
[ad_1]
Many doctors mistakenly rely on serum B12 levels in the blood to test for vitamin B12 deficiency.
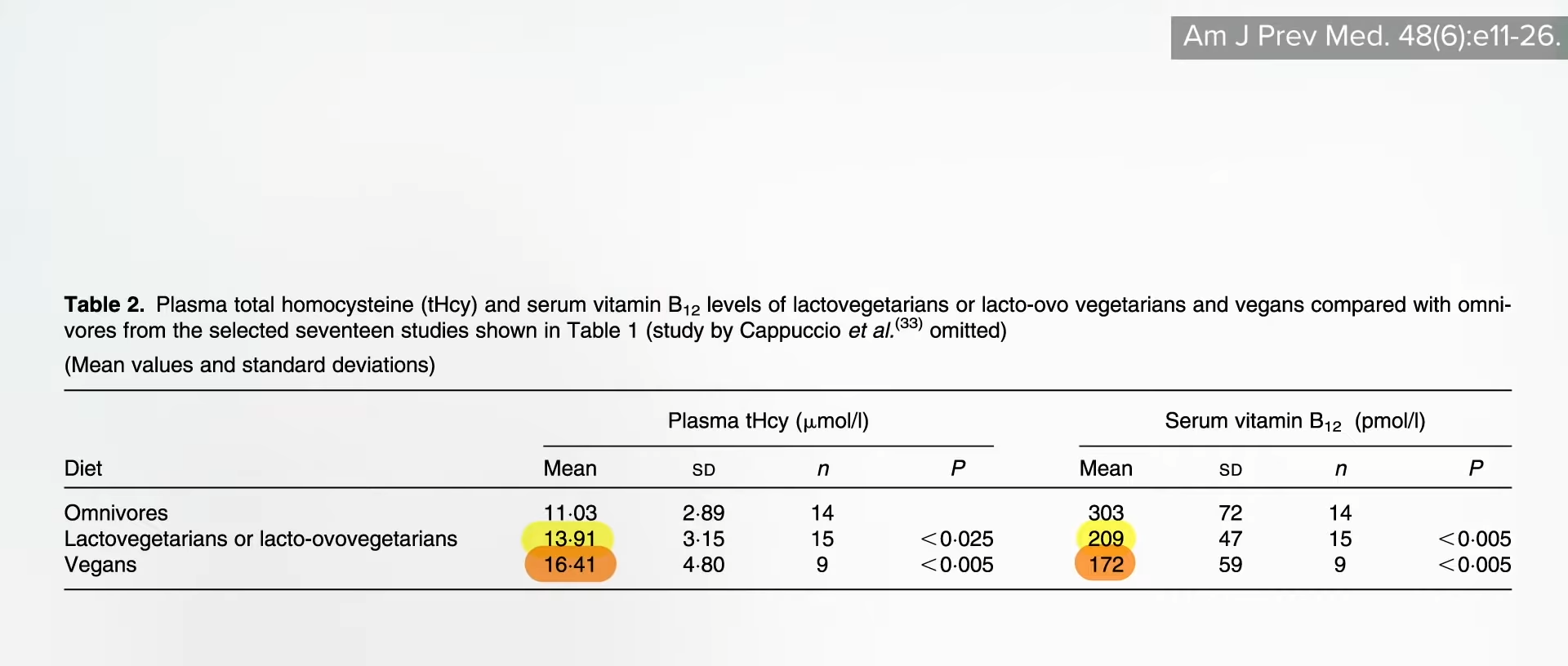
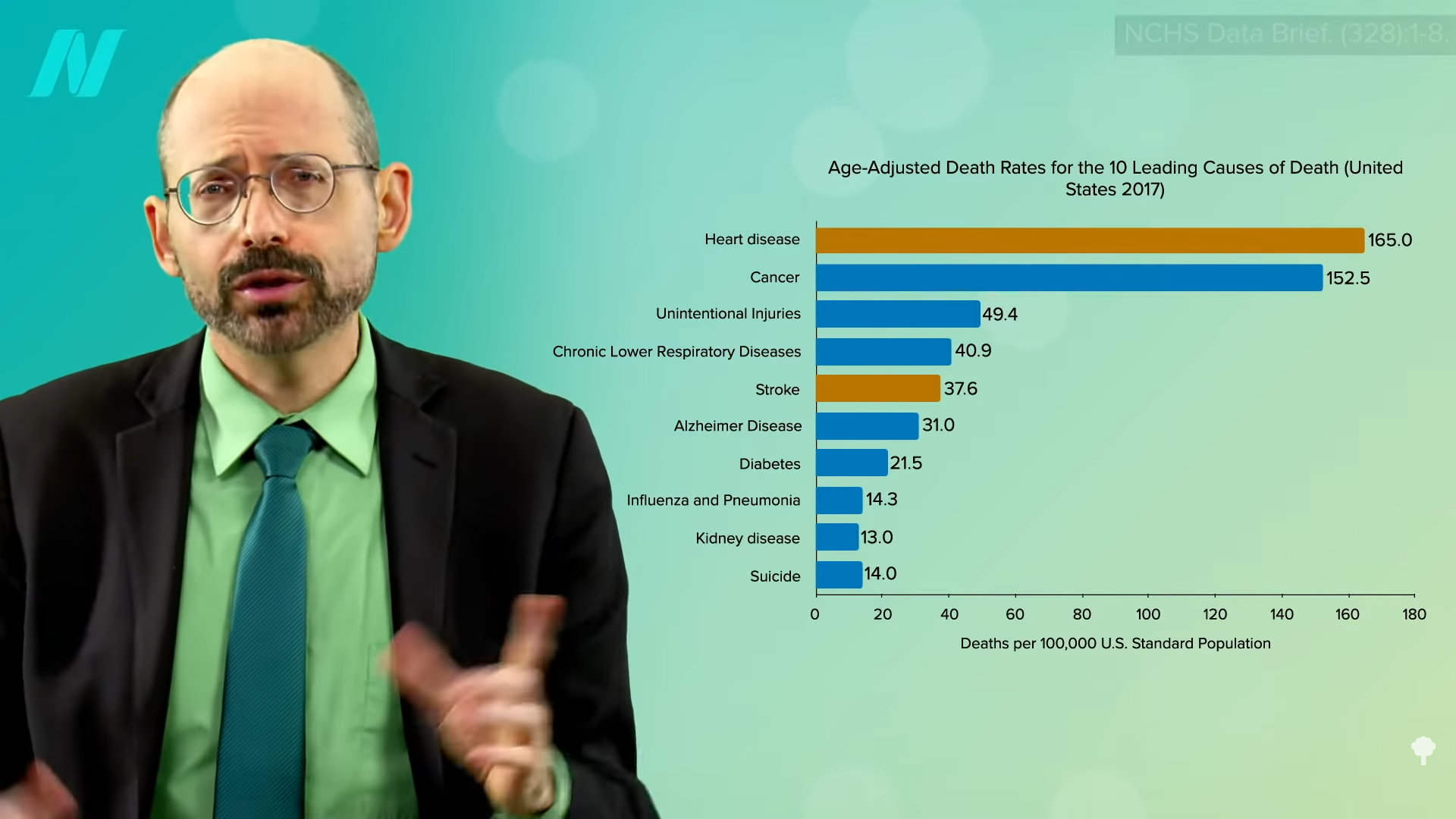
There were two cases of young, strictly vegetarian individuals with no known vascular risk factors. One suffered a stroke, and the other had multiple strokes. Why? Most probably because they weren’t taking vitamin B12 supplements, which leads to high homocysteine levels, which can attack our arteries.
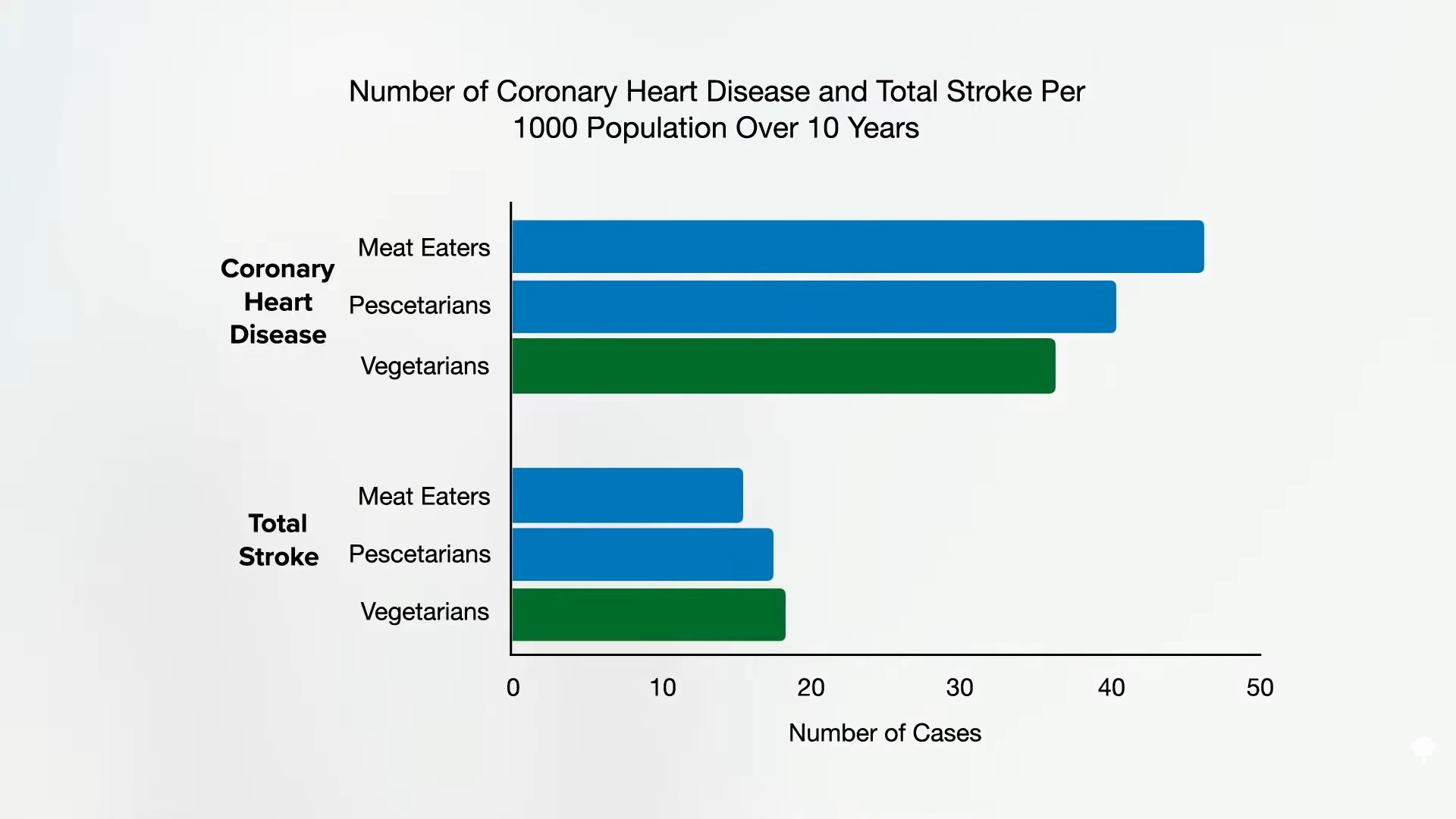
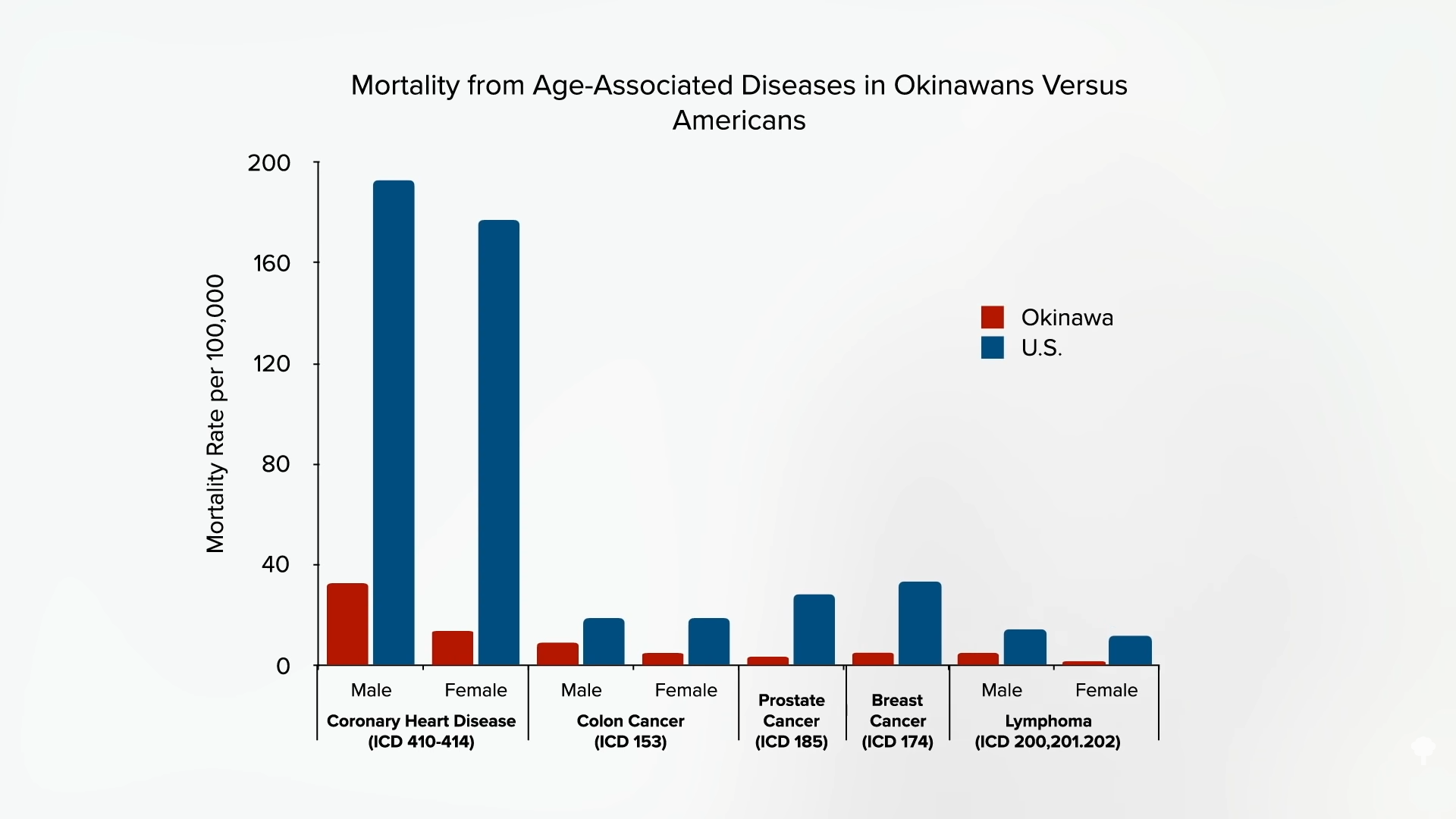
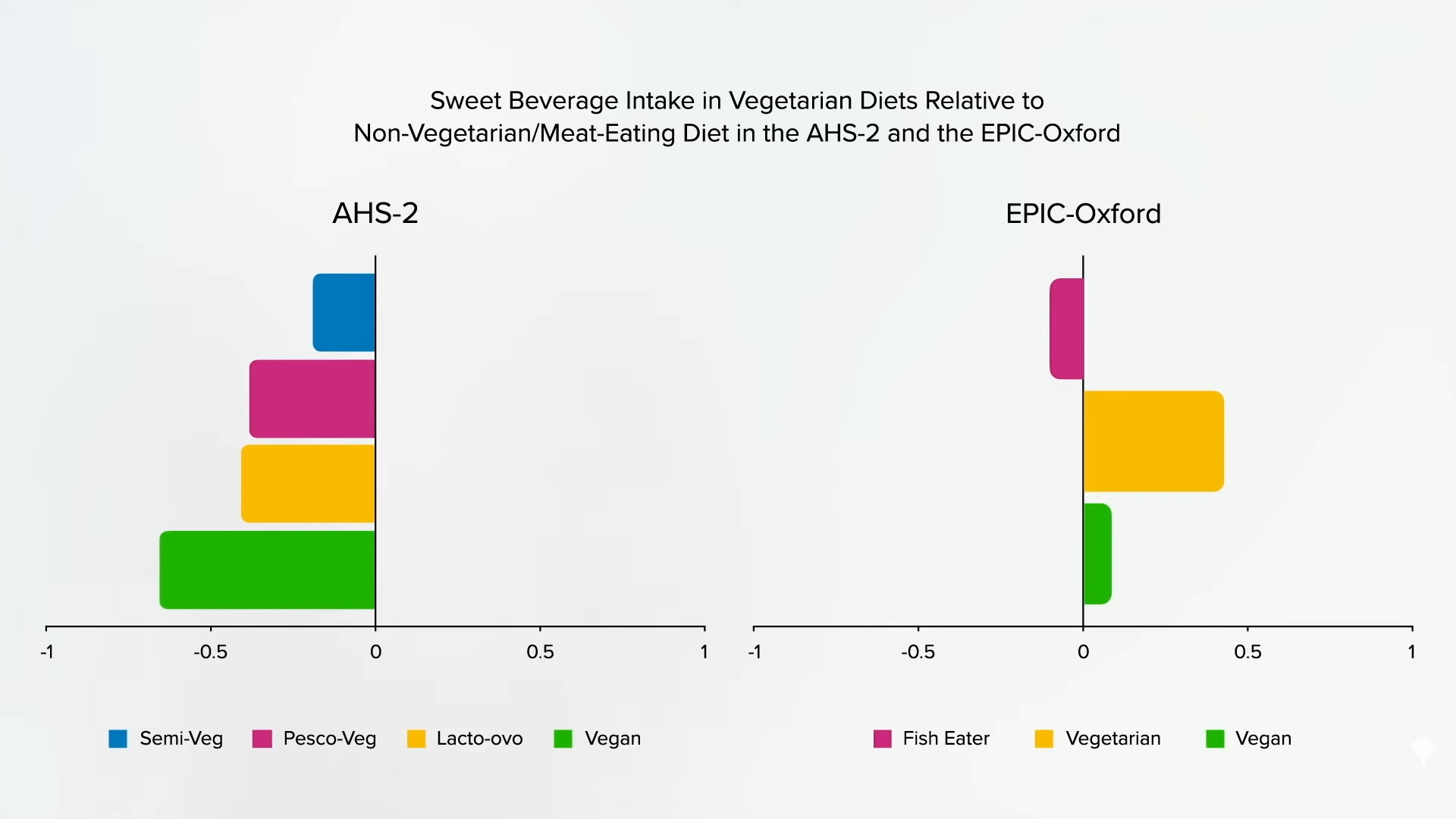
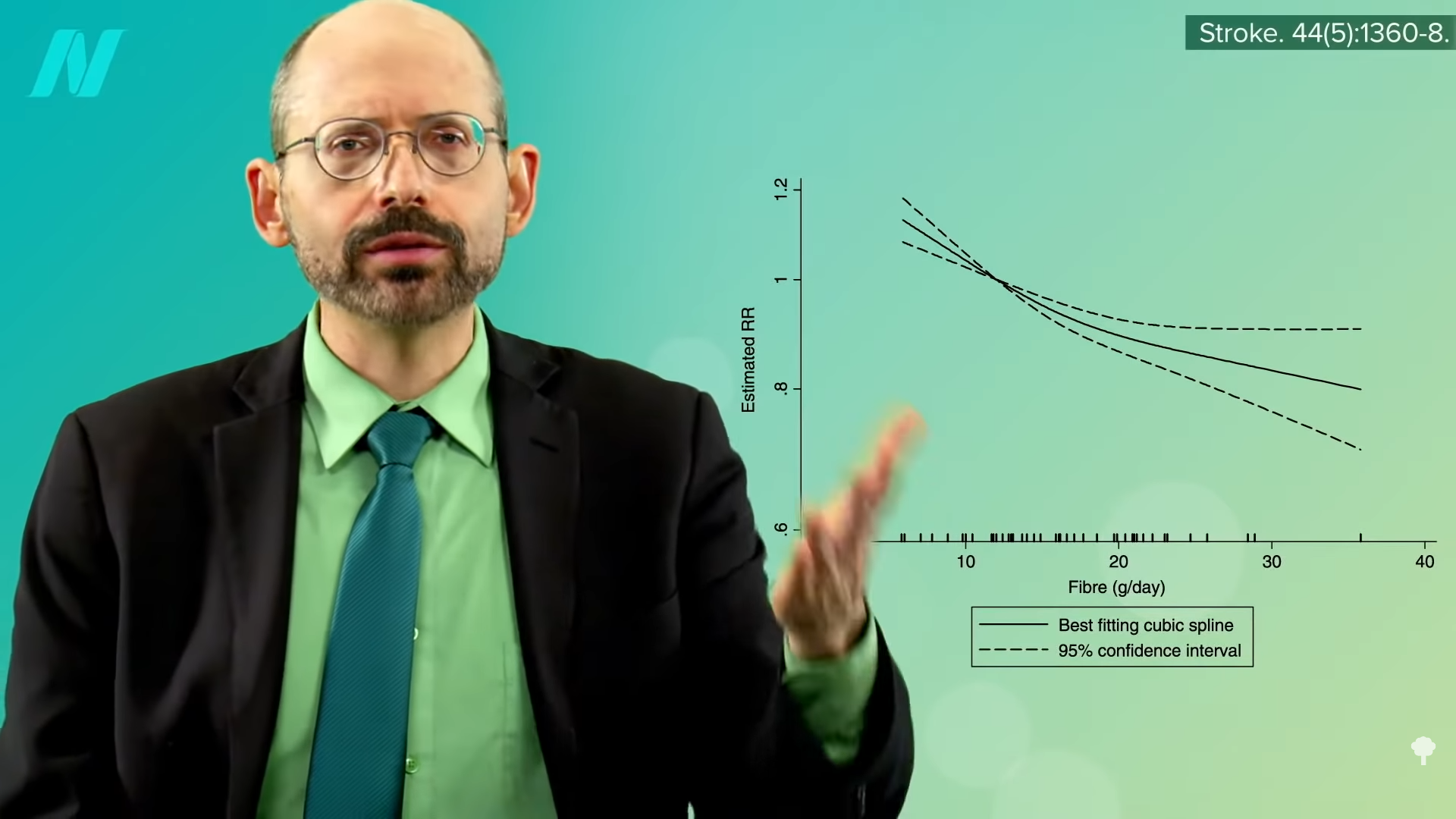
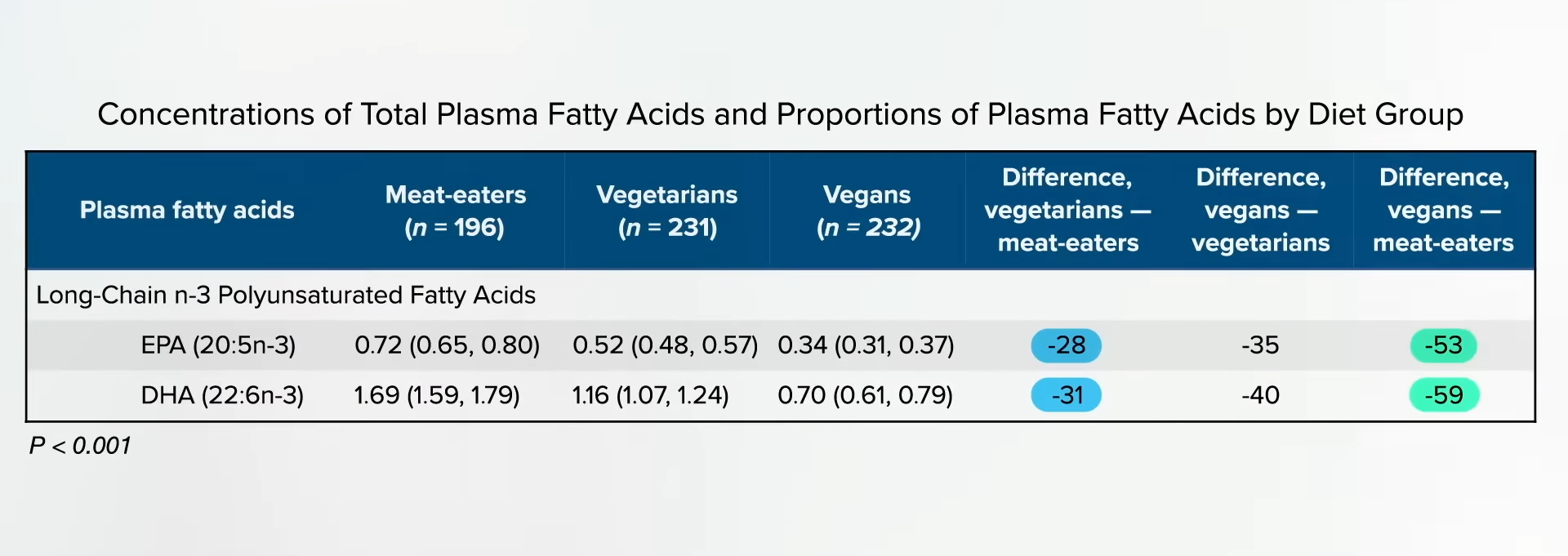
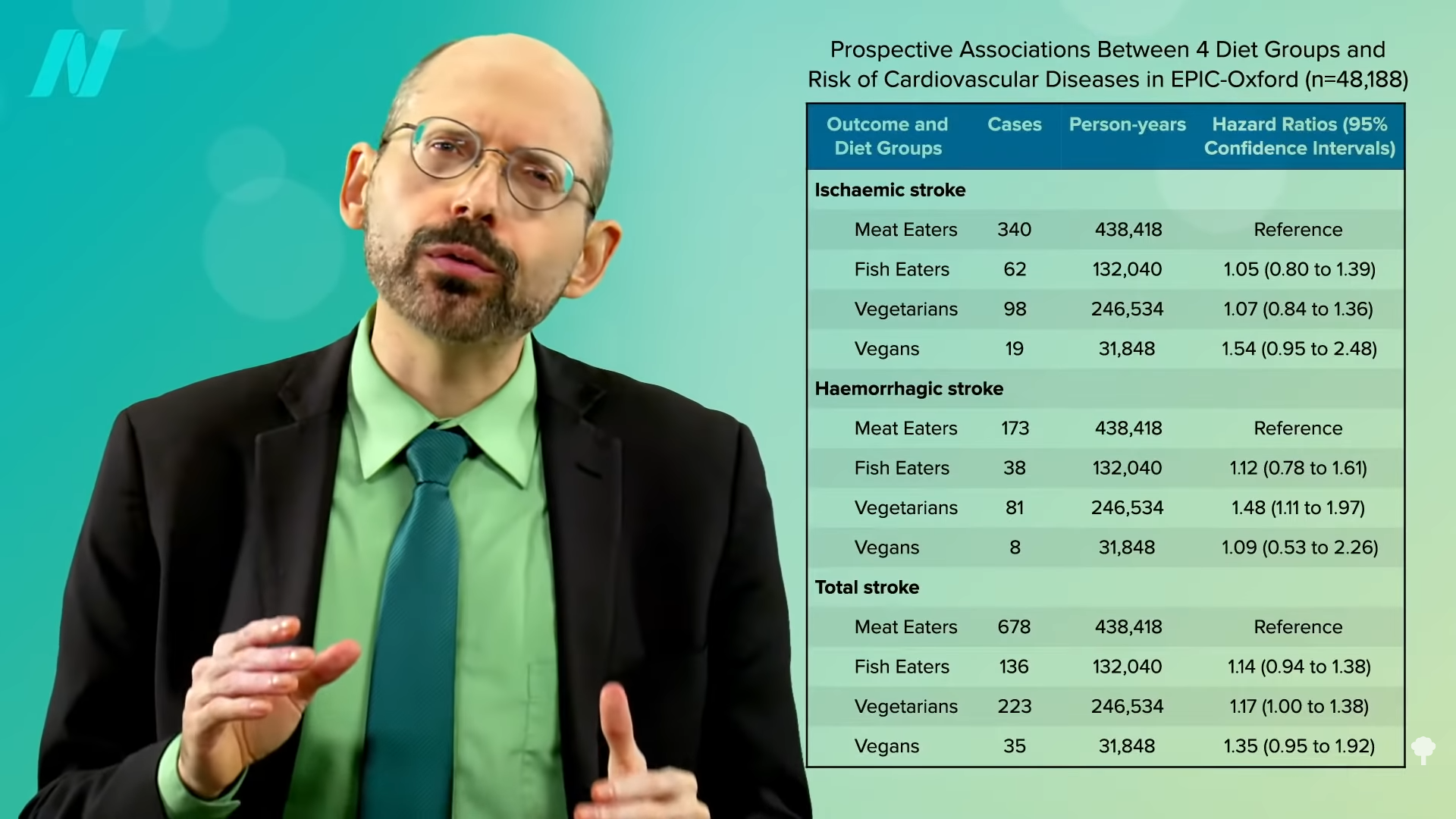
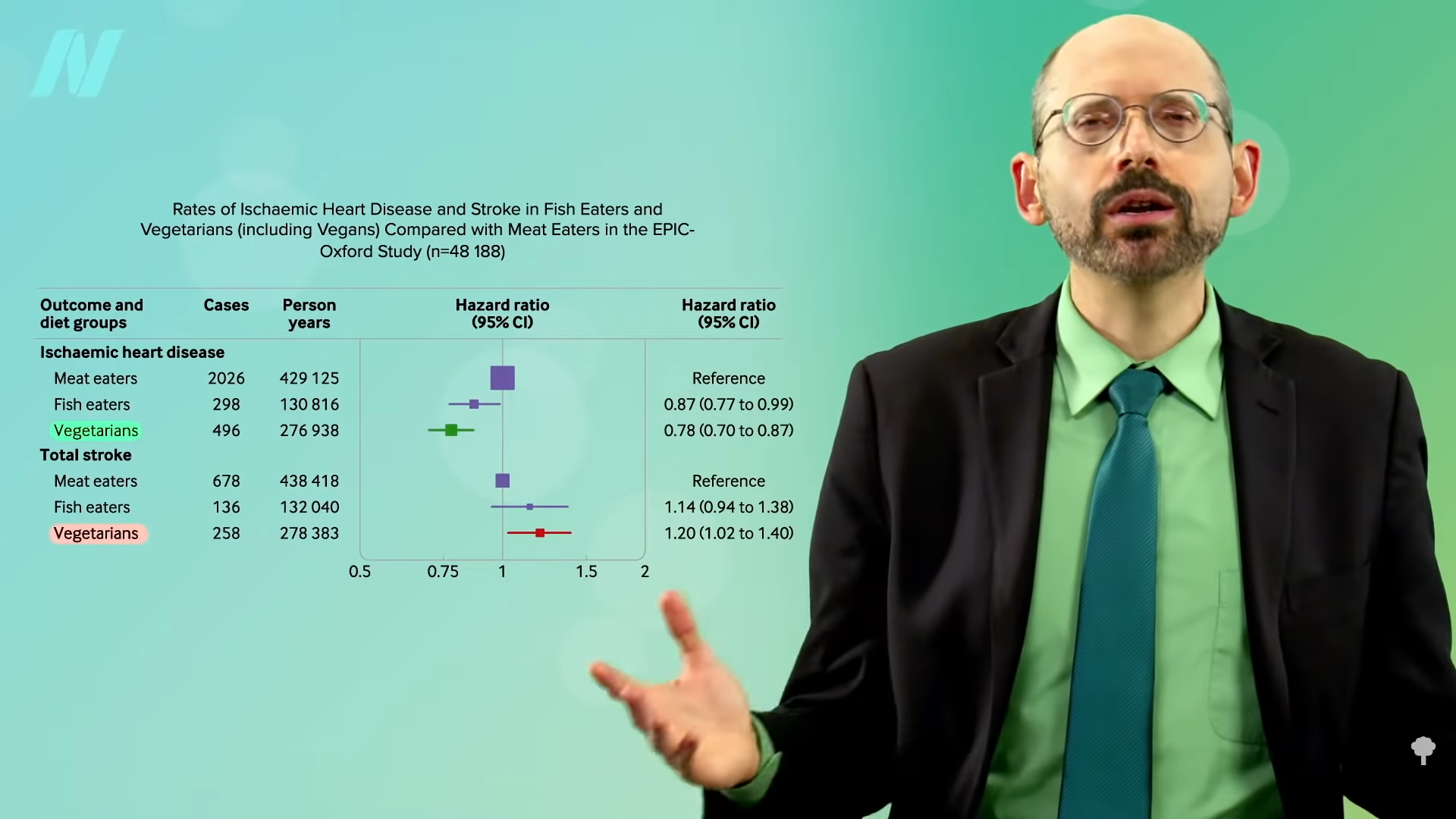
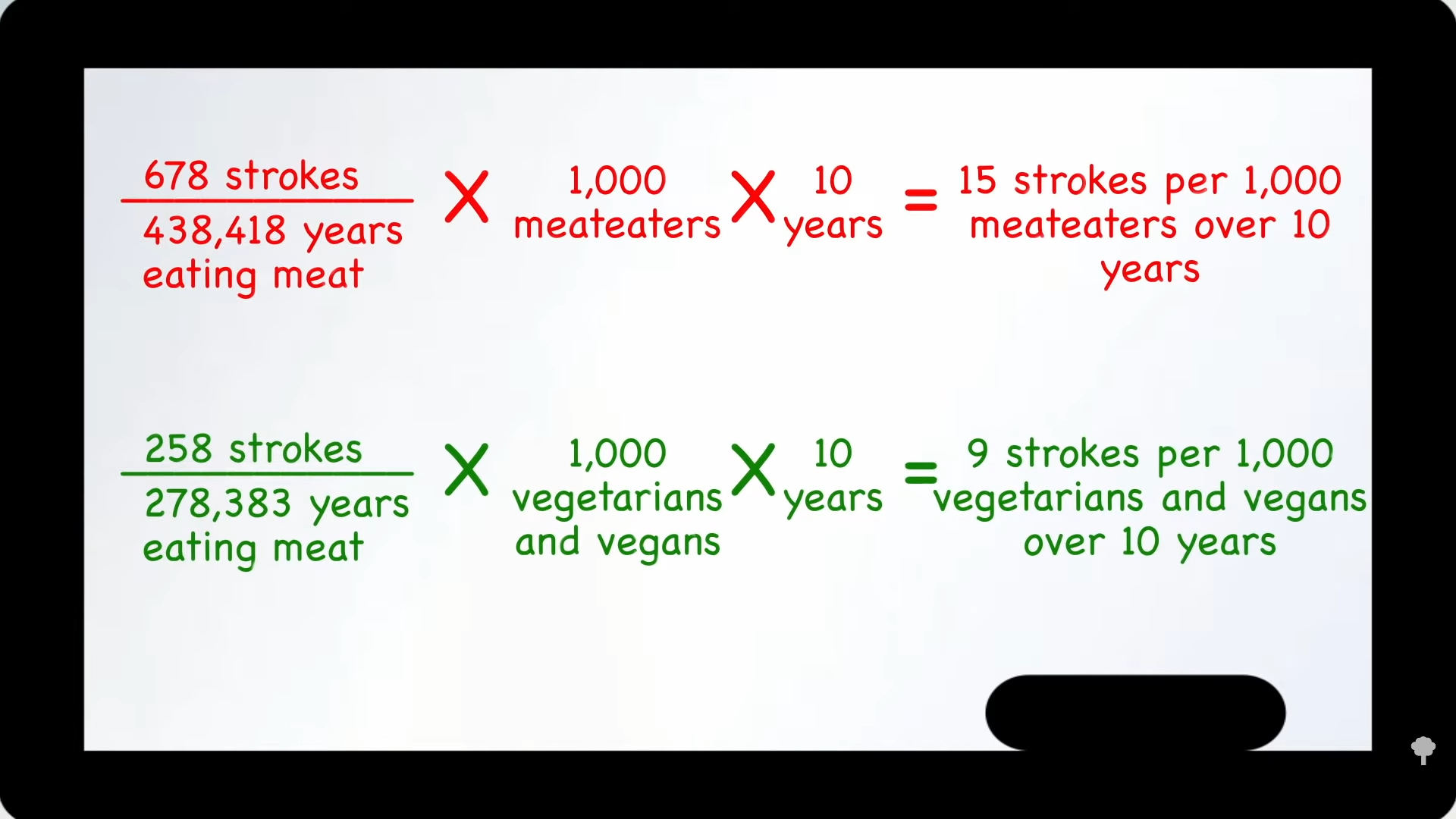
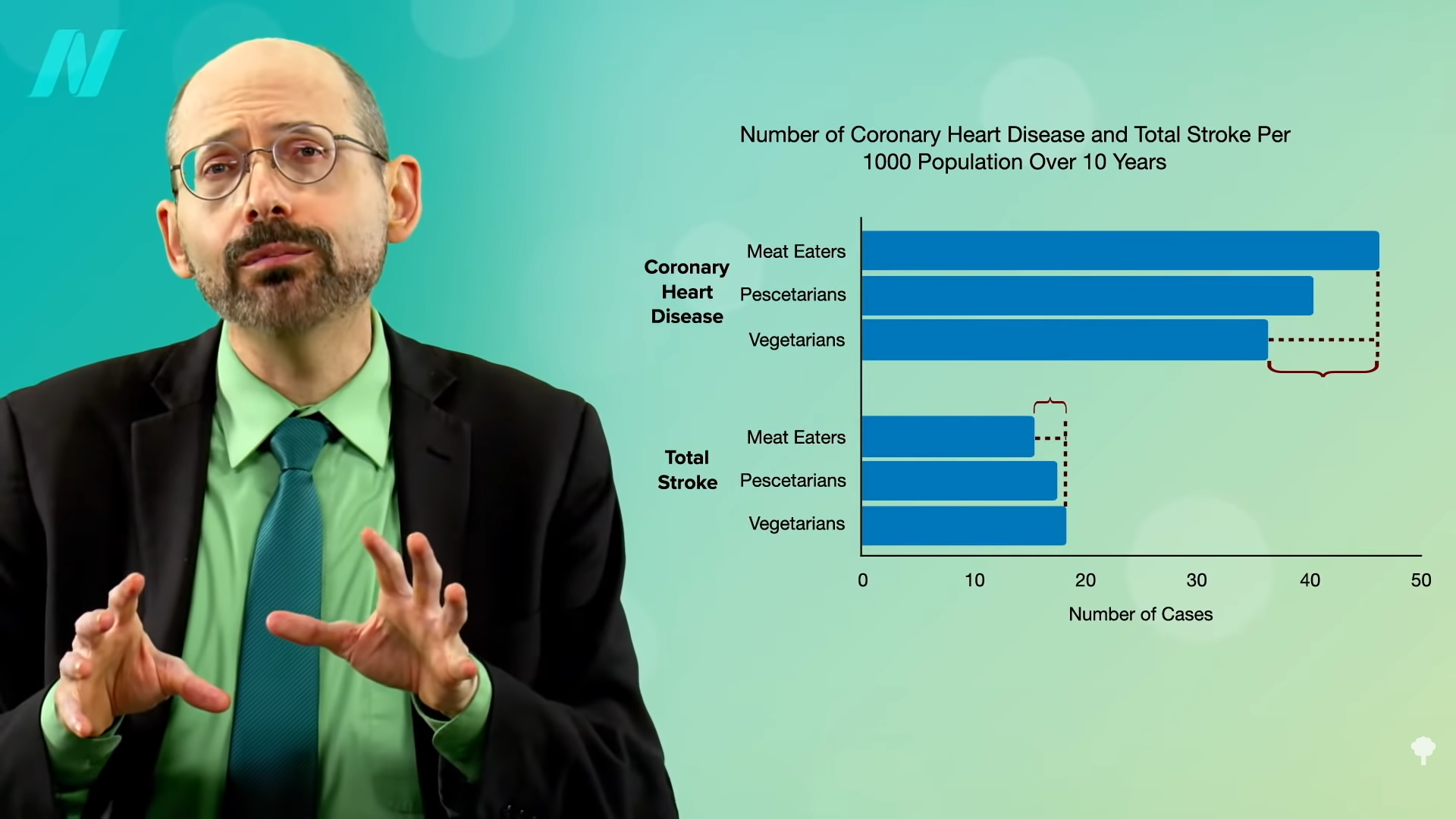
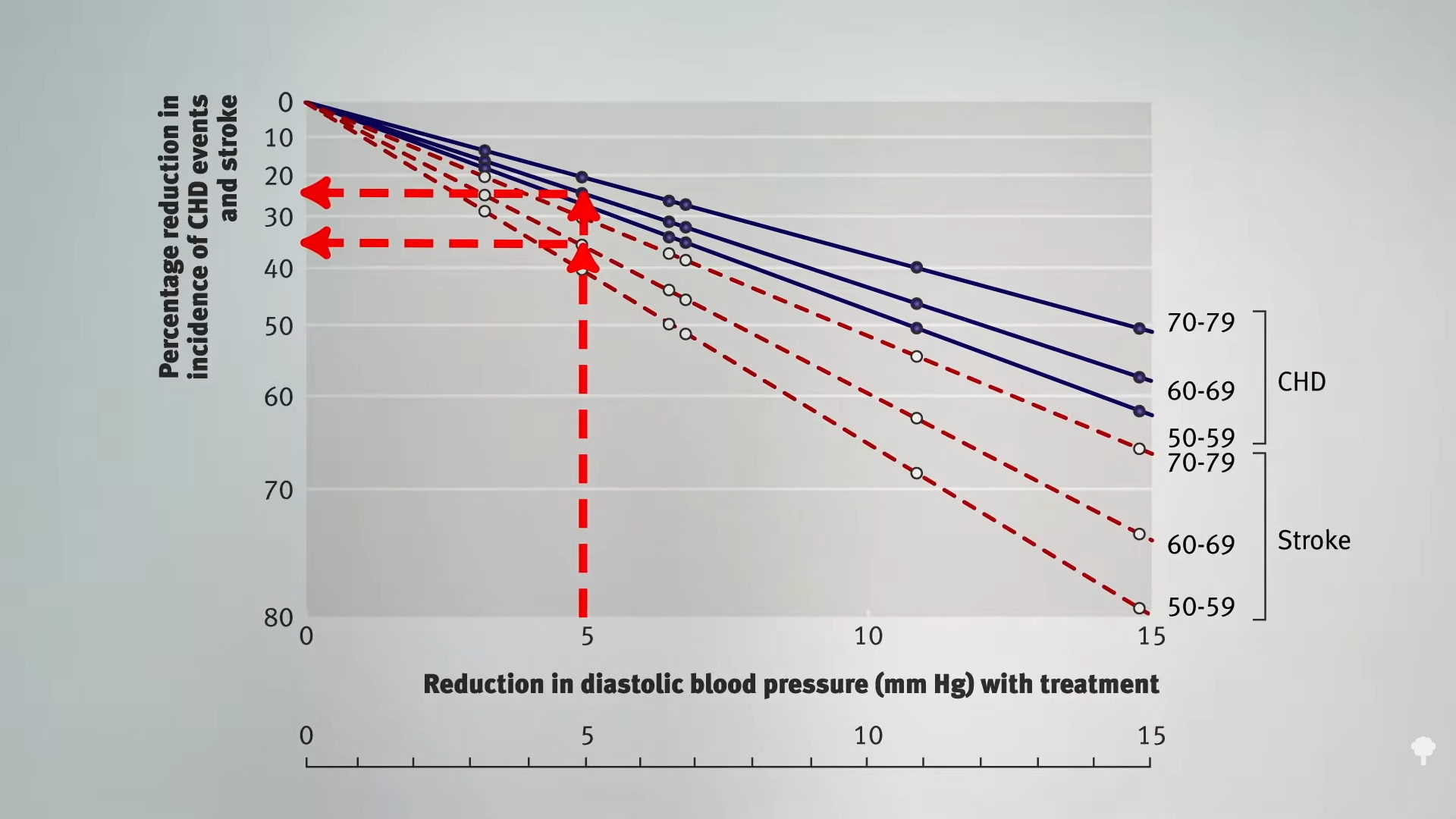
So, those eating plant-based who fail to supplement with B12 may increase their risk of both heart disease and stroke. However, as you can see in the graph below and at 0:47 in my video How to Test for Functional Vitamin B12 Deficiency, vegetarians have so many heart disease risk factor benefits that they are still at lower risk overall, but this may help explain why vegetarians were found to have more stroke. This disparity would presumably disappear with adequate B12 supplementation, and the benefit of lower heart disease risk would grow even larger.
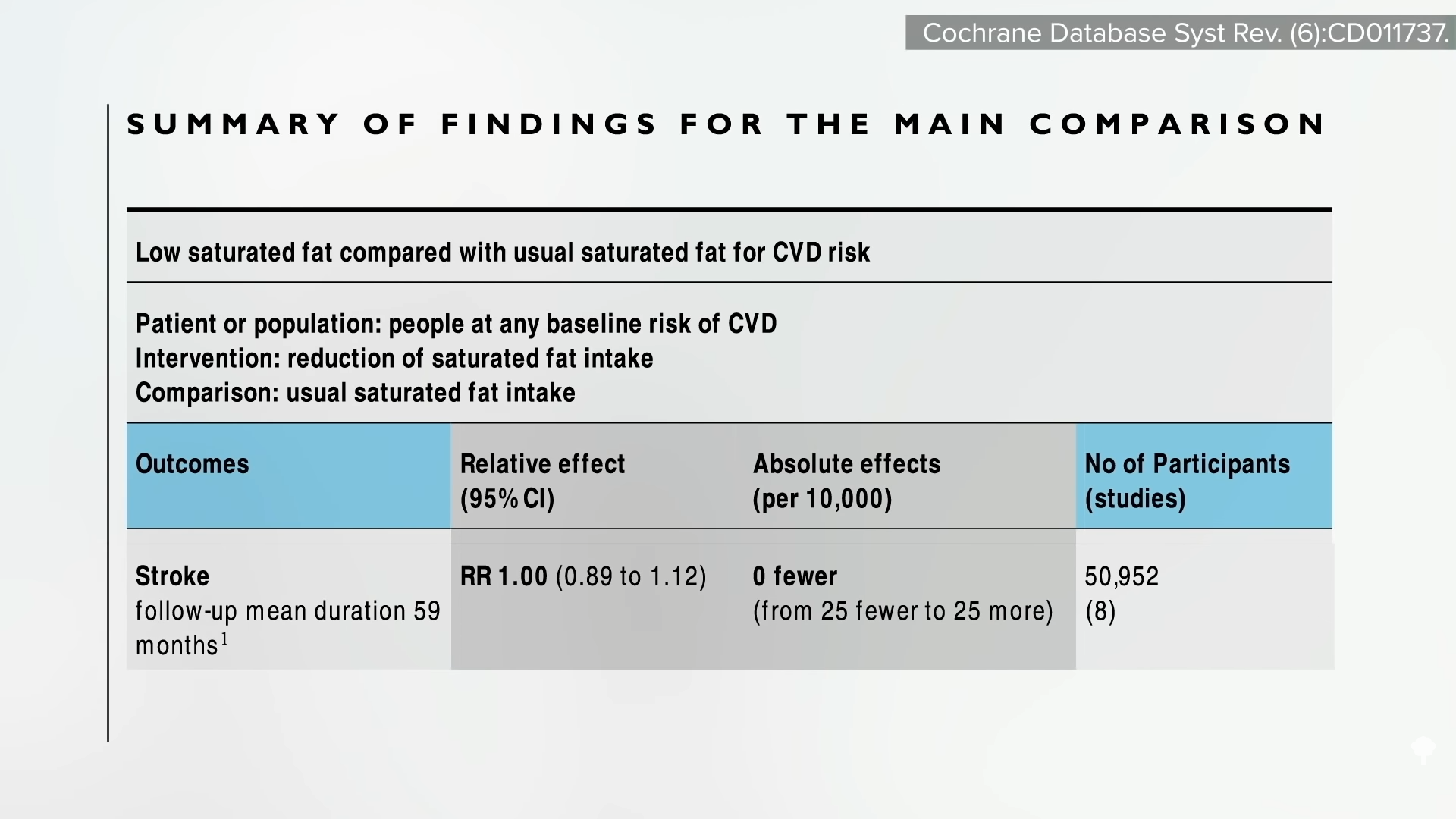
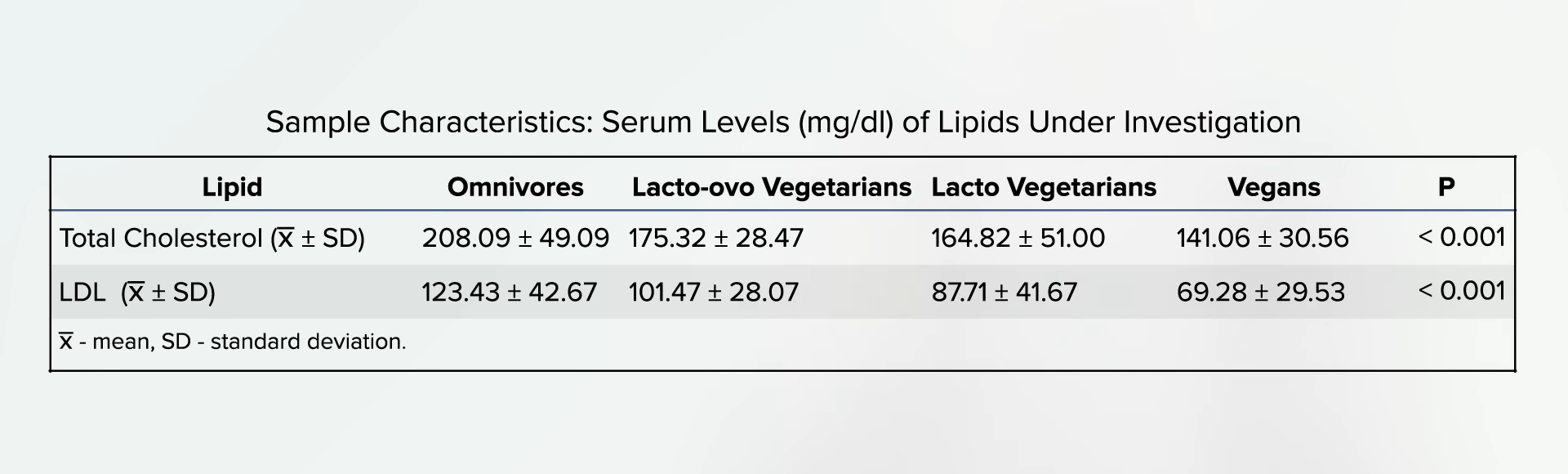
Compared with non-vegetarians, vegetarians enjoy myriad other advantages, such as better cholesterol, blood pressure, blood sugars, and obesity rates. But, what about that stroke study? Even among studies that have shown benefits, “the effect was not as pronounced as expected, which may be a result of poor vitamin B12 status due to a vegetarian diet. Vitamin B12 deficiency may negate the cardiovascular disease prevention benefits of vegetarian diets. To further reduce the risk of cardiovascular disease, vegetarians should be advised to use vitamin B12 supplements.”
How can you determine your B12 status? By the time you’re symptomatic with B12 deficiency, it’s too late. And, initially, the symptoms can be so subtle that you might even miss them. What’s more, you develop metabolic vitamin B12 deficiency well before you develop a clinical deficiency, so there’s “a missed opportunity to prevent dementia and stroke” when you have enough B12 to avoid deficiency symptoms, but not enough to keep your homocysteine in check. “Underdiagnosis of this condition results largely from a failure to understand that a normal serum [blood level] B12 may not reflect an adequate functional B12 status.” The levels of B12 in our blood do not always represent the levels of B12 in our cells. We can have severe functional deficiency of B12 even though our blood levels are normal or even high.
“Most physicians tend to assume that if the serum B12 is ‘normal,’ there is no problem,” but, within the lower range of normal, 30 percent of patients could have metabolic B12 deficiency, with high homocysteine levels.
Directly measuring levels of methylmalonic acid (MMA) or homocysteine is a “more accurate reflection of vitamin B12 functional statuses.” Methylmalonic acid can be checked with a simple urine test; you’re looking for less than a value of 4 micrograms per milligram of creatinine. “Elevated MMA is a specific marker of vitamin B12 deficiency while Hcy [homocysteine] rises in both vitamin B12 and folate deficiencies.” So, “metabolic B12 deficiency is strictly defined by elevation of MMA levels or by elevation of Hcy in folate-replete individuals,” that is, in those getting enough folate. Even without eating beans and greens, which are packed with folate, folic acid is added to the flour supply by law, so, these days, high homocysteine levels may be mostly a B12 problem. Ideally, you’re looking for a homocysteine level in your blood down in the single digits.
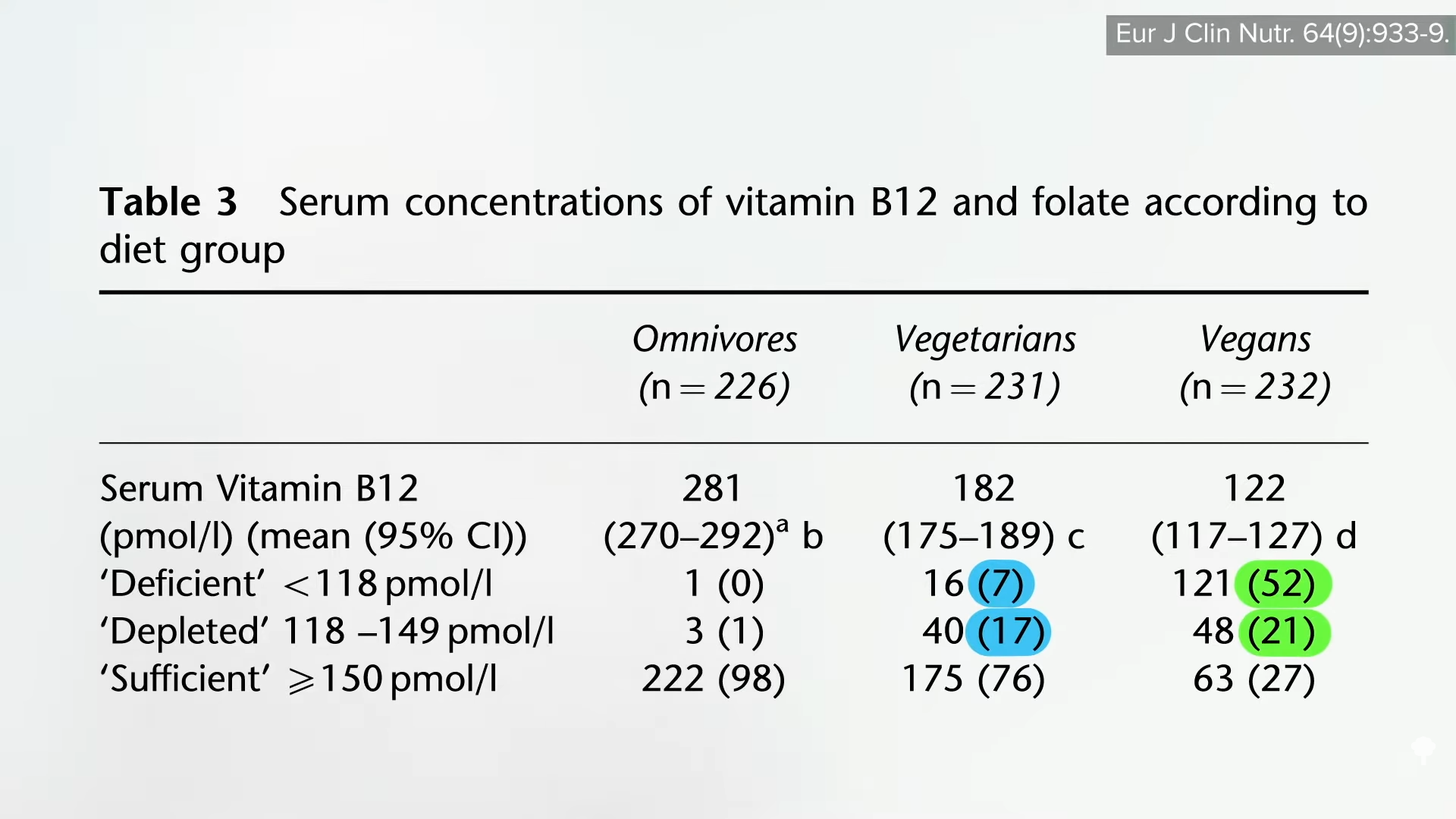
Measured this way, “the prevalence of subclinical functional vitamin B12 deficiency is dramatically higher than previously assumed…” We’re talking about 10 to 40 percent of the general population, more than 40 percent of vegetarians, and the majority of vegans who aren’t scrupulous about getting their B12. Some suggest that those on plant-based diets should check their vitamin B12 status every year, but you shouldn’t need to if you’re adequately supplementing.
There are rare cases of vitamin B12 deficiency that can’t be picked up on any test, so it’s better to just make sure you’re getting enough.
If you do get your homocysteine tested and it’s still too high, up in the double digits despite B12 supplementation and eating beans and greens, I have a suggestion for you in the final videos of this series, which we’ll turn to next with: Should Vegetarians Take Creatine to Normalize Homocysteine? and The Efficacy and Safety of Creatine for High Homocysteine.
How did we end up here? To watch the full series if you haven’t yet, check the related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link






















 Even compared to spinach? As you can see in the graph below and at 3:14 in my
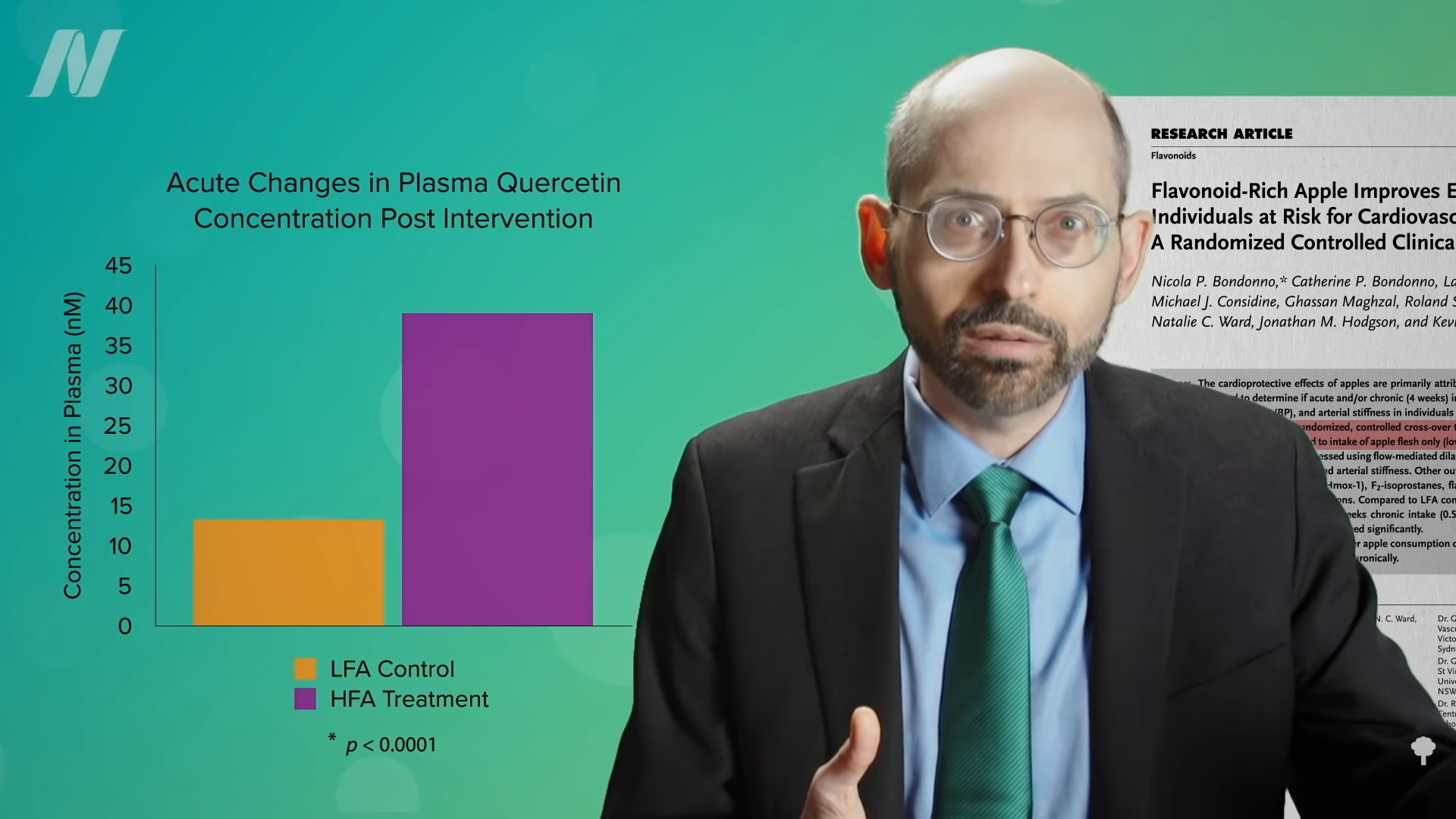
Even compared to spinach? As you can see in the graph below and at 3:14 in my 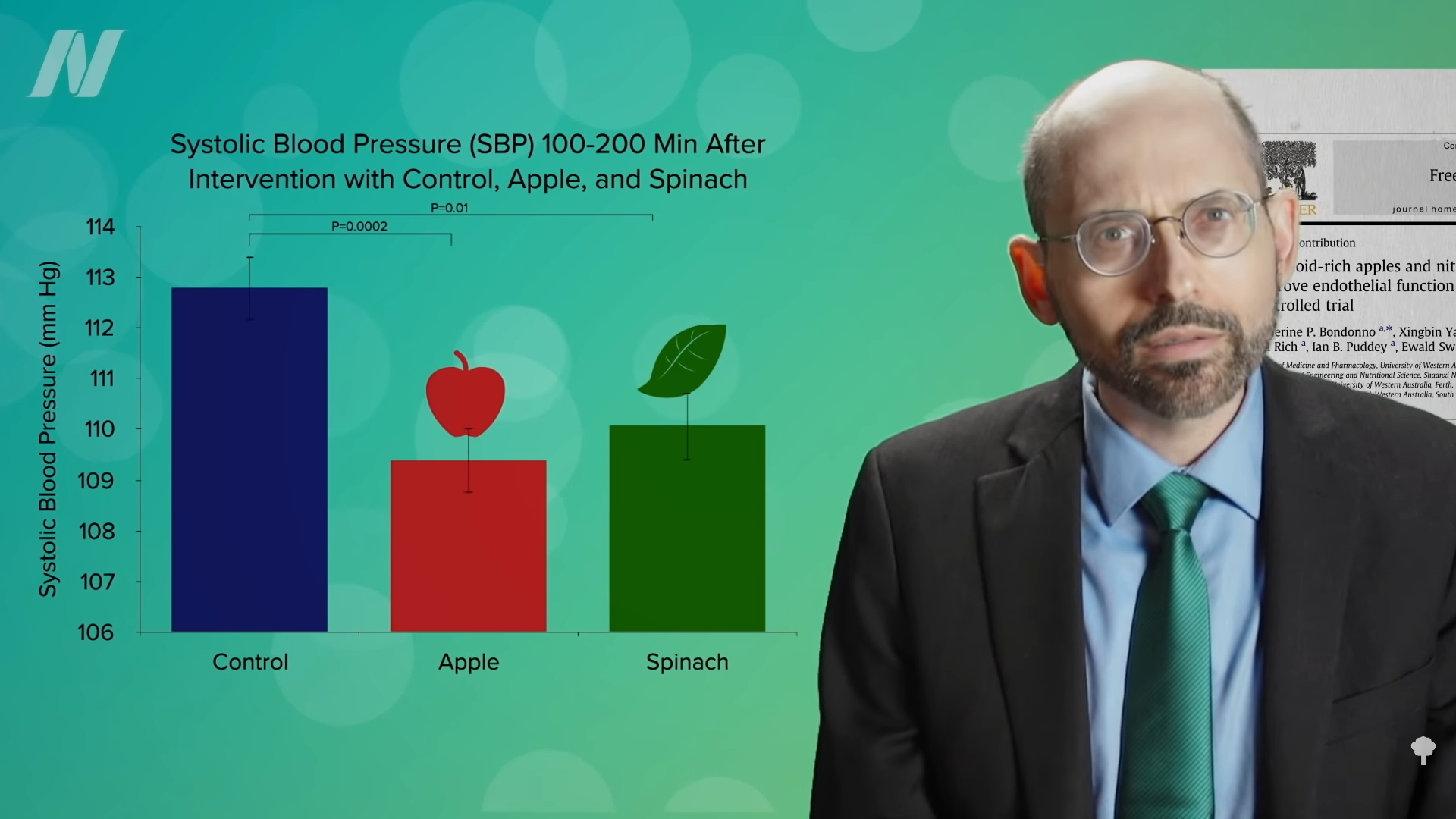 What’s nice about these results is that we’re talking about whole foods, not some supplement or extract. So, easily, “this could be translated into a natural and low-cost method of reducing the cardiovascular risk profile of the general population.”
What’s nice about these results is that we’re talking about whole foods, not some supplement or extract. So, easily, “this could be translated into a natural and low-cost method of reducing the cardiovascular risk profile of the general population.”