[ad_1]
What is the best type of pots and pans to use?
In my last video, I expressed concerns about the use of aluminum cookware. So, what’s the best type of pots and pans to use? As I discuss in my video Stainless Steel or Cast Iron: Which Cookware Is Best? Is Teflon Safe?, stainless steel is an excellent option. It’s the metal chosen for use “in applications where safety and hygiene are considered to be of the utmost importance, such as kitchenware.” But what about studies showing that the nickel and chromium in stainless steel, which keeps the iron in stainless unstained by rust, can leach into foods during cooking? The leaching only seems to occur when the cookware is brand new. “Metal leaching decreases with sequential cooking cycles and stabilizes after the sixth cooking cycle,” after the sixth time you cook with it. Under more common day-to-day conditions, the use of stainless steel pots is considered to be safe even for most people who are acutely sensitive to those metals.
A little leaching metal can even be a good thing in the case of straight iron, like a cast iron skillet, which can have the “beneficial effect” of helping to improve iron status and potentially reduce the incidence of iron deficiency anemia among children and women of reproductive age. The only caveat is that you don’t want to fry in cast iron. Frying isn’t healthy regardless of cookware type, but, at hot temperatures, vegetable oil can react with the iron to create trans fats.
What about using nonstick pans? Teflon, also known as polytetrafluoroethylene (PTFE), “is used as an inner coating material in nonstick cookware.” Teflon’s dark history was the subject of a 2019 movie called Dark Waters, starring Mark Ruffalo and Anne Hathaway. Employees in DuPont’s Teflon division started giving birth to babies with deformities before “DuPont removed all female staff” from the unit. Of course, the corporation buried it all, hiding it from regulators and the public. “Despite this significant history of industry knowledge” about how toxic some of the chemicals used to make Teflon were, it was able to keep it hidden until, eventually, it was forced to settle for more than half a billion dollars after one of the chemicals was linked to “kidney and testicular cancers, pregnancy-induced hypertension, ulcerative colitis, and high cholesterol.”
“At normal cooking temperatures, PTFE-coated cookware releases various gases and chemicals that present mild to severe toxicity.” As you can see below and at 2:38 in my video, different gases are released at different temperatures, and their toxic effects have been documented.
You’ve heard of “canaries in the coal mine”? This is more like “canaries in the kitchen, as cooking with Teflon cookware is well known to kill pet birds,” and Teflon-coated heat lamp bulbs can wipe out half a flock of chickens.
“Apart from the gases released during heating the cooking pans, the coating itself starts damaging after a certain period. It is normally advised to use slow heating when cooking in Teflon-coated pans,” but you can imagine how consumers might ignore that. And, if you aren’t careful, some of the Teflon can start chipping off and make its way into the food, though the effects of ingestion are unknown.
I could find only one study that looks at the potential human health effects of cooking with nonstick pots and pans. Researchers found that the use of nonstick cookware was associated with about a 50 percent increased risk of colorectal cancer, but that may be because of what they were cooking. “Non-stick cookware is used in hazardous cooking methods (i.e. broiling, frying, grilling or barbecuing) at high temperatures mainly for meat, poultry or fish,” in which carcinogenic heterocyclic amines (HCA) are formed from the animal protein. Then, the animal fat can produce another class of carcinogens called polycyclic aromatic hydrocarbons (PAH). Though it’s possible it was the Teflon itself, which contains suspected carcinogens like that C8 compound from the movie Dark Waters, also known as PFOA, perfluorooctanoic acid.
“Due to toxicity concerns, PFOA has been replaced with other chemicals such as GenX, but these new alternatives are also suspected to have similar toxicity.” We’ve already so contaminated the Earth with it, though, that we can get it prepackaged in food before it’s even cooked, particularly in dairy products, fish, and other meat; now, “meat is the main source of human exposure” to these toxic pollutants. Of those, seafood is the worst. In a study of diets from around the world, fish and other seafood were “major contributors” of the perfluoroalkyl substances, as expected, given that everything eventually flows into the sea. Though the aquatic food chain is the “primary transfer mechanism” for these toxins into the human diet, “food stored or prepared in greaseproof packaging materials,” like microwave popcorn, may also be a source.
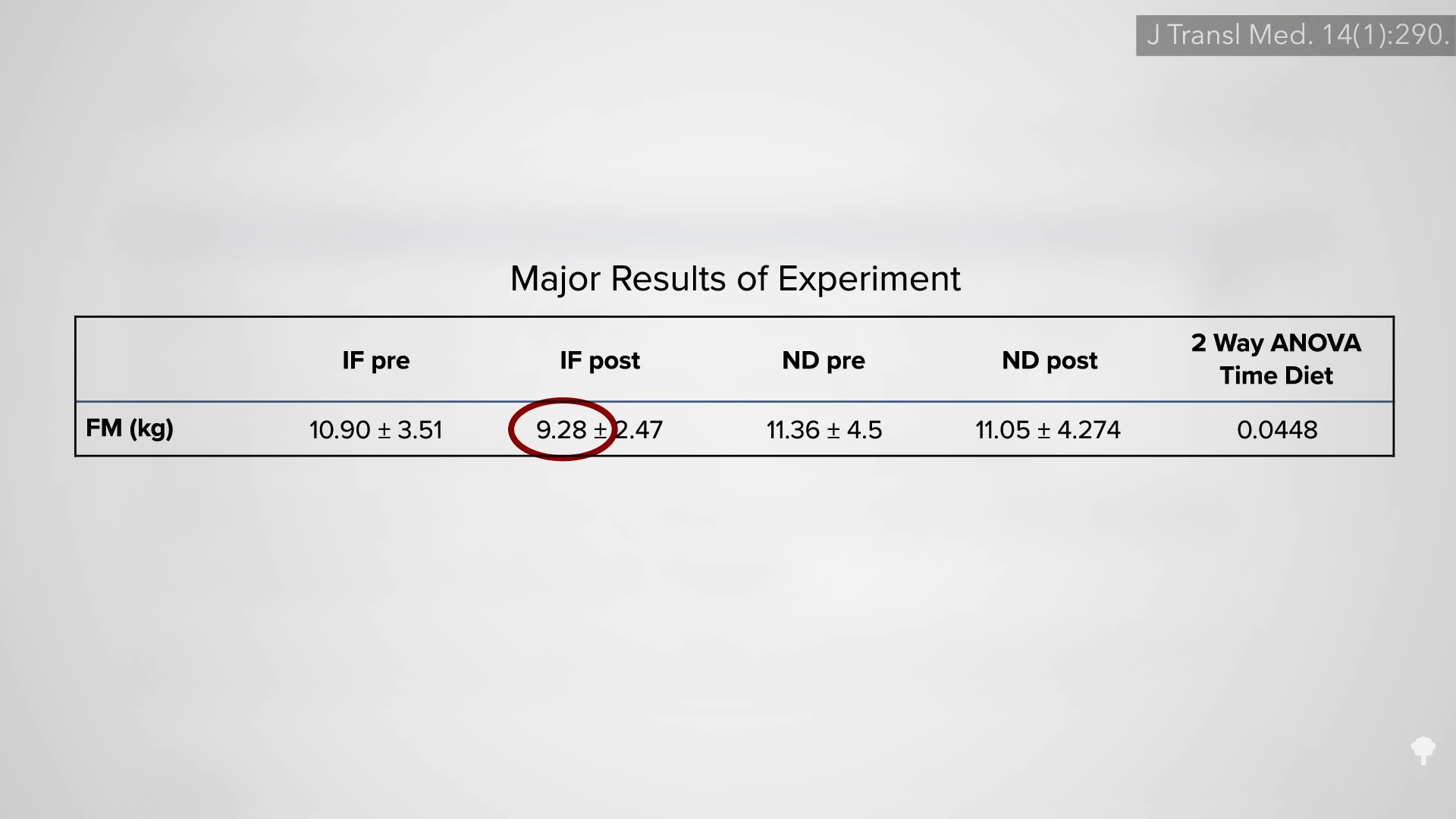
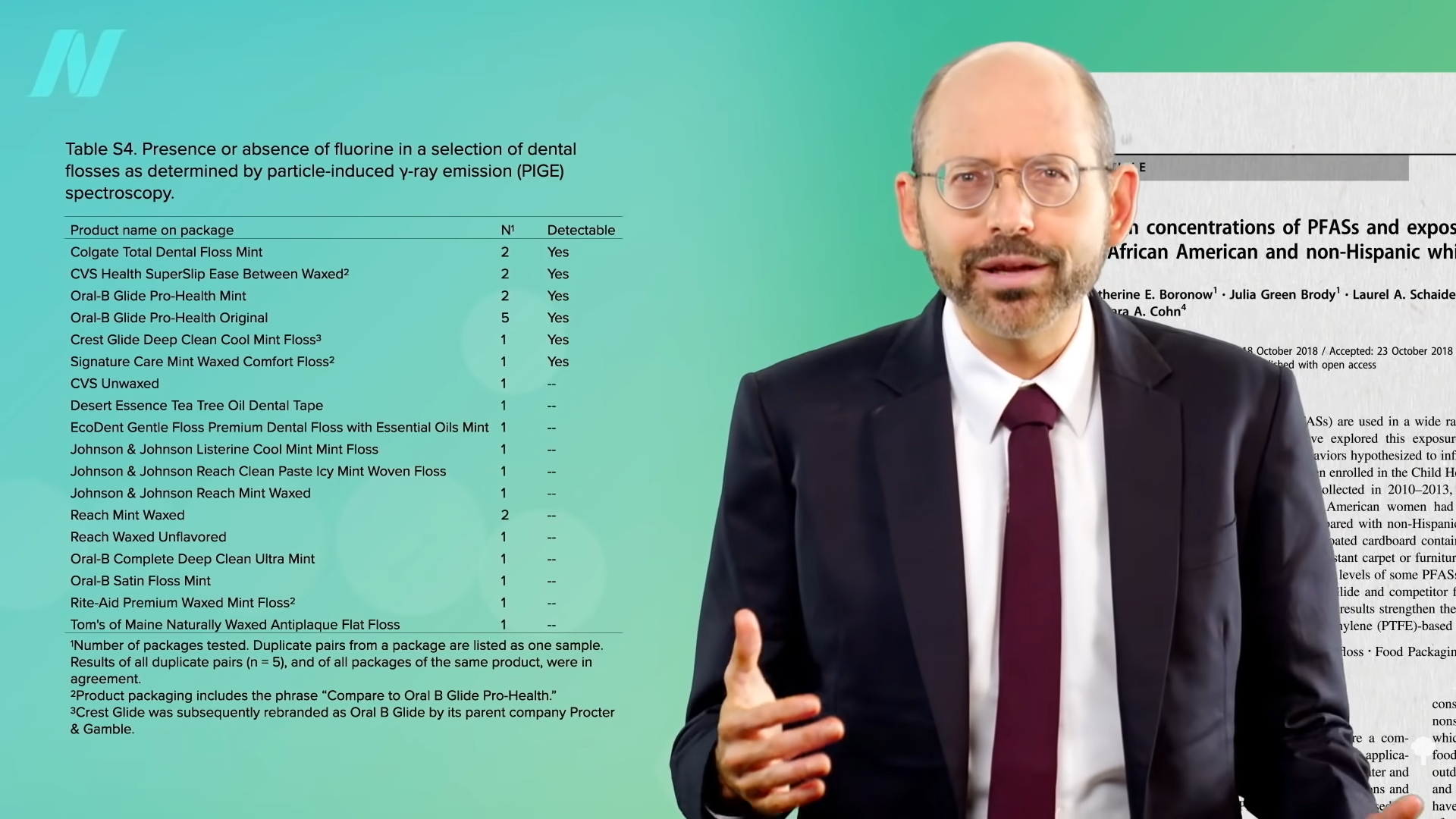
In 2019, Oral-B Glide dental floss was tested. Six out of 18 dental floss products researchers tested showed evidence of Teflon-type compounds. Did those who used those kinds of floss end up with higher levels in their bloodstream? Yes, apparently so. Higher levels of perfluorohexanesulfonic acid were found in Oral-B Glide flossers, as you can see below and at 5:28 in my video.
There are a lot of environmental exposures in the modern world we can’t avoid, but we shouldn’t make things worse by adding them to consumer products. At least we have some power to “lower [our] personal exposure to these harmful chemicals.”
This is the second in a three-video series on cookware. The first was Are Aluminum Pots, Bottles, and Foil Safe?, and the next is Are Melamine Dishes and Polyamide Plastic Utensils Safe?.
What about pressure cooking? I covered that in Does Pressure Cooking Preserve Nutrients?.
So, what is the safest way to prepare meat? See Carcinogens in Meat.
[ad_2]
Michael Greger M.D. FACLM
Source link