[ad_1]
Walnuts, almonds, and hazelnuts are put to the test for erectile and sexual function, sperm count, and semen quality.
In 2013, I posted a video based on a study that found that men with erectile dysfunction who ate 100 grams of pistachios (a little more than three handsful) a day for three weeks had “a significant improvement in erectile function.” It’s always nice to see a whole-food intervention have clinical effects, and I was curious to revisit the topic and see what’s been published since.
Even if you ignore all the lab animal studies on hazelnuts improving the function of rat testicles—really, there’s a study titled “Hazelnut Consumption Improves Testicular Antioxidant Function and Semen Quality in Young and Old Male Rats”—you still never know what you’ll find searching the medical literature for nuts and sexual function. I found “a case of penile strangulation with a metal hex nut” in which someone put one on his penis “for sexual pleasure” but couldn’t remove it. (I guess some kinds of nuts can sometimes make things worse.) They tried the Dundee technique, which involves creating 20 puncture holes to relieve the pressure, but that didn’t work, so then they tried a diamond disk cutter. It slipped a few times, but the hex nut was successfully removed. All’s well that ends well.
That got me curious. Evidently, penile entrapment is so common that there is an entire grading system that emergency room doctors can use, as you can see here and at 1:21 in my video Mixed Nuts Put to the Test for Erectile Dysfunction. If a drill isn’t available, the surgeons advised, “a hammer and chisel may be used to remove nuts.”
A drill? Oh, they mean a dental drill. Doctors describing one case bragged about the “precisely cut edges,” but it looks pretty jagged to me. You can see for yourself below and at 1:38 in my video.
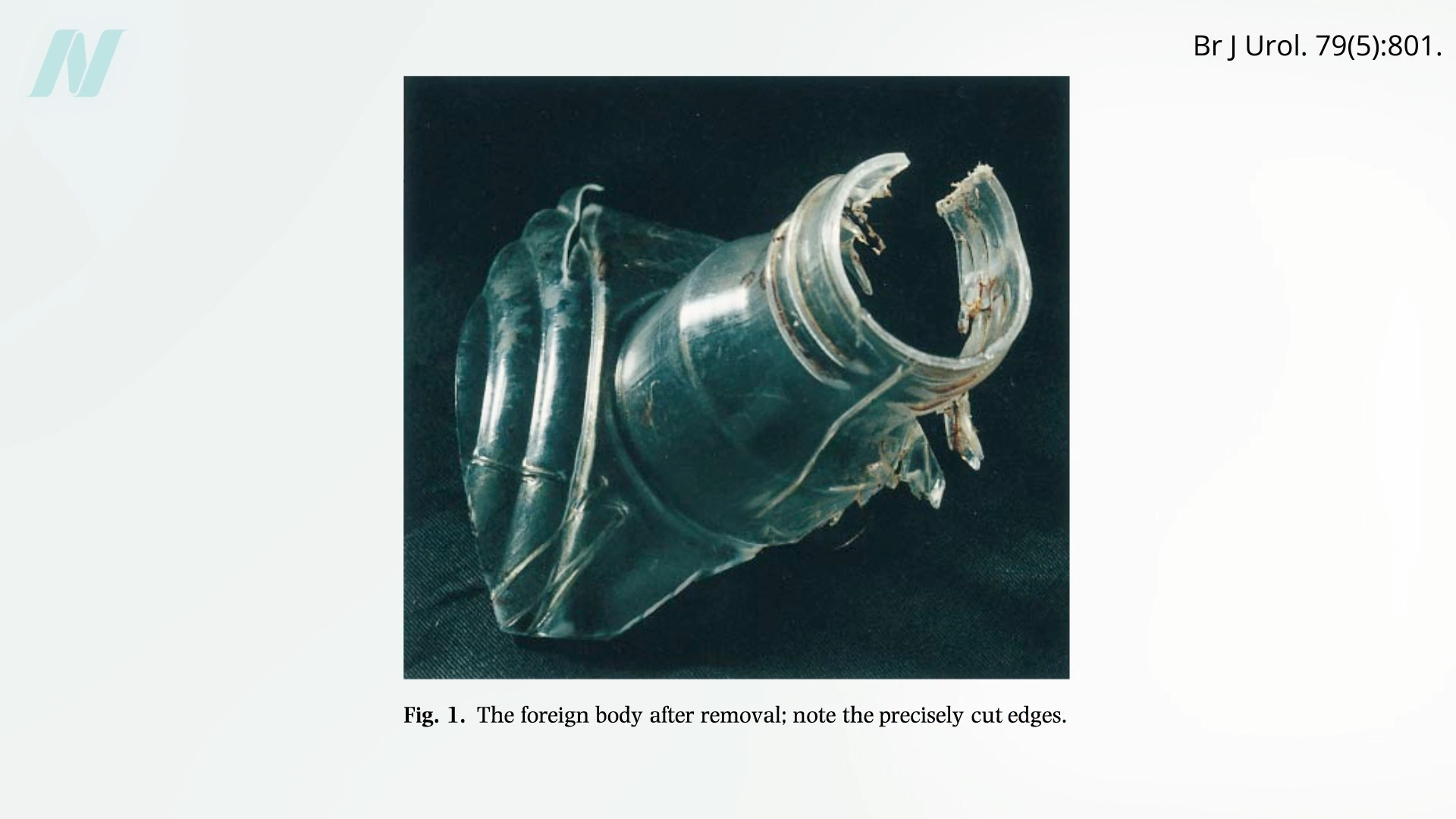
To “preserve the penis from fatal outcomes” (that’s a strange way to put it), urologists should be aware of all the available tools and approaches, and if you don’t know how to operate the saw, you can always call in the local blacksmith—but only if “special consent [is] taken from the patient”!
But how are you going to remove an iron barbell or steel sledgehammer head? “With a heavy-duty air grinder provided by the fire department,” requiring six hours of cutting and fire coats to protect the patient from the sparks. Use whatever it takes—hack saw, “cement eater.” You can even use the silk winding method pioneered by Dong et al.
Back to the task at hand! Consuming “at least one serving of vegetables a day and more than two servings of nuts a week was associated with a more than 50% decrease in the probability of ED” [erectile dysfunction] in a snapshot-in-time cross-sectional study. But such observational studies can’t prove cause and effect. It’s like finding that men who eat healthier have better sperm motility. Maybe men who eat nuts are just health nuts, and the improvement is due to some other factor, like exercise. What we need is an interventional trial.
And there is one: a randomized controlled trial studied the “effect of nut consumption on semen quality and functionality.” Healthy men were fed the standard American diet with or without a mixture of nuts—a handful (30 grams) of walnuts and half a handful (15 grams) each of almonds and hazelnuts. Individuals in the nut group experienced significant improvements in their total sperm count, vitality, motility, and shape, perhaps because those “in the nut group showed a significant reduction in SDF”—sperm DNA fragmentation. The nuts appeared to protect their sperm DNA. It’s too bad that the researchers didn’t measure the men’s erectile and sexual dysfunction while they were at it. Oh, but they did!
What is the effect of nut consumption on erectile and sexual function from that same study? The researchers report that those in the nut group saw a significant increase in orgasmic function and sexual desire, but what about erectile function? Any time you see this kind of selective glass-half-full reporting, you suspect some kind of industry funding, and, indeed, that was the case here; the study was partially funded by the International Nut and Dried Fruit Council. Yes, there was a marginal increase in orgasmic function and sexual desire of questionable clinical significance, but there was no improvement in erectile function, intercourse satisfaction, or overall satisfaction. As with so many comparisons, even the so-called significant findings may not even be statistically significant.
But why did the pistachios I talked about back in 2013 work, while these other nuts didn’t? Well, the original study was done on men mostly in their 40s and 50s who already had chronic erectile dysfunction for at least one year, whereas the average age of participants in the newer study was 24. So, the individuals in the later study may have started out with near-maximum circulation, not leaving much room for the nuts to work any magic.
Doctor’s Note
Sorry for that crazy tangent! I just wanted to give people a taste of what it can be like when you dive deep into the medical literature.
The 2013 video I mentioned is Pistachio Nuts for Erectile Dysfunction.
What about walnuts for arterial blood flow? See Walnuts and Artery Function.
More on fertility and sexual function in the related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link
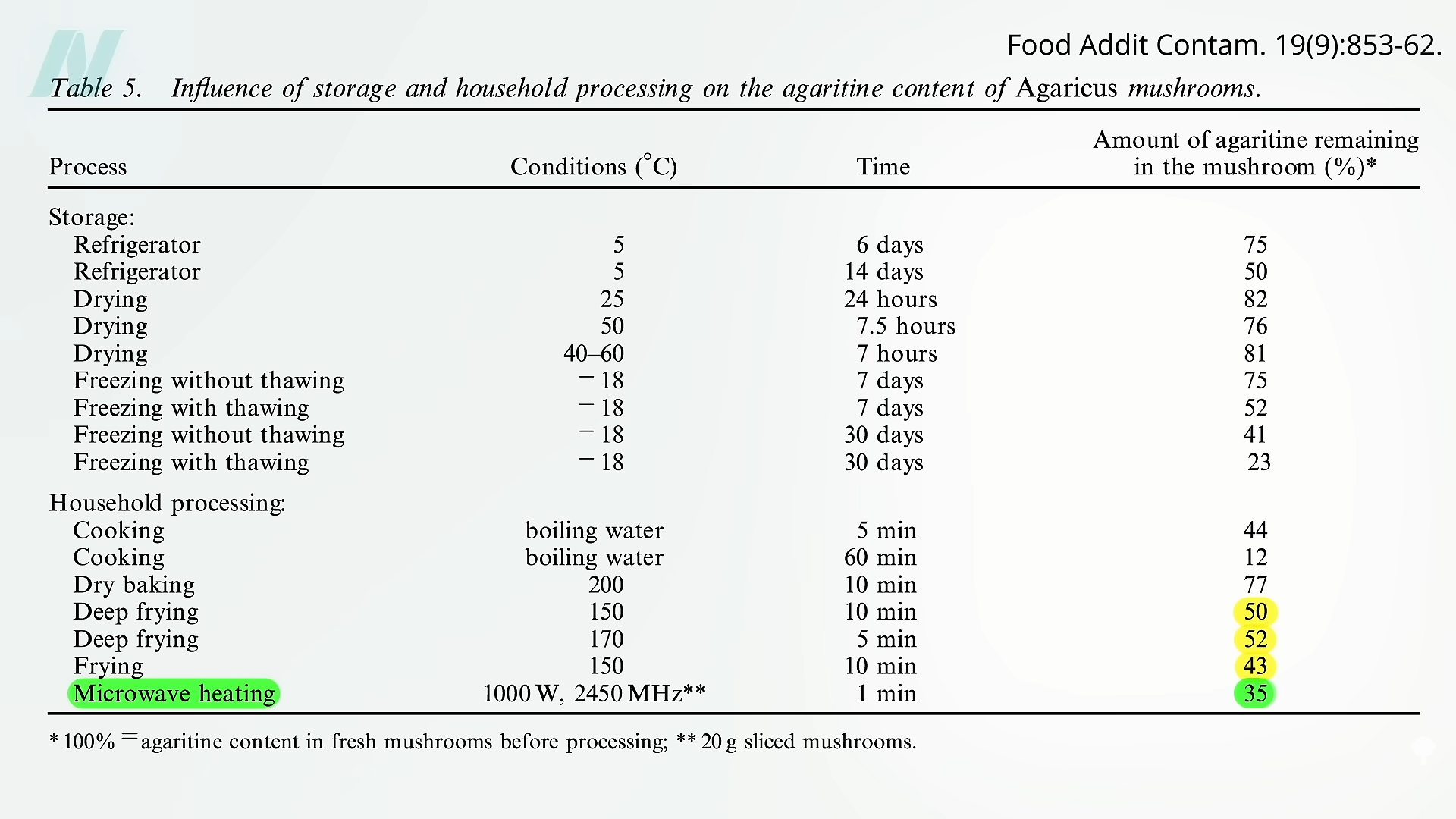 My technique is to add dried mushrooms into the pasta water when I’m making spaghetti. Between the reductions of 20 percent or so from the drying and 60 percent or so from boiling for ten minutes and straining, more than 90 percent of agaritine is eliminated.
My technique is to add dried mushrooms into the pasta water when I’m making spaghetti. Between the reductions of 20 percent or so from the drying and 60 percent or so from boiling for ten minutes and straining, more than 90 percent of agaritine is eliminated. But, again, this is all
But, again, this is all