[ad_1]
What are the effects of eating only five days a week or following a fasting-mimicking diet five days a month?
Instead of eating every other day, what if you ate five days a week and fasted for the other two? As I discuss in my video The 5:2 Diet and the Fasting-Mimicking Diet Put to the Test, the available data are similar to that of alternate-day fasting: About a dozen pounds of weight loss was reported in overweight men and also reported in overweight women over six months, with no difference found between participants on the 5:2 intermittent fasting regimen and those on a continuous 500-calories-a-day restriction. The largest trial to date found an 18-pound weight loss within six months in the 5:2 group, which isn’t significantly different from the 20 pounds lost in the continuous calorie restriction group. Weight maintenance over the subsequent six months was also found to be no different.
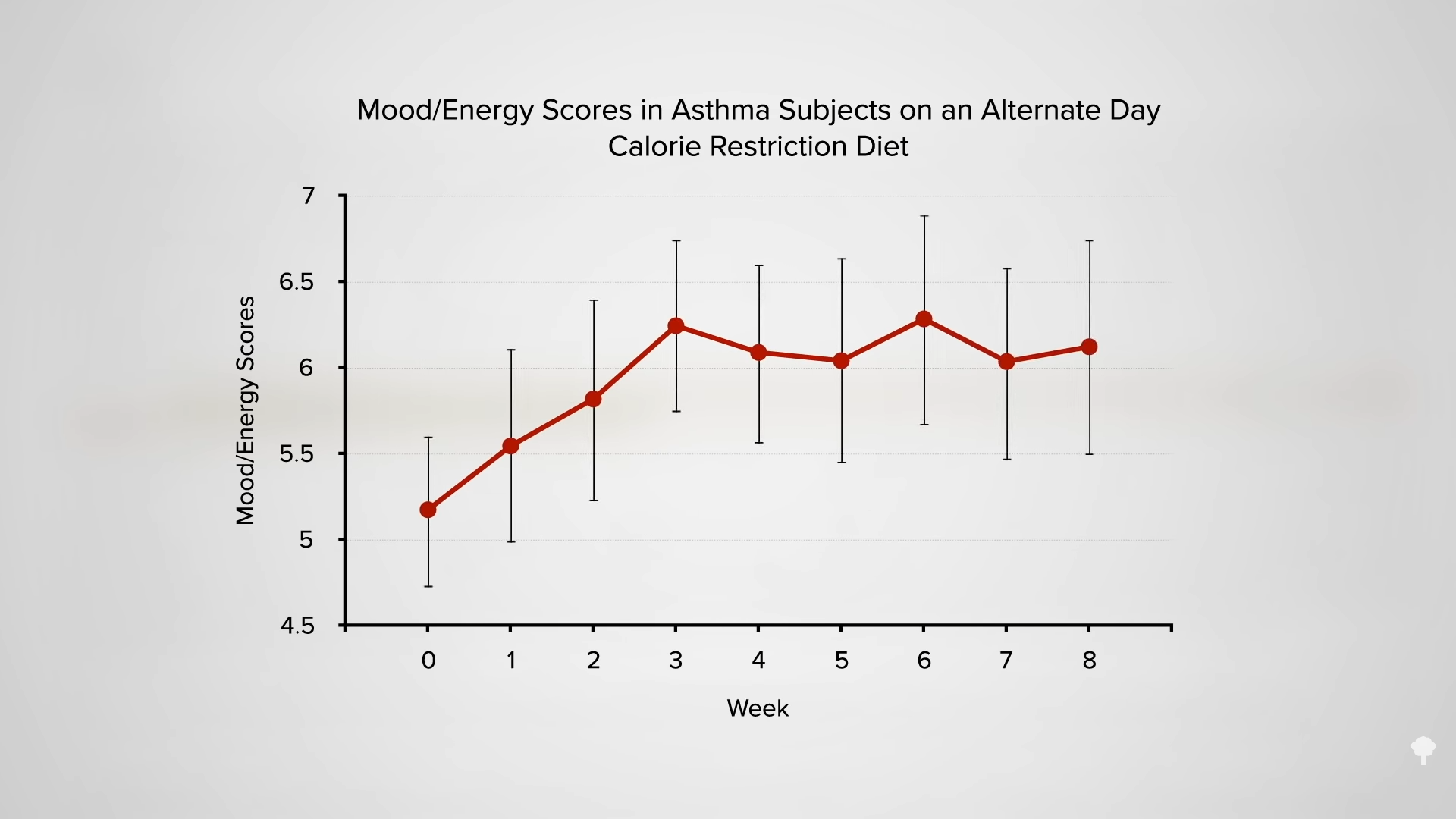
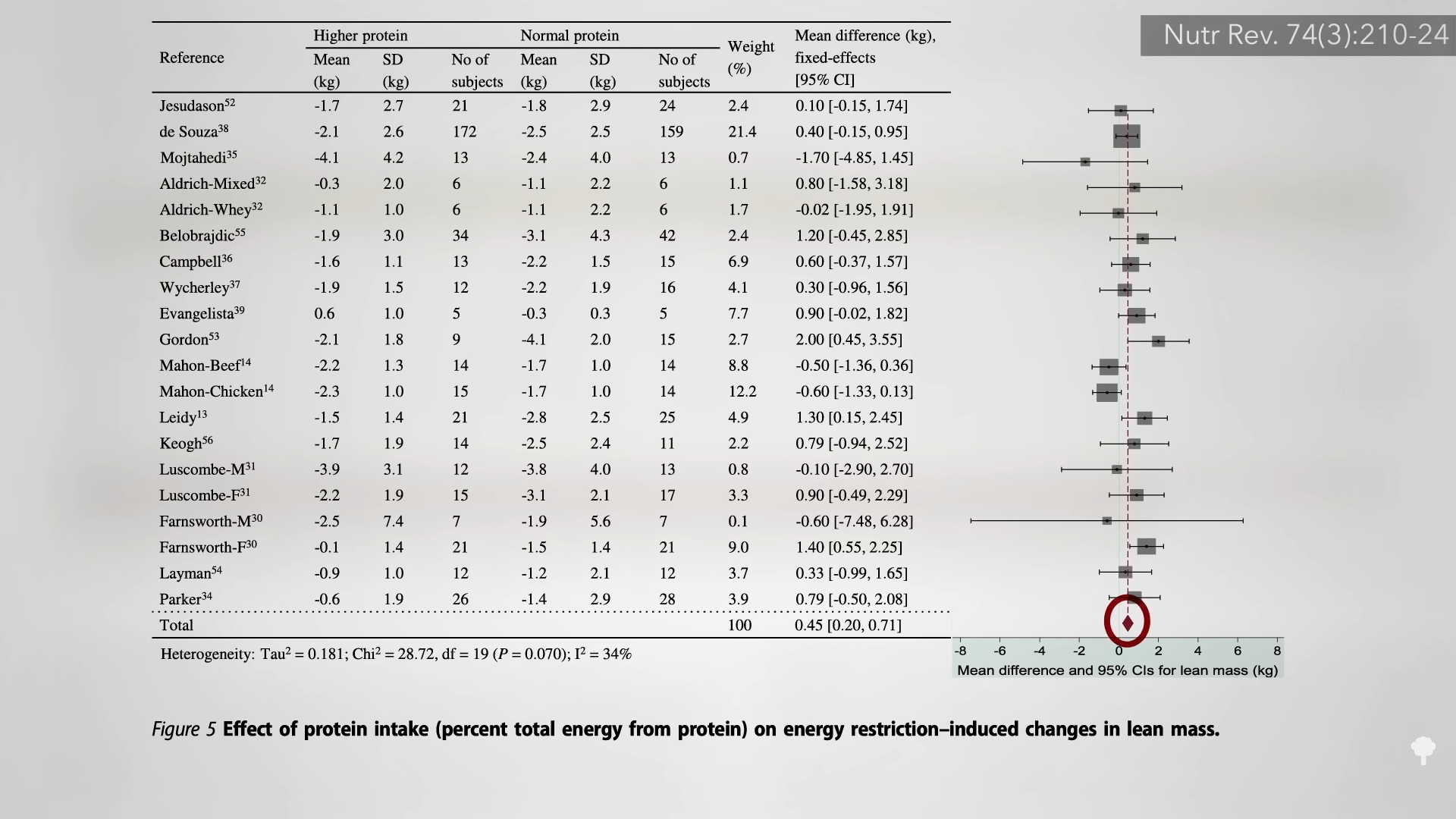
Though feelings of hunger may be more pronounced on the 5:2 pattern than on an equivalent level of daily calorie cutting, it does not seem to lead to overeating on non-fasting days. One might expect going two days without food may negatively impact mood, but no such adverse impact was noted for those fully fasting on zero calories or sticking to just two packets of oatmeal on each of the “fasting” days. (The oatmeal provides about 500 calories a day.) Like alternate-day fasting, the 5:2 fasting pattern appeared to have inconsistent effects on cognition and on preserving lean mass, and it also failed to live up to the “popular notion” that intermittent fasting would be “easier” to adhere to than daily calorie restriction.
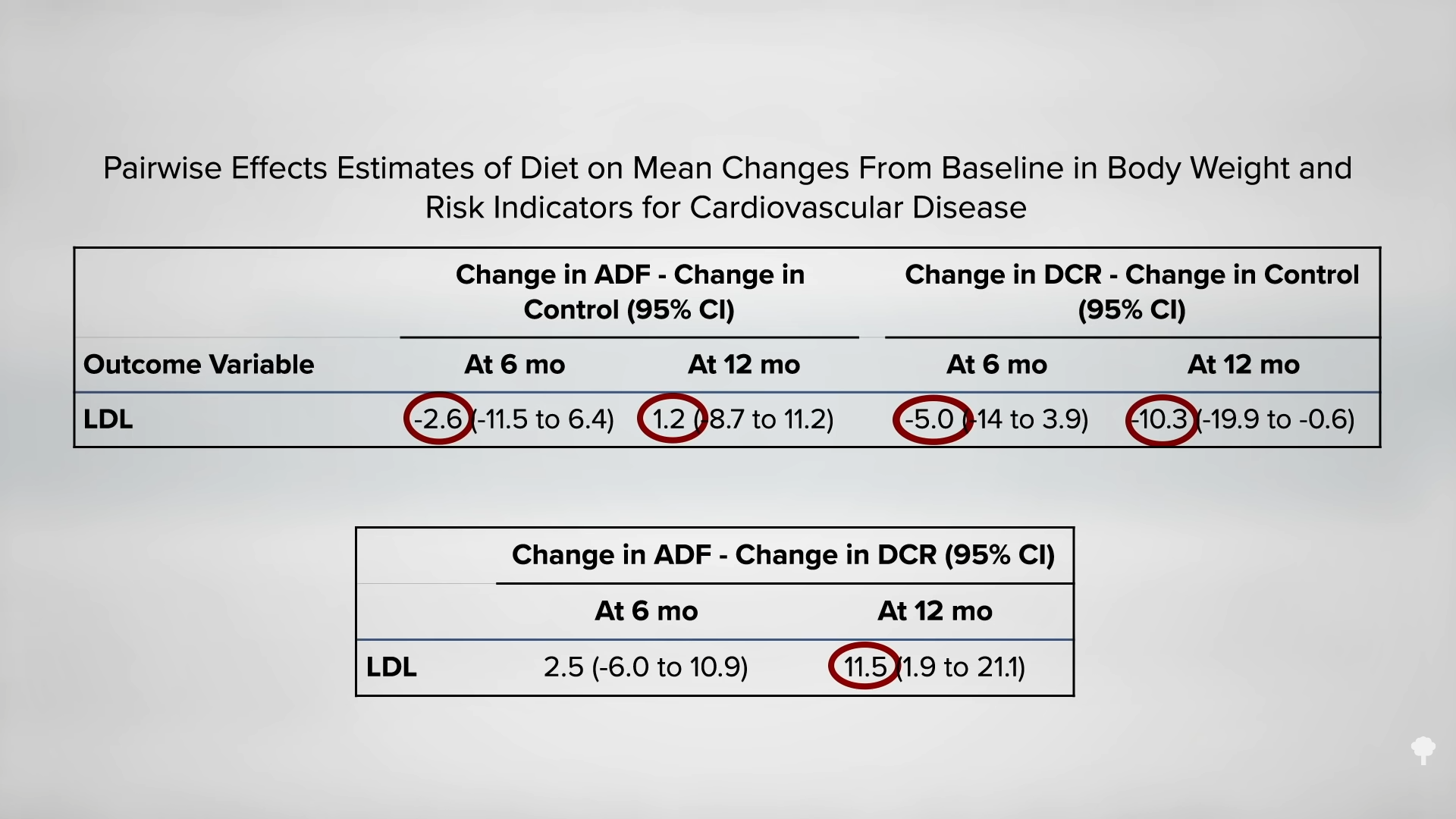
Compared to those in the continuous-restriction control group, fewer subjects in the 5:2 pattern group expressed interest in continuing their diet after the study was over. This was attributed to quality-of-life issues, with 5:2 fasting participants citing headaches, lack of energy, and difficulty fitting the fasting days into their weekly routine. However, as you can see below and at 1:53 in my video, there has yet to be a single 5:2 diet study showing elevated LDL cholesterol compared with continuous calorie restriction at six months. Nor has it been shown for a year. This offers a potential advantage over alternate-day regimens.
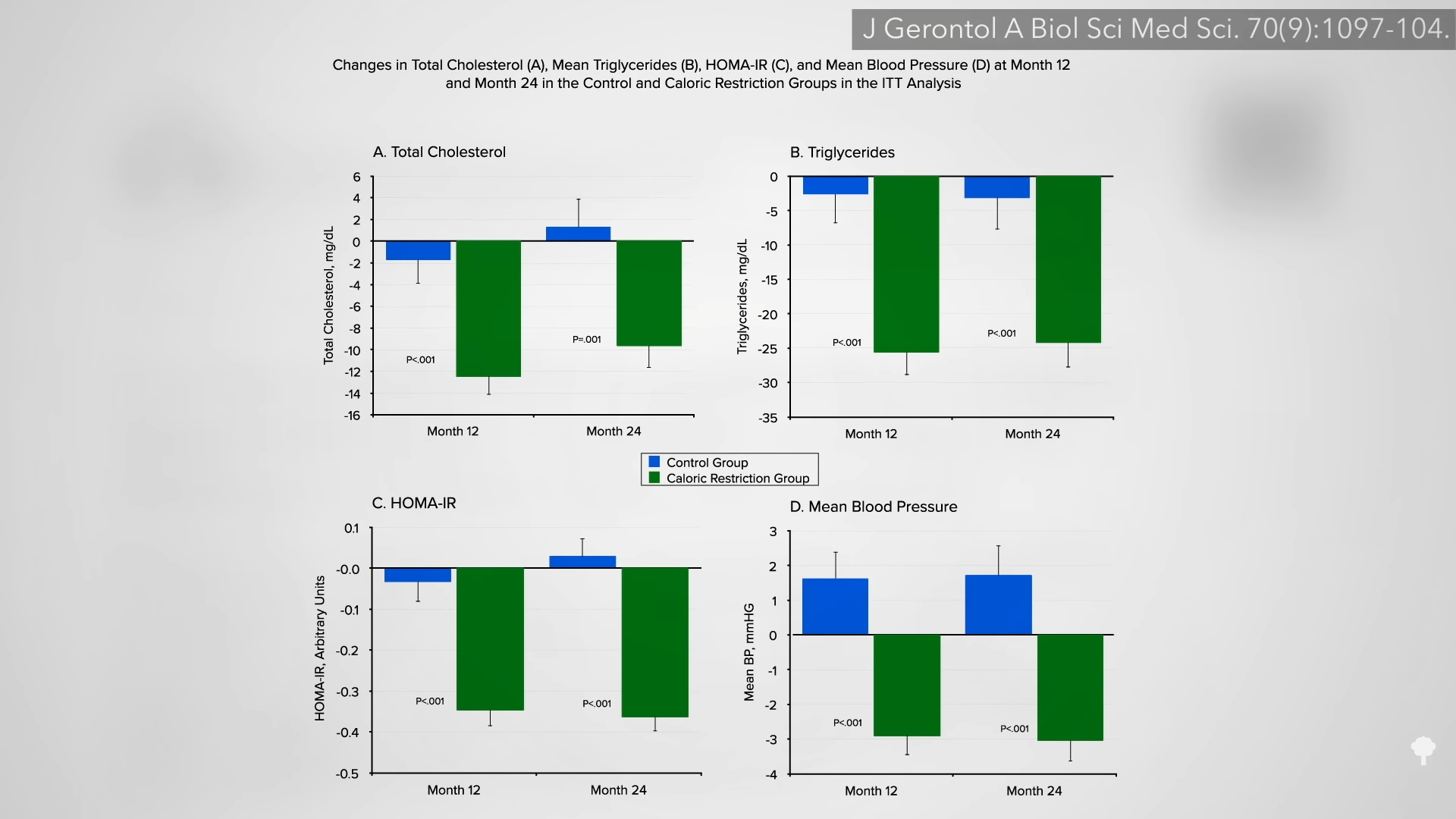
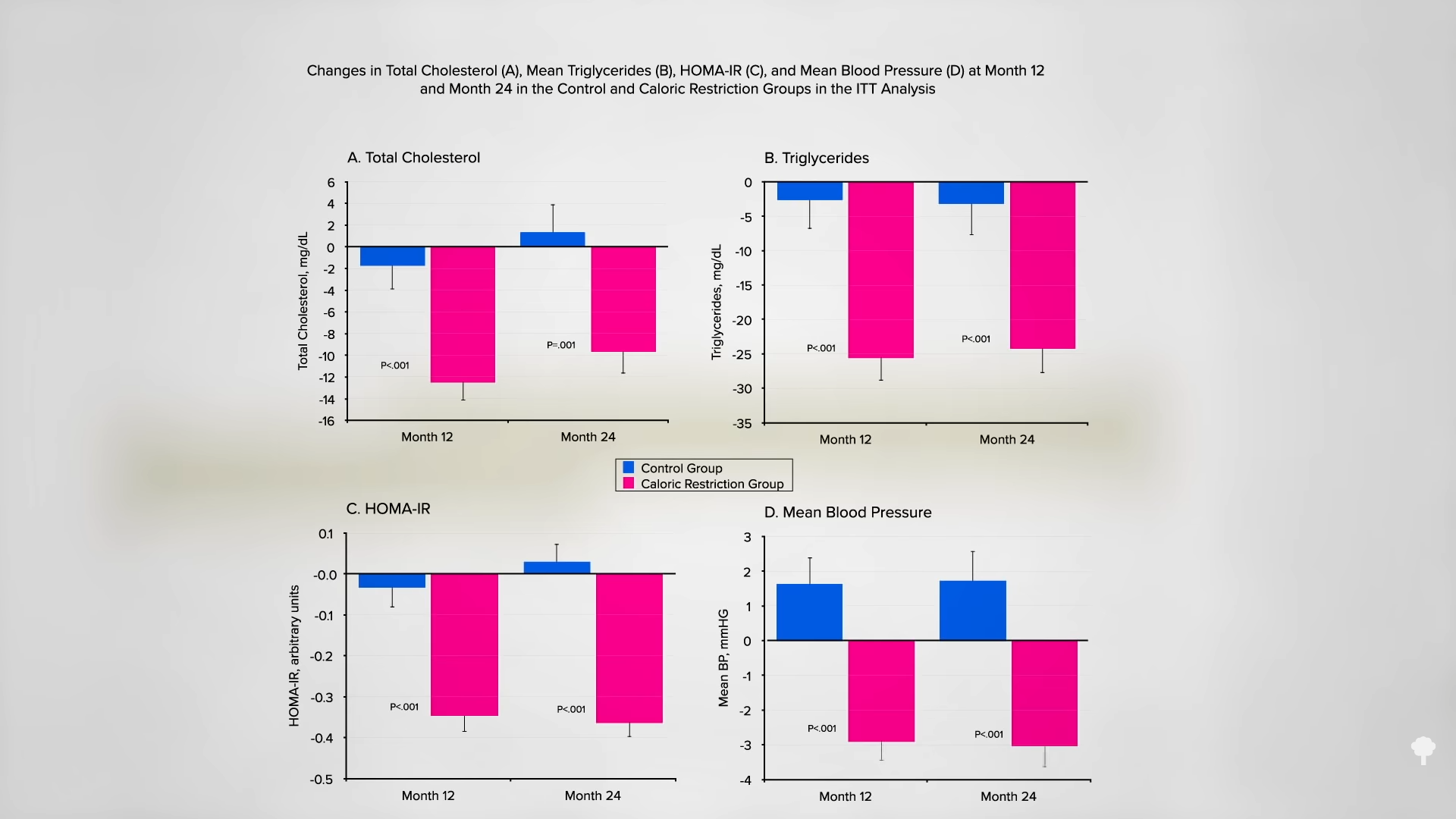
Instead of 5:2, what about 25:5, spending five consecutive days a month on a “fasting-mimicking diet” (FMD)? Longevity researcher Valter Longo designed a five-day meal plan to try to simulate the metabolic effects of fasting by being low in protein, sugars, and calories with zero animal protein and zero animal fat. By making the diet plant-based, he hoped to lower the level of the cancer-promoting growth hormone IGF-1. He indeed accomplished this goal, along with a drop in markers of inflammation, after three cycles of his five-days-a-month program, as you can see below and at 2:33 in my video. 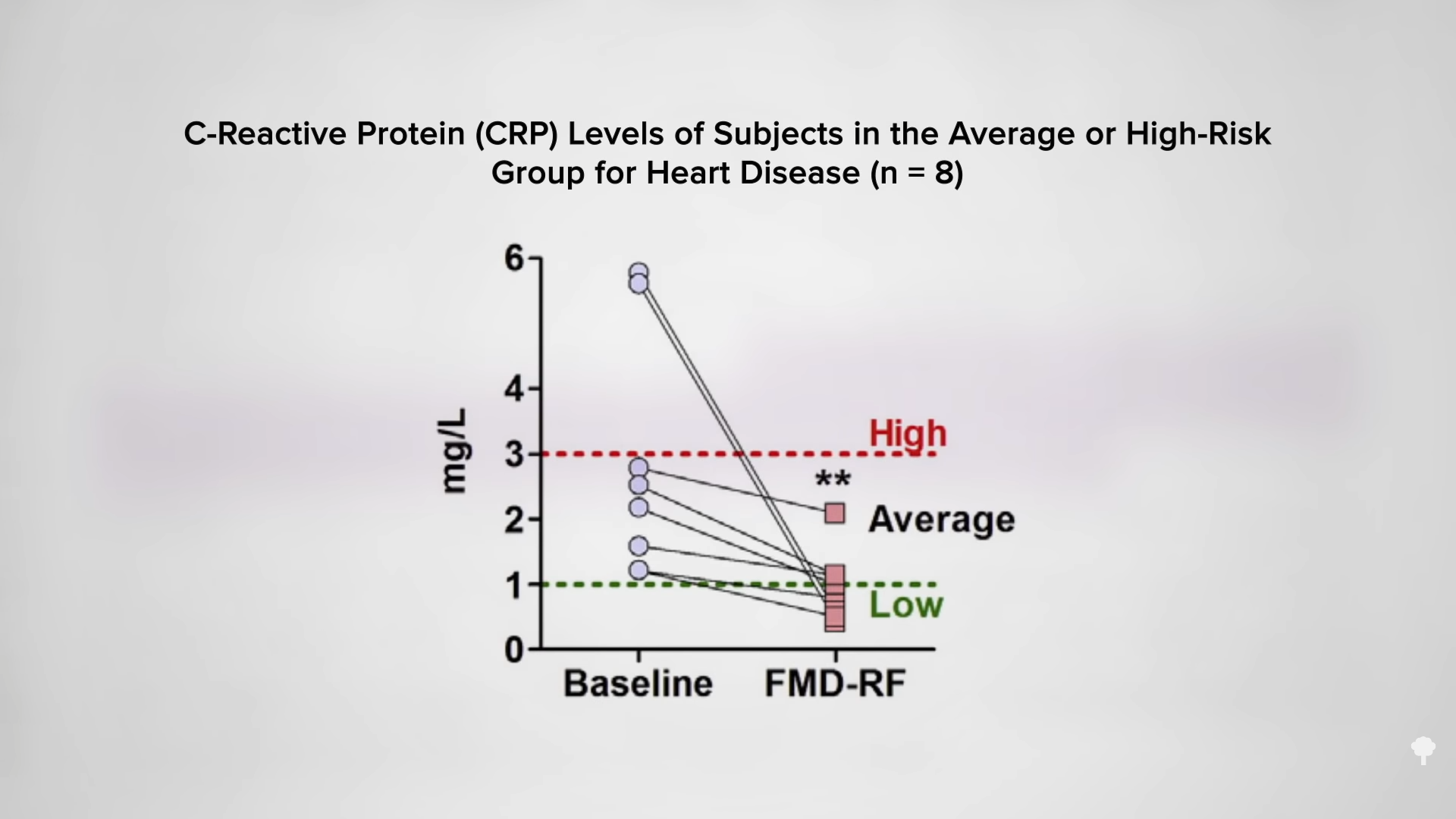
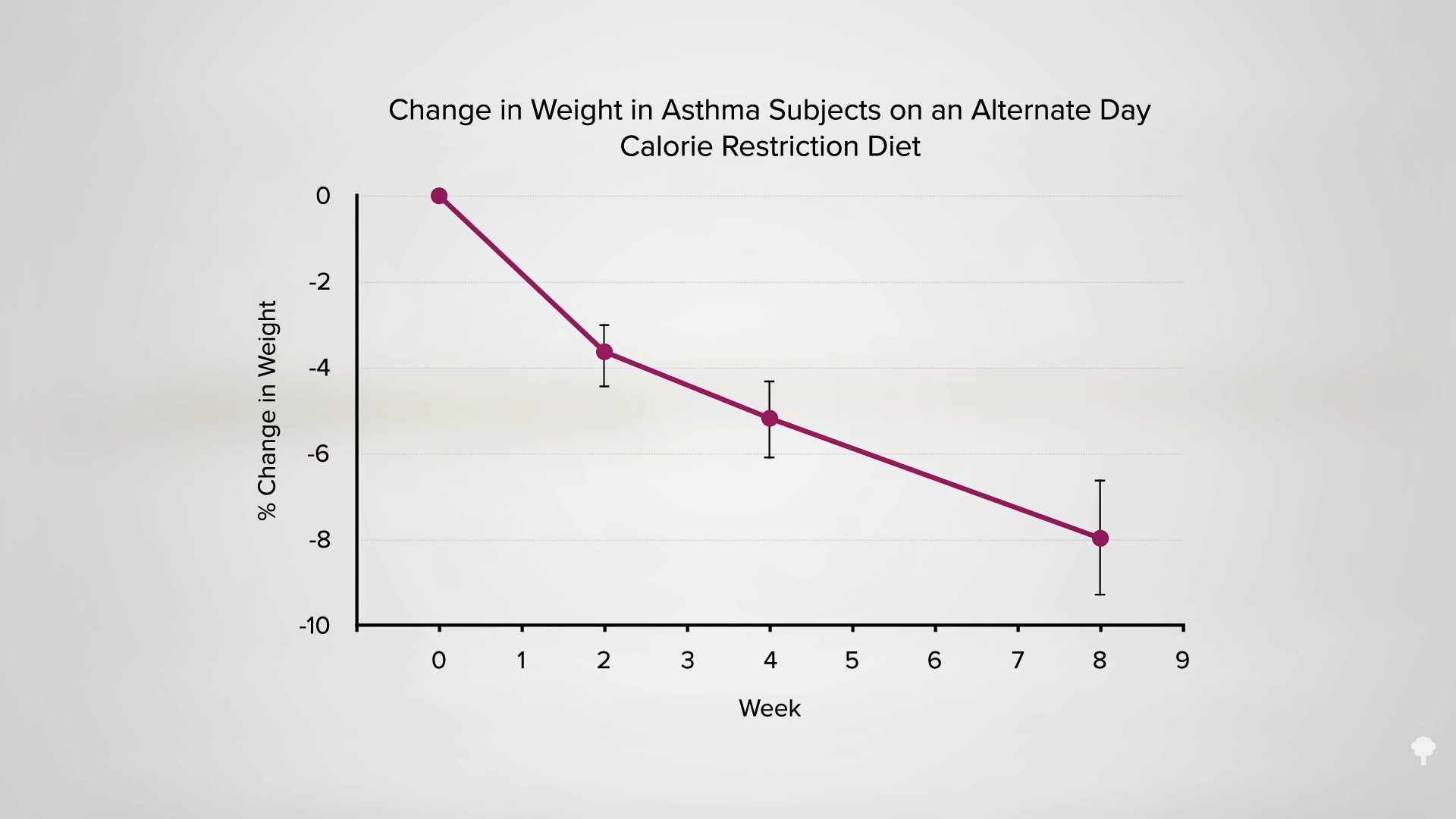
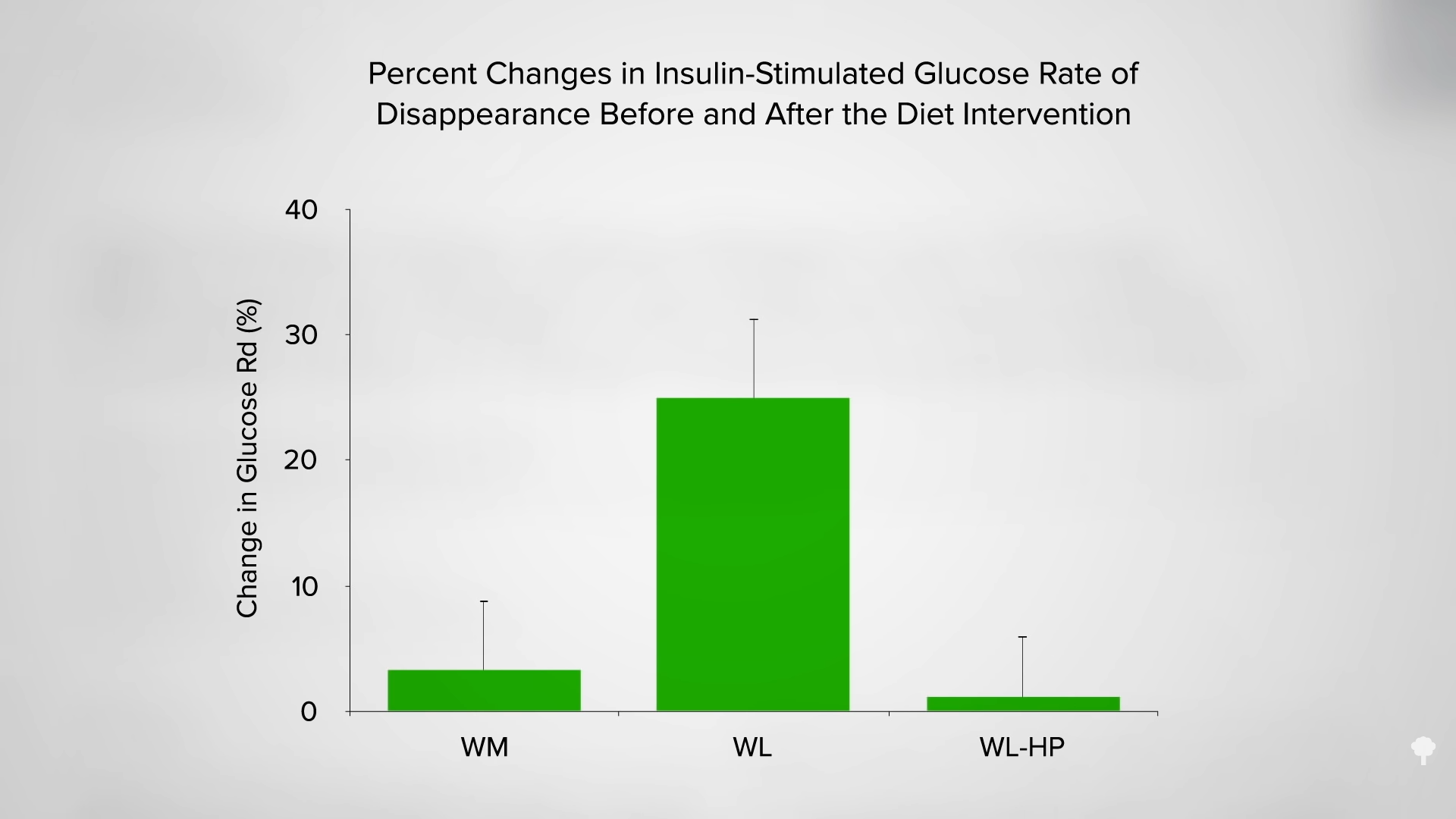
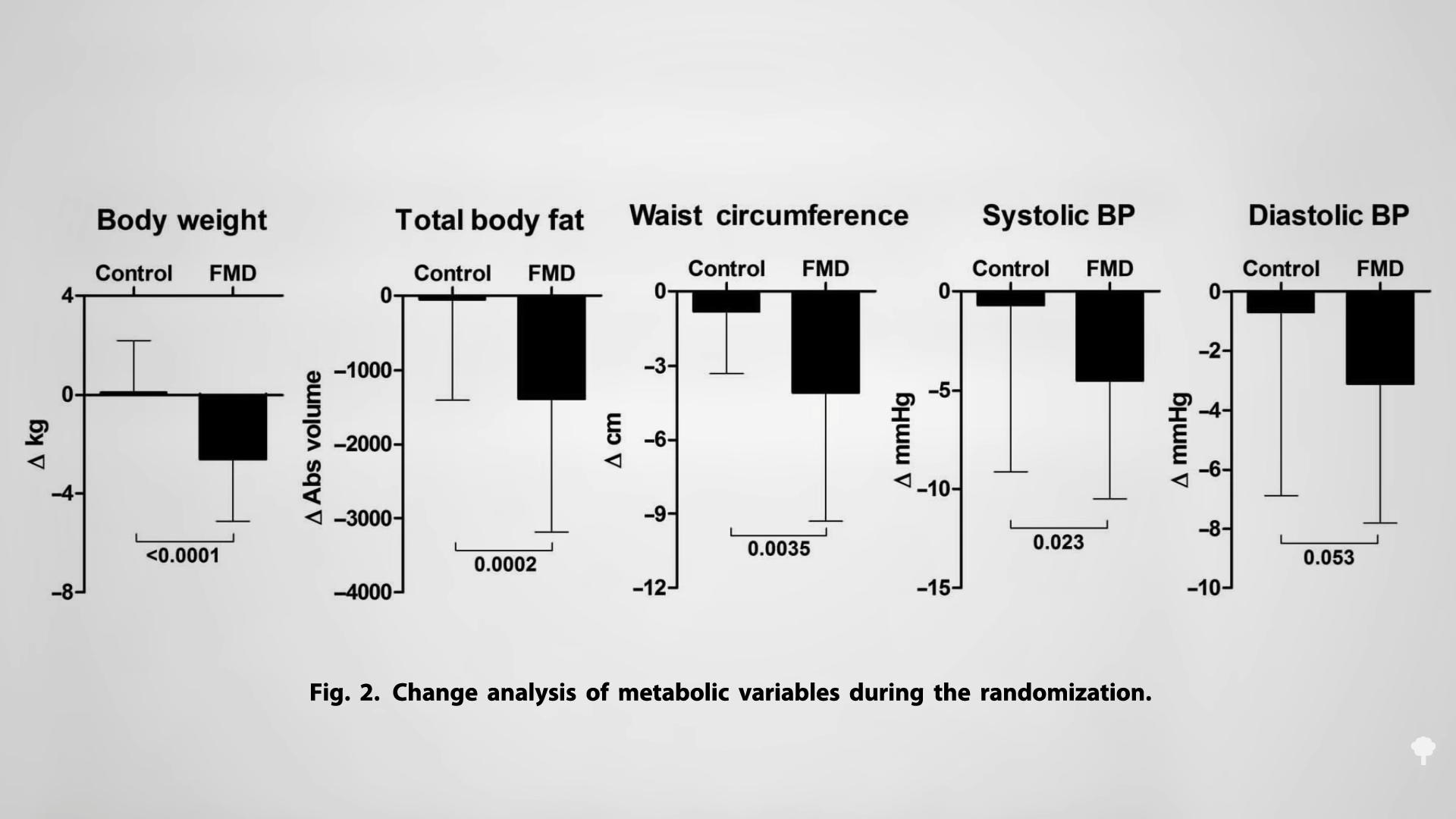
One hundred men and women were randomized to consume his fasting-mimicking diet for five consecutive days per month or maintain their regular diet the whole time. As you can see in the graph below and at 2:47 in my video, after three months, the FMD group was down about six pounds compared to the control group, with significant drops in body fat and waist circumference, accompanied by a drop in blood pressure.
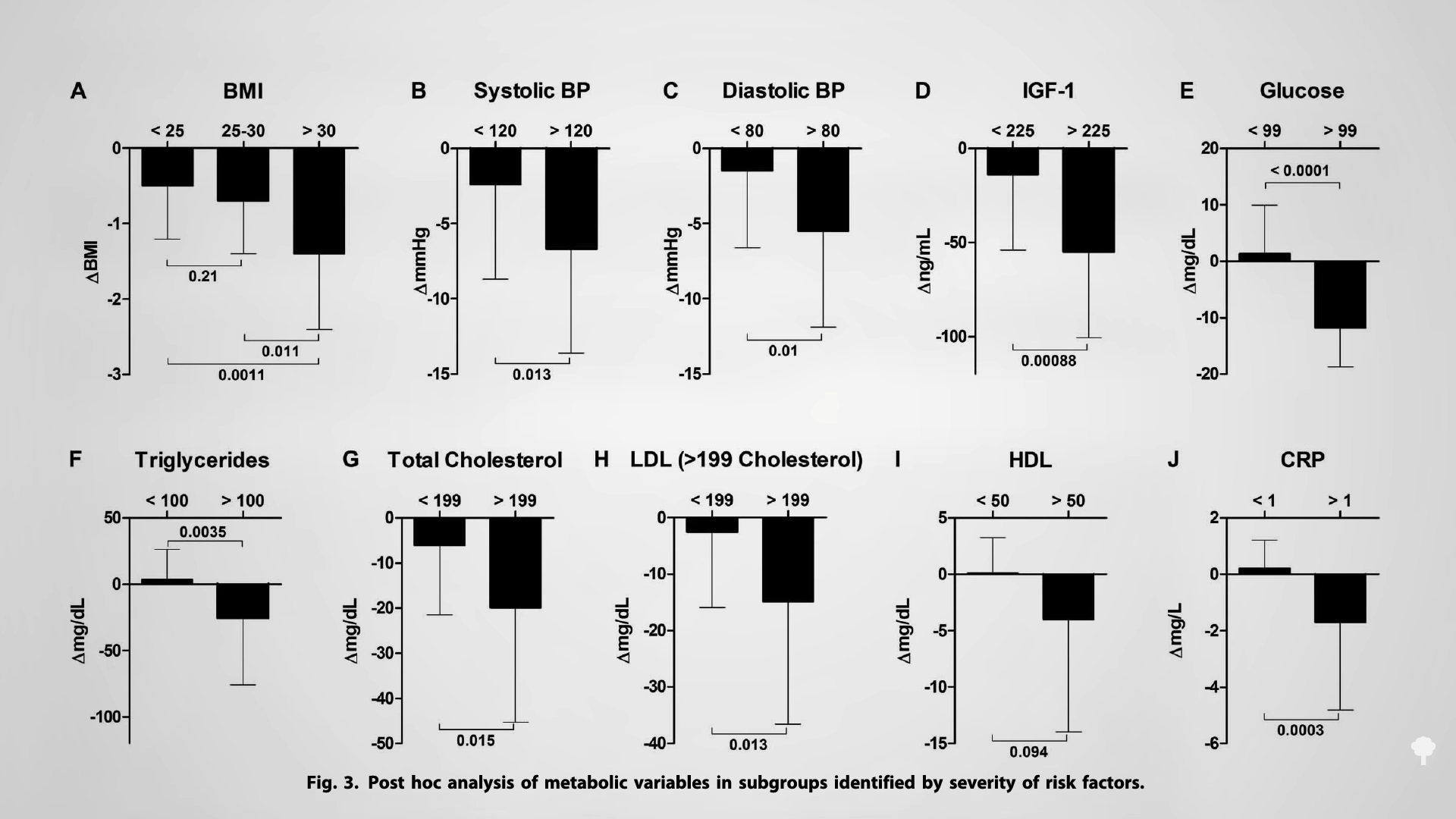
Those who were the worst off accrued the most dramatic benefits, as seen in the graph below and at 3:04 in my video. What’s even wilder is that three further months after completion, some of the benefits appeared to persist, suggesting the effects “may last for several months.” It’s unclear, though, if those randomized to the FMD group used it as an opportunity to make positive lifestyle changes that helped maintain some of the weight loss.
Dr. Longo created a company to market his meal plan commercially, but, to his credit, says “he does not receive a salary or a consulting fee from the company…and will donate 100% of his shares to charity.” The whole diet appears to be mostly dehydrated soup mixes, herbal teas like hibiscus and chamomile, kale chips, nut-based energy bars, an algae-based DHA supplement, and a multivitamin dusted with vegetable powder. Why spend 50 dollars a day on a few processed snacks when you could instead eat a few hundred calories a day of real vegetables?
How interesting was that? All-you-can-eat above-ground vegetables for five days would have the same low amount of protein, sugars, and calories with zero animal protein or animal fat. But we’ll probably never know if it works as well, better, or worse because it’s hard to imagine such a study ever getting done without the financial incentive.
To learn more about IGF-1, see my video Flashback Friday: Animal Protein Compared to Cigarette Smoking.
In this series on fasting, I’ve covered several topics, including the basics of calories and weight loss, water-only fasting, and the types of alternate-day fasting, see them all in the related videos below.
I close out the series with videos on time-restricted eating: Time-Restricted Eating Put to the Test and The Benefits of Early Time-Restricted Eating.
If you want all of the videos in one place, I’ve done three webinars on fasting—Intermittent Fasting, Fasting for Disease Reversal, and Fasting and Cancer—and they’re all available for download now.
[ad_2]
Michael Greger M.D. FACLM
Source link