
[ad_1]
Type “is fructose bad for you” into your search engine and you’ll get a slew of articles telling you that fructose (aka fruit sugar) can cause diabetes, obesity, gout, fatty liver disease, and even cancer. If you believe the headlines, you might be worried that every time you bite into a banana, you’re hammering a big squishy yellow nail into your future fruity coffin. Yet public health officials, and even pediatric obesity specialist Dr. Robert Lustig, who goes so far as to call fructose a poison, continue to advise us to eat fruit. Confused? In this post, I provide a review of the science and clear, simple answers about the connection between fructose, glucose, and common health problems so that you have the information you need to make smart decisions about your health.
I put all of these diseases in a single blog post not to overwhelm you, but because they belong together. Although these conditions seem very different on the outside, as you’re about to see, they are actually just different faces of the same basic underlying metabolic problem: insulin resistance. You’ll also quickly discover that all kinds of sugar are risky when it comes to your health, and that fructose is probably the least of your worries.
[Note: this article is part three of a five-part series on sugar and health. To begin with article one, see “Has Fructose Been Framed?”]
Ok, so let’s get to the bottom of these, once and for all. [You can use the links below if you want to skip to a particular section.]
Note: Because fructose malabsorption differs metabolically from the above diseases, I decided to cover it in a separate post.
Q: Does fructose cause TYPE 2 (“adult-onset”) DIABETES?
A: There’s no evidence that reasonable amounts of fructose increase risk for diabetes more than other sugars do. Excessive intake of sugars of any kind can lead to high blood glucose levels and type 2 diabetes in susceptible people, but glucose raises blood glucose and insulin levels more than fructose does (except at very high doses), so glucose is arguably the more dangerous of the two sugars.
Type 2 diabetes is a disease characterized by “insulin resistance,” which can gradually lead to high insulin levels and high blood glucose levels. Insulin resistance means that your body has become less sensitive to the effects of insulin, a powerful hormone released after meals that tells your body what to do with the calories you eat. For example, after eating a meal, insulin tells muscle and liver cells to soak up excess glucose from your blood stream to keep your blood sugar from going too high. The most powerful trigger for insulin release is glucose (from sugars and starches); fructose does not directly stimulate insulin production.
If you eat too much sugar and/or starch too often, as most people do, your blood glucose will spike frequently and your body will have to release lots of insulin over and over again to deal with those glucose spikes. Eventually your cells can become so accustomed to insulin spikes that they become less responsive to insulin. If your cells become numbed to insulin’s signals, they can’t absorb extra glucose from the bloodstream as well, and your blood sugar could stay too high for too long after meals. In response, the body releases even more insulin to try to get cells to respond better. One result of this vicious cycle can be type 2 diabetes, a disease marked by high blood sugar and high insulin levels. I highly recommend this wonderful video of Dr. Andreas Eenfeldt interviewing kidney specialist Dr. Jason Fung explaining why it makes no sense to treat type 2 diabetes with insulin.
Excess consumption of sugars in general is well-established as a major risk factor in the development of insulin resistance, but is there quality evidence to suggest that fructose in particular is any more dangerous than any other sugar in this regard? Does fructose increase fasting insulin, fasting glucose, or insulin resistance more than glucose does?
It depends on who you ask and what kinds of doses we’re talking about.
It turns out that low to moderately high amounts of fructose are no worse than glucose and often are superior to glucose when it comes to these metabolic markers in human studies.
That is to say that fasting insulin, fasting glucose, hemoglobin A1C (a measure of blood sugar over time) and insulin resistance often look better when people consume fructose than when they consume glucose. This makes sense because it is well-known that glucose is a far more powerful trigger of blood sugar and insulin spikes than fructose.
However, at very high doses (more than 100 grams per day) fructose actually starts to look a little worse than glucose.
The fact that fructose behaves so differently at very high doses is responsible for some of the confusion and disagreement among scientists about whether fructose is worse than glucose for diabetes or not. [Read article two in this series to see how studies using excessively high doses of fructose produce unreliable results.]
There is no good scientific evidence to support the idea that sugar (which is a 50/50 mix of fructose and glucose) is metabolically any worse than starch (glucose) when appropriate amounts are considered.
However, just because fructose is no worse than glucose does not mean that either one of them is innocent. When it comes to the big picture and common sense recommendations to reduce your risk for diabetes, I wholeheartedly agree with the conclusions reached by Dr. James DiNicolantonio and colleagues in a recent review of the subject:
“There is no need for added fructose or any added sugars in the diet; reducing intake to 5% of total calories (the level now suggested by the World Health Organization) has been shown to improve glucose tolerance in humans and decrease prevalence of diabetes and metabolic derangements that often precede and accompany it.”
Bottom line about fructose and diabetes
Type 2 diabetes is a disease of insulin resistance, which leads to high fasting insulin and blood sugar levels. Except at very high doses, glucose may actually be worse than fructose when it comes to diabetes risk. However, because much of the fructose we consume turns into glucose (see article one), it is wise to be careful with both of these sugars.
The sad truth is that diabetes is simply your body’s way of telling you that you can’t process carbohydrates anymore. The happy truth is that diabetes is a dietary disease, so it can usually be treated by changing what you eat. In article five I’ll provide lots of helpful advice about how to eat if you want to prevent or reverse diabetes.
Q: Does fructose cause CANCER?
A: There’s no evidence that fructose causes cancer, however it may play a role in the spread of the disease. Cancer cells require glucose, not fructose, for energy and survival. High blood glucose and insulin levels set the stage for cancer growth in the body, so individuals with insulin resistance, high blood sugar, and type 2 diabetes are at higher risk. There is some evidence to support the notion that fructose may make it easier for certain kinds of cancer to spread, but no cancer cell can live without glucose.
It is an undisputed fact that cancer cells are addicted to glucose, which is found in virtually all sweet and starchy foods.
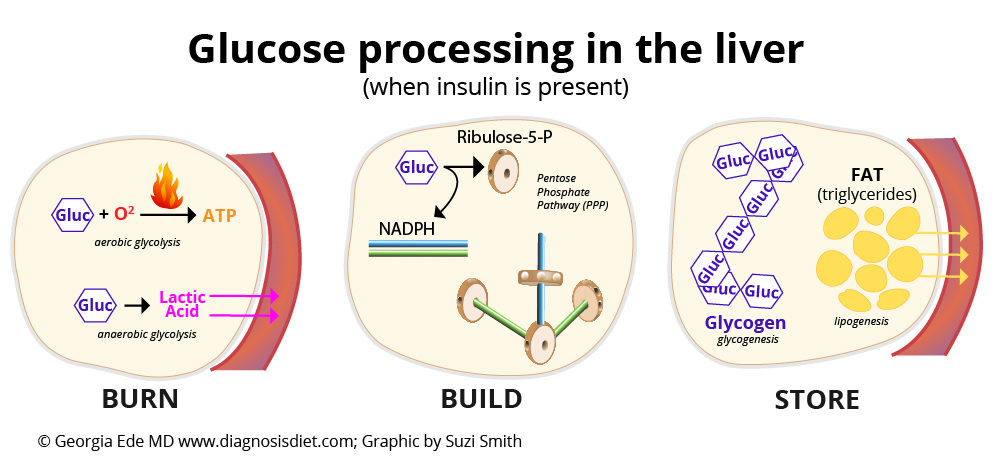
Cancer cells need a LOT more glucose than healthy cells because they rely mainly on a process called “anaerobic glycolysis” to fuel their furious growth rate. This means that instead of using oxygen to burn glucose for energy (aerobic glycolysis) like most healthy cells do, they ferment glucose into lactic acid for energy. Fermentation is very inefficient, so cancer cells demand high amounts of glucose to stay alive. [To learn more about how cancer cells operate, please see my series “What Causes Cancer?“]
Malignant cancer cells display high numbers of glucose transporters on their surfaces; without these special sugar transporters, glucose molecules would not be able to enter cancer cells from the bloodstream.
The more glucose you have in your bloodstream, the happier cancer cells are, so it makes perfect sense that high blood sugar levels would be a strong risk factor for cancer. Insulin resistance makes it hard to process glucose properly, so blood glucose levels rise. To make matters worse, cancer cells love high insulin levels, too, because insulin is a growth hormone that helps cells to grow. People with high insulin levels are at higher risk for cancer and have a worse prognosis once they develop cancer. High blood sugar and insulin levels are seen in people with insulin resistance, type 2 diabetes, and obesity, all of which belong to a group of related conditions collectively known as “metabolic syndrome.”
“Several studies indicate a strong association between MS [metabolic syndrome] and increased risk of cancer. The underlying mechanism of this association is not fully understood but, obesity, hyperglycemia, and hyperinsulinemic states are definitely involved. . . . Increased insulin levels in MS may lead not only to cancer initiation but also to its progression.”
Okay, so when it comes to cancer, too much glucose in the blood is BAD. But what about fructose and cancer? Do tumor cells eat fructose, too? Do cancer cells have enough fructose transporters on their surfaces to use fructose as an energy source?
Yes, some cancer cells do eat fructose.
In humans, certain types of cancer cells are capable of sporting significant numbers of fructose transporters on their surfaces (in addition to the required high number of glucose receptors): certain kidney cancer cells, breast cancer cells, and certain brain cancer cells (gliomas).
The most recent review of the possible role of fructose in cancer was written by scientists at the University of Maryland and Boston University in 2012 and is quite good.
The authors of this review emphasize that it is well established that cancer cells love glucose and that excess glucose fuels cancer growth. However, they believe that fructose may be even more dangerous than glucose under certain circumstances. Almost all of the evidence used to support their argument against fructose comes either from epidemiological studies or from laboratory studies of specialized cell cultures under extreme conditions, but there are important exceptions that make their conclusions worth our attention:
- Interestingly, there is an autopsy study showing that lung cancer tumor cells that had metastasized (spread) to the liver displayed higher numbers of fructose transporters than the primary (original) lung tumor cells that hadn’t left the lung.
- Certain kidney cancer cells (clear cell renal carcinoma cells) display significant numbers of fructose transporters on their surfaces and have certain features that could make them more likely to metastasize (spread).
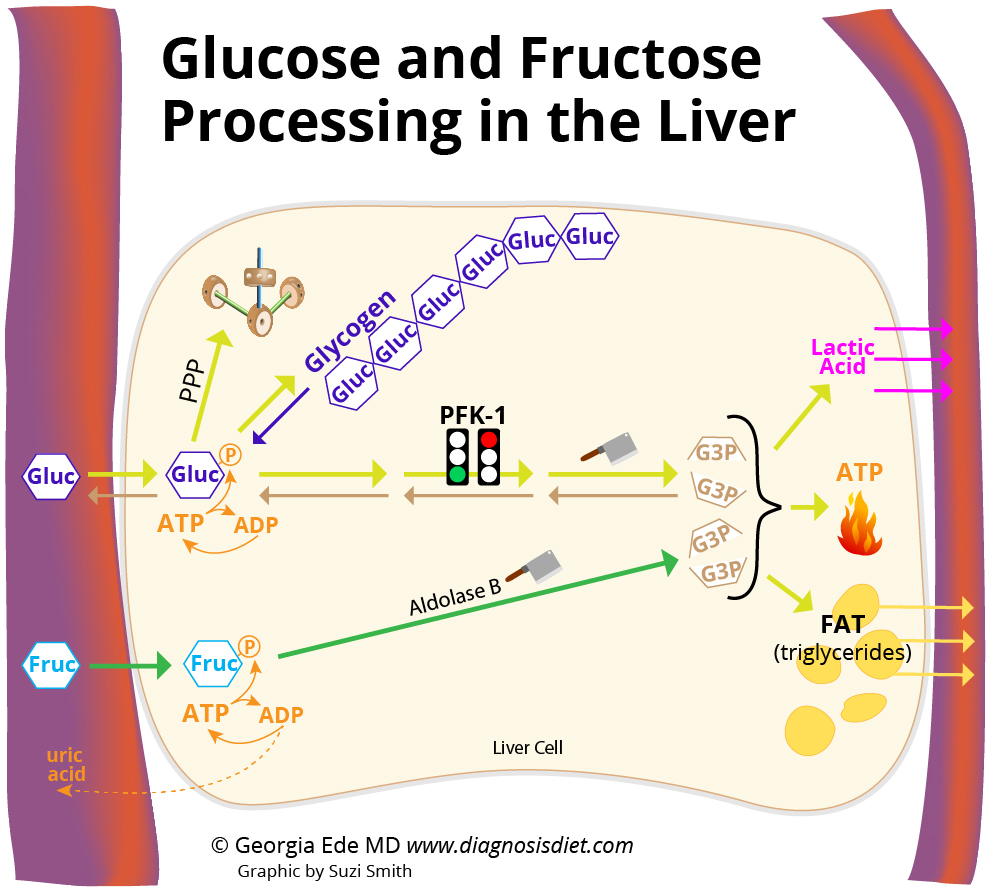
- In the laboratory, if you put cancer cells in Petri dishes and feed them fructose instead of glucose, they grow much more slowly than they do on glucose, but they also produce smaller amounts of self-destructive lactic acid, and produce more protein (via the pentose phosphate pathway—see article one). The thinking is this: If a cancer cell can use fructose in addition to glucose, it might be able to survive better because it produces less lactic acid, and its ability to crank out proteins may make it easier for it to break free and travel (metastasize).
“Fructose appears to be a superior precursor for protein synthesis over glucose by enhancing flux through biosynthetic pathways. Together, glucose and fructose may act synergistically to support malignant growth. . . . Fructose may also promote a more aggressive phenotype in cancer cells and increase the likelihood of metastasis. Further research into the specific effects of fructose, together with glucose, at physiologic levels on malignant growth is warranted.”
Keep in mind that, unless you are in the habit of consuming high doses of fructose, most cancer cells are unlikely to be able to get much fructose out of your bloodstream. This is because, if you recall from article one, the liver sops up the vast majority of the fructose we absorb from foods and beverages before it has a chance to circulate, as long as the amount you consume is not too high. The only theoretical exception to this rule might be cancers of the digestive tract, which could be exposed to any fructose that you can’t absorb (we’ll look at fructose absorption problems in part four). Regardless, it appears that some cancer cells have come up with ways to exploit whatever fructose might be floating around and use it to their advantage.
Bottom line about fructose and cancer
Glucose is your bad boy when it comes to cancer because cancer cells require high amounts of glucose and insulin to take hold, grow, and thrive. This is why people with insulin resistance (high blood sugar and high insulin levels) are at higher risk for cancer and have a worse prognosis. However, some cancers, including breast, and certain brain and kidney cancers, may be able to use fructose to supplement their glucose habit and improve their ability to spread.
If I had cancer, I wouldn’t touch a carbohydrate with a ten-foot pole.
Q: Does fructose cause OBESITY?
A: There’s no evidence that reasonable amounts of fructose cause more weight gain than other sugars. However, too many sugary calories (of any kind) can absolutely cause weight gain, especially in people with insulin resistance.
An excellent 2012 review of human studies funded by the Canadian Institutes of Health Research concludes convincingly that fructose does NOT cause weight gain compared to other sugars unless people are fed extra calories.
Yet, when high doses of fructose that add lots of extra calories to the diet are given to people, yes, some studies do show weight gain.
Given that only a tiny fraction of pure fructose is turned into fat (see article one), it’s unlikely that fructose on its own could be responsible for the obesity epidemic. HOWEVER, in real life, fructose and glucose are almost always eaten together. Fructose itself doesn’t cause much of an insulin response, but glucose certainly does, so when fructose and glucose are eaten together, insulin will spike and turn on fat building in the liver. It should be no surprise that big doses of fructose, when eaten with glucose, can make people fat.
But it’s important to point out that eating a big dose of glucose can make people just as fat.
A good example of a study that illustrates this point compared the effects of glucose drinks to fructose drinks on older overweight men and women. The sweetened drinks provided 25% of daily caloric intake (for a 2000 calorie/day diet, that would be 500 calories worth of fructose or glucose per day). Despite the fact that this study uses high doses of these sugars, it is interesting to note that, after 8 weeks, both glucose and fructose had caused the same amount of weight gain—more than 3 pounds, suggesting that overeating either type of sugar can make you fat.
There is a consensus building that “central obesity” is a disease of insulin resistance. This means that if you tend to gain weight around your middle, like an apple, you probably have insulin resistance and therefore your body will tend to turn sugars and starches into fat very easily and have a harder time burning it for energy. [Take my quiz: “How Carbohydrate Sensitive Are You?]”
Bottom line about fructose and obesity
Fructose is no worse than glucose when it comes to weight gain. Overeating either of these sugars can make susceptible people fat. Sugars and starches raise insulin levels, which turns fat burning OFF and turns fat storage ON. It’s awfully hard to lose fat when carbs are literally telling your body to make more fat! It is not dietary fat that makes us fat. It is excess carbohydrate.
Q: Does fructose cause GOUT?
A: There’s no evidence that reasonable amounts of fructose raise uric acid levels, let alone cause gout. High doses of fructose do raise uric acid levels more than glucose does, but high uric acid levels alone are not enough to cause gout. In fact, most people with high uric acid levels will never develop gout.
Gout is a special type of arthritis marked by painful deposits of uric acid crystals in joints. Uric acid is a normal by-product of everyday cellular activity, so we all have uric acid in our blood all the time, whether we eat fructose or not, but some people have more uric acid floating around in their bloodstream than others do. It is unclear why some people are more prone to gout, but we do know that people with insulin resistance are at higher risk. This is partly because high insulin levels tell the kidney to hold on to extra uric acid instead of excreting it in the urine, the way it normally would.
Studies consistently show that very high doses of fructose do raise uric acid levels more than glucose does (see article one) However, when studies use a normal number of calories, fructose does not raise uric acid more than other sugars do. For more information about diet and gout, please see my post “Got Gout But Love Meat?“
Bottom line about fructose and gout
Fructose doesn’t cause gout, but improving your insulin sensitivity could be very helpful in allowing your body to eliminate uric acid more efficiently, as well as reduce your tendency to develop inflammation. You’ll see how to improve insulin sensitivity in article five.
Q: Does fructose cause FATTY LIVER DISEASE?
A: There’s no evidence that reasonable amounts of fructose lead to fatty changes in the liver. However, excessive intake of sugar of any kind can lead to fatty changes in the liver.
Non-alcoholic fatty liver disease (NAFLD) affects 30% of Americans [wow!]. It is characterized by insulin resistance and fatty deposits in the liver, which can lead to liver damage over time.
A recent review of all available controlled feeding studies in humans concluded that there is no evidence that fructose at ordinary doses can cause fatty liver changes in healthy people.
It is important to point out that when certain people (typically people with insulin resistance) overeat sugars of any kind, the liver can start to become fatty, because insulin orchestrates the movement, usage, and storage of sugars and fats throughout the body. If insulin signaling isn’t working properly, fats can end up in the wrong places. In one study, when overweight men drank 25% of their daily calories as either glucose or fructose, after two weeks BOTH groups exhibited the kinds of changes that can lead to fatty liver, not just the fructose group.
Bottom line about fructose and fatty liver disease
Fructose does not raise your risk for fatty liver any more than other sugars can. Since fatty liver disease is an insulin-resistant condition, improving your insulin sensitivity could be the most effective way to reduce fat buildup in the liver. I’ll show you ways to improve insulin sensitivity in article five.
Q: Does fructose raise your blood pressure, cholesterol and triglyceride levels, increasing your risk for HEART DISEASE?
A: Fructose is no worse than glucose for your overall cardiovascular health, and may even have some advantages over glucose when it comes to blood pressure.
An excellent review about this topic summarizes what is currently known about the effects of fructose on various heart health markers. Unfortunately most of the human evidence comes from studies using too many calories, but nevertheless, even when high doses of fructose are compared to equally high doses of glucose, some differences do appear.
Cholesterol levels (fasting): There are no differences between fructose and glucose when it comes to LDL (so-called “bad cholesterol”) or HDL (so-called “good cholesterol”). However, fructose does raise total cholesterol in some people more than glucose does. But total cholesterol levels do not tell us anything about our risk for heart disease. When it comes to standard cholesterol test results, HDL is the only number worth paying attention to in estimating heart disease risk.
Triglyceride levels: Fructose temporarily raises triglycerides (blood fats) after eating more than glucose does, but does not affect fasting triglyceride levels any differently than glucose does, and it is fasting triglycerides that are used to help predict heart attack risk. If you already read article one, you saw that pure fructose has almost no effect on fat production in the liver, so you may wonder how fructose can raise blood fats, even temporarily. If fructose is eaten in combination with glucose (which is almost always the case in the real world and in human experiments), then glucose will trigger an insulin spike, and insulin will tell the liver to build fat (triglycerides). Fructose also temporarily slows down the removal of triglycerides from the blood, so the level can appear to rise even if the liver isn’t making any more triglycerides than usual.
Blood pressure: Diets high in sugars in general can raise blood pressure, at least partly because sugar can raise adrenaline levels. However, glucose raises blood pressure more than fructose in some people. This makes sense because hypertension is known to be an insulin-resistant condition, and it is high levels of glucose that overtax insulin.
Bottom line about fructose and heart disease
Fructose is no worse than glucose when it comes to increasing your chances for heart attacks, and may even be safer than glucose when it comes to blood pressure. Excess sugars in general should be your target when it comes to preventing high blood pressure and reducing your risk for heart disease.
Learn more about insulin resistance and heart disease
So, is fructose bad for you?
It turns out that excess GLUCOSE, the source of most of the sugar in our diet, is just as risky, and often riskier than fructose when it comes to these health conditions, primarily because of how glucose affects insulin and blood sugar. However, fructose at very high doses, or in people with cancer, poses health risks as well, so both of these sugars are worth minimizing.
Each and every single one of these health problems—type 2 diabetes, cancer, obesity, gout, fatty liver disease, and heart disease—is an insulin-resistant condition. Insulin resistance, which leads to high blood glucose and high insulin levels, is the scourge of our time.
Any lifestyle change you can make to improve insulin resistance, lower insulin levels and lower blood sugar, is well worth making, and will go a long way toward protecting and perhaps even completely restoring your good health. I can think of no better target, no better use of your time and energy.
In article five of this series: “How to Diagnose, Prevent, and Treat Insulin Resistance” we finally crawl out of the test tube and back into reality. I’ll show you which of your favorite foods and beverages contain the most glucose and fructose and share with you strategies you can use to improve your insulin sensitivity (including some recommendations that may surprise you). But first, we’ll take a quick detour and look at the one health problem that is absolutely caused by fructose and not glucose: fructose malabsorption. Until then, how about you?
What do you think about the connection between fructose and these common diseases? Are you any more or less afraid of fructose than you were before? Have you tried a low-fructose, low-sugar, or low-carbohydrate diet for diabetes, gout, weight loss, fatty liver, high blood pressure, or even cancer? What has your experience been?
[ad_2]






























 *Cassava bears special mention here. You may have heard of it because it is the starchy root vegetable from which tapioca is made, but cassava is also a popular staple food in many Third World countries, where it is eaten boiled, mashed, or ground into flour. Fresh cassava root contains a harmless substance called linamarin, which can turn into hydrocyanic acid (aka cyanide!) when the plant is damaged or eaten. Flaxseeds also contain linamarin. Cyanide is very toxic, so the human body converts it into thiocyanate (which, although it does interfere with thyroid function, is less toxic than cyanide and easier for the body to eliminate).
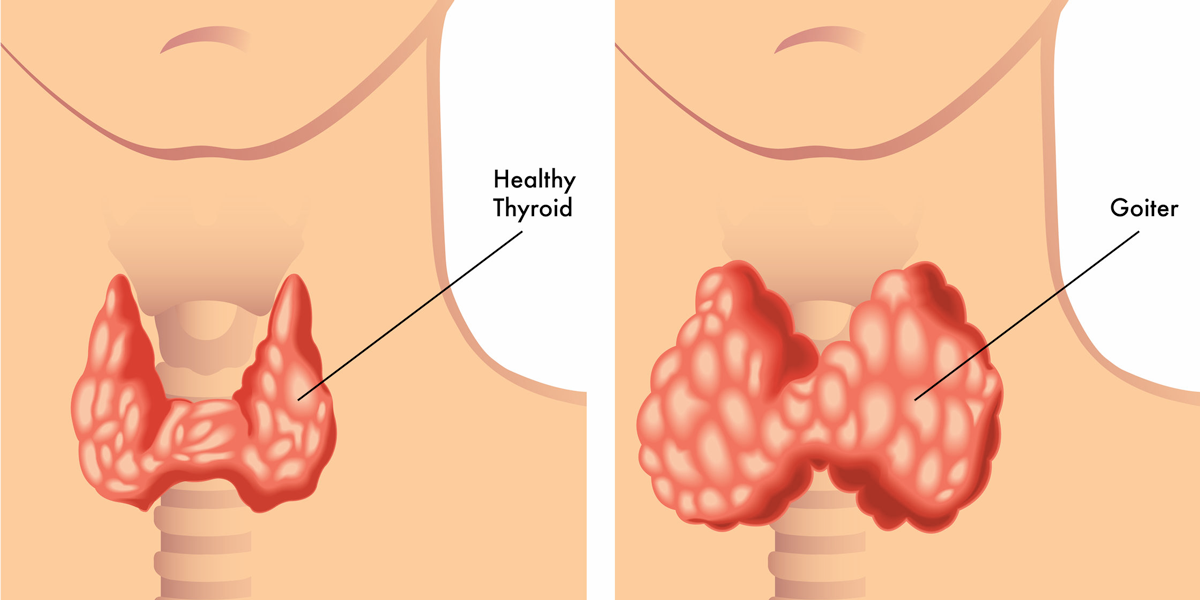
*Cassava bears special mention here. You may have heard of it because it is the starchy root vegetable from which tapioca is made, but cassava is also a popular staple food in many Third World countries, where it is eaten boiled, mashed, or ground into flour. Fresh cassava root contains a harmless substance called linamarin, which can turn into hydrocyanic acid (aka cyanide!) when the plant is damaged or eaten. Flaxseeds also contain linamarin. Cyanide is very toxic, so the human body converts it into thiocyanate (which, although it does interfere with thyroid function, is less toxic than cyanide and easier for the body to eliminate). Soy flavonoids are perhaps better known as “soy isoflavones”, which we are usually told are good for us. Yet, “it is well described but little known that the soybean and goiter have long been associated in animals and humans.” [Doerge 2002]
Soy flavonoids are perhaps better known as “soy isoflavones”, which we are usually told are good for us. Yet, “it is well described but little known that the soybean and goiter have long been associated in animals and humans.” [Doerge 2002] Millet is most familiar to us in the developed world as birdseed, but it is also a common staple grain eaten by people in developing countries, because it grows well in hot places with poor quality soil.
Millet is most familiar to us in the developed world as birdseed, but it is also a common staple grain eaten by people in developing countries, because it grows well in hot places with poor quality soil. The foods most commonly associated with excess iodine are seaweed and iodized salt. A single gram (0.035 ounce) of seaweed can contain anywhere between 16 and 2,984 micrograms of iodine!
The foods most commonly associated with excess iodine are seaweed and iodized salt. A single gram (0.035 ounce) of seaweed can contain anywhere between 16 and 2,984 micrograms of iodine!

 *Cassava bears special mention here. You may have heard of it because it is the starchy root vegetable from which tapioca is made, but cassava is also a popular staple food in many Third World countries, where it is eaten boiled, mashed, or ground into flour. Fresh cassava root contains a harmless substance called linamarin, which can turn into hydrocyanic acid (aka cyanide!) when the plant is damaged or eaten. Flaxseeds also contain linamarin. Cyanide is very toxic, so the human body converts it into thiocyanate (which, although it does interfere with thyroid function, is less toxic than cyanide and easier for the body to eliminate).
*Cassava bears special mention here. You may have heard of it because it is the starchy root vegetable from which tapioca is made, but cassava is also a popular staple food in many Third World countries, where it is eaten boiled, mashed, or ground into flour. Fresh cassava root contains a harmless substance called linamarin, which can turn into hydrocyanic acid (aka cyanide!) when the plant is damaged or eaten. Flaxseeds also contain linamarin. Cyanide is very toxic, so the human body converts it into thiocyanate (which, although it does interfere with thyroid function, is less toxic than cyanide and easier for the body to eliminate). Soy flavonoids are perhaps better known as “soy isoflavones”, which we are usually told are good for us. Yet, “it is well described but little known that the soybean and goiter have long been associated in animals and humans.” [Doerge 2002]
Soy flavonoids are perhaps better known as “soy isoflavones”, which we are usually told are good for us. Yet, “it is well described but little known that the soybean and goiter have long been associated in animals and humans.” [Doerge 2002] Millet is most familiar to us in the developed world as birdseed, but it is also a common staple grain eaten by people in developing countries, because it grows well in hot places with poor quality soil.
Millet is most familiar to us in the developed world as birdseed, but it is also a common staple grain eaten by people in developing countries, because it grows well in hot places with poor quality soil. The foods most commonly associated with excess iodine are seaweed and iodized salt. A single gram (0.035 ounce) of seaweed can contain anywhere between 16 and 2,984 micrograms of iodine!
The foods most commonly associated with excess iodine are seaweed and iodized salt. A single gram (0.035 ounce) of seaweed can contain anywhere between 16 and 2,984 micrograms of iodine!