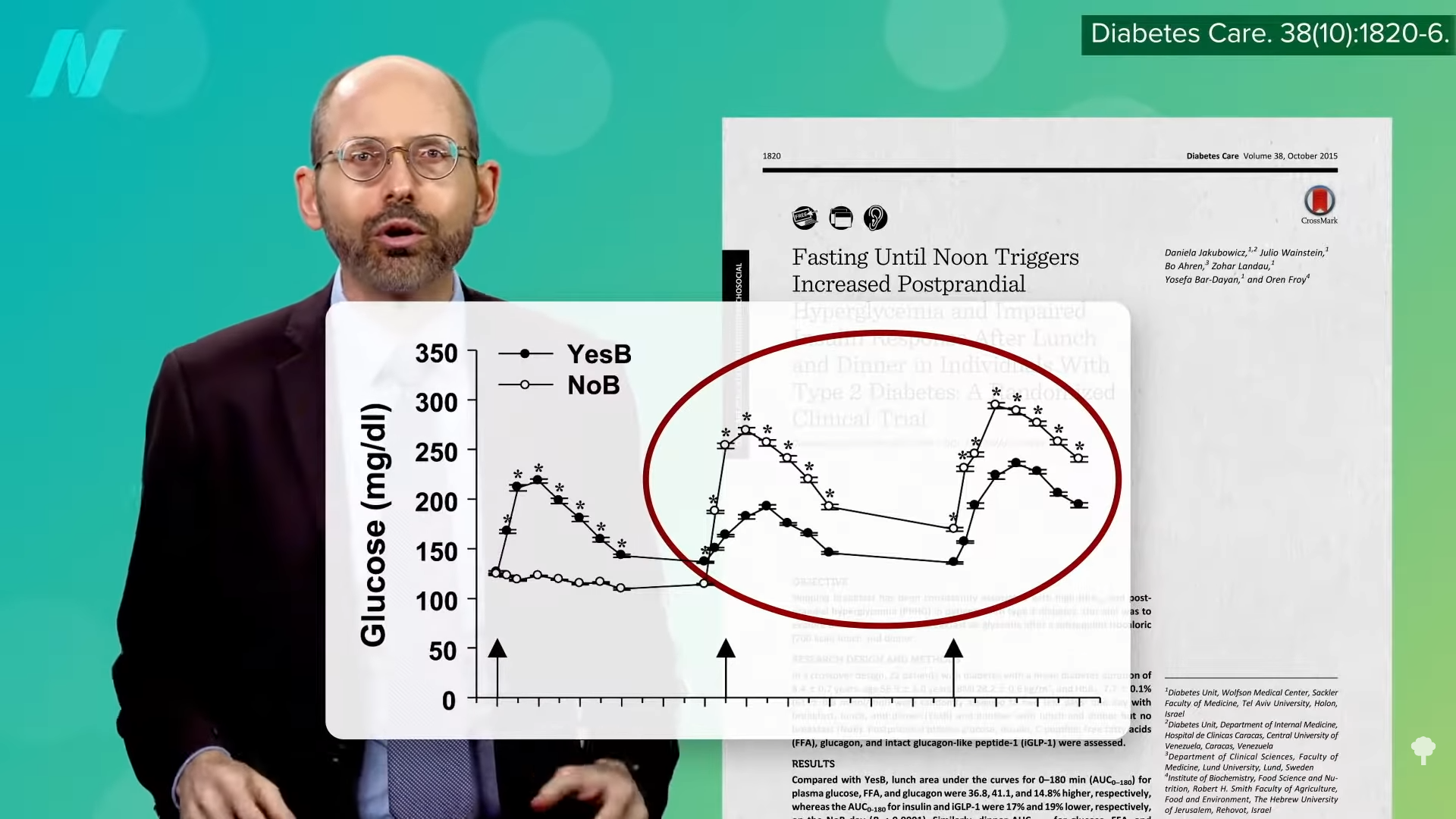
So, these revelations of chronobiology bring the breakfast debate full circle. Skipping breakfast not only generally fails to cause weight loss, but it worsens overall daily blood sugar control in both diabetic individuals and people who are not diabetic, as you can see in the graph below and at 3:44 in my video.
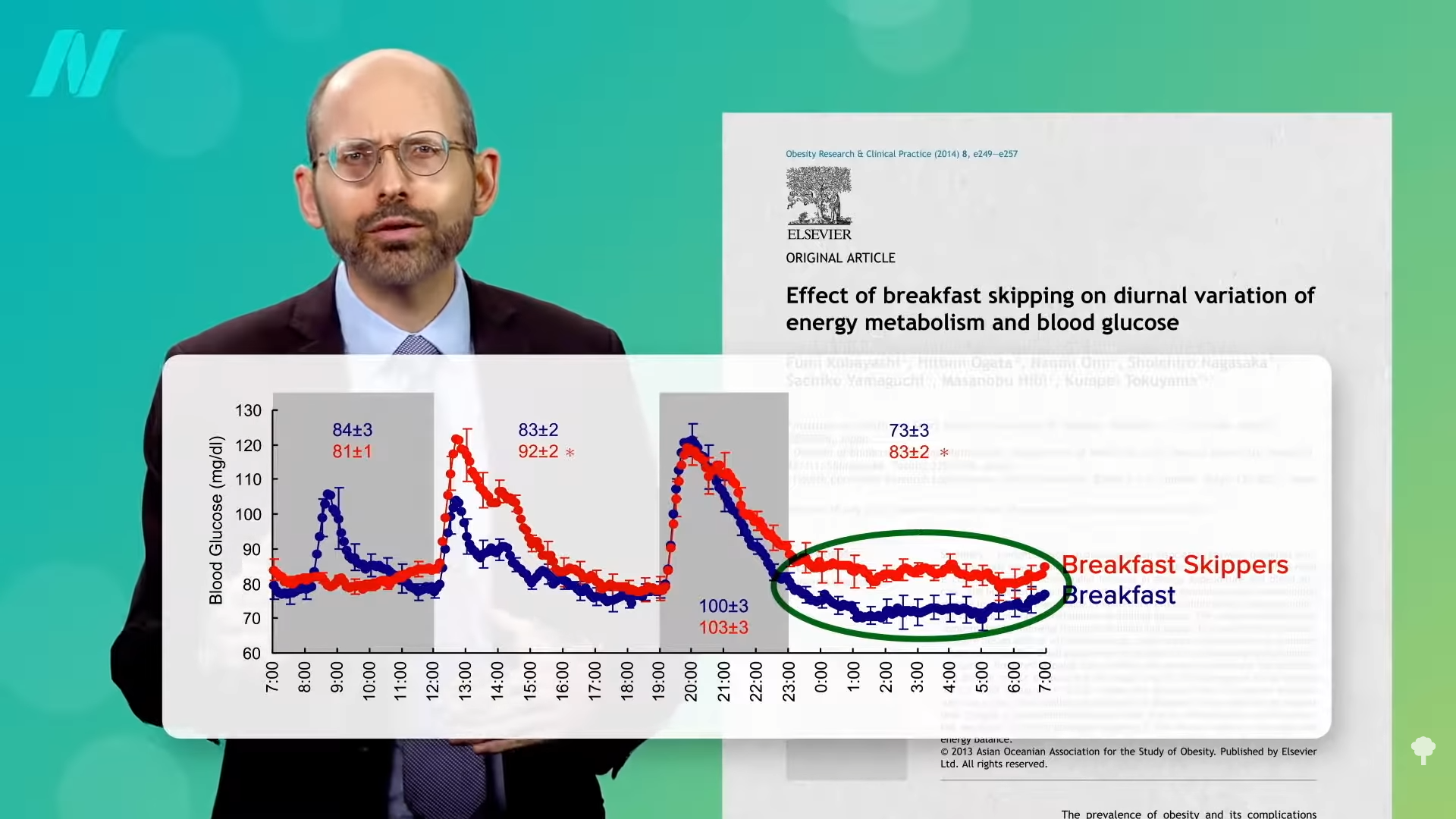
Below and at 3:53, you can see a graph showing how the breakfast skippers have higher blood sugars even while they’re sleeping 20 hours later. This may help explain why those who skip breakfast appear to be at higher risk of developing type 2 diabetes in the first place.
Breakfast skippers also tend to have higher rates of heart disease, as well as having higher rates of atherosclerosis, in general. Is this just because “skipping breakfast tends to cluster with other unhealthy choices, including smoking” and sicklier eating habits overall? The link between skipping breakfast and heart disease—even premature death in general—seems to survive attempts to control for these confounding factors, but you don’t really know until you put it to the test.
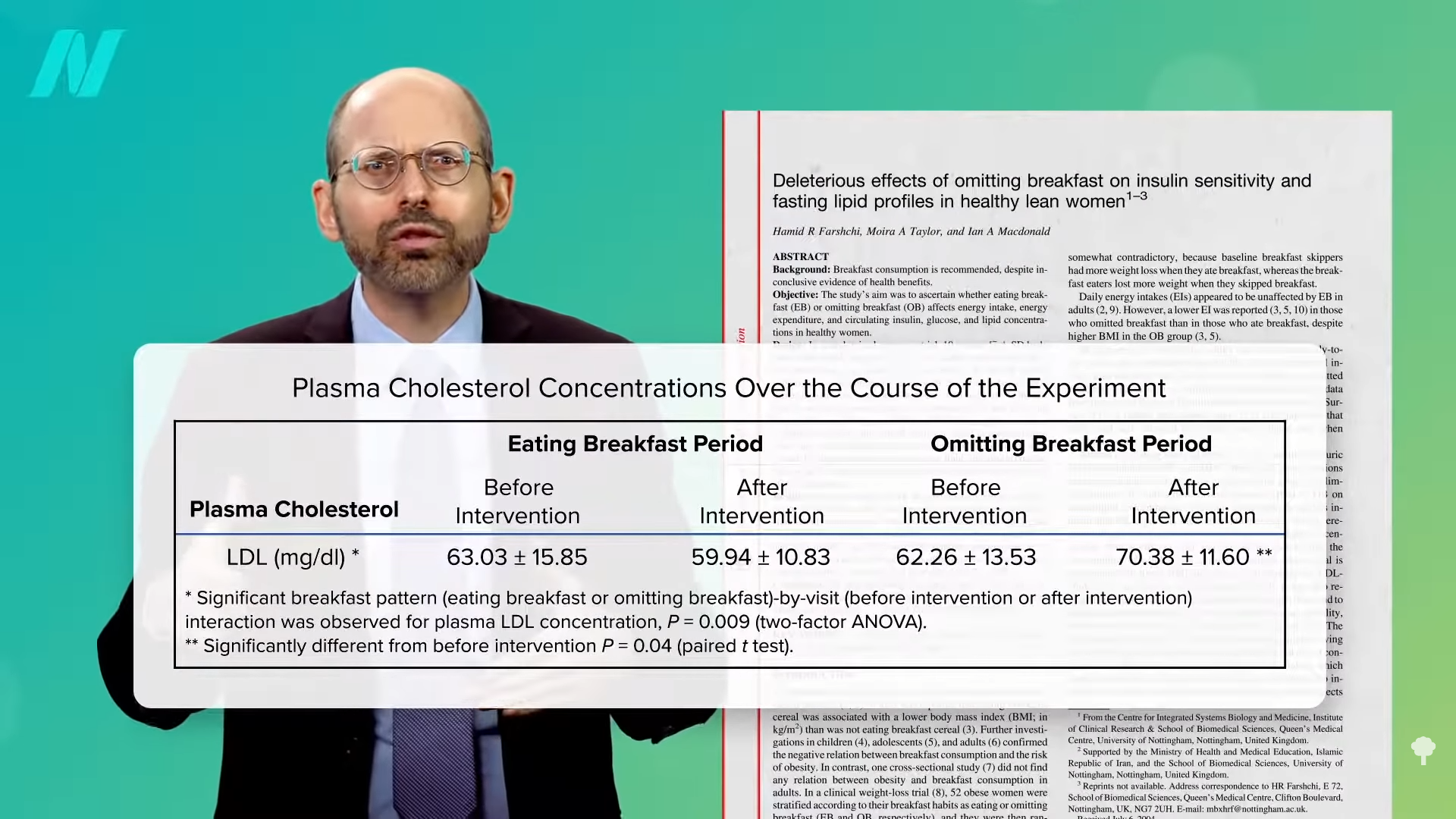
Does skipping breakfast lead to higher cholesterol, for example? Yes, researchers found a significant rise in LDL (bad) cholesterol in study participants randomized to skip breakfast; they were about 10 points higher within just two weeks, as you can see below and at 4:45 in my video.
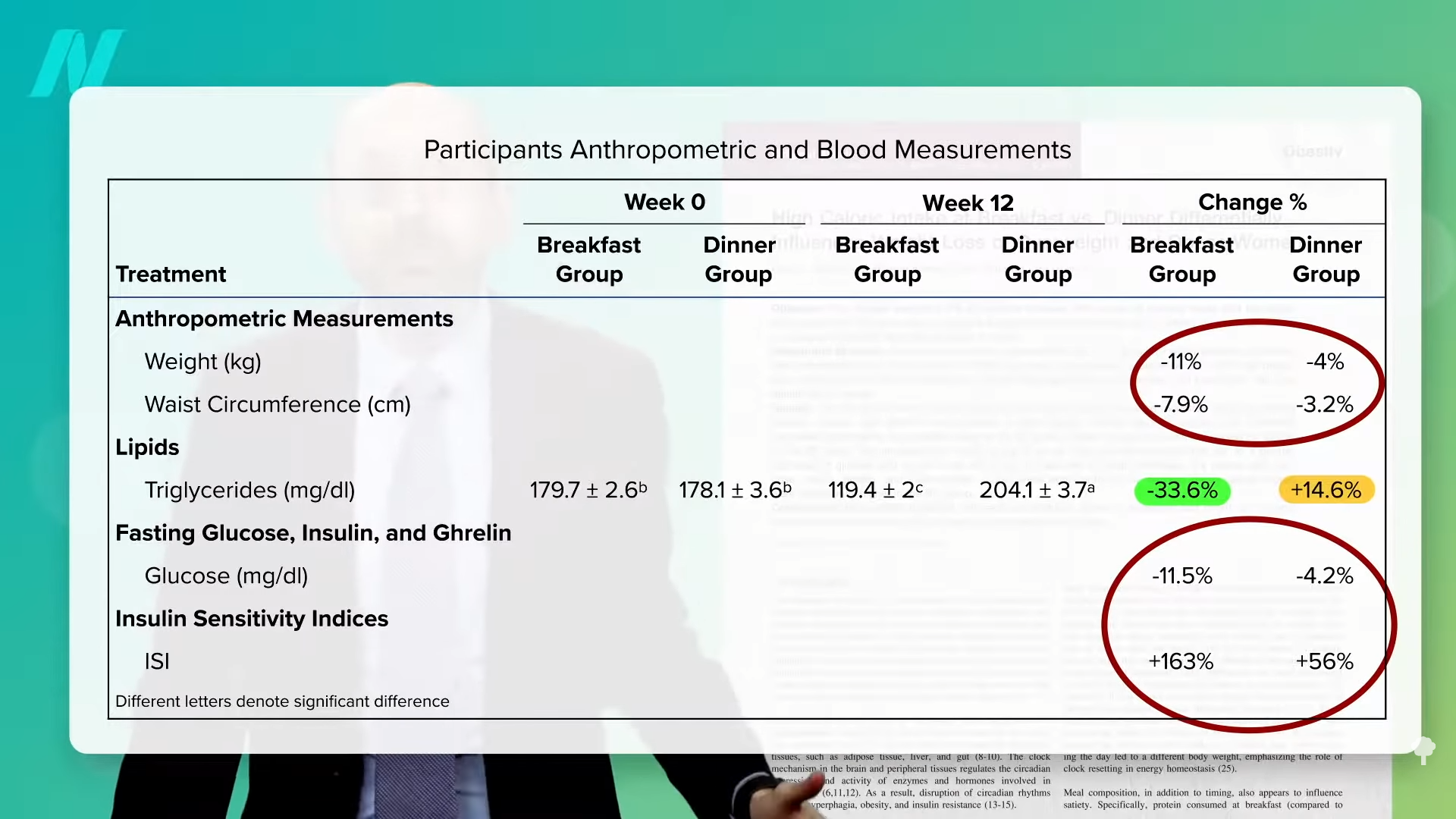
The Israeli study with the caloric distribution of 700 calories for breakfast, 500 for lunch, and 200 for dinner that I’ve discussed previously found that the triglycerides of the king-prince-pauper group (those eating more at breakfast versus dinner) got significantly better—a 60-point drop—while those of the pauper-prince-king group got significantly worse (a 26-point rise). So, consuming more calories in the morning relative to the evening may actually have a triple benefit: more weight loss, better blood sugar control, and lower heart disease risk, as you can see below and at 5:18 in my video.
If you’re going to skip any meal, whether you’re practicing intermittent fasting or time-restricted feeding (where you try to fit all of your food intake into a certain time window each day), it may be safer and more effective to skip dinner rather than breakfast.
I’m back with the next installment of the chronobiology series! I previously explored eating breakfast for weight loss (Is Breakfast the Most Important Meal for Weight Loss? and Is Skipping Breakfast Better for Weight Loss?), introduced chronobiology (How Circadian Rhythms Can Control Your Health and Weight), and looked at the science on eating more in the mornings than the evenings (Eat More Calories in the Morning to Lose Weight, Breakfast Like a King, Lunch Like a Prince, Dinner Like a Pauper, and Eat More Calories in the Morning Than the Evening).
Next, you’ll see How to Sync Your Central Circadian Clock to Your Peripheral Clocks.
The series will wrap up in the next couple of weeks. See videos and blogs in related posts below.
Note: The Israeli 700/500/200 study that I mentioned is detailed in the Breakfast Like a King, Lunch Like a Prince, Dinner Like a Pauper video if you want to know more. Also, check the corresponding blog in related posts.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
OMAHA, Neb. — When Creighton basketball player Isaac Traudt’s teammates take a break at practice, they might grab a drink of water, chat it up or go over assignments.
Traudt does that, too, but not before he checks a device attached to his body that tells him his blood glucose level. Depending on what it says, he might need to grab some energy chews for a sugar bump. The routine is the same at halftime of games.
“I don’t think I’ve ever seen anybody put down a packet of chews faster than Isaac,” athletic trainer Ben McNair said. “He can probably put a pack of those down in 10 to 15 seconds.”
Traudt was diagnosed with Type 1 diabetes 16 years ago, at age 4, and he’s never let it stop him from pursuing the sport he loves. He will be with the Bluejays on Thursday when they open the NCAA Tournament against Akron in Pittsburgh.
The 6-foot-10, 235-pound forward grew up in Grand Island, 130 miles west of Omaha, and was a two-time all-state player and Nebraska high school player of the year in 2022. He spent his first college season at Virginia, sitting out as a redshirt, and announced his transfer to Creighton last March.
Traudt has appeared in 28 of the Bluejays’ 32 games, averaging just under 10 minutes per game and shooting 43.6% on 3-pointers. He started two games early in the season, and made five 3s and scored a season-high 18 points off the bench against Central Michigan.
Former NBA players Chris Dudley, Adam Morrison and Gary Forbes and former WNBA player Lauren Cox are among the high-level basketball players who have had to manage diabetes.
Traudt said he has had a number of parents of recently diagnosed children ask him to give their kids encouragement.
“It’s just important for them to know their dreams can still be accomplished,” Traudt said. “They can still compete in their sports. I think that’s what a lot of them worry about. I just want to inspire them and show you can play at the highest level.
“It doesn’t really matter if you have diabetes or not. It just takes more responsibility. It’s more demanding, but at the end of the day it’s possible.”
Dr. Lori Laffel, an endocrinologist and clinical investigator who works with children and young adults at the Harvard Medical School’s Joslin Diabetes Center, said technological advances have made it easier for athletes to manage their diabetes.
In the 1950s, she said, people diagnosed with Type 1 diabetes were discouraged from engaging in strenuous physical activity because of the dangers of low blood glucose. Later research showed positive effects from exercise, but athletes had to go through the inconvenience of pricking their fingers in practices and games to check their glucose.
In recent years, athletes have used continuous glucose monitors that communicate with insulin pumps to maintain glucose levels in their target ranges. The CGM sends readings to an app on the athlete’s phone showing glucose levels at five-minute intervals and also whether it is trending higher or lower.
Traudt said he had daily insulin injections until he switched at age 7 to an insulin pump. The modern insulin pump that he now uses can automatically adjust insulin, for example, delivering more insulin if his glucose goes too high and reducing insulin delivery when it goes too low. The pump and Dexcom CGM, which he has used since he was 13, are attached to his body under his uniform.
“Obviously, in my short lifetime it’s come a really long way,” he said. “Compared to 40 years ago, I couldn’t even imagine going through this without the technology. It would be really difficult.”
He doesn’t really need the CGM to know when his body is out of whack. When his blood sugar is low, he gets dizzy and fatigued. When it’s high, he gets thirsty and has body aches.
McNair said Traudt does a good job anticipating when he needs to up his blood glucose during practices and games.
“As soon as he feels like he’s going downhill a little bit, we do the chews for the most part and not too long after that he’s pretty much back on the floor,” McNair said.
Laffel, who has not treated Traudt and does not know him, said she can tell from hearing his story he has had strong support from his family and the medical and coaching staffs at Creighton.
“It’s always a thrill,” Laffel said, “when I know people are playing to their potential, working to their potential and thriving while living with Type 1 diabetes.”
___
AP March Madness bracket: https://apnews.com/hub/ncaa-mens-bracket and coverage: https://apnews.com/hub/march-madness
[ad_2]

[ad_1]
(Associated Press) – Yogurt sold in the U.S. can make claims that the food may reduce the risk of type 2 diabetes based on limited evidence.
The U.S. Food and Drug Administration has agreed that eating at least 2 cups of yogurt a week might reduce the risk of the disease.
The agency granted a request for a qualified health claim from Danone North America.
Such claims lack full scientific support but are allowed as long as they include disclaimers.
Other such allowed claims include that some types of cocoa may reduce heart disease and cranberry juice might reduce the risk of recurrent UTIs.
More about:
[ad_2]
Grant McHill
Source link

[ad_1]
Eating every other day can raise your cholesterol.
Are there any downsides to fasting every other day? For example, might go all day without eating impair your ability to think clearly? Surprisingly, as I discuss in my video Is Alternate-Day Intermittent Fasting Safe?, the results appear to be “equivocal.” Some studies show no measurable effects and the ones that do fail to agree on which cognitive domains are affected. Might the cycles of fasting and feasting cause eating disorder–type behaviors, like bingeing? So far, no harmful psychological effects have been found. In fact, there may be some benefit. However, the studies that have put it to the test specifically excluded those with a documented history of eating disorders, for whom the effects may differ.
What about bone health? No change in bone mineral density was noted after six months of alternate-day fasting despite about 16 pounds of weight loss, which would typically result in a dip in bone mass. However, the researchers did not note any skeletal changes in the control group either, and they lost a similar amount of weight using continuous caloric restriction. They suggested this is because both groups tended to be “more physically active than the average obese American,” getting about 1,000 to 2,000 more steps a day.
Proponents of intermittent fasting suggest it can better protect lean body mass, but most of the intermittent trials have employed less accurate methods of body composition analysis, whereas the majority of continuous caloric restriction trials used “vastly more accurate techniques.” So, to date, it is not clear if there’s a difference in lean mass preservation.
Improvements in blood pressure and triglycerides have been noted on intermittent fasting regimens, though this is presumed to be due to the reduction in body fat since the effect appears to be “dependent on the amount of weight lost.” Alternate-day fasting can improve artery function, too, as you can see in the graph below and at 1:55 in my video, though it does depend on what you’re eating on the non-fasting day. For study participants randomized to an alternate-day diet high in saturated fat, their artery function worsened despite a ten-pound weight loss, whereas it improved, as expected, in the lower-fat group. The decline in artery function was presumed to be because of the pro-inflammatory nature of saturated fat.
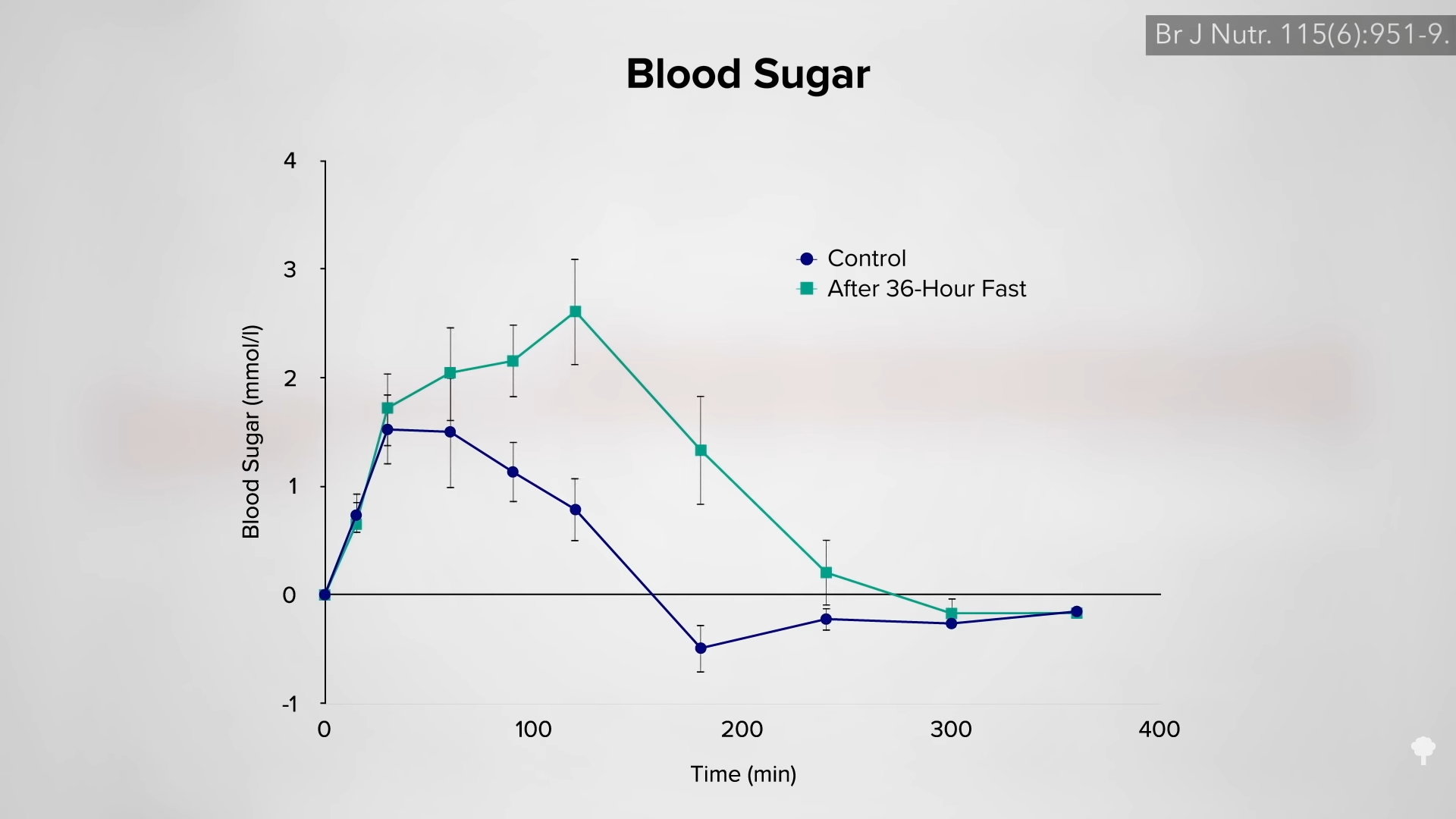
A concern has been raised about the effects of alternate-day fasting on cholesterol. After 24 hours without food, LDL cholesterol may temporarily bump up, but this is presumably because so much fat is being released into the system by the fast. As you can see in the graph below and at 2:33 in my video, an immediate negative effect on carbohydrate tolerance may stem from the same phenomenon—the repeated elevations of free fat floating around in the bloodstream. After a few weeks, though, LDL levels start to drop as the weight comes off. However, results from the largest and longest trial of alternate-day fasting have given me pause.
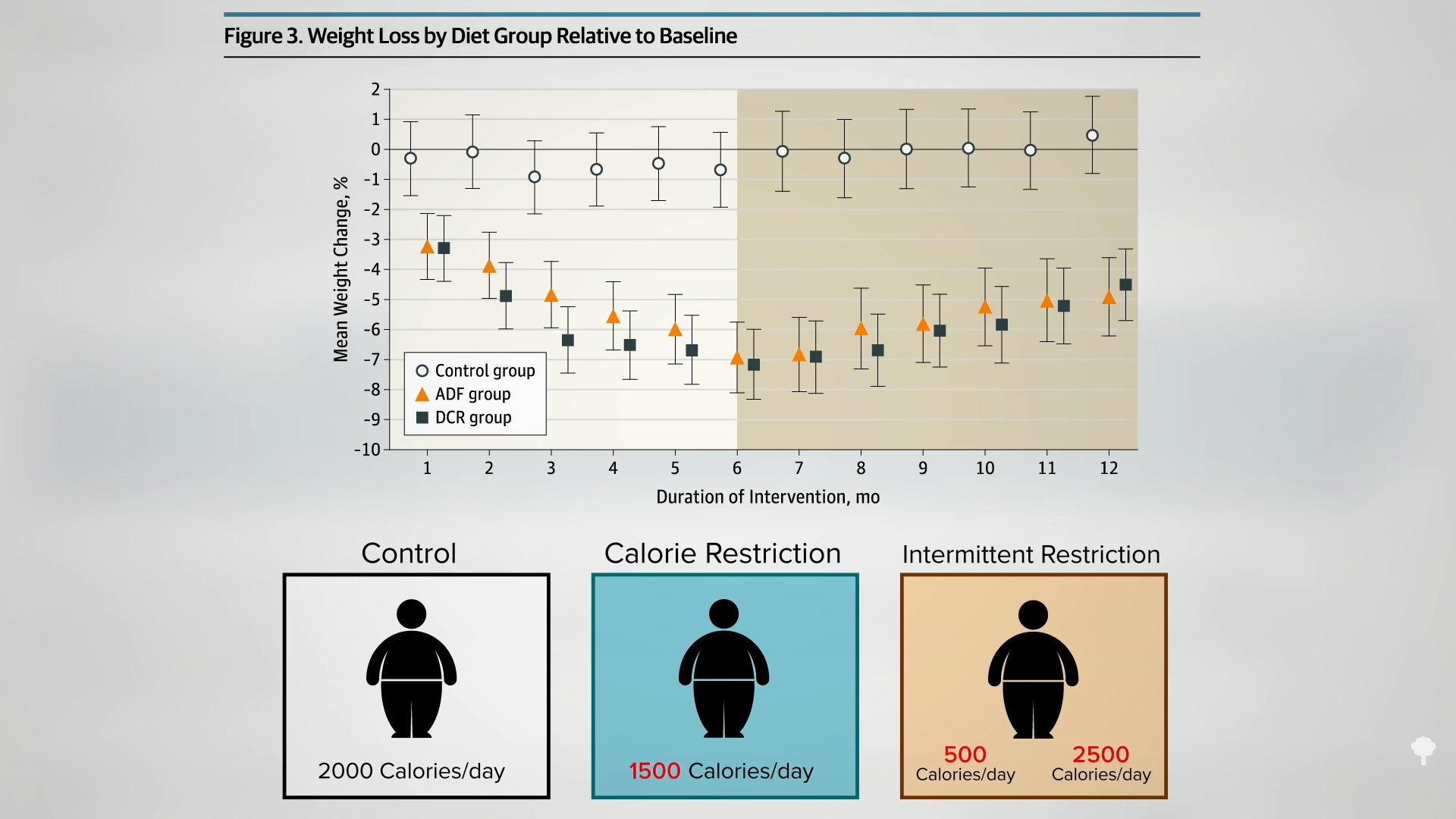
A hundred obese men and women were randomized into one of three groups: alternate-day modified fasting (25 percent of their baseline calories on fasting days and 125 percent calories on eating days), continuous, daily caloric restriction (75 percent of baseline), or a control group instructed to maintain their regular diet. So, for those going into the trial eating 2,000 calories a day, they would continue to eat 2,000 calories a day in the control group. The calorie-restriction group would get 1,500 calories every day, and the intermittent-restriction group would alternate between 500 calories a day and 2,500 calories the next.
As you can see in the graph below and at 3:32 in my video, with the same overall, average, prescribed calorie cutting in the two weight-loss groups, they both lost about the same amount of weight, but, surprisingly, the cholesterol effects were different. In the continuous calorie-restriction group, the LDL levels dropped as expected compared to the control group as the pounds came off.
But, in the alternate-day modified fasting group, they didn’t, as you can see below, and at 3:55 in my video. At the end of the year, the LDL cholesterol in the intermittent fasting group ended up being 10 percent higher than in the constant calorie-restriction group—despite the same loss of body fat. Given that LDL cholesterol is a prime causal risk factor for heart disease, our number one killer—or is even the prime risk factor—this strikes a significant blow against alternate-day fasting. If you want to try it anyway, I would advise you to have your cholesterol monitored to make sure it comes down with your weight.
If you’re diabetic, you must talk with your physician about medication adjustment for any changes in diet, including fasting of any duration. Even with proactive medication reduction, advice to immediately break the fast should sugars drop too low, and weekly medical supervision, people with type 2 diabetes who fasted for even just two days a week were twice as likely to suffer from hypoglycemic episodes compared to an unfasted control group. We still don’t know the best way to tweak blood sugar medications to prevent blood sugar from dropping too low on fasting days.
Even fasting for just one day can significantly slow the clearance of some drugs (like the blood-thinning drug Coumadin) or increase the clearance of others (like caffeine). Fasting for 36 hours can cut your caffeine buzz by 20 percent. So, consultation with your medical professional before fasting is an especially good idea for anyone on any kind of medication.
If you missed it, check out Alternate-Day Intermittent Fasting Put to the Test.
So, with ambiguous cognitive, lean mass, and bone effects, plus these cholesterol findings, I wouldn’t suggest alternate-day fasting for weight loss, but dropping pounds isn’t the only thing this way of eating is purported to do. Check out Does Intermittent Fasting Increase Human Life Expectancy?.
For other types of intermittent fasting, total fasting, and more on fasting, check out the related videos below.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
Newswise — Certain populations of mosquitoes are more heat tolerant and better equipped to survive heat waves than others, according to new research from Washington University in St. Louis.
This is bad news in a world where vector-borne diseases are an increasingly global health concern. Most models that scientists use to estimate vector-borne disease risk currently assume that mosquito heat tolerances do not vary. As a result, these models may underestimate mosquitoes’ ability to spread diseases in a warming world.
Researchers led by Katie M. Westby, a senior scientist at Tyson Research Center, Washington University’s environmental field station, conducted a new study that measured the critical thermal maximum (CTmax), an organism’s upper thermal tolerance limit, of eight populations of the globally invasive tiger mosquito, Aedes albopictus. The tiger mosquito is a known vector for many viruses including West Nile, chikungunya and dengue.
“We found significant differences across populations for both adults and larvae, and these differences were more pronounced for adults,” Westby said. The new study is published Jan. 8 in Frontiers in Ecology and Evolution.
Westby’s team sampled mosquitoes from eight different populations spanning four climate zones across the eastern United States, including mosquitoes from locations in New Orleans; St. Augustine, Fla.; Huntsville, Ala.; Stillwater, Okla.; St. Louis; Urbana, Ill.; College Park, Md.; and Allegheny County, Pa.
The scientists collected eggs in the wild and raised larvae from the different geographic locations to adult stages in the lab, tending the mosquito populations separately as they continued to breed and grow. The scientists then used adults and larvae from subsequent generations of these captive-raised mosquitoes in trials to determine CTmax values, ramping up air and water temperatures at a rate of 1 degree Celsius per minute using established research protocols.
The team then tested the relationship between climatic variables measured near each population source and the CTmax of adults and larvae. The scientists found significant differences among the mosquito populations.
The differences did not appear to follow a simple latitudinal or temperature-dependent pattern, but there were some important trends. Mosquito populations from locations with higher precipitation had higher CTmax values. Overall, the results reveal that mean and maximum seasonal temperatures, relative humidity and annual precipitation may all be important climatic factors in determining CTmax.
“Larvae had significantly higher thermal limits than adults, and this likely results from different selection pressures for terrestrial adults and aquatic larvae,” said Benjamin Orlinick, first author of the paper and a former undergraduate research fellow at Tyson Research Center. “It appears that adult Ae. albopictus are experiencing temperatures closer to their CTmax than larvae, possibly explaining why there are more differences among adult populations.”
“The overall trend is for increased heat tolerance with increasing precipitation,” Westby said. “It could be that wetter climates allow mosquitoes to endure hotter temperatures due to decreases in desiccation, as humidity and temperature are known to interact and influence mosquito survival.”
Little is known about how different vector populations, like those of this kind of mosquito, are adapted to their local climate, nor the potential for vectors to adapt to a rapidly changing climate. This study is one of the few to consider the upper limits of survivability in high temperatures — akin to heat waves — as opposed to the limits imposed by cold winters.
“Standing genetic variation in heat tolerance is necessary for organisms to adapt to higher temperatures,” Westby said. “That’s why it was important for us to experimentally determine if this mosquito exhibits variation before we can begin to test how, or if, it will adapt to a warmer world.”
Future research in the lab aims to determine the upper limits that mosquitoes will seek out hosts for blood meals in the field, where they spend the hottest parts of the day when temperatures get above those thresholds, and if they are already adapting to higher temperatures. “Determining this is key to understanding how climate change will impact disease transmission in the real world,” Westby said. “Mosquitoes in the wild experience fluctuating daily temperatures and humidity that we cannot fully replicate in the lab.”
[ad_2]
Washington University in St. Louis
Source link
[ad_1]
BYLINE: Nakaysha Gonzalez
Newswise — Pregnancy weight and biochemical markers measured in blood from women with gestational diabetes mellitus (GDM) were related to increased risk of poor pregnancy outcomes, suggesting a new direction for precision diagnostics, according to researchers.
The study led by Ellen C. Francis, an assistant professor in the Department of Biostatistics and Epidemiology at Rutgers School of Public Health, and published in Nature Communications Medicine, evaluated the diagnostic value of these markers before or at the time of screening for GDM, a type of diabetes that can develop during pregnancy.
“Although we found that obesity is a risk factor for offspring born larger for their gestational age, evidence suggests that the metabolic alterations that accompany obesity increase the risk of adverse outcomes,” said Francis. GDM, characterized by elevated blood sugar (glucose) levels during pregnancy, is the most common metabolic condition among pregnant women and poses risks to both mother and child. While standard treatments are applied, clinical outcomes can differ among individuals.
Francis said the research demonstrates the need for a more nuanced approach to diagnose GDM, which may help improve outcomes. It is the first systematic review of the literature to assess the potential of subtypes in GDM and to examine whether nonglycemic markers could refine risk stratification. Francis said some of the literature suggested insulin profiles and triglyceride levels may serve as promising non-glucose indicators of risk.
“To really assess the clinical implications of precision diagnostics in GDM, we first need to understand if insulin resistance or higher triglycerides are causally linked to adverse outcomes, and whether we can safely target them in pregnancy,” Francis said.
Overall, researchers found a critical gap in the existing literature in which most studies hadn’t focused on comparing clinical, biochemical or sociocultural differences among women who develop GDM.
“In our full text screening of 775 studies, we found that only recently has there been a focus on clinical, biochemical, or sociocultural markers that could improve who is at greatest risk of poor outcomes, and on comparing clinical outcomes between different subtypes of GDM,” said Francis. “The data from these studies indicate that in the future, we may be able to refine how we diagnose GDM by using anthropometric or biochemical information in combination with current diagnostic approaches.”
Future research should delve into mechanistic studies on precision biomarkers, large diverse population studies for replication, and multinational studies focusing on environmental and behavioral factors, Francis said. It should also explore potential insights on casual pathways of heterogeneity within GDM and its outcomes from genetic and multi-omics data using advanced analytical approaches.
Study co-authors include researchers from collaborating institutions in the United States, the United Kingdom, Singapore, South Korea and Australia.
[ad_2]
Rutgers University-New Brunswick
Source link

[ad_1]
What are the metabolic and behavioral adaptations that slow weight loss?
Thanks to millions of years of evolution hard-wiring us to survive scarcity, our body has compensatory survival mechanisms to defend against weight loss. When we start losing weight, we may unconsciously begin to move less as a “behavioral adaptation” to conserve energy. There are metabolic adaptations as well; our metabolism slows down. Every pound of weight loss may reduce our resting metabolic rate by seven calories a day. This may only translate to a few percent differences for most, but it can rapidly snowball for those who achieve massive weight loss. I discuss this phenomenon in my video The Reason Weight Loss Plateaus When You Diet.
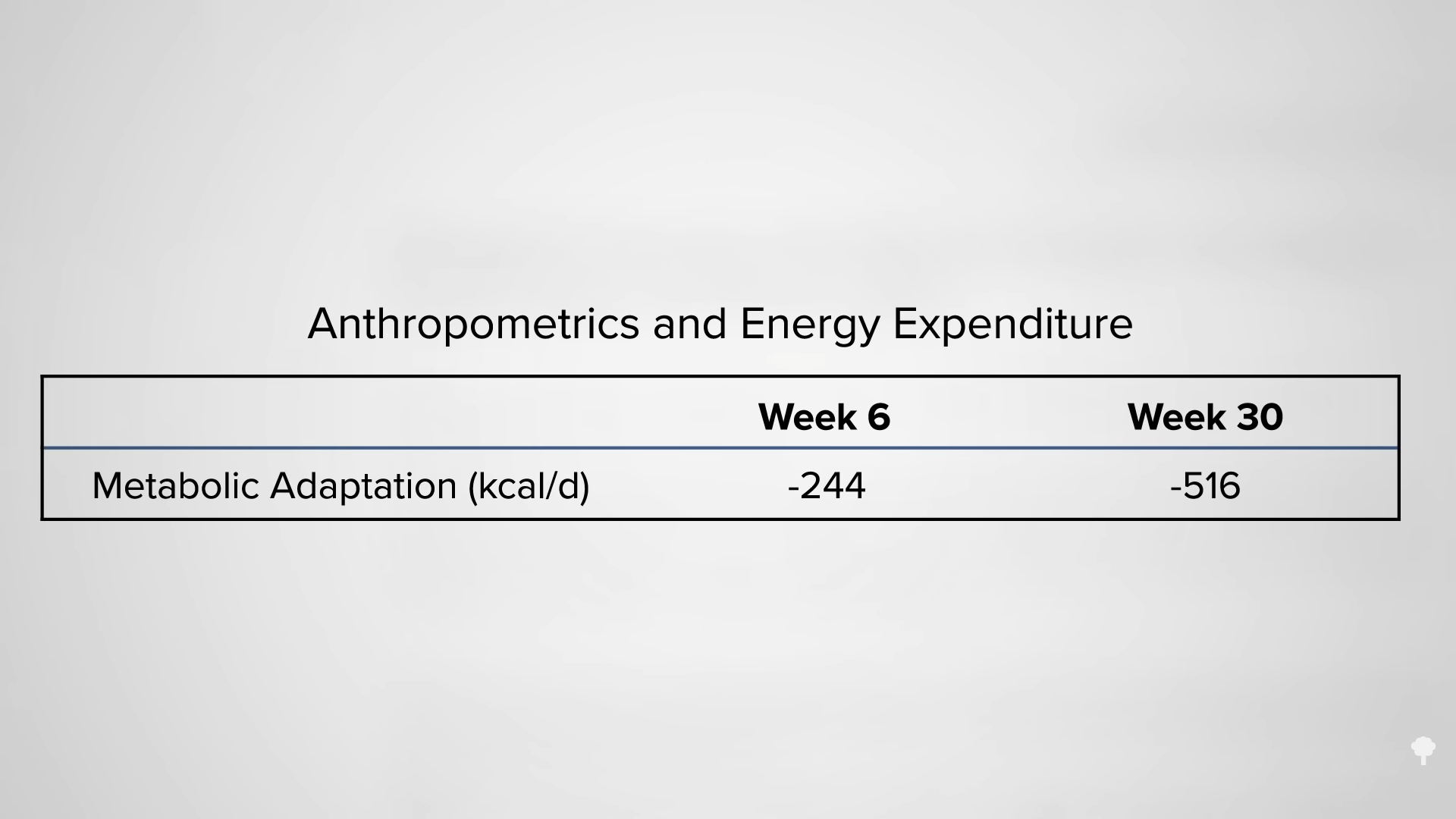
During one season of the television show The Biggest Loser, some of the contestants famously had their metabolic rates tracked. As you can see in the graphs below, above and beyond the hundreds of fewer calories it takes to just exist when more than a hundred pounds lighter (at 0:55 in my video), by the end of the season, their metabolic rates had slowed by an extra 500 calories a day (at 1:03 in my video).
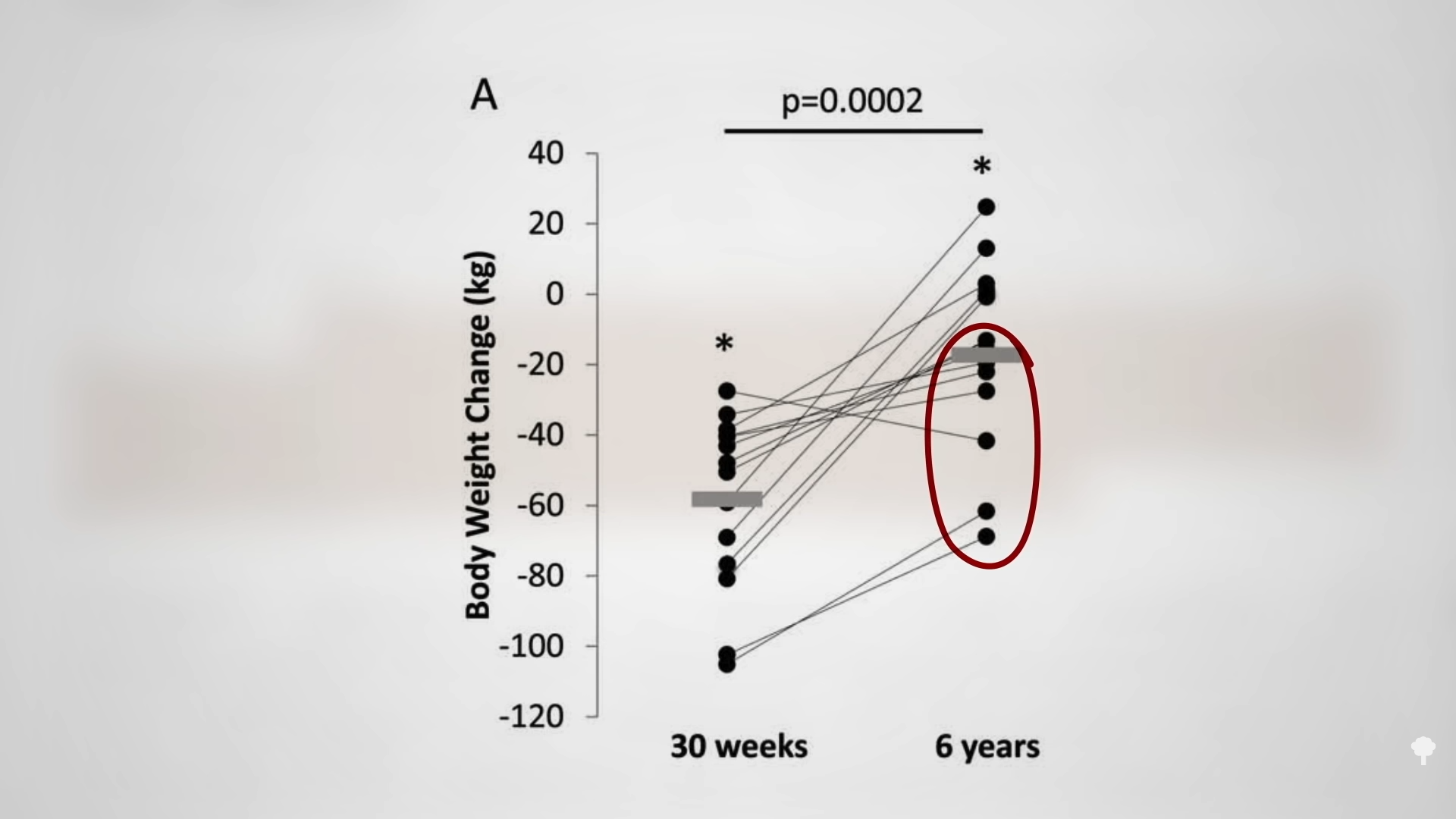
What’s mind-blowing is that when they were retested six years later, they still had the 500-calorie-a-day handicap. So, the contestants had to cut 500 more calories than anyone else their size to maintain the same weight loss. No wonder the bulk of their weight loss was regained. As you can see in the graph below and at 1:23 in my video, most remained at least 10 percent lower than their starting weight, though.
Even a 7 percent drop has been shown to cut diabetes rates about in half, as seen in the graph below and at 1:31 in my video. Still, the metabolic slowing means you have to work that much harder than everyone else just to stay in place.  Analyzing four seasons of The Biggest Loser minute-by-minute, researchers noted that 85 percent of the focus was on exercise rather than diet, though the exercise component accounted for less than half of the weight loss. Even six years after their season ended, the contestants had been maintaining an hour of daily, vigorous exercise, yet still regained most of the weight they had lost. Why? Because they had started eating more. They could have limited their exercise to just 20 minutes a day and still maintained 100 percent of their initial weight loss if they had just been able to keep their intake to less than 3,000 calories a day. That may not sound like much of a challenge, but weight loss doesn’t just slow your metabolism. It also boosts your appetite.
Analyzing four seasons of The Biggest Loser minute-by-minute, researchers noted that 85 percent of the focus was on exercise rather than diet, though the exercise component accounted for less than half of the weight loss. Even six years after their season ended, the contestants had been maintaining an hour of daily, vigorous exercise, yet still regained most of the weight they had lost. Why? Because they had started eating more. They could have limited their exercise to just 20 minutes a day and still maintained 100 percent of their initial weight loss if they had just been able to keep their intake to less than 3,000 calories a day. That may not sound like much of a challenge, but weight loss doesn’t just slow your metabolism. It also boosts your appetite.
If it were just a matter of your weight settling at the point at which your reduced caloric intake matches your reduced caloric output, it would take years for your weight loss to plateau. Instead, it often happens within six to eight months. You can see illustrative graphs below and at 2:34 and 2:43 in my video. You may know the drill: Start the diet, stick to the diet, then weight loss stalls six months later. What happened? Don’t blame your metabolism—that only plays a small part. Instead, you likely stopped sticking to your diet because your appetite went on a rampage.
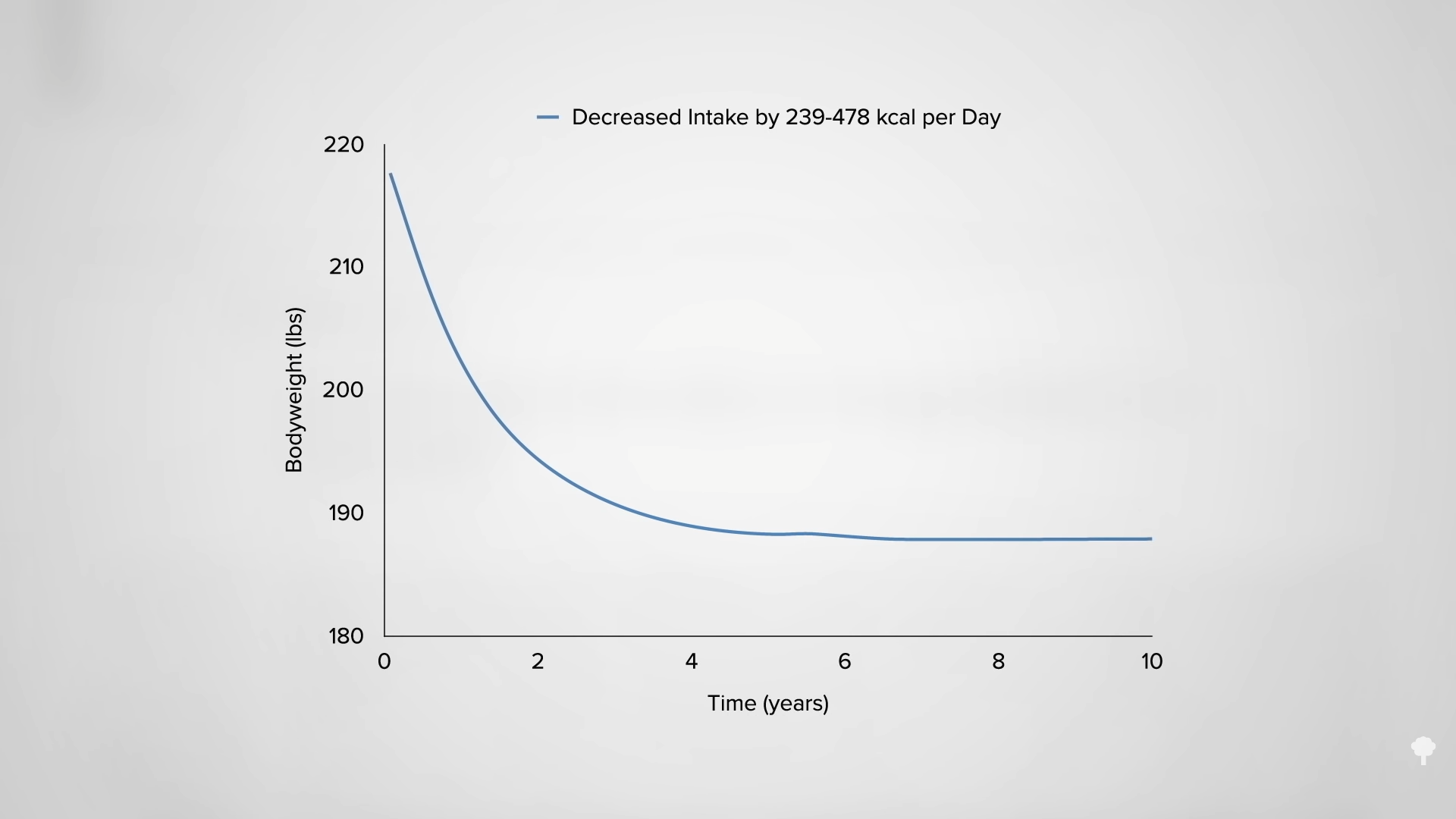
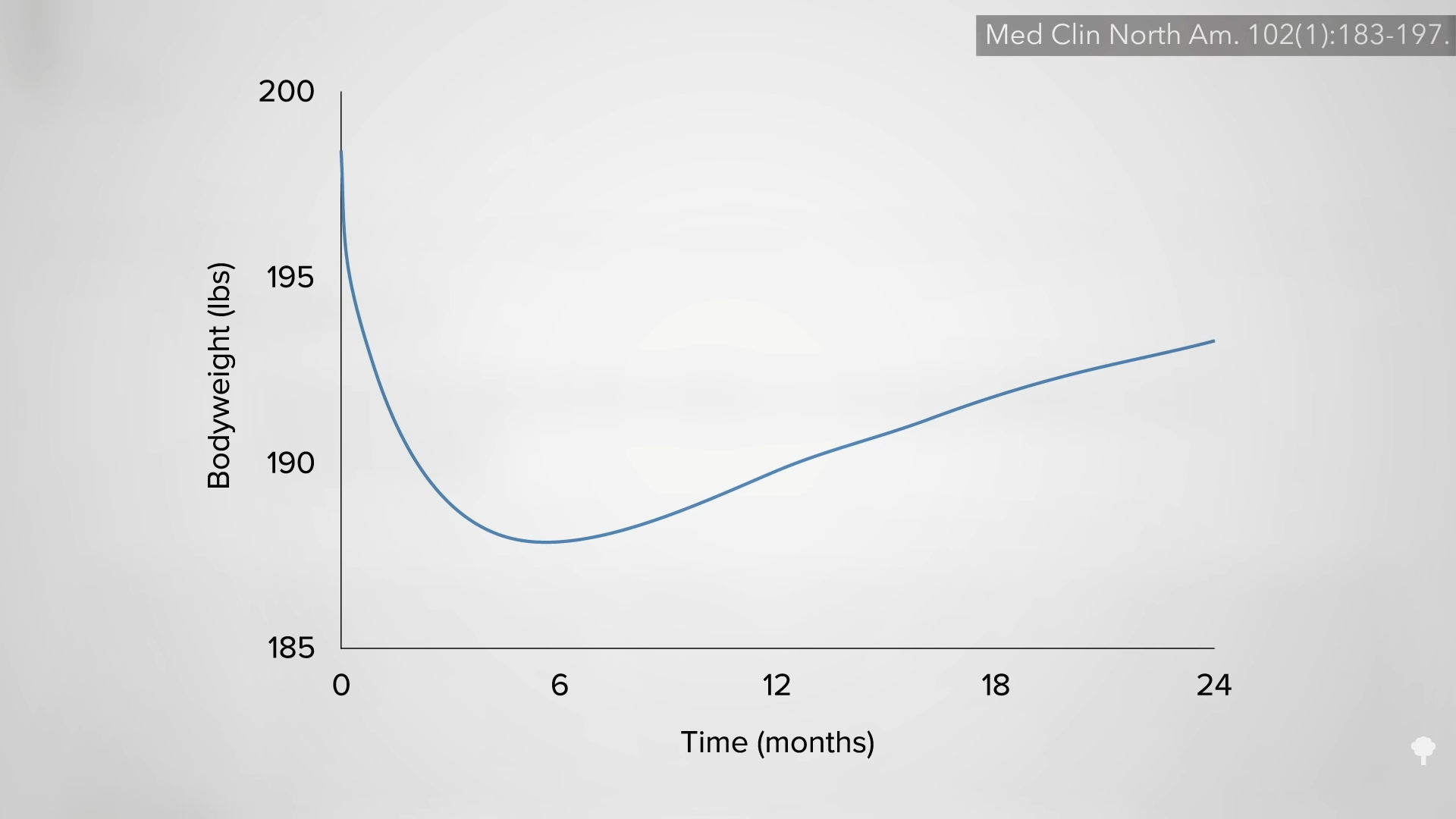 Let’s break it down. If you cut 800 calories out of your daily diet—going from 2,600 calories a day down to 1,800, for instance—and your weight loss stalls after six months, what may have happened is, at the end of the first month, you think you’re still cutting 800 calories, but you may actually only be down about 600 calories a day. By month two, you may only be down about 500 calories, 300 by month three, and, by month six, you may only be eating 200 calories less than before you went on the diet. In other words, you may have inadvertently suffered an exponential increase in caloric intake over those six months. But, you may not even realize it because, by that time, your body may have ramped up your appetite by 600 calories. So, it still feels as if you are eating 800 calories less, but it’s actually only 200 fewer calories. Since an 800-calorie drop in intake may slow your metabolism and physical activity by about 200 calories a day, with no difference between calories in and calories out at six months, no wonder your weight loss grinds to a complete halt.
Let’s break it down. If you cut 800 calories out of your daily diet—going from 2,600 calories a day down to 1,800, for instance—and your weight loss stalls after six months, what may have happened is, at the end of the first month, you think you’re still cutting 800 calories, but you may actually only be down about 600 calories a day. By month two, you may only be down about 500 calories, 300 by month three, and, by month six, you may only be eating 200 calories less than before you went on the diet. In other words, you may have inadvertently suffered an exponential increase in caloric intake over those six months. But, you may not even realize it because, by that time, your body may have ramped up your appetite by 600 calories. So, it still feels as if you are eating 800 calories less, but it’s actually only 200 fewer calories. Since an 800-calorie drop in intake may slow your metabolism and physical activity by about 200 calories a day, with no difference between calories in and calories out at six months, no wonder your weight loss grinds to a complete halt.
The slow upward drift in caloric intake on a new diet is not because you got lazy. Once your appetite is boosted by 600 calories after dieting for a while, eating 200 fewer calories at the end is as hard as eating 800 fewer calories at the beginning. So, you can maintain the same disciplined level of willpower and self-control yet still end up stagnating. To prevent this from happening, you need to maintain the calorie deficit. How is that possible in the face of a ravenous appetite?
Hunger is a biological drive. Asking someone to eat smaller portions is like asking someone to take fewer breaths. You can white-knuckle it for a bit, but, eventually, nature wins out. That’s why I wrote How Not to Diet. There are foods that can counter the slowing of our metabolism and suppress our appetite, as well as ways of eating to counter the behavioral adaptation and even eat more food—yet still lose weight.
Due to “the ongoing slowing of metabolism and increased appetite associated with the lost weight,” sustained weight loss requires a persistent calorie deficit of 300 to 500 calories a day. This can be accomplished without reducing portion sizes simply by lowering the calorie density of meals, which can result in the rare combination of weight loss with both an increase in quality and even quantity of food consumed. (See the two graphs below and at 5:34 and 5:40 in my video.) The bottom line is that sustainable weight loss is not about eating less food. It’s about eating better food.
 In my previous video, I dive into how The 3,500 Calorie per Pound Rule Is Wrong. In that case, what’s The New Calories per Pound of Weight Loss Rule? Watch that video to find out.
In my previous video, I dive into how The 3,500 Calorie per Pound Rule Is Wrong. In that case, what’s The New Calories per Pound of Weight Loss Rule? Watch that video to find out.
My book How Not to Diet is all about weight loss and how to break the diet cycle. For more on weight loss, see related videos below.
See the Weight Loss topic page for more relevant videos.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
Watch CBS News
Be the first to know
Get browser notifications for breaking news, live events, and exclusive reporting.
[ad_2]

[ad_1]
Ketogenic diets are put to the test for diabetes reversal.
As you can see at the start of my video Does a Ketogenic Diet Help Diabetes or Make It Worse?, ketogenic diets can lower blood sugars better than conventional diets. So much so, in fact, that there is a keto product company that claims ketogenic diets can “reverse” diabetes. However, they are confusing the symptom (high blood sugars) with the disease (carbohydrate intolerance). People with diabetes can’t properly handle carbohydrates, and this manifests as high blood sugars. Clearly, if you stick to eating mostly fat, your blood sugars will stay low, but you may be actually making the underlying disease worse at the same time.
We’ve known for nearly a century that if you put people on a ketogenic diet, their carbohydrate intolerance can skyrocket within just two days. Below and at 0:46 in my video, you can see a graph from the study showing the blood sugar response two days after eating sugar. On a high-carb diet, blood sugar response is about 90 mg/dL. But, the blood sugar response to the same amount of sugar after a high-fat diet is about 190 mg/dL, nearly double. The intolerance to carbohydrates skyrocketed on a high-fat diet.
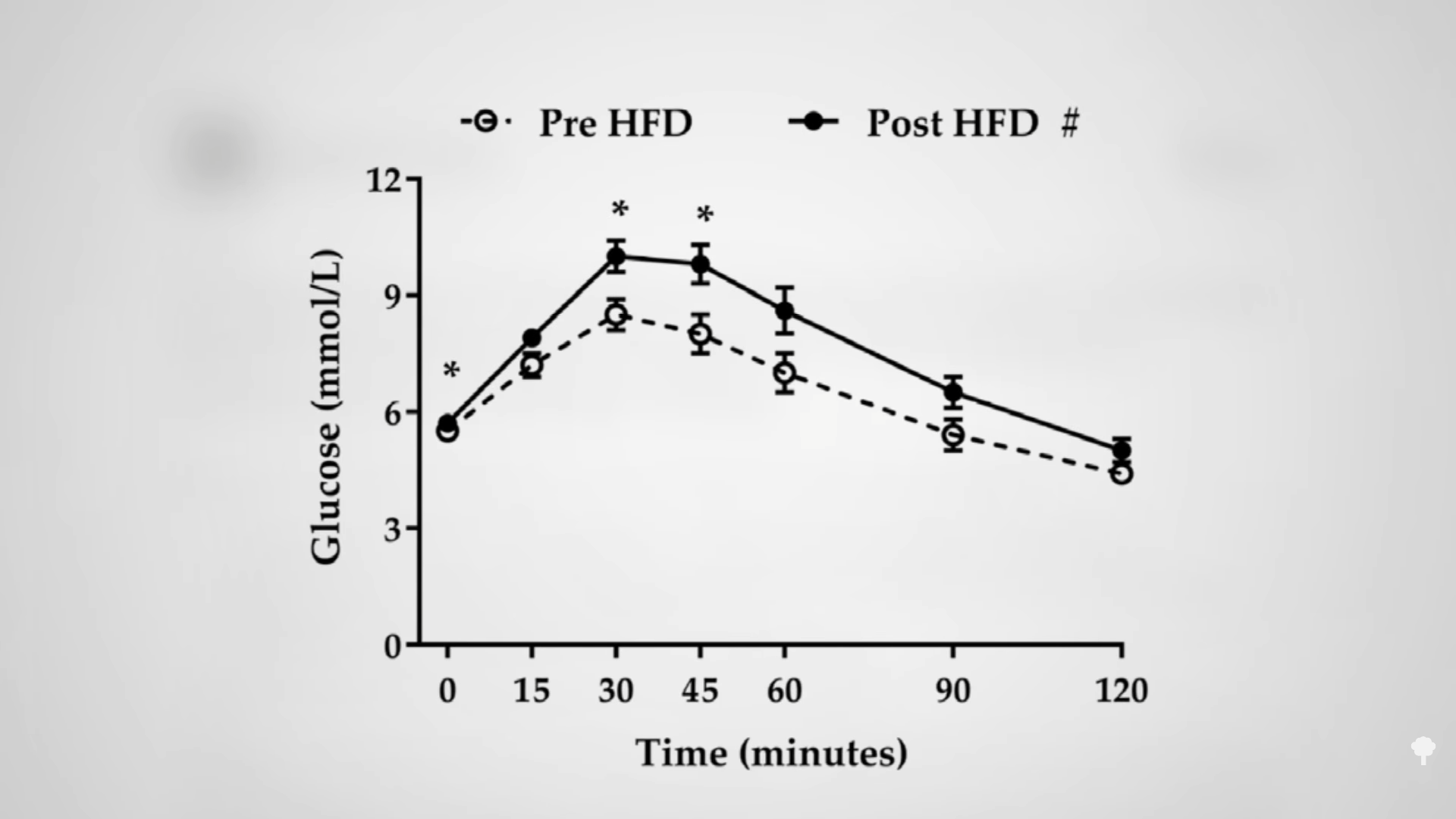
After one week on an 80 percent fat diet, you can quintuple your blood sugar spike in reaction to the same carb load compared to a week on a low-fat diet, as you can see in the graph below and at 1:12 in my video. 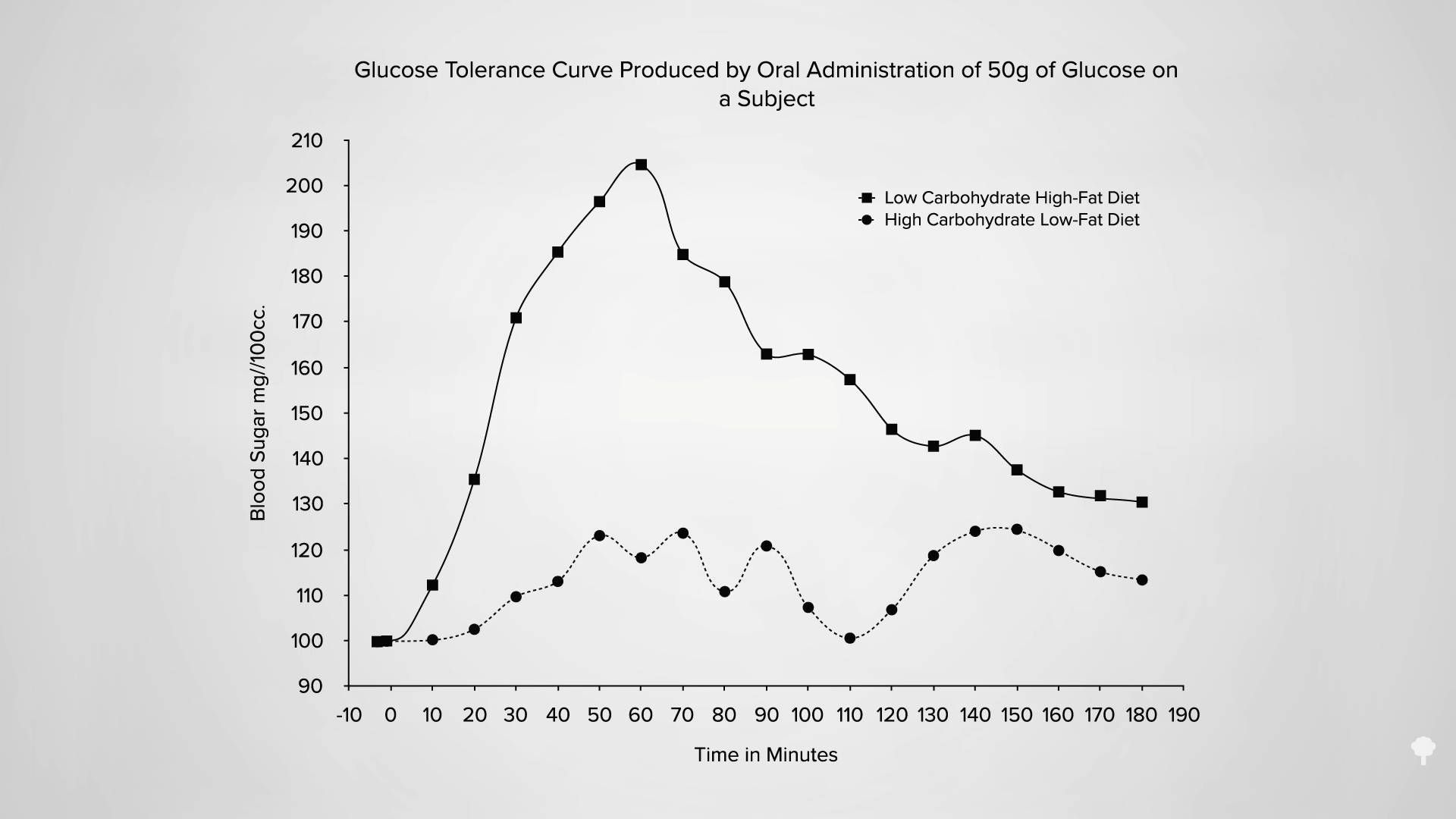
Even a single day of excessive dietary fat intake can do it, as you can see in the graph below and at 1:26 in my video. If you’re going in for a diabetes test, having a fatty dinner the night before can adversely affect your results. Just one meal high in saturated fat can make carbohydrate intolerance, the cause of diabetes, worse within four hours.
Given enough weight loss by any means, whether from cholera or bariatric surgery, type 2 diabetes can be reversed, but a keto diet for diabetes may not just be papering over the cracks, but actively throwing fuel on the fire.
I’ve been trying to think of a good metaphor. It’s easy to come up with things that just treat the symptoms without helping the underlying disease, like giving someone with pneumonia aspirin for their fever instead of antibiotics. However, a keto diet for diabetes is worse than that because it may treat the symptoms while actively worsening the disease. It may be more like curing the fever by throwing that pneumonia patient out into a snow bank or “curing” your amputated finger by amputating your hand. One of the co-founders of masteringdiabetes.org suggested it’s like a CEO who makes their bad bottom line look better by borrowing tons of cash. The outward numbers look better, but on the inside, the company is just digging itself into a bigger hole.
Do you remember The Club, that popular car anti-theft device that attaches to the steering wheel and locks it in place so the steering column can only turn a few inches? Imagine you’re in a car at the top of a hill with the steering wheel locked. Then, the car starts rolling down the hill. What do you do? Imagine there’s also something stuck under your brake pedal. The keto-diet equivalent response to this situation is who cares if you’re barreling down into traffic with a locked steering wheel and no brakes—just stick to really straight deserted roads without any stop signs or traffic lights. If you do that, problem solved! The longer you go, the more speed you’ll pick up. If you should hit a dietary bump in the road or start to veer off the path, the consequences could get more and more disastrous over time. However, if you stick to the keto straight and narrow, you’ll be a-okay! In contrast, the non-keto response would be to just unlock the steering wheel and dislodge whatever’s under your brake. In other words, fix the underlying problem instead of just whistling past—and then into—the graveyard.
The reason keto proponents claim they can “reverse” diabetes is they can successfully wean type 2 diabetics off their insulin. That’s like faith-healing someone out of the need for a wheelchair by making them stay in bed the rest of their life. No need for a wheelchair if you never move. Their carbohydrate intolerance isn’t gone. Their diabetes isn’t gone. In fact, it could be just as bad or even worse. Type 2 diabetes is reversed when you are weaned off insulin while eating a normal diet like everyone else. Then and only then do you not have diabetes anymore. A true diabetes reversal diet, as you can see below and at 4:58 in my video, is practically the opposite of a ketogenic diet: getting diabetics off their insulin within a matter of weeks by eating more than 300 grams of carbs a day! 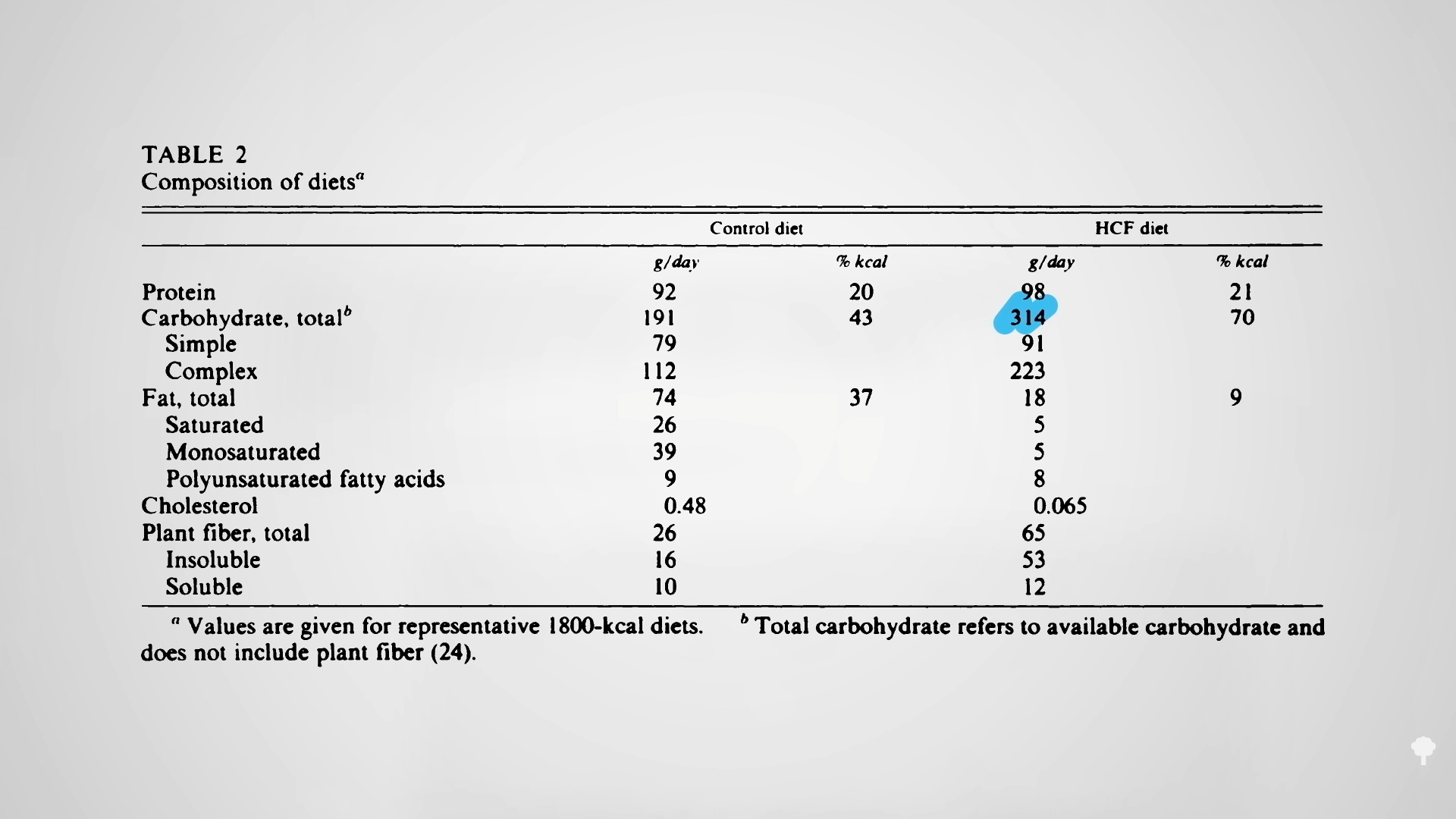 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal is the most potent creator of advanced glycation end products (AGEs), which are implicated in degenerative diseases—from Alzheimer’s and cataracts to kidney disease and strokes, as you can see below and at 5:31 in my video.
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal is the most potent creator of advanced glycation end products (AGEs), which are implicated in degenerative diseases—from Alzheimer’s and cataracts to kidney disease and strokes, as you can see below and at 5:31 in my video.
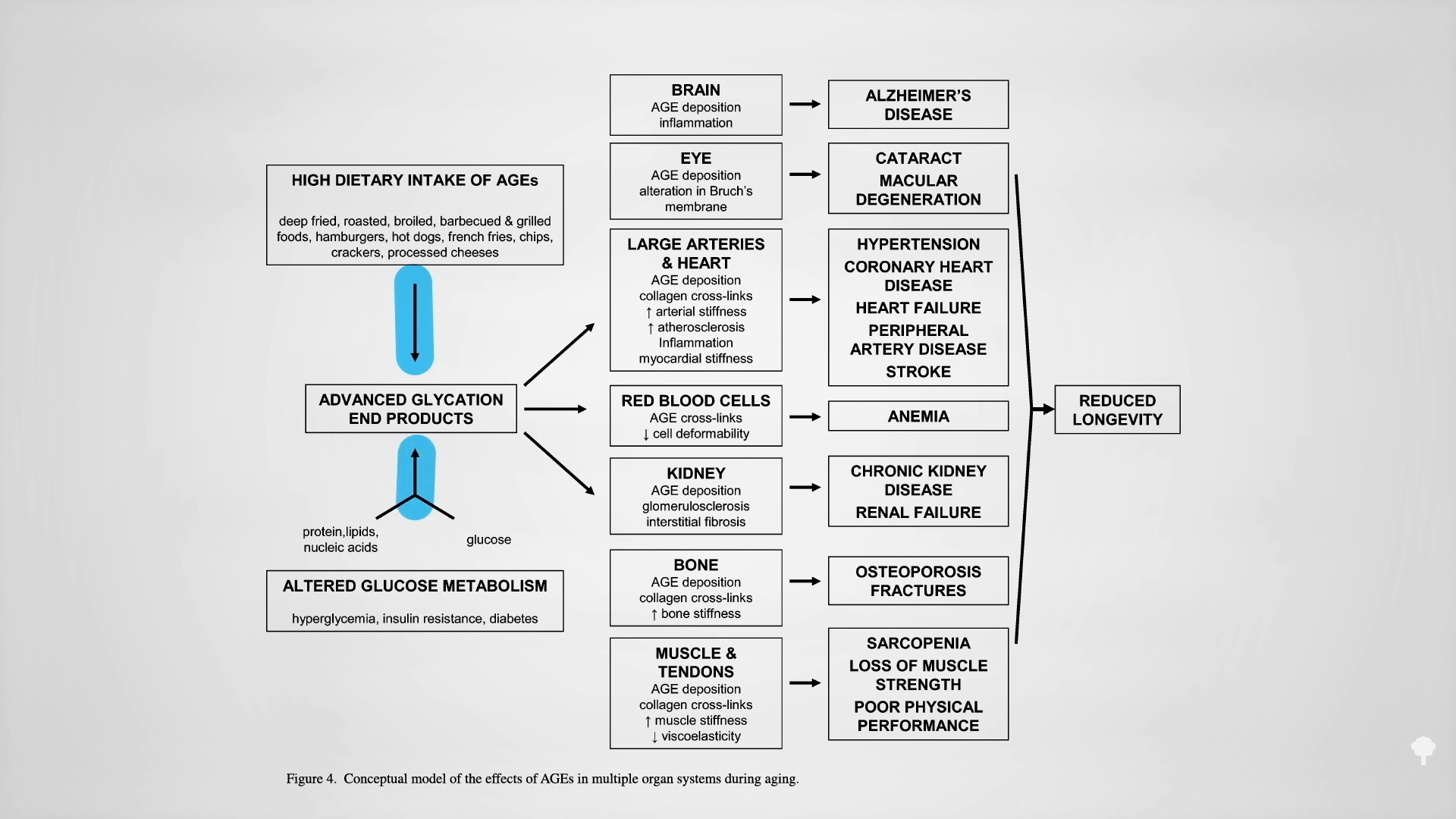
You get AGEs in your body from two sources: You can eat them preformed in your diet or make them internally from methylglyoxal if you have high blood sugar levels. On a keto diet, one would expect high exposure to preformed AGEs, since they’re found concentrated in animal-derived foods high in fat and protein, but we would expect less internal, new formation due to presumably low levels of methylglyoxal, given lower blood sugars from not eating carbs. Dartmouth researchers were surprised to find more methylglyoxal! As shown in the graph below and at 6:11 in my video, a few weeks on the Atkins diet led to a significant increase in methylglyoxal levels. Those in active ketosis did even worse, doubling the level of this glycotoxin in their bloodstream.
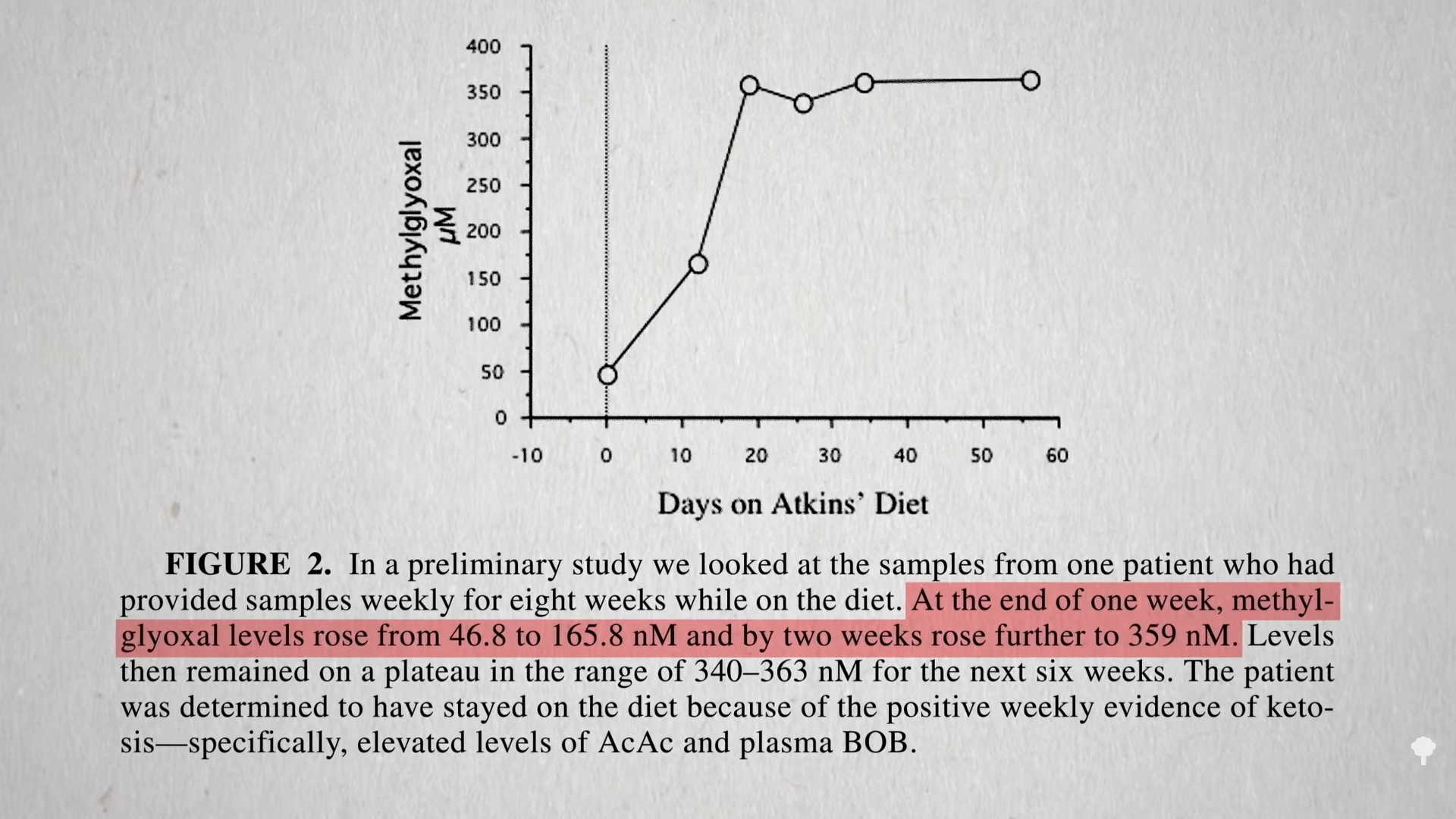
It turns out that high sugars may not be the only way to create this toxin, as you can see below and at 6:24 in my video. One of the ketones you make on a ketogenic diet is acetone (known for its starring role in nail polish remover). Acetone does more than just make keto dieters fail breathalyzer tests, “feel queasy and light-headed, and develop what’s been described as ‘rotten apple breath.’” Acetone can oxidize in the blood to form acetol, which may be a precursor for methylglyoxal. 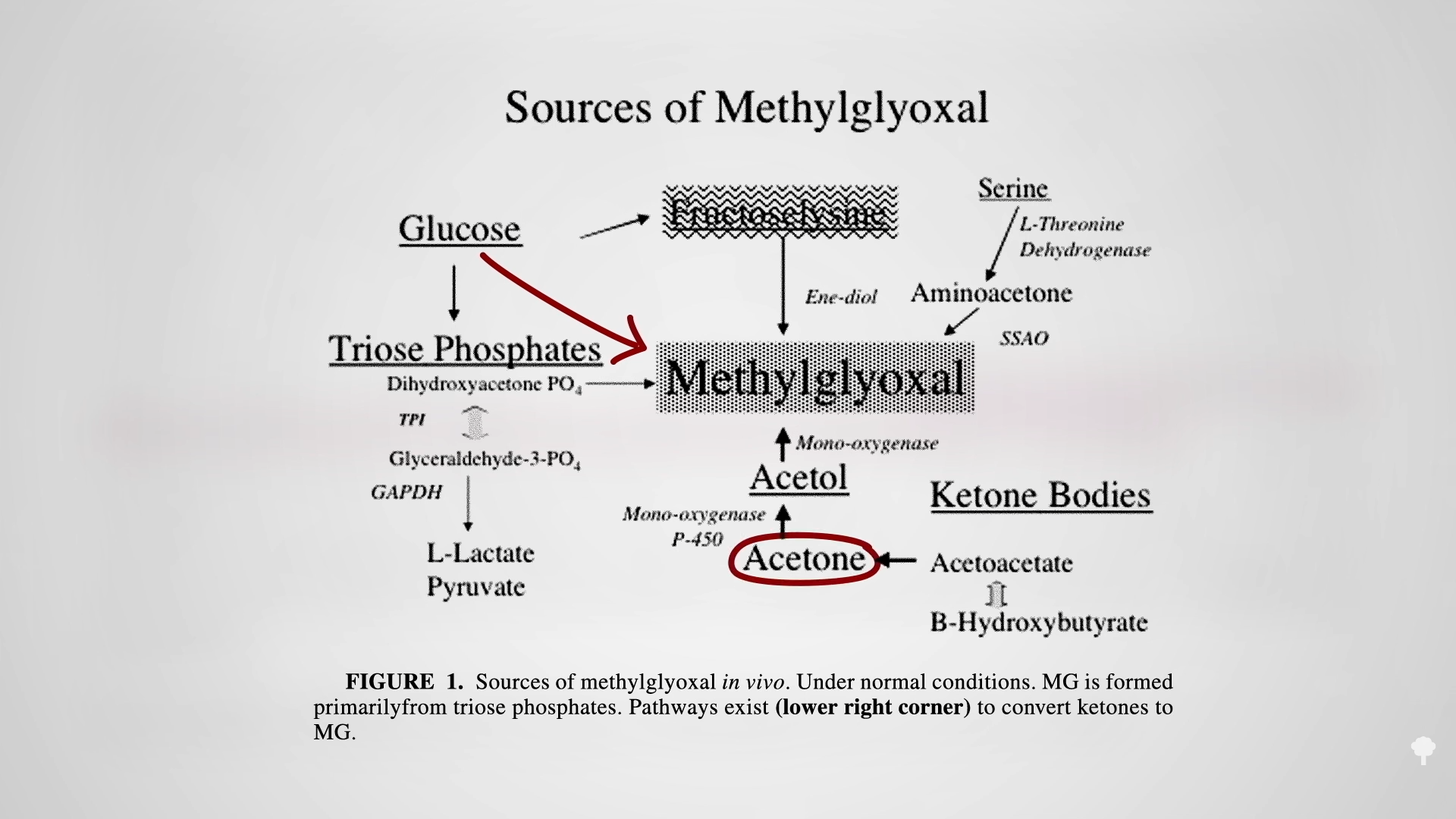
That may be why keto dieters can end up with levels of this glycotoxin as high as those with out-of-control diabetes, which can cause the nerve damage and blood vessel damage you see in diabetics. That’s another way keto dieters can end up with a heart attack. The irony of treating diabetes with a ketogenic diet may extend beyond just making the underlying diabetes worse, but by mimicking some of the disease’s dire consequences.
This is part of a seven-video series on keto, which you can find in related videos below.
I also recently tackled diabetes.
[ad_2]
Michael Greger M.D. FACLM
Source link
[ad_1]
Newswise — Do epigenetic changes cause type 2 diabetes, or do the changes occur only after a person has become ill? A new study by researchers at Lund University provides increased support for the idea that epigenetic changes can cause type 2 diabetes. The researchers behind the new findings published in Nature Communications now aim to develop methods for disease prevention.
We inherit our genes from our parents, and they seldom change. However, epigenetic changes that arise due to environmental and lifestyle factors can affect the function of genes.
“Our new extensive study confirms our previous findings from smaller studies, showing that epigenetic changes can contribute to the development of type 2 diabetes. In this study, we have also identified new genes that impact the development of the disease. Our hope is that with the help of these results, we can develop methods that can be used to prevent type 2 diabetes,” says Charlotte Ling, professor of diabetes and epigenetics at Lund University’s Diabetes Centre (LUDC), who led the study.
The same epigenetic changes
The researchers studied epigenetics in insulin-producing cells from donors and found 5584 sites in the genome with changes that differed between 25 individuals with type 2 diabetes and 75 individuals without the disease. The same epigenetic changes found in people with type 2 diabetes were also found in individuals with elevated blood sugar levels, which increase the risk of developing the disease.
“Those of us who study epigenetics, have long tried to understand whether epigenetic changes cause type 2 diabetes or if the changes occur after the disease has already developed. Because we saw the same epigenetic changes in people with type 2 diabetes and individuals at risk for the disease, we conclude that these changes may contribute to the development of type 2 diabetes,” says Tina Rönn, lead author and researcher at LUDC.
The study identified 203 genes with different expression in individuals with type 2 diabetes compared to the control group. The researchers found that the gene RHOT1 showed epigenetic changes in people with type 2 diabetes and that it also played a key role in insulin secretion in insulin-producing cells. When they knocked out the gene expression of RHOT1 in cells from donors without type 2 diabetes, insulin secretion decreased.
“When we examined the same type of cells in rats with diabetes, we found a lack of RHOT1, confirming the gene’s importance for insulin secretion,” says Tina Rönn.
Methods that can prevent the disease
One goal of the research is to develop a blood-based biomarker that can predict who is at risk of developing type 2 diabetes. Therefore, the researchers investigated whether their results from insulin-producing cells in the pancreas were reflected in the blood of living people. They found epigenetic changes in the blood of a group of 540 people without the disease and they linked this to the future development of type 2 diabetes in half of the individuals.
Factors such as unhealthy diet, sedentary lifestyle, and ageing increase the risk of type 2 diabetes, and they also affect our epigenetics. With the new study, researchers have identified new mechanisms that may make it possible to develop methods to help prevent type 2 diabetes.
“If we succeed in developing an epigenetic biomarker, we can identify individuals with epigenetic changes before they become ill. These individuals can, for example, receive personalised lifestyle advice that can reduce their risk of disease, or we can develop methods that aim to correct the activity of certain genes using epigenetic editing,” says Charlotte Ling.
[ad_2]
Newswise
Source link
[ad_1]
Newswise — Starting menstrual cycles at a young age—before the age of 13—is linked to a heightened risk of developing type 2 diabetes in mid-life, finds US research published online in the open access journal BMJ Nutrition Prevention & Health.
And it also seems to be associated with an increased risk of having a stroke before the age of 65 in those with the disease, particularly those who started having periods before the age of 10 or younger, the findings indicate.
Diabetes and its complications are on the rise among young and middle aged US adults, while the age at which women start having periods is falling worldwide, note the researchers.
They therefore wanted to find out if there might be a link between these two phenomena in younger women, and drew on responses to the nationally representative National Health and Nutrition Examination Survey (NHANES) 1999–2018.
Some 17,377 women aged between 20 and 65 were included in the study, all of whom specified the age at which they had had their first menstrual cycle. This was categorised as 10 or younger, 11, 12, 13, 14 and 15 and older.
Of the total, 1773 (10%) reported a diagnosis of type 2 diabetes. And of these, 205 (11.5%) reported some type of cardiovascular disease.
Starting periods before the average age of 13 was associated with a heightened risk of type 2 diabetes, after accounting for a range of potentially influential factors, including age, race/ethnicity, education, motherhood, menopausal status and family history of diabetes, smoking, physical activity, alcohol consumption and weight (BMI).
This ranged from 32% greater (10 or younger) through 14% greater (age 11) to 29% greater (age 12).
Among women with diabetes, earlier age at first menstrual cycle was associated with a heightened risk of stroke, although not cardiovascular disease in general, after accounting for the same set of potentially influential factors.
Very early age at first menstrual cycle—10 or younger—was associated with a more than doubling in stroke risk among women below the age of 65 with diabetes, after similar adjustments for influential factors.
This risk fell in tandem with increasing age: 81% among those with their first menstrual bleed at the age of 11, to 32% at the age of 12, and to 15% at the age of 14.
This is an observational study, and as such, can’t establish causal factors. But, suggest the researchers: “Earlier age at [first menstrual cycle] may be one of early life indicators of the cardiometabolic disease trajectory in women.”
They explain: “One potential pathway explanation may be that [such] women are exposed to oestrogen for longer periods of time, and early [menstruation] has been associated with higher oestrogen levels.”
They point out that while the observed associations between age at first menstrual cycle and stroke complications weakened slightly after accounting for weight, these still remained statistically significant.
“Therefore, adiposity may also play a role in the observed association between early age at [first menstrual cycle] and stroke complications, as higher childhood adiposity is associated with earlier age at [menstruation] and with cardiometabolic diseases later in life,” they suggest.
“These findings add another dimension to the potentially less well understood determinants of cardiometabolic risk, particularly in women who have been relatively underrepresented in this area of research,” comments Professor Sumantra Ray, Executive Director of the NNEdPro Global Centre for Nutrition & Health, which co-owns BMJ Nutrition Prevention & Health.
“And they provide a clear steer on the need to design interventional studies looking at the prevention of cardiometabolic disease in ethnically diverse groups of women who start menstruating at a young age,” he adds.
[ad_2]
BMJ
Source link