Grape juice and whole grapes are put to the test for brain function, including cognitive decline in early Alzheimer’s.
In 2010, the first controlled trial was published that examined how the brain responds to grape juice. It helped aged rats, but what about people? “Concord grape juice supplementation improves memory function in older adults with mild cognitive impairment”—or so says the title. The problem is that the study was funded by Welch’s, and, though the authors claim they have no financial interest in the outcome, that seems disingenuous. I mean, do they think Welch’s would ever fund them again if they found grape juice wasn’t good for you? And, indeed, that title is a bit of industry spin. I’m sure that’s what they wanted to find.
Older adults with memory decline (but not dementia) were randomized into a placebo-controlled, double-blind trial with Concord grape juice versus a similarly looking and tasting Kool-Aid type of drink with the same calories and same sugars. That’s a solid study design. And, berries have those wonderful polyphenol phytonutrients, which have anti-inflammatory and antioxidant properties, so it certainly could help brain function and it did seem to help with verbal learning, as you can see in the graph below and at 1:21 in my video Friday Favorites: Benefits of Grapes for Brain Health.
The odds you’d get such notable results just by chance are like 1 in 25, whereas the higher recall scores are not considered to be statistically significant, since even if there wasn’t an effect, you might get those kinds of results by chance 1 in every 8 or 10 times you’d run the experiment, as shown in the graph below and at 1:38 in my video. And, by convention, we like at least 1 in 20—a p-value of 0.05 or less—especially if we’re looking at multiple outcomes, which increases the likelihood that something will pop up as a fluke. The bottom line is that we’re less confident in these memory outcomes. If this study hadn’t had industry funding, I imagine it would be titled more accurately. Perhaps “Concord grape juice supplementation improves verbal learning in older adults with mild cognitive impairment”—which is still an important finding, and we have the Welch’s corporation to thank for it. Without industry funding, a study like this might never get done.
The findings suggest that drinking grape juice is superior to drinking a grape Kool-Aid type of beverage, not necessarily for helping memory, but maybe for helping with learning. When the study was repeated, though, it did seem to help one measure of memory, but no benefit was found for verbal learning, even when using the same test as before, which calls the previous results into question. So, we’re left uncertain about what effects, if any, grape juice has on the aging brain.
What about the brains of middle-aged mothers? The Welch’s-funded researchers noted significant improvements in one measure of memory and driving performance as measured in a fancy driving simulator, suggesting you might be able to stop a dozen yards earlier on the highway after drinking grape juice than if you had instead had a grape Kool-Aid type of drink. I do like how they tried to translate the cognitive effects into more meaningful metrics, but it’s important to acknowledge, as they did, that no effects were found for the majority of cognitive consequences. And, when you study 20 different outcomes, the odds are pretty good that you’d just get a statistically significant result or two by chance, as you can see below and at 3:33 in my video.
The latest study involved giving a single dose of a cup of purple grape juice or white grape juice (to which flavor and color had been added to disguise it) to young adults with an average age of 21. In this way, researchers could see if there’s something special about those deep purple polyphenol pigments in Concord grape juice. Their findings? They got the same kind of results: two cognitive measures just reaching statistical significance, but that’s out of seven different outcomes, as you can see below and at 4:12 in my video. So, instead of a p-value of 0.05 as the cut-off for significance, we’d really like to see closer to 0.007, and none hit that. Maybe it’s because they didn’t use whole food like in that blueberry study I profiled before.
There was a study that looked at actual grape consumption by utilizing freeze-dried grape powder to capture the whole food (instead of just the juice) versus a sugar-matched placebo. The researchers used PET scans to track changes in brain metabolism associated with early Alzheimer’s in a group of older adults already suffering from mild cognitive decline. Although the changes couldn’t be picked up on neuropsychological testing, in those early-stage Alzheimer’s regions, the placebo group continued to worsen, but the grape group “was spared such decline,” suggesting a protective effect of grapes. You can see these points illustrated in a graph and brain mapping pictures below and from 5:11 in my video. You can see locations where brain metabolism declined after eating six months of placebo grapes (colored red in the video), compared to the level of decline in a brain after six months of eating actual grapes.
When commercial entities fund studies, it’s more for marketing purposes than science. That doesn’t necessarily mean the findings are invalid, but you do have to pay special attention to things like the framing of the research question, the experimental methods, statistical analysis, biased interpretation of results, or spin.
Teammates remember how much he loved playing for the Mets. A slick-fielding shortstop on the 1969 Miracle Mets World Series team, Harrelson played with pride, passion and with an edge to his game. When the former Mets infielder and manager died at 79 after a battle with Alzheimer’s disease earlier this month, the tributes came pouring in from all over the baseball world.
Even Pete Rose paid tribute to Harrelson, remembering him as a “good guy.” Harrelson, a smaller, scrappier player, infamously took on baseball’s controversial hit king during the 1973 NLCS, starting a scuffle that led to a benches-clearing brawl at Shea Stadium.
Fans remember Harrelson as an affable, friendly face. He sat for long lines of autographs and he posed for photos with kids. Born Derrel McKinley Harrelson, the nickname “Buddy” was apt since everyone who met him felt like he was their buddy.
“Bud was the same friendly giving individual whether you met him at the ballpark or the gas station,” Frank Boulton, his longtime business partner with the Long Island Ducks, told the Daily News.
Make no mistake, while much of his career came in Queens, his influence went far beyond. It extended to those he helped get back into affiliated baseball and it extended to other families affected by Alzheimer’s, with the Harrelson family having helped to raise $61,000 for the Walk to End Alzheimer’s.
With the Mets, Harrelson played in two World Series (1969 and 1973) and coached in another (1986). He managed Mets affiliates in the 1980s and in the big leagues when was named the successor to Davey Johnson in 1990. It was this experience that became key for Harrelson a decade later.
A native of the San Francisco Bay Area, Harrelson made his home on Long Island and it truly did become a home for him. This is why Harrelson brought the Ducks to Long Island and why, after receiving his diagnosis in 2016, he helped raise money for the local chapter of the Alzheimer’s Association.
While his accomplishments later in life may look like a footnote compared to his illustrious Major League career, to him, it was his legacy.
“Bud, on many occasions, claimed the Ducks were the best thing he ever did in professional baseball,” Boulton said. “I truly believe the connection with our fan base was the driving factor. He loved to engage with our fans.”
Bud Harrelson
Boulton founded the Atlantic League in 1998, not long before he was connected with Harrelson.
Independent leagues have come and gone throughout the years, but the Atlantic League has seen considerable success. It can often be seen as a last stop of sorts for players who are unable to get contracts with affiliated teams, but it’s much more than that. Players have parlayed Atlantic League contracts into second chances at affiliated ball, or even a second chance in the big leagues.
The league now works with MLB to test new rules and has even welcomed women onto its teams.
Harrelson’s first foray into minor league ownership was with Boulton. A former trader from Brightwaters, Boulton was introduced to Harrelson in 1991. He previously owned two minor league teams affiliated with the Yankees and Harrelson expressed interest in minor league ownership. The two purchased the Peninsula Pilots, a Class-A Carolina League team, and relocated it to Wilmington Delaware.
Boulton and Harrelson would talk about their desire to bring a minor league team to Long Island on car rides up from Delaware to New York.
“Bud and I, on rides back and forth to Wilmington, knew that if we could bring professional baseball to Long Island it would be successful,” Boulton said. “And 24 years later and 9 million fans through our gates, we accomplished our goal of bringing affordable family entertainment to our friends and neighbors on Long Island.”
Harrelson took great pride in bringing a quality product to his home when the team was founded in 2000. He was the Atlantic League’s first president and the Ducks’ first manager, helping to bring credibility to an emerging team.
Harrelson was a fixture at the ballpark even after he stopped managing. He would make the drive from his home in Hauppauge often, interacting with fans, players and even the mascot, QuackerJack.
“He coached from 2001-2018, he would be the first base coach at home games, catch a ceremonial first pitch from a sponsor, then he would want to go upstairs [with the fans],” said Michael Pfaff, the Ducks president and chief business officer. “He’d go up to the luxury suites and he would take pictures with fans and sign autographs. He would just be everybody’s buddy. He created a tremendous amount of memories.”
Pfaff came to the Ducks in 2022 from the NFL where he worked for the office of the commissioner. When he pulled into the parking lot of the ballpark for his interview, Harrelson was in the parking lot waving to him as if the two had known each other for years.
“But had a very unique talent of making everyone feel like he knew them,” Pfaff said. “From the minute they met him, he made them feel like they had been lifelong friends. And I’m no different in that regard.”
Harrelson kept coming to the ballpark even after his Alzheimer’s diagnosis in 2016, though not as much as he once did. It was around that time that he started going to support group meetings with the Long Island chapter of the Alzheimer’s Association, along with his ex-wife, Kim Battaglia, who became his caretaker. Harrelson didn’t go public with the diagnosis right away, but when he did, he made sure the Alzheimer’s Association was involved.
They got in touch with the chapter’s executive director Doug Davidson, who feared that Harrelson would find out that he was a Chicago Cubs fan during an introductory dinner.
“I was scared out of my mind,” Davidson joked.
Battaglia, Harrelson and his five kids formed “Team Harrelson.” They not only managed his care as the disease progressed but they also got involved with advocacy efforts. Harrelson and Battaglia joined the board of directors and he became a chairman of the walk. The Ducks put together an Alzheimer’s awareness night at the ballpark, where his daughter, Kassandra, “brought down the house” with a speech.
It was so impressive, she ended up becoming the keynote speaker at a caregiver conference.
“The family became so full-on with the mission,” Davidson said. “Bud’s message was that he wanted to help educate others and help spread awareness. I just was blown away that a man who had accomplished all this was helping. It was unfortunate enough to be suffering with this horrible disease, and yet he was still so selfless in wanting to help others.”
A study released last year showed that the east and southeastern U.S. have the highest prevalence of Alzheimer’s disease. In 2023, Suffolk County, where Harrelson resided, ranked 11th of 62 counties with a prevalence rate of 11.7%. More than 30,000 people over the age of 65 are estimated to be living with Alzheimer’s in the county.
Disease doesn’t discriminate. Harrelson might have been a member of the Mets Hall of Fame and a beloved member of his community, and still, Alzheimer’s took hold of him, erasing his memory and his motor functions. What we’re left with is memories of Harrelson.
His memory will live on with the Alzheimer’s Association, with the money he raised helping other families understand how to cope with a terrible disease.
His memory will live on with the Ducks. The team already retired his number in 2018, holding a night dedicated just for him. They plan to play with patches embroidered with No. 3 on them this season. He is still listed as an owner on the team website, along with Boulton and Seth Waugh.
Harrelson made an imprint on New York baseball that few could ever forget.
“The Ducks are part of the fabric of the community that he cared so much about,” Pfaff said. “Providing affordable entertainment in a market where that doesn’t exist is something that is a benefit to the community. It’s a quality of life benefit… We consider it an honor to continue that legacy for as long as the Ducks play.”
Anyone who has had experience with Alzheimer’s disease knows the agony of watching someone fade away as it steals memory and at the end – a person’s own identity. Tonight – we’ll show you an experimental way to try and beat back Alzheimer’s. It’s been tested on just a handful of patients – but it caught our attention because of the doctor involved, Dr. Ali Rezai, who 60 Minutes first met 20 years ago. Dr. Rezai is a neuroscience pioneer who has developed treatments for Parkinson’s disease and other brain disorders. Over the last year we followed this master of the mind as he attempted to delay the progression of Alzheimer’s disease and its worst symptoms using ultrasound. We saw a cutting-edge approach to brain surgery…with no cutting.
Dr. Ali Rezai: If we can, we should not be doing brain surgery.
Sharyn Alfonsi: You’re a brain surgeon!
Dr. Ali Rezai: I am, but I should be out of a job, because brain surgery, it’s cutting the skin, opening the skull. It can be barbaric.
It looked like a scene from a sci-fi movie. A halo wrapped patient, pushed into a tube…as a team of doctors manipulate his brain from the other side of the glass.
Dr. Ali Rezai allowed us to witness his revolutionary attempt to use ultrasound to slow down the cognitive decline in three patients diagnosed with Alzheimer’s disease. It’s never been done before.
Dr. Ali Rezai: There’s no miracle cures here. It’s advancing medicine with calculated risks and pushing the frontiers.
Dr. Rezai and his team are focused on these red patches in the patient’s brain scans. The red indicates the densest beta-amyloid protein. That gummy protein is believed to play a major role in Alzheimer’s by disrupting communication between brain cells.
Dr. Ali Rezai: In people with Alzheimer’s it accumulates much faster. And over time, these protein aggregates, we call them plaques. Like plaques in the arteries, they keep on accumulating and impacting function.
Sharyn Alfonsi and Dr. Ali Rezai
60 Minutes
There are two FDA approved drugs on the market …that can help break up that brain plaque. Aducanumab was approved in 2021…followed by lecanemab last year. Both are given intravenously… but they work slowly.
Dr. Ali Rezai: Typically, you go into the clinic, and you get an IV, and you have the antibody infusion over one to two hours. And you have to do it once a month or twice a month for 18 months and longer. And during those 12 to 18 months, the brain is continuing to progress. Alzheimer’s is not going away.
It takes so long because the drugs have a hard time getting through something called the blood brain barrier. This tight filter of cells line the blood vessels to keep toxins from leaking into the brain…but it also prevents almost all of the medication from getting in too.
Dr. Rezai thought he could solve that problem with ultrasound – the same technology that’s been used for 70 years to give doctors a view of organs and fetal development.
He chose ultrasound because it easily penetrates the skull and can be focused — like sunlight through a magnifying glass – to help open the blood brain barrier and allow the drugs to rush in.
Dr. Ali Rezai: This way we’re getting the payload– the therapeutic payload exactly to the area it needs to go with a high penetration. But we gotta be careful because we wanna be safe about this. You don’t wanna deliver too much. Don’t wanna open the blood-brain barrier too much…
Sharyn Alfonsi: Because if you open it too much, what could happen–
Dr. Ali Rezai: You can get bleeding in the brain, you can get swelling in the brain, you can get many other problems. So you have to get it just right.
We will show you exactly how that worked and the early results in a minute…
But to understand why one of the country’s most accomplished brain surgeons is betting on ultrasound…
You have to go back to 2002…when Dr. Rezai first caught our attention in a story Morley Safer reported on treating Parkinson’s disease.
Dr. Rezai in 2002 Morley Safer piece: “Look up…show me your teeth…stick your tongue out…Very good.”
Dr. Rezai was among the first to implant a pacemaker-type device in the brain which stopped uncontrollable movements suffered by Parkinson’s patients.
Dr. Rezai in 2002 Morley Safer piece: “It’s like traveling through a labyrinth as in the Greek myth and around every corner you have that bloodthirsty monster that can jump on you so you want to be careful to avoid these areas.”
That kind of implant surgery is now routine for advanced Parkinson’s. Dr. Rezai went on to write hundreds of scientific papers, secure dozens of patents and present his Parkinson’s research to Congress and the White House. He could have gone to any big city research center, but, true to form, he chose to try something different and moved to Morgantown, West Virginia – where he is the executive director of the Rockefeller Neuroscience Institute.
Dr. Ali Rezai: It was a fantastic move, because we’re able to achieve so many things that would have been difficult at other institutions. Sometimes in the bigger institutions you may not be hungry as much for it, or you may have a thousand different agendas and priorities. Here we think we have a very nimble and agile team that can quickly get outcomes.
Like in 2019…this is video Dr. Rezai’s team took when they were among the first to use ultrasound to treat tremors. For 15 years, Dan Wahl had been suffering from essential tremor- a neurological disorder.
(2019 RNI video)
Dr. Ali Rezai: You OK?
Dan Wahl: I’m OK.
Dr. Ali Rezai: You got a hat on now. Alright very good.
Rezai’s team focused ultrasound into a part of the brain called the thalamus to destroy a pin-point sized patch of tissue doctors believed was responsible for the tremors.
Dr. Ali Rezai: These are the 980 elements converging right there.
Wahl was awake during the procedure.
Doctor: Touch my finger with your finger…
After two hours, the 71 year old’s tremor was gone.
Dan Wahl: I’m still afraid I’m gonna drop it.
Doctor: You got it!
Dan Wahl: I got it.
Doctor: Really good. Do you wanna show off?
Mrs. Wahl: Praise the lord.
That success helped convince Dr. Rezai that focused ultrasound could be adapted to patients with other brain disorders…including Alzheimer’s disease.
Dan Miller and his wife
60 Minutes
Dan Miller: My first symptoms that I noticed were that I was having trouble typing at work.
Sharyn Alfonsi: Did you think you had Alzheimer’s?
Dan Miller: No. I didn’t
Dan Miller is just 61 years old. His wife Kathy began noticing changes four years ago.
Kathy Miller: He kinda hid it pretty well. And then I noticed he was– having trouble– his clothes would be backwards and those kinds of things.
Sharyn Alfonsi: Just little things.
Kathy Miller: Just little things. Yes.
A scan of his brain…revealed what Dan had been hiding. The red spots indicated a build up of those beta-amyloid proteins…the so-called brain plaque…a marker of Alzheimer’s. Dr. Rezai explained to Miller he couldn’t cure him of the disease, but he hoped to slow its progression.
Sharyn Alfonsi: Why take part in the trial if it’s not a cure?
Dan Miller: I have to explain to you that I was at the point, you know, like in Dante’s “Inferno” where– where it says, “Abandon all hope, (laugh) you who enter here.” For me it was just– you know, let’s do this. You know? What do I have to lose?
Here’s how it worked. Hours before the procedure, Miller was given an IV treatment of aducanumab, one of those two new drugs to reduce beta-amyloid plaque.
Miller was then fitted with this million dollar helmet…similar to the one the team used to treat tremor patients. it directs nearly a thousand beams of ultrasound energy at a target the size of a pencil point.
Dr. Ali Rezai: Basically a patient lies on the MRI table and the head goes inside the helmet and the patient is immobilized with a halo or with a mouthpiece because we don’t want movements to cause errors in our targeting in the brain.
Once inside, the MRI machine gave Dr. Rezai a 3D-view of the plaque he would target in Dan Miller’s brain. The next step was an IV solution that contained microscopic bubbles. When hit with ultrasound energy, the bubbles pry open that blood brain barrier.
Dr. Ali Rezai: The bubbles start vibrating.
Sharyn Alfonsi: They’re moving.
Dr. Rezai and Sharyn Alfonsi
60 Minutes
Dr. Ali Rezai: They’re moving. They start expanding so you can open the barrier temporarily. Now it’s open for 24 to 48 hours and then it reseals. So this gives you a tremendous opportunity for 24 to 48 hours with the barrier being open so now therapeutics can get inside the brain.
You can’t hear ultrasound…that noise is a signal to tell Rezai’s team the ultrasound is doing its work.
Dr. Ali Rezai: Each dot represents an area where all the waves– all the ultrasound waves converge and open the blood-brain barrier.
Sharyn Alfonsi: So this is just one blast, if you will?
Dr. Ali Rezai: One blast getting there.
Sharyn Alfonsi: And you’re hitting one point?
Dr. Ali Rezai: One point, and then it moves to the next one.
Even though patients were awake, they told us they didn’t feel a thing. It all took a couple of hours and they went home when it was over. The three patients were given the treatments of ultrasound with infusion once a month over six months. The result: beta-amyloid plaque targeted with ultrasound were reduced 50% more than areas treated by infusion alone. Dr. Rezai shared the three patients’ brain scans with us.
Dr. Ali Rezai: And the red indicates more density of beta amyloid plaques in the brain so you can see as you treat it with ultrasound…
Look closely at the areas outlined in white that were targeted with ultrasound and the drug.
Dr. Ali Rezai: You get reduction.
Sharyn Alfonsi: Whoa.
Dr. Ali Rezai: Right there–
Sharyn Alfonsi: That’s after?
Dr. Ali Rezai: That’s after. You can see the plaques are very significantly reduced by opening the blood-brain barrier just in one — area.
Dr. Ali Rezai
60 Minutes
Dan Miller and the third patient in the trial had larger areas of their brain targeted with ultrasound.
Dr. Ali Rezai: And this is his baseline and then you can see here after–
Sharyn Alfonsi: Wow.
Dr. Ali Rezai: –26 weeks, there’s a very dramatic reduction in the beta amyloid in the areas as outlined by this white mark.
Sharyn Alfonsi: And now we’re gonna look at patient number three.
Dr. Ali Rezai: And this patient underwent antibody infusion therapy plus ultrasound. You can see this area–
Sharyn Alfonsi: Wow.
Dr. Ali Rezai: –which is really amazing. The ultrasound opened the blood-brain barrier and the antibody went in faster and cleaned out the plaques.
Sharyn Alfonsi: What was your reaction when you saw this scan?
Dr. Ali Rezai: Uh. I mean, my jaw dropped. I’m like, “Whoa.” I– I was actually even in the clinic seeing patients and the PET scan technician called and said– “Oh yeah, there’s a big change.” I’m like, “How do you know? We have to analyze it.” He was like, “No, you can see it on the screen.” So…
Sharyn Alfonsi: What did you think when Dr. Rezai shared the scans with you?
Dan Miller: It was surreal.
Sharyn Alfonsi: You can really see it. You don’t have to be a doctor to understand what’s going on there.
Kathy Miller: No. Absolutely not.
Kathy Miller says she can see it in her husband, too…who slips up once in a while…but hasn’t slipped further away.
Kathy Miller: He has trouble finding things. I’ll send him into the kitchen to get somethin’ and he’s like, “It’s not there.” And like, “Yes, it is. I can see it.” But he can’t see it. But if that’s the worst, that’s nothing.
Sharyn Alfonsi: You’ll take it.
Kathy Miller: I’ll take it.
Sharyn Alfonsi: You feel hopeful about the future?
Dan Miller: I do. Yes. I learned that what I needed to do is accept that the old Dan is gone and then– start working on the new me, which has a future.
Dr. Rezai’s team told us there has been no change in the ability of the three patients to do their daily activities since the ultrasound treatments ended in July.
Now that Dr. Rezai has shown focused ultrasound can clear beta-amyloid plaques faster, he has FDA approval to use ultrasound to try and restore brain cell function lost to Alzheimer’s.
Sharyn Alfonsi: What’s the result of breaking up all those plaques to the damage that’s already been done to the brain?
Dr. Ali Rezai: We don’t know if it’s gonna reverse the damage to the brain, because Alzheimer’s, the underlying cause is still occurring. So we have another study that we’re looking at with ultrasound. First, clear the plaques. Then deliver ultrasound in a different dose to see now if we can reverse it or boost the brain more for people with Alzheimer’s.
The human brain contains 100 billion neurons. That’s as many cells as there are stars across the milky way. Dr. Ali Rezai has spent 25 years exploring this frontier of medicine. The surgical techniques and therapies he pioneered are in use around the world. Dr. Rezai allowed us to see his latest research over the last year at the Rockefeller Neuroscience Institute in Morgantown, West Virginia. It includes revolutionary treatments for a brain disease suffered by 24 million Americans – addiction. The results so far have been life changing for the people we met once trapped by drugs.
Gerod Buckhalter: Looking back, I didn’t have a chance.
Sharyn Alfonsi: What do you mean you didn’t have a chance?
Gerod Buckhalter: I couldn’t do anything without having that drug–um in my system.
Sharyn Alfonsi with Gerod Buckhalter
60 Minutes
Gerod Buckhalter is the son of a coal miner. At 6 foot 3, he was a high school football standout…who dreamed of playing wide receiver at Penn State…but after a shoulder injury, he got hooked on painkillers.
Gerod Buckhalter: The very first time that I– that I took that first pill, um — I– I knew that I wanted that feeling for the rest of my life.
Sharyn Alfonsi: What did it feel like?
Gerod Buckhalter: It’s just pure euphoria.
He took us to where he said he often went to buy drugs, including heroin.
Gerod Buckhalter: Everybody in Morgantown knows to come here. I was probably 17, 18 years old…you know…just a kid.
Buckhalter still looks like an athlete…it’s hard to imagine he was an addict for more than 15 years. He told us he does not remember how many times he overdosed and that he couldn’t stay clean for more than four days at a time.
Gerod Buckhalter: I didn’t know where I was gonna sleep some nights. You know, my family didn’t want me around anymore. I just– I did so many things to hurt them that, you know, it was just too much for them to deal with.
Four years ago, a psychologist who’d worked with Buckhalter introduced him to Dr. Ali Rezai, who was gearing up to perform a new kind of brain surgery to treat severe addiction.
Dr. Ali Rezai: Our protocol was people that have failed everything.
Sharyn Alfonsi: Once you’ve tried everything.
Dr. Ali Rezai: Everything. Residential programs, multiple failures, detox multiple times, outpatient, inpatient, multiple overdoses.
Gerod Buckhalter: I think he classified it as– end-stage drug user.
Sharyn Alfonsi: I mean, end stage makes you think that this is the end of your life.
Gerod Buckhalter: Correct. And hearing that at the age of 34 um, it – it was crazy.
Dr. Rezai thought he might be able to adapt technology he helped develop years earlier to treat Parkinson’s disease to treat people with severe addiction.
Dr. Ali Rezai: We’ve been able to map out with neuroscience imaging there’s a specific part of the brain that is electrically and chemically malfunctioning that is associated with addiction.
Sharyn Alfonsi: So it’s not just willpower. It’s what’s happening in the brain.
Dr. Ali Rezai: It’s a brain disease, it’s an electrical and chemical abnormality in the brain that occurs over time with recurrent use of drugs. And this can be any substance, alcohol, can be opioids, amphetamines, cocaine and they all are involving the same part of the brain.
Sharyn Alfonsi: And so your idea was what with the implant?
Dr. Ali Rezai: Parkinson’s we implant that in the movement part of the brain that is electrically malfunctioning causing shaking. In this case, we’re going in the behavioral regulation, anxiety, and craving parts of the brain.
Dr. Rezai has seen the impact of addiction in his community. The problem is so severe in Morgantown…a vending machine dispenses the overdose antidote narcan for free.
The National Institute on Drug Abuse agreed to support Dr. Rezai’s attempt to fight addiction with a brain implant. In 2019, the FDA gave him a green light to attempt the groundbreaking surgery.
That is Gerod Buckhalter. He agreed to be the first addiction patient in the U.S. to get the implant. Dr. Rezai’s team interviewed him the day before the surgery.
Gerod Buckhalter (during Rockefeller Neuroscience Institute pre-surgery interview): “The best outcome possible would be just to cut the cravings out, make me feel a little bit better. If you know, if those couple of things happen you know…that’s all I could possibly ask for.”
Gerod Buckhalter: At that time I was so desperate for a better life that I was willing to do just about anything and I signed up to do it.
Sharyn Alfonsi: I think some people might look at this and think, “An electronic implant in the brain sounds a little creepy.”
Dr. Ali Rezai: People maybe 50 years ago, they say “A implant in the heart sounds creepy.” Now it’s, like, normal. Twenty-five years ago, people are saying, “What are you doing? You’re putting an implant in the brain for Parkinson’s?” but now it’s routine part of standard of care for advanced Parkinson’s.
This is video from the seven-hour procedure. A surgery so new…it didn’t have a name yet. Dr. Rezai opened a nickel-sized hole in burkhalter’s skull. then he directed a thin wire with four electrodes deep inside.
Sharyn Alfonsi: Gerod was awake during the surgery. Why was that necessary?
Dr. Ali Rezai: To map the brain we have tiny microphones the size of a hair we put inside the brain. And they’re going slowly with micro-robots. They go at increments of a thousandth of a millimeter. Very slow, we drive them into the brain, and we’re listening to the neurons talking to each other. In addiction, we want to find the area in the reward center, so that confirms where we are in the brain. Once we listen, we say, “Okay, that’s the right sound,” then we put the final therapeutic pacemaker.
Sharyn Alfonsi: What does it sound like?
Dr. Ali Rezai: Static electricity, which may be electricity to you but its music to my ears.
Music because, Dr. Rezai says, it’s a signal that he found the right spot in the brain for the implant.
Once in place, the wire was connected to a device placed below the collarbone.
The electrical pulses it sends to the brain are intended to suppress cravings. Buckhalter said it was painless. Post surgery, the system is adjusted remotely with a tablet computer as needed.
Gerod Buckhalter: When they turned the– the unit on it was an immediate change.
Sharyn Alfonsi: What was the change?
Gerod Buckhalter: Just felt better. You know, just felt like I did prior to ever using drugs, but a little bit better. And it was at that point that I knew that I was gonna have a legitimate shot at doing well.
In all – four patients with severe drug addiction had the implant surgery. One had a minor relapse. Another dropped out of the trial completely. But two have been drug free since their operations, including Gerod Buckhalter, whose been clean for four years.
Sharyn Alfonsi: If you hadn’t met Doctor Rezai, if you hadn’t gone through this implant, do you think you’d be sitting here talking to me today?
Gerod Buckhalter: You may be talking to my parents you know, those that have lost their– their loved ones to a drug overdose, but you wouldn’t be talking to me. There’s– there’s no doubt about that.
The surgery was a success but opening someone’s skull is always risky. Dr. Rezai thought he could reach more patients quickly if he used ultrasound. He was already using it to treat other brain disorders…and was convinced focused ultrasound could target the same area of the brain as the implant.
Sharyn Alfonsi: Is this brain surgery without a knife?
Dr. Ali Rezai: It is, indeed. So this is, there’s no skin cutting. There’s no opening the skull. So it is brain surgery without cutting the skin, indeed.
Dr. Rezai explained how his team would be the first to treat addicts by aiming hundreds of beams of ultrasound to a precise point deep inside the brain.
Dr. Ali Rezai: So the area that we’re treating is the reward center in the brain, which is the nucleus accumbens, which is right down at the base of this dark area. And then we deliver– ultrasound waves to that specific part of the brain, and we watch how acutely, on the table your cravings and your anxiety changes in response to ultrasound.
Sharyn Alfonsi: How is the ultrasound making a change here?
Dr. Ali Rezai: Ultrasound energy is changing the electrical and chemical milieu, or activity, in this structure in the brain involving addiction and cravings.
Sharyn Alfonsi: Just resetting them and giving them kind of a fresh start?
Dr. Ali Rezai: At this point, it seems like the brain is being reset, or rebooting of the brain, and the cravings are less, they are managed, anxiety is better. So now that allows them to interact with the therapist. It’s very important to know that this is not a cure, but an augmentation of the therapy by reducing the cravings and anxiety that’s so overwhelming that the therapist has difficulty working with the patient.
Last February, we watched Dr. Rezai use focused ultrasound to treat Dave Martin who told us he has been surrounded by friends and family who use drugs his whole life.
Dave Martin
60 Minutes
Sharyn Alfonsi: When did you start using drugs?
Dave Martin: When I was seven years old.
Sharyn Alfonsi: Seven?
Dave Martin: Yes. I did drugs for 37 years.
Sharyn Alfonsi: What kind of drugs were you using?
Dave Martin: Anything I could get my hands on.
Inside the MRI, Martin was shown these images of drug use to stoke his cravings.
A simultaneous brain scan allowed Dr. Rezai and his team to immediately spot the area in the nucleus accumbens that was most active.
90-watts of ultrasound energy were beamed at a target the size of a gumdrop.
Within minutes, we noticed Martin’s foot – that had been anxiously bouncing – was still. And he told Rezai’s team that those same images of drugs he was shown earlier, were now… not sparking the need for a fix.
Dave Martin: The day of the procedure, it was the best day of my life. I didn’t experience the same effect as, like, the times before —
Sharyn Alfonsi: You didn’t feel like, “I need that.” I want that —
Dave Martin: No. I didn’t feel like I needed the urge or the desire to use wasn’t there anymore.
Dr. Ali Rezai: So within 15 to 20 minutes of treatment, the craving and anxiety melts away, and we’re seeing this pattern in multiple instances.
Sharyn Alfonsi: Then they can walk away after this? There’s no–
Dr. Ali Rezai: They get off the table and go home.
Sharyn Alfonsi: And how long does this entire procedure take?
Dr. Ali Rezai: One hour.
Sharyn Alfonsi: One hour.
Dr. Ali Rezai: One hour.
Sharyn Alfonsi: Have you been around people still using drugs?
Dave Martin: Yes, yes, unfortunately, I have. Um.
Sharyn Alfonsi: And what happens?
Dave Martin: It didn’t even trigger me. I used to use intraven– intravenously with needles and… It was a little while ago not too far back but this one individual was tryin’ to hit theirself. And they couldn’t hit. And they asked me, “Can– can you hit me?”
Sharyn Alfonsi: So you actually put drugs into this person?
Dave Martin: Yeah, I actually -stuck them, drew the blood back. You know, now before when I drew blood back, it would, like, make– make me sweat ’cause I couldn’t wait to hit myself. but this time it was just like god I hope they don’t OD and I kill them here you know. But I didn’t have any urges or desire or anything, so.
Dr. Rezai’s team told us Dave Martin did admit to taking one painkilling pill at a party in December. Still — 10 of the 15 patients in the ultrasound clinical trials have remained completely drug free.
Dr. Ali Rezai is trying the same ultrasound therapy on 45 more addiction patients and is already thinking about expanding the use of ultrasound to help people with other brain disorders including post traumatic stress disorder and obesity.
Dr. Ali Rezai: This is serious business, research that’s never been done before. We have to learn more. We have to replicate our findings.
Sharyn Alfonsi: Is there any risk at running towards something quickly?
Dr. Ali Rezai: There’s always risk, but you cannot advance and make discoveries without risk. But we need to push forward and take the risk, because people with addiction and Alzheimer’s is not going away, it’s here so why wait ten, 20 years? Do it now.
Produced by Guy Campanile and Lucy Hatcher. Broadcast associate, Erin DuCharme. Edited by Jorge J. García.
Hope is on the horizon for millions of Alzheimer’s disease patients as scientists develop a new target for Alzheimer’s treatment: the immune system.
Alzheimer’s affects roughly 5.8 million Americans, according to the Centers for Disease Control and Prevention (CDC). The progressive disease is the most common form of dementia and is associated with memory loss and cognitive decline in regions of the brain involved in thought, memory and language.
Scientists believe that Alzheimer’s is caused by the abnormal buildup of proteins in and around the brain cells, but exactly what triggers this is still unclear.
Today, there is no known cure for Alzheimer’s. However, new medications may offer relief to patients and slow the disease’s progression. And our body’s immune system can help with this.
“There are many approaches that are in various stages of development that target the immune system, which is now known to play a key role in Alzheimer’s disease,” Todd Golde, a professor of pharmacology, chemical biology and neurology at Emory University, told Newsweek.
One particularly exciting approach involves the use of antibodies that can target and bind to the abnormal protein clumps that form in the brain. “This results in clearance or reduction of [the protein clumps],” Golde said.
Golde and colleague Allan Levey have summarized this approach in a recently published perspective in the journal Science.
Precisely what mediates this interaction is still unknown, but Golde said that the brain’s private squad of immune cells may play an important role. These cells, called microglia, are found exclusively in the brain and central nervous system and can engulf problematic proteins and infectious particles like bacteria. Therefore, researchers believe that the antibodies may act as little molecular flags to signal to the microglial cells that a mess needs cleaning up—a mess in the form of an Alzheimer ‘s-associated protein clump.
Based on clinical trials, these antibodies offer a very promising avenue for future treatments.
“These treatments slow decline in the very earliest symptomatic stages of Alzheimer’s disease on average by about 25 to 30 percent over 18 months of treatment,” Golde said. “Notably, the antibodies show quite remarkable impacts on amyloid deposits [aka the protein clumps] themselves.”
Unlike previous therapies designed to ease symptoms and boost cognitive function, Golde said that these antibodies represent the first therapies capable of altering the course of the disease.
“Having a disease-modifying therapy (like this) is in some ways a game changer for Alzheimer’s disease, as it says that we can alter the course of this devastating disease and slow it down,” Golde said. “This is just a start, and that either improved versions of these therapies, other types of disease-modifying therapies, or combination therapies will likely in the future lead to treatments with bigger impacts, halting or preventing disease.”
Artist’s impression of a nerve cell surrounded by antibodies. Antibody treatments may be the future of Alzheimer’s therapy. peterschreiber.media/Getty
Two of the antibodies used in these trials have already been FDA approved; the third is expected to be approved in 2024. However, care still needs to be taken over their use.
“Because of potential for side effects, the need to treat patients early in the symptomatic phase of the disease in individuals [and] the fact that they are currently given through multiple IV infusions and require careful monitoring, there are some barriers to widespread use [of these antibodies],” Golde said. “Indeed, there is appropriate caution among most clinicians to ensure that the right patients most likely to benefit from these therapies are treated.”
Golde stresses that, while these results are fascinating, we are still a long way from effectively treating Alzheimer’s.
“Though this represents an initial success, huge unmet medical need remains,” he said. “We need continuing investment in the public and private sectors to ensure that we can meet that need and build off this initial, but limited, success.”
Is there a health issue that’s worrying you? Do you have a question about Alzheimer’s? Let us know via health@newsweek.com. We can ask experts for advice, and your story could be featured on Newsweek.
Uncommon Knowledge
Newsweek is committed to challenging conventional wisdom and finding connections in the search for common ground.
Newsweek is committed to challenging conventional wisdom and finding connections in the search for common ground.
Ketogenic diets are put to the test for diabetes reversal.
As you can see at the start of my video Does a Ketogenic Diet Help Diabetes or Make It Worse?, ketogenic diets can lower blood sugars better than conventional diets. So much so, in fact, that there is a keto product company that claims ketogenic diets can “reverse” diabetes. However, they are confusing the symptom (high blood sugars) with the disease (carbohydrate intolerance). People with diabetes can’t properly handle carbohydrates, and this manifests as high blood sugars. Clearly, if you stick to eating mostly fat, your blood sugars will stay low, but you may be actually making the underlying disease worse at the same time.
We’ve known for nearly a century that if you put people on a ketogenic diet, their carbohydrate intolerance can skyrocket within just two days. Below and at 0:46 in my video, you can see a graph from the study showing the blood sugar response two days after eating sugar. On a high-carb diet, blood sugar response is about 90 mg/dL. But, the blood sugar response to the same amount of sugar after a high-fat diet is about 190 mg/dL, nearly double. The intolerance to carbohydrates skyrocketed on a high-fat diet.
After one week on an 80 percent fat diet, you can quintuple your blood sugar spike in reaction to the same carb load compared to a week on a low-fat diet, as you can see in the graph below and at 1:12 in my video.
Even a single day of excessive dietary fat intake can do it, as you can see in the graph below and at 1:26 in my video. If you’re going in for a diabetes test, having a fatty dinner the night before can adversely affect your results. Just one meal high in saturated fat can make carbohydrate intolerance, the cause of diabetes, worse within four hours.
Given enough weight loss by any means, whether from cholera or bariatric surgery, type 2 diabetes can be reversed, but a keto diet for diabetes may not just be papering over the cracks, but actively throwing fuel on the fire.
I’ve been trying to think of a good metaphor. It’s easy to come up with things that just treat the symptoms without helping the underlying disease, like giving someone with pneumonia aspirin for their fever instead of antibiotics. However, a keto diet for diabetes is worse than that because it may treat the symptoms while actively worsening the disease. It may be more like curing the fever by throwing that pneumonia patient out into a snow bank or “curing” your amputated finger by amputating your hand. One of the co-founders of masteringdiabetes.org suggested it’s like a CEO who makes their bad bottom line look better by borrowing tons of cash. The outward numbers look better, but on the inside, the company is just digging itself into a bigger hole.
Do you remember The Club, that popular car anti-theft device that attaches to the steering wheel and locks it in place so the steering column can only turn a few inches? Imagine you’re in a car at the top of a hill with the steering wheel locked. Then, the car starts rolling down the hill. What do you do? Imagine there’s also something stuck under your brake pedal. The keto-diet equivalent response to this situation is who cares if you’re barreling down into traffic with a locked steering wheel and no brakes—just stick to really straight deserted roads without any stop signs or traffic lights. If you do that, problem solved! The longer you go, the more speed you’ll pick up. If you should hit a dietary bump in the road or start to veer off the path, the consequences could get more and more disastrous over time. However, if you stick to the keto straight and narrow, you’ll be a-okay! In contrast, the non-keto response would be to just unlock the steering wheel and dislodge whatever’s under your brake. In other words, fix the underlying problem instead of just whistling past—and then into—the graveyard.
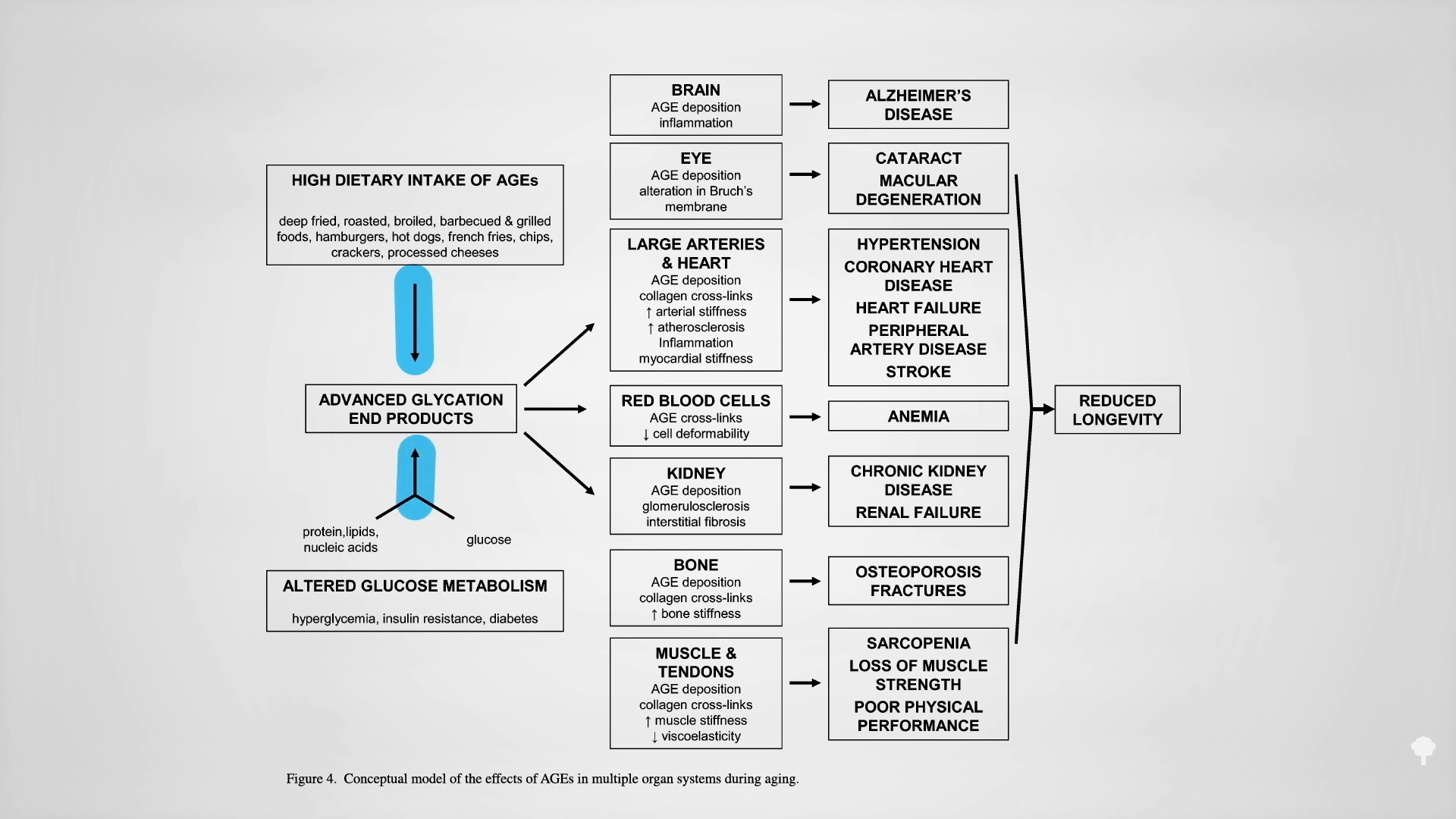
The reason keto proponents claim they can “reverse” diabetes is they can successfully wean type 2 diabetics off their insulin. That’s like faith-healing someone out of the need for a wheelchair by making them stay in bed the rest of their life. No need for a wheelchair if you never move. Their carbohydrate intolerance isn’t gone. Their diabetes isn’t gone. In fact, it could be just as bad or even worse. Type 2 diabetes is reversed when you are weaned off insulin while eating a normal diet like everyone else. Then and only then do you not have diabetes anymore. A true diabetes reversal diet, as you can see below and at 4:58 in my video, is practically the opposite of a ketogenic diet: getting diabetics off their insulin within a matter of weeks by eating more than 300 grams of carbs a day! The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal is the most potent creator of advanced glycation end products (AGEs), which are implicated in degenerative diseases—from Alzheimer’s and cataracts to kidney disease and strokes, as you can see below and at 5:31 in my video.
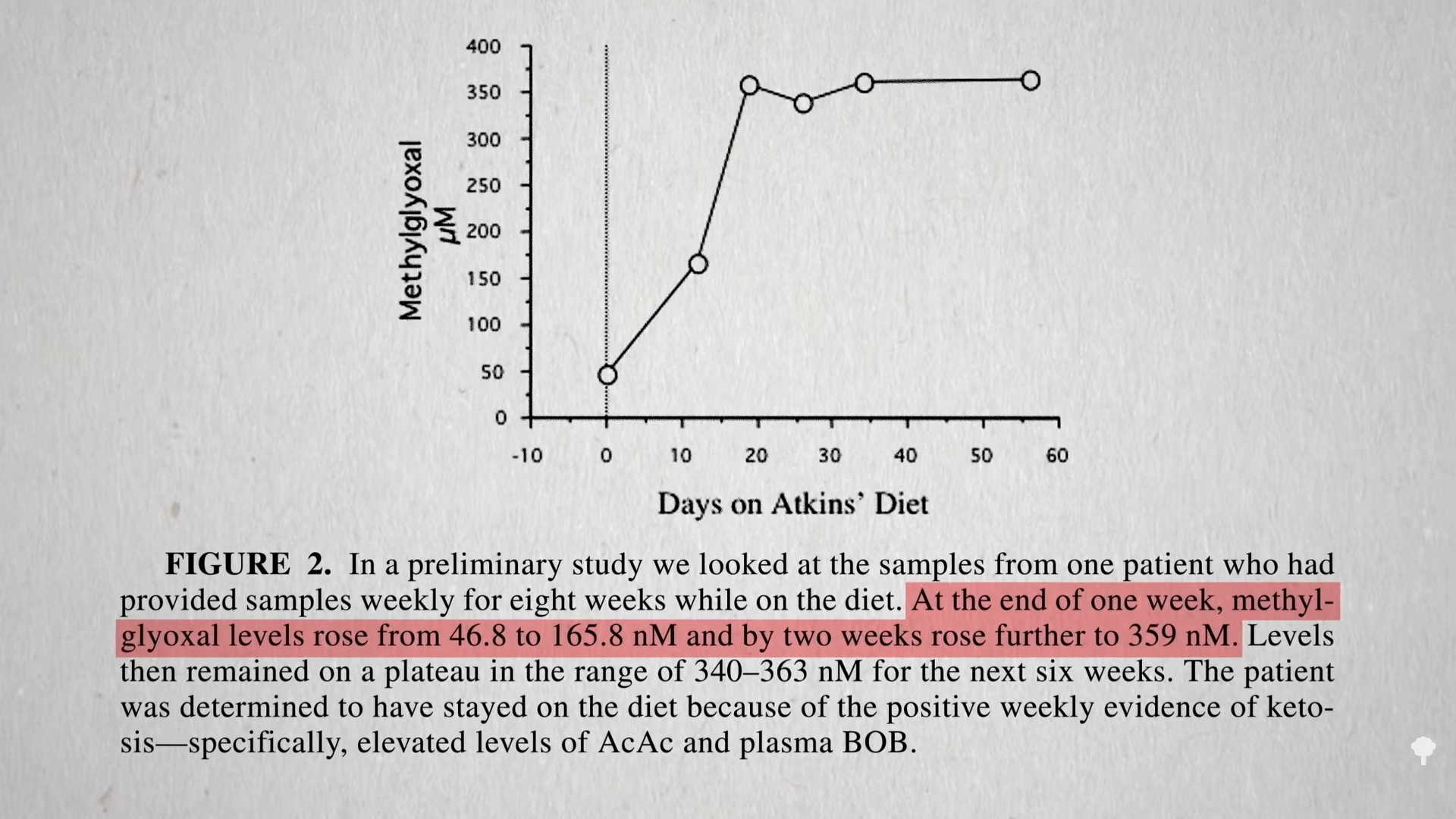
You get AGEs in your body from two sources: You can eat them preformed in your diet or make them internally from methylglyoxal if you have high blood sugar levels. On a keto diet, one would expect high exposure to preformed AGEs, since they’re found concentrated in animal-derived foods high in fat and protein, but we would expect less internal, new formation due to presumably low levels of methylglyoxal, given lower blood sugars from not eating carbs. Dartmouth researchers were surprised to find more methylglyoxal! As shown in the graph below and at 6:11 in my video, a few weeks on the Atkins diet led to a significant increase in methylglyoxal levels. Those in active ketosis did even worse, doubling the level of this glycotoxin in their bloodstream.
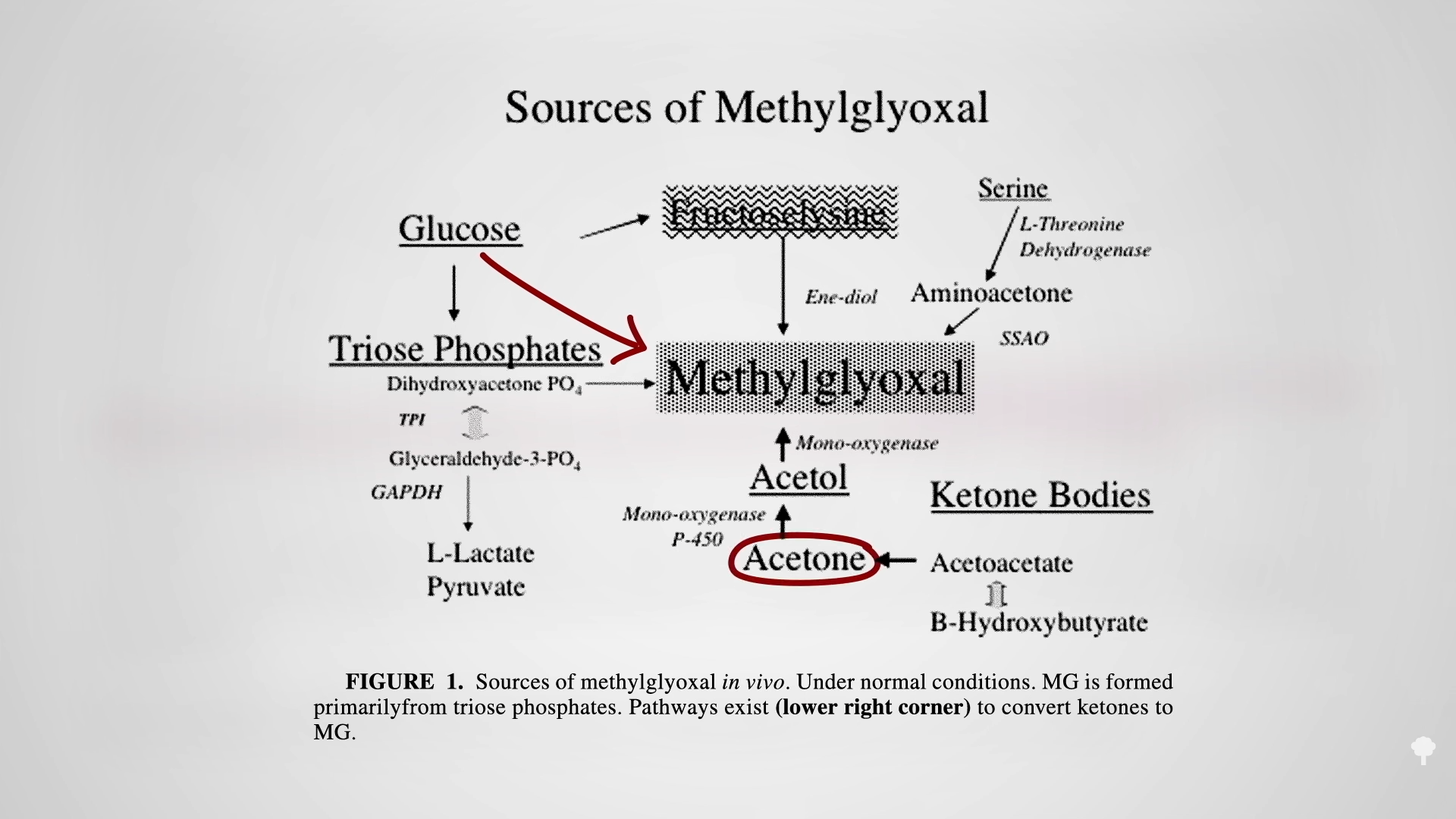
It turns out that high sugars may not be the only way to create this toxin, as you can see below and at 6:24 in my video. One of the ketones you make on a ketogenic diet is acetone (known for its starring role in nail polish remover). Acetone does more than just make keto dieters fail breathalyzer tests, “feel queasy and light-headed, and develop what’s been described as ‘rotten apple breath.’” Acetone can oxidize in the blood to form acetol, which may be a precursor for methylglyoxal.
That may be why keto dieters can end up with levels of this glycotoxin as high as those with out-of-control diabetes, which can cause the nerve damage and blood vessel damage you see in diabetics. That’s another way keto dieters can end up with a heart attack. The irony of treating diabetes with a ketogenic diet may extend beyond just making the underlying diabetes worse, but by mimicking some of the disease’s dire consequences.
This is part of a seven-video series on keto, which you can find in related videos below.
Cannabidiol, or CBD, is known and widely used for a wide array of potential benefits, including pain relief, sleep, stress and anxiety relief, its anti-seizure properties — the list goes on. While the non-psychotropic cannabinoid already boasts a number of positive effects, could preventing and alleviating Alzheimer’s disease be among them?
According to a new study, the prospects are looking strong.
By 2050, the number of people over the age of 65 with Alzheimer’s could grow to a projected 12.7 million, according to the Alzheimer’s Association, underscoring the need to explore potential options to alleviate or prevent the disease. Currently, there are no cures for Alzheimer’s, though some medications can provide relief and mitigate symptoms.
Alzheimer’s is progressive disease characterized by changes in the brain, resulting in distorted and lost memory along with other important mental processes over time.
So where exactly does CBD fit in? Researchers from China Pharmaceutical University took a closer look at the neuroprotective and anti-inflammatory mechanisms of the cannabinoid in their study titled “Assessing Cannabidiol as a Therapeutic Agent for Preventing and Alleviating Alzheimer’s Disease Neurodegeneration,” published in the journal Cells.
They found that CBD may enhance cognitive function and offer protection against the protein Aβ1–42, a biomarker associated with the onset of Alzheimer’s. Aβ42 is also related to other similar conditions and symptoms like mild cognitive impairment and vascular dementia.
CBD’s Anti-Inflammatory, Neurological Benefits and Alzheimer’s
Authors note that CBD may specifically work against Alzheimer’s, given the role that neuroinflammation plays in ongoing synaptic and neuronal damage. CBD is already well known for its anti-inflammatory properties, so researchers conducted experiments on mice to model Alzheimer’s disease using Aβ1–42. They also utilized an RNA-seq analysis to further understand some of the actions CBD may have to offer when it comes to Alzheimer’s.
Ultimately, they found that CBD did not cause significant damage or cell death. Instead, CBD appeared to counteract cognitive and memory impairments induced by Aβ1–42.
Researchers administered Aβ1–42 to the mice, which were then put to the Morris water maze test. This test is often used to assess spatial learning, cognitive functions and memory in rodents.
Those mice treated with Aβ1–42 took longer to complete the maze, indicating increased cognitive issues. After being treated with CBD, it took mice significantly less time to escape, implying better cognitive function. CBD also helped to combat the negative impacts Aβ1–42 had on learning over a five-day period.
Additionally, researchers looked at the navigation patterns of mice, concluding that CBD had the potential to boost spatial memory among Alzheimer’s models.
Promising Findings Show the Need for Expanded Research
“Our findings suggest CBD’s efficacy in moderating microglial and astrocytic activation, offering anti-inflammatory benefits that protect synaptic function and alleviate AD-associated cognitive deficits,” authors note. “Our data support CBD’s potential therapeutic role in countering AD-related neuroinflammation.”
Along with demonstrating CBD’s ability to counteract certain cognitive impairments caused by Aβ1–42, researchers said the study left them with “invaluable insights” surrounding CBD’s role in modulating critical genes within the inflammatory reaction, “underscoring its robust anti-inflammatory potential.”
They also note that the equivalent dose for humans from the study is about 115 mg of CBD, which would make it a viable oral supplement. Still, researchers reference that the potential role of CBD in combating Alzheimer’s “remains conspicuously absent from contemporary guidelines.”
“Our research substantiates CBD’s efficacy in either preventing or mitigating the effects of AD. Thus, future formulations of CBD supplements might be strategically positioned to include indications for AD prevention and alleviation, expanding its therapeutic repertoire,” the study concludes.
Alzheimer’s and Cannabinoids: An Emerging Field of Research
While it may still be limited in the grand scheme, the exploration of cannabinoids and Alzheimer’s isn’t brand new. Denver-based MedPharm Holdings received funding in 2022 to move forward to study cannabinoids as they relate to neuropharmacology, specifically Alzheimer’s.
Other research has noted the “promising” potential that cannabinoids like CBD hold when it comes to Alzheimer’s and dementia-related symptoms, specifically citing findings in rodent models showing the effect of cannabinoids in reducing amyloid plaque deposition and stimulating hippocampal neurogenesis.
A Toronto-based biotech company is also researching the potential of new pharmaceutical formulations of the psychedelic drug Dimenthyltryptamine (DMT).
Japan’s health ministry has approved Leqembi, a drug for Alzheimer’s decease that was jointly developed by Japanese and U.S. pharmaceutical companies
ByMARI YAMAGUCHI Associated Press
September 26, 2023, 2:18 AM
TOKYO — Japan’s health ministry has approved Leqembi, a drug for Alzheimer’s disease that was jointly developed by Japanese and U.S. pharmaceutical companies. It’s the first drug for treatment of the disease in a country with a rapidly aging population.
Developed by Japanese drugmaker Eisai Co. and U.S. biotechnology firm Biogen Inc., the drug’s approval in Japan comes two months after it was endorsed by the U.S. Food and Drug Administration.
Leqembi is for patients with mild dementia and other symptoms in the early stages of Alzheimer’s disease, and the first medicine that can modestly slow their cognitive decline.
Prime Minister Fumio Kishida, who announced Japan’s approval of Leqembi on Monday, called it “a breakthrough” and said that the “treatment of dementia has now entered a new era.”
Kishida has pledged to step up support for the growing number of dementia patients and their families and is due to launch a panel this week to discuss measures for a dementia-friendly society.
According to the health ministry, Japan’s number of dementia patients who are 65 years of age or older will rise to 7 million in 2025, from the current 6 million.
The drug, however, does not work for everyone and — as with other Alzheimer’s drugs that target plaques in the brain — can cause dangerous side effects such as brain swelling and bleeding in rare cases.
Eisai said it will conduct a post-marketing special use survey in all patients administered the drug until enough data is collected from unspecified number of patients under Japanese health ministry procedures.
The drug will be partially covered by health insurance and is expected to be ready for clinical use by the end of the year. The price is yet to be decided but is expected to be expensive, Kyodo News agency reported.
Eisai is committed to delivering Leqembi to people who need it and their families “as a new treatment,” said Haruo Naito, the company’s CEO.
“We aim to create impact on issues surrounding dementia in Japanese society,” he said.
The first drug purporting to slow the advance of Alzheimer’s disease is likely to cost the U.S. health care system billions annually even as it remains out of reach for many of the lower-income seniors most likely to suffer from dementia.
Medicare and Medicaid patients will make up 92% of the market for lecanemab, according to Eisai Co., which sells the drug under the brand name Leqembi. In addition to the company’s $26,500 annual price tag for the drug, treatment could cost U.S. taxpayers $82,500 per patient per year, on average, for genetic tests and frequent brain scans, safety monitoring, and other care, according to estimates from the Institute for Clinical and Economic Review, or ICER. The FDA gave the drug full approval July 6. About 1 million Alzheimer’s patients in the U.S. could qualify to use it.
Patients with early Alzheimer’s disease who took lecanemab in a major clinical trial declined an average of five months slower than other subjects over an 18-month period, but many suffered brain swelling and bleeding. Although those side effects usually resolved without obvious harm, they apparently caused three deaths. The great expense of the drug and its treatment raises questions about how it will be paid for, and who will benefit.
“In the history of science, it’s a significant achievement to slightly slow down progression of dementia,” said John Mafi, a researcher and associate professor of medicine at the David Geffen School of Medicine at UCLA. “But the actual practical benefits to patients are very marginal, and there is a real risk and a real cost.”
To qualify for Leqembi, patients must undergo a PET scan that looks for amyloid plaques, the protein clumps that clog the brains of many Alzheimer’s patients. About 1 in 5 patients who took Leqembi in the major clinical test of the drug developed brain hemorrhaging or swelling, a risk that requires those taking the drug to undergo frequent medical checkups and brain scans called MRIs.
In anticipation of additional costs from the Leqembi drug class, the Centers for Medicare & Medicaid Services in 2021 increased monthly premiums for Medicare patients by 15%, and premiums may rise again in 2024 after a slight decline this year.
Such increases can be a significant burden for many of the 62 million Medicare subscribers who live on fixed incomes. “Real people will be affected,” Mafi said. He contributed to a study that estimated lecanemab and related care would cost Medicare $2 billion to $5 billion a year, making it one of the most expensive taxpayer-funded treatments.
In its analysis, ICER suggested that Leqembi could be cost-effective at an annual price of $8,900 to $21,500. In an interview, David Rind, ICER’s chief medical officer, said $10,000 to $15,000 a year would be reasonable. “Above that range doesn’t seem like a good place,” he said.
The Alzheimer’s drug Leqembi
EISAI / Handout via Reuters
Whatever its price, patients may be delayed getting access to Leqembi because of the relative shortage of specialists capable of managing the drug, which will require genetic and neuropsychological testing as well as the PET scan to confirm a patient’s eligibility. A similar drug, Eli Lilly’s donanemab, is likely to win FDA approval this year.
Already there are long waits for the testing needed to assess dementia, Mafi said, noting that one of his patients with mild cognitive impairment had to wait eight months for an evaluation.
Such testing is not readily at hand because of the paucity of effective treatment for Alzheimer’s, which has helped to make geriatrics a relatively unappealing specialty. The United States has about a third as many dementia specialists per capita as Germany, and about half as many as Italy.
“Time is of the essence” for the neuropsychological testing, Mafi said, because once a patient’s cognitive ability declines below a certain threshold, they become ineligible for treatment with the drug, which was tested only in patients in the earliest stages of the disease.
Mafi’s study estimates that patients will have to pay about $6,600 out-of-pocket for each year of treatment. That could put it out of reach for many of the 1 in 7 “dual eligible” Medicare beneficiaries whose income is low enough to simultaneously qualify them for state Medicaid programs. Those programs are responsible for about 20% of physician bills for drug infusions, but they don’t always cover the full amount.
Some practitioners, such as cancer centers, cover their Medicaid losses by receiving higher rates for privately insured patients. But since almost all lecanemab patients are likely to be on government insurance, that “cross-subsidization” is less of an option, said Soeren Mattke, director of the Center for Improving Chronic Illness Care at the University of Southern California.
This poses a serious health equity issue because “dual eligibles are low-income patients with limited opportunities and education, and at higher risk of chronic illnesses including dementia,” Mattke said in an interview. Yet many doctors may not be willing to treat them, he said. “The idea of denying access to this group is just appalling.”
Eisai spokesperson Libby Holman said the company was reaching out to specialists and primary care physicians to make them aware of the drug, and that reimbursement options were improving. Eisai will provide the drug at no cost to patients in financial need, she said, and its “patient navigators” can help lock down insurance coverage.
“A lot of clinicians are excited about the drug, and patients are hearing about it,” said David Moss, chief financial officer of INmune Bio, a company that has another Alzheimer’s drug in development. “It’s a money center for infusion centers and MRI operators. It provides reasons for patients to come into the office, which is a billing thing.”
Outstanding doubts about Leqembi and related drugs have given urgency to efforts to monitor patient experiences. CMS is requiring Leqembi patients to be entered into a registry that tracks their outcomes. The agency has established a registry, but the Alzheimer’s Association, the leading advocacy group for dementia patients, is funding its own database to track those being treated, offering physician practices $2,500 to join it and up to $300 per patient visit.
In a letter to CMS on July 27, a group of policy experts said CMS should ensure that any and all Leqembi registries create and share data detailed enough for researchers and FDA safety teams to obtain a clear picture of the drug’s real-world profile.
The anti-amyloid drugs like lecanemab have created a polarized environment in medicine between those who think the drugs are a dangerous waste of money and those who believe they are a brilliant first step to a cure, said ICER’s Rind, who thinks lecanemab has modest benefits.
“People are as dug in on this as almost anything I’ve ever seen in medicine,” he said. “I don’t think it’s healthy.”
KFF Health News, formerly known as Kaiser Health News (KHN), is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
NEW YORK — What do Paul McCartney, Queen Latifah, Lady Gaga and Stevie Wonder have in common?
Oh, and Aretha Franklin, k.d. lang, Bono and Billy Joel. Not to mention Carrie Underwood, Judy Garland, John Legend and Placido Domingo. And let’s not forget…
Stop. Listing all of the musicians who performed duets with Tony Bennett would take up our remaining space. His place in music history is already secure.
Bennett, who died at 96 on Friday, was indeed “the last of the great saloon singers of the mid-20th century,” as Charles J. Gans wrote for The Associated Press. Yet that summation befits a man frozen in time, consigned to a specific era, and Tony Bennett was anything but that.
Instead, Bennett transcended generations in a way few musicians have.
He was rightly beloved by older listeners for the way he interpreted the works of songwriters Irving Berlin, Cole Porter, Jerome Kern and George Gershwin in a strong and stalwart voice that remained true into his 90s. He was influenced by and helped popularize jazz, and marched with the Rev. Martin Luther King to fight for civil rights.
He was also admired by those who, if they left their hearts in San Francisco, it was at the corner of Haight-Ashbury, or a trendy dance club.
“I have to think it comes down to the man itself,” said singer Ben Folds, at age 56 four decades younger than Bennett was at the end.
“You hear his voice, it’s super kind, casual and in the moment,” Folds said. “His phrasing is that way, too. There’s nothing that sounds uptight. It’s very generous. A lot of people in his generation didn’t have that appeal because at the end of the day, you didn’t feel that they cared about you.”
Many of Bennett’s successful late-career duets were a tribute to the savvy marketing of his son and manager, Danny, who kept his dad’s career going long past most peers hit their expiration date.
But famous duet partners could have said no. Few did.
Don’t think they didn’t notice the sweet and tender manner he brought to the studio working with people like Lady Gaga and Amy Winehouse, Folds said. Bennett’s duet with Winehouse on “Body and Soul” was the last studio recording she made before she died.
Gaga, the New Yorker born Stefani Germanotta who could appreciate the New Yorker born Anthony Benedetto, became like family and ushered him through musical triumphs with love even as he suffered from Alzheimer’s Disease. Bennett drew and signed an image of Miles Davis’ trumpet that Gaga wears as a tattoo on her arm.
k.d. lang’s formidable voice bowed to no one when she brought it to a series of memorable performances with Bennett in the 1990s.
“He was a place of refuge for the American songbook,” lang told the Associated Press. “He made sure that he loved a song. He would not sing any song that he didn’t love.”
Make no mistake: Bennett brought the goods. Watch a video of him coming on to a Shea Stadium stage to sing “New York State of Mind” with Billy Joel. His guest steals the song, and Joel beams as he watches.
His handiwork has just been blessed by Tony Bennett.
At a San Francisco fundraiser a few years ago, with Alzheimer’s insidious impact already apparent, Folds watched stunned as Bennett switched from remarks to a few bars of “I Left My Heart in San Francisco,” in perfect pitch.
Bennett exuded an older generation’s class, always performing in a tuxedo or tailored suit. In a Los Angeles hotel room in 1994 when an earthquake hit before dawn, Bennett took the time to change into a suit before joining bathrobe-wearing evacuees, the Los Angeles Times noted.
In all of the work he did with contemporary artists, he never sounded age inappropriate, said music critic Jim Farber. Bennett always bent them to his musical will, never the other way around, he said.
“There’s this multitude of singers, from Gaga to Diana Krall to John Mayer,” lang said. “Now they can carry a certain understanding that they received firsthand from him.”
Something more important was usually happening in the audience.
Two years ago, writer Christine Passarella recalled sitting in lawn chairs in a Brooklyn park in the 1980s with her mother and baby daughter, listening to Bennett sing.
“Seeing him live felt like watching an uncle embracing me and my mom, as his music helped us remember my father, my mom’s one and only love,” she wrote.
Countless numbers of people remember similar moments with family over the years, hearing Bennett’s voice wash warmly over them while sitting with a mother or father, a son or daughter. I’m among them.
That is, ultimately, a legacy to be treasured above all.
___
This story corrects Bennett’s age at death to 96, not 95.
When Tony Bennett and Lady Gaga released their first album together in 2014, some may have found them an unlikely pair. But the singers had gotten close and continued to create music as a duo, with Gaga even crediting Bennett, who died on Friday at age 96, with “saving” her.
“Six months ago I didn’t even want to sing anymore,” Gaga, whose real name is Stefani Germanotta, told Parade Magazine in 2014 during an interview with Bennett as they promoted their album “Cheek to Cheek.”
“Do you know what Duke Ellington said? He said, ‘Number one, don’t quit. Number two, listen to number one,’” Bennett quipped.
“Right! The other day, Tony said, ‘I’ve never once in my career not wanted to do this.’ It stung. Six months ago I didn’t feel that way. I tell Tony every day that he saved my life,” Gaga replied.
It appears the pressure of the music industry had gotten to Gaga, who released her album “Art Pop” the previous year.
“I’m not going to say any names, but people get irrational when it comes to money—with how they treat you, with what they expect from you,” she told Parade. “But if you help an artist, it doesn’t give you the right, once the artist is big, to take advantage of them.”
“I was so sad. I couldn’t sleep. I felt dead,” she said. “And then I spent a lot of time with Tony. He wanted nothing but my friendship and my voice.”
Bennett held Gaga’s hand and replied: “I understand.”
“It meant a lot to me, Tony. I don’t have many people I can relate to,” she said.
Lady Gaga performs with Tony Bennett during her residency at Park Theater at Park MGM on January 20, 2019 in Las Vegas, Nevada.
Kevin Mazur/Getty Images for Park MGM Las Vegas
While many call the pop superstar “Gaga,” Bennett referred to her as “Lady.” After “Cheek to Cheek,” the pair recorded a second album, “Love for Sale,” released in 2021. Gaga also honored Bennett at the Grammy’s in 2022, singing the tracks “Love for Sale” and “Do I Love You” solo, because Bennett had retired after being diagnosed with Alzheimer’s disease at 94.
“Love for Sale” was the last project Bennett released. In 2021, he and Gaga put on a sold-out performance at Radio City Music Hall in New York City and broadcast on CBS.
Bennett had been diagnosed with Alzheimer’s by then, but when he sang, he came alive, his accompanist Lee Musiker and Gaga both said in an interview with Anderson Cooper for “60 Minutes.”
“When that music comes on (SNAP), it’s– something happens to him,” Gaga said. “He knows exactly what he’s doing. And what’s important for me, actually, just to make sure that I don’t get in the way of that.”
Bennett died in New York City at the age of 96 on Friday. Over his decades-long career, Bennett recorded 60 studio albums, plus dozens of live albums and compilations. Seven of his albums hit the Top 10 on the Billboard charts.
He won 19 Grammy Awards. One of them was with Gaga for Best Traditional Pop Vocal Album for “Cheek to Cheek.”
The eastern and southeastern United States have the highest prevalences of Alzheimer’s dementia, according to new research released Monday at the Alzheimer’s Association International Conference in Amsterdam.
The study, by researchers at Rush Medical College in Chicago, includes county-level estimates of Alzheimer’s rates among adults age 65 and older in all 3,142 U.S. counties.
Medicare last week agreed to cover the new drug Leqembi, the first medication proven to slow the progression of Alzheimer’s disease, following the U.S. Food and Drug Administration’s green light of the pricey drug.
The decision was cheered by the Alzheimer’s Association and others who advocate for the 6.7 million U.S. seniors with the progressive disease, which has no cure and which primarily affects people over the age of 65.
The approval to cover the drug is significant because the vast majority of Americans with Alzheimer’s get their health coverage through Medicare. Yet some patients and families could still face hurdles in getting access to the medication. For one, Medicare — the health care plan for people who are 65 years and older — won’t cover the entire cost of the drug.
Secondly, Leqembi, pronounced “leh-KEM-bee,” might not be appropriate or even accessible for every patient, according to experts.
Here’s what to know about the drug.
What is Leqembi’s price?
Leqembi, from drugmakers Eisai and Biogen, is priced at about $26,500 for a typical year’s worth of treatment.
What is the out-of-pocket cost for Medicare enrollees?
Medicare on Thursday noted that enrollees in its Original Medicare will have to pay a co-payment of 20% of the cost of the drug, after meeting their deductible.
That means that people on Original Medicare could pay about $5,000 out of pocket annually for Leqembi, according to health-care research group KFF.
Medicare Advantage enrollees typically also pay 20% of drugs’ costs, up to their plan’s out-of-pocket maximum, KFF noted, which means that people on these plans may also face high out-of-pocket costs for the medication.
That could prove unaffordable for many Medicare enrollees, as more than half earn less than $30,000 annually.
Will the Inflation Reduction Act help lower costs for Leqembi?
The Inflation Reduction Act, signed into law last year by President Joe Biden, has a provision to cap out-of-pocket drug costs for Medicare recipients at $2,000 starting in 2025 — but unfortunately, the new law won’t do anything to help patients who are prescribed Leqembi.
That’s because the IRA targets drug costs prescribed through Medicare’s Part D, the section that generally covers prescription drugs. But Leqembi is approved under Medicare’s Part B, the part of the insurance plan that covers doctor’s services.
Part B covers drugs that generally administered in a doctor’s office, like Leqembi, and therefore are considered a doctor’s service.
That means the IRA cost-capping provision won’t apply to Leqembi’s out-of-pocket costs.
Who is eligible for Leqembi?
Medicare said it will approve coverage of the drug for enrollees:
Who have been diagnosed with “mild cognitive impairment or mild Alzheimer’s disease dementia”
And who have documented evidence of beta-amyloid plaque, which is present in people with Alzheimer’s, on the brain
And whose doctor participates in a qualifying registry and who has an appropriate clinical team and follow-up care
That means patients with Alzheimer’s or impairment beyond the early stages may not be approved for the medication.
How do patients document beta-amyloid plaque?
Typically, patients will need to undergo additional tests to determine if they have the plaque, which are pieces of protein that band together between neurons in the brain. These tests include either a PET scan or a lumbar puncture, otherwise known as a spinal tap.
“It’s also not clear if insurers will pay for the brain scans and other services necessary to administer the drug,” Dr. Mallika Marshall told CBS Boston.
How is the drug administered?
Patients taking Leqembi must have it administered intravenously in their doctor’s office, according to Medicare.
“Patients have to get an infusion every 2 weeks for 18 months, in order to slow the progression of the disease by about 6 months,” Marshall told CBS Boston.
What are the side effects of Leqembi?
“Some patients will experience brain bleeding or swelling” as a side effect, Dr. Marshall said.
Other reported side effects are infusion-related reactions and headaches, according to the Alzheimer’s Association. In a Leqembi study by drugmaker Eisai, 13% of drug recipients had swelling and 17% has small brain bleeds.
“Some patients and families may decide that the benefits don’t outweigh the possible risks,” Dr. Marshall added.
WASHINGTON — U.S. officials granted full approval to a closely watched Alzheimer’s drug on Thursday, clearing the way for Medicare and other insurance plans to begin covering the treatment for people with the brain-robbing disease.
The Food and Drug Administration endorsed the IV drug, Leqembi, for patients with mild dementia and other symptoms caused by early Alzheimer’s disease. It’s the first medicine that’s been convincingly shown to modestly slow the cognitive decline caused by Alzheimer’s.
Japanese drugmaker Eisai received conditional approval from the FDA in January based on early results suggesting Leqembi worked by clearing a sticky brain plaque linked to the disease.
The FDA confirmed those results by reviewing data from a larger, 1,800-patient study in which the drug slowed memory and thinking decline by about five months in those who got the treatment, compared to those who got a dummy drug.
“This confirmatory study verified that it is a safe and effective treatment for patients with Alzheimer’s disease,” said FDA’s neurology drug director, Dr. Teresa Buracchio, in a statement.
The drug’s prescribing information will carry the most serious type of warning, indicating that Leqembi can cause brain swelling and bleeding, side effects that can be dangerous in rare cases. The label notes that those problems are seen with other plaque-targeting Alzheimer’s drugs.
The process of converting a drug to full FDA approval usually attracts little attention. But Alzheimer’s patients and advocates have been lobbying the federal government for months after Medicare officials announced last year they wouldn’t pay for routine use of drugs like Leqembi until they receive FDA’s full approval.
There were concerns that the cost of new plaque-targeting Alzheimer’s drugs could overwhelm the program’s finances, which provide care for 60 million seniors. Leqembi is priced at about $26,500 for a year’s supply of IVs every two weeks.
The vast majority of Americans with Alzheimer’s get their health coverage through Medicare. And private insurers have followed its lead by withholding coverage for Leqembi and a similar drug, Aduhelm, until they receive FDA’s full endorsement. An FDA decision on full approval for Aduhelm is still years away.
Medicare administrator, Chiquita Brooks-LaSure, said in a statement Thursday the program will begin paying for the drug now that it has full FDA approval. But the government is also setting extra requirements, including enrollment in a federal registry to track the drug’s real-world safety and effectiveness.
Medicare “will cover this medication broadly while continuing to gather data that will help us understand how the drug works,” Brooks-LaSure said.
Some Medicare patients could be responsible for paying the standard 20% of the cost of Leqembi, though the amount will vary depending on their plans and other coverage details.
Hospitals and medical clinics have cautioned that it may take time to get people started on the drug.
Doctors need to confirm that patients have the brain plaque targeted by Leqembi before prescribing it. Nurses need to be trained to administer the drug and patients must be monitored with repeated brain scans to check for swelling or bleeding. The imaging and administration services carry extra costs for hospitals beyond the drug itself.
Eisai has told investors that about 100,000 Americans could be diagnosed and eligible to receive Leqembi by 2026. The drug is co-marketed with Cambridge, Massachusetts-based Biogen.
“We want to ensure that appropriate patients only are the ones that get this product,” said Alexander Scott, a vice president with Eisai.
Eisai studied the drug in people with early or mild disease who were evaluated using a scale measuring memory, thinking and other basic skills. After 18 months, those who got Leqembi declined more slowly — a difference of less than half a point on the scale — than participants who received a dummy infusion. Some Alzheimer’s experts say that delay is likely too subtle for patients or their families to notice.
But federal health advisers said the difference could still be meaningful and recommended that FDA fully approve the drug at a public meeting in June.
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Science and Educational Media Group. The AP is solely responsible for all content.
“Today’s action is the first verification that a drug targeting the underlying disease process of Alzheimer’s disease has shown clinical benefit in this devastating disease,” Teresa Buracchio, acting director of the Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release.
Leqembi, from drugmakers Eisai and Biogen, is the first medication that’s been shown to slow the progression of Alzheimer’s disease, including declines in memory and thinking, by targeting the disease’s underlying biology.
“Today marks a breakthrough in the treatment of Alzheimer’s disease, and we are proud to be at the forefront of ushering in a new era of advances for a disease that was previously considered untreatable,” Biogen president and CEO Christopher A. Viehbacher said in a statement.
He said the company will be “working alongside Eisai with the goal of making [Leqembi] accessible to eligible patients as soon as possible.”
The Alzheimer’s drug Leqembi is seen in this undated handout photo.
EISAI Handout via Reuters
The FDA’s initial approval in January was based on one mid-stage study in 800 people with early signs of Alzheimer’s who were still able to live independently or with minimal assistance. Eisai later published the results of a larger 1,800-patient study that the FDA assessed as part of the full approval process.
The larger study tracked patients’ results on an 18-point scale measuring memory and other cognitive functions. Results showed a difference of less than half a point after 18 months, sparking debate over whether this qualifies as a meaningful improvement.
According to the latest news release, the decision was unanimous, with all committee members voting that the study results verified the drug’s benefit. Buracchio noted in her statement: “This confirmatory study verified that it is a safe and effective treatment for patients with Alzheimer’s disease.”
“This drug is not a cure. It doesn’t stop people from getting worse, but it does measurably slow the progression of the disease,” Dr. Joy Snider, a neurologist at Washington University in St. Louis, told The Associated Press in January. “That might mean someone could have an extra six months to a year of being able to drive.”
Snider said that Leqembi (pronounced “leh-KEM-bee”) also comes with downsides, including the need for twice-a-month infusions and possible side effects like brain swelling. Other reported side effects are infusion-related reactions and headaches, according to the Alzheimer’s Association.
Access is another issue, with the drug expected to be priced at about $26,500 for a typical year’s worth of treatment, without insurance.
On Thursday, the head of the Centers for Medicare and Medicaid Services, Chiquita Brooks-Lasure, pledged to “cover this medication broadly while continuing to gather data that will help us understand how the drug works” — a decision that will make it more affordable for many. Brooks-Lasure called the FDA’s approval “welcome news for the millions of people in this country and their families who are affected by this debilitating disease.”
Her office had previously said it expected to extend coverage once full FDA approval was granted.
The FDA defines Alzheimer’s disease as “an irreversible, progressive brain disorder affecting more than 6.5 million Americans that slowly destroys memory and thinking skills and, eventually, the ability to carry out simple tasks.”
In a news release from the initial approval, the FDA called the medication “an important advancement in the ongoing fight to effectively treat Alzheimer’s disease.”
“Alzheimer’s disease immeasurably incapacitates the lives of those who suffer from it and has devastating effects on their loved ones,” Dr. Billy Dunn, former director of the Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in the release. “This treatment option is the latest therapy to target and affect the underlying disease process of Alzheimer’s, instead of only treating the symptoms of the disease.”
The decision on Leqembi follows controversy over the FDA’s handling of a previous Alzheimer’s drug, Aduhelm, which was also developed by Biogen and Eisai. Aduhelm won approval in 2021 despite warnings from independent medical advisers that it had not been shown to be effective and carried significant risks. The FDA later updated labeling to significantly limit the drug’s use.
Alex Tin contributed reporting. The Associated Press also contributed to this report.
The Food and Drug Administration on Thursday approved the Alzheimer’s treatment Leqembi, a pivotal decision that is expected to expand access to the expensive drug for older Americans.
Medicare has promised to start covering Leqembi, with some conditions, on the same day the FDA approves the antibody treatment. Leqembi is made by Japanese pharmaceutical company Eisai and its Cambridge, Massachusetts, partner, Biogen.
Leqembi is the first Alzheimer’s antibody treatment to receive full FDA approval. It is also the first such drug that is expected to receive broad coverage through Medicare.
Medicare coverage is a crucial step to help older Americans with early Alzheimer’s disease pay for the treatment. With a median income of about $30,000, most people on Medicare cannot afford the $26,500 annual price of Leqembi set by Eisai without insurance coverage.
Leqembi is not a cure. The treatment slowed cognitive decline from early Alzheimer’s disease by 27% over 18 months during Eisai’s clinical trial. The antibody, administered twice monthly through intravenous infusion, targets a protein called amyloid that is associated with Alzheimer’s disease.
Joanna Pike, president of the Alzheimer’s Association, the lobby group that advocates on behalf of people living with the disease, said although Leqembi is not a cure, it will help patients in the early stages of the disease maintain their independence, conduct their daily lives, and spend more time with their families.
“This gives people more months of recognizing their spouse, children and grandchildren,” Pike said in a statement Thursday. “This also means more time for a person to drive safely, accurately and promptly take care of family finances, and participate fully in hobbies and interests.”
But the treatment carries serious risks of brain swelling and bleeding. Three patients who participated in Eisai’s study died. FDA scientists have said it is unclear if Leqembi played a role in these deaths.
Alzheimer’s disease is the most common cause of dementia among older adults and the sixth leading cause of death in the U.S., according to the FDA.
Dr. David Knopman, a neurologist who specializes in Alzheimer’s disease at the Mayo Clinic in Minnesota, said Leqembi clearly demonstrated a benefit to patients in Eisai’s trial, though he cautioned the efficacy of the treatment was modest.
Knopman said appropriately diagnosed and informed patients should be able to decide for themselves whether they want to take Leqembi after weighing the benefits and risks of the treatment as well as the potential logistical challenges of finding a place to receive the twice-monthly infusions.
Medicare plans to impose conditions on how it will cover Leqembi. Patients enrolled in Medicare who are diagnosed with early Alzheimer’s disease will have to find a health-care provider participating in a registry system that collects real-world data on the drug’s benefits and risks.
The system is controversial. The Alzheimer’s Association and some members of Congress are worried this requirement will create barriers to treatment.
There are concerns that the number of health-care providers participating in such registries will be limited, and that people in rural towns and other underserved communities will have to travel long hours to find such a provider.
The Centers for Medicare and Medicaid Services has promised to set up a nationwide portal that will make it easy for health-care providers to submit the required data on patients receiving Leqembi. The agency has said the free-to-use portal will be available when the FDA approves the treatment.
CNBC Health & Science
Read CNBC’s latest health coverage:
Rep. Anna Eshoo of California, the ranking Democrat on the House Subcommittee on Health, and Rep. Nanette Barragan, D-Calif., raised concerns in a letter to CMS last month that patients could struggle to find a doctor participating in the system.
Alzheimer’s is typically diagnosed with the help of a PET scan to detect the amyloid protein associated with the disease or in some cases with a spinal tap. Medicare currently only covers one PET scan per lifetime for dementia. It is unclear if the program plans to change that policy.
There’s also concern that there could be too few specialist physicians and locations to administer the infusions if Leqembi is broadly embraced as a treatment and patient demand for the antibody is high.
Some studies have estimated that wait times for antibody treatments like Leqembi could range from months to even years over the next decade depending on demand.
Tomas Philipson, who advised the FDA commissioner and CMS administrator during the second Bush administration, said the registry is an unnecessary hurdle and Medicare should drop it, but he doesn’t believe the requirement will create an insurmountable barrier to patients accessing Leqembi.
If demand for Leqembi is high, doctors will have an incentive to participate in the registry and the drug companies will want to help, said Philipson, an expert on health-care economics at the University of Chicago.
How high demand will be for Leqembi is uncertain, he said. Families worried about the serious side effects may opt not to take the treatment, while others will decide the benefits outweigh those risks, he said.
Leqembi’s price tag and the treatment’s benefit-risk profile are also controversial.
Patients could still face up to $6,600 in annual out-of-pocket costs for Leqembi even with Medicare coverage, according to a study published in the journal JAMA Internal Medicine. The treatment could cost Medicare up to $5 billion a year depending on how many people receive the infusions, the study estimated.
Sen. Bernie Sanders, I-Vt., chair of the Senate Health Committee, has called Leqembi’s price “unconscionable” and in a letter last month asked Health and Human Services Secretary Xavier Becerra to take action to reduce the cost.
Sanders said patient out-of-pocket costs for Leqembi would amount to a sixth of many seniors’ total annual income and noted the high cost of the treatment could increase premiums for everyone on Medicare.
Eisai says its $26,500 annual list price for Leqembi is lower than the company’s estimate of $37,600 for the total value of the treatment for each patient. The Institute for Clinical and Economic Review, a nonprofit that analyzes health-care costs, estimated in April it should be priced at $8,900 to $21,500 per year.
Philipson said delaying Medicare coverage of Leqembi would result in increased health-care spending as people with mild Alzheimer’s disease, which can be managed at home, progress to more serious disease that requires expensive nursing home care.
Philipson and his colleagues at the University of Chicago estimated that delaying Medicare coverage of Alzheimer’s antibody treatments by one year would result in $6.8 billion in increased spending. By 2040, health-care spending would rise by $248 billion.
Thursday’s full FDA approval comes after a panel of six outside advisors voted unanimously in June in support of the drug’s clinical benefit to patients. The panel was unusually small because some members recused themselves due to conflicts of interest.
The American Academy of Neurology stated in a February letter to CMS that there is a consensus among its experts that Eisai’s clinical trial of Leqembi was well designed and the results were “clinically and statistically significant.”
Some nonprofit groups such as Public Citizen, a consumer advocacy organization, strongly opposed FDA approval of Leqembi. A representative from Public Citizen told the advisory panel that the evidence for the drug’s benefit does not outweigh significant risks of brain swelling and bleeding.
And representatives from the National Center for Health Research and Doctors for America, also nonprofits, told the panel that Eisai’s clinical trial did not include enough Black patients, who are at higher risk for Alzheimer’s disease.
Leqembi has technically been approved for the U.S. market since January, when the FDA cleared the treatment under an accelerated pathway. The FDA uses expedited approvals to save time and get drugs to patients suffering from serious diseases more quickly.
But Medicare refused to cover the Leqembi at that time, asking for more evidence that the expensive treatment had a real clinical benefit for patients that outweighed the risks.
The program’s cautious coverage policy stems from the FDA’s controversial 2021 approval of another Alzheimer’s antibody treatment called Aduhelm, also made by Eisai and Biogen.
The FDA’s advisory committee declined to endorse Aduhelm because the data did not support a clinical benefit to patients. Three advisors resigned after the agency’s decision to approve the treatment anyway.
Knopman is one of the advisors who resigned over the FDA’s decision on Aduhelm. He said the data for Leqembi is different. Eisai conducted a clean trial that showed the antibody had a modest clinical benefit for patients, Knopman said.
An investigation by Congress subsequently found that the FDA’s approval of Aduhelm was “rife with irregularities.”
Sanders, in his letter to Becerra, said the FDA “has a special responsibility to restore the public trust after its inappropriate relationship with Biogen during the agency’s review of a prior Alzheimer’s drug, Aduhelm.”
The U.S. Food and Drug Administration on Thursday granted full approval to the Biogen BIIB and Eisai Co. Ltd. ESALF Alzheimer’s treatment Leqembi, a step that secures Medicare reimbursement for the first drug shown to slow the progress of the disease, rather than just treating its symptoms.
Leqembi, also known as lecanemab, is a monoclonal antibody designed to reduce the buildup of amyloid beta plaque in the brain, a marker of Alzheimer’s disease.
Jack Hanna’s family recently spoke about his Alzheimer’s diagnosis for the first time publicly. The zookeeper and media personality’s family spoke to The Columbus Dispatch about the disease, which affects cognitive function and memory, saying it has progressed to the point where Hanna doesn’t know most of his family.
Hanna, who served as director of the Columbus Zoo from 1978 to 1992, first had symptoms of the disease in 2017. The 76-year-old had a long career as media personality, appearing as an animal expert on talk shows and hosting his own syndicated shows like “Jack Hanna’s Animal Adventures.”
Alzheimer’s is the most common form of dementia, a term that describes a group of symptoms including memory loss and loss of other cognitive abilities, according to the Alzheimer’s Association. While it mainly affects adults 65 and older, it is not a normal part of aging. The disease usually progresses, with late-stage Alzheimer’s patients sometimes unable to carry on a conversation.
About 55 million people in the world have Alzheimer’s, and there is no direct cause but genetics may be a factor, according to the association. There is no cure for the disease, but there are treatments such as medication, which Hanna’s family says he takes to help combat symptoms.
This year, an experimental Alzheimer’s drug by Eli Lilly, donanemab, showed 35% less decline in thinking skills in patients receiving the infusions.
The Hanna family said in tweets they welcomed the Dispatch into their Montana home “for a real-world look into living with Alzheimer’s disease.”
1. We welcomed the @DispatchAlerts into our home for a real-world look into living with Alzheimer’s disease. While Dad/Jack is still mobile, his mind fails him, the light in his eyes has dimmed, and we miss who he was each & every moment of the day. https://t.co/ssU7hE2W7r
“While Dad/Jack is still mobile, his mind fails him, the light in his eyes has dimmed, and we miss who he was each & every moment of the day,” they wrote.
Hanna was officially diagnosed with Alzheimer’s in 2019, and retired from the zoo in 2020, shortly after his final stage performance with animals.
“He would have worked until the day he died. He only retired due to the Alzheimer’s,” his daughter, Kathaleen, told the Dispatch. “He was embarrassed by it. He lived in fear the public would find out.”
Suzi said it “killed her” to break her promise and go public about his diagnosis. But still, Hanna doesn’t know his family told the public, they said.
Before his diagnosis, Hanna showed signs of memory loss – sometimes forgetting what city he was in or the names of animals he had with him during stage performances.
Since then, his Alzheimer’s has advanced, his family said. “He just stopped remembering who I was in all ways,” his daughter, Suzanne, said on the phone during the Dispatch interview. “Whether it was in person or by phone, he had no idea I was his daughter.”
When his other daughter, Julie, was diagnosed with a tumor, Hanna didn’t fully understand what was happening to her.
Kathaleen explained why the family is now sharing his story.
“If this helps even one other family, it’s more than worth sharing dad’s story,” she said. “He spent a lifetime helping everyone he could. He will never know it or understand it, but he is still doing it now.”
The family said on Twitter they have no plans for additional interviews.
FREDERICKSBURG, Va. — Constance Guthrie is not yet dead, but her daughter has begun to plan her funeral.
It will be, Jessica Guthrie says, in a Black-owned funeral home, with the songs of her ancestors. She envisions a celebration of her mother’s life, not a tragic recitation of her long decline.
As it should be. Constance has lived 74 years, many of them good, as a Black woman, a mother, educator and businesswoman.
But she will die of Alzheimer’s disease, a scourge of Black Americans that threatens to grow far worse in coming decades.
Black people are more likely to develop Alzheimer’s than white people in the United States. They are less likely to be correctly diagnosed, and their families often struggle to get treatment from a medical system filled with bias against them.
About 14% of Black people in America over the age of 65 have Alzheimer’s, compared with 10% of white people, according to the Centers for Disease Control and Prevention. The disparity is likely even more, because many Black people aren’t correctly diagnosed.
And by 2060, cases are expected to increase fourfold among Black Americans.
While some risk factors may differ by race, the large disparities among racial groups can’t be explained just by genetics.
The problems start much earlier in life. Health conditions like heart disease and diabetes are known risk factors. Both are more common among Black populations, because of where they live in relation to polluting industries, lack of healthy food choices, and other factors. Depression, high blood pressure, obesity and chronic stress can also raise the likelihood of developing Alzheimer’s. So can poverty.
Across the board, Black people don’t receive the same quality of health care throughout life as white people.
So they don’t get high quality treatment — or any treatment — for all those conditions that are risk factors. Then, at the end, they’re less likely to get medication to ease the symptoms of Alzheimer’s and dementia-related disorders.
And there’s the insidious impact of a life experiencing racism.
Racism is trauma that can lead to increased stress, which can in turn cause health problems like inflammation, which is a risk factor for cognitive decline, said Dr. Carl V. Hill, chief diversity, equity and inclusion officer of the Alzheimer’s Association.
“But because of this structural racism that creates poor access to health, medication, housing, those who experience racism and discrimination are not provided a pathway to lower their risk,” Hill said.
It is, he said, “a one-two punch.”
For Jessica, it has meant the final years of her mother’s life have been filled not with peace, but heartache and frustration, as she navigates doctors who don’t believe her when she says her mom is suffering. In the slow, plodding walk that is her mother’s final years, she has few health care partners.
“It has been pervasive across multiple doctors, emergency rooms and hospital doctors,” Jessica said. “Not being listened to, not believed, not given the full treatment.”
“To be a caregiver of someone living with Alzheimer’s is that you watch your loved one die every day. I’ve been grieving my mom for seven years.”
___
EDITOR’S NOTE: This story is part of an AP series examining the health disparities experienced by Black Americans across a lifetime.
___
The salon was called “Hair by Connie,” and for 18 years it was the place to go in Alexandria, Virginia, if you were a Black woman who wanted to look her best. Reigning over the shop was its owner, Constance Guthrie.
She traveled the world, attending hair shows. She opened her salon to fashion shows like the “Tall, Full and Sassy” event advertised in an old flyer she now keeps in a box of mementos. She donned dazzling, colorful and flamboyant outfits to match her larger-than-life personality.
In the 1990s, she made the difficult decision to move and close her beloved salon. She bought a home in Fredericksburg so her daughter could attend the best schools, and later became a paraprofessional in the local school district, which allowed her to have a schedule where she never missed oratorical contests or choir recitals.
She was always there for Jessica, who is her only child. They often stayed up into the wee hours of the night working on school projects together. Despite meager means, Jessica grew up surrounded by encouragement and love.
“My mother gave up everything to make sure that I had the greatest support, the greatest opportunities,” Jessica Guthrie recalled. “We were like two peas in a pod.”
Her mother’s hard work paid off. Jessica became a teacher and later moved to Dallas to build her own life and chase her dreams, where she was a successful chief program officer for an education service.
Then, seven years ago, Constance began her descent into dementia.
She started to forget simple things, like where her keys were. She lost her way coming home from work on a familiar route she traveled almost daily for 18 years. She got into a car accident.
The frequency of troubling incidents began to increase, worrying Jessica who was still hundreds of miles away in Texas.
They tried to use Post-it notes to remind Constance of daily tasks. Some of the colorful notes still line the walls of the family’s home.
For a woman who had grown accustomed to being so independent, it was hard for her to accept that she needed help.
“She spent so long trying to hide it,” Jessica said. “Like, ‘Oh, I’m good, I’m fine. I just forgot.’ But you could tell that a lot of her anxiety and stress was because she was trying to cover this up from other people.”
She began to wander around her neighborhood. Jessica and nearby loved ones tried to bolt the door to prevent her from wandering.
A neurologist confirmed she was suffering early cognitive decline and that it was likely Alzheimer’s.
She was just 66 when she was diagnosed.
Soon after, Jessica made the tough decision to pack up and leave Dallas behind to care for her mother full time. She recently began working remotely again after taking an extended leave of absence to care for her mother.
Constance never had diabetes nor high blood pressure — which are common risk factors. She was fairly active and healthy, and would often walk around her neighborhood. But in 2015, Constance suffered a transient ischaemic attack, or a “mini stroke,” which is a brief disruption in the blood supply to part of the brain.
Jessica believes the mini stroke could have been caused in part by the heavy stress her mother endured at her job, where she worked for 18 years as a special education paraprofessional.
She also questions the role genetics played in her mother’s diagnosis. Her mother’s aunts are all living with the disease. Her mother’s brother, who was a doctor, has started to experience cognitive decline. ___
Lost in her own mind, Constance can no longer testify to the difficulties she endured — as a mother, a Black entrepreneur running a business on her own.
But her daughter, Jessica, can attest to the struggles she’s had, as a Black caregiver, trying to ensure that her mother receives appropriate care.
In 2018, her mother started pointing at her stomach, repeatedly, trying to tell her daughter she was in pain. Jessica took her to her primary care physician, who is white and brushed the concerns aside.
“My mother couldn’t articulate that there was significant pain in the moment and the doctor of the practice basically said, ‘Oh, well, you know, sometimes they just come in and put on a show and it seems like she’s fine,’” Jessica said. “They asked, ‘Are you sure she’s in so much pain?’”
They sent her home without performing further diagnostic tests. But the pain persisted.
Jessica took her mother to the emergency room the next day and a Black male doctor ordered the necessary imaging. She needed emergency surgery to correct a painful, protruding hernia.
Then there was the time she took her mother to the emergency room for intense leg pain. She had arthritis in her knee but Jessica suspected something more serious.
The doctor told her she likely just needed rehab for her bad knee. Jessica advocated for more testing and it turned out Constance had a blood clot in her leg.
“Racism is implicit and deeply rooted in the air that we breathe,” said Jessica, who has started an Instagram account to chronicle her experiences.
The problems Black people face getting medical care are pervasive. Black people living with serious illnesses get less help managing pain and other symptoms, and they have worse communication with doctors, according to the Center to Advance Palliative Care.
Studies show they are less likely to receive dementia-related medication that can help ease symptoms like hallucinations and depression that make the disease particularly terrifying for families.
Among non-white caregivers, half or more say they have faced discrimination when navigating health care settings for their care recipient. Their top concern: Because of their race, providers or staff do not listen to them.
And there are barriers to even being diagnosed properly. A recent study found that Black participants in Alzheimer’s disease research studies were 35% less likely to be diagnosed than white participants. Part of the problem is a lack of Black doctors. Just 1 in 3 of the nation’s physicians is Black, Indigenous, Hispanic or Asian. That lack of representation has had a compounding effect on the care that Black people receive — especially later in life when older Americans suffering from illnesses like Alzheimer’s lack the ability to advocate for themselves.
All these things put an outsized burden on Black families providing care.
Through her Instagram, Jessica regularly hears from other Black caregivers, mostly women, who have eerily similar stories of not being heard, feeling isolated or being denied proper treatment.
“I think that part of my journey would have looked significantly different if I were a middle-aged white person or a white male,” she said. “I would have been listened to the first time.” ___ Jessica has spent the past several months preparing for her mother’s imminent death, making sure every detail is perfect.
But in an unexpected twist, she learned in February that her mother would be discharged from home hospice care in early March. Medicare typically covers hospice care for those who are terminally ill, with a life expectancy of six months or less.
Although she remains in the last stage of Alzheimer’s disease, Constance has been deemed stable.
Both her appetite and water intake are great. Her skin is glowing. She still has glimmers of her sassy spirit.
On the surface, this is good news. Jessica’s relishing every extra day she has with her mother.
Still, the discharge feels like a slap in the face.
Several studies have found that Black patients, across various serious illness diagnoses, are less likely to be referred to hospice or use hospice.
Losing hospice services means Jessica will lose all equipment and supplies, including the hospital grade bed that her mother sleeps in, the lift she uses to get her out of bed and her wheelchair. She has lost the weekly nurse visits, vital checks, the social worker and the extra services that her mother loved — music and massage therapy.
Jessica is concerned about how she’ll handle the next medical emergency. She’ll have to rely on local hospitals that provided her mother with problematic care before.
“Everything’s gone and it feels like I’m back at square one again,” she said. “I feel like the system’s failed us and has failed so many other caregivers.”
It’s the latest, but maybe not the last, burden, and it’s taking its toll.
At 34, many of her friends are married, starting families, traveling and investing money for the future.
But she’s had to spend money on her mother’s care and largely put her life on hold.
“When you think about how I spent so long trying not to repeat this cycle of poverty, now I’m sitting in a place where I make a pretty good salary, and yet I’m not setting myself up for the future that I know that I should have,” she said.
Some days she mourns the life that could have been and everything she has had to sacrifice. She sees undeniable parallels between all that her mother sacrificed and what she now has given up. But she wouldn’t change a thing.
Her exhausting experience as a caregiver has added purpose to her life. She feels she is also helping other Black caregivers to be seen and heard.
For now, she is happy to spend time with the woman she calls “CG.”
Every morning after Constance wakes up, Jessica flips on the TV in her mother’s small room to the gospel music station. “Music brightens my mom. She would sing no matter if she was on key or not.”
Now, the daughter sings to her mother as she’s changing or feeding her. On a recent day Jessica tried making it through “Take My Hand, Precious Lord,” as she massaged her mother’s fingers, before her voice cracked and her shoulders bounced as she cried.
“You saying goodbye?” her mother mumbled.
Constance doesn’t sing or clap along anymore, but she lightly tapped her feet under her blanket. And she let out a low, steady hum.
___
Kat Stafford, based in Detroit, is a national investigative race writer for the AP’s Race and Ethnicity team. She was a 2022 Knight-Wallace Reporting Fellow at the University of Michigan. Follow her on Twitter: https://twitter.com/kat__stafford.
Eli Lilly said Wednesday its experimental Alzheimer’s drug appeared to slow worsening of the mind-robbing disease in a large study, sending its stock up by 5% on investor optimism about the results.
In the 18-month trial, people in the early stages of Alzheimer’s who received infusions of donanemab showed 35% less decline in thinking skills compared to those given a dummy drug, Lilly announced in a press release. About 6 million people in the U.S. have Alzheimer’s, which gradually attacks areas of the brain needed for memory, reasoning, communication and daily tasks.
Shares of Lilly jumped nearly $19, or 4.7%, to $423 in morning trading.
The Eli Lilly drug is designed to target and clear away a sticky protein called beta-amyloid that builds up into brain-clogging plaques that are one hallmark of Alzheimer’s.
A similar amyloid-targeting drug, Eisai and Biogen’s Leqembi, recently hit the market with similar evidence that it could modestly slow Alzheimer’s — and also some safety concerns, brain swelling or small brain bleeds.
Donanemab also comes with that risk. Lilly said in its study, the brain side effects caused the deaths of two participants and a third also died after a serious case.
The preliminary study results haven’t been vetted by outside experts. Indianapolis-based Lilly plans to release more details at an international Alzheimer’s meeting this summer and is seeking Food and Drug Administration approval of the drug.
Thanks for reading CBS NEWS.
Create your free account or log in for more features.

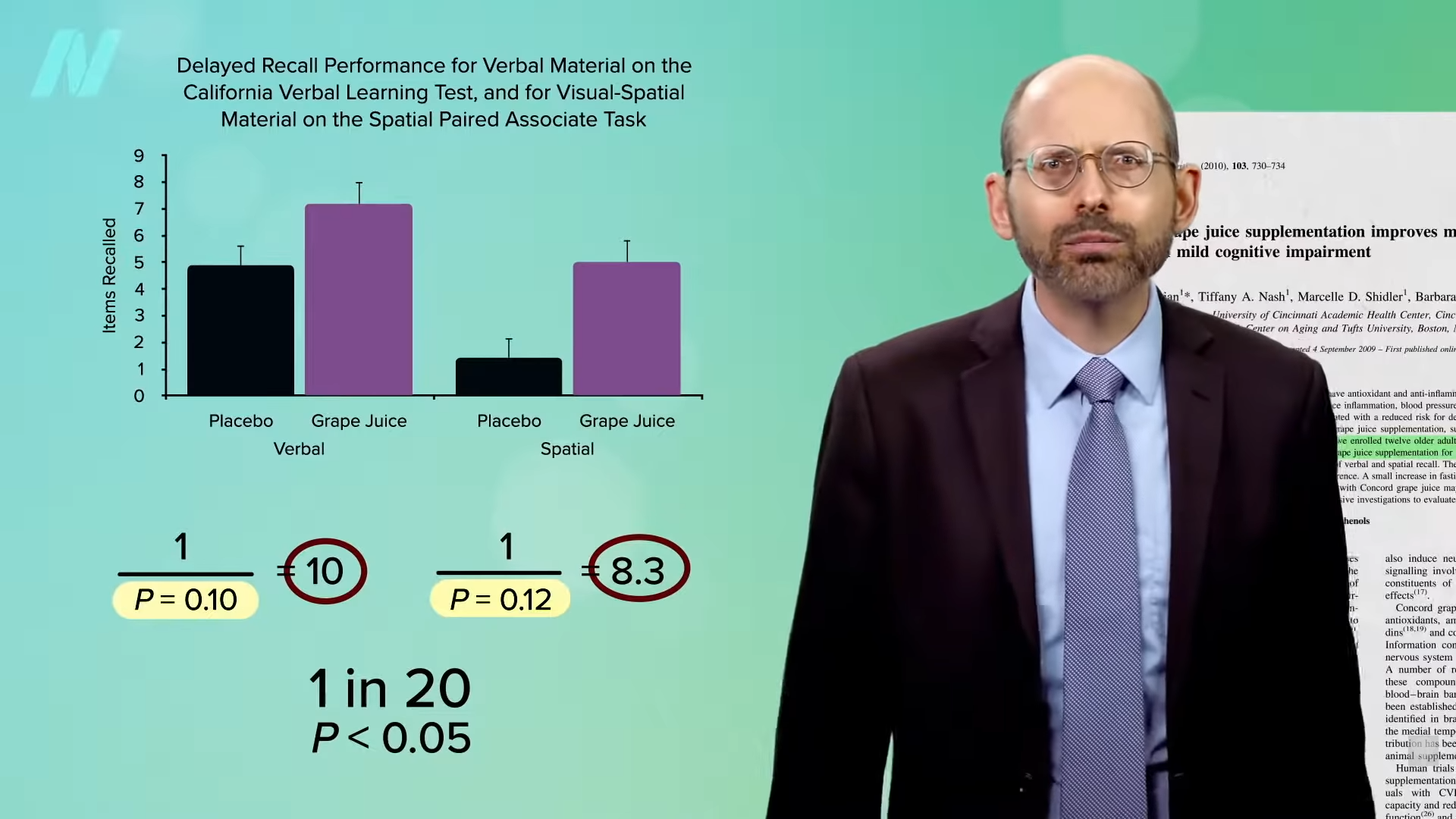
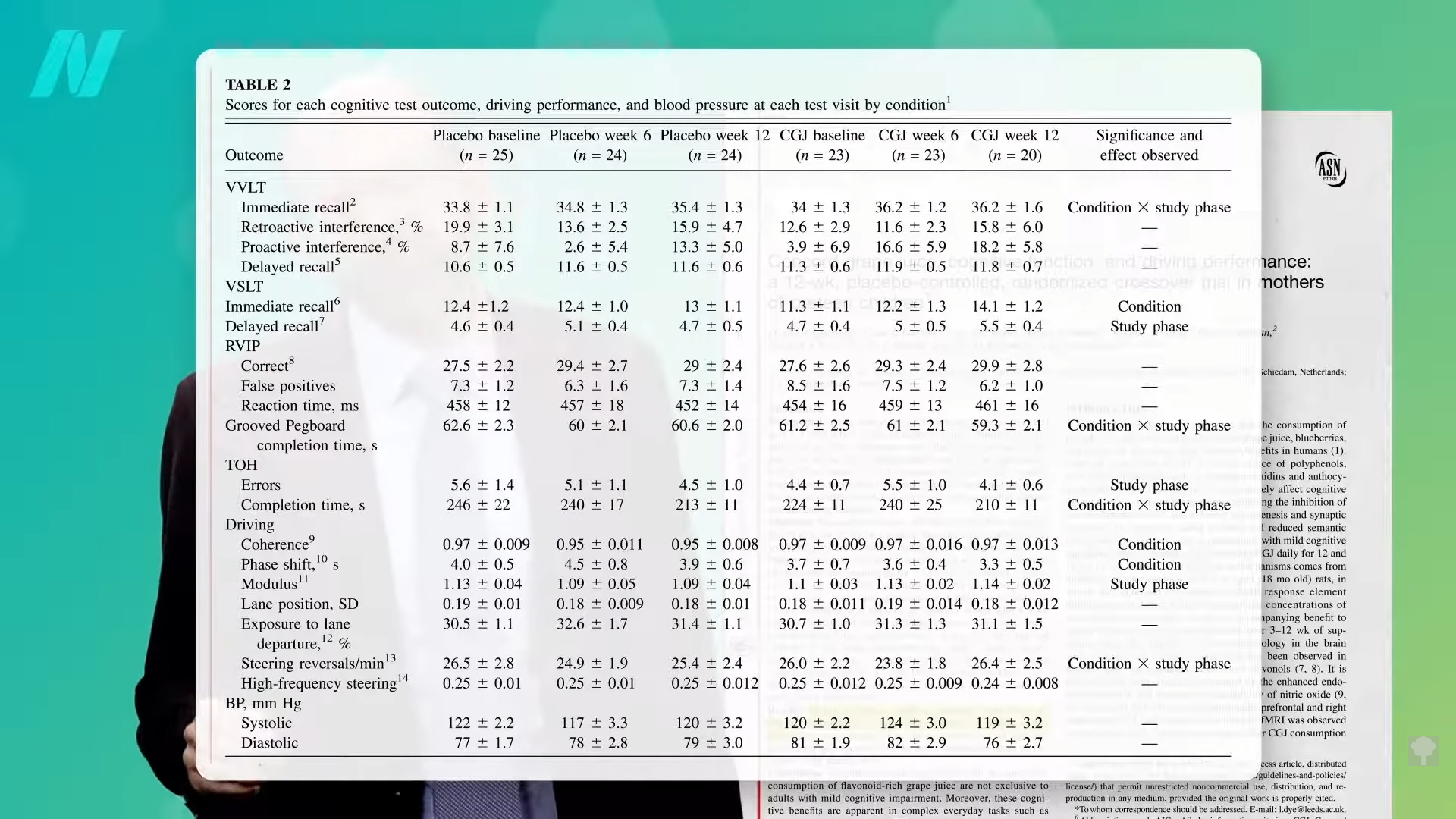
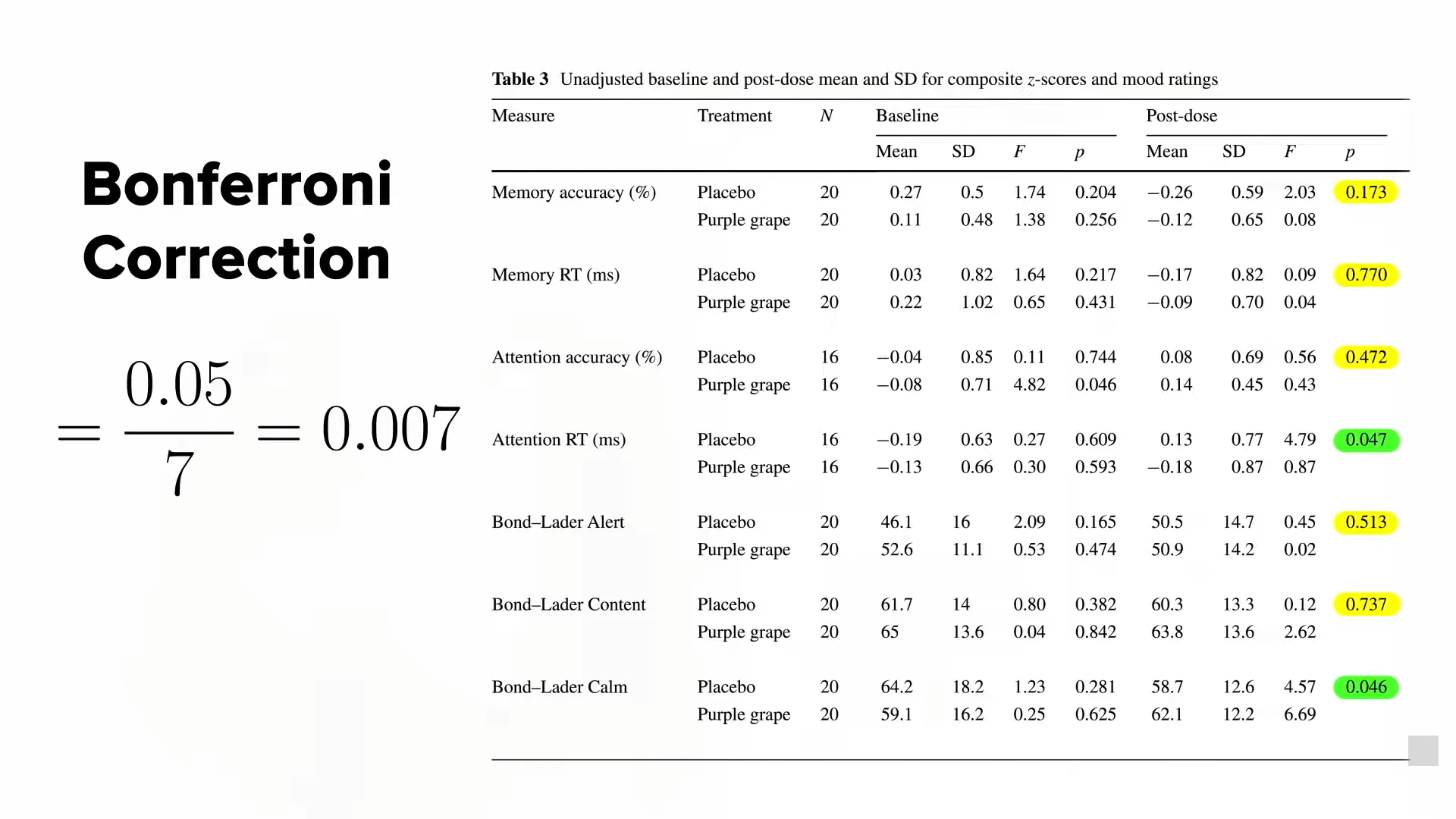
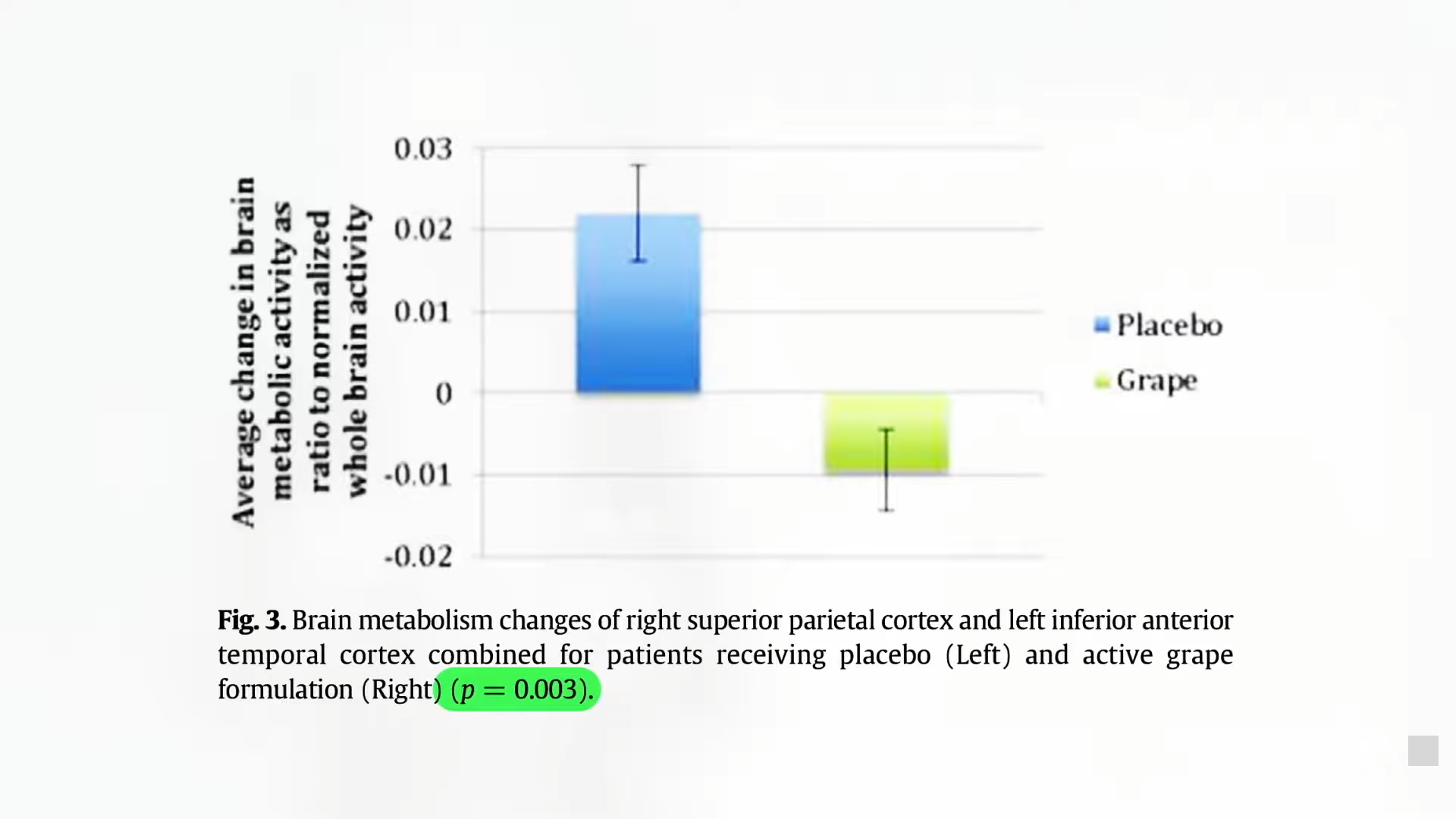










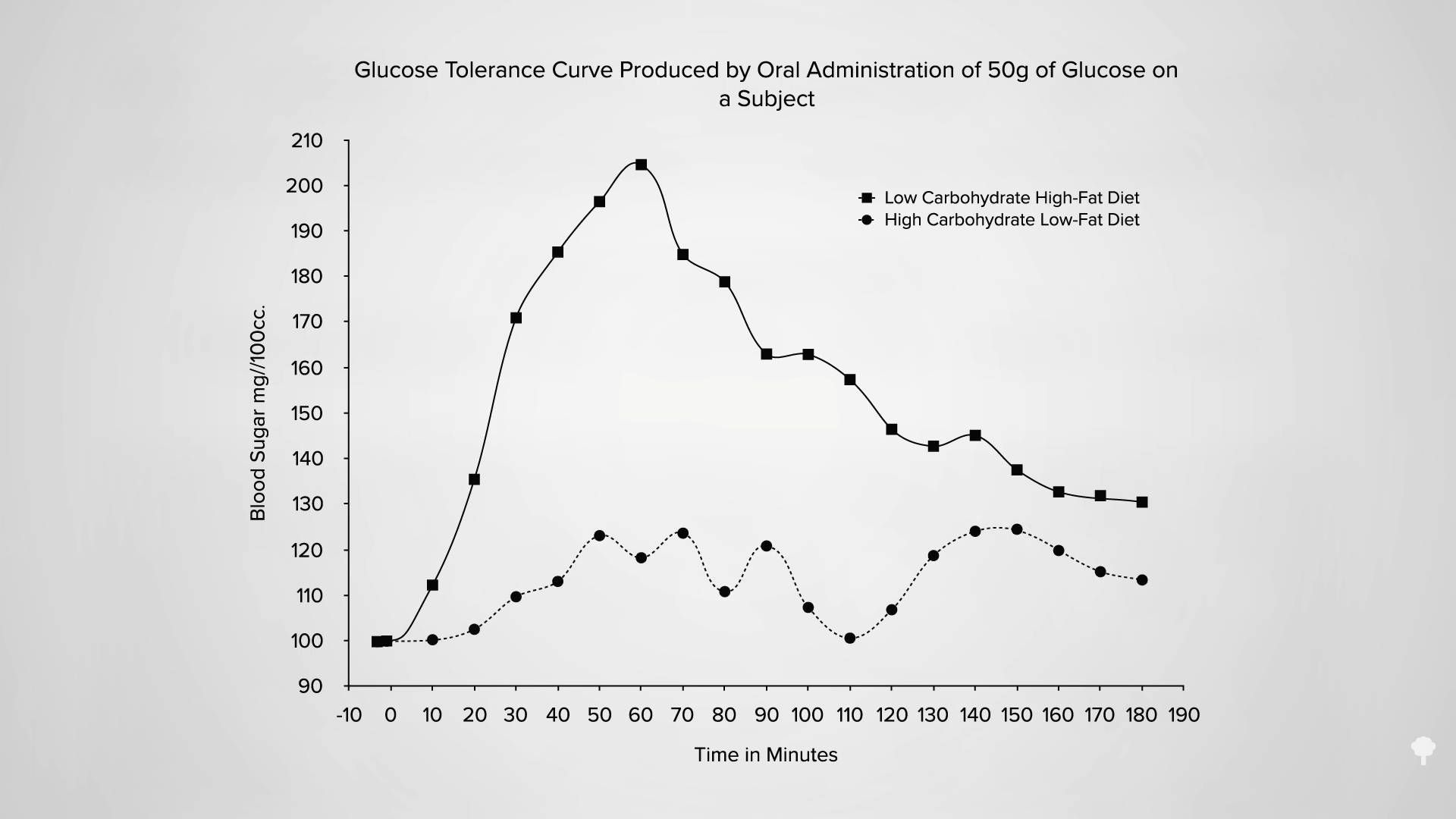
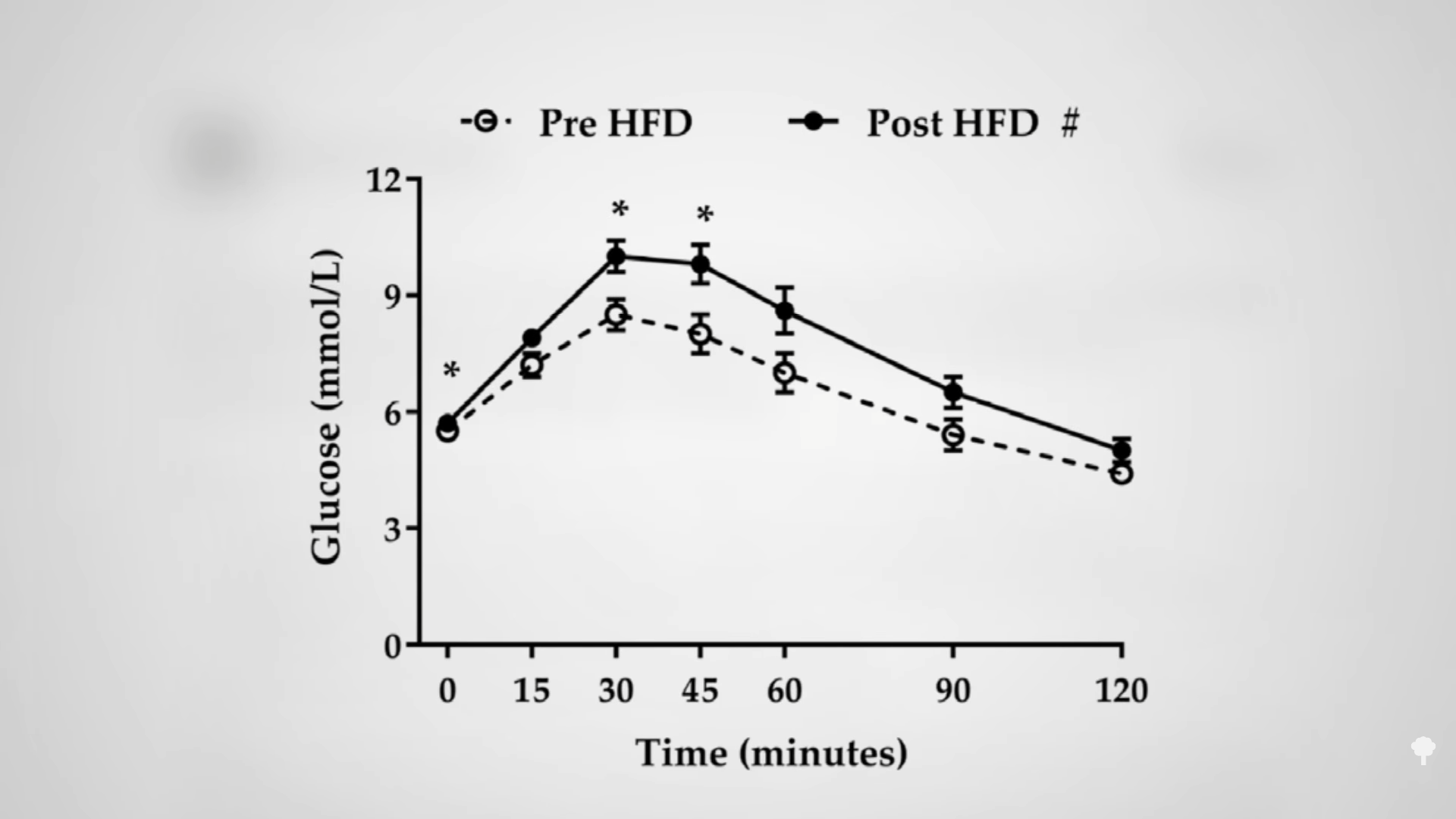
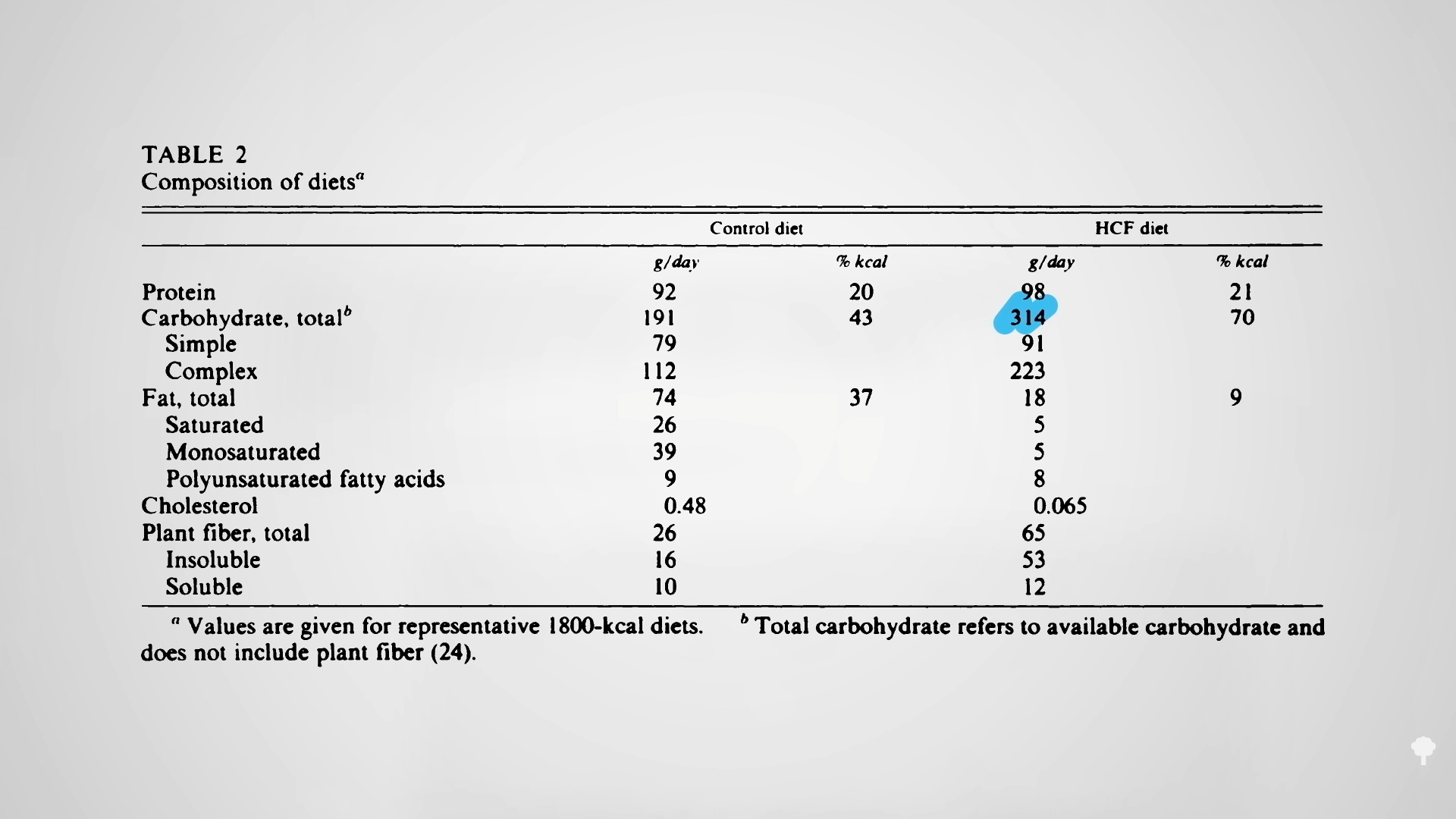 The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal
The irony doesn’t stop there. One of the reasons people with diabetes suffer such nerve and artery damage is due to an inflammatory metabolic toxin known as methylglyoxal, which forms at high blood sugar levels. Methylglyoxal