The American Medical Association passed a resolution encouraging hospitals to offer healthy plant-based food options.
“Globally, 11 million deaths annually are attributable to dietary factors, placing poor diet ahead of any other risk factor for death in the world.” Given that diet is our leading killer, you’d think that nutrition education would be emphasized during medical school and training, but there is a deficiency. A systematic review found that, “despite the centrality of nutrition to a healthy lifestyle, graduating medical students are not supported through their education to provide high-quality, effective nutrition care to patients…”
It could start in undergrad. What’s more important? Learning about humanity’s leading killer or organic chemistry?
In medical school, students may average only 19 hours of nutrition out of thousands of hours of instruction, and they aren’t even being taught what’s most useful. How many cases of scurvy and beriberi, diseases of dietary deficiency, will they encounter in clinical practice? In contrast, how many of their future patients will be suffering from dietary excesses—obesity, diabetes, hypertension, and heart disease? Those are probably a little more common than scurvy or beriberi. “Nevertheless, fully 95% of cardiologists [surveyed] believe that their role includes personally providing patients with at least basic nutrition information,” yet not even one in ten feels they have an “expert” grasp on the subject.
If you look at the clinical guidelines for what we should do for our patients with regard to our number one killer, atherosclerotic cardiovascular disease, all treatment begins with a healthy lifestyle, as shown below and at 1:50 in my video Hospitals with 100-Percent Plant-Based Menus.
“Yet, how can clinicians put these guidelines into practice without adequate training in nutrition?”
Less than half of medical schools report teaching any nutrition in clinical practice. In fact, they may be effectively teaching anti-nutrition, as “students typically begin medical school with a greater appreciation for the role of nutrition in health than when they leave.” Below and at 2:36 in my video is a figure entitled “Percentage of Medical Students Indicating that Nutrition is Important to Their Careers.” Upon entry to different medical schools, about three-quarters on average felt that nutrition is important to their careers. Smart bunch. Then, after two years of instruction, they were asked the same question, and the numbers plummeted. In fact, at most schools, it fell to 0%. Instead of being educated, they got de-educated. They had the notion that nutrition is important washed right out of their brains. “Thus, preclinical teaching”— the first two years of medical school—“engenders a loss of a sense of the relevance of the applied discipline of nutrition.”
Following medical school, during residency, nutrition education is “minimal or, more typically, absent.” “Major updates” were released in 2018 for residency and fellowship training requirements, and there were zero requirements for nutrition. “So you could have an internal medicine graduate who comes out of a terrific program and has learned nothing—literally nothing—about nutrition.”
“Why is diet not routinely addressed in both medical education and practice already, and what should be done about that?” One of the “reasons for the medical silence in nutrition” is that, “sadly…nutrition takes a back seat…because there are few financial incentives to support it.” What can we do about that? The Food Law and Policy Clinic at Harvard Law School identified a dozen different policy levers at all stages of medical education and the kinds of policy recommendations there could be for the decision-makers, as you can see here and at 3:48 in my video.
For instance, the government could require doctors working for Veterans Affairs (VA) to get at least some courses in nutrition, or we could put questions about nutrition on the board exams so schools would be pressured to teach it. As we are now, even patients who have just had a heart attack aren’t changing their diet. Doctors may not be telling them to do so, and hospitals may be actively undermining their future with the food they serve.
The good news is that the American Medical Association (AMA) has passed a resolution encouraging hospitals to offer healthy food options. What a concept! “Our AMA hereby calls on [U.S.] Health Care Facilities to improve the health of patients, staff, and visitors by: (a) providing a variety of healthy food, including plant-based meals, and meals that are low in saturated and trans fat, sodium, and added sugars; (b) eliminating processed meats from menus; and (c) providing and promoting healthy beverages.” Nice!
“Similarly, in 2018, the State of California mandated the availability of plant-based meals for hospital patients,” and there are hospitals in Gainesville (FL), the Bronx, Manhattan, Denver, and Tampa (FL) that “all provide 100% plant-based meals to their patients on a separate menu and provide educational materials to inpatients to improve education on the role of diet, especially plant-based diets, in chronic illness.”
Let’s check out some of their menu offerings: How about some lentil Bolognese? Or a cauliflower scramble with baked hash browns for breakfast, mushroom ragu for lunch, and, for supper, white bean stew, salad, and fruit for dessert. (This is the first time a hospital menu has ever made me hungry!)
The key to these transformations was “having a physician advocate and increasing education of staff and patients on the benefits of eating more plant-based foods.” A single clinician can spark change in a whole system, because science is on their side. “Doctors have a unique position in society” to influence policy at all levels; it’s about time we used it.
For more on the ingrained ignorance of basic clinical nutrition in medicine, see the related posts below.
Treat the underlying cause of chronic lifestyle diseases.
It’s been said that more than 2,000 years ago, Hippocrates declared, “Let food be thy medicine and medicine be thy food.” In actuality, it appears that he never actually said those words, but there’s “no doubt about the relevance of food…and its role in health and disease states” in his writings. Regardless, 2,000 years ago, disease was thought to arise from a bad sense of “humors,” as you can see here and at 0:32 in my video Lifestyle and Disease Prevention: Your DNA Is Not Your Destiny.
Now, we have science, and there is “an overwhelming body of clinical and epidemiological evidence illustrating the dramatic impact of a healthy lifestyle on reducing all-cause mortality”—meaning death from all causes put together—“and preventing chronic diseases such as coronary heart disease, stroke, diabetes, and cancer.” But don’t those diseases just run in our family? What if we just have bad genes?
According to the esteemed former chair of nutrition at Harvard, for most of the diseases that have contributed “importantly” to mortality in Western peoples, we’ve long known that non-genetic factors often account for at least 80% to 90% of risk. We know this because rates of the leading killers, like major cancers and cardiovascular diseases, vary up to 100-fold around the world, and, “when groups migrate from low- to high-risk countries, their disease rates almost always change to those of the new environment.” Modifiable behavioral factors have been identified, “including specific aspects of diet, overweight, inactivity, and smoking that account for over 70% of stroke and colon cancer, over 80% of coronary heart disease, and over 90% of adult-onset [type 2] diabetes”—diseases that can largely be prevented by our own actions.
If most of the power is in our own hands, why do we allocate massively more resources to treatment than prevention? And speaking of prevention, “even preventive strategies are heavily biased towards pharmacology rather than supporting improvements in diet and lifestyle that could be more cost-effective. For example, treatment of [high] serum cholesterol with statins alone could cost approximately 30 billion dollars per year in the United States and would have only a modest impact on coronary heart disease incidence. The inherent problem is that most pharmacologic strategies don’t address the underlying causes of ill health in Western countries, which are not drug deficiencies.”
Ironically, the chronic diseases that are most amenable to lifestyle treatment are the same ones most profitably treated by drugs. Why? If you don’t change your diet, you have to pop the pills every day for the rest of your life. So, the cash-cow drugs are the very drugs we need the least. “Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy, physicians often do not follow these recommendations.” “By ignoring the root causes of disease and neglecting to prioritize lifestyle measures for prevention, the medical community is placing people at harm.”
“Traditional medical care relies primarily on the application of pharmacologic and surgical interventions after the development of illness,” whereas lifestyle medicine relies primarily on “the use of optimal nutrition (a whole foods, plant-based diet) and exercise in the prevention, arrest, and reversal of chronic conditions leading to premature disability and death. It looks in a holistic way at the underlying causes of illness.”
Dr. Adriane Fugh-Berman, director of PharmedOut, a wonderful organization I’m proud to support, wrote a great editorial entitled “Doctors Must Not Be Lapdogs to Drug Firms.” “The illusion that the relationship between medicine and the drug industry is collegial, professional, and personal is carefully maintained by the drug industry, which actually views all transactions with physicians in finely calculated financial terms…The drug industry is happy to play the generous and genial uncle until physicians want to discuss subjects that are off limits, such as the benefits of diet or exercise, or the relationship between medicine and pharmaceutical companies…Let us not be a lapdog to Big Pharma. Rather than sitting contentedly in our master’s lap, let us turn around and bite something tender.”
Doctor’s Note
The organization I mentioned, PharmedOut, is a project of Georgetown University Medical Center.
For more on Lifestyle Medicine, see related videos below.
How can you calculate your own personal heart disease risk to help you determine if you should start on a cholesterol-lowering statin drug?
The muscle-related side effects from cholesterol-lowering statins “are often severe enough for patients to stop taking the drug. Of course, these side effects could be coincidental or psychosomatic and have nothing to do with the drug,” given that many clinical trials show such side effects are rare. “It is also possible that previous clinical trials”—funded by the drug companies themselves—“under-recorded the side effects of statins.” The bottom line is that there’s an urgent need to establish the true incidence of statin side effects.
“What proportion of symptomatic side effects in patients taking statins are genuinely caused by the drug?” That’s the title of a journal article that reports that, even in trials funded by Big Pharma, “only a small minority of symptoms reported on statins are genuinely due to the statins,” and those taking statins are significantly more likely to develop type 2 diabetes than those randomized to placebo sugar pills. Why? We’re still not exactly sure, but statins may have the double-whammy effect of impairing insulin secretion from the pancreas while also diminishing insulin’s effectiveness by increasing insulin resistance.
Even short-term use of statins may “approximately double the odds of developing diabetes and diabetic complications.” As shown below and at 1:49 in my video Who Should Take Statins?, fewer people develop diabetes and diabetic complications off statins over a period of about five years than those who do develop diabetes while on statins. “Of more concern, this increased risk persisted for at least 5 years after statin use stopped.”
“In view of the overwhelming benefit of statins in the reduction of cardiovascular events,” the number one killer of men and women, any increase in risk of diabetes, our seventh leading cause of death, would be outweighed by any cardiovascular benefits, right? That’s a false dichotomy. We don’t have to choose between heart disease and diabetes. We can treat the cause of both with the same diet and lifestyle changes. The diet that can not only stop heart disease, but also reverse it, is the same one that can reverse type 2 diabetes. But what if, for whatever reason, you refuse to change your diet and lifestyle? In that case, what are the risks and benefits of starting statins? Don’t expect to get the full scoop from your doctor, as most seemed clueless about statins’ causal link with diabetes, so only a small fraction even bring it up with their patients.
“Overall, in patients for whom statin treatment is recommended by current guidelines, the benefits greatly outweigh the risks.” But that’s for you to decide. Before we quantify exactly what the risks and benefits are, what exactly are the recommendations of current guidelines?
How should you decide if a statin is right for you? “If you have a history of heart disease or stroke, taking a statin medication is recommended, without considering your cholesterol levels.” Period. Full stop. No discussion needed. “If you do not yet have any known cardiovascular disease,” then the decision should be based on calculating your own personal risk. If you know your cholesterol and blood pressure numbers, it’s easy to do that online with the American College of Cardiology risk estimator or the Framingham risk profiler.
My favorite is the American College of Cardiology’s estimator because it gives you your current ten-year risk and also your lifetime risk. So, for a person with a 5.8 percent risk of having a heart attack or stroke within the next decade, if they don’t clean up their act, that lifetime risk jumps to 46 percent, nearly a flip of the coin. If they improved their cholesterol and blood pressure, though, they could reduce that risk by more than tenfold, down to 3.9 percent, as shown below and at 4:11 in my video.
Since the statin decision is based on your ten-year risk, what do you do with that number? As you can see here and at 4:48 in my video, under the current guidelines, if your ten-year risk is under 5 percent, then, unless there are extenuating circumstances, you should just stick to diet, exercise, and smoking cessation to bring down your numbers. In contrast, if your ten-year risk hits 20 percent, then the recommendation is to add a statin drug on top of making lifestyle modifications. Unless there are risk-enhancing factors, the tendency is to stick with lifestyle changes if risk is less than 7.5 percent and to move towards adding drugs if above 7.5 percent.
Risk-enhancing factors that your doctor should take into account when helping you make the decision include a bad family history, really high LDL cholesterol, metabolic syndrome, chronic kidney or inflammatory conditions, or persistently high triglycerides, C-reactive protein, or LP(a). You can see the whole list here and at 4:54 in my video.
If you’re still uncertain, guidelines suggest you consider getting a coronary artery calcium (CAC) score, but even though the radiation exposure from that test is relatively low these days, the U.S. Preventive Services Task Force has explicitly concluded that the current evidence is insufficient to conclude that the benefits outweigh the harms.
(CNN) — President Donald Trump’s strategy to ‘Make America Healthy Again’ includes investigating vaccine injuries and pharmaceutical practices but stops short of new regulatory action, for now.
US Health and Human Services Secretary Robert F. Kennedy Jr. unveiled the MAHA strategy on Tuesday, joined by Agriculture Department Secretary Brooke Rollins, Environmental Protection Agency Administrator Lee Zeldin, and other top Trump officials.
The report hews closely to a draft document circulated in August that cites earlier Trump administration announcements — developing a definition for ultraprocessed foods, educating the public about synthetic kratom — but largely bypassed industry crackdowns.
Language around pesticides strategy also remained unchanged. Environmental and food activists had rallied for the administration to include steps to reduce pesticide usage and probe potential health risks of commonly used chemicals such as RoundUp.
The report says that USDA, EPA and the National Institutes of Health will develop a framework to study cumulative exposures to chemicals including pesticides and microplastics. USDA and EPA will also invest in new farming approaches to reduce chemical use, and EPA will launch a public awareness campaign about the limited risk of approved products.
The commission’s first report this May suggested a broad range of factors driving chronic disease in the US, including ultraprocessed foods, environmental exposures, and overprescription of pharmaceuticals like antidepressants.
The report noted previous announcements that HHS, the NIH and the Centers for Medicare and Medicaid Services are studying the causes of autism. Kennedy had previously promised some answers on the root causes in September; NIH is expected to announce autism research grants this month.
Recent reports suggest that HHS will issue a report that links the development of autism to taking Tylenol during pregnancy.
Medicines and vaccines
Kennedy has drawn criticism for suggesting antidepressants, particularly those that are part of a family known as SSRIs are as addictive as heroin and can be dangerous. Following the August 27 shooting in Minneapolis, he told Fox News that HHS is launching studies “on the potential contribution of some of the SSRI drugs and some of the other psychiatric drugs that might be contributing to violence.”
SSRIs, or selective serotonin reuptake inhibitors, are the most prescribed class of antidepressants for depression, anxiety disorders and many other mental health conditions. Several SSRIs have been on the market in the United States since the 1990s, including Prozac, Zoloft and Celexa. Experts agree that there is no scientific evidence or correlation between these drugs and violence towards others.
Tuesday’s report states that HHS will assemble a working group of federal officials to evaluate SSRI prescribing patterns, specifically among children. HHS will also “evaluate the therapeutic harms and benefits of current diagnostic thresholds,” or the current common practices doctors use to diagnose patients with mental health disorders.
Dr. Theresa Miskimen Rivera, president of the American Psychiatric Association said access to care, not over-medication is the bigger problem when it comes to helping kids’ mental health in the country, and there is no mention of the issue in the report. The report said addressing a child’s nutrition, screen time, and exercise can improve their mental health, but can’t address everything. “Psychiatric conditions are complex in nature,” she said. Extreme poverty, post traumatic stress disorder, trauma-related factors should also be addressed, but there is no mention in the report of any of those issues either.
“In terms of over medication, that’s not what we do. We have a comprehensive evaluation and we are evidence based. We diagnose than create a comprehensive treatment plan, “ Miskimen Rivera told CNN. “Medication can save lives, not only in children, but in adults and elderly.”
When asked about whether or not the commission chose to consider gun violence – the leading cause of death for children – as one of the issues to be investigated, Kennedy doubled down on the issue of prescription drugs, saying “We are doing studies now, or initiating studies to look at the correlation and the connection, potential connection between over medicating our kids and this violence.”
HHS will also work with the White House Domestic Policy Council on a new vaccine framework that, the report said, will ensure “America has the best childhood vaccine schedule” and ensure “scientific and medical freedom.”
The report comes as Kennedy continues to defend his shakeup of the US Centers for Disease Control and Prevention over vaccine policy, including the ouster of CDC Director Dr. Susan Monarez.
The administration will also increase oversight of “deceptive” direct-to-consumer advertising of pharmaceutical products, including from social media influencers and telehealth companies, it said.
Food policy stays the course
FDA will continue work on developing a definition for ultraprocessed foods, but the report bypasses recommendations, like those of former FDA Director Dr. David Kessler, to essentially order certain additives off the market until they are reviewed.
Dr. Dariush Mozaffarian, director of Tufts Food is Medicine Institute said a definition of ultraprocessed foods would be “really important.” With more than half of calories in the food supply coming from ultraprocessed foods, addressing this and other issues involving the nation’s diet would mean a “massive fight with the industry and is going to be incredibly controversial, but is much needed.”
“Overall, this is really quite thorough, quite specific, and even if parts of this are accomplished, this could have tremendous positive impact for Americans,” Mozaffarian told CNN.
Other experts, like Marion Nestle, agreed the report was ambitious in scope, but noted it fell short on regulatory action. “What’s still missing is regulation. So much of this is voluntary, work with, promote, partner,” said Nestle, who is the Paulette Goddard professor emerita of nutrition, food studies and public health at New York University.
The report also nods to new, user-friendly dietary guidelines expected later this year. Kennedy has promised a vastly shortened set of recommendations that will emphasize whole foods.
The commission also cited ongoing work to reduce ultraprocessed foods in the Supplemental Nutrition Assistance Program (SNAP) and Head Start.
While the report also touches on agriculture deregulation with the aim of making it easier for small farms to get greater access to markets and schools, Ken Cook, co-founder of the Environmental Working Group, a health advocacy organization said the report abandons earlier MAHA promises to ban toxic pesticides and instead “echoes the pesticide industry’s talking points.”
“Secretary Kennedy and President Trump cynically convinced millions they’d protect children from harmful farm chemicals – promises now exposed as hollow,” Cook said in a statement.
There were minor changes from the draft document leaked in August. For instance, the August 6 draft stated that the FDA and other agencies will crack down on “Illegal Chinese Vapes,” while the final version promises enforcement on vapes more broadly.
“We support the goal of making children healthier and addressing and preventing chronic disease, but unfortunately, the recommendations fall short in some really critical ways,” Laura Kate Bender, vice president nationwide advocacy and public policy for the American Lung Association told CNN.
“They continue to cast doubt on vaccines, one of the most, important, proven public health interventions that we can have for kids health. They don’t address some major contributors to diseases in kids like pollution, tobacco use, beyond the mention of vaping, and this report is coming out at the same time that we’re continuing to see dramatic cuts in staff and funding of a lot of the programs that could make the good parts of the report a reality.”
The report’s emphasis on kids’ health can help overall, Dr. Michelle Macy, director of the Mary Ann & J. Milburn Smith Child Health Outcomes, Research and Evaluation Center in Chicago told CNN. “I’m really trying to look for bright spots in this report, and I think that the focus on data and infrastructure for us to be able to answer big questions about what environmental and food exposures and medication exposures do to shape the trajectory of someone’s health and chronic disease across the lifespan is something that has promise and potential.”
Dr. Richard Besser, pediatrician and president and CEO of the Robert Wood Johnson Foundation said that having a focus on preventing chronic disease in children is a good thing, but he said, with Kennedy’s track record that includes firing thousands of federal health employees, slashing millions in health research funding, dismantling entire offices that managed important issues like smoking and chronic disease specifically, in addition to his “assault on vaccinations” will undermine any potential good of this kind of report.
“Neither RFK Jr.’s record, nor his policies outlined in the report give me confidence that he is going to make any difference whatsoever on chronic diseases in children,” Besser told CNN.
The leading risk factor for death in the United States is the American diet.
About a decade ago, the American Heart Association (AHA) expressed concern that its “2020 target of improving cardiovascular health by 20% by 2020 will not be reached if current trends continue.” By 2006, most people were already not smoking and had nearly achieved their goal for exercise. But when it came to healthy diet score, only about 1 percent got a 4 or 5 out of its diet quality score of 0 to 5, as you can see below and at 0:35 in my video, Friday Favorites: The Scientific Consensus on a Healthy Diet. And that’s with such “ideal” criteria as drinking less than four and a half cups of soda a week.
In the last decade, the AHA saw a bump in the prevalence of the ideal healthy diet score to about 1 percent of Americans reaching those kinds of basic criteria, but, given its “aggressive” goal of reaching a “20% target” by 2020, it hoped to turn that 1 percent into about 1.2 percent. (Really, as you can see here and at 1:01 in my video.)
So, how’d we do? According to the 2019 update, it seems we’ve slipped down to as low as one in a thousand, and American teens scored a big fat zero. No wonder, perhaps, that “for all mortality-based metrics, the US rank declined…to 27th or 28th among 34 OECD [industrialized] countries. Citizens living in countries with a substantially lower gross domestic product and health expenditure per capita…have lower mortality rates than those in the United States.” Slovenia, for example, beat the United States, ranking 24th in life expectancy. More recently, the United States’s life expectancy slipped further, down to 43rd in the world, although the United States spent the most ($3.0 trillion) on health care…”
What is the leading risk factor for death in the United States? As seen below and at 2:04 in my video, it is the standard American diet. Those trillions in health care spending aren’t addressing the root cause of disease, disability, and death.
Here are some of the lung cancer death curves, below and at 2:08 in my video:
It took decades to finally turn the corner, but it’s so nice to finally see those drops. When will we see the same with diet?
“Approximately 80% of chronic disease and premature death could be prevented by not smoking, being physically active, and adhering to a healthful dietary pattern.” What exactly is meant by “healthy diet”? “Unfortunately, media messages surrounding nutrition are often inconsistent, confusing, and do not enable the public to make positive changes in health behaviors….Certainly, there is pressure within today’s competitive journalism market for sensationalism. There may even be a disincentive to present the facts in the context of the total body of information consumers need to act on dietary recommendations.” And there’s an incentive to sell more magazines and newspapers. The paper I’m quoting was written in 1997, before the lure of clickbait headlines. In fact, about three-quarters of a century ago, it was noted: “It is unfortunate that the subject of nutrition seems to have a special appeal to the credulous, the social zealot and, in the commercial field, the unscrupulous….The combination is one calculated to strike despair in the hearts of the sober, objective scientist.”
Indeed, the most important health care problem we face may be “our poor lifestyle choices based on misinformation.” It is like the climate change deniers: “Analogous to outspoken cynics denying climate change and influencing public opinion, healthy lifestyle and dietary advice are overshadowed by critics, diet books, the food industry, and misguided information in the media.” Maybe we need an entity like the Intergovernmental Panel on Climate Change (IPCC)—but for nutrition.
These days, “no single expert, regardless of academic stature or reputation, has the prominence to overcome the obstacles created by confusing media messages and deliver the fundamental principles of healthy living effectively to the public.”
What if there were “a global coalition consisting of a variety of nutrition experts, who collectively represent the views held by the majority of scientists, physicians, and health practitioners” that could “serve as the guiding resource of sound nutrition information for improved health and prevention of disease”?
Enter the True Health Initiative, which “was conceived for that very purpose.” A nonprofit coalition of hundreds of experts from dozens of countries has agreed to a consensus statement on the fundamentals of healthy living. See www.truehealthinitiative.org.
Spoiler alert: The healthiest diet is one generally comprised mostly of minimally processed plants.
Green smoothies are put to the test for the autoimmune disease lupus.
There are dozens and dozens of journals I try to stay on top of every month, and one I always anticipate is TheInternational Journal of Disease Reversal and Prevention, a peer-reviewed medical “journal created to document the science of nutrition and lifestyle to prevent, suspend and reverse disease,” with an editor-in-chief no less prestigious than Dr. Kim Williams, past president of the American College of Cardiology. I was honored to join its editorial advisory board, along with so many of my heroes. The best part? It’s free. Go to IJDRP.org and put in your email to subscribe at no cost, and you’ll be alerted when new issues are out, which you can download in full in PDF form. (Did I mention it’s free?)
When it comes to chronic lifestyle diseases, wrote Dr. Williams, “Instead of preventing chronic lifestyle diseases, we [doctors] manage. Never cure, just mitigate. Why? Because of finance, culture, habit, and tradition.” There are many of us, though, who “envision a world where trillions of dollars are not spent on medical care that should never have been necessary, but rather on infrastructure, environment, education, and advancing science. For this reason, comes TheInternational Journal of Disease Reversal and Prevention (IJDRP).” After all, wrote the journal’s co-founder, “Without data, you’re just another person with an opinion.”
To give you a taste of the journal: How about pitting plants against one of the most inflammatory diseases out there—lupus, an autoimmune disease in which your body can start attacking your DNA? Kidney inflammation is a common consequence, and even with our armamentarium of immunosuppressant drugs and steroids, lupus-induced kidney inflammation can lead to end-stage renal disease, which means dialysis, and even death. That is, unless you pack your diet with some of the most anti-inflammatory foods out there and your kidney function improves so much you no longer need dialysis or a kidney transplant. Another similar case was presented with a resolution in symptoms and normal kidney function, unless the patient deviated from the diet and his symptoms then reappeared.
As I discuss in my video Anti-Inflammatory Diet for Lupus, even just cutting out animal products can make a difference. Researchers randomized people to remove meat, eggs, and dairy from their diets without significantly increasing fruit and vegetable intake and found that doing just that can lower C-reactive protein levels by nearly a third within eight weeks, as you can see below and at 2:21 in my video. (Our C-reactive protein level is a sensitive indicator of whole-body inflammation.)
But with lupus, the researchers didn’t mess around. Each day, the study subjects were to eat a pound of leafy greens and cruciferous vegetables like kale, fruits like berries, and lots of chia or flax, and drink a gallon of water. We’re talking about a green smoothie diet to extinguish lupus flares. (Note, though, that if your kidneys are already compromised, this should be done under physician supervision so they can monitor your electrolytes like potassium and make sure you don’t get overloaded with fluid.) Bottom line? With such remarkable improvements due to dietary changes alone, the hope is that researchers will take up the mantle and formally put it to the test.
Reversals of autoimmune inflammatory skin disease can be particularly striking visually. A woman with a 35-year history of psoriasis that had been unsuccessfully managed for 19 years with drugs suffered from other autoimmune conditions, including Sjogren’s syndrome. She was put on an extraordinarily healthy diet packed with greens and other vegetables, fruits, nuts, seeds, avocados, and some whole grains, and boom! Within one year, she went from 40 percent of her entire body surface area inflamed and affected down to 0 percent, completely clear, and, as a bonus, her Sjogren’s symptoms resolved, too, while helping to normalize her weight and cholesterol. You can see before and after photos below and at 3:39 in my video.
I think I only have one other video on lupus: Fighting Lupus with Turmeric: Good as Gold. It’s not for lack of trying, though. There just hasn’t been much research out there.
Those on a healthy plant-based diet who have elevated homocysteine levels despite taking sufficient vitamin B12 may want to consider taking a gram a day of contaminant-free creatine.
The average blood levels of homocysteine in men are about 1.5 points higher than in women, which may be one of the reasons men tend to be at higher risk for cardiovascular disease. Women don’t need to make as much creatine as men since they tend to have less muscle mass. That may help explain “the ‘gender gap’ in homocysteine levels.” If you remember from my previous video and as seen below and at 0:36 in The Efficacy and Safety of Creatine for High Homocysteine, in the process of making creatine, our body produces homocysteine as a by-product. So, for people with stubbornly high homocysteine levels that don’t respond sufficiently to B vitamins, “creatine supplementation may represent a practical strategy for decreasing plasma homocysteine levels”—that is, lowering the level of homocysteine into the normal range.
It seemed to work in rats. What about humans? Well, it worked in one study, but it didn’t seem to work in another. It didn’t work in yet another either. And, in another study, homocysteine levels were even driven up. So, this suggestion that taking creatine supplements would lower homocysteine was called into question.
However, all those studies were done with non-vegetarians, so they were already effectively supplementing with creatine every day in the form of muscle meat. In that way, researchers were testing higher versus lower supplementation. Those eating strictly plant-based make all their creatine from scratch, so they may be more sensitive to an added creatine source. There weren’t any studies on creatine supplementation in vegans to lower homocysteine until now.
Researchers took vegans who were not supplementing their diets with vitamin B12, so some of their homocysteine levels were through the roof. A few were as high as 50 when the ideal is more like under 10, for example. After taking some creatine for a few weeks, all of their homocysteine levels normalized. You can see the before and after in the graph below and at 2:04 in my video.
Now, they didn’t normalize, as that would have been a level under 10, but that’s presumably because they weren’t taking any B12. Give vegetarians and vegans vitamin B12 supplements, either dosing daily or once a week, and their levels normalize in a matter of months, as you can see below and at 2:20 in my video. However, the fact that you could bring down homocysteine levels with creatine alone, even without any B12, suggests—to me at least—that if your homocysteine is elevated (above 10) on a plant-based diet despite taking B12 supplements and eating greens and beans to get enough folate, it might be worth experimenting with supplementing with a gram of creatine a day for a few weeks to see if your homocysteine comes down.
Why just a single gram? That’s approximately how much non-vegetarians do not have to make themselves; it’s the amount that erased vegetarian discrepancies in blood and muscle, as you can see in the graph below and at 3:01 in my video, and how much has been shown to be safe in the longer term.
How safe is it? We can take a bit of comfort in the fact that it’s “one of the world’s best-selling dietary supplements,” with literally billions of servings taken, and the only consistently reported side effect has been weight gain, presumed to be from water retention. The only serious side effects appear to be among those with pre-existing kidney diseases taking whopping doses closer to 20 grams a day. A concern was raised that creatine could potentially form a carcinogen known as N-nitrososarcosine when it hit the acid bath of the stomach, but, when it actually put to the test, researchers found this does not appear to be a problem.
Bottom line: Doses of supplemental creatine up to 3 grams a day are “unlikely to pose any risk,” provided “high purity creatine” is used. However, as we all know, dietary supplements in the United States “are not regulated by the US Food and Drug Administration and may contain contaminants or variable quantities of the desired supplement” and may not even contain what’s on the label. We’re talking about “contaminants…that may be generated during the industrial production.” When researchers looked at 33 samples of creatine supplements made in the United States and Europe, they found that they all actually contained creatine, which is nice, but about half exceeded the maximum level recommended by food safety authorities for at least one contaminant. The researchers recommend that “consumers give their preference to products obtained by producers that ensure the highest quality control and certify the maximum amount of contaminants present in their products.” Easier said than done.
Because of the potential risks, I don’t think people should take creatine supplements willy-nilly, but the potential benefits may exceed the potential risks if, again, you’re on a healthy plant-based diet and taking B12, and your homocysteine levels are still not under 10. In that case, I would suggest giving a gram a day of creatine a trying to see if it brings it down.
The reason I did this whole video series goes back to “Risks of Ischaemic Heart Disease and Stroke in Meat Eaters, Fish Eaters, and Vegetarians Over 18 Years of Follow-Up: Results from the Prospective EPIC-Oxford Study,” which found that, although the overall cardiovascular risk is lower in vegetarians and vegans combined, they appeared to be at slightly higher stroke risk, as you can see in the graph below and at 5:06 in my video.
I went through a list of potential causes, as you can see at 5:11 and below, and arrived at elevated homocysteine. What’s the solution? A regular, reliable source of vitamin B12. The cheapest, easiest method that I personally use is one 2,500 mcg chewable tablet of cyanocobalamin, the most stable source of B12, once a week. (In fact, you can just use 2,000 mcg once a week.) And, again, a backup plan for those doing that but still having elevated homocysteine is an empirical trial of a single gram a day of creatine supplementation, which was shown to improve at least capillary blood flow in those who started out with high homocysteine levels.
In sum, plant-based diets appear to “markedly reduce risk” for multiple leading killer diseases—heart disease, type 2 diabetes, and many common types of cancer—but “an increased risk for stroke may represent an ‘Achilles heel.’ Nonetheless, vegans have the potential to achieve a truly exceptional ‘healthspan’ if they face this problem forthrightly by restricting salt intake and taking other practical measures that promote cerebrovascular [brain artery] health…Nonetheless, these considerations do not justify nutritional nihilism. On balance, low-fat vegan diets offer such versatile protection for long-term health that they remain highly recommendable. Most likely, the optimal strategy is to adopt such a [plant-based] diet, along with additional measures—appropriate food choices, exercising training, judicious supplementation [of vitamin B12]—that will mitigate the associated stroke risk.” And try not to huff whipped cream charging canister gas. Leave the “whippets” alone.
This concludes my series on stroke risk. If you missed any of the other videos, see the related posts below.
I’m assuming that nearly everyone taking their B12 will have normal homocysteine levels, so these last two videos are just for the rare person who doesn’t. However, those on a healthy plant-based diet with elevated homocysteine levels despite taking sufficient vitamin B12 should consider taking a gram a day of contaminant-free creatine, which should be about a quarter teaspoon.
Where do you get contaminant-free creatine? Since regulations are so lax, you can’t rely on supplement manufacturers no matter what they say, so I would recommend going directly to the chemical suppliers that sell it to laboratories and guarantee a certain purity. Here are some examples (in alphabetical order) of some of the largest companies where you can get unadulterated creatine: Alfa Aesar, Fisher Scientific, Sigma-Aldrich, and TCI America.
Why are U.S. taxpayers giving billions of dollars to support the likes of the sugar and meat industries?
The rise in calorie surplus sufficient to explain the obesity epidemic was less a change in food quantity than in food quality. Access to cheap, high-calorie, low-quality convenience foods exploded, and the federal government very much played a role in making this happen. U.S. taxpayers give billions of dollars in subsidies to prop up the likes of the sugar industry, the corn industry and its high-fructose syrup, and the production of soybeans, about half of which is processed into vegetable oil and the other half is used as cheap feed to help make dollar-menu meat. You can see a table of subsidy recipients below and at 0:49 in my video The Role of Taxpayer Subsidies in the Obesity Epidemic. Why do taxpayers give nearly a quarter of a billion dollars a year to the sorghum industry? When was the last time you sat down to some sorghum? It’s almost all fed to cattle and other livestock. “We have created a food price structure that favors relatively animal source foods, sweets, and fats”—animal products, sugars, and oils.
The Farm Bill started out as an emergency measure during the Great Depression of the 1930s to protect small farmers but was weaponized by Big Ag into a cash cow with pork barrel politics—including said producers of beef and pork. From 1970 to 1994, global beef prices dropped by more than 60 percent. And, if it weren’t for taxpayers “sweetening the pot” with billions of dollars a year, high-fructose corn syrup would cost the soda industry about 12 percent more. Then we hand Big Soda billions more through the Supplemental Nutrition Assistance Program (SNAP), formerly known as the Food Stamps Program, to give sugary drinks to low-income individuals.Why is chicken so cheap? After one Farm Bill, corn and soy were subsidized below the cost of production for cheap animal fodder. We effectively handed the poultry and pork industries about $10 billion each. That’s not chicken feed—or rather, it is!
As you can see below and at 2:03 in my video, thanks in part to subsidies, dairy, meats, sweets, eggs, oils, and soda were all getting relatively cheaper compared to the overall consumer food price index as the obesity epidemic took off, whereas the relative cost of fresh fruits and vegetables doubled. This may help explain why, during about the same period, the percentage of Americans getting five servings of fruits and vegetables a day dropped from 42 percent to 26 percent. Why not just subsidize produce instead? Because that’s not where the money is.
“To understand what is shaping our foodscape today, it is important to understand the significance of differential profit.” Whole foods or minimally processed foods, such as canned beans or tomato paste, are what the food business refers to as “commodities.” They have such slim profit margins that “some are typically sold at or below cost, as ‘loss leaders,’ to attract customers to the store” in the hopes that they’ll also buy the “value-added” products. Some of the most profitable products for producers and vendors alike are the ultra-processed, fatty, sugary, and salty concoctions of artificially flavored, artificially colored, and artificially cheap ingredients—thanks to taxpayer subsidies.
Different foods reap different returns. Measured in “profit per square foot of selling space” in the supermarket, confectionaries like candy bars consistently rank among the most lucrative. The markups are the only healthy thing about them. Fried snacks like potato chips and corn chips are also highly profitable. PepsiCo’s subsidiary Frito-Lay brags that while its products represented only about 1 percent of total supermarket sales, they may account for more than 10 percent of operating profits for supermarkets and 40 percent of profit growth.
It’s no surprise, then, that the entire system is geared towards garbage. The rise in the calorie supply wasn’t just more food but a different kind of food. There’s a dumb dichotomy about the drivers of the obesity epidemic: Is it the sugar or the fat? They’re both highly subsidized, and they both took off. As you can see below and at 4:29 and 4:35 in my video, along with a significant rise in refined grain products that is difficult to quantify, the rise in obesity was accompanied by about a 20 percent increase in per capita pounds of added sugars and a 38 percent increase in added fats.
More than half of all calories consumed by most adults in the United States were found to originate from these subsidized foods, and they appear to be worse off for it. Those eating the most had significantly higher levels of chronic disease risk factors, including elevated cholesterol, inflammation, and body weight.
If it really were a government of, by, and for the people, we’d be subsidizing healthy foods, if anything, to make fruits and vegetables cheap or even free. Instead, our tax dollars are shoveled to the likes of the sugar industry or to livestock feed to make cheap, fast-food meat.
Speaking of sorghum, I had never had it before and it’s delicious! In fact, I wish I had discovered it before How Not to Diet was published. I now add sorghum and finger millet to my BROL bowl which used to just include purple barley groats, rye groats, oat groats, and black lentils, so the acronym has become an unpronounceable BROLMS. Anyway, sorghum is a great rice substitute for those who saw my rice and arsenic video series and were as convinced as I am that we need to diversify our grains.
We now turn to marketing. After all of the taxpayer-subsidized glut of calories in the market, the food industry had to find a way to get it into people’s mouths. So, next: The Role of Marketing in the Obesity Epidemic.
We’re about halfway through this series on the obesity epidemic. If you missed any so far, check out the related videos below.
Here is a review of reviews on the health effects of tea, coffee, milk, wine, and soda.
If you’ve watched my videos or read my books, you’ve heard me say, time and again, the best available balance of evidence. What does that mean? When making decisions as life-or-death important as what to feed ourselves and our families, it matters less what a single study says, but rather what the totality of peer-reviewed science has to say.
Individual studies can lead to headlines like “Study Finds No Link Between Secondhand Smoke and Cancer,” but to know if there is a link between secondhand smoke and lung cancer, it would be better to look at a review or meta-analysis that compiles multiple studies. The problem is that some reviews say one thing—for instance, “breathing other people’s tobacco smoke is a cause of lung cancer”—and other reviews say another—such as, the effects of secondhand smoke are insignificant and further such talk may “foster irrational fears.” And, while we’re at it, you can indulge in “active smoking of some 4-5 cigarettes per day” without really worrying about it, so light up!
Why do review articles on the health effects of secondhand smoke reach such different conclusions? As you can imagine, about 90 percent of reviews written by researchers affiliated with the tobacco industry said it was not harmful, whereas you get the opposite number with independent reviews, as you can see below and at 1:18 in my video Friday Favorites: What Are the Best Beverages?. Reviews written by the tobacco industry–affiliated researchers had 88 times the odds of concluding that secondhand smoke was harmless. It was all part of “a deliberate strategy to use scientific consultants to discredit the science…” In other words, “the strategic and long run antidote to the passive smoking issue…is developing and widely publicizing clear-cut, credible, medical evidence that passive smoking [secondhand smoke] is not harmful to the non-smoker’s health.”
Can’t we just stick to the independent reviews? The problem is that industry-funded researchers have all sorts of sneaky ways to get out of declaring conflicts of interest, so it can be hard to follow the money. For instance, it was found that “77% failed to disclose the sources of funding” for their research. But, even without knowing who funded what, the majority of reviews still concluded that secondhand smoke was harmful. So, just as a single study may not be as helpful as looking at a compilation of studies on a topic, a single review may not be as useful as a compilation of reviews. In that case, looking at a review of reviews can give us a better sense of where the best available balance of evidence may lie. When it comes to secondhand smoke, it’s probably best not to inhale, as you can see in the graph below and at 2:30 in my video.
Wouldn’t it be cool if there were reviews of reviews for different foods and drinks? Voila! Enter “Associations Between Food and Beverage Groups and Major Diet-Related Chronic Diseases: An Exhaustive Review of Pooled/Meta-Analyses and Systematic Reviews.” Let’s start with the drinks. As you can see below and at 2:51 in my video, the findings were classified into three categories: protective, neutral, or deleterious.
First up: tea versus coffee. As you can see in the graph below and at 2:58, most reviews found both beverages to be protective for whichever condition they were studying, but you can see how this supports my recommendation for tea over coffee. Every cup of coffee is a lost opportunity to drink a cup of green tea, which is even healthier.
It’s no surprise that soda sinks to the bottom, as you can see below and at 3:20 in my video, but 14 percent of reviews mentioned the protective effects of drinking soda. What?! Well, most were references to papers like “High Intake of Added Sugar Among Norwegian Children and Adolescents,” a cross-sectional study that found that eighth-grade girls who drank more soda were thinner than girls who drank less. Okay, but that was just a snapshot in time. What do you think is more likely? That the heavier girls were heavier because they drank less soda, or that they drank less sugary soda because they were heavier? Soda abstention may therefore be a consequence of obesity, rather than a cause, yet it gets marked down as having a protective association.
Study design flaws may also account for wine numbers, as seen below and at 4:07 in my video. This review of reviews was published in 2014, before the revolution in our understanding of “alcohol’s evaporating health benefits,” suggesting that the “presumed health benefits from ‘moderate’ alcohol use [may have] finally collapsed”—thanks in part to a systematic error of misclassifying former drinkers as if they were lifelong abstainers, as I revealed in a deep dive in a video series on the subject.
Sometimes there are unexplainable associations. For example, one of the soft drink studies found that increased soda consumption was associated with a lower risk of certain types of esophageal cancers. Don’t tell me. Was the study funded by Coca-Cola? Indeed. Does that help explain the positive milk studies, as you can see in the graph below and at 5:02 in my video? Were they all just funded by the National Dairy Council?
As shown below and at 5:06, even more conflicts of interest have been found among milk studies than soda studies, with industry-funded studies of all such beverages “approximately four to eight times more likely to be favorable to the financial interests of the [study] sponsors than articles without industry-related funding.”
Funding bias aside, though, there could be legitimate reasons for the protective effects associated with milk consumption. After all, those who drink more milk may drink less soda, which is even worse, so they may come out ahead. It may be more than just relative benefits, though. The soda-cancer link seems a little tenuous and not just because of the study’s financial connection to The Coca-Cola Company. It’s hard to imagine a biologically plausible mechanism, whereas even something as universally condemned as tobacco isn’t universally bad. As I’ve explored before, more than 50 studies have consistently found a protective association between nicotine and Parkinson’s disease. Even secondhand smoke may be protective. Of course, you’d still want to avoid it. Passive secondhand smoke may decrease the risk of Parkinson’s, but it increases the risk of stroke, an even deadlier brain disease, not to mention lung cancer and heart disease, which has killed off millions of Americans since the first Surgeon General’s report was released, as you can see below and at 6:20 in my video.
Thankfully, by eating certain vegetables, we may be able to get some of the benefits without the risks, and the same may be true of dairy. As I’ve described before, the consumption of milk is associated with an increased risk of prostate cancer, leading to recommendations suggesting that men may want to cut down or minimize their intake, but milk consumption is also associated with decreased colorectal cancer risk. This appears to be a calcium effect. Thankfully, we may be able to get the best of both worlds by eating high-calcium plant foods, such as greens and beans.
What does our review-of-reviews study conclude about such plant-based foods, in comparison to animal-based foods? We’ll find out next.
Stay tuned for the exhaustive review of meta-analyses and systematic reviews on major diet-related chronic diseases found for food groups in What Are the Best Foods?.
Ancient types of wheat, like kamut, are put to the test for inflammation, blood sugar, and cholesterol control.
The number one killer in the United States and around the world is what we eat. As you can see in the graph below and at 0:15 in my video Friday Favorites: Are Ancient Grains Healthier?, our diet kills millions more than tobacco. What are the five most important things we can do to improve our diets, based on the single most comprehensive global study of the health impact of nutrition? Eat less salt, eat more nuts, eat more non-starchy vegetables, eat more fruit, and, finally, eat more whole grains. Any particular type of whole grains? What about so-called ancient grains? Are they any better than modern varieties? For instance, what about kamut, described as “mummy wheat” and supposedly unearthed from an Egyptian tomb?
After WWII, the wheat industry selected particularly high-yielding varieties for pasta and bread. Over the past few years, though, some of the more ancient grains—“defined as those species that have remained unchanged over the last hundred years” despite agricultural revolutions—have been reintroduced to the market.
As you can see below and at 1:13 in my video, nutritionally, kamut and einkorn wheat, which is the oldest wheat, have more eyesight-improving yellow carotenoid pigments, such as lutein and zeaxanthin, compared to modern bread and pastry wheat, because the pigments have been bred out of the bread intentionally. People want their white bread white, but modern pasta flour (durum wheat) maintains much of that yellow nutritional hue.
As you can see in the graph below and at 1:41 in my video, modern wheat may have less lutein, but it tends to have more vitamin E, as seen in the graph below and at 1:45. Based on straight vitamin and mineral concentrations, it’s pretty much a wash. Both modern and primitive kinds of wheat have a lot of each, but primitive wheats do have more antioxidant capacity, likely due to their greater polyphenol content, as you can see in the graph below and at 2:00 in my video. To know if that makes any difference, though, we have to put it to the test.
If you expose human liver cells to digested bread made out of ancient grains (kamut and spelt), heritage kinds of wheat, or modern strains, then expose the cells to an inflammatory stimulus, the modern wheat strains seem less able to suppress the inflammation, as you can see in the graphs below and at 2:09 in my video. The investigators conclude that even though these different grains seem to be very similar nutritionally, they appear to exert different effects on human cells, “confirming the potential health benefits of ancient grains.” That was in a petri dish, though. What about people? If ancient kinds of wheat are better at suppressing inflammation, what if you took people with irritable bowel syndrome (IBS) and randomized them to receive six weeks of wheat products made out of modern wheat or ancient wheat—in this case, kamut? Same amount of wheat, just different types. If there is no difference between the wheats, there’d be no difference in people’s symptoms, right? But, when study participants in the control group were switched to the ancient wheat kamut, they experienced less abdominal pain, less frequent pain, less bloating, more satisfaction with stool consistency, and less interference with their quality of life, compared to the modern wheat. So, after switching to the ancient wheat, they had “a significant global improvement in the extent and severity of symptoms related to IBS…”
What about liver inflammation? The liver function of those with nonalcoholic fatty liver disease randomized to eat kamut improved, compared to those eating the same amount of regular wheat, suggesting kamut is superior, as you can see below and at 3:47 in my video.
People with diabetes, had better cholesterol and better insulin sensitivity on the same ancient grain, as shown below and at 3:57.
And those with heart disease? They had better blood sugar control and better cholesterol, as shown below and at 4:03.
And, people without overt heart disease had better artery function, as you can see below and at 4:06 in my video.
The bottom line is that findings derived from human studies suggest that ancient wheat products are more anti-inflammatory and may improve things like blood sugar control and cholesterol. “Given that the overall number of human interventional trials conducted to date are numerically insufficient, it is not possible to definitively conclude that ancient wheat varieties are superior to all commercial, modern wheat counterparts in reducing chronic disease risk.” However, the best available data do suggest they’re better for us.
Regardless of what type of wheat you may eat, a word to the wise: Don’t eat the plastic bread-bag clip. A 45-year-old man presented with bloody stools, and his CT scan showed the offending piece of plastic from his bag of bread, as you can see below and at 4:53 in my video. When the patient was questioned, he “admitted to habitually eating quickly without chewing properly.”
Whole grains—ideally intact ones and ancient and modern varieties alike—are an integral part of my Daily Dozen checklist, the healthiest of healthy things I encourage everyone to try to fit into their daily routines.
Whole grains are especially good for our microbiome. Learn more in the related posts below. What about gluten? Also, see the related posts below.
Calories eaten in the morning count less than calories eaten in the evening, and they’re healthier, too.
Time-restricted feeding, where you limit the same amount of eating to a narrow evening window, has benefits compared to eating in the evening and earlier in the day, but it also has adverse effects because you’re eating so much, so late, as you can see below and at 0:12 my video The Benefits of Early Time-Restricted Eating.
The best of both worlds was demonstrated in 2018 when researchers put time-restricted feeding into a narrow window earlier in the day. As you can see below and at 0:28 in my video, individuals who were randomized to eat the same food, but only during an 8:00 a.m. to 3:00 p.m. eating window, experienced a drop in blood pressure, oxidative stress, and insulin resistance, even when all of the study subjects were maintained at the same weight. Same food, same weight, but with different results. The drops in blood pressure were extraordinary, from 123/82 down to 112/72 in five weeks, and that is comparable to the effectiveness of potent blood-pressure drugs.
The longest study to date on time-restricted feeding only lasted for 16 weeks. It was a pilot study without a control group that involved only eight people, but the results are still worth noting. Overweight individuals, who, like most of us, had been eating for more than 14 hours a day, were instructed to stick to a consistent 10- to 12-hour feeding window of their own choosing, as you can see below and at 1:17 in my video. On average, they were able to successfully reduce their daily eating duration by about four and a half hours and had lost seven pounds within 16 weeks.
They also reported feeling more energetic and sleeping better, as seen in the graph below and at 1:32 in my video. This may help explain why “all participants voluntarily expressed an interest in continuing unsupervised with the 10-11 hr time-restricted eating regimen after the conclusion of the 16-week supervised intervention.” You don’t often see that after weight-loss studies.
Even more remarkably, eight months later and even one year post-study, they had retained their improved energy and sleep (see in the graph below and 1:55 in my video), as well as retained their weight loss (see in the graph below and 1:58 in my video)—all from one of the simplest of interventions: sticking to a consistent 10- to 12-hour feeding window of their own choosing. How did it work? Even though the study “participants were not overtly asked to change nutrition quality or quantity,” they appeared to unintentionally eat hundreds of fewer calories a day. With self-selected time frames for eating, you wouldn’t necessarily think to expect circadian benefits, but because they had been asked to keep the eating window consistent throughout the week, “metabolic jet lag could be minimized.” The thinking is that because people tend to start their days later on weekends, they disrupt their own circadian rhythm. And, indeed, it is as if they had flown a few time zones west on Friday evening, then flew back east on Monday morning, as you can see in the graph below and at 2:40 in my video. So, some of the metabolic advantages may have been due to maintaining a more regular eating schedule.
Early or mid-day time-restricted feeding may have other benefits as well. Prolonged nightly fasting with reduced evening food intake has been associated with lower levels of inflammation and has also been linked to better blood sugar control, both of which might be expected to lower the risk of diseases, such as breast cancer. So, data were collected on thousands of breast cancer survivors to see if nightly fasting duration made a difference. Those who couldn’t go more than 13 hours every night without eating had a 36 percent higher risk of cancer recurrence. These findings have led to the suggestion that efforts to “avoid eating after 8 pm and fast for 13 h or more overnight may be a beneficial consideration for those patients looking to decrease cancer risk and recurrence,” though we would need a randomized controlled trial to know for sure.
Early time-restricted feeding may even play a role in the health of perhaps the longest-living population in the world, the Seventh-day Adventist Blue Zone in California. As you can see in the graph below and at 3:55 in my video, slim, vegetarian, nut-eating, exercising, non-smoking Adventists live about a decade longer than the general population.
Their greater life expectancy has been ascribed to these healthy lifestyle behaviors, but there’s one lesser-known component that may also be playing a role. Historically, eating two large meals a day, breakfast and lunch, with a prolonged overnight fast, was a part of Adventist teachings. Today, only about one in ten Adventists surveyed were eating just two meals a day. However, most of them, more than 60 percent of them, reported that breakfast or lunch was their largest meal of the day, as you can see below and at 4:26 in my video. Though this has yet to be studied concerning longevity, frontloading one’s calories earlier in the day with a prolonged nightly fast has been associated with significant weight loss over time. This led the researchers to conclude: “Eating breakfast and lunch 5–6 h apart and making the overnight fast last 18–19 h may be a useful practical strategy” for weight control. The weight may be worth the wait.
My big takeaway from all of the intermittent fasting research I looked at is, whenever possible, eat earlier in the day. At the very least, avoid late-night eating whenever you can. Eating breakfast like a king and lunch like a prince, with or without an early dinner for a pauper, would probably be best.
For more on fasting, fasting for disease reversal, and fasting and cancer, check the related videos below.
Alternate-day modified fasting is put to the test for lifespan extension.
Is it true that alternate-day calorie restriction prolongs life? Doctors have anecdotally attributed improvements in a variety of disease states to alternate-day fasting, including asthma; seasonal allergies; autoimmune diseases, such as rheumatoid arthritis and osteoarthritis; infectious diseases, such as toenail fungus, periodontal disease, and viral upper respiratory tract infections; neurological conditions, such as Tourette’s syndrome and Meniere’s disease; atrial fibrillation; and menopause-related hot flashes. The actual effect on chronic disease, however, remains unclear, as I discuss in my video Does Intermittent Fasting Increase Human Life Expectancy?.
Alternate-day fasting has been put to the test for asthma in overweight adults, and researchers found that asthma-related symptoms and control significantly improved, as did the patients’ quality of life, including objective measurements of lung function and inflammation. As you can see in the graphs below and at 0:56 in my video, there were significant improvements in peak airflow, mood, and energy. Their weight also improved—about a 19-pound drop in eight weeks—so it’s hard to tease out the effects specific to the fasting beyond the benefits we might expect from weight loss by any means. For the most remarkable study on alternate-day fasting, you have to go back more than a half-century. Though the 2017 cholesterol findings were the most concerning data I could find on alternate-day fasting, the most enticing was published in Spain in 1956. The title of the study translates as “The Hunger Diet on Alternate Days in the Nutrition of the Aged.” Inspired by the data being published on life extension with caloric restriction on lab rats, researchers split 120 residents of a nursing home in Madrid into two groups. Sixty residents continued to eat their regular diet, and the other half were put on an alternate-day modified fast. On the odd days of the month, they ate a regular 2,300-calorie diet; on the even days, they were given only a pound of fresh fruits and a liter of milk, estimated to add up to about 900 calories. This continued for three years. So, what happened?
As you can see below and at 2:16 in my video, throughout the study, 13 participants died in the control group, compared to only 6 in the intermittent fasting group, but those numbers were too small to be statistically significant.
What was highly significant, though, was the number of days spent hospitalized: Residents in the control group spent a total of 219 days in the infirmary, whereas the alternate-day fasting group only chalked up 123 days, as you can see below and at 2:38 in my video.
This is held up as solid evidence that alternate-day fasting may improve one’s healthspan and potentially even one’s lifespan, but a few caveats must be considered. It’s not clear how the residents were allocated to their respective groups. If, instead of being randomized, healthier individuals were inadvertently placed in the intermittent fasting group, that could skew the results in their favor. As well, it appears the director of the study was also in charge of medical decisions at the nursing home. In that role, he could have unconsciously been biased toward hospitalizing more folks in the control group. Given the progress that has been made in regulating human experimentation, it’s hard to imagine such a trial being run today, so we may never know if such impressive findings can be replicated.
Well, that was interesting! I had never even heard of that study until I started digging into the topic.
Check out my fasting series and popular videos on the subjecthere.
Ketogenic diets are put to the test for diabetes reversal.
As you can see at the start of my video Does a Ketogenic Diet Help Diabetes or Make It Worse?, ketogenic diets can lower blood sugars better than conventional diets. So much so, in fact, that there is a keto product company that claims ketogenic diets can “reverse” diabetes. However, they are confusing the symptom (high blood sugars) with the disease (carbohydrate intolerance). People with diabetes can’t properly handle carbohydrates, and this manifests as high blood sugars. Clearly, if you stick to eating mostly fat, your blood sugars will stay low, but you may be actually making the underlying disease worse at the same time.
We’ve known for nearly a century that if you put people on a ketogenic diet, their carbohydrate intolerance can skyrocket within just two days. Below and at 0:46 in my video, you can see a graph from the study showing the blood sugar response two days after eating sugar. On a high-carb diet, blood sugar response is about 90 mg/dL. But, the blood sugar response to the same amount of sugar after a high-fat diet is about 190 mg/dL, nearly double. The intolerance to carbohydrates skyrocketed on a high-fat diet.
After one week on an 80 percent fat diet, you can quintuple your blood sugar spike in reaction to the same carb load compared to a week on a low-fat diet, as you can see in the graph below and at 1:12 in my video.
Even a single day of excessive dietary fat intake can do it, as you can see in the graph below and at 1:26 in my video. If you’re going in for a diabetes test, having a fatty dinner the night before can adversely affect your results. Just one meal high in saturated fat can make carbohydrate intolerance, the cause of diabetes, worse within four hours.
Given enough weight loss by any means, whether from cholera or bariatric surgery, type 2 diabetes can be reversed, but a keto diet for diabetes may not just be papering over the cracks, but actively throwing fuel on the fire.
I’ve been trying to think of a good metaphor. It’s easy to come up with things that just treat the symptoms without helping the underlying disease, like giving someone with pneumonia aspirin for their fever instead of antibiotics. However, a keto diet for diabetes is worse than that because it may treat the symptoms while actively worsening the disease. It may be more like curing the fever by throwing that pneumonia patient out into a snow bank or “curing” your amputated finger by amputating your hand. One of the co-founders of masteringdiabetes.org suggested it’s like a CEO who makes their bad bottom line look better by borrowing tons of cash. The outward numbers look better, but on the inside, the company is just digging itself into a bigger hole.
Do you remember The Club, that popular car anti-theft device that attaches to the steering wheel and locks it in place so the steering column can only turn a few inches? Imagine you’re in a car at the top of a hill with the steering wheel locked. Then, the car starts rolling down the hill. What do you do? Imagine there’s also something stuck under your brake pedal. The keto-diet equivalent response to this situation is who cares if you’re barreling down into traffic with a locked steering wheel and no brakes—just stick to really straight deserted roads without any stop signs or traffic lights. If you do that, problem solved! The longer you go, the more speed you’ll pick up. If you should hit a dietary bump in the road or start to veer off the path, the consequences could get more and more disastrous over time. However, if you stick to the keto straight and narrow, you’ll be a-okay! In contrast, the non-keto response would be to just unlock the steering wheel and dislodge whatever’s under your brake. In other words, fix the underlying problem instead of just whistling past—and then into—the graveyard.
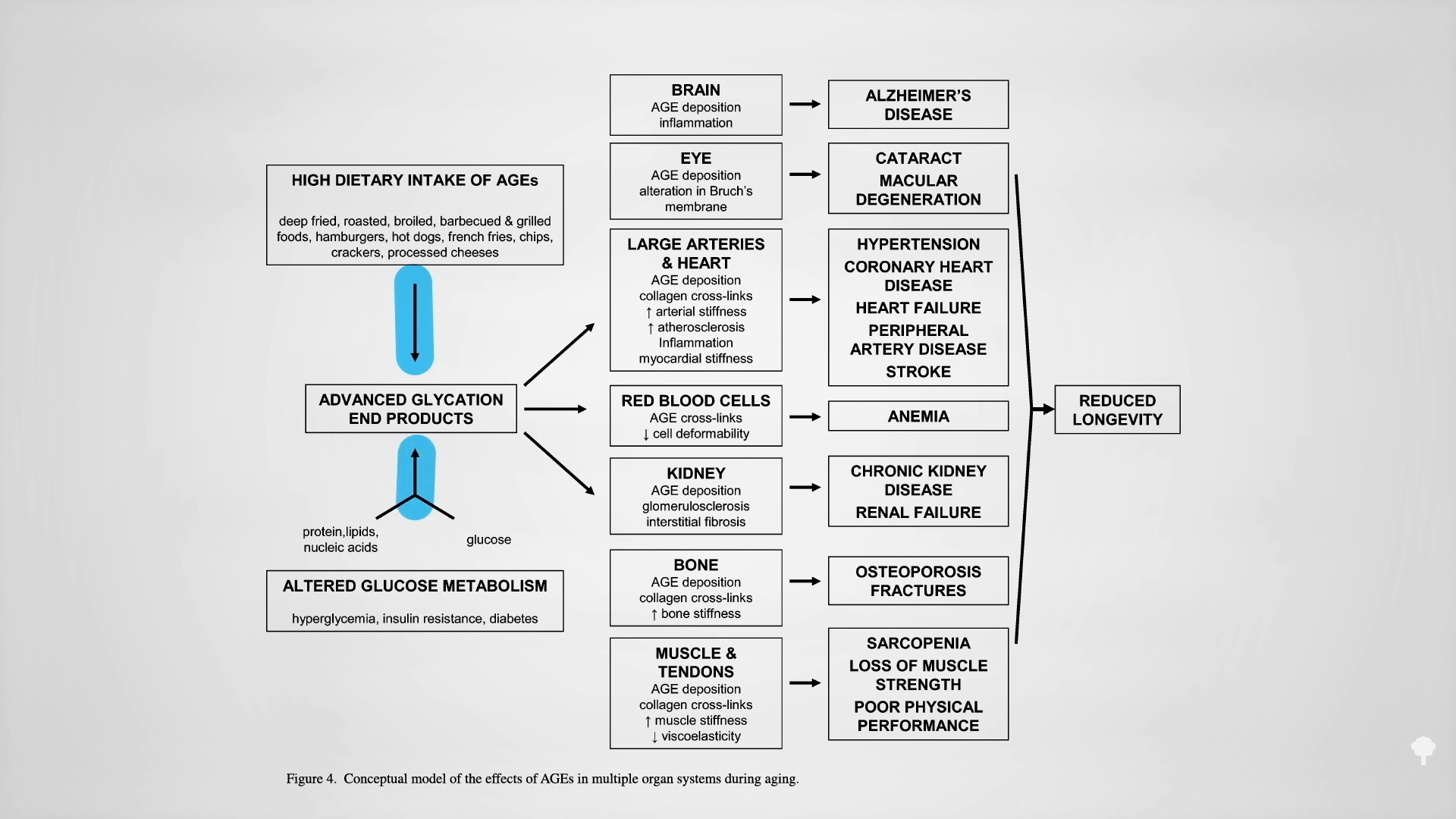
The reason keto proponents claim they can “reverse” diabetes is they can successfully wean type 2 diabetics off their insulin. That’s like faith-healing someone out of the need for a wheelchair by making them stay in bed the rest of their life. No need for a wheelchair if you never move. Their carbohydrate intolerance isn’t gone. Their diabetes isn’t gone. In fact, it could be just as bad or even worse. Type 2 diabetes is reversed when you are weaned off insulin while eating a normal diet like everyone else. Then and only then do you not have diabetes anymore. A true diabetes reversal diet, as you can see below and at 4:58 in my video, is practically the opposite of a ketogenic diet: getting diabetics off their insulin within a matter of weeks by eating more than 300 grams of carbs a day! The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal is the most potent creator of advanced glycation end products (AGEs), which are implicated in degenerative diseases—from Alzheimer’s and cataracts to kidney disease and strokes, as you can see below and at 5:31 in my video.
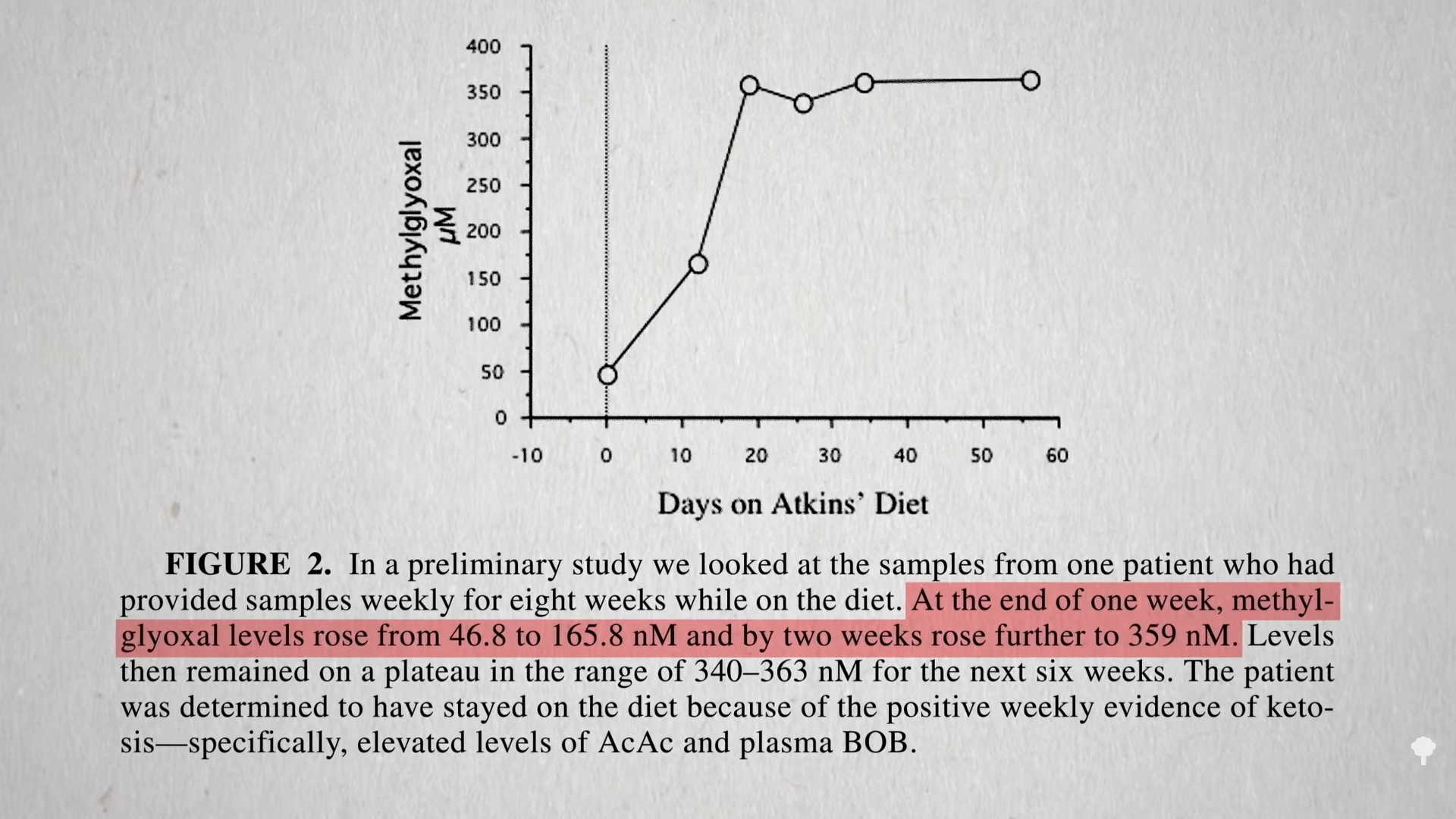
You get AGEs in your body from two sources: You can eat them preformed in your diet or make them internally from methylglyoxal if you have high blood sugar levels. On a keto diet, one would expect high exposure to preformed AGEs, since they’re found concentrated in animal-derived foods high in fat and protein, but we would expect less internal, new formation due to presumably low levels of methylglyoxal, given lower blood sugars from not eating carbs. Dartmouth researchers were surprised to find more methylglyoxal! As shown in the graph below and at 6:11 in my video, a few weeks on the Atkins diet led to a significant increase in methylglyoxal levels. Those in active ketosis did even worse, doubling the level of this glycotoxin in their bloodstream.
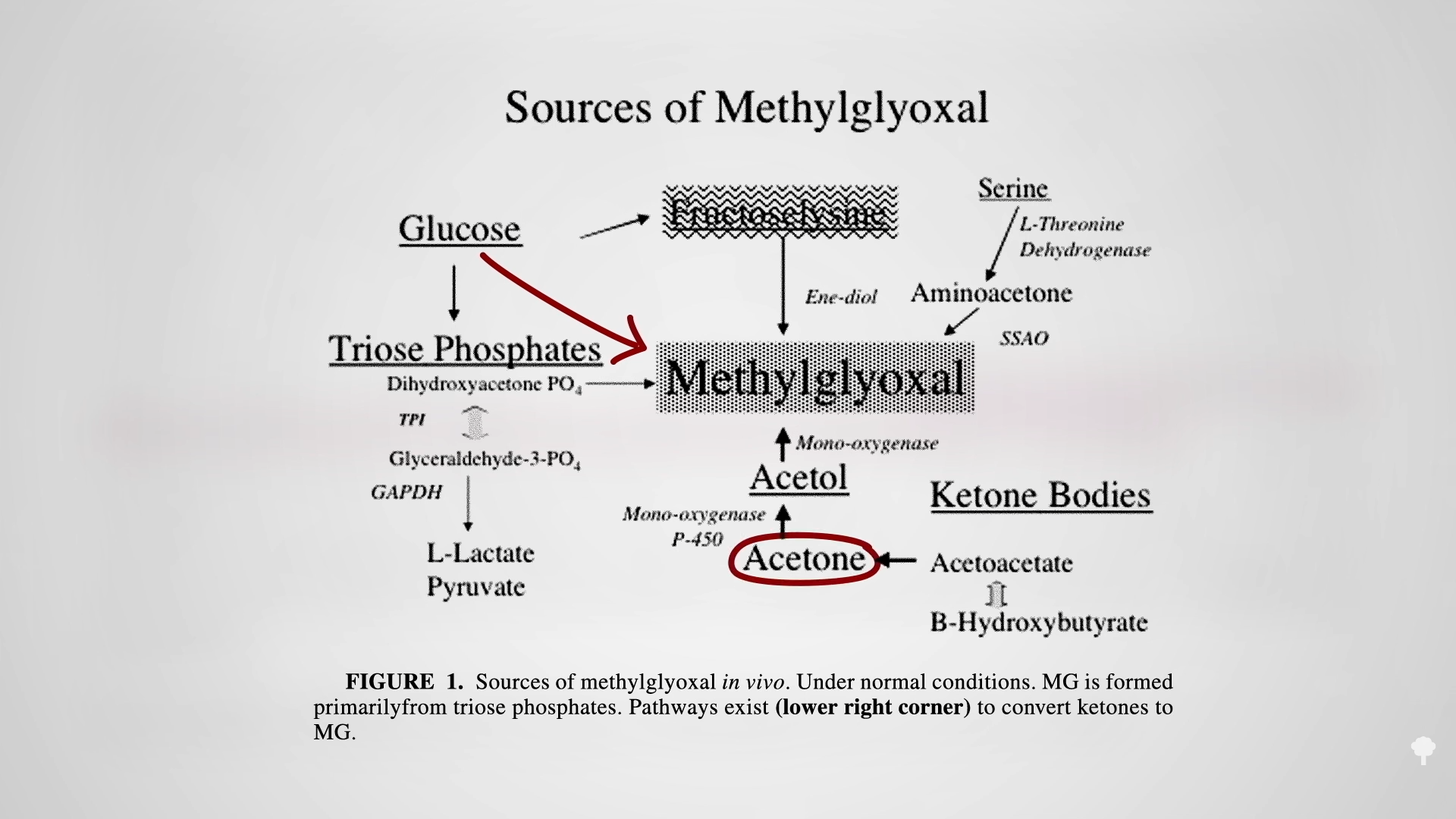
It turns out that high sugars may not be the only way to create this toxin, as you can see below and at 6:24 in my video. One of the ketones you make on a ketogenic diet is acetone (known for its starring role in nail polish remover). Acetone does more than just make keto dieters fail breathalyzer tests, “feel queasy and light-headed, and develop what’s been described as ‘rotten apple breath.’” Acetone can oxidize in the blood to form acetol, which may be a precursor for methylglyoxal.
That may be why keto dieters can end up with levels of this glycotoxin as high as those with out-of-control diabetes, which can cause the nerve damage and blood vessel damage you see in diabetics. That’s another way keto dieters can end up with a heart attack. The irony of treating diabetes with a ketogenic diet may extend beyond just making the underlying diabetes worse, but by mimicking some of the disease’s dire consequences.
This is part of a seven-video series on keto, which you can find in related videos below.
Plant-based diets are the single most important—yet underutilized—opportunity to reverse the pending obesity and diabetes-induced epidemic of disease and death.
Dr. Kim Williams, immediate past president of the American College of Cardiology, started out an editorial on plant-based diets with the classic Schopenhauer quote: “All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident.” In 2013, plant-based diets for diabetes were in the “ridiculed” stage in the official endocrinology practice guidelines and placed in the “Fad Diets” section. The guidelines acknowledged that strictly plant-based diets “have been shown to reduce the risk for T2DM [type 2 diabetes] and improve management of T2DM” better than the American Diabetes Association recommendations, then inexplicably went on to say that it “does not support the use of one type of diet over another” with respect to diabetes or in general. “The best approach for a healthy lifestyle is simply the ‘amelioration of unhealthy choices’”—whatever that means.
But, by 2015, the clinical practice guidelines from the same professional associations explicitly endorsed a plant-based diet as its general recommendation for diabetic patients. The times they are a-changin’!
As I discuss in my video Plant-Based Diets Recognized by Diabetes Associations, the American Diabetes Association itself is also now on board, listing plant-based eating as one of the dietary patterns acceptable for the management of the condition. The Canadian Diabetes Association, however, has really taken the lead. “Type 2 diabetes mellitus is considered one of the fastest growing diseases in Canada, representing a serious public health concern,” so it isn’t messing around and recommends plant-based diets for disease management “because of their potential to improve body weight and A1C [blood sugar control], LDL-cholesterol, total cholesterol and non-HDL-cholesterol levels, in addition to reducing the need for diabetes medications.” The Canadian Diabetes Association uses the Kaiser Permanente definition for that eating pattern: “a regimen that encourages whole, plant-based foods and discourages meats, dairy products and eggs, as well as all refined and processed foods,” that is, junk.
It recommends that diabetes education centers in Canada “improve patients’ perceptions of PBDs [plant-based diets] by developing PBD-focused educational and support as well as providing individualized counseling sessions addressing barriers to change.” The biggest obstacle identified to eating plant-based was ignorance. Nearly nine out of ten patients interviewed “had not heard of using a plant-based diet to treat or manage T2DM.” Why is that? “Patient awareness of (and interest in) the benefits of a plant-based diet for the management of diabetes…may be “influenced by the perception of diabetes educators and clinicians.” Indeed, most of the staff were aware of the benefits of plant-based eating for treating diabetes, yet only about one in three were recommending it to their patients.
Why? One of the common reasons given was they didn’t think their patients would eat plant-based, so they didn’t even bring it up, but “[t]his notion is contrary to the patient survey results that almost two-thirds of patients were willing” to at least give it a try. The researchers cite the PCRM Geico studies I’ve covered in other videos, in which strictly plant-based diets were “well accepted with over 95% adherence rate,” presumably because the study participants just felt so much better, reporting “increased energy level, better digestion, better sleep, and increased satisfaction when compared with the control group.”
A number of staff members also expressed they were unclear about the supportive scientific evidence as their second reason for not recommending this diet, but it’s been shown to be more effective than an American Diabetes Association–recommended diet at reducing the use of diabetes medications, long-term blood sugar control, and cholesterol. It’s therefore possible that the diabetes educators were simply behind the times, as there is “a lag-time” in the dissemination of new scientific findings from the literature to the clinician and finally to the patient. Speeding up this process is one of the reasons I started NutritionFacts.org.
As Dr. Williams put it, “the ‘truth’ (i.e., evidence) for the benefits of plant-based nutrition continues to mount. This now includes lower rates of stroke, hypertension, diabetes mellitus, obesity, myocardial infarction, and mortality [heart attacks and cardiac death], as well as many non-cardiac issues that affect our patients in cardiology, ranging from cancer to a variety of inflammatory conditions.” We’ve got the science. The bigger challenge is overcoming the “inertia, culture, habit, and widespread marketing of unhealthy foods.” He concludes, “Reading the existing literature and evaluating the impact of plant-based nutrition, it clearly represents the single most important yet underutilized opportunity to reverse the pending obesity and diabetes-induced epidemic of morbidity and mortality,” disease and death.
What there is instead is an acceptance among most Democratic leaders that they may still have to wait a while for Biden to make it official – and a grudging embrace of that.
To the confident advisers in the Biden orbit and their wider circle of supporters, the Kennedy challenge only serves to reinforce the president’s strength. Kennedy and spiritual author Marianne Williamson – mocked at a daily White House press briefing after her primary campaign launch – are the extent of the challenge Biden has drawn.
The Democratic National Committee has made very clear, meanwhile, that the party apparatus is aligned with Biden. No plans for primary debates are underway. A White House aide did not respond when asked for comment about Kennedy’s kick-off.
The furthest that New Hampshire Democratic Party Chairman Ray Buckley, who has been critical of Biden’s efforts to stop his state from holding its traditional first-in-the-nation primary, would go when asked about Kennedy’s candidacy was to say, “You just never know what catches the fancy of the voters.”
“I think the president’s done a fantastic job. The amount of accomplishments is simply breathtaking,” Buckley said. “I don’t see a singular issue galvanizing opposition to him.”
For at least a few hours on Wednesday, though, it looked like a real challenge. Like the bar across Boston Common that has the iconic “Cheers” sign but doesn’t actually look much like the set of the sitcom inside, Kennedy launch event at the Boston Park Plaza – with the “I’m a Kennedy Democrat” signs waving, the security with earpieces buzzing around – could, with a squint, look like any of the many campaigns from his famous family, including two against incumbent Democratic presidents, both of which ended with Republican wins.
What many attendees were there for, they said, was Kennedy-style truth telling. What many of them cheered most loudly for through his meandering speech – “this is what happens when you censor somebody for 18 years,” he joked with an hour left to go – were the oblique references to his Covid-19 vaccine skepticism. That skepticism has ostracized Kennedy from nearly every scientist, most Democratic leaders and many members of his family.
Kennedy acknowledged that distance from his family, previously reported by CNN, by naming those family members who did attend the event, as well as others he said had written him “beautiful letters of love” about his launch even though they are opposed to him running.
Inside the crowded ballroom on Wednesday, Kennedy told hundreds of supporters he knows he’s already being counted out.
That, he said, was part of the point, and what made him just like his father and namesake, whose 1968 primary campaign took on Lyndon Johnson.
“He was running against a president in his own party. He was running against a war. He was running at a time of unprecedented polarization in our country,” Kennedy said, calling his father getting into the 1968 race feeling like he had no chance to win.
“That hopelessness of his campaign,” Kennedy said, “freed him to tell the truth to the American people.”
Former Ohio Rep. Dennis Kucinich, a two-time presidential candidate from the left, compared Kennedy to Paul Revere in his own introduction of the candidate. Kennedy noted that he’d timed his campaign launch to the anniversary of that ride, even reciting a bit of the famous Henry Longfellow poem, which he noted his grandmother Rose had made all her 29 grandchildren memorize.
A new American Revolution is coming, he said, calling his campaign a mission to “end the corrupt merger of state and corporate power.”
But much of Kennedy’s speech returned to themes of how he had been trying to tell people what he thought was right, despite the government working against him – whether in his environmental work or when he called for an end to Covid-19 lockdowns.
As a corner of Twitter lit up with “Curb Your Enthusiasm” jokes following the introduction of his wife Cheryl Hines (a star in the show), Kennedy plowed through his concerns at length. There were mentions of the CIA. There were mentions of the butterflies he worried his grandchildren would never get to see because of environmental degradation and the songbirds they’d never get to hear. There was an extended critique of the American health care system, which he said has failed in not effectively treating chronic diseases. “If I have not significantly dropped the number of children with chronic disease by the end of my second term, I do not want to get reelected,” he said. There were questions about whether the war in Ukraine is in the national interest.
Kennedy knows he gets dismissed as a purveyor of misinformation, he said in his speech, but “a lot of the misinformation is just statements that depart from government orthodoxy.”
More than an hour into his speech, the crowd erupted as he spoke about the rise in autism diagnoses since 1989, arguing that he has never met someone his age with autism.
“Why aren’t we asking the question – what happened?” Kennedy asked.
Over two hours – including when a fire alarm briefly interrupted the speech – Kennedy never explicitly said the word “vaccine” once.
“He’s a truth teller,” said Rich Prunier, a native of Worcester, Massachusetts, who remembered meeting John F. Kennedy during his 1956 Senate campaign and attended Wednesday’s event.
Asked what he felt Robert F. Kennedy, Jr. tells the truth about, Prunier said, “name a subject.” His wife – wearing a matching “I’m a Kennedy Democrat” 2024 T-shirt – held up her copy of Kennedy’s book about “The Real Anthony Fauci.”
Prunier, who said he has received other vaccines but none of the Covid-19 shots, said he had voted for Vermont Sen. Bernie Sanders for the Democratic nomination in 2016 and 2020, but abstained in the 2020 general election because he didn’t like Biden or Donald Trump. He said he just peeled his Sanders bumper sticker off and will soon be replacing it with the Kennedy one he just picked up.
Elsewhere in the crowd, a small group posed for an iPhone photo while saying, “Freedom!”
Karen Huntley, a 60-year-old bookkeeper who’d come from Connecticut after reading about the launch from a well-known vaccine skeptic, said she wasn’t ready to commit but that Kennedy “sounds like a good candidate” because of his position on vaccines.
Huntley said she’d voted for Trump twice, but wouldn’t again – because of Operation Warp Speed, the Trump administration effort that helped accelerate development of the Covid-19 vaccine.
“I consider Trump the father of the vaccine,” she said.
His opposition to the vaccine, many leading Democrats say, disqualified Kennedy immediately.
“Being a vaccine denier and causing harm to public health is not progressive,” California Democratic Rep. Robert Garcia, one of the newest progressive leaders elected to Congress, told CNN. “The Democratic Party – and the progressive wing – will be solidly behind President Biden. There is no support or appetite for a challenger.”
Vaccine skepticism led Kennedy to a meeting at Trump Tower during the 2016 transition, after which he said the then-president-elect asked him to chair a commission on vaccines (the Trump transition later denied this, and the commission never came to be).
Asked back then what his father or late uncles Ted Kennedy or John F. Kennedy would think of Trump as president, Robert F. Kennedy said, “He’s probably come into office less encumbered by ideology or by obligations than anybody who’s won the presidency since Andrew Jackson. We’ll see what happens.”
By 2020, he said he had fully turned on Trump.
“He’s a bully, and I don’t like bullies, and that’s part of American tradition. I think in many ways he’s discredited the American experiment with self-governance,” Kennedy told Yahoo News three years ago.
While Kennedy says he’s running as a progressive, his first interview after declaring his candidacy was with Fox’s Tucker Carlson, in which he insisted that the American government is lying about the casualty rate in Ukraine.
Roger Stone, the longtime Trump adviser and proud dirty trickster, wrote up his own thoughts about a campaign he called “intriguing and potentially substantially impactful on the 2024 presidential race.”
“I believe that if he can pull together a minimally effective campaign, he could garner as much as a third of the Democrat primary vote,” Stone argued about Kennedy.
Stone predicted that Democratic Party leaders would try to block that from happening, but if he turns out to be wrong, “Given America’s state of peril, if RFK performs better than expected, the former President should consider the drafting of RFK as the Republican vice presidential candidate in a ‘bipartisan’ unity ticket.”
But though he and Kennedy were in a photo together backstage at an event last July, as part of the far-right Reawaken America tour, Stone said he has nothing to do with this campaign.
“We are acquaintances,” Stone told CNN about Kennedy. “I met him once. I have no idea who is running his campaign, and therefore no contact with them.”
In a long tweet last week, Kennedy denied speculation that has circulated in news reports that ties him to former Trump adviser Steve Bannon.
“Is it a sign of my campaign’s strength that the Elite of DC’s establishment media simultaneously and shamelessly published an orchestrated and baseless lie to smear me, even before I announce my presidential campaign?” Kennedy wrote. “Steve Bannon has nothing to do with my presidential campaign. I have never discussed a presidential run with Mr. Bannon.”
Charlie McCone has been struggling with the symptoms of long COVID since he was first infected, in March 2020. Most of the time, he is stuck on his couch or in his bed, unable to stand for more than 10 minutes without fatigue, shortness of breath, and other symptoms flaring up. But when I spoke with him on the phone, he seemed cogent and lively. “I can appear completely fine for two hours a day,” he said. No one sees him in the other 22. He can leave the house to go to medical appointments, but normally struggles to walk around the block. He can work at his computer for an hour a day. “It’s hell, but I have no choice,” he said. Like many long-haulers, McCone is duct-taping himself together to live a life—and few see the tape.
McCone knows 12 people in his pre-pandemic circles who now also have long COVID, most of whom confided in him only because “I’ve posted about this for three years, multiple times a week, on Instagram, and they’ve seen me as a resource,” he said. Some are unwilling to go public, because they fear the stigma and disbelief that have dogged long COVID. “People see very little benefit in talking about this condition publicly,” he told me. “They’ll try to hide it for as long as possible.”
I’ve heard similar sentiments from many of the dozens of long-haulers I’ve talked with, and the hundreds more I’ve heard from, since first reporting on long COVID in June 2020. Almost every aspect of long COVID serves to mask its reality from public view. Its bewilderingly diverse symptoms are hard to see and measure. At its worst, it can leave people bed- or housebound, disconnected from the world. And although milder cases allow patients to appear normal on some days, they extract their price later, in private. For these reasons, many people don’t realize just how sick millions of Americans are—and the invisibility created by long COVID’s symptoms is being quickly compounded by our attitude toward them.
Most Americans simply aren’t thinking about COVID with the same acuity they once did; the White House long ago zeroed in on hospitalizations and deaths as the measures to worry most about. And what was once outright denial of long COVID’s existence has morphed into something subtler: a creeping conviction, seeded by academics and journalists and now common on social media, that long COVID is less common and severe than it has been portrayed—a tragedy for a small group of very sick people, but not a cause for societal concern. This line of thinking points to the absence of disability claims, the inconsistency of biochemical signatures, and the relatively small proportion of severe cases as evidence that long COVID has been overblown. “There’s a shift from ‘Is it real?’ to ‘It is real, but …,’” Lekshmi Santhosh, the medical director of a long-COVID clinic at UC San Francisco, told me.
Yet long COVID is a substantial and ongoing crisis—one that affects millions of people. However inconvenient that fact might be to the current “mission accomplished” rhetoric, the accumulated evidence, alongside the experience of long haulers, makes it clear that the coronavirus is still exacting a heavy societal toll.
As it stands, 11 percent of adults who’ve had COVID are currently experiencing symptoms that have lasted for at least three months, according to data collected by the Census Bureau and the CDC through the national Household Pulse Survey. That equates to more than 15 million long-haulers, or 6 percent of the U.S. adult population. And yet, “I run into people daily who say, ‘I don’t know anyone with long COVID,’” says Priya Duggal, an epidemiologist and a co-lead of the Johns Hopkins COVID Long Study. The implication is that the large survey numbers cannot be correct; given how many people have had COVID, we’d surely know if one in 10 of our contacts was persistently unwell.
But many factors make that unlikely. Information about COVID’s acute symptoms was plastered across our public spaces, but there was never an equivalent emphasis that even mild infections can lead to lasting and mercurial symptoms; as such, some people who have long COVID don’t even know what they have. This may be especially true for the low-income, rural, and minority groups that have borne the greatest risks of infection. Lisa McCorkell, a long-hauler who is part of the Patient-Led Research Collaborative, recently attended a virtual meeting of Bay Area community leaders, and “when I described what it is, some people in the chat said, ‘I just realized I might have it.’”
Admitting that you could have a life-altering and long-lasting condition, even to yourself, involves a seismic shift in identity, which some people are understandably loath to make. “Everyone I know got Omicron and got over it, so I really didn’t want to concede that I didn’t survive this successfully,” Jennifer Senior, a friend and fellow staff writer at The Atlantic, who has written about her experience with long COVID, told me. Duggal mentioned an acquaintance who, after a COVID reinfection, can no longer walk the quarter mile to pick her kids up from school, or cook them dinner. But she has turned down Duggal’s offer of an appointment; instead, she is moving across the country for a fresh start. “That is common: I won’t call it ‘long COVID’; I’ll just change everything in my life,” Duggal told me. People who accept the condition privately may still be silent about it publicly. “Disability is often a secret we keep,” Laura Mauldin, a sociologist who studies disability, told me. One in four Americans has a disability; one in 10 has diabetes; two in five have at least two chronic diseases. In a society where health issues are treated with intense privacy, these prevalence statistics, like the one-in-10 figure for long COVID, might also intuitively feel like overestimates.
Some long-haulers are scared to disclose their condition. They might feel ashamed for still being sick, or wary about hearing from yet another loved one or medical professional that there’s nothing wrong with them. Many long-haulers worry that they’ll be perceived as weak or needy, that their friends will stop seeing them, or that employers will treat them unfairly. Such fears are well founded: A British survey of almost 1,000 long-haulers found that 63 percent experienced overt discrimination because of their illness at least “sometimes,” and 34 percent sometimes regretted telling people that they have long COVID. “So many people in my life have reached out and said, ‘I’m experiencing this,’ but they’re not telling the rest of our friends,” McCorkell said.
Imagine that you interact with 50 people on a regular basis, all of whom got COVID. If 10 percent are long-haulers, that’s five people who are persistently sick. Some might not know what long COVID is or might be unwilling to confront it. The others might have every reason to hide their story. “Numbers like 10 percent are not going to naturally present themselves in front of you,” McCone told me. Instead, “you’ll hear from 45 people that they are completely fine.”
Illustration by Paul Spella / The Atlantic; Getty
The same factors that stop people from being public about their condition—ignorance, denial, or concerns about stigma—also make them less likely to file for disability benefits. And that process is, to put it mildly, not easy. Applicants need thorough medical documentation; many long-haulers struggle to find doctors who believe their symptoms are real. Even with the right documents, applicants must hack their way through bureaucratic overgrowth, likely while fighting fatigue or brain fog. For these reasons, attempting to measure long COVID through disability claims is a profoundly flawed exercise. Even if people manage to apply, they face an average wait time of seven months and a two-in-three denial rate. McCone took six weeks to put an application together, and, despite having a lawyer and extensive medical documentation, was denied after one day. McCorkell knows many first-wavers—people who’ve had long COVID since March 2020—“who are just getting their approvals now.”
An alternative source of data comes from the Census Bureau’s Current Population Survey, which simply asks working-age Americans if they have any of six forms of disability. Using that data, Richard Deitz, an economics-research adviser at the Federal Reserve Bank of New York, calculated that about 1.7 million more people now say they do than in mid-2020, reversing a years-long decline. These numbers are lower than expected if one in 10 people who gets COVID really does become a long-hauler, but the survey doesn’t directly capture many of the condition’s most common symptoms, such as fatigue, neurological problems beyond brain fog, and post-exertional malaise, where a patient’s symptoms get dramatically worse after physical or mental exertion. About 900,000 of the newly disabled people are also still working. David Putrino, who leads a long-COVID rehabilitation clinic at Mount Sinai, told me that many of his patients are refused the accommodations required under the Americans With Disabilities Act. Their employers won’t allow them to work remotely or reduce their hours, because, he said, “you look at them and don’t see an obvious disability.”
Long COVID can also seem bafflingly invisible when people look at it with the wrong tools. For example, a 2022 study by National Institutes of Health researchers compared 104 long-haulers with 85 short-term COVID patients and 120 healthy people and found no differences in measures of heart or lung capacities, cognitive tests, or levels of common biomarkers—bloodstream chemicals that might indicate health problems. This study has been repeatedly used as evidence that long COVID might be fictitious or psychosomatic, but in an accompanying editorial, Aluko Hope, the medical director of Oregon Health and Science University’s long-COVID program, noted that the study exactly mirrors what long-haulers commonly experience: They undergo extensive testing that turns up little and are told, “Everything is normal and nothing is wrong.”
The better explanation, Putrino told me, is that “cookie-cutter testing” doesn’t work—a problem that long COVID shares with other neglected complex illnesses, such as myalgic encephalomyelitis/chronic-fatigue syndrome and dysautonomia. For example, the NIH study didn’t consider post-exertional malaise, a cardinal symptom of both ME/CFS and long COVID; measuring it requires performing cardiopulmonary tests on two successive days. Most long-haulers also show spiking heart rates when asked to simply stand against a wall for 10 minutes—a sign of problems with their autonomic nervous system. “These things are there if you know where to look,” Putrino told me. “You need to listen to your patients, hear where the virus is affecting them, and test accordingly.”
Contrary to popular belief, researchers have learned a huge amount about the biochemical basis of long COVID, and have identified several potential biomarkers for the disease. But because long COVID is likely a cluster of overlapping conditions, there might never be a singular blood test that “will tell you if you have long COVID 100 percent of the time,” Putrino said. The best way to grasp the scale of the condition, then, is still to ask people about their symptoms.
Large attempts to do this have been relatively consistent in their findings: The U.S. Household Pulse Survey estimates that one in 10 people who’ve had COVID currently have long COVID; a large Dutch study put that figure at one in eight. The former study also estimated that 6 percent of American adults are long-haulers; a similar British survey by the Office for National Statistics estimated that 3 percent of the general population is. These cases vary widely in severity, and about one in five long-haulers is barely affected by their symptoms—but the remaining majority very much is. Another one in four long-haulers (or 4 million Americans) has symptoms that severely limit their daily activities. The others might, at best, wake every day feeling as if they haven’t had any rest, or feel trapped in an endless hangover. They might work or socialize when their tidal symptoms ebb, but only by making big compromises: “If I work a full day, I can’t also then make dinner or parent without significant suffering,” JD Davids, who has both long COVID and ME/CFS, told me.
Some people do recover. A widely cited Israeli study of 1.9 million people used electronic medical records to show that most lingering COVID symptoms “are resolved within a year from diagnosis,” but such data fail to capture the many long-haulers who give up on the medical system precisely because they aren’t getting better or are done with being disbelieved. Other studies that track groups of long-haulers over time have found less rosy results. A French one found that 85 percent of people who had symptoms two months after their infection were still symptomatic after a year. A Scottish team found that 42 percent of its patients had only partially recovered at 18 months, and 6 percent had not recovered at all. The United Kingdom’s national survey shows that 69 percent of people with long COVID have been dealing with symptoms for at least a year, and 41 percent for at least two.
The most recent data from the U.S. and the U.K. show that the total number of long-haulers has decreased over the past six months, which certainly suggests that people recover in appreciable numbers. But there’s a catch: In the U.K., the number of people who have been sick for more than a year, or who are severely limited by their illness, has gone up. A persistent pool of people is still being pummeled by symptoms—and new long-haulers are still joining the pool. This influx should be slower than ever, because Omicron variantsseem tocarry alower risk of triggering long COVID, while vaccines and the drug Paxlovid can lower that risk even further. But though the odds against getting long COVID are now better, more people are taking a gamble, because preventive precautions have been all but abandoned.
Even if prevalence estimates were a tenth as big, that would still mean more than 1 million Americans are dealing with a chronic illness that they didn’t have three years ago. “When long COVID first came on the scene, everyone told us that once we have the prevalence numbers, we can do something about it,” McCorkell told me. “We got those numbers. Now people say, ‘Well, we don’t believe them. Try again.’”
To a degree, I sympathize with some of the skepticism regarding long COVID, because the condition challenges our typical sense of what counts as solid evidence. Blood tests, electronic medical records, and disability claims all feel like rigorous lines of objective data. Their limitations become obvious only when you consider what the average long-hauler goes through—and those details are often cast aside because they are “anecdotal” and, by implication, unreliable. This attitude is backwards: The patients’ stories are the ground truth against which all other data must be understood. Gaps between the data and the stories don’t immediately invalidate the latter; they just as likely show the holes in the former.
Laura Mauldin, the disability sociologist, argues that the U.S. is primed to discount those experiences because the country’s values—exceptionalism, strength, self-reliance—have created what she calls the myth of the able-bodied public. “We cannot accept that our bodies are fallible, or that disability is utterly ordinary and expected,” she told me. “We go to great pains to pretend as though that is not the case.” If we believe that a disabling illness like long COVID is rare or mild, “we protect ourselves from having to look at it.” And looking away is that much easier because chronic illnesses like long COVID are more likely to affect women—“who are more likely to have their symptoms attributed to psychological problems,” Mauldin said—and because the American emphasis on work ethic devalues people who can’t work as much or as hard as their peers.
Other aspects of long COVID make it hard to grasp. Like other similar, neglected chronic illnesses, it defies a simplistic model of infectious disease in which a pathogen causes a predictable set of easily defined symptoms that alleviate when the bug is destroyed. It challenges our belief in our institutions, because truly contending with what long-haulers go through means acknowledging how poorly the health-care system treats chronically ill patients, how inaccessible social support is to them, and how many callous indignities they suffer at the hands of even those closest to them. Long COVID is a mirror on our society, and the image it reflects is deeply unflattering.
Most of all, long COVID is a huge impediment to the normalization of COVID. It’s an insistent indicator that the pandemic is not actually over; that policies allowing the coronavirus to spread freely still carry a cost; that improvements such as better indoor ventilation are still wanting; that the public emergency may have been lifted but an emergency still exists; and that millions cannot return to pre-pandemic life. “Everyone wants to say goodbye to COVID,” Duggal told me, “and if long COVID keeps existing and people keep talking about it, COVID doesn’t go away.” The people who still live with COVID are being ignored so that everyone else can live with ignoring it.
This article originally misstated the name of the bank where Richard Deitz works.
Editor’s Note: Sign up for CNN’s Eat, But Better: Mediterranean Style. Our eight-part guide shows you a delicious expert-backed eating lifestyle that will boost your health for life.
CNN
—
Gobbling up too many refined wheat and rice products, along with eating too few whole grains, is fueling the growth of new cases of type 2 diabetes worldwide, according to a new study that modelsdata through 2018.
“Our study suggests poor carbohydrate quality is a leading driver of diet-attributable type 2 diabetes globally,” says senior author Dr. Dariush Mozaffarian, a professor of nutrition at Tufts University and professor of medicine at Tufts School of Medicine in Boston, in a statement.
Another key factor: People are eating far too much red and processed meats, such as bacon, sausage, salami and the like, the study said. Those three factors — eating too few whole grains and too many processed grains and meats — were the primary drivers of over 14 million new cases of type 2 diabetes in 2018, according to the study, which was published Monday in the journal Nature Medicine.
In fact, the study estimated 7 out of 10 cases of type 2 diabetes worldwide in 2018 were linked to poor food choices.
“These new findings reveal critical areas for national and global focus to improve nutrition and reduce devastating burdens of diabetes,” said Mozaffarian, who is also the editor in chief of the Tufts Health & Nutrition Letter.
Mozaffarian and his team developed a research model of dietary intake between 1990 and 2018 and applied it to 184 countries. Compared with 1990, there were 8.6 million more cases of type 2 diabetes due to poor diet in 2018, the study found.
Researchers found eating too many unhealthy foods was more of a driver of type 2 diabetes on a global level than a lack of eatingwholesome foods, especially for men compared with women, younger compared to older adults, and in urban versus rural residents.
Over 60% of the total global diet-attributable cases of the disease were due to excess intake of just six harmful dietary habits: eating too much refined rice, wheat and potatoes; too many processed and unprocessed red meats; and drinking too many sugar-sweetened beverages and fruit juice.
Inadequate intake of five protective dietary factors — fruits, nonstarchy vegetables, nuts, seeds, whole grains and yogurt — was responsible for just over 39% of the new cases.
People in Poland and Russia, where diets tend to focus on potatoes and red and processed meat, and other countries in Eastern and Central Europe as well as Central Asia, had the highest percentage of new type 2 diabetes cases linked to diet.
Colombia, Mexico and other countries in Latin America and the Caribbean also had high numbers of new cases, which researchers said could be due to a reliance on sugary drinks and processed meat, as well as a low intake of whole grains.
“Our modeling approach does not prove causation, and our findings should be considered as estimates of risk,” the authors wrote.
The US National Institute on Aging is moving forward with efforts to build a real-world Alzheimer’s disease database as part of its aim to improve, support and conduct more dementia research.
Last month, the agency, part of the National Institutes of Health, posted a notice of the grant for the six-year database project, setting its earliest start date as April 2024.
The NIH confirmed Tuesday that plans are underway to fund the Alzheimer’s disease and Alzheimer’s disease-related dementias’ real-world data platform.
The National Institute on Aging intends to commit $50 million per year, starting in fiscal year 2024, to fund one award.
The nonprofit Alzheimer’s Association is among those planning to apply for the grant.
“The newly-announced NIA funding for a large-scale Alzheimer’s disease research database is truly exciting and a very important step forward for our field, and the Alzheimer’s Association will apply for that grant,” Maria C. Carrillo, Alzheimer’s Association chief science officer, said in an email Tuesday.
“The Association is already leading ALZ-NET, which is a national network of physicians that is collecting data – including measures of cognition, function and safety – for patients treated with new FDA-approved Alzheimer’s treatments,” Carrillo said. “The NIA funding could expand ALZ-NET’s scope to the benefit of all stakeholders.”
She added that the Alzheimer’s Association believes everyone should have access to treatments, regardless of their registration status.
The real-world database “aims to transform” the Alzheimer’s disease research enterprise “by serving as a central hub of research access,” the National Institute on Aging said last week in its announcement of a webinar about the project that’s scheduled for April 19.
According to the announcement, the aim of the data registry is to provide a comprehensive and diverse database that can “improve applicability and generalizability of findings,” be used as a tool for researchers and allow scientific questions to be answered more quickly.
Last year, the National Institute on Aging convened an exploratory workshop to discuss gaps in real-world data and opportunities to expand real-world data sources for dementia research.
More than 6 million Americans are living with dementia caused by Alzheimer’s disease, according to the Alzheimer’s Association, and the number of people affected is projected to double in the next two decades, rising to 13 million in 2050.
Researchers in New York developed a virtual reality maze for mice in an attempt to demystify a question that’s been plaguing neuroscientists for decades: How are long-term memories stored?
What they found surprised them. After forming in the hippocampus, a curved structure that lies deep within the brain, the mice’s memories were actually rooted through what’s called the anterior thalamus, an area of the brain that scientists haven’t typically associated with memory processing at all.
“The thalamus being a clear winner here was very interesting for us, and unexpected,” said Priya Rajasethupathy, an associate professor at Rockefeller University and one of the coauthors of a peer-reviewed study published in the journal Cell this week. The thalamus “has often been thought of as a sensory relay, not very cognitive, not very important in memory.”
This new research, however, indicates that it could play a vital role in converting short-term memories to long-term memories. And Rajasethupathy said that should make the thalamus a key area of study for researchers attempting to help patients who suffer from conditions such as Alzheimer’s, who are able to recall old memories but may have trouble remembering new information.
“it implicates a part of the brain — the thalamus — in the long-term storage of memories in a way that wasn’t even hypothesized by anyone else,” said Loren Frank, a professor of physiology at the University of California San Francisco, who was not involved in the study.
Rajasethupathy noted that neuroscientists have long known that memories take shape in the hippocampus, and is the focus of the vast majority of research around conditions like amnesia and Alzheimer’s.
Past research has “led to this model where memories are formed in the hippocampus but then become independent over time and slowly stabilized in the cortex,” the wrinkled, outermost portion of the brain. The question has been exactly how memories travel from one area to another, Rajasethupathy said.
“That process has been mysterious, I would say, for more than 50 years,” Rajasethupathy said.
It was the right time for her lab to attempt to pinpoint an answer, she added, thanks to new technology that allowed the researchers to track activity in multiple parts of each subject’s brain. The innovations enabled the team to trace how memories are traveling as the mice learned to navigate a maze.
“I think what they did was technically very challenging,” Frank said. “Particularly where they were trying to (observe) activity from multiple neurons in three different areas at once, using this sort of fiber microscopes. That’s a pretty state of the art thing.”
The study — led by Rockefeller graduate students Andrew Toader and Josue Regalado, working inside Rajasethupathy’s lab — involved strapping the mice into a headpiece designed to hold them steady while a machine used optical fibers to record their brain activity.
The maze took them into various “rooms” that offered either incentives, such as sugar water, or deterrents, like a puff of air to the face.
The mice returned to the maze for days, enough time for them to create long-term memories.
“The analogy would be your birthday dinner versus the dinner you had three Tuesdays ago,” Toader said in a statement. “You’re more likely to remember what you had on your birthday because it’s more rewarding for you—all your friends are there, it’s exciting—versus just a typical dinner, which you might remember the next day but probably not a month later.”
Meanwhile, the researchers used chemicals to inhibit parts of the mice’s brains to determine how it affected their ability to create and store memories.
Not only did they find that the anterior thalamus was a crucial waypoint for these memories — they also found that by stimulating that area in the rodents’ brains, the researchers were “able to help mice retain memories that they would usually forget,” according to a news release about the study.
Rajasethupathy added, “Some memories are more important to us than others. We found that, not only do mice need the anterior thalamus to consolidate memories, but that by activating it, we could enhance consolidation of a memory that mice would usually forget.”
Rajasethupathy noted that there were some limitations to the study. It does not, for example, indicate that traveling through the anterior thalamus is the only route memories can take on their way to long-term storage.
“I want to beclear that this is not the end all be all,” she said. “Maybe everything isn’t consolidated through this pathway. But I’m very confident this is one very important circuit.”
This study also relied on mice, who don’t have identical brains to humans but have proven to be extremely useful models for discovering how our own brains function. The long-term memory storage process takes weeks in rodents, whereas it can take months for humans, Rajasethupathy added.
It’s also possible that different types of memory take different highways, she noted. There are explicit memories, which focus on facts, figures and specific data points, and implicit memories are typically tied to emotion and can form without a person realizing it. The thalamus may not be involved in the same manner for both types of information.
But Frank, the UCSF professor, said the study will have broad implications for future research, spurring more investigations into the thalamus’ role in memory storage.
“It’s nice for the field to getting to the point where we can think about the long-term evolution of memories and really try to understand how that works,” he said. “And the study is definitely a step in that direction.”
Advisers to the World Health Organization will consider next month whether to add liraglutide, the active ingredient in certain diabetes and obesity medications, to its list of essential medicines.
The list, which is updated every two years, includes medicines “that satisfy the priority health needs of the population,” WHO says. “They are intended to be available within the context of function health systems at all times, in adequate amounts in the appropriate dosage forms, of assured quality and at prices that individuals and the community can afford.”
The list is “a guide for the development and updating of national and institutional essential medicine lists to support the procurement and supply of medicines in the public sector, medicines reimbursement schemes, medicine donations, and local medicine production.”
The WHO Expert Committee on the Selection and Use of Essential Medicines is scheduled to meet April 24-28 to discuss revisions and updates involving dozens of medications. The request to add GLP-1 receptor agonists such as liraglutide came from four researchers at US institutions including Yale University and Brigham and Women’s Hospital.
These drugs mimic the effects of an appetite-regulating hormone, GLP-1, and stimulate the release of insulin. This helps lower blood sugar and slows the passage of food through the gut. Liraglutide was developed to treat diabetes but approved in the US as a weight-loss treatment in 2014; its more potent cousin, semaglutide, has been approved for diabetes since 2017 and as an obesity treatment in 2021.
The latter use has become well-known thanks to promotions from celebrities and on social media. It’s sold under the name Ozempic for diabetes and Wegovy for weight loss. Studies suggest that semaglutide may help people lose an average of 10% to 15% of their starting weight – significantly more than with other medications. But because of this high demand, some versions of the medication have been in shortage in the US since the middle of last year.
The US patent on liraglutide is set to expire this year, and drugmaker Novo Nordisk says generic versions could be available in June 2024.
The company has not been involved in the application to WHO, it said in a statement, but “we welcome the WHO review and look forward to the readout and decision.”
“At present, there are no medications included in the [Essential Medicines List] that specifically target weight loss for the global burden of obesity,” the researchers wrote in their request to WHO. “At this time, the EML includes mineral supplements for nutritional deficiencies yet it is also described that most of the population live in ‘countries where overweight and obesity kills more people than underweight.’ “
WHO’s advisers will make recommendations on which drugs should be included in this year’s list, expected to come in September.
“This particular drug has a certain history, but the use of it probably has not been long enough to be able to see it on the Essential Medicines List,” Dr. Francesco Blanca, WHO director for nutrition and food safety, said at a briefing Wednesday. “There’s also issues related to the cost of the treatment. At the same time, WHO is looking at the use of drugs to reduce weight excess in the context of a systematic review for guidelines for children and adolescents. So we believe that it is a work in progress, but we’ll see what the Essential Medicines List committee is going to conclude.”
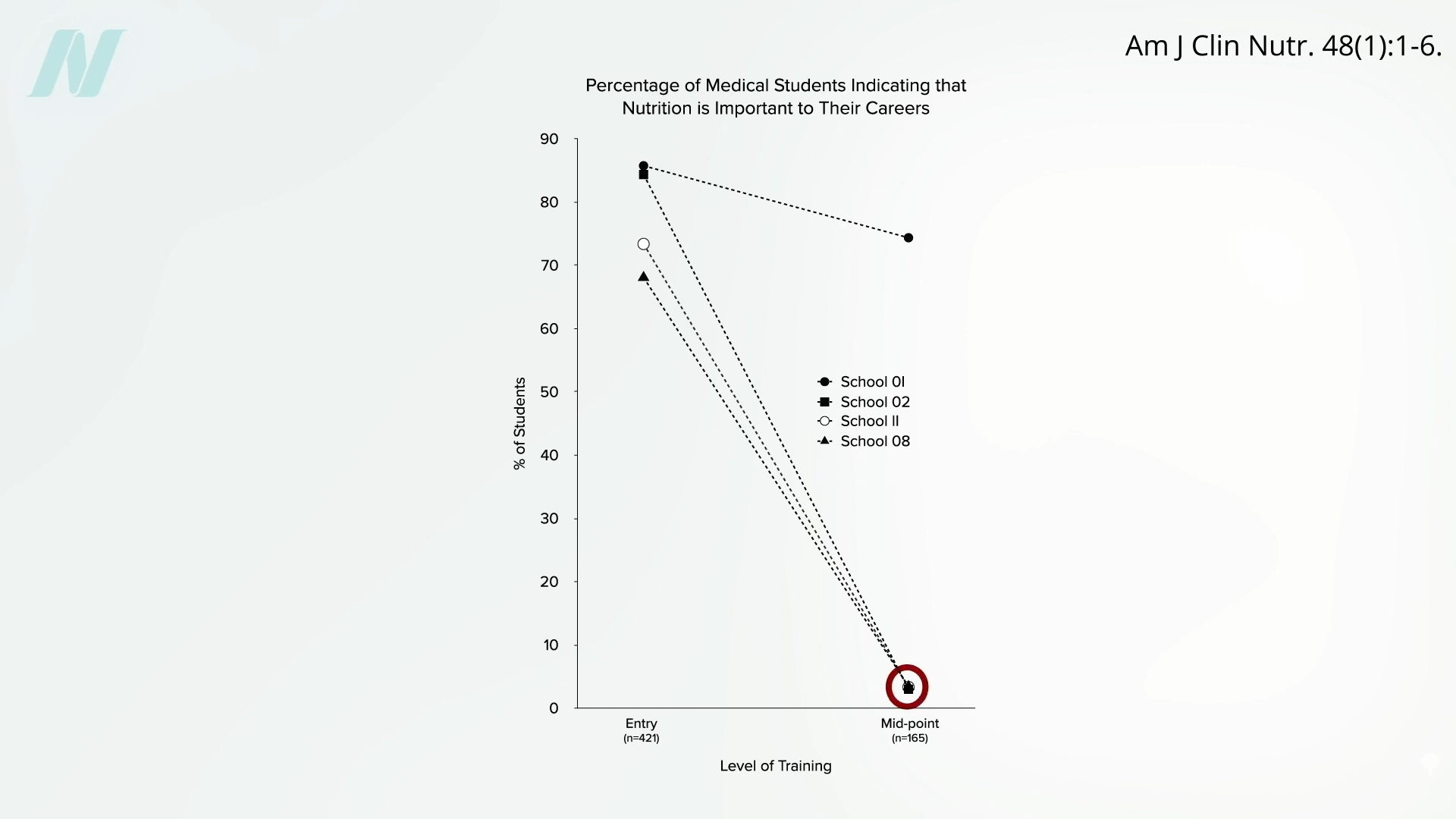
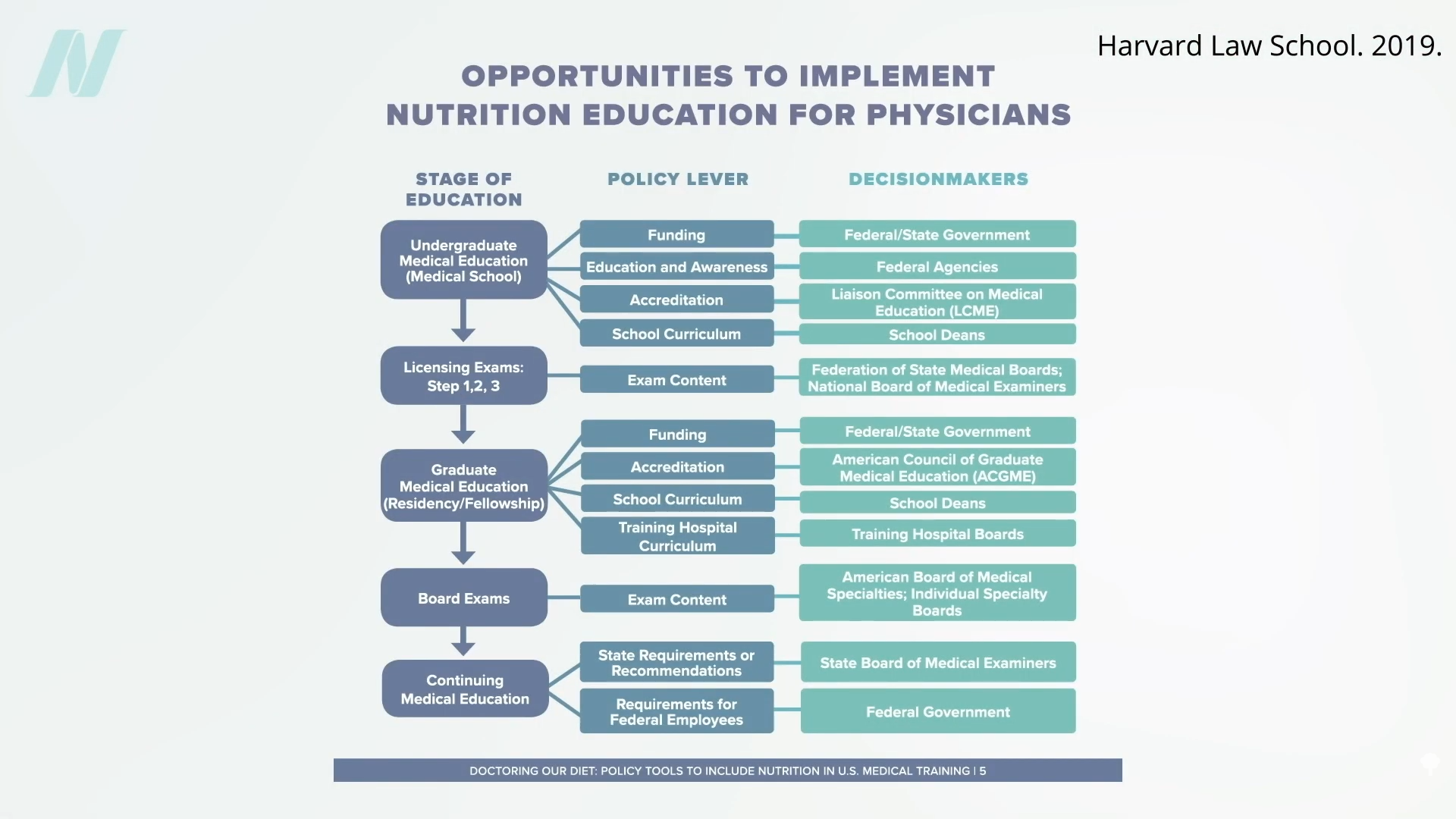
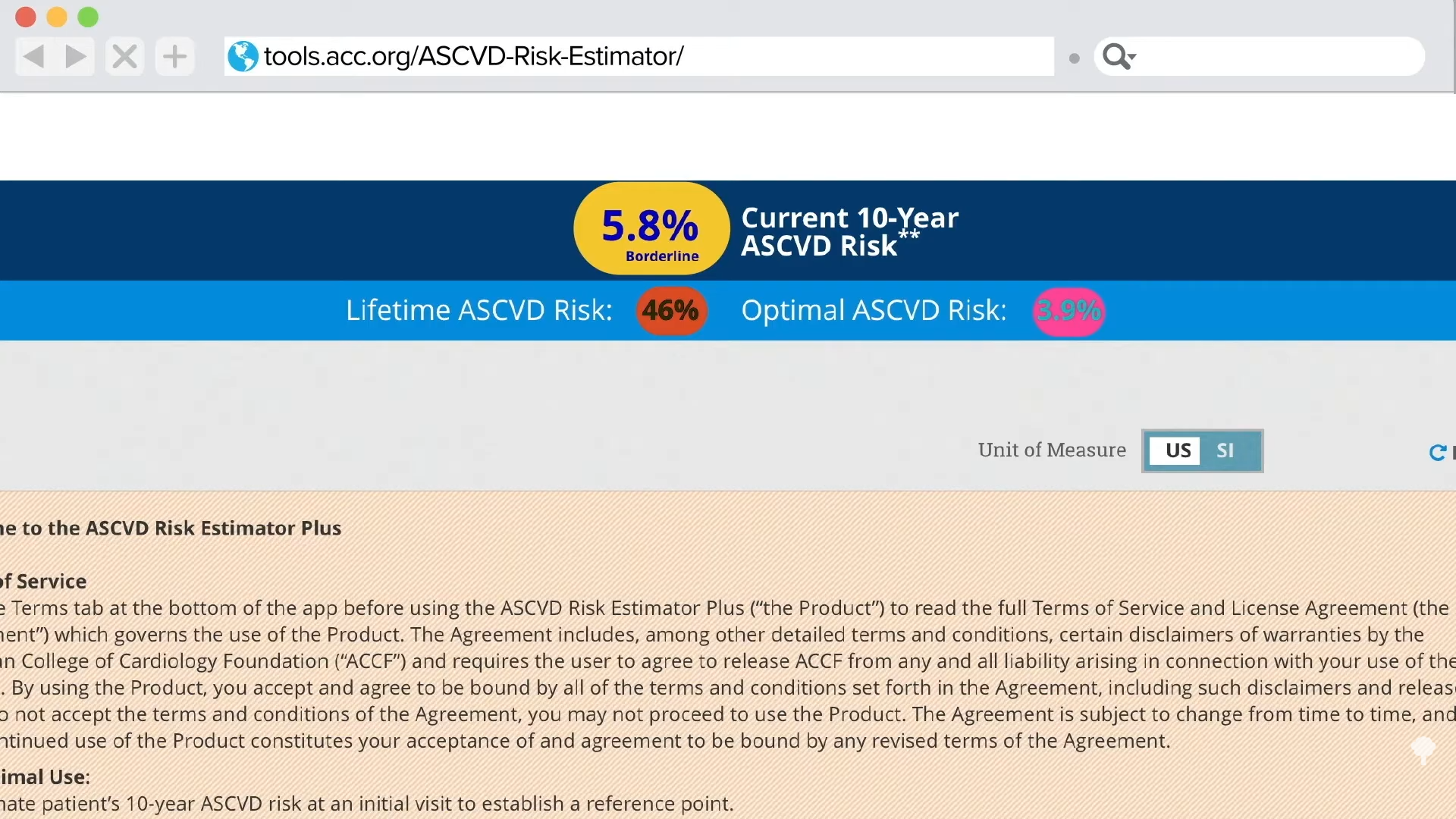
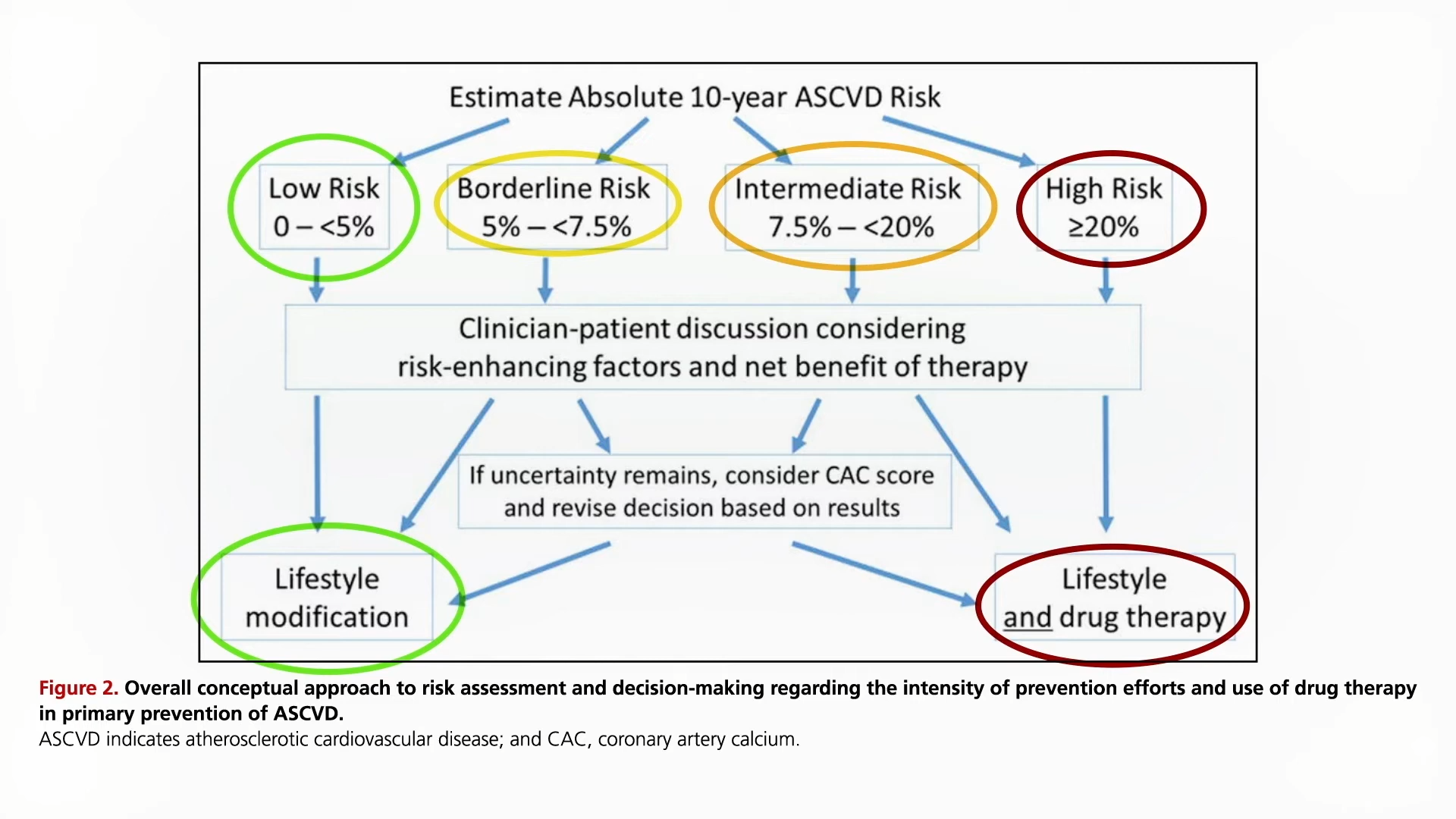
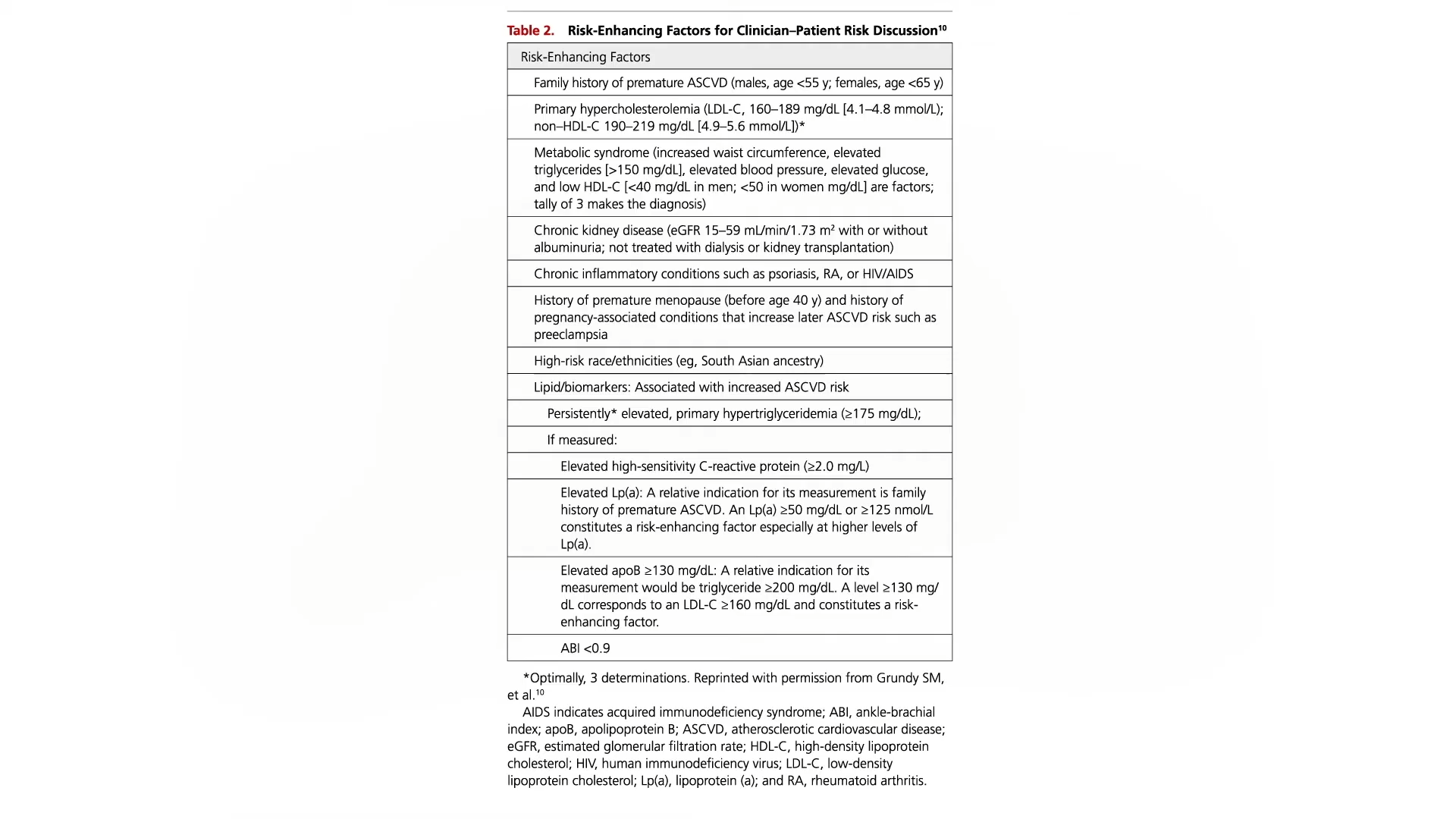
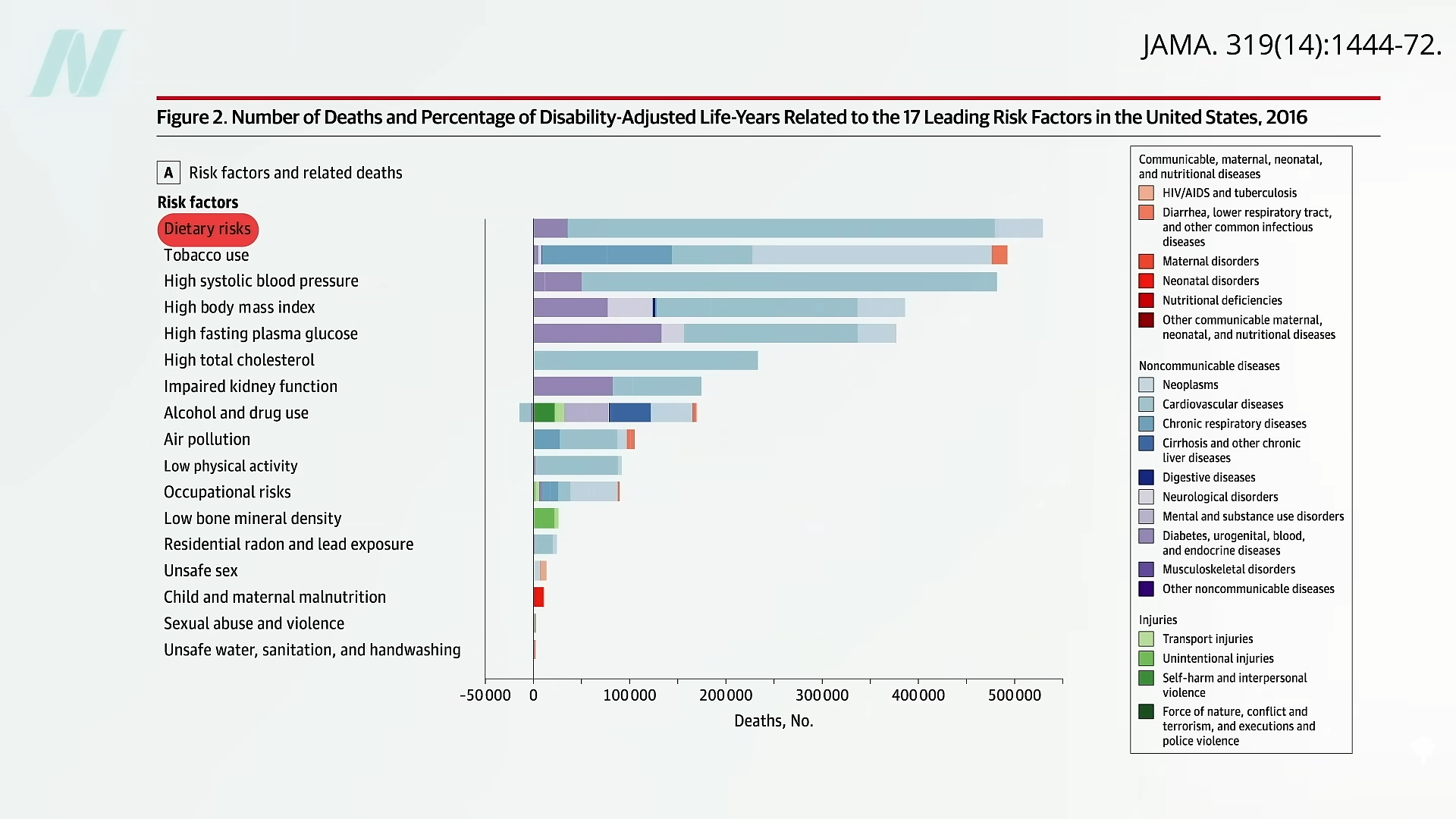
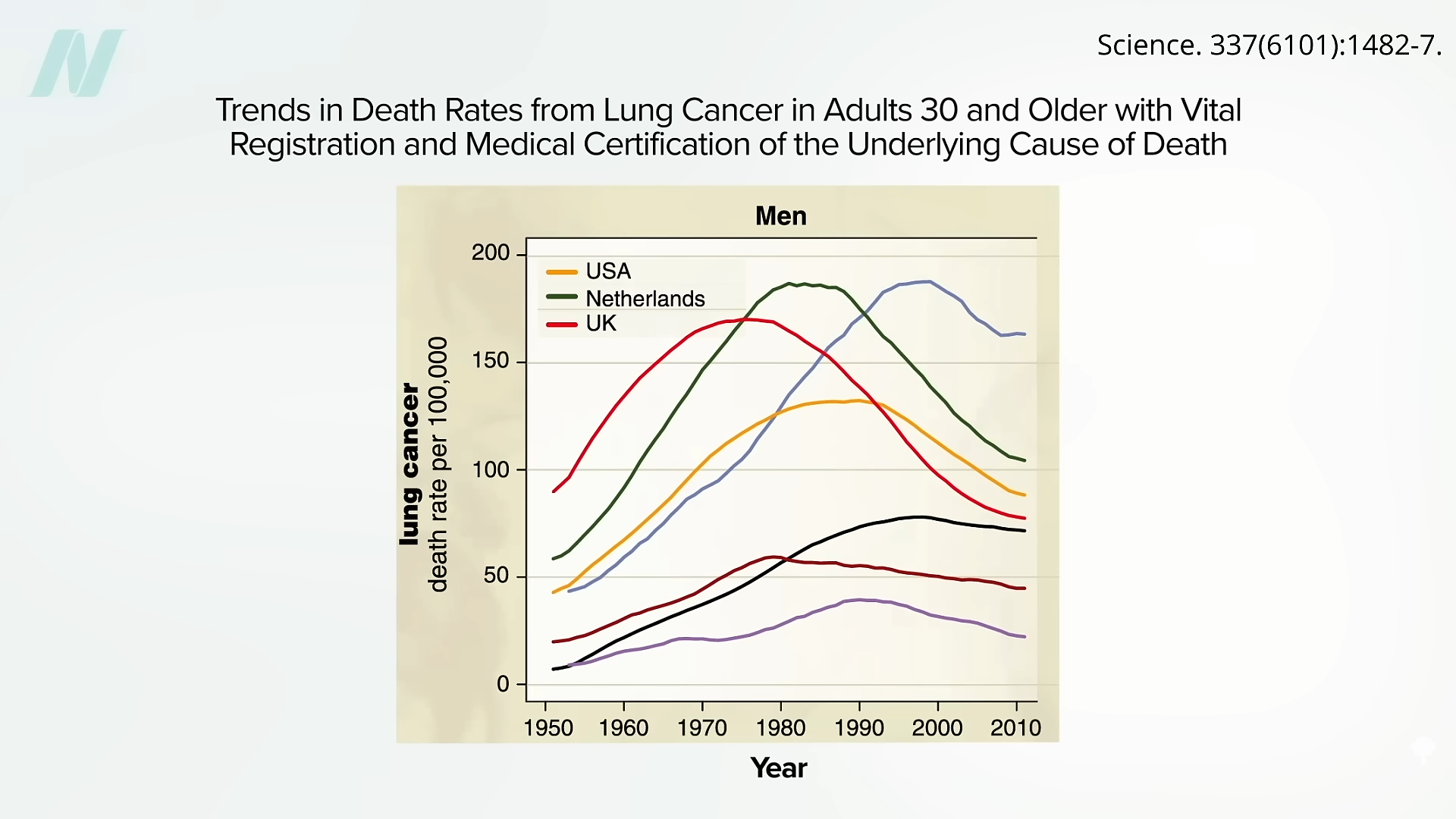

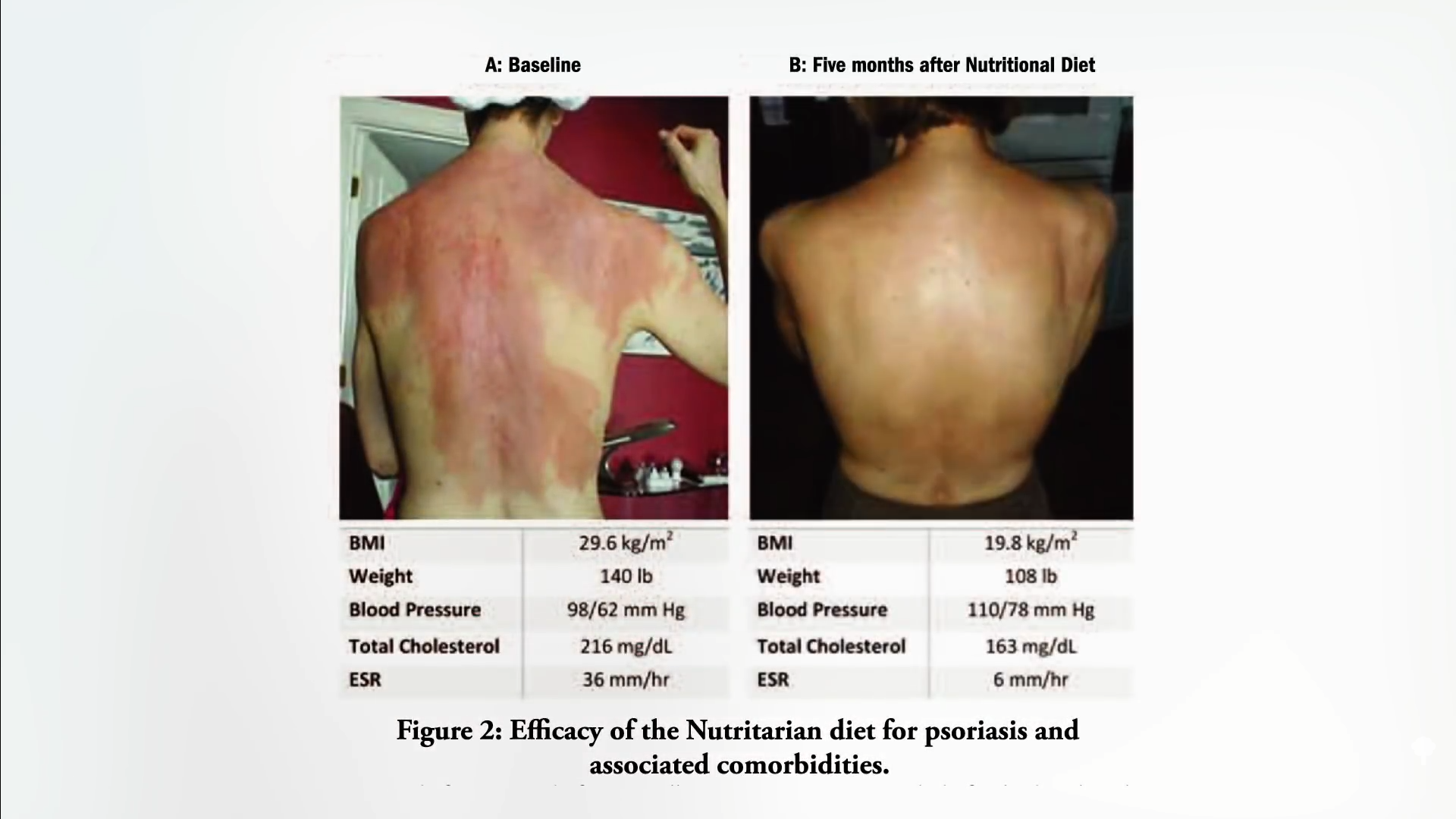

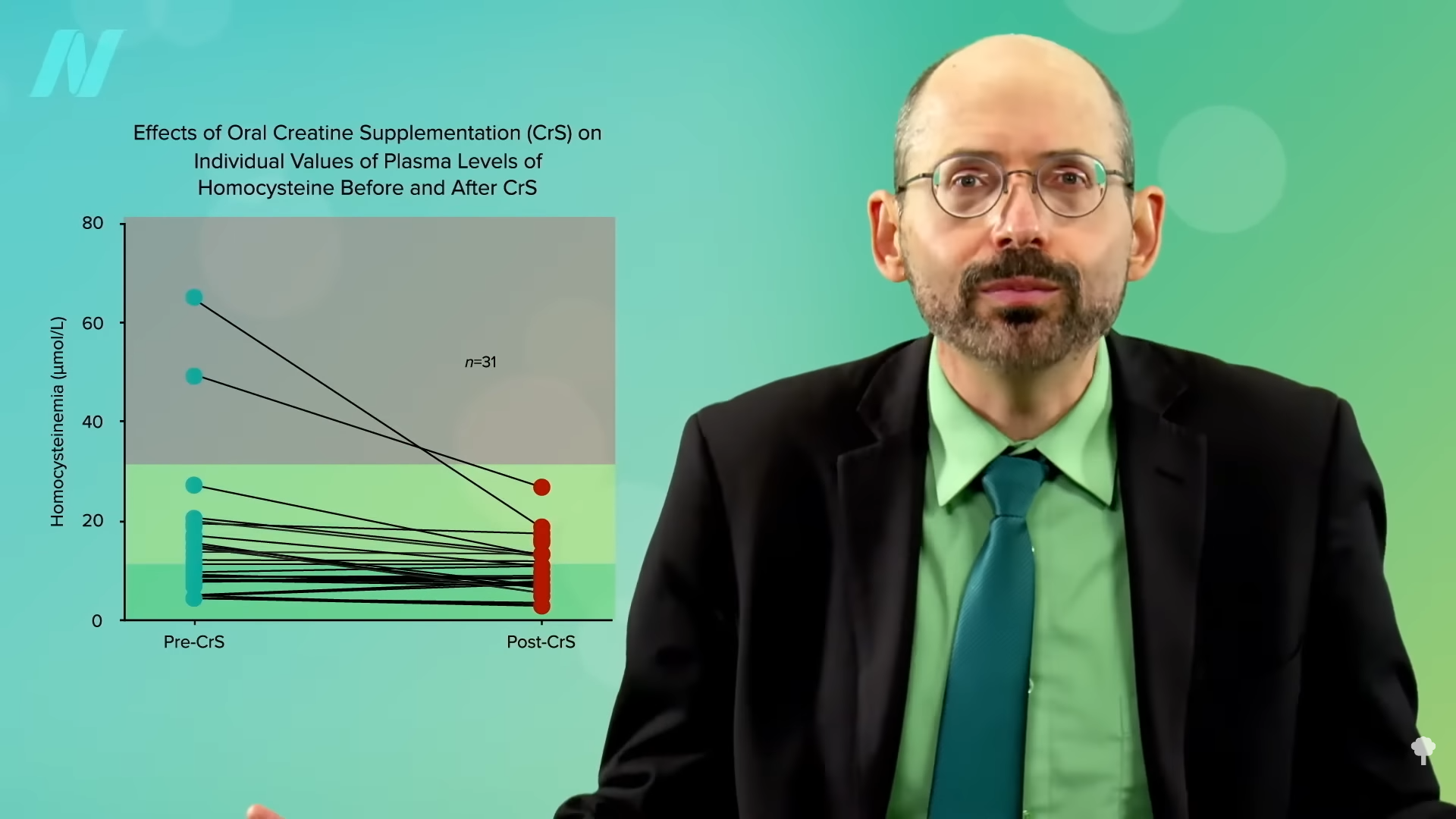
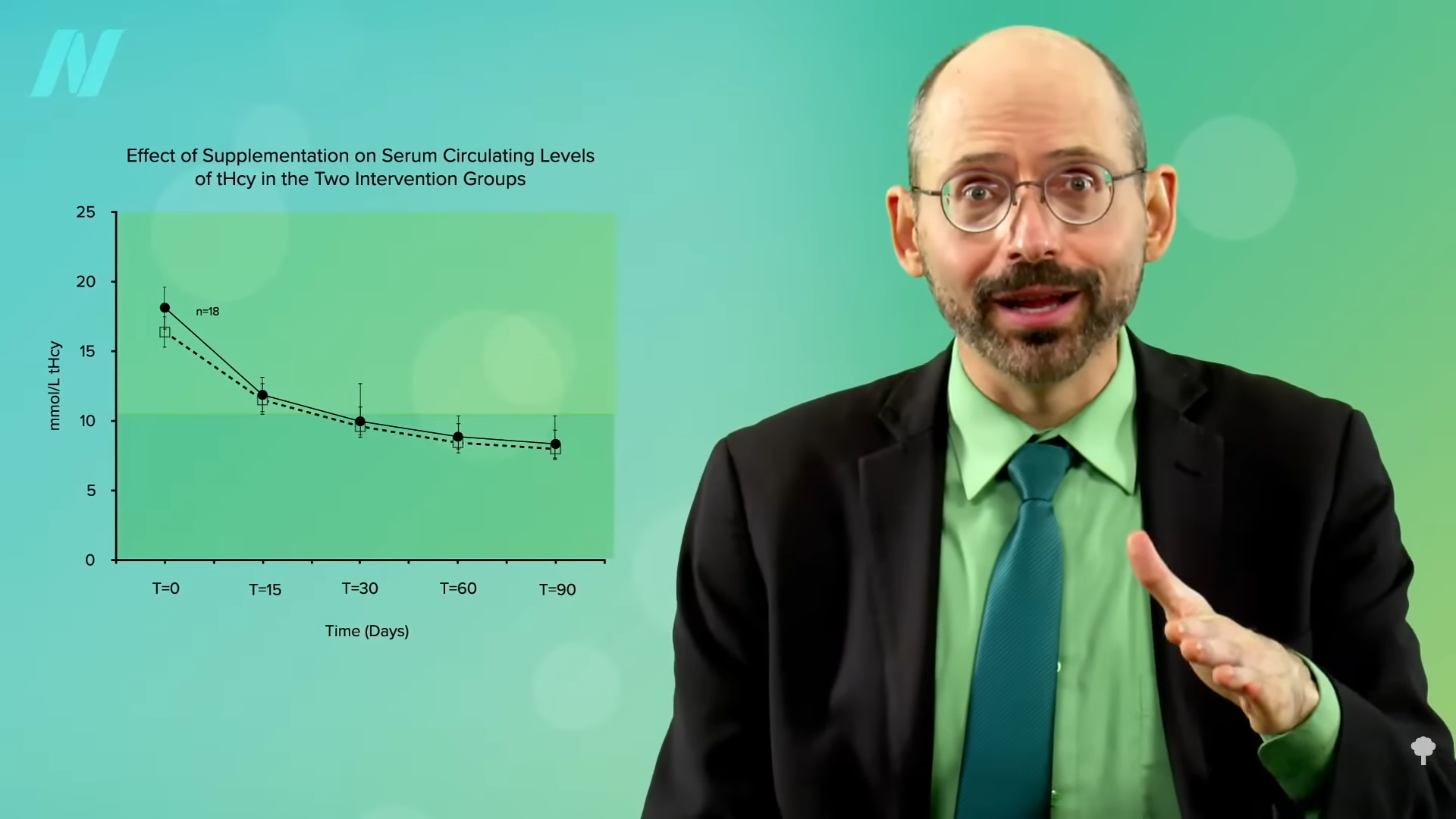
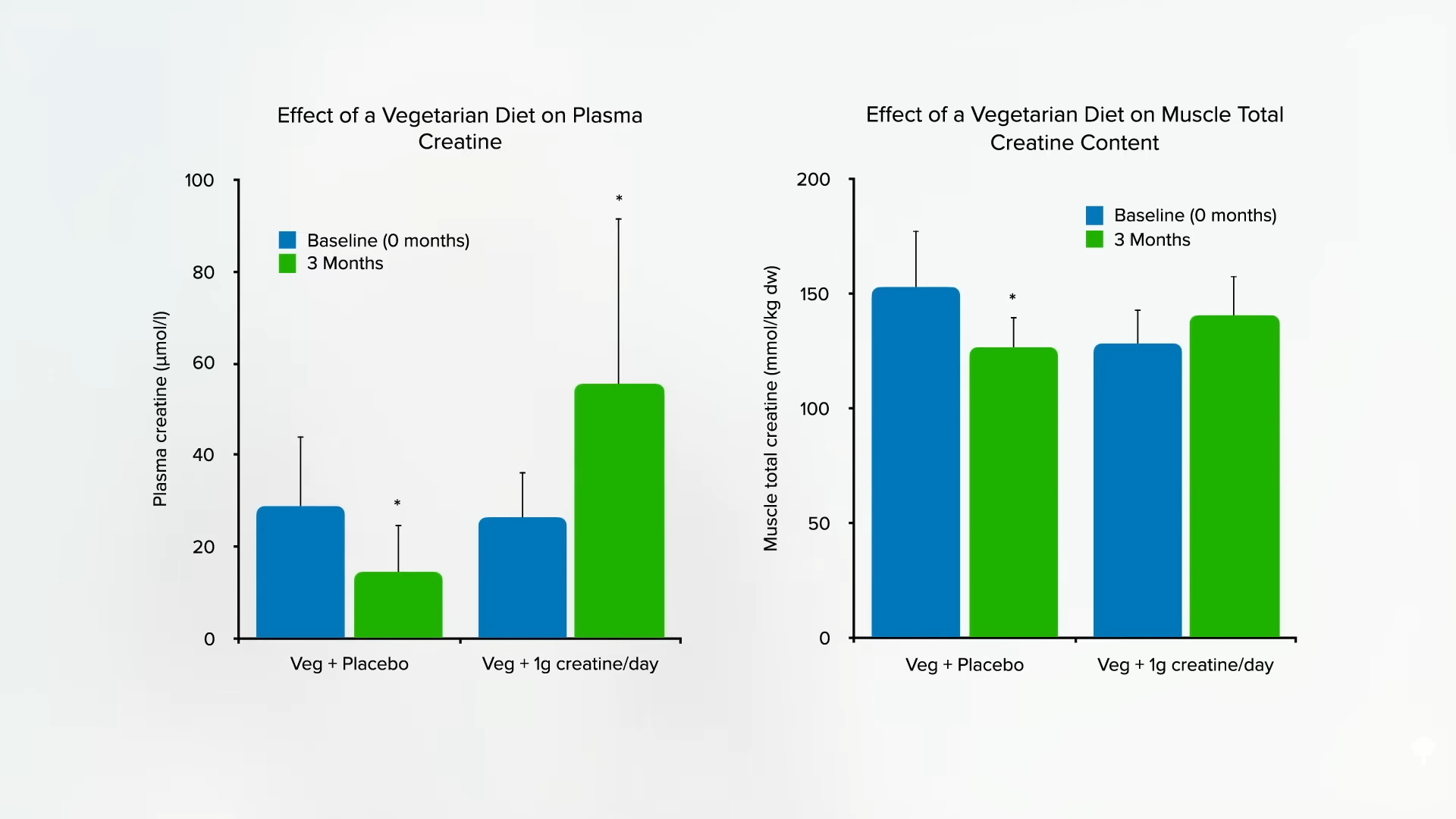
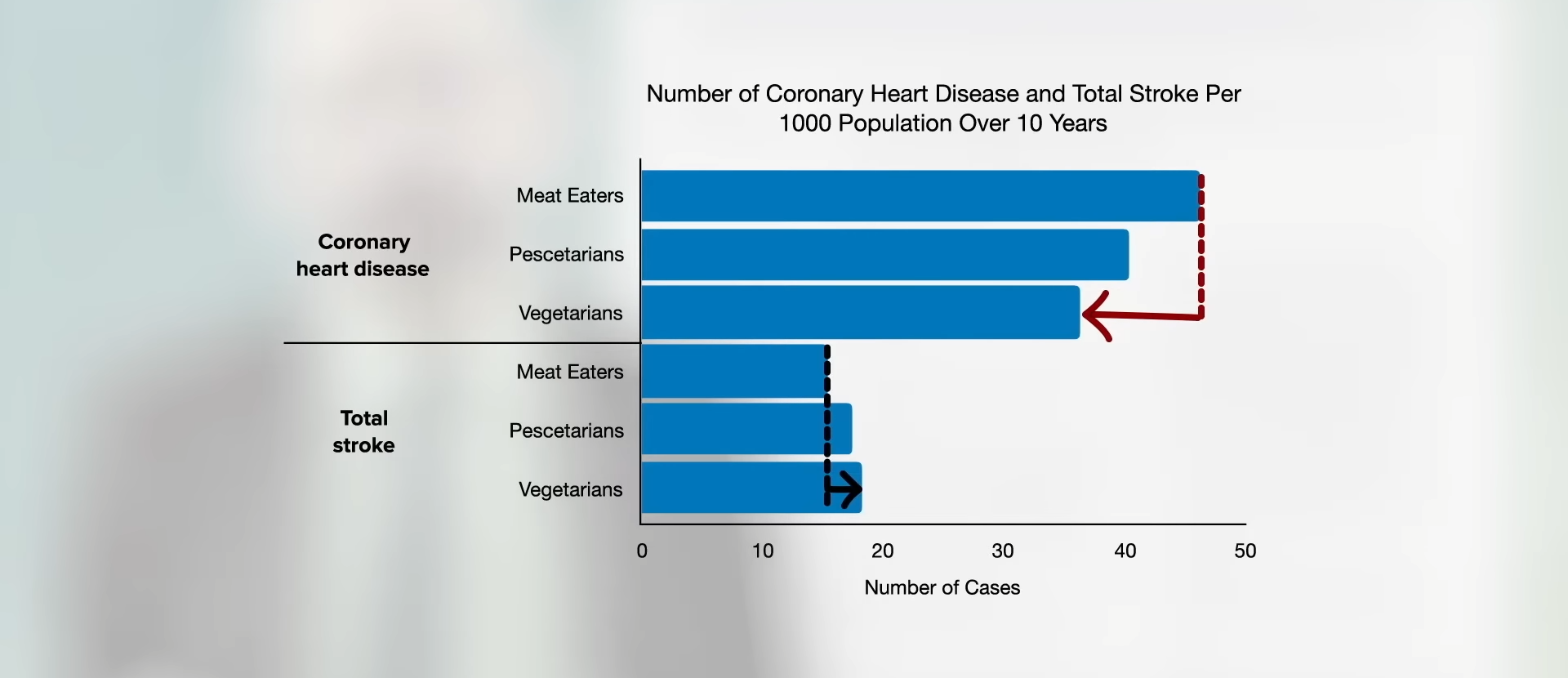
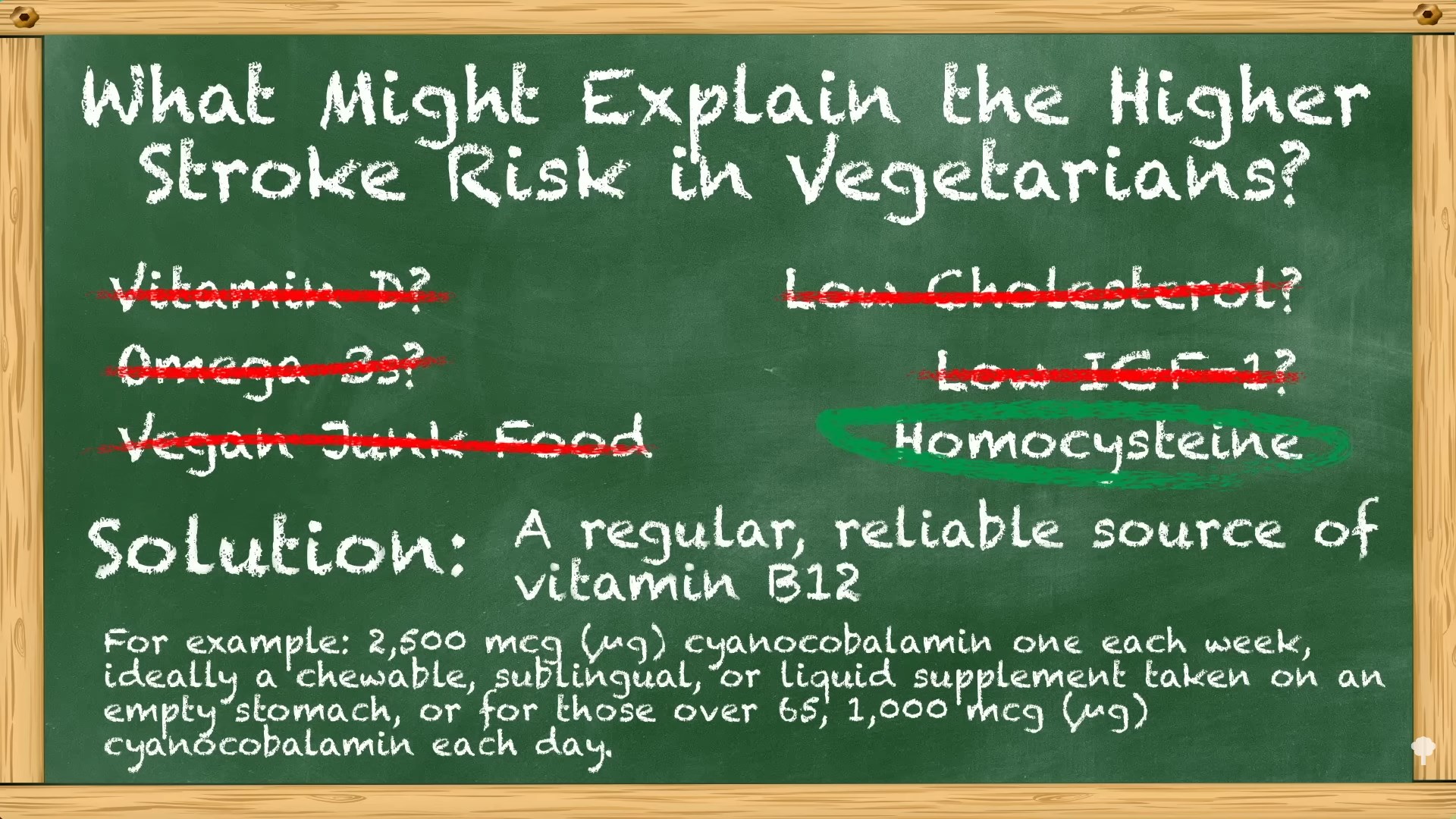

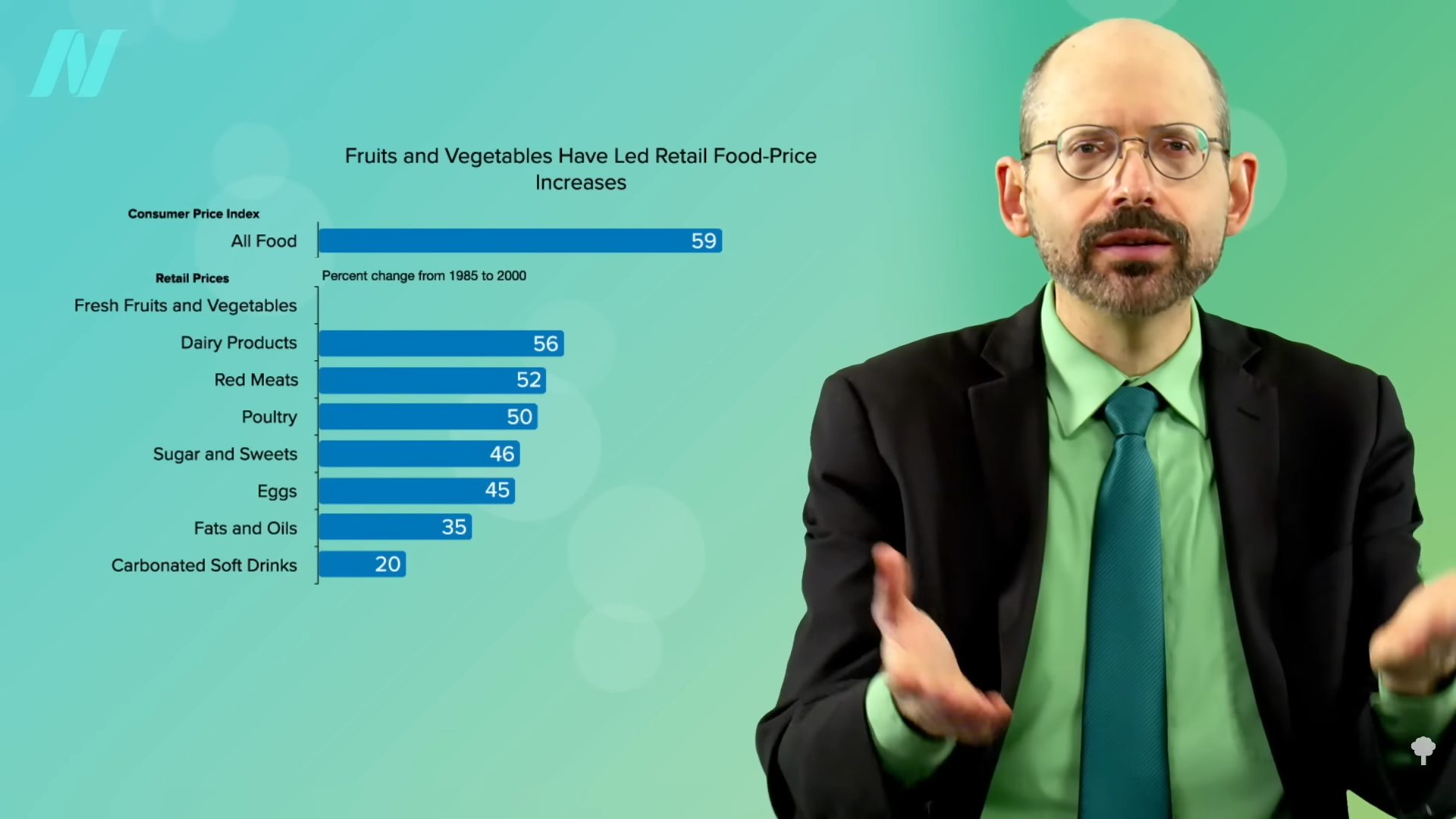
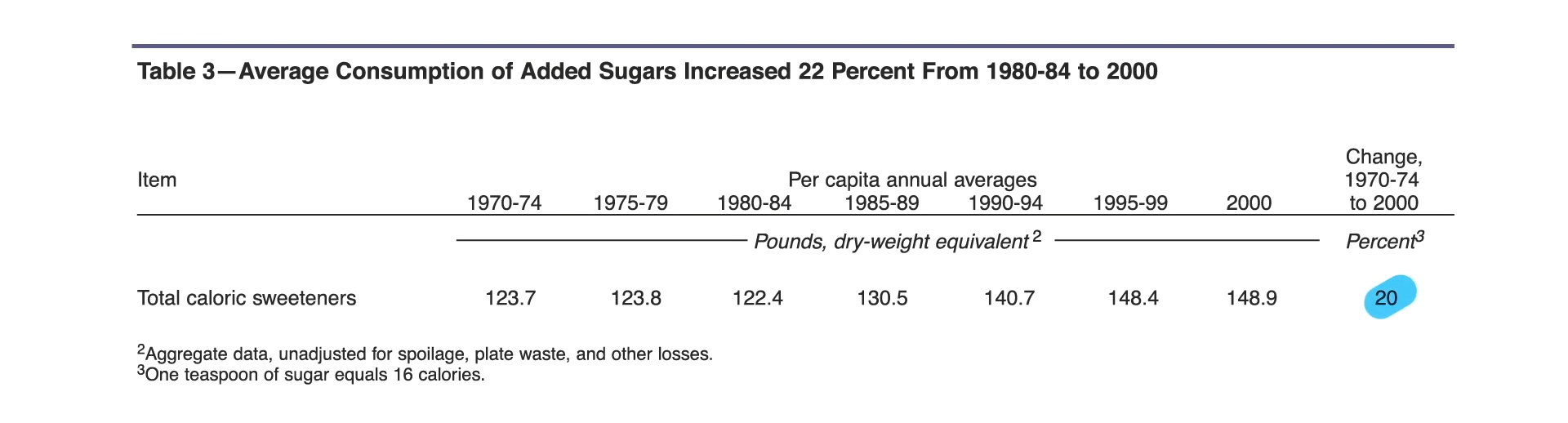
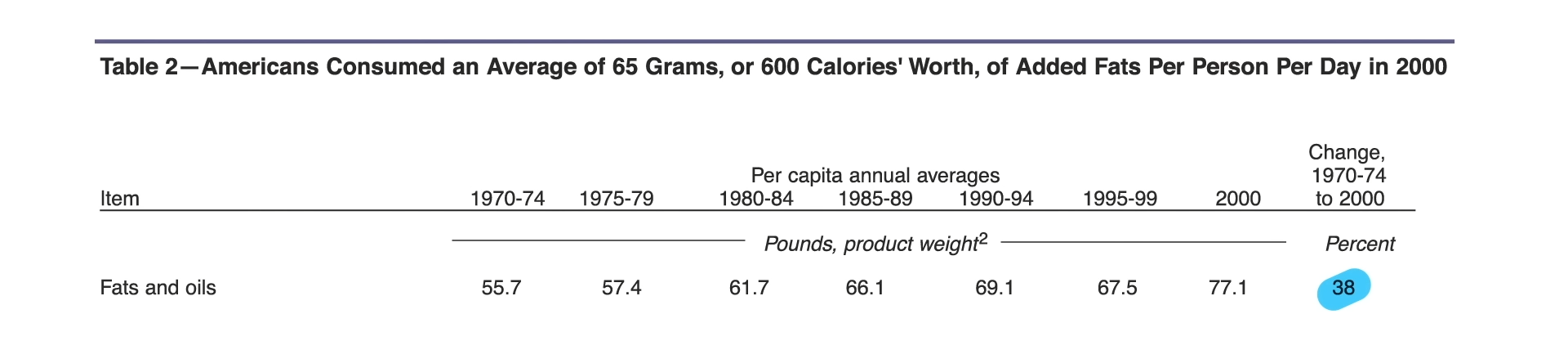

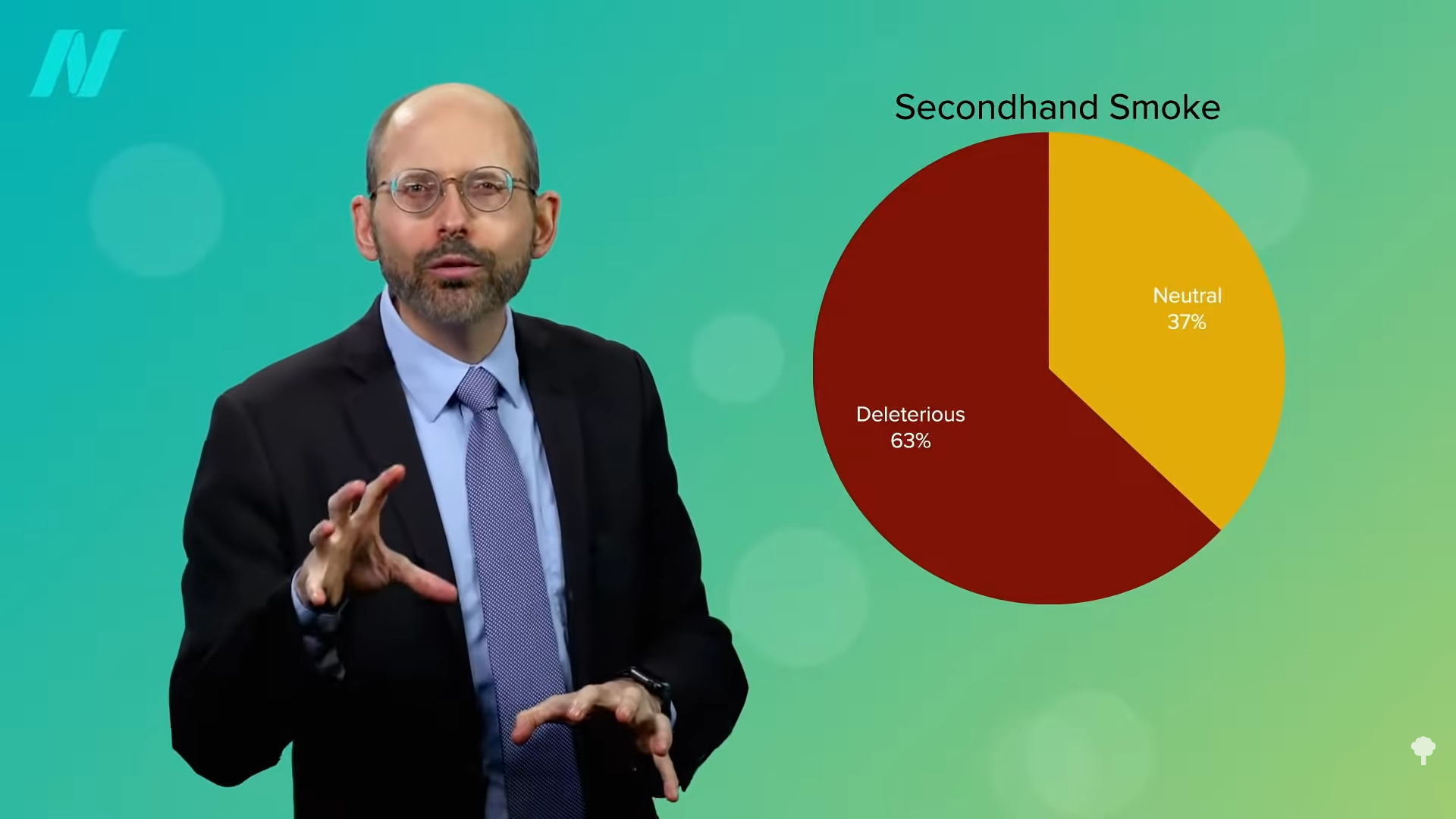
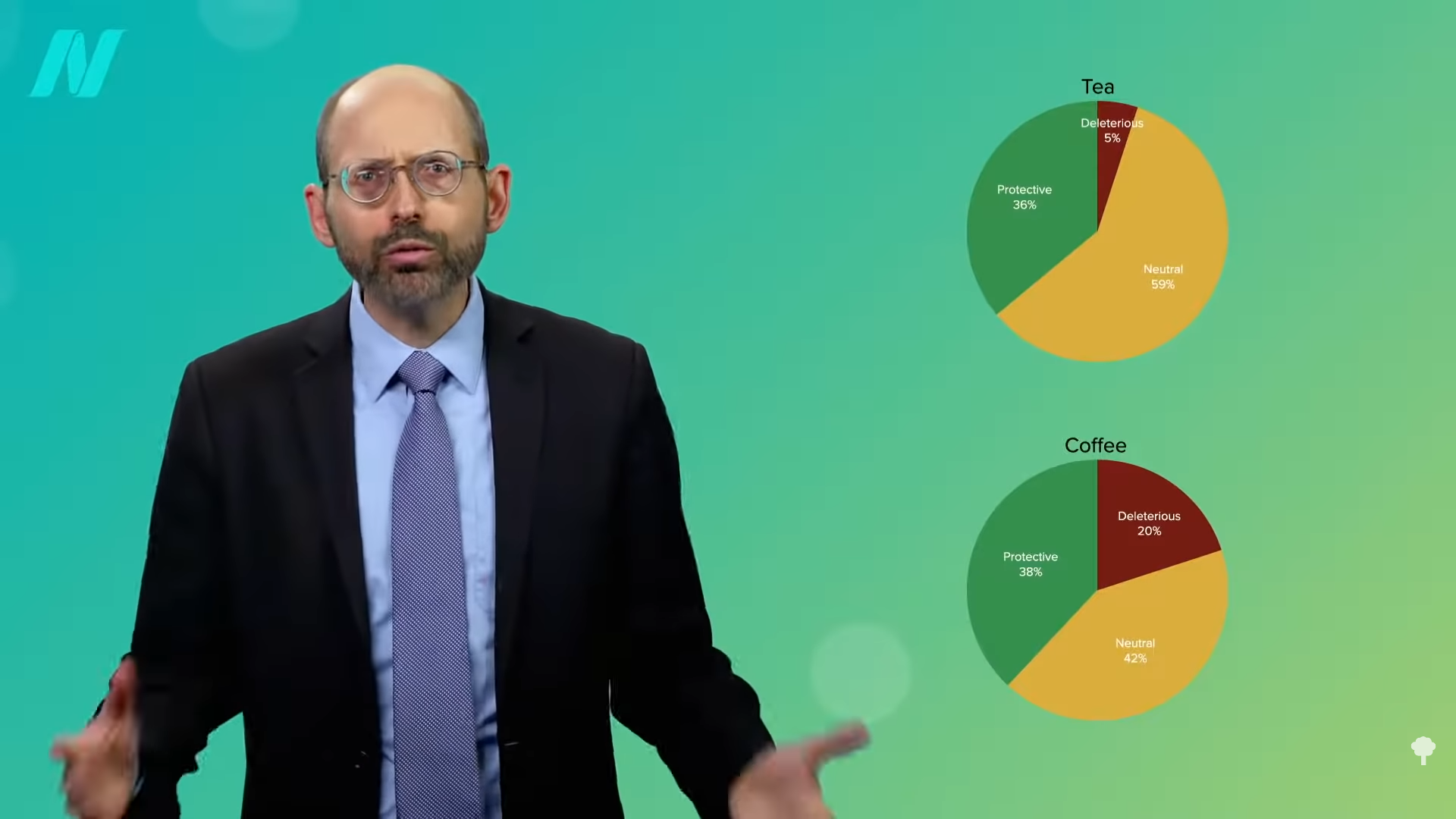
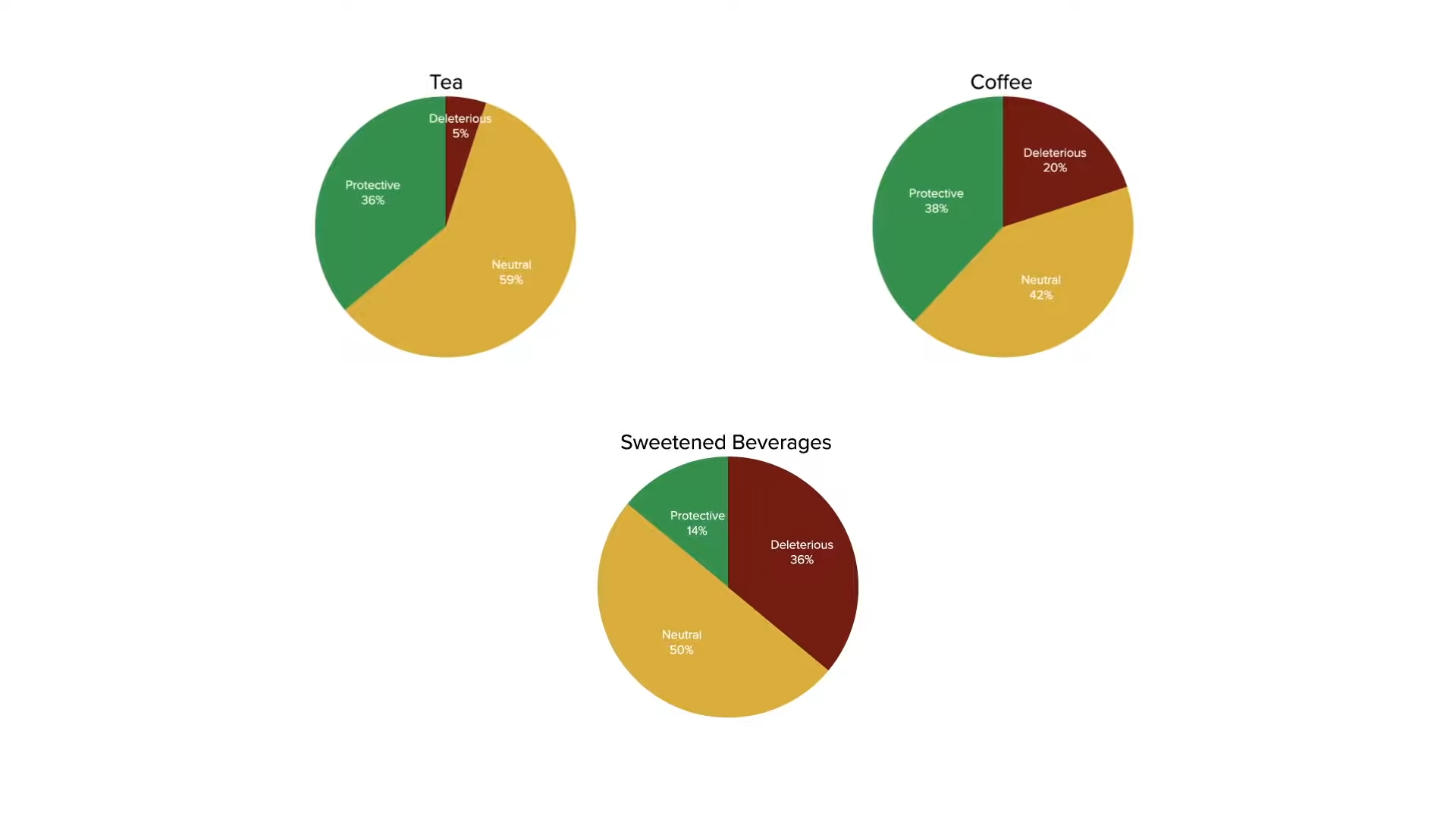
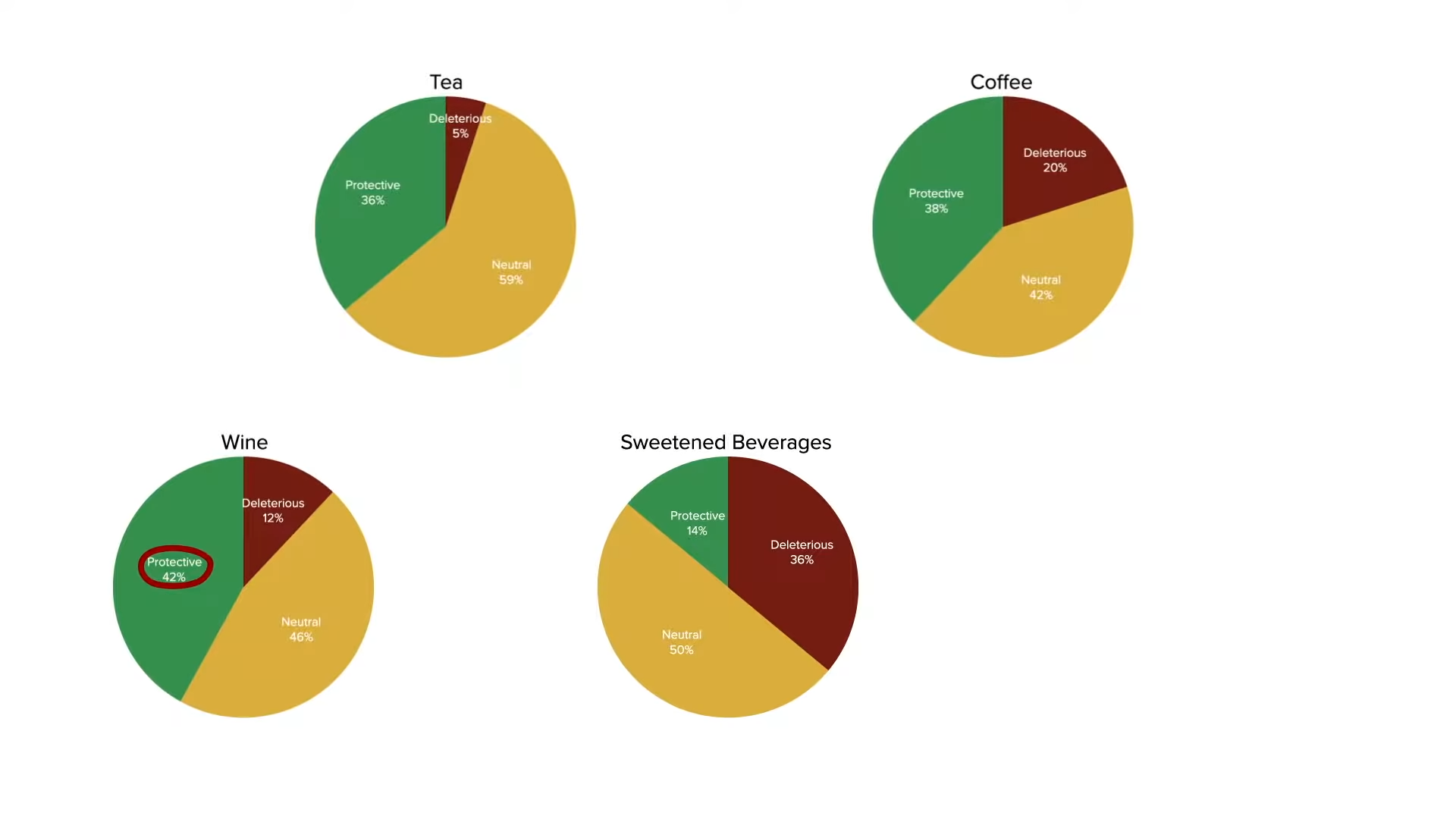
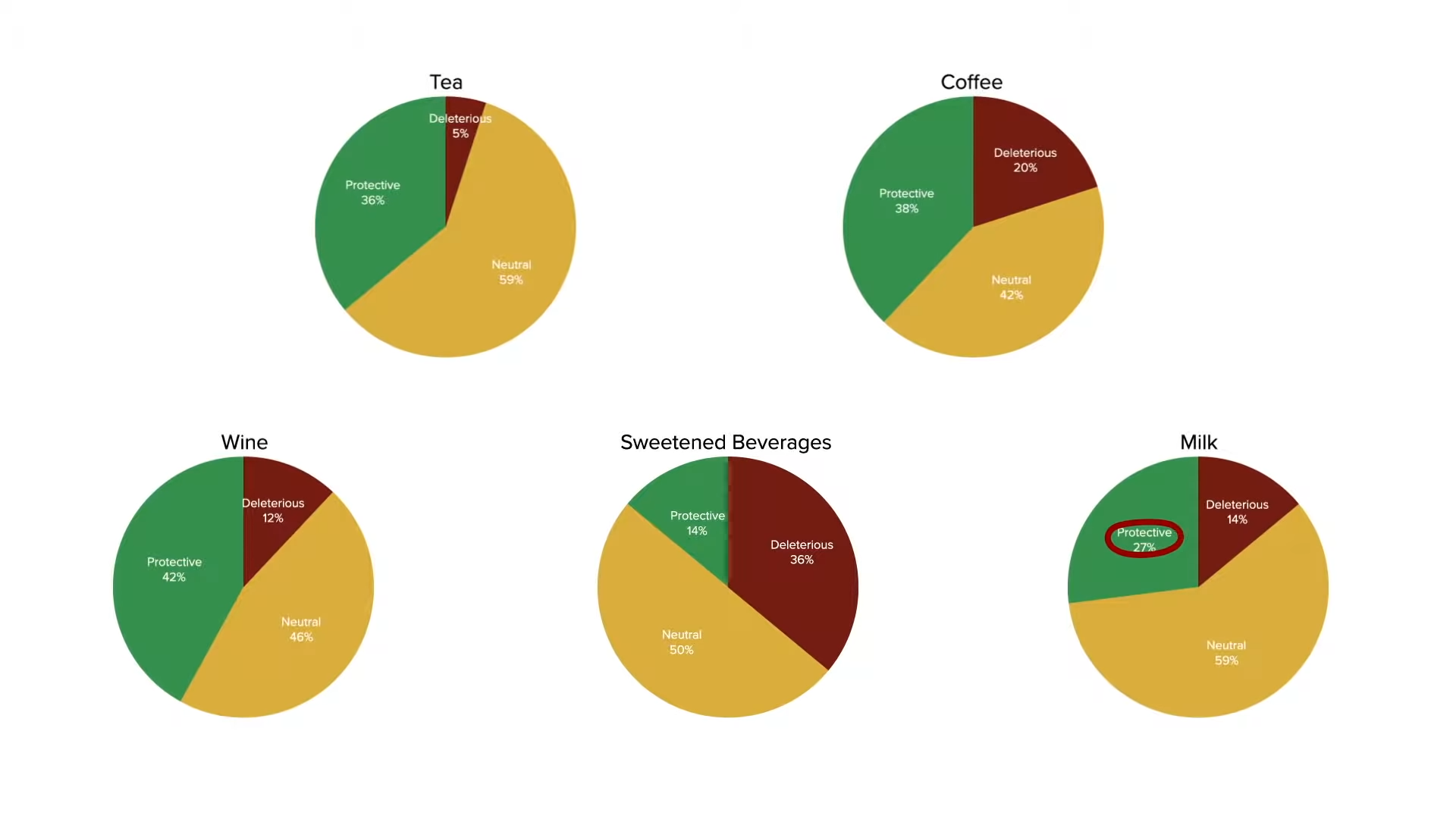
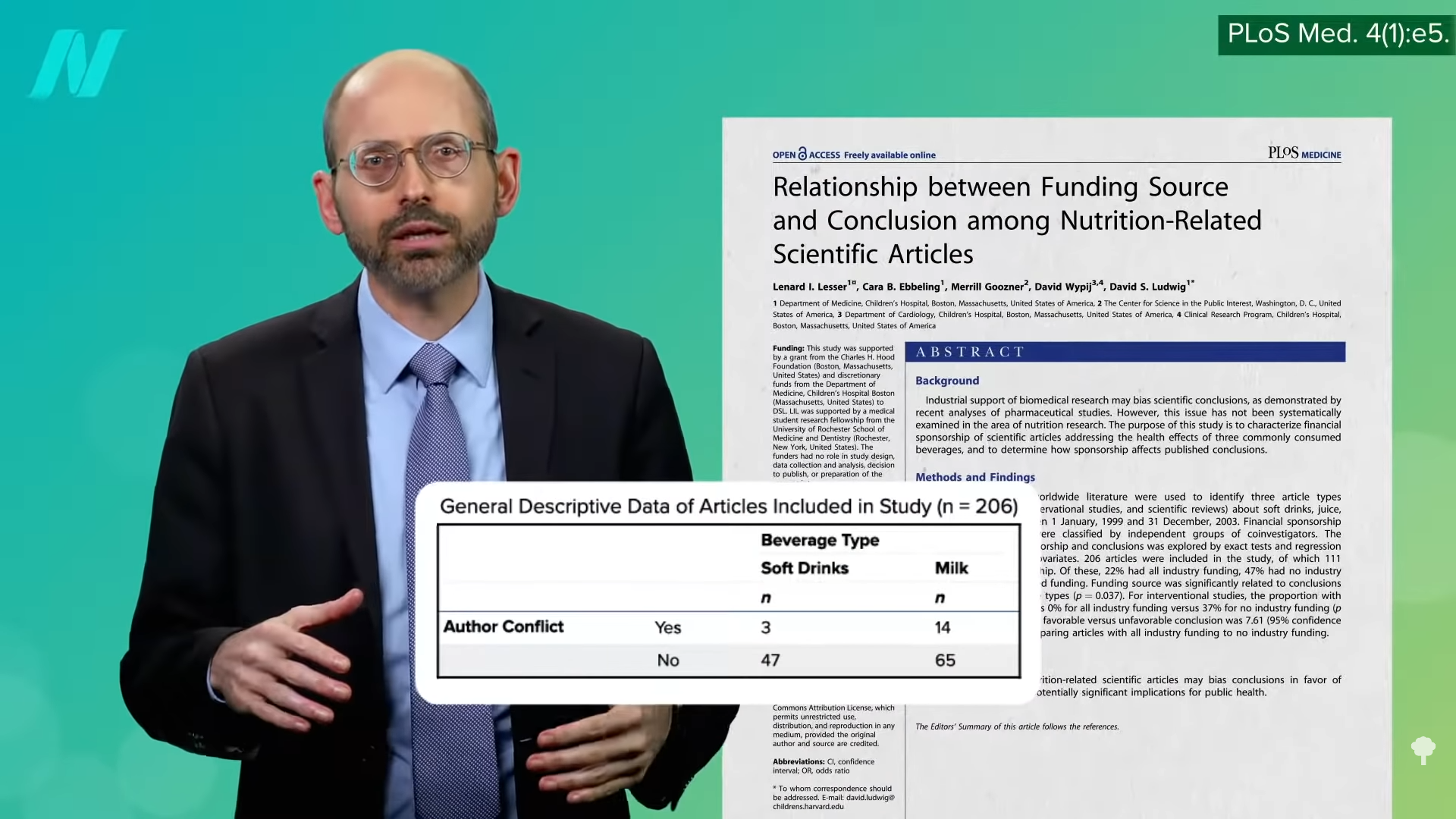
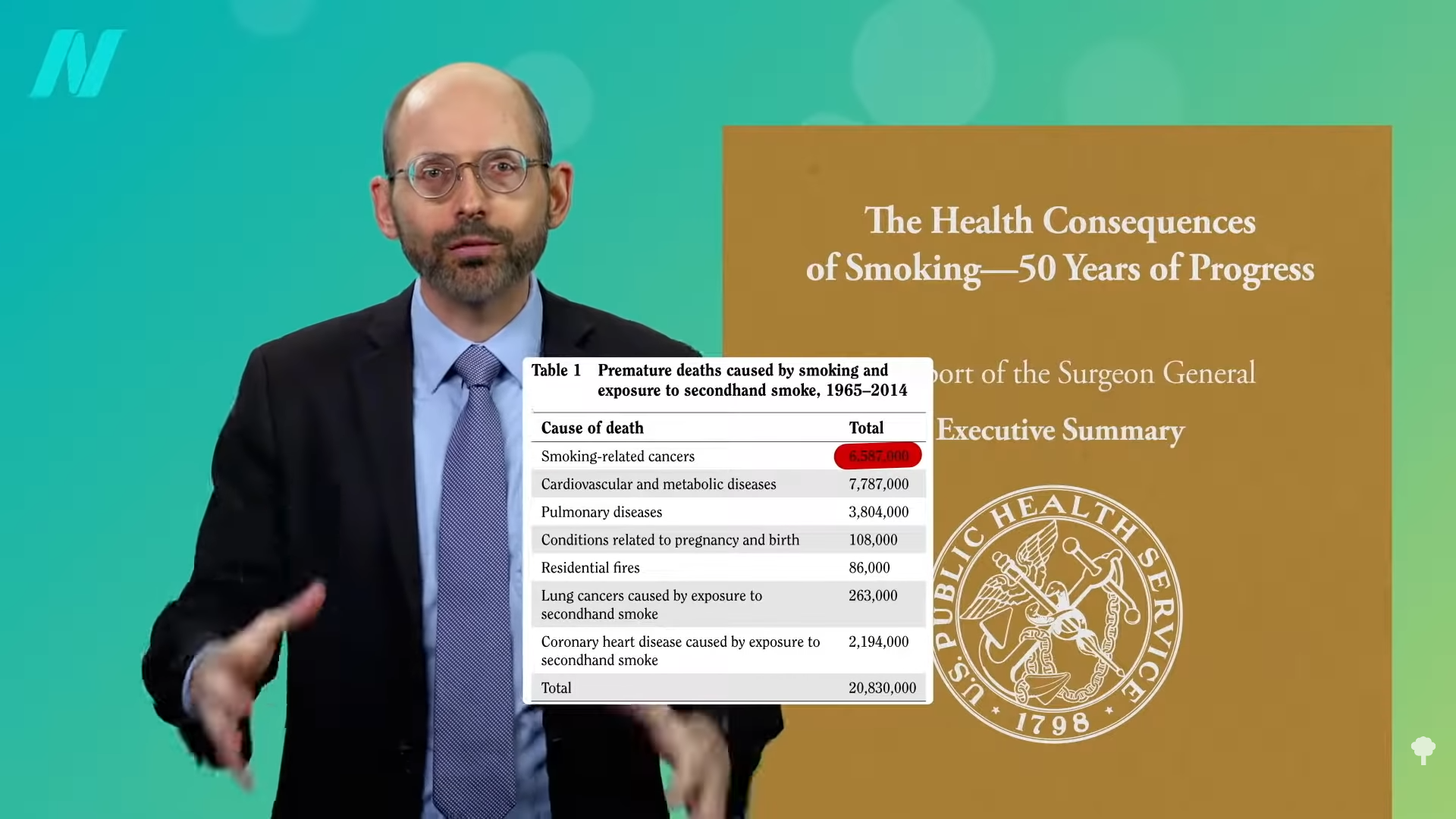

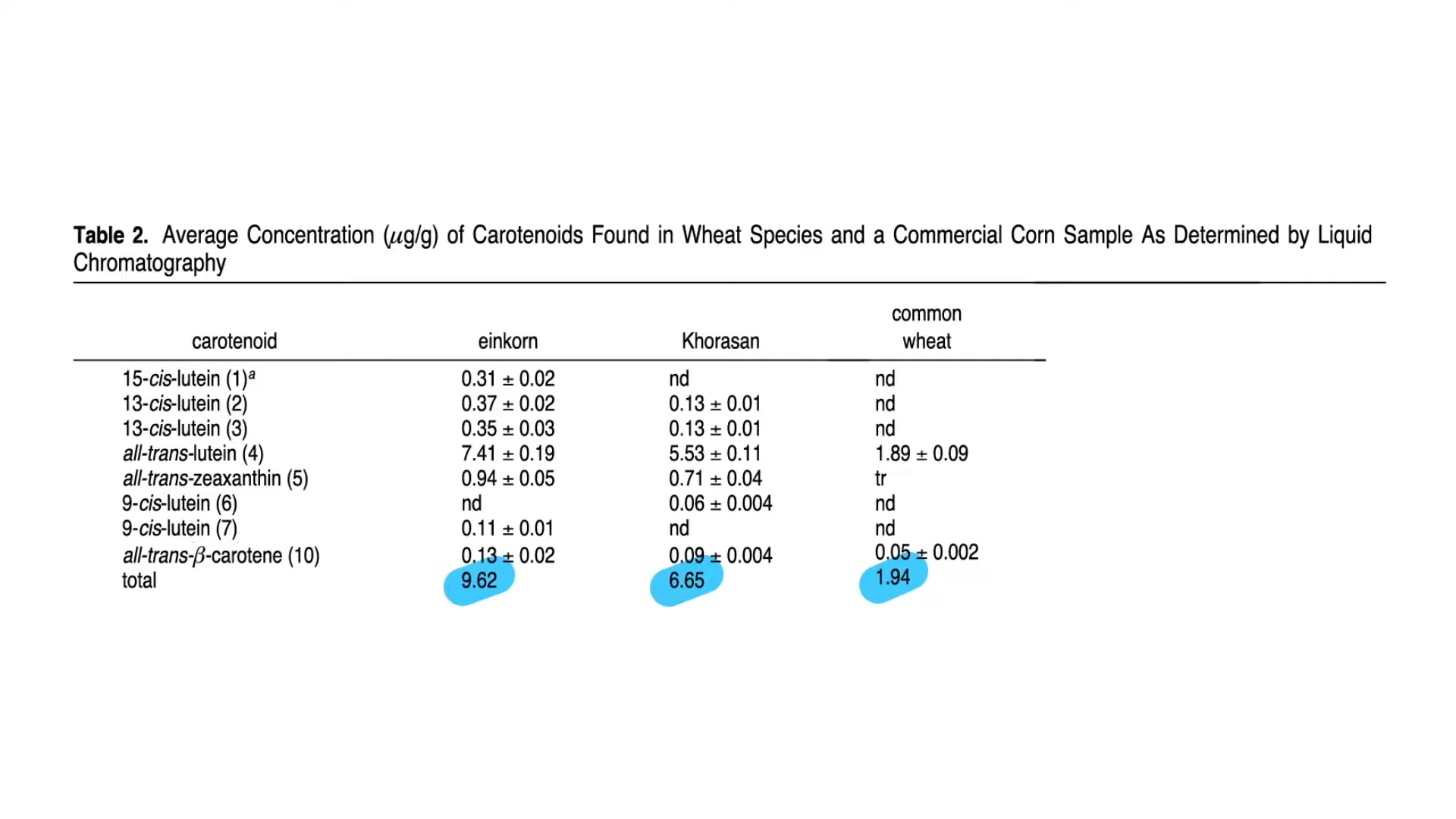
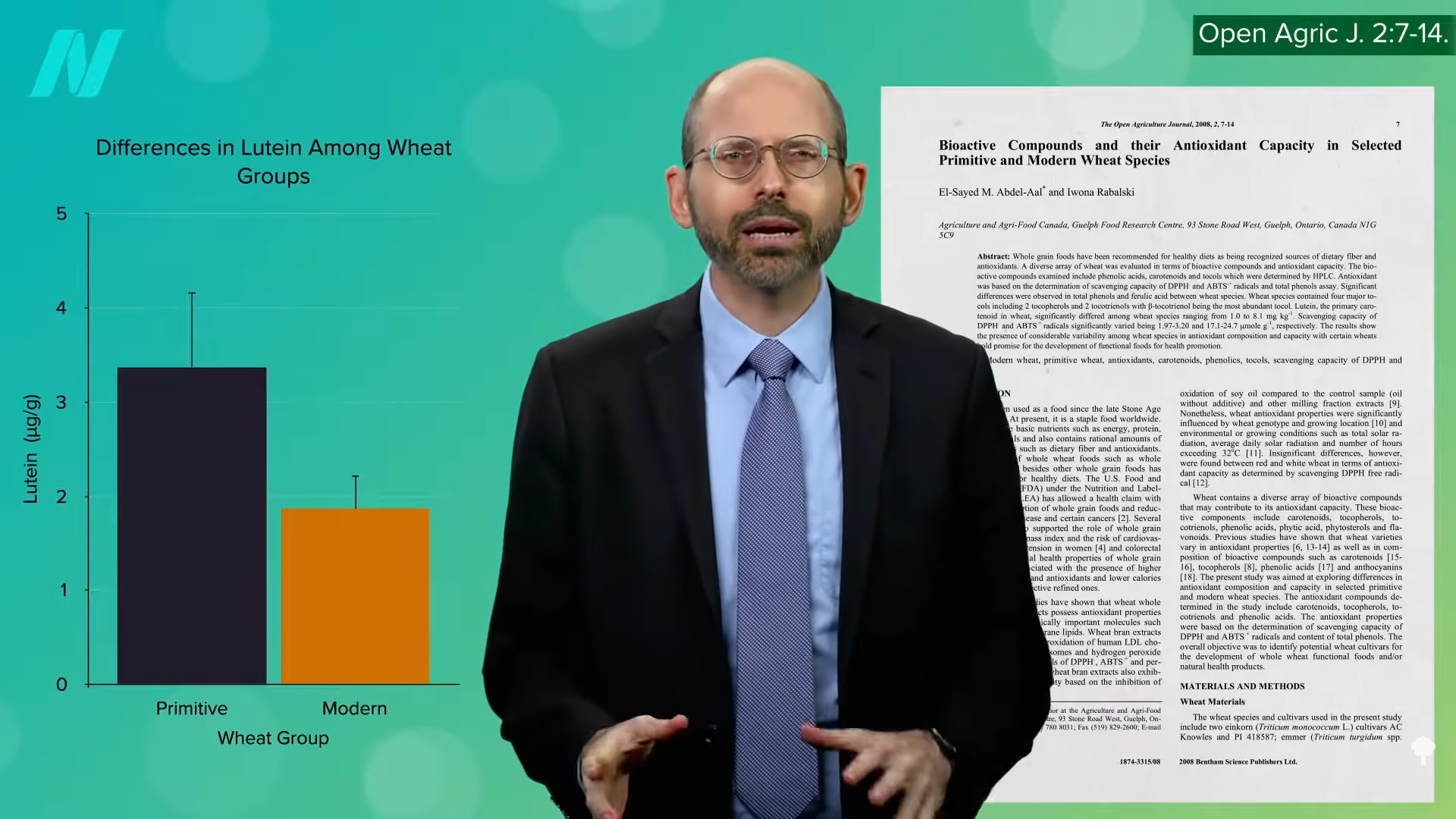
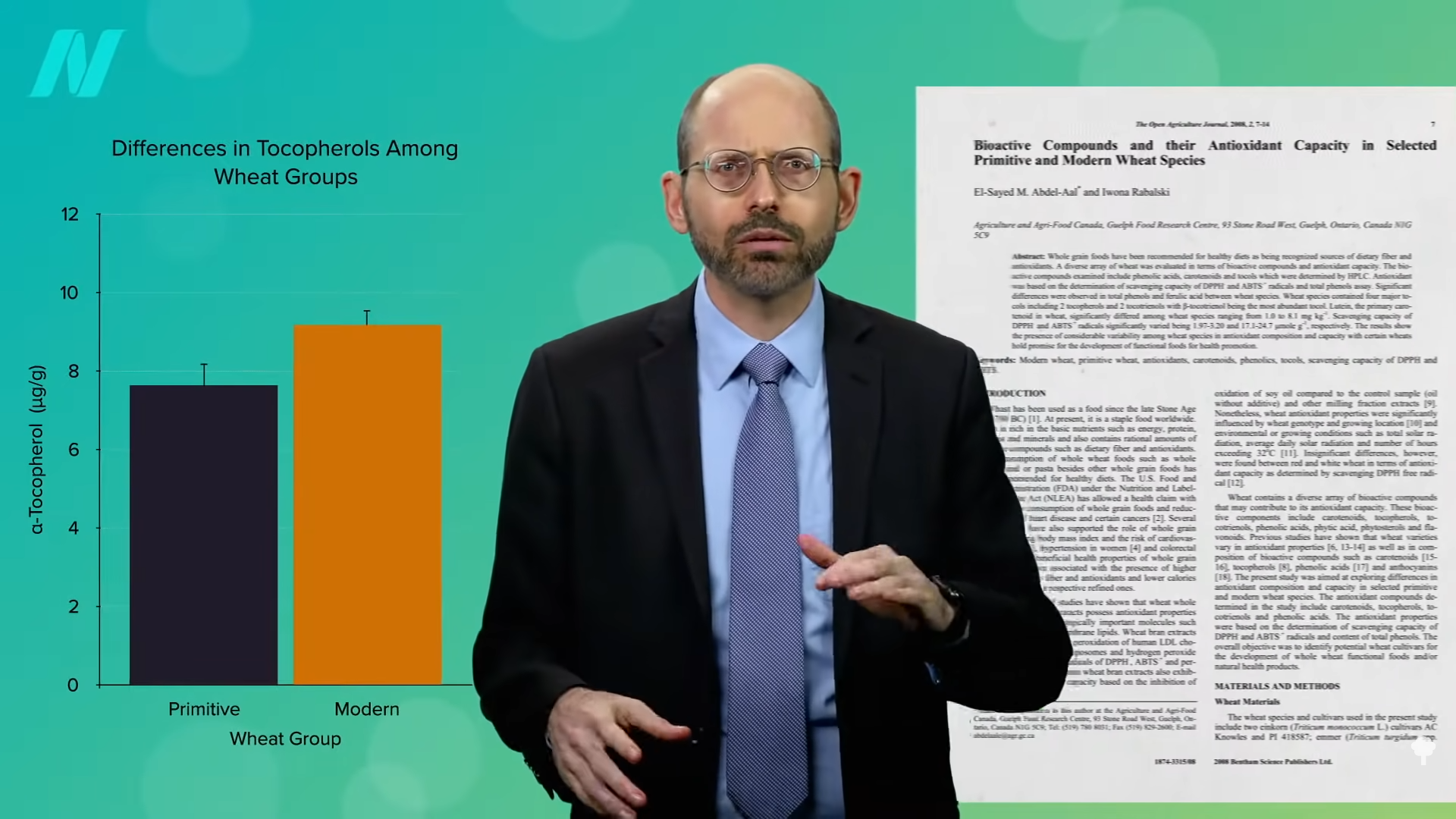
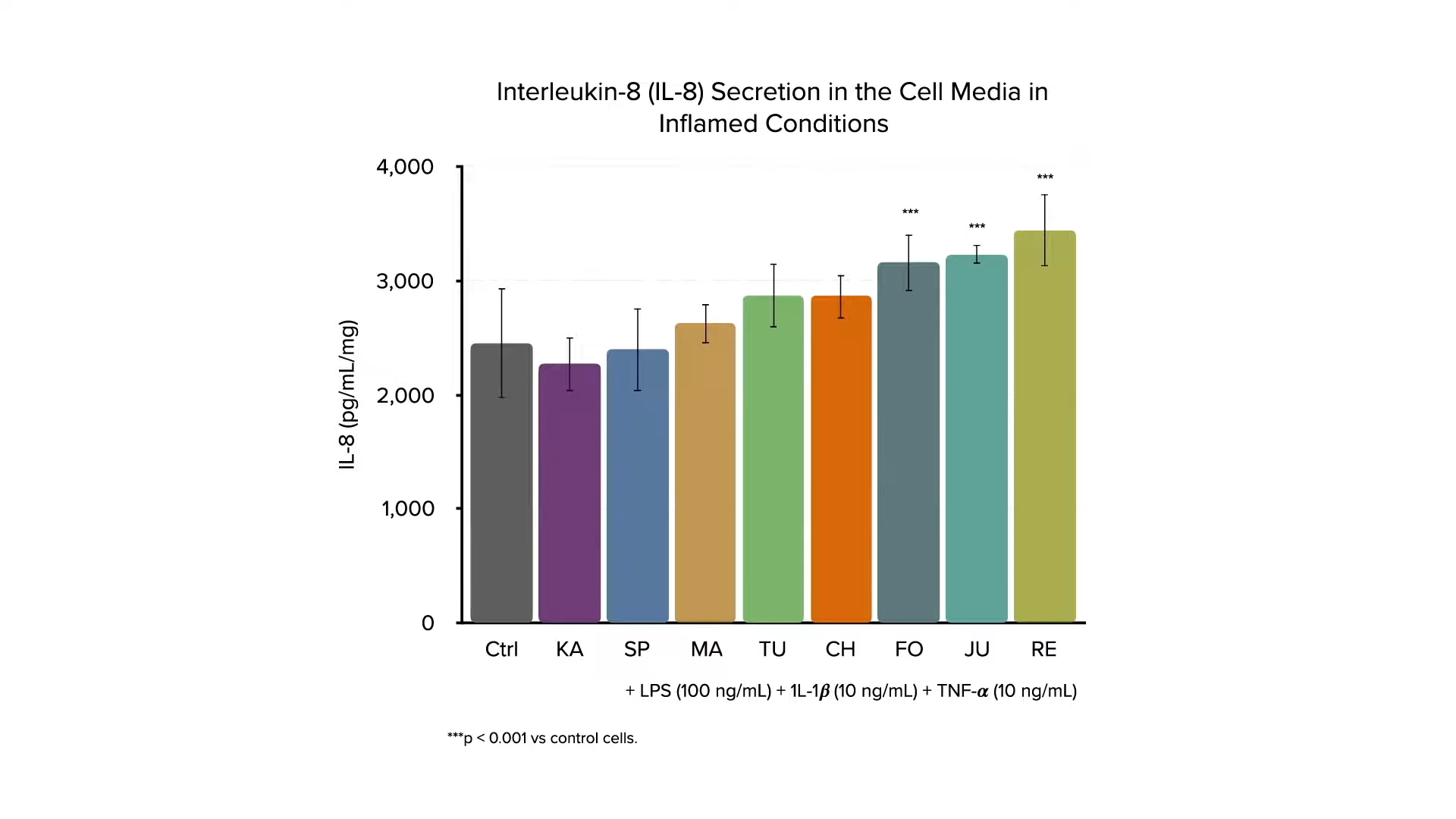
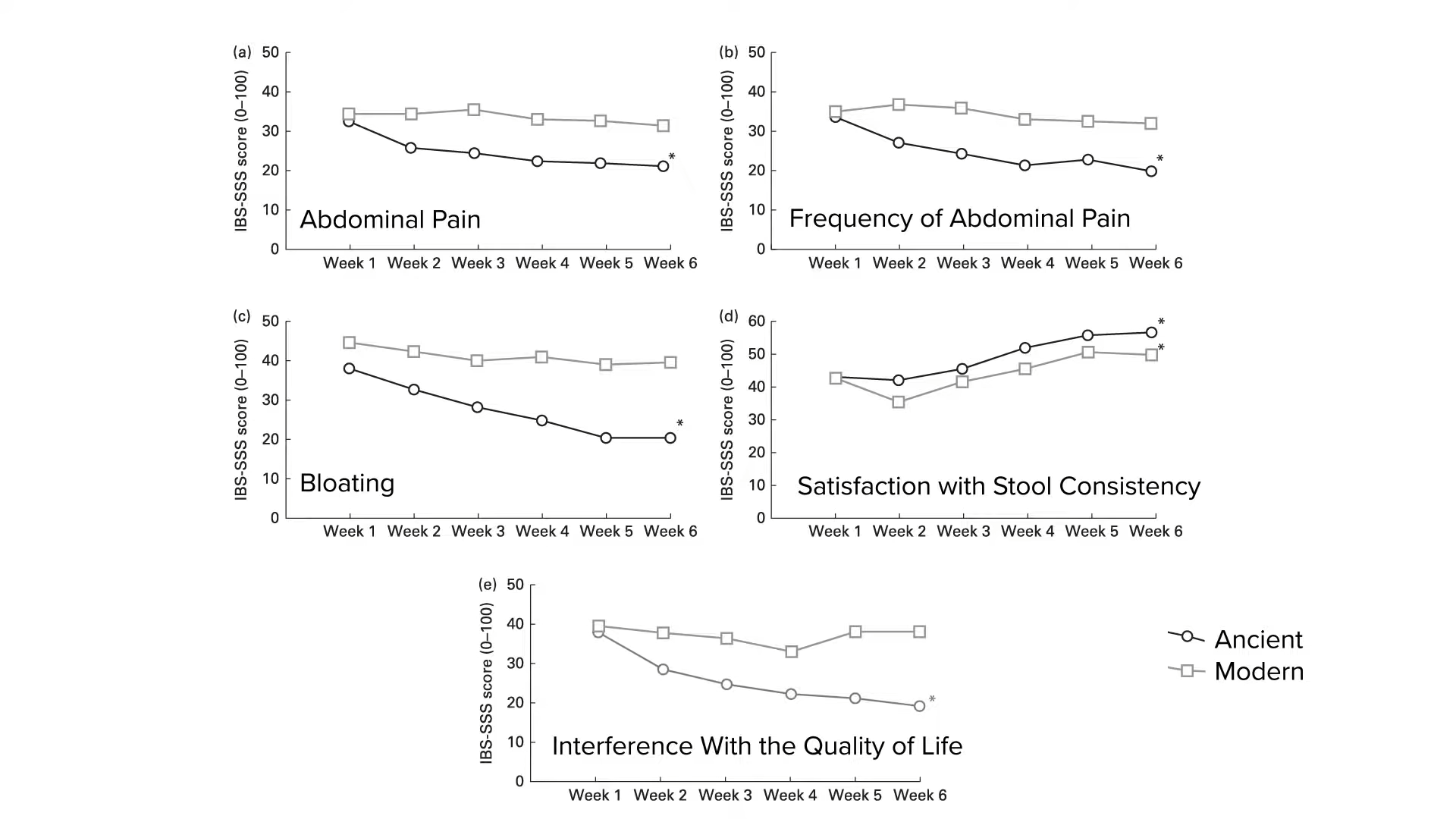

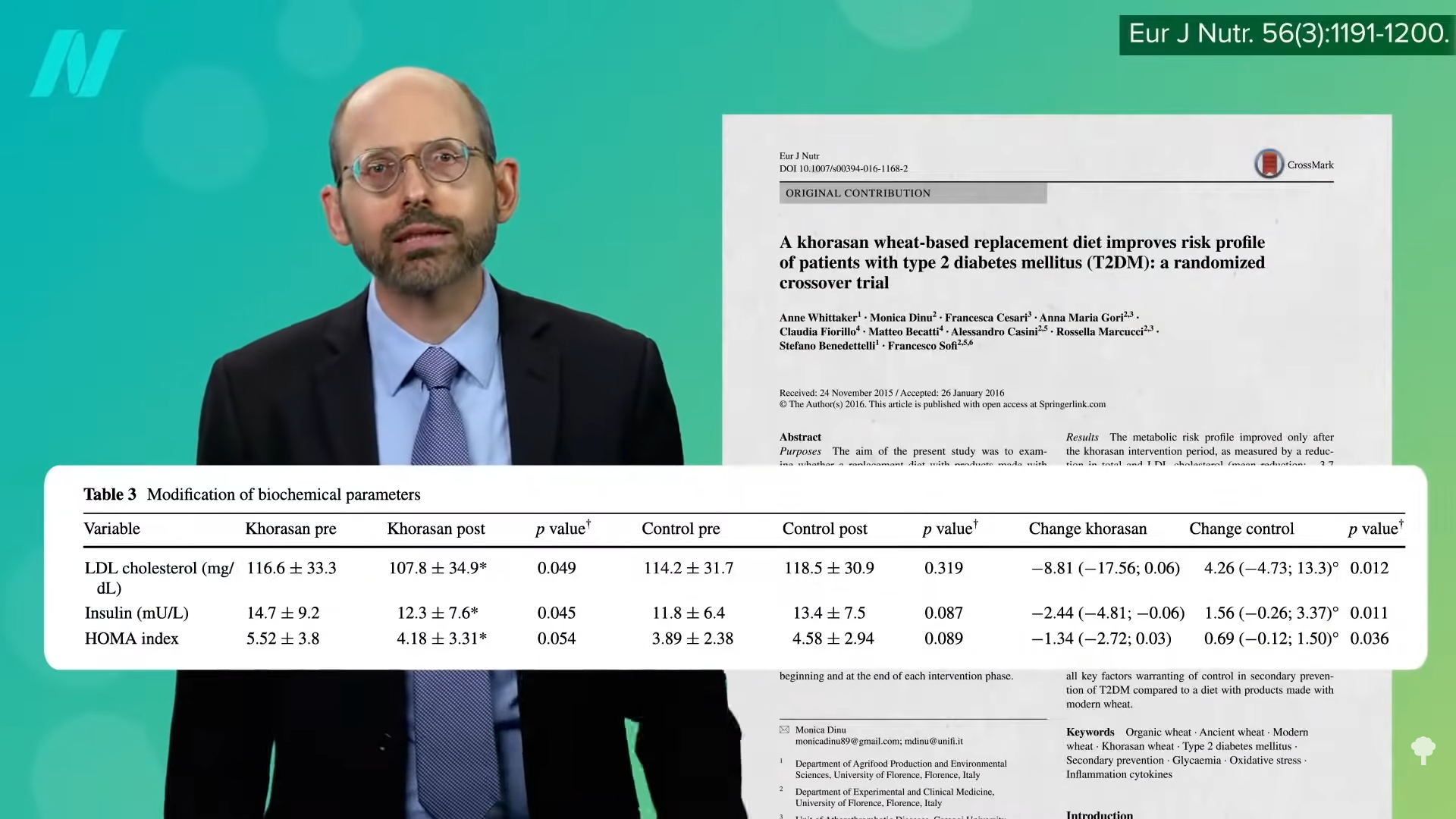
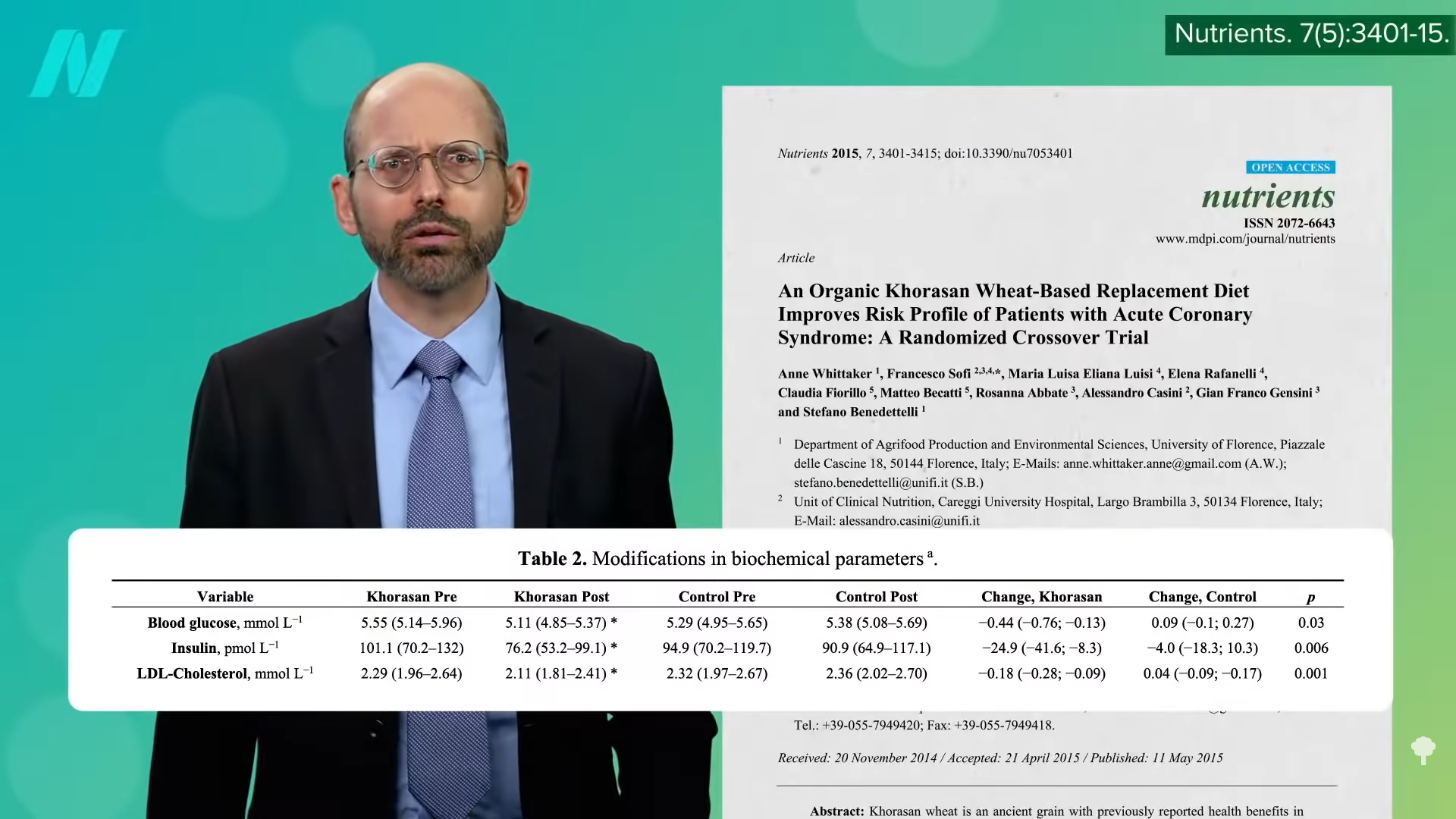
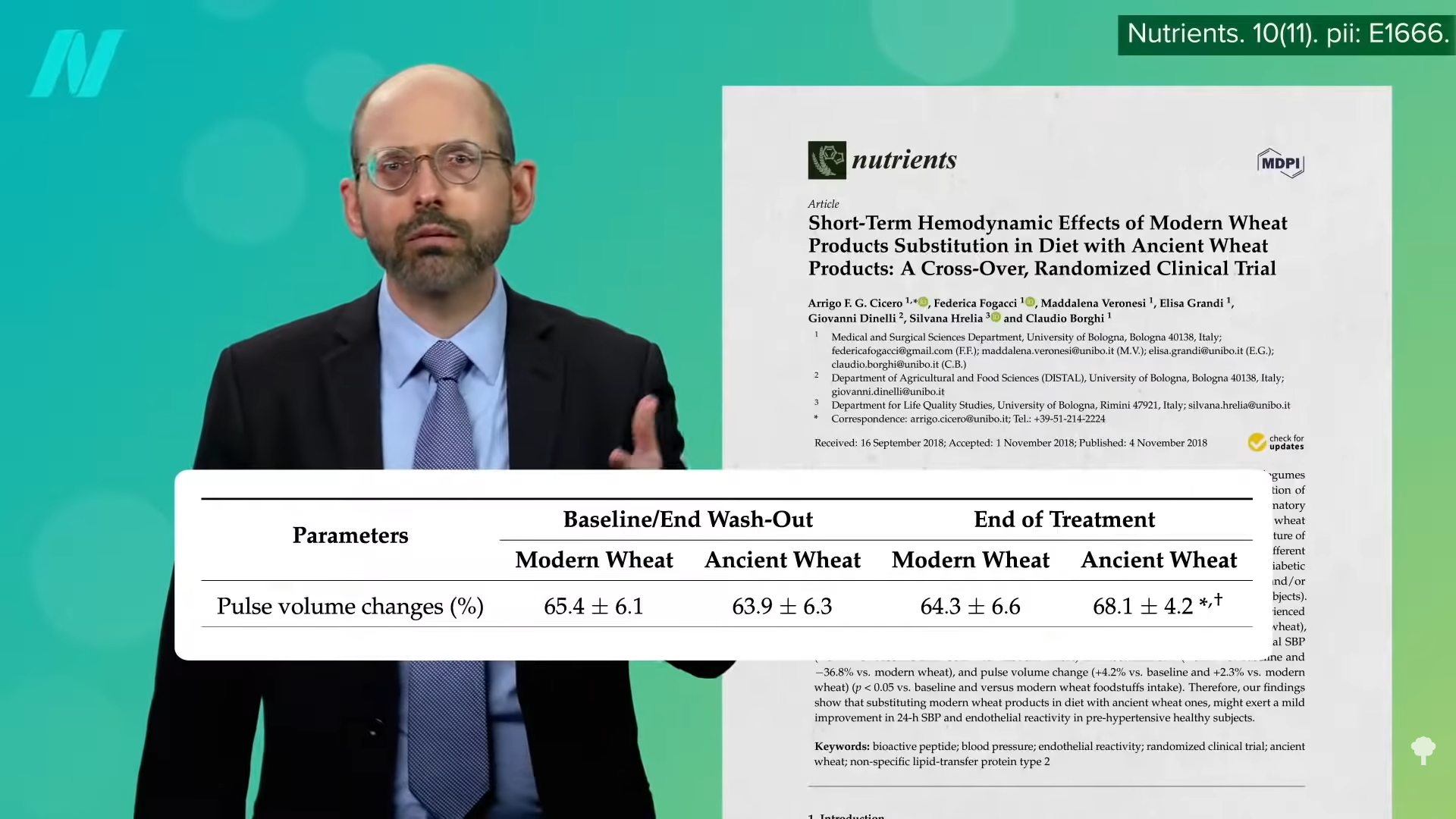
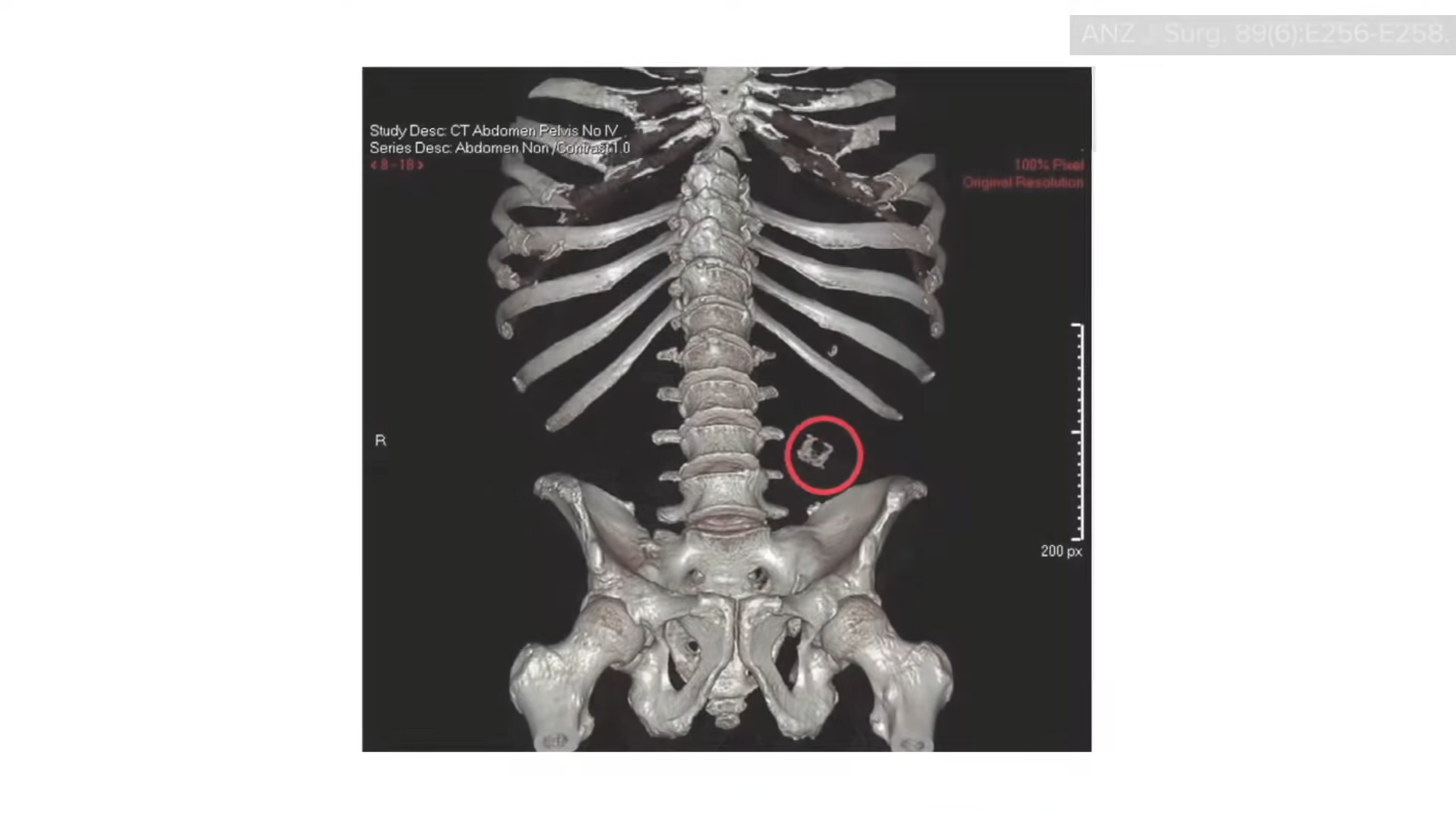

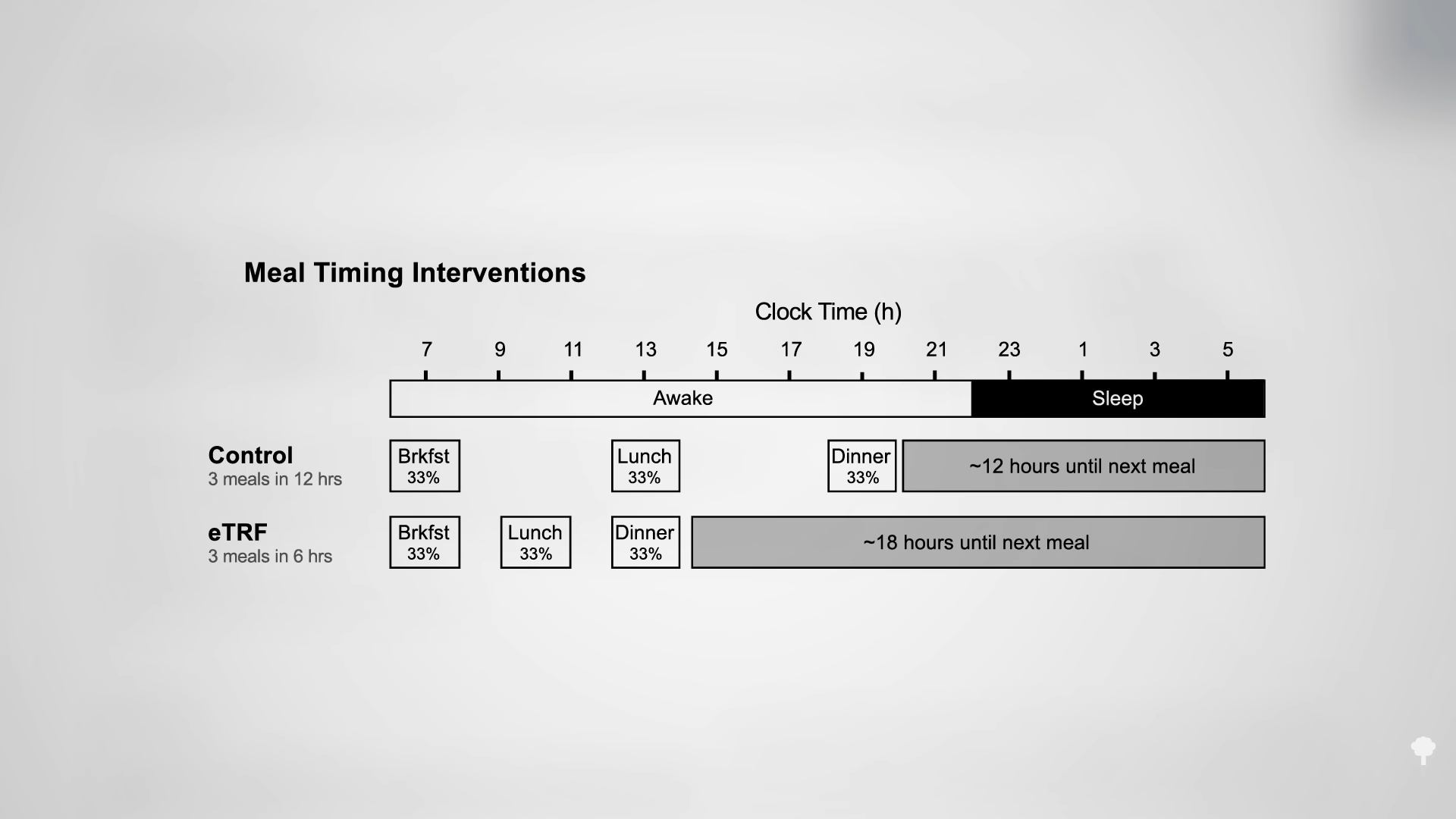
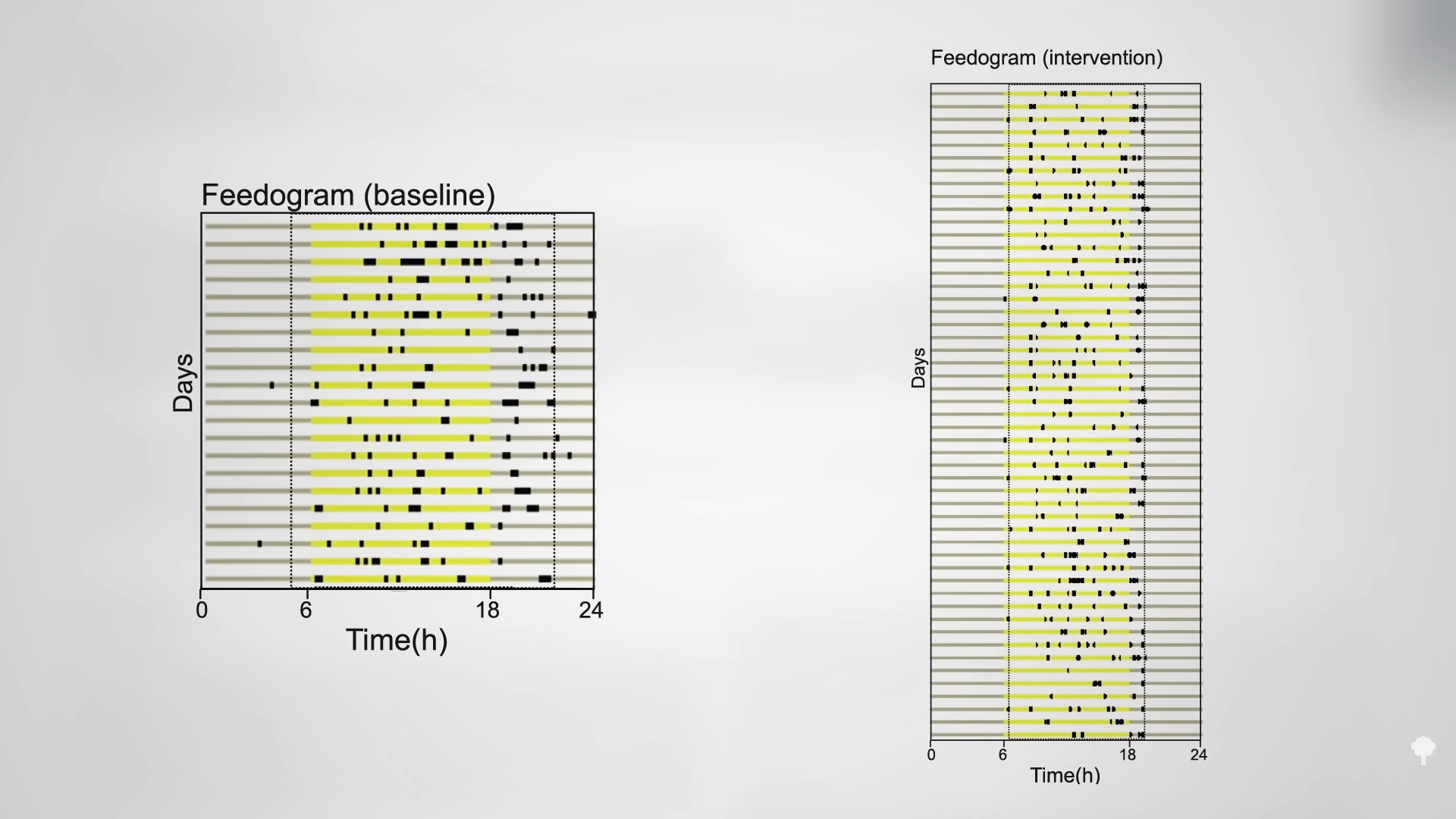
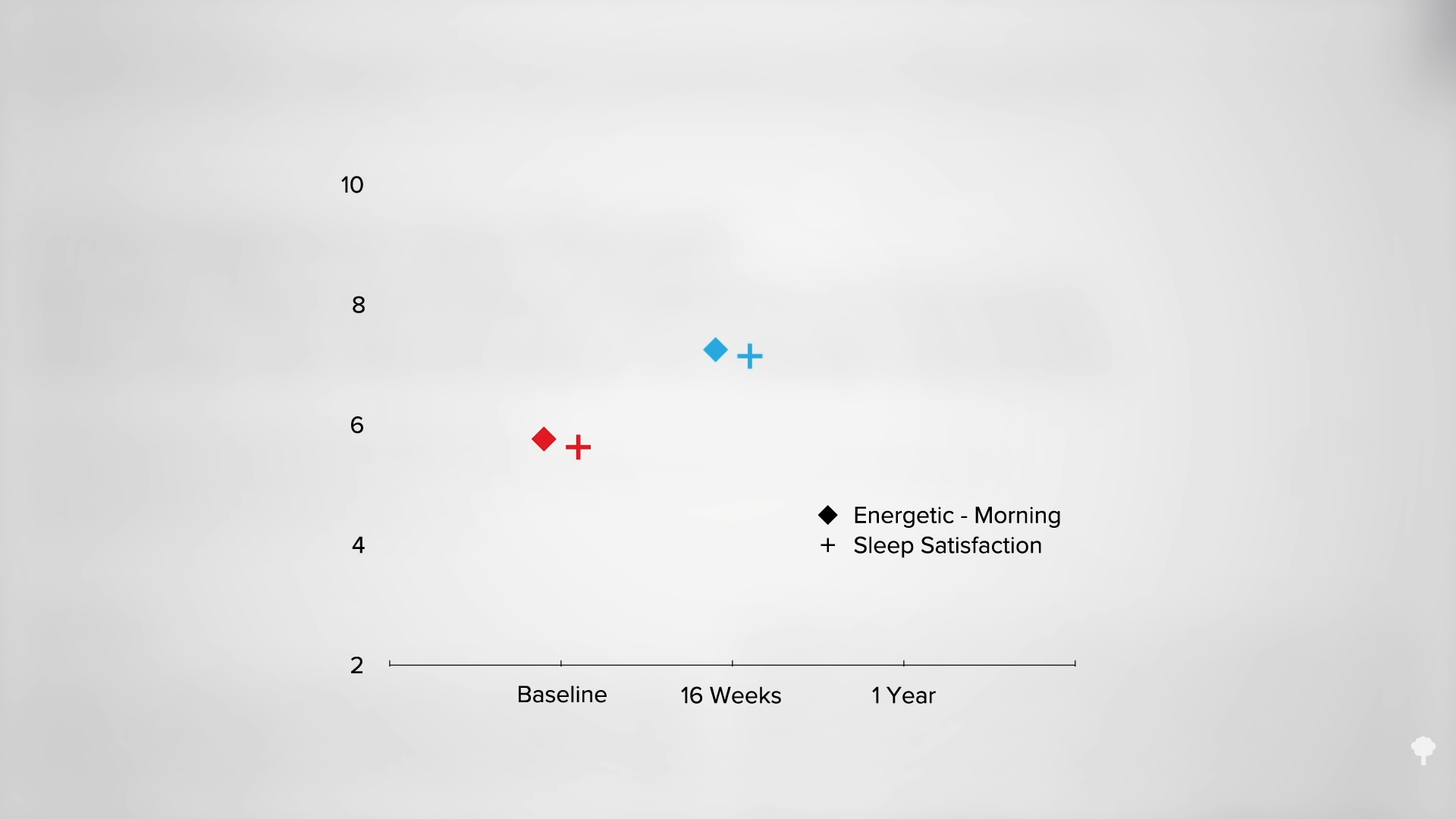
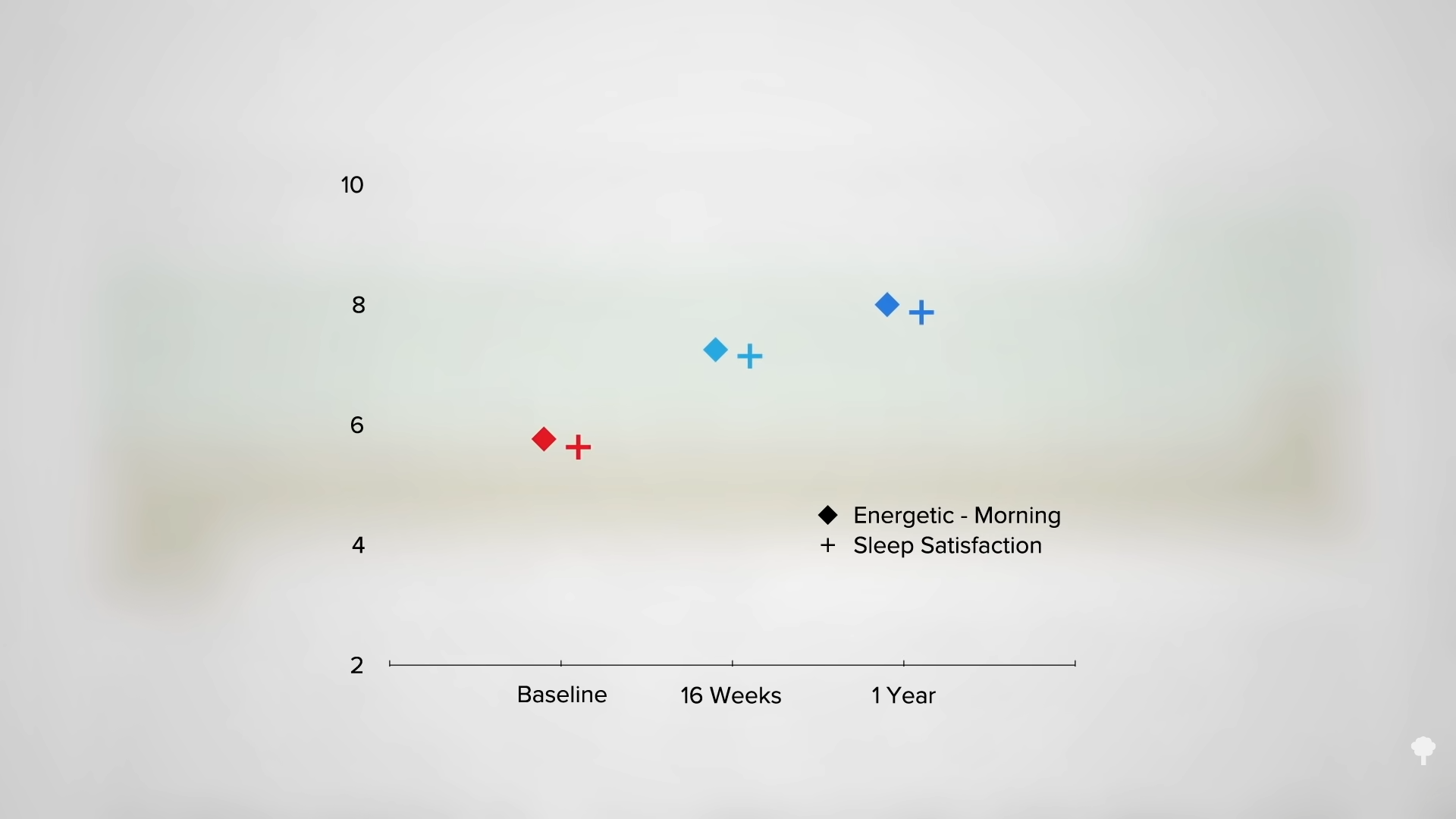
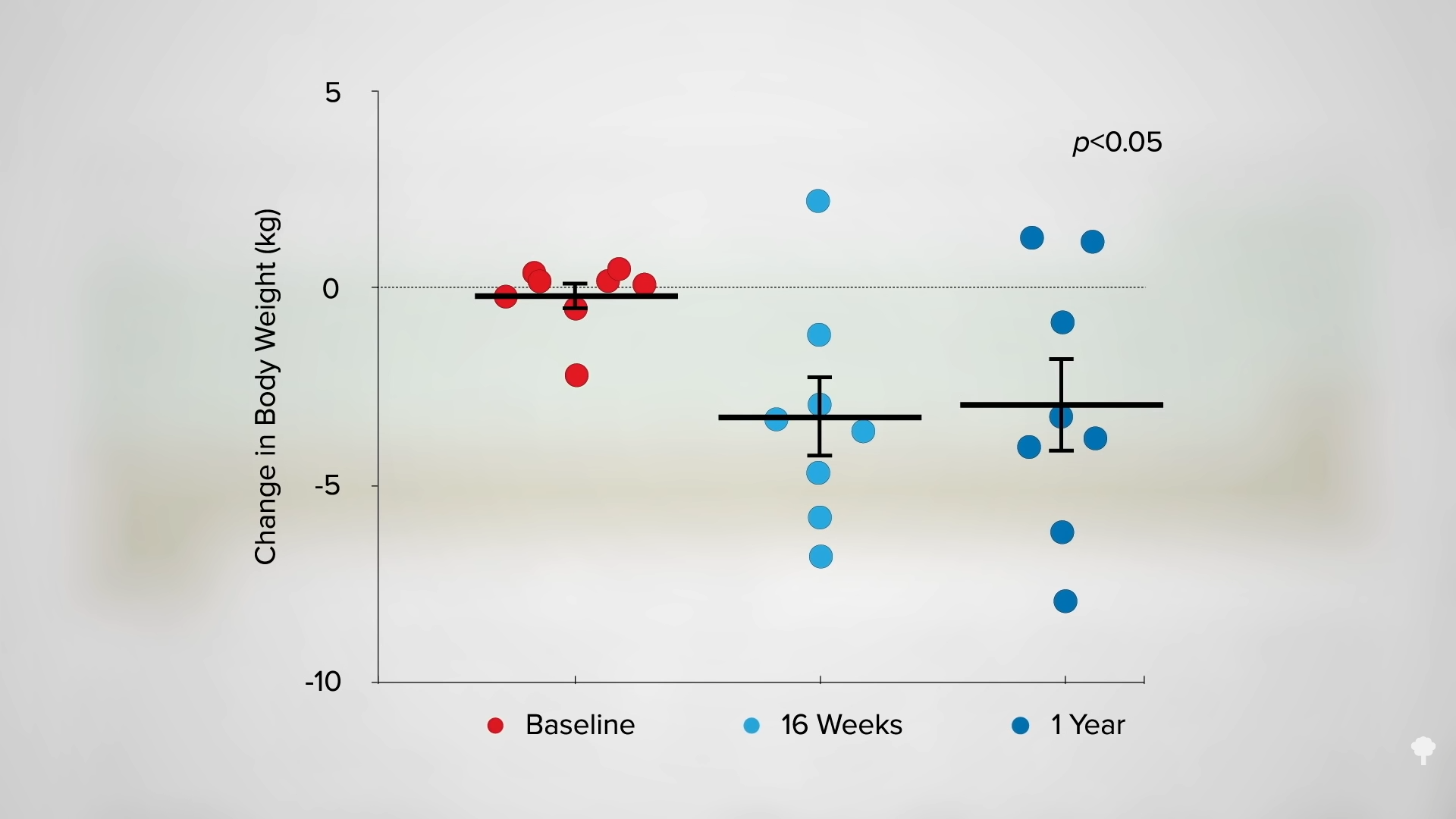
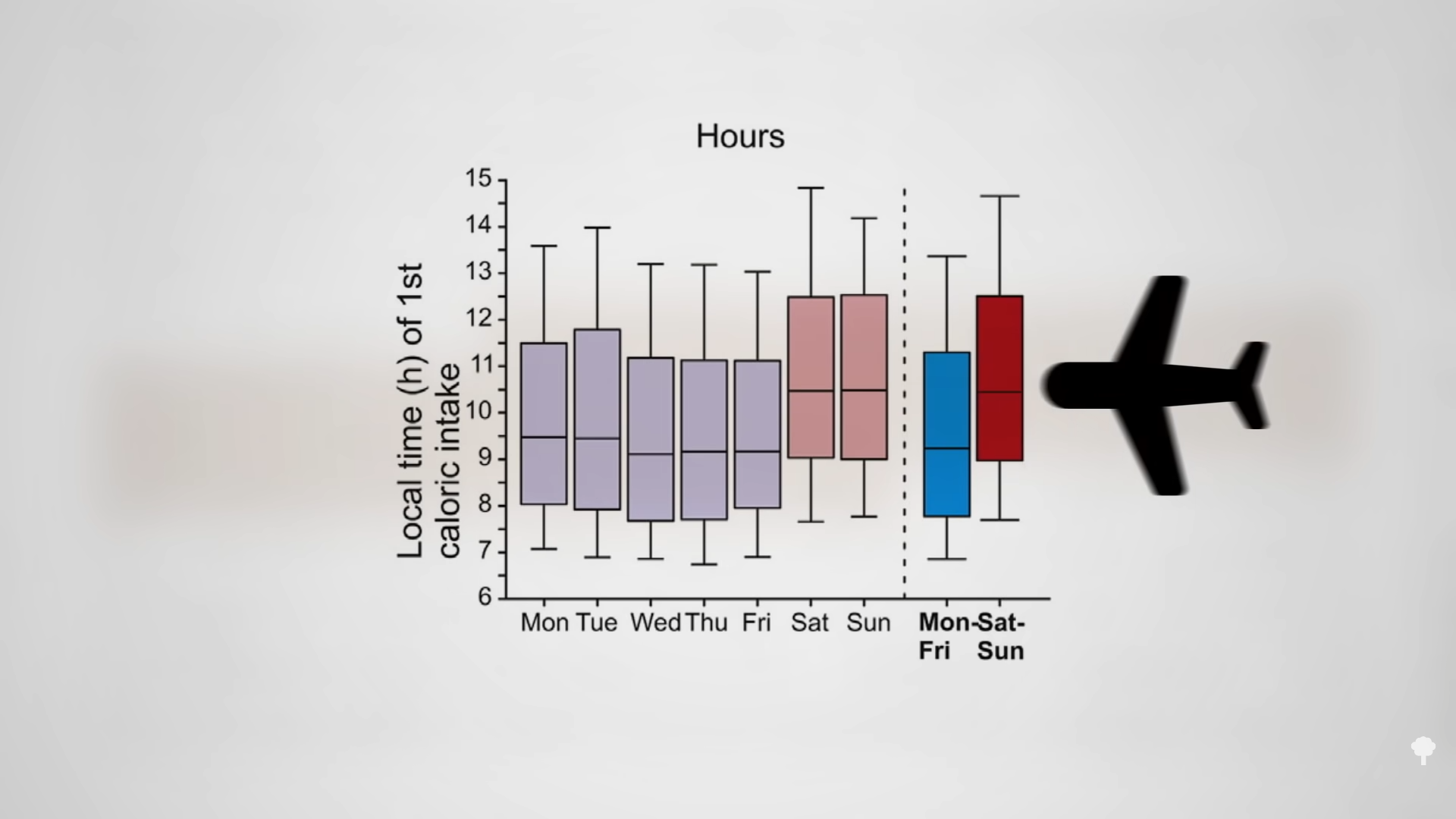
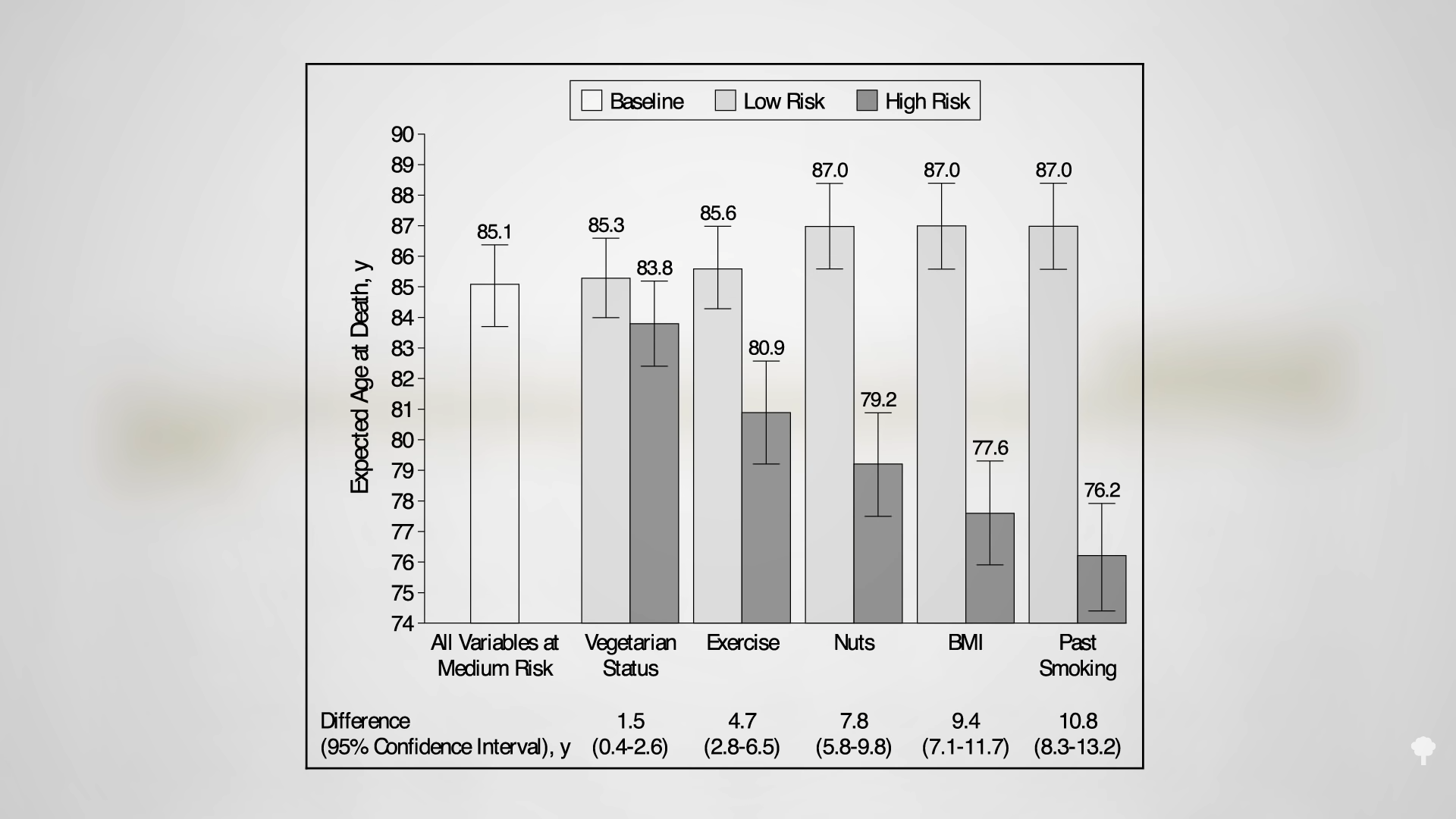
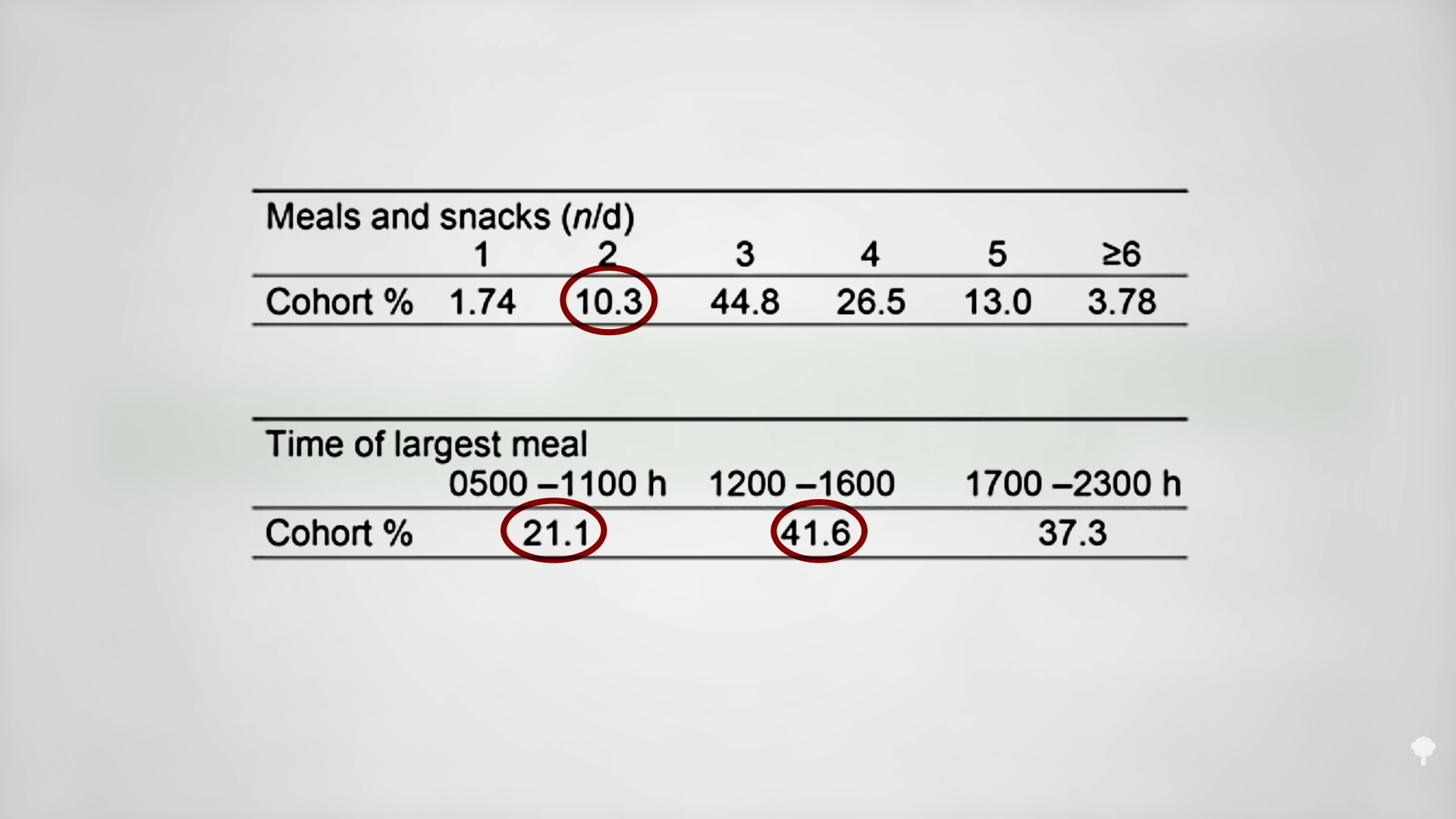

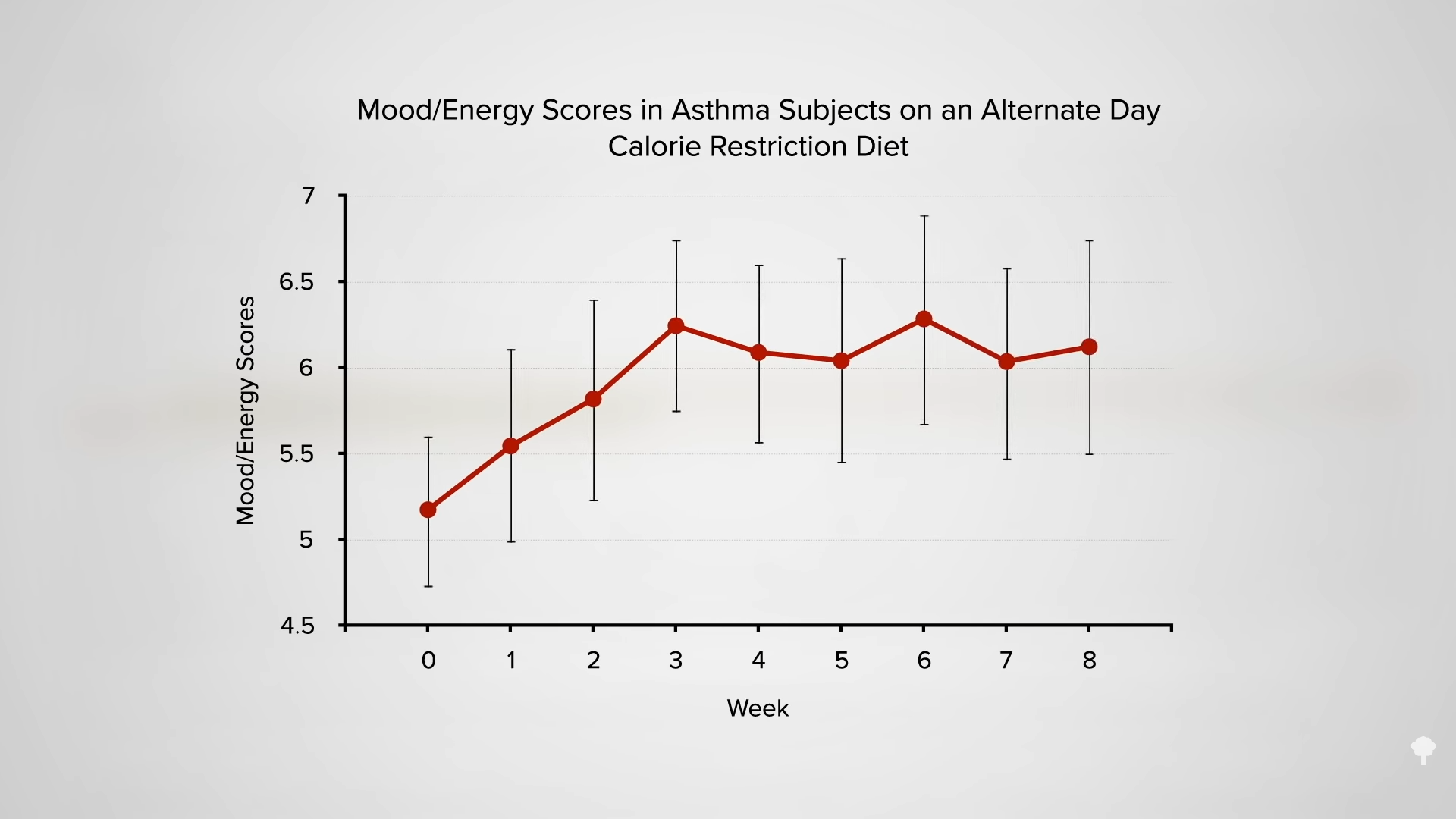
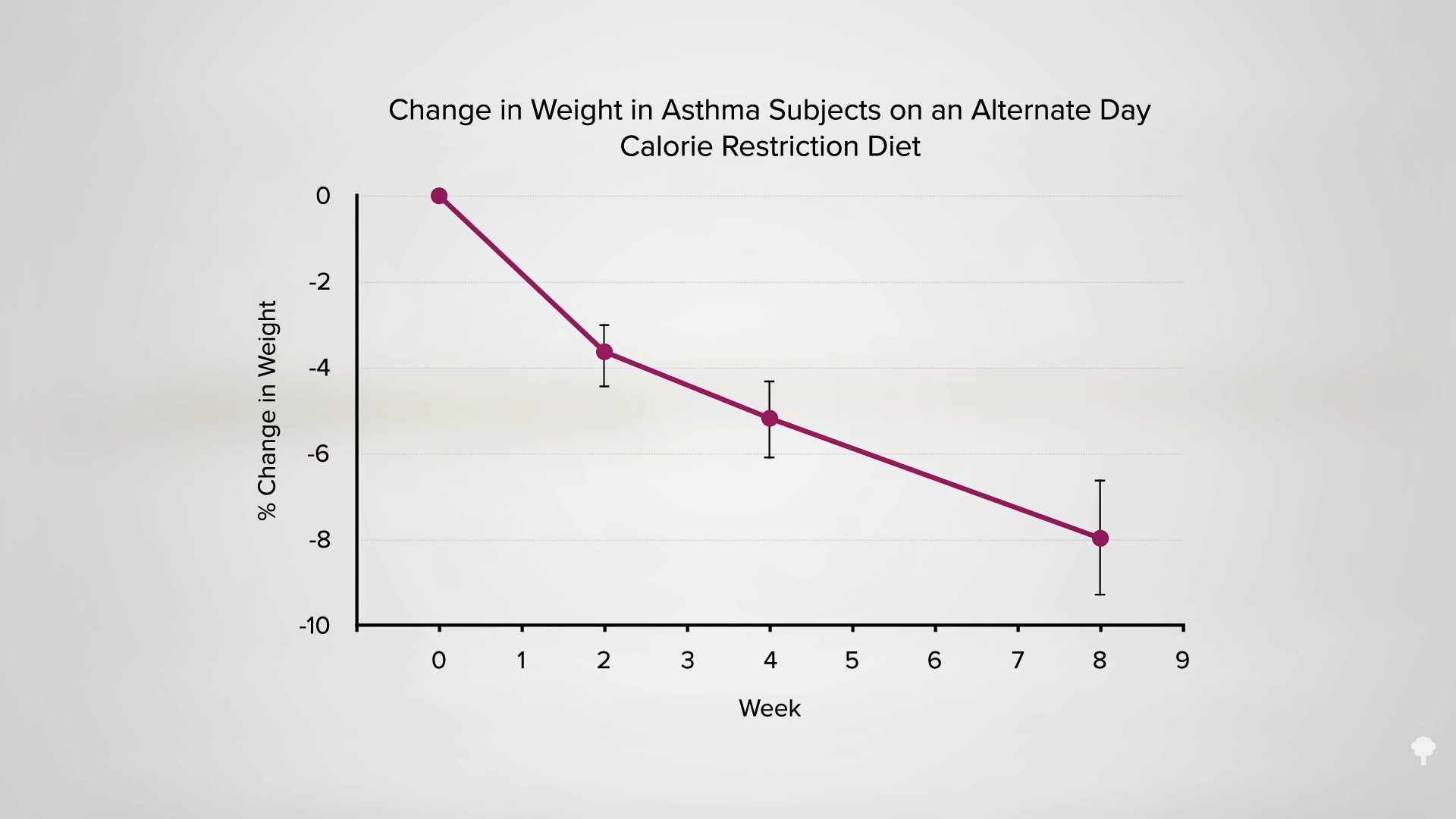
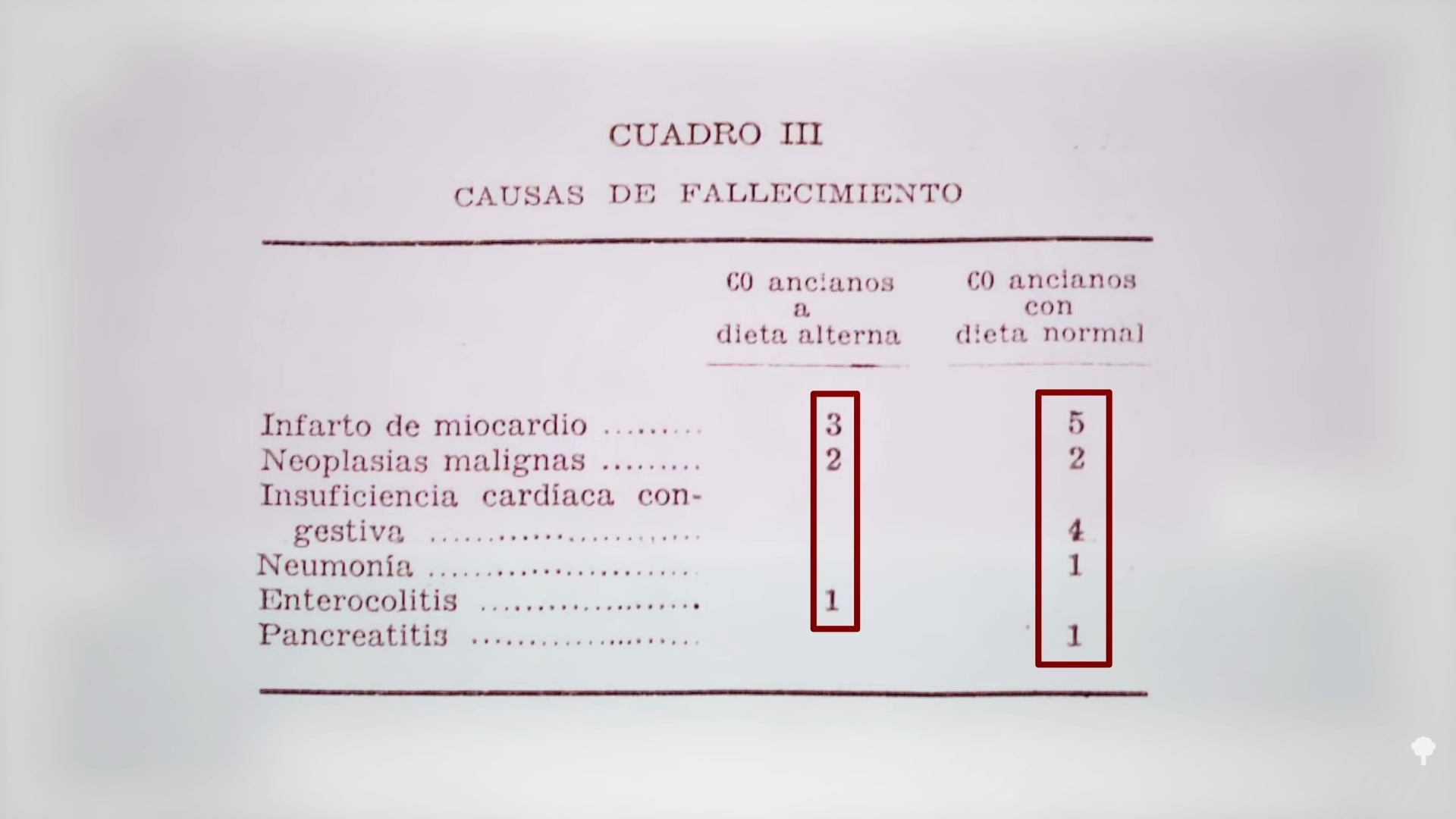
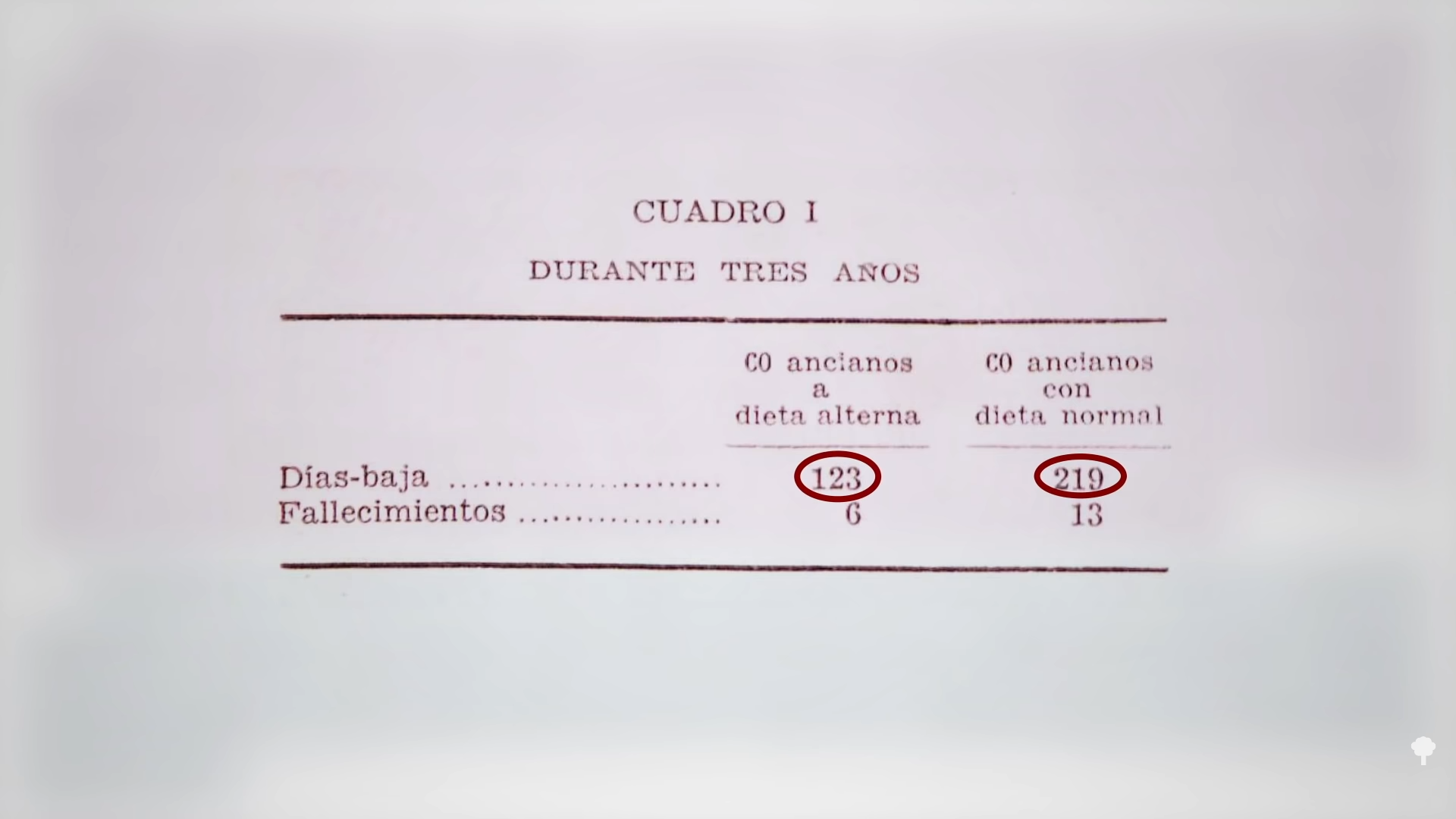

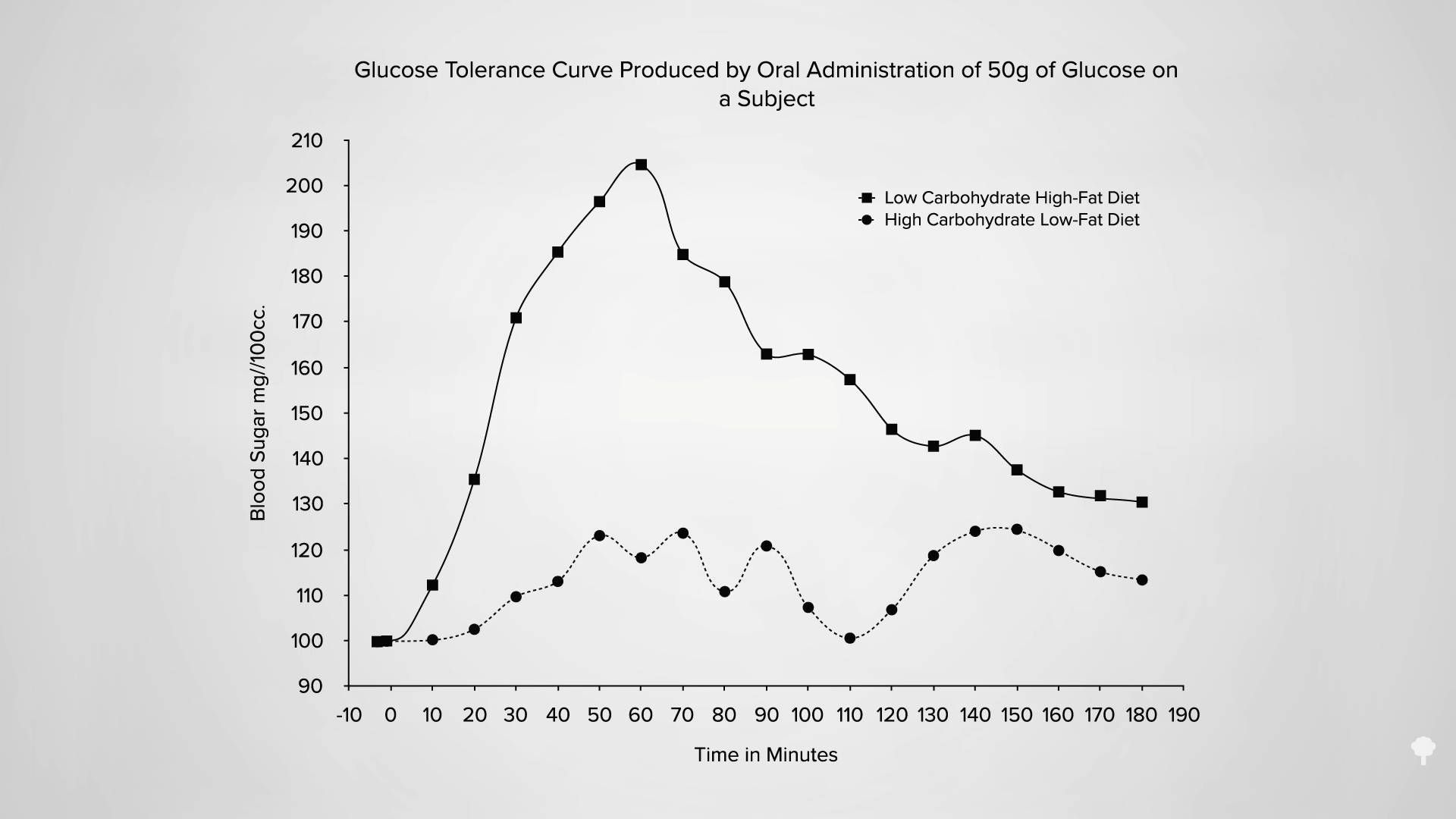
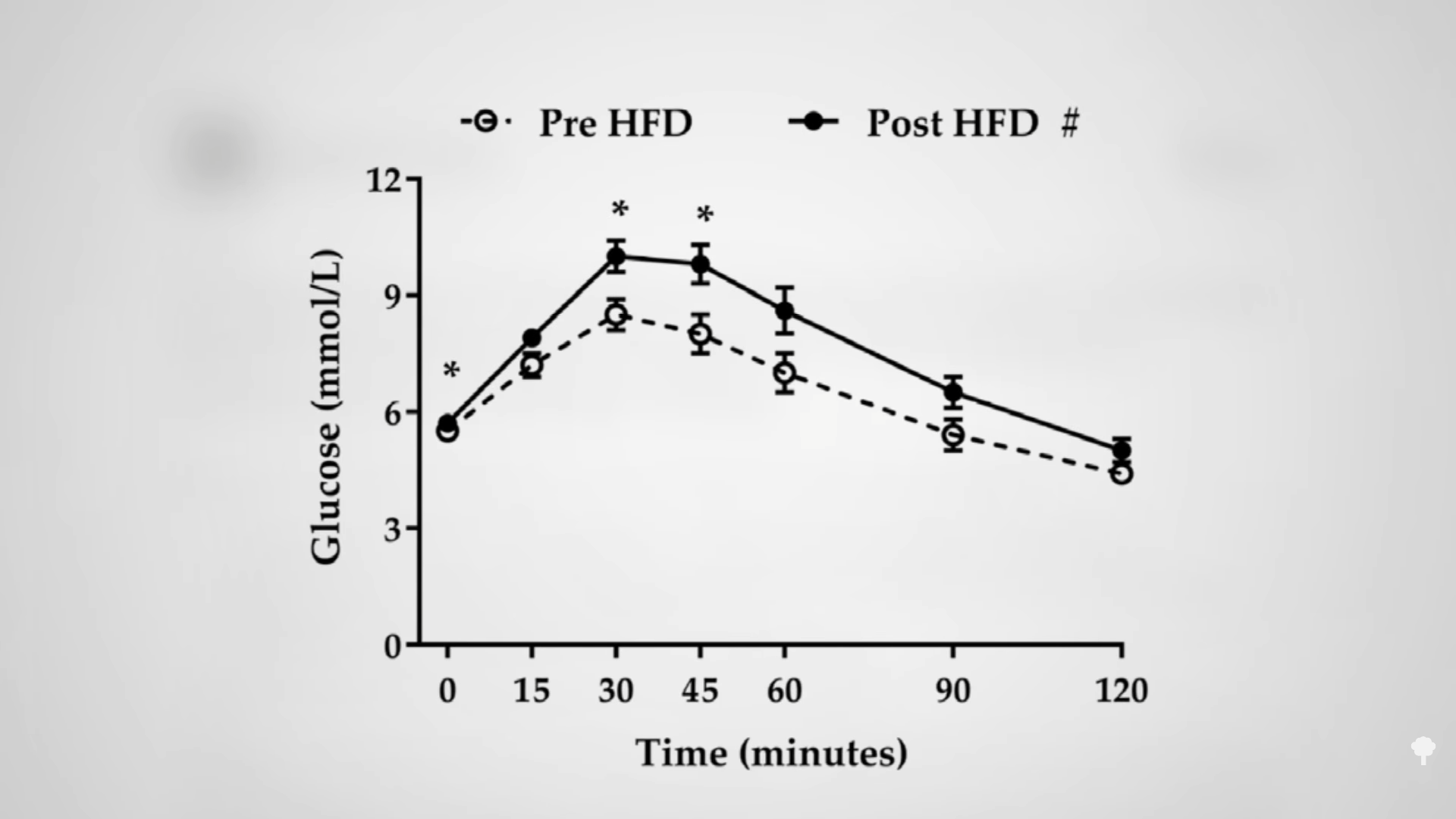
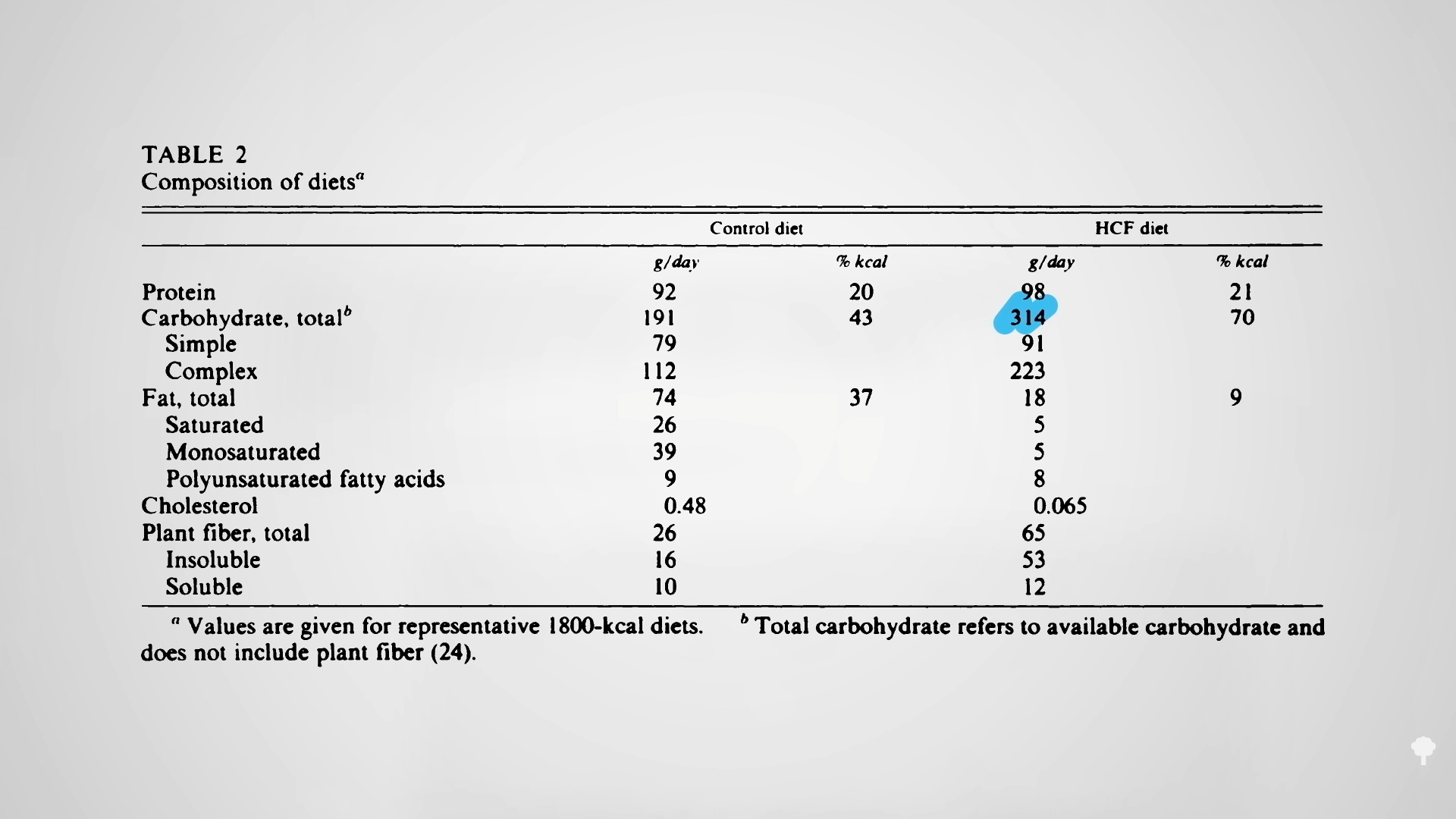 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal