[ad_1]
From the 1970’s until very recently, we were told that all fats were bad, and we should eat as little fat as possible. We now know that polyunsaturated omega-3 fatty acids are not only good for us, they are essential. What is the difference between saturated and unsaturated fats? Are some fats “good” and other fats “bad”?
What is fat?

Fats and oils are large molecules made of carbon, hydrogen, and a little bit of oxygen. Each fat molecule contains 3 fatty acid tails attached to a glycerol backbone. The result is called a “triglyceride.” Every fat molecule (or triglyceride) has the same glycerol backbone; it’s the different types of fatty acids attached to that backbone that give different kinds of fats their unique properties. Each fatty acid is essentially a long chain of carbon atoms with lots of hydrogen atoms attached to it along both sides, and an “acid” group on one end.
Fat is good.
We think of fat as bad; as something we want to get rid of. We think that the less we have of it the healthier we are. When we have too much of it, we feel ugly and unhappy. But the truth is that fat is incredibly important. Fat is vital to human life and health.
Fat is our portable battery pack.
Fat is an efficient, lightweight, flexible, and portable source of energy. All animals store energy as fat for these reasons. If we were meant to burn carbohydrates for energy, we would have the ability to sprout big lumps of starch all over our bodies, the way plants do. But Mother Nature is smart. She knows that animals need to move around in the world and can’t afford to be weighed down by heavy potato-like structures. Our bodies can only store hours’ worth of energy as starch (glycogen), but we can store months’ worth of energy as fat.
Fat contains more than twice the amount of energy per pound than carbohydrates do. You probably already know this but may not have thought about it this way: carbohydrate contains 4 calories per gram and fat contains 9 calories per gram. Calories are units of energy. Fat can pack a lot more energy than starch can.
Saturated fat is the preferred fuel of the heart, which is why the heart has some saturated fat wrapped around it.
Our brains are mostly made of fat.
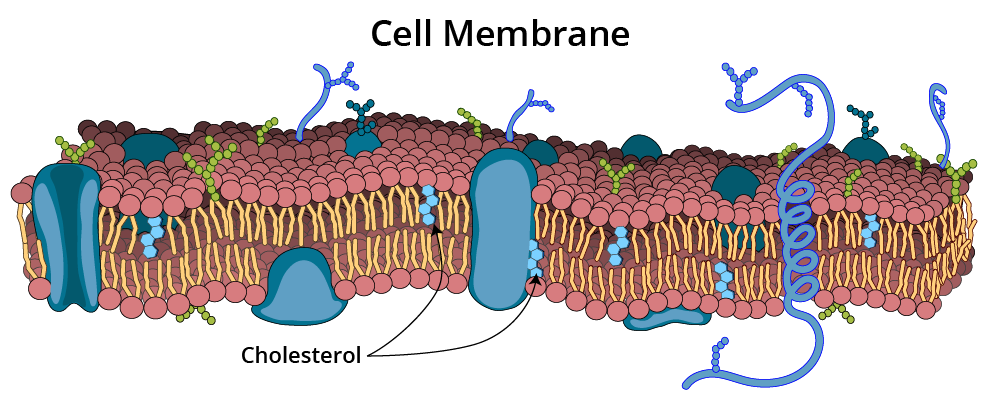
Approximately 60% of the brain is made out of fat. In addition to being an important component of every brain cell membrane, fat also is a major component of myelin, the special insulating material that is wrapped around the electrical wiring pathways of our brain (damage to myelin is the hallmark of Multiple Sclerosis). Myelin is approximately 50% fat and 50% cholesterol.

Fat protects us.
Fat cushions our delicate vital organs so they won’t be bruised or damaged when we run, jump, or fall. Fat is a critical component of our skin—the barrier between us and the outside world—preventing us from randomly absorbing everything we come into contact with. Fats are integral parts of the outer lining (membrane) of every cell in our bodies, forming a water-tight seal that keeps stuff that should be inside the cell inside and stuff that should stay outside of the cell outside. What’s more, inside each cell are mini-compartments, like the nucleus and the mitochondria, that need to keep their contents separate from the inside of the rest of the cell, so they each have fatty membranes, as well.
Fats lubricate our moving parts.
Fats are important ingredients in tears, joint fluids, and other slippery substances that we need to function properly.
Dietary fat is required for vitamin absorption.
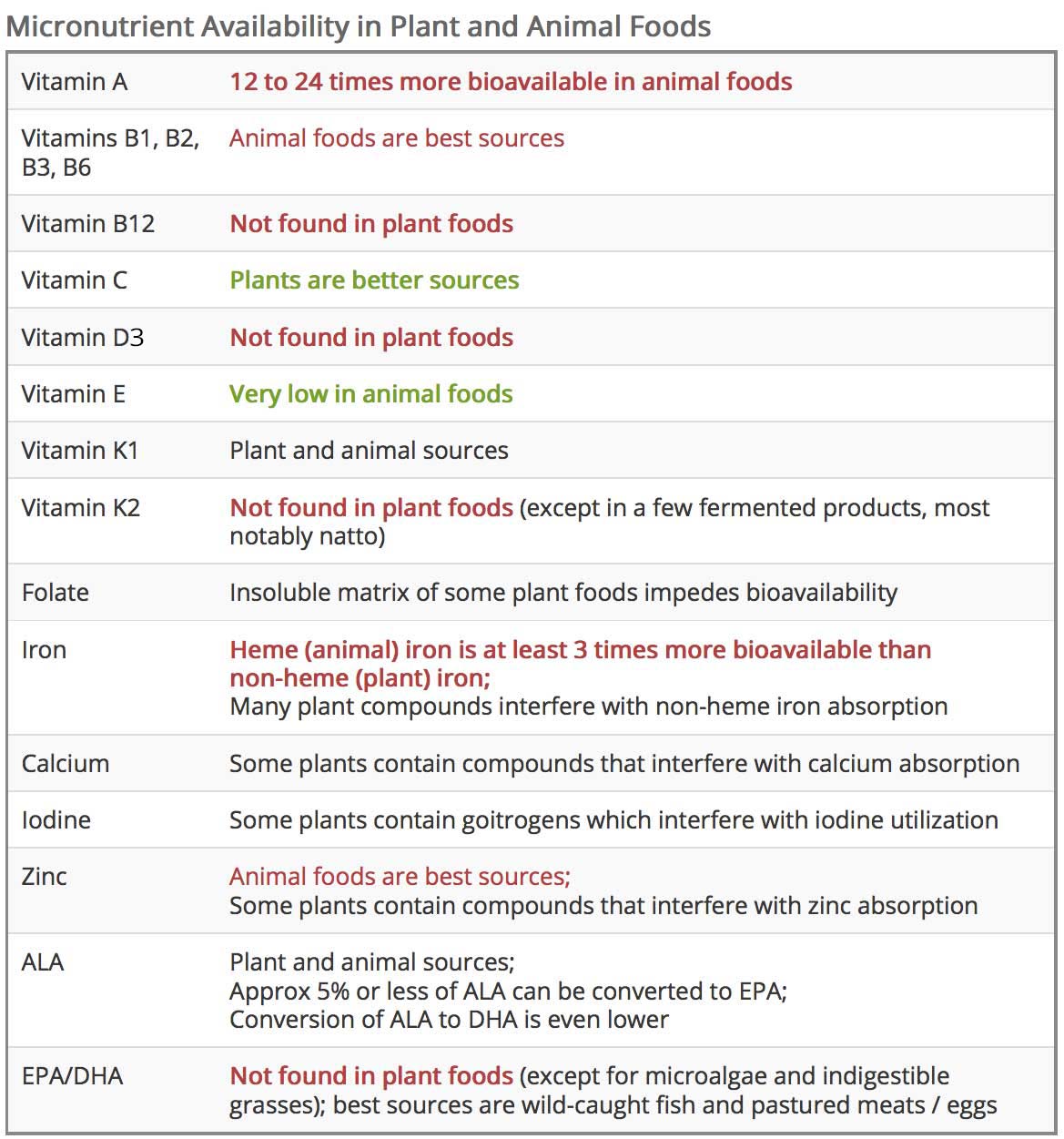
Certain essential vitamins, such as A, D, E and K, all require fat in order to be absorbed by our intestines. Fat itself is so important to our health and survival, that we are designed to absorb about 99% of all the fat we eat. This is not true of many plant substances that we think of as so important to our health, such as vegetable iron and beta-carotene.
How much fat do we need to eat?
This is a difficult question. Fat is so important to every cell in our bodies that we can make fat out of anything—we can make it out of dietary proteins from animals and plants, and we can make it out of carbohydrates, like sugar and starch. That doesn’t mean that these are the ideal ways to obtain fats—for all we know, the body would prefer to get its fat directly from the diet so that it doesn’t have to go through the hassle of turning other dietary ingredients into fat—it just means that it’s possible. There are only a few fats (essential fatty acids) that we absolutely must eat because we can’t make them ourselves (see below).
What is the difference between saturated and unsaturated fat?
A saturated fatty acid has the most hydrogen atoms it can possibly carry—it is therefore “saturated” with hydrogen. Every carbon atom is attached to as many hydrogen atoms as it can hold. Each carbon-hydrogen bond carries energy, so the more hydrogen atoms that are bound to a fat, the more energy you can get out of that fat when you burn it. Saturated fat has more energy, and therefore more calories, per pound.
Unsaturated fats have less hydrogen—at least one of the carbons will have a hydrogen missing. Since there is no hydrogen for that carbon to bind to, the carbon atom forms a double bond to a neighboring carbon atom instead. If a fat has one double bond, it is called “monounsaturated” (missing one hydrogen). Oleic acid, the primary fatty acid in olive oil, is a well-known example of a monounsaturated fatty acid, or MUFA. If it has more than one double bond, it is called “polyunsaturated” (missing more than one hydrogen). Omega-3 and omega-6 fatty acids (see below) are well-known examples of polyunsaturated fatty acids, or PUFAs.

Most fats occurring in nature contain mixtures of saturated, monounsaturated, and polyunsaturated fatty acids. Olive oil contains approximately 17% saturated fatty acids, 71% MUFA (oleic acid), and 11% PUFAs. Coconut oil contains more than 90% saturated fat. Beef fat contains nearly equal parts saturated fat and monounsaturated fat (most of which is oleic acid, the primary fatty acid in olive oil) and approximately 5% polyunsaturated fat, depending on what the animal is fed.
Saturated fats, with their full load of energy-packed hydrogen bonds, are straight molecules that stack together efficiently, and are therefore solid at room temperature (like lard, cocoa butter and coconut oil). Unsaturated fats, with their weaker double bonds, are crooked, because double bonds create kinks in the backbone. They do not pack together efficiently and are therefore liquid at room temperature (like olive oil). Imagine a box full of straight straws—they pack easily and you can fit a lot of straws into the box. However you can’t fit as many bendy straws into that same box because they take up more space. They also move around more inside the box.
When molecules have room to move around easily, they are more likely to form liquids than solids. Saturated fats are very stable, whereas unsaturated fats (oils) are fragile. The carbon double bonds in unsaturated fats are weak and vulnerable to chemical attack compared to the strong carbon-hydrogen bonds in saturated fats. This is why unsaturated fats (oils) go rancid (become oxidized) when exposed to air, whereas you can leave lard or butter on the countertop for a long time without worrying about it. Ghee, which is butter with all of its proteins removed (pure butterfat), can be stored at room temperature indefinitely.
Are saturated fats unhealthy?
Our bodies need both types of fats—saturated and unsaturated. Saturated fats are good for things like insulation (myelin), cushioning (abdominal fat around our organs), and storage (body fat under the skin) purposes. Unsaturated fats are good for flexibility and fluidity purposes, such as in membranes and body fluids. It doesn’t make sense to think of one kind as inherently healthy and the other kind as inherently unhealthy.
Saturated fats are chemically rather boring—they are quite stable (especially as compared to the reactive PUFAs) and it is hard from a common sense point of view to imagine them causing the kinds of trouble they are accused of causing—such as burrowing into heart vessel walls and causing inflammatory plaques that rupture into heart attacks. These are by nature long, smooth, non-irritating substances.
You would not want all of your body fat to be unsaturated. All of your fat would be liquid instead of firm and compact. Not only would you sag everywhere, and begin to resemble a Shar Pei, but your body would have to be bigger, because liquid fats take up more space (like the bent straws in the box).
The misguided belief that saturated fats cause heart disease is rooted in a famous study published in 1970 called “The Seven Countries Study,” in which renowned scientist Ancel Keys claimed that people in countries where more animal fat was eaten had more heart disease then people in countries where less animal fat was eaten. Not only was this study an epidemiological study, and therefore incapable of proving a causal link between any dietary factor and any disease, but there have been numerous studies showing no connection at all between saturated fat and heart disease, including a study of 22 countries published by Yerushalmy and Hilleboe in 1957 (see references below).
The hypothesis that saturated fat causes heart disease now stands on very shaky ground; it is now controversial at best, if not obsolete. Researchers are finding much stronger evidence linking cholesterol dysregulation and heart disease to refined carbohydrates than to saturated fats [Halton 2006, Howard 2006, Mente 2009, Astrup 2010, and Jakobsen 2010].
What are omega-3 fatty acids?
Omega-3 fatty acids are polyunsaturated fatty acids (PUFAs). This means they each have more than one carbon double bond in place of a hydrogen atom. Omega-3 just means that the first double bond in the fat chain is at carbon #3 in the backbone. They are liquid fats (oils).
Even if you eat a 100% fat-free diet, your body will find a way to make almost all of the important fats it needs out of the protein and carbohydrate you eat, but it cannot make omega-3 fatty acids. There are three omega-3 fatty acids that are often called “essential” to our health: ALA (alpha-linolenic acid), EPA (eicosapentaenoic acid), and DHA (docosahexaenoic acid). Because we can’t make them from scratch, we have to eat them.
What is ALA?
ALA is the mother of all omega-3 fatty acids. It is an 18-carbon fatty acid that we can build upon to make EPA (20 carbons), which can in turn be converted to DHA (22 carbons). This process happens in the liver. The problem is that our bodies are not very good at adding carbons to ALA, so we convert only a very small percentage (less than 5%) of the ALA we eat into EPA, and far less of that EPA into DHA. So, the vast majority of the ALA we eat does not turn into precious EPA and DHA; it simply gets burned for energy or stored as fat.
It appears as if ALA itself isn’t required by the body as an important component of any particular cell or molecule; it may only be important as a building block for EPA and DHA. Therefore, if you get enough EPA and DHA in your diet, you may not need any ALA.
What are EPA and DHA?
EPA and DHA, on the other hand, serve important roles in the body. I mention them together because they are almost always found together in nature, and because researchers almost always study them in combination, not individually. Therefore, it can be confusing to try to figure out which one of these compounds is responsible for which benefits. Both EPA and DHA serve as building blocks for anti-inflammatory, pro-healing compounds called “resolvins” and “protectins”, which help to prevent chronic inflammation. They also stabilize the electrical activity of cardiac cell membranes, reducing risk of arrhythmias.
It seems as if DHA may be the most essential of the essential omega-3 fatty acids. The brain and retina require large amounts of DHA for their cells to function properly. It is found in the cell membranes of the brain and retina, helping to keep those membranes fluid and flexible. This is important, because membranes don’t simply act as water-tight walls. They have to be able to wrap around and envelop important nutrients to take them in, or fold outward to let them out. Membranes are very dynamic structures. [I wrote an entire post about the critical role of DHA in the brain and how to include it in your diet in my Psychology Today post: “The Brain Needs Animal Fat.”]
What are good dietary sources of ALA?
ALA is easy to obtain because it is found in such a wide variety of plant and animal foods. Interestingly, Americans obtain more of their daily ALA from animal foods than from plant foods. Oils of seeds, grains, nuts, and legumes contain ALA, with the highest concentrations being found in flaxseed oil, walnuts, canola oil and chia seeds. These foods are therefore marketed as being “rich in omega-3s.” There is also a significant amount of ALA in purslane, an edible succulent green vegetable, and small amounts of ALA in spinach leaves.
The problem is that these sources only contain one of the three essential omega-3 fatty acids; they do not contain any DHA or EPA. And the body can only convert a very small percentage of ALA into EPA (3-8%) and has an even harder time converting ALA into DHA (0-4%), although there are some studies that suggest that, in the complete absence of dietary DHA (such as may occur for vegans), the body may be able to ramp up its ability to convert ALA into DHA to some extent.
What are good dietary sources of EPA and DHA?
EPA and DHA are synthesized primarily by algae and grasses—things that people don’t eat and don’t digest well:
- Marine microalgae
- Seaweed
- Grasses
However, many land animals eat grasses (or should) and many fish (especially small fish) eat algae. Animals eating these green foods accumulate EPA and DHA in their tissues, especially in their fats, livers, and brains. Therefore, good sources of EPA and DHA include:
- Meat from grass-fed animals
- Liver from grass-fed animals (much higher amounts than muscle meats)
- Pasture-raised poultry meat
- Liver from pasture-raised poultry (much higher amounts than bird meat)
- Animal brain
- Small oily fish (anchovy, herring, sardines and mackerel)
- Large oily fish that eat small oily fish (bluefish, tuna, salmon, halibut, bass, and trout)—even farmed fish often contain omega-3’s because of what they are fed.
- Fish liver oils, such as cod liver oil.
- Oysters
Eggs from pastured poultry contain some DHA but are a poor source of EPA.
Full-fat dairy products, especially from grass-fed animals, contain some EPA but are a poor source of DHA.
What are omega-6 fatty acids?
Omega-6 fatty acids are liquid polyunsaturated fatty acids (PUFAs) just like omega-3s are, but they have their first double bond at carbon #6 instead of carbon #3. Whereas there are three important omega-3 fatty acids for human health, there is only one essential omega-6 fatty acid: linoleic acid (LA).
What is linoleic acid (LA)?
It is so unfortunate that linoleic acid, the mother of all omega-6 fatty acids, and alpha-linolenic acid, the mother of all omega-3 fatty acids, have such similar names, because many people confuse the two, but so be it. LA is an 18-carbon polyunsaturated omega-6 fatty acid that we can build upon to make other important molecules, most notably, a 20-carbon omega-6 fatty acid called arachidonic acid.
Linoleic acid is present in all of our cell membranes so that it will be available to form arachidonic acid whenever called upon to do so. Arachidonic acid is required for the process of inflammation to begin. You might be thinking that inflammation is a bad thing, but without it, we cannot mount an immune response to things like bacterial infections and physical injuries. Inflammation is our first line of defense and requires specialized molecules that are made from arachidonic acid: prostaglandins, leukotrienes, and thromboxanes.
While you may not have heard of any of those inflammatory chemicals, you have probably heard of the medicines that are marketed to reduce their activity. NSAIDs such as ibuprofen reduce prostaglandin synthesis. Aspirin reduces prostaglandin synthesis and thromboxane activity. Singulair® is an asthma medication that reduces leukotriene activity.
Do You Have Arachiphobia?
I wrote an entire post for Psychology Today dedicated to busting the nutrition myth that arachidonic acid is dangerously inflammatory for our system: “Do You Have Arachiphobia?” Written as a personal testimony of a misunderstood fatty acid that deserves our respect, it is a fun piece that details the numerous critical functions of this important nutrient.

What are good dietary sources of Linoleic Acid?
Our Western diet is loaded with LA, so not to worry. In fact, we get far more LA than we need. Linoleic acid is present in all kinds of plant and animal foods, but it is present in especially high amounts in vegetable oils (nut and seed oils). Animal fats contain approximately 10-20 % LA, whereas seed oils contain between 50-80% LA. We have been told for decades to avoid animal fats and to choose plant oils instead, and the result is that most of us now get far too much LA in our diet.

The omega ratio problem: are you off-balance?
So, the omega-3 fatty acids are used to create chemicals that have anti-inflammatory properties (resolvins, protectins) and the omega-6 fatty acid LA is used primarily to create chemicals that have pro-inflammatory properties (prostaglandins, leukotrienes, and thromboxanes).
All creatures need a proper balance of these two forces in order to defend themselves (pro-inflammatory elements) and heal (anti-inflammatory elements). Mother Nature understood this, which is why we are gifted with both pathways. In fact, these pathways are intricately connected to each other to keep one another in check. It’s a brilliant system. The pathway that leads from the omega-3 ALA to EPA and DHA uses the very same enzymes as the pathway leading from the omega-6 LA to arachidonic acid. The omega-3 and omega-6 pathways have to share these enzymes, so the pathways actually compete with one another.
This is why some scientists believe that it is important to eat a balance of omega-3 and omega-6 fatty acids. There is good evidence to suggest that our ancestors ate diets that contained roughly equal amounts of omega-3 and omega-6, depending on where they lived; at most their diets may have had 2 to 4 times more omega-6 than omega-3. However, these days our diets contain 20 to 30 times more omega-6 than omega-3, tipping the scale mightily toward inflammation and away from healing. This may be one of the most important reasons why so many people experience chronic pain and inflammation and find themselves turning so often to medications like ibuprofen to turn down the activity of the omega-6 pathway.
The same problem occurs in animals. Grass is high in ALA, the omega-3 parent molecule, whereas grains are high in LA, the omega-6 parent molecule. Therefore, grain-fed cows, for example, have an excess of omega-6 fatty acids and a deficit of omega-3 fatty acids. Grass-fed beef has an average omega-6 to omega-3 ratio of 1.53 to 1, whereas grain-fed beef has a ratio of 7.65 to 1.
If you don’t regularly eat foods naturally rich in omega-3, you should consider taking a supplement. There are three forms of omega-3 fatty acids: ALA, EPA and DHA, and supplements vary greatly in quantities of each form. Aim for about 1000 mg of EPA + DHA (combined—not 1000 mg of each) per day. An example of a good choice for fish oil is Nordic Naturals Ultimate Omega. An example of a good choice for an algae-derived vegetarian/vegan-friendly omega-3 supplement is NuTru Vegan Omega 3 EPA+DHA. [I do not have financial relationships with either of these manufacturers]


Is it possible to eat too much omega-3?
Theoretically, yes. If you ate a diet consisting only of a high-omega-3 fish, such as mackerel or salmon, your omega-6 intake would be very low in comparison to your omega-3, and it is possible that your ratio could turn upside-down. Would that be bad for your health? The theoretical possibilities include increased risk of bleeding and reduced ability to mount an appropriate inflammatory response to injuries and infections. I found two studies that can help us to address this question.
In the first study [Siess et al 1980], researchers fed men a diet consisting of unlimited carbohydrate + mackerel for one week, so that mackerel was the only source of fat or protein. This diet provided 7 to 11 grams of omega-3 fatty acids per day. The number of platelets (blood clotting bodies) in the blood of these men was reduced and platelets were less sticky in laboratory tests compared to platelets of those eating a standard diet. The authors of the study concluded that these were healthy developments, because they could potentially decrease the risk of blood clots in people who are at risk for strokes and heart attacks.
In the second study, researchers compared one diet containing essentially no omega-3 fatty acids, to another diet containing 10 grams per day of omega-3 fatty acids in the form of salmon and salmon oil. After 3 weeks, in the high omega-3 group, platelet counts dropped (in a couple of cases to below normal–the lowest count was 90,000, whereas the normal lower limit is considered to be 150,000), platelets became less sticky, and bleeding time was lengthened to about 10 minutes on average (normal upper limit considered to be about 9 minutes). The authors did not conclude whether these findings meant that the high omega-3 diet was healthier or riskier than the omega-3 free diet.
The typical recommended dose of omega-3 fatty acids is between 1 and 2 grams per day. Since the scientific jury is still out about the potential risks involved in taking very high doses of omega- 3, it would be best to use common sense here. It is nearly impossible to eat a natural diet that is too high in omega-3 and too low in omega-6. However, eating a diet of 100% oily fish (there are no studies of such a diet) or taking very high doses of omega-3 fatty acids could theoretically throw your ratio off-balance to the point that bleeding and resistance to infection could become problematic.
Bottom line about fats
- Healthy fats are healthy for you.
- Include healthy animal fats in your daily diet if you can, as these are naturally good sources of EPA and DHA.
- Reduce the amount of vegetable oils (nut and seed oils) in your diet to improve your omega-3 to omega-6 ratio.
- If you choose to eat a vegan diet, be sure to include some DHA/EPA from microalgae sources, and gravitate towards plant foods that are high in ALA and low in LA.
To learn why dietary cholesterol is not bad for you, read my cholesterol page.
References Practice and Contact Information
Astrup A, Dyerberg J, Elwood P,et al. The role of reducing intakes of saturated fat in the prevention of cardiovascular disease: where does the evidence stand in 2010? Am J Clin Nutr. 2010;93:684-688.
Bradbury J. Docosahexaenoic Acid (DHA): an ancient nutrient for the modern human brain. Nutrients. 2011;3(5):529-554.
Clancy K. Greener Pastures: How Grass-Fed Beef and Milk May Contribute to Healthy Eating. Cambridge, MA: Union of Concerned Scientists; 2006.
Daley CA, Abbott A, Doyle PS, Nader GA, Larson S. A review of fatty acid profiles and antioxidant content in grass-fed and grain-fed beef. Nutr J. 2010;9:10.
Deckelbaum RJ, Torrejons C. The omega-3 fatty acid nutritional landscape: health benefits and sources. J Nutr. 2012;142(3):587S-591S.
Enig MG. Know Your Fats: The Complete Primer for Understanding the Nutrition of Fats, Oils, and Cholesterol. Silver Spring, MD: Bethesda Press; 2011.
Enser M, Hallett KG, Hewett B, Fursey GA, Wood JD, Harrington G. The polyunsaturated fatty acid composition of beef and lamb liver. Meat Sci. 1998;49(3):321-327.
Gebauer SK, Psota TL, Harris WS, Kris-Etherton PM. n-3 Fatty acid dietary recommendations and food sources to achieve essentiality and cardiovascular benefits. Am J Clin Nutr. 2006;83(suppl):1526S–1535S.
Goodnight SH Jr, Harris WS, Connor WE. The effects of dietary omega 3 fatty acids on platelet composition and function in man: a prospective, controlled study. Blood. 1981;58(5):880-885.
Halton TL1, Willett WC, Liu S et al. Low-carbohydrate diet score and risk of coronary heart disease in women. N Engl J Med. 2006 Nov 9;355(19):1991-2002.
Howard BV, Van Horn L, Hsia J, et al. Low-fat dietary pattern and risk of cardiovascular disease: the Women’s Health Initiative randomized controlled dietary modification trial. JAMA 2006;295(6):655-666.
Jakobsen MU, Dethlefsen C, Joensen AM et al. Intake of carbohydrates compared with intake of saturated fatty acids and risk of myocardial infarction: importance of the glycemic index. Am J Clin Nutr. 2010;91(6):1764-1768.
Keys A. Coronary heart disease in seven countries. Nutrition. 1997;13(3):250-252.
Kouba M, Mourot J. A review of nutritional effects on fat composition of animal products with special emphasis on n-3 polyunsaturated fatty acids. Biochimie. 2011;93(1):13-17.
Kris-Etherton PM, Taylor DS, Yu-Poth S, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr. 2000;71(suppl):179S-188S.
Mente A, de Koning L, Shannon HS, Anand SS. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med. 2009;169(7):659-669.
Mozaffarian D, Wu J. (n-3) fatty acids and cardiovascular health: are effects of EPA and DHA shared or complementary? J Nutr. 2012;142(3):614S–625S.
Schmid A. The role of meat fat in the human diet. Crit Rev Food Sci Nutr. 2011;51(1):50-66.
Shikany JM, Vaughan LK, Baskin ML, Cope MB, Hill JO, Allison DB. Is dietary fat “fattening”? A comprehensive research synthesis. Crit Rev Food Sci Nutr. 2010;50(8):699-715.
Siess W, Roth P, Scherer B, et al. Platelet-membrane fatty acids, platelet aggregation, and thromboxane formation during a mackerel diet. Lancet. 1980;1(8166):441-444.
Simopoulos A and Salem M. Purslane: a terrestrial source of omega-3 fatty acids. N Engl J Med. 1986;315(13):833.
Willett W. The great fat debate: total fat and health. J Am Diet Assoc. 2011;111(5):660-662.
Yerushalmy J, Hilleboe H. Fat in the diet and mortality from heart disease: a methodologic note. NY State J Med. 1957;57(14):2343-2354.
[ad_2]










 So, the original free radicals are now stable (phew), but now we have two new problems:
So, the original free radicals are now stable (phew), but now we have two new problems:



 So, the original free radicals are now stable (phew), but now we have two new problems:
So, the original free radicals are now stable (phew), but now we have two new problems: