Donald Trump’s renewed pledge on social media and in campaign rallies to repeal and replace the Affordable Care Act has put him on a collision course with a widening circle of Republican constituencies directly benefiting from the law.
In 2017, when Trump and congressional Republicans tried and failed to repeal the ACA, also known as Obamacare, they faced the core contradiction that many of the law’s principal beneficiaries were people and institutions that favored the GOP. That list included lower-middle-income workers without college degrees, older adults in the final years before retirement, and rural communities.
In the years since then, the number of people in each of those groups relying on the ACA has grown. More than 40 million Americans now receive health coverage through the law, about 50 percent more than the roughly 27 million the ACA covered during the repeal fight in 2017. In the intervening years, nine more states, most of them reliably Republican, have accepted the law’s federal funding to expand access to Medicaid for low-income working adults.
Read: The real reason Republicans couldn’t kill Obamacare
“Republicans came very close to repealing and replacing the ACA in 2017, but that may have been their best window before the law had fully taken hold and so many people have benefited from it,” Larry Levitt, the executive vice president for health policy at KFF, a nonpartisan think tank that studies health-care issues, told me. “I think it gets harder and harder to repeal as more people benefit.”
Trump’s repeated declarations over the past several weeks that he intends to finally repeal the ACA if reelected surprised many Republicans. Few GOP leaders have talked about uprooting the law since the party’s last effort failed, during Trump’s first year as president. At that point, Republicans controlled both chambers of Congress. But whereas the House, with Trump’s enthusiastic support, narrowly voted to rescind the law, the Senate narrowly rejected repeal. Three GOP senators blocked the repeal effort by voting no—including the late Senator John McCain, who dramatically doomed the proposal by signaling thumbs-down on the Senate floor. (Trump mocked McCain while calling the ACA “a catastrophe” as he campaigned in Iowa last weekend.)
Republicans lost any further opportunity to repeal the law in the 2018 election when Democrats regained control of the House of Representatives. With the legislative route blocked, Trump instead pursued an array of regulatory and legal efforts to weaken the ACA during his final years in office. But since the 2017 vote, the GOP has never again held the unified control of the White House, the House, and the Senate required to launch a serious legislative repeal effort.
If Republicans did win unified control of Congress and the White House next November, most health-care experts I spoke with agreed that Trump would follow through on his promises to again target the ACA. Leslie Dach, the founder of Protect Our Care, a liberal group that supports the law, says that he takes Trump’s pledge to pursue repeal seriously, “because he is still trying to overturn the legacy of John McCain, and it’s one of the few things he lost. He doesn’t like to be a loser.”
Trump hasn’t specified his plan to replace the ACA. But whatever alternative Trump develops will inevitably face one of the main problems that confounded Republicans’ last attempt at repeal: Every plan they put forward raised costs and diminished access to care for core groups in their electoral coalition.
That was apparent in the contrast between how the ACA and the GOP alternatives treated the individual insurance market. The ACA created exchanges where the uninsured could buy coverage, provided them with subsidies to help them afford it, and changed the rules about what kind of policies insurers could sell them. Key among those changes were provisions that barred insurers from denying coverage to people with preexisting health conditions, required them to offer a broad package of essential health benefits in all policies, and prevented them from charging older consumers more than three times the premiums of younger people.
The common effect of all these and many other requirements was to require greater risk sharing in the insurance markets. The ACA made coverage in the individual insurance market more available and affordable for older and sicker consumers partly by requiring younger and healthier consumers to purchase more expensive and comprehensive plans than they might have bought before the law went into effect. That shift generated complaints from relatively younger and healthier consumers in the ACA’s early years as their premiums increased.
Every alternative that Republicans proposed during the Trump years sought to lower premiums by unraveling the ACA provisions that required more sharing of risks and costs. For instance, the House GOP plan allowed insurers to charge seniors five times as much as young people, reduced the number of guaranteed essential benefits, and allowed states to exempt insurers from the requirement to cover all applicants with preexisting health conditions.
One problem the GOP faced was that although this approach might have lowered premiums for the young and healthy (albeit while leaving them with less comprehensive coverage), it would have significantly raised costs and reduced access for the old or sick. “A lot of ‘repeal and replace’ was putting more cost back on people with health-care problems,” Linda Blumberg, an institute fellow at the Urban Institute’s Health Policy Center, told me. The Rand Corporation calculated that for individuals with modest incomes, the House GOP plan would have cut premiums for the majority of those under age 45 while raising them for virtually everyone older than 45. The Congressional Budget Office, in its assessment of the House-passed GOP bill, projected that it would nearly double the number of people without health insurance by 2026, and that the greatest coverage losses would happen “among older people with lower income.”
As I wrote in 2017, the paradox was that the Republican plans would have hurt older working-age adults—a preponderantly GOP-leaning constituency—while lowering costs for younger generations that mostly vote Democratic. I called this inversion the “Trumpcare conundrum.”
The congressional Republican alternatives to the ACA under Trump also uniformly made deep cuts to Medicaid, the joint state-federal health-care program for low-income people. But GOP constituencies were big winners as well in the ACA provisions that expanded eligibility for Medicaid.
Until the ACA, Medicaid was generally available only to adults earning less than the federal poverty level. But the law provided states with generous federal financing to expand coverage to low-income individuals earning up to 138 percent of the poverty level. Particularly in interior states, research showed that many of those low-income workers covered under the Medicaid expansion were white people without a college degree, the cornerstone of the modern Republican electoral coalition.
Another big beneficiary from the Medicaid expansion was rural communities, which have become more reliably Republican in the Trump years. Expanding access to Medicaid was especially important to rural places because studies have consistently found that more people in those areas than in metropolitan centers suffer from chronic health problems, while fewer obtain health insurance from their employer, and more lack insurance altogether.
The increased number of people covered under Medicaid gave rural hospitals a lifeline by reducing the amount of uncompensated care they needed to provide for patients lacking insurance. “When you go out to the rural areas, frankly most hospital executives, like other business people, they tend to be pretty conservative,” Timothy McBride, a co-director of the Center for Advancing Health Services, Policy & Economics Research at Washington University in St. Louis, told me. “And they don’t like government intervention. But I would go to see these people and they would say, ‘I’m for Medicaid expansion,’ because they had to deal with the uninsured.”
The Medicaid expansion also quickly became a crucial source of financing for addiction treatment in states ravaged through the 2010s by the opioid epidemic. Before the ACA, addiction treatment programs relied on “a little bit of block grant money here, a local voucher there, kind of out-of-pocket payments, and a little bit of spit and glue,” Brendan Saloner, a professor at the Johns Hopkins Bloomberg School of Public Health who studies addiction, told me. “Then Medicaid came along, and it provided a much more reliable and stable source of payment.”
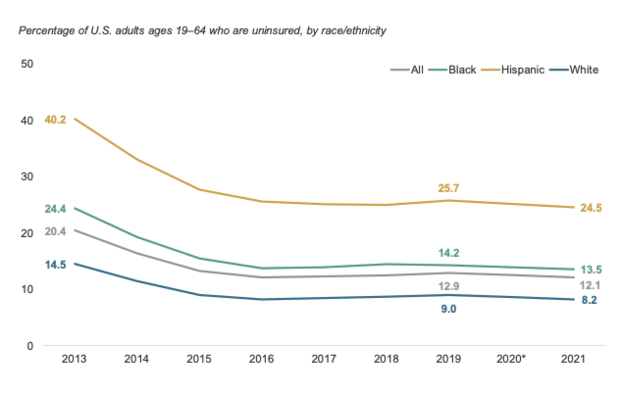
Since the 2017 legislative battle, the ACA’s impact on all these fronts has only deepened. Biden and congressional Democrats both increased the federal subsidies to buy insurance on the Obamacare exchanges and expanded eligibility to families further into the middle class. Largely as a result, the number of people obtaining insurance through the exchanges soared from about 10 million then to more than 15 million as of this past December.
Similarly, a majority of the 31 states that had expanded Medicaid by 2017 were solidly Democratic-leaning. But the nine additional states that have broadened eligibility since then include seven that voted for Trump in 2016 and 2020.
That has not only increased the total number of low-income workers covered through the Medicaid expansion (from about 16 million then to well over 24 million now), but also broadened the red-state constituency for the ACA. McBride estimates that the federal government has annually pumped $2 billion into the health-care system in Missouri alone since voters there approved a Medicaid expansion in 2020. The federal Department of Health and Human Services recently calculated that the likelihood of rural hospitals closing was more than twice as high in the states that have refused to expand Medicaid than in those that have. Simultaneously, the amount of funding that Medicaid provides for the treatment of substance abuse has at least doubled since 2014, allowing it to serve nearly 5 million people, according to calculations by Tami Mark, a distinguished fellow in behavioral health at RTI International, a nonprofit independent research institute.
Even more fundamentally, Blumberg argues, the pandemic showed the ACA’s value as a safety net. Through either the exchanges or Medicaid, the law provided coverage to millions who lost their job, and insurance, during the crisis. “This law was critical in protecting us from unforeseen circumstances even beyond the value that people had seen in 2017,” she told me. “If we had not had that in place, we would have seen massive amounts of uninsurance and people who could not have accessed vaccines and could not have accessed medical care when they became sick.”
For all of these reasons and more, Douglas Holtz-Eakin, the president of the American Action Forum, a conservative think tank, told me that he believes it’s a mistake for Trump and the GOP to seek repeal once again. Holtz-Eakin, a former director of the Congressional Budget Office, remains critical of the ACA, which he says has not done enough to improve the quality of coverage or control costs.
But, he points out, during the Trump years, Republicans succeeded in repealing some of the law’s elements that they disliked most, including the tax penalty on uninsured people who did not buy coverage. “I don’t think we should be happy with the current system,” Holtz-Eakin told me. “But it’s not fruitful to try to roll the clock back to 2010.”
Beyond the policy challenges of excising the ACA from the health-care system, the political landscape also appears less hospitable to a renewed repeal drive. In 2017, KFF polling found that the share of Americans who viewed the law favorably only slightly exceeded the share dubious of it; in the group’s most recent survey measuring attitudes toward the law, more than three-fifths of Americans expressed favorable views, while only slightly more than one-third viewed it negatively. Support for individual provisions in the law, such as the ban on denying coverage because of preexisting conditions or the requirement that insurers allow kids to stay on their parents’ plans through age 26, runs even higher in polls.
Read: Republicans are trapped by preexisting conditions
Yet even with all these obstacles, Trump’s promise to seek repeal again virtually ensures another round of the ACA war next year if Republicans win unified control of the federal government. By historical standards, that’s a remarkable, even unprecedented, prospect. Though Barry Goldwater, the 1964 GOP nominee, had opposed the creation of Medicare, for instance, no Republican presidential nominee ever proposed to repeal it after Lyndon B. Johnson signed it into law in 1965.
If Trump wins the nomination, by contrast, it would mark the fourth consecutive time the GOP nominee has run on ending the ACA. (Among Trump’s main competitors, Florida Governor Ron DeSantis has also promised to produce an alternative to the ACA, and Nikki Haley, who has spoken less definitively on the topic, might feel irresistible pressure to embrace repeal too.) Congressional Republicans may have been surprised that Trump committed them to charging up that hill again, but that doesn’t mean they would refuse his command to do so. “He wants to reverse a loss and take it off the books,” Dach told me. “And we’ve learned that that party follows him. It’s not like they are going to stand up against him, especially in the House. They will destroy the law if they can.”