Small changes can make a big difference! These easy swaps can help reduce additives, preservatives, and seed oils in your diet — while keeping flavour and nutrition in check.
1. Butter Blend → Pure Butter
Have you ever checked the ingredients in your butter — especially spreadable ones? Pure butter should only contain cream or cream and salt (if salted).
Swapping from butter blends to pure butter in a block or spreadable form helps reduce your intake of:
Vegetable and seed oils
Flavours
Emulsifiers
Pure butter options to try:
Westgold Butter Block
Mainland Buttersoft Pure Butter
Western Star Salted Butter Block
2. Ham/Bacon → Nitrate-Free Ham or Bacon
Ham and bacon are household staples — perfect for sandwiches, omelettes, or pasta dishes. However, most supermarket and deli versions contain nitrates (like sodium nitrate), which are used as preservatives to prevent bacterial growth and extend shelf life.
When combined with protein and heat, nitrates can become carcinogenic compounds. While it’s fine to enjoy processed meats occasionally, choosing nitrate-free options where possible is a great way to minimise exposure.
Look for these brands:
Uncle’s Smallgoods
Murray River Smokehouse
Proper Meat
🛒 Tip: Some delis or Harris Farm stores stock nitrate-free varieties — just ask!
3. Shredded Cheese → Block Cheese
Pre-shredded cheese is convenient, but did you know it often contains:
Preservative 200 (Sorbic Acid) – prevents mould and bacteria
Anti-caking agent 460 (Cellulose) – keeps cheese from clumping
While generally considered safe, excessive intake may cause allergic reactions or digestive discomfort.
Try this instead: Buy block cheese and grate it yourself, or choose cheese slices to reduce additive intake.
Peanut butter should be simple — just peanuts or peanuts and salt. Many commercial brands add vegetable oils, sugar, and antioxidant 320 (BHA) — a synthetic preservative used to prevent fats from spoiling.
Choose these natural options:
Macro Organic
Bega Simply Nuts
Mayver’s
Byron Bay
5. Dried Fruit with Sulphites → Sulphite-Free Dried Fruit
Preservative 220 (Sulphur Dioxide) is commonly used in dried fruit to preserve colour and softness. While safe for most, sulphites can trigger asthma in sensitive individuals and cause digestive issues like bloating or stomach pain.
Opt for brands that contain only fruit:
Sunny Fruit Organic
Honest to Goodness
Macro Wholefoods
Ready to make the swap?
Start small — pick one or two swaps this week and notice how much better your food tastes and feels. For more guidance on reducing additives and improving your nutrition, book an appointment with our Body Fusion dietitians today 💛
What does the gut have to do with developing Parkinson’s disease?
Parkinson’s disease is an ever-worsening neurodegenerative disorder that results in death and affects about 1 in 50 people as they get older. A small minority of cases are genetic, running in families, but 85% to 90% of cases are sporadic, meaning they seem to pop up out of nowhere. Parkinson’s is caused by the death of a certain kind of nerve cell in the brain. Once about 70% of them are gone, the symptoms start. What kills off those cells? It still isn’t completely clear, but the abnormal clumping of a protein called alpha-synuclein or α-synuclein is thought to be involved. Why? Researchers injected blended Parkinson’s brains into the heads of rats and monkeys, and Parkinson’s pathology and symptoms were induced. It can even happen when injecting just the pure, clumped α-synuclein strands themselves. How, though, do these clumps naturally end up in the brain?
As I discuss in my video The Role Meat May Play in Triggering Parkinson’s Disease, it all seems to start in the gut. The part of the brain where the pathology often first appears is directly connected to the gut, and we have direct evidence of the spread of Parkinson’s pathology from the gastrointestinal (GI) tract to the brain: α-synuclein from brains of Parkinson’s patients is taken up in the gut wall and creeps up the vagal nerves from the gut into the brain—at least that was the case in rats. If only we could go back and look at people’s colons before they got Parkinson’s. Indeed, we can. Old colon biopsies from people who would later develop Parkinson’s were dredged up, and, years before symptoms arose, you could see the α-synuclein in their gut.
Research supported by the Michael J. Fox Foundation has found that you can reliably distinguish the colons of patients from controls by the presence of this Parkinson’s protein lodged in the gut wall. But how did it get there in the first place? Are “vertebrate food products…a potential source of prion-like α-synuclein”? Indeed, nearly all the animals with backbones that we consume—cows, chickens, pigs, and fish—express the protein α-synuclein. So, when we eat common meat products, when we eat skeletal muscle, we’re eating nerves, blood cells, and the muscle cells themselves. Every pound of meat contains, on average, half a teaspoon of blood, and that alone could be an α-synuclein source to potentially trigger a clumping cascade of our own α-synuclein in the gut. Though “it may seem intuitive that dietary α-synuclein could seed aggregation in the gut,” this kind of buildup, what evidence do we have that it’s actually happening?
We have some pretty interesting data. There’s a surgical procedure called a vagotomy, in which the big nerve that goes from our gut to our brain—the vagus nerve—is cut as an old-timey treatment for stomach ulcers. Would cutting communication between the gut and the brain reduce Parkinson’s risk? Apparently so, suggesting that the gut to brain’s vagal nerve may be critically involved in the development of Parkinson’s disease.
Of course, “many people regularly consume meat and dairy products, but only a small fraction of the general population will develop PD,” Parkinson’s disease. So, there must be other factors at play that “may provide an opportunity for unwanted dietary α-synuclein to enter the host, and initiate disease.” For example, our gut becomes leakier as we age, so might that play a role? What else makes our gut leaky? “Dietary fiber deprivation has also been shown to degrade the intestinal barrier and enhance pathogen entry.” So, this raises “possibilities for food-based therapies.”
Parkinson’s patients have significantly less Prevotella in their gut, a friendly fiber-eating flora that bolsters our intestinal barrier function. So, low levels of Prevotella are linked to a leaky gut, which has been linked to intestinal α-synuclein deposition, but fiber-rich foods may bring Prevotella levels back up. “Therefore, it is possible that by adopting a plant-based diet, in addition to the beneficial effects of phytonutrients, increasing overall fiber intake may modify gut microbiota and gut permeability [leakiness] in beneficial ways for people with PD.”
So, does a vegan diet—one with lots of fiber and no meat—reduce risk for Parkinson’s? Parkinson’s “appears to be rare in quasi-vegan cultures,” with rates that are about five times lower in rural sub-Saharan Africa, for instance. All this time, we were thinking the benefits seen for Parkinson’s from plant-based diets were due to the antioxidants and anti-inflammatory nature of the animal-free diets, but maybe it’s also due to the increased intestinal exposure to fiber and decreased intestinal exposure to ingested nerves, muscles, and blood.
Wasn’t that fascinating? For more on Parkinson’s, see the related posts below.
Back in 2019, scientists proposed a new theory of endurance. For efforts lasting more than about a day, they suggested, the ultimate limit is dictated by how much food you’re able to digest. Your heart and mind and muscles can adapt to do amazing things, but they all need fuel. The most calories you can digest seems to be about 2.5 times your resting metabolism—so that’s what limits how much physical activity you can do day after day over weeks, months, or years.
This idea of a “metabolic ceiling” sparked lots of discussion, but it also left some open questions. Does it really apply to top-level endurance athletes—like, say, Kilian Jornet, who just finished climbing 72 1,400-foot summits and cycling 2,500 miles in just 31 days while quaffing olive oil for calories? A newly published study in Current Biology sets out to answer some of these questions, measuring calorie data from 14 world-class ultrarunners and triathletes and analyzing the training logs of notable athletes like Jornet. Here’s what they found.
What They Did
The study was led by Andrew Best of the Massachusetts College of Liberal Arts and Herman Pontzer of Duke University, the latter of whom was one of the key authors of the original 2019 paper. The key data in the paper comes from 14 ultra-endurance athletes who drank special isotope-labeled water that enabled the scientists to calculate exactly how many calories they were burning at different times. They collected this data during events like a six-day ultramarathon, a 24-hour record attempt, and Joe McConaughy’s 13-day FKT on the Arizona Trail. They also collected calorie data during one or more training weeks, for reasons we’ll get into below.
The calorie data from races blew through the theorical limit of 2.5 times resting metabolism. That’s because you can afford to go into calorie debt for short periods of time, meaning that you’re burning stored fat (and sometimes muscle) and losing weight. “Joe lost tons of weight running the Arizona Trail,” Best told me. But that can’t continue indefinitely. If you’re burning 9,000 calories a day (as Jornet estimates he was during his most recent challenge) but only consuming 7,000 calories a day, you might be able to keep doing that for a month or two, but you’ll eventually hit a wall.
That’s why Best also measured calories during training weeks. By taking at least two measurements for each runner, one during a competition or hard training week and the other during a relatively easy training week, he created a personalized formula for each runner to estimate how many calories they burn as a function of how much they’re running. Then he applied this formula to a year’s worth of training data to see how many calories they could burn over a 12-month period rather than just during a week or two of competition. That’s where the 2.5 resting metabolism limit shows up again.
Here’s a graph showing “metabolic scope” (which is how many calories per day you’re burning expressed as a multiple of resting metabolism) for different durations:
The longer the duration, the lower the daily calorie burn you’re able to sustain. (Photo: Current Biology)
The dark blue circles on the left side of the graph show the direct measurements of calorie burn during training and racing. There are values as high as seven times resting metabolism, which corresponds to a one-day record attempt on a 90-mile trail.
The light blue circles are calculated from the athletes’ training logs based on training periods of various lengths. For example, at the six-week mark (42 days), you can see a range of light blue circles between about 2.5 and 4. The circle at 4 corresponds to a runner who ran an astounding 1,989 miles over a six-week period, which is 332 miles per week. But that was during a 46-day FKT attempt on the Appalachian Trail, so clearly not a level the subject could sustain for an entire year.
As you extend to longer durations like 30 or 52 weeks, you can see that the light blue circles all cluster around 2.5. Some are a little higher, others a little lower, but none of these elite ultra athletes are sustaining values that are significantly higher than the proposed limit.
What about true super-elites like Kilian Jornet and triathlon star Kristian Blummenfelt? Based on their publicly available training data, along with the training hours-to-calories formula that the new study generated, Best estimates that Blummenfelt averages about 2.8 to 2.9 times his resting metabolism over the course of an entire year, while Jornet hits 2.75. So the best of the best may edge slightly above the usual limit of 2.5, but not by much.
What It Means
There are two interesting features in the graph I included above. The first and most important is the flat line on the right side of the graph, which corresponds to the proposed asymptote of 2.5 based on the limits of digestion. The new results bolster my confidence that this really is a consistent phenomenon. If Jornet isn’t breaking it (by much), I don’t know who is. So I was surprised, when I checked in with Herman Pontzer, to find that he’s less confident than he was in 2019 that this is an ironclad rule.
One of his reasons is that more data has emerged from elite cyclists at Grand Tours where they seem to be burning enormous numbers of calories without losing weight—which implies that they’re absorbing a comparable number of calories. A study of seven cyclists in the Giro d’Italia, for example, found that they burned more than four times their resting metabolism over the course of 24 days without losing weight. It may be that sports scientists’ quest to produce ever-more digestible carbohydrates is enabling cyclists to push back the limits of digestibility.
The other interesting feature in the graph is the shape of the curve on the left. You see a similar curve when you plot your speed in shorter distance (i.e. a few hours or less) races against the time elapsed, as I did for my own track times here. In that situation, the asymptote corresponds to a quantity called critical speed, which represents your long-term sustainable pace. The shape of the curve is dictated by another parameter sometimes referred to as anaerobic capacity, which you can think of (very loosely) as the amount of energy you’re able to “borrow” when running faster than critical speed before you hit a wall. Milers and other middle-distance runners tend to have a very high anaerobic capacity.
Something has to dictate the shape of Pontzer’s multi-day energy curve, and at this point he’s not sure what that something is. Intuitively, you can think of it as analogous to anaerobic capacity: you can “borrow” a lot of calories for a short period of time, putting you way above the 2.5 line; or you can borrow a lesser amount over an extended period of time. If you want to keep going for, say, six months, you can’t really borrow anything: calories out has to be balanced by calories in.
But what determines the shape of that curve? If you’re carrying a lot of body fat, does that enable you to borrow more for longer? Or, more likely, if you’ve trained your metabolism to burn fat more rapidly, does that raise the curve? Does the precise shape of the curve depend on the mix of fat and carbohydrate that you burn at different exercise intensities? Or are there other non-metabolic factors that come into play, like muscle recovery or mental fatigue? The physiology of multi-day endurance challenges is still a relatively young scientific field—which means there should be lots of more insights, and lots more fun, still to come.
In Thriving in Midlife, Claudine Francois, a functional medicine and holistic health practitioner shares her story. This episode is centered around Claudine’s new book, ‘Your Midlife Body Code’, which aims to help midlife women decode their health symptoms and realign with their bodies to achieve lasting energy, clarity, and confidence. Claudine shares her personal health journey from being a CFO to becoming a functional health practitioner and the profound impact the FDN system had on her life and career.
Claudine discusses the frustrations many women face during midlife, such as unexplained weight gain, brain fog, and fatigue, despite living healthy lives. She emphasizes the importance of identifying and addressing root causes of these symptoms like mineral depletion, gut dysfunction, hormonal imbalances, and improper stress management. Claudine aims to provide structured and targeted advice through her book, enabling women to understand and support their bodies effectively without relying solely on generic health advice or traditional medicine.
Additionally, Claudine shares real client success stories, including one of an extreme athlete who regained her energy and mental clarity by following Claudine’s recommendations based on FDN principles. She stresses the significance of foundational health practices, such as proper nutrition, sleep, and stress release, before considering lab tests. The episode wraps up by encouraging listeners to visit Claudine’s website for more information or to purchase her book, ‘Your Midlife Body Code‘.
* The original EAT Lancet diet was published in The Lancet in January 2019. A revised version (called the Planetary Health Diet) was published in October 2025.
* I analysed the nutritional content of the Planetary Health Diet (PHD) in both publications. There are many serious deficiencies in vital nutrients.
* Both reports are anti-meat and anti-ruminant.
* Following the 2019 publication, a Professor in California entered into communications with the EAT science director. The EAT science director stated categorically that the meat consumption limits were set “solely in light of health recommendations” i.e., not for climate reasons.
* The 2025 report restated this position “The PHD is based entirely on the direct effects of different diets on human health, not on environmental criteria.”
* That didn’t stop the 2025 report attacking ruminants for both health and climate reasons and calling for substantial reductions in meat and dairy production.
* The 2025 report claimed that adopting the Planetary Health Diet “could avert approximately 15 million deaths per year (27% of total deaths worldwide).” In this note I unpack how those numbers were created.
* This note also shares some of the demands/wish lists of the recent report and starts to put this in the context of a bigger agenda going on.
Introduction
Last week we reviewed the nutritional deficiencies in the revised EAT Lancet diet, now called the Planetary Health Diet (Ref 1). I reflected on this note after writing it. I wondered if the reiterated nutritional deficiencies could be attributed to ignorance or malfeasance. Do the authors not know about plant vs animal sources of nutrients, or do they not care? I don’t know the answer to that. What I do know is that the latest report has an agenda and it is part of a much bigger agenda. This week we’re going to look at the agenda. Next week we are going to look at the much bigger agenda. The agenda is anti-meat and anti-ruminant. The much bigger agenda is quite eye opening.
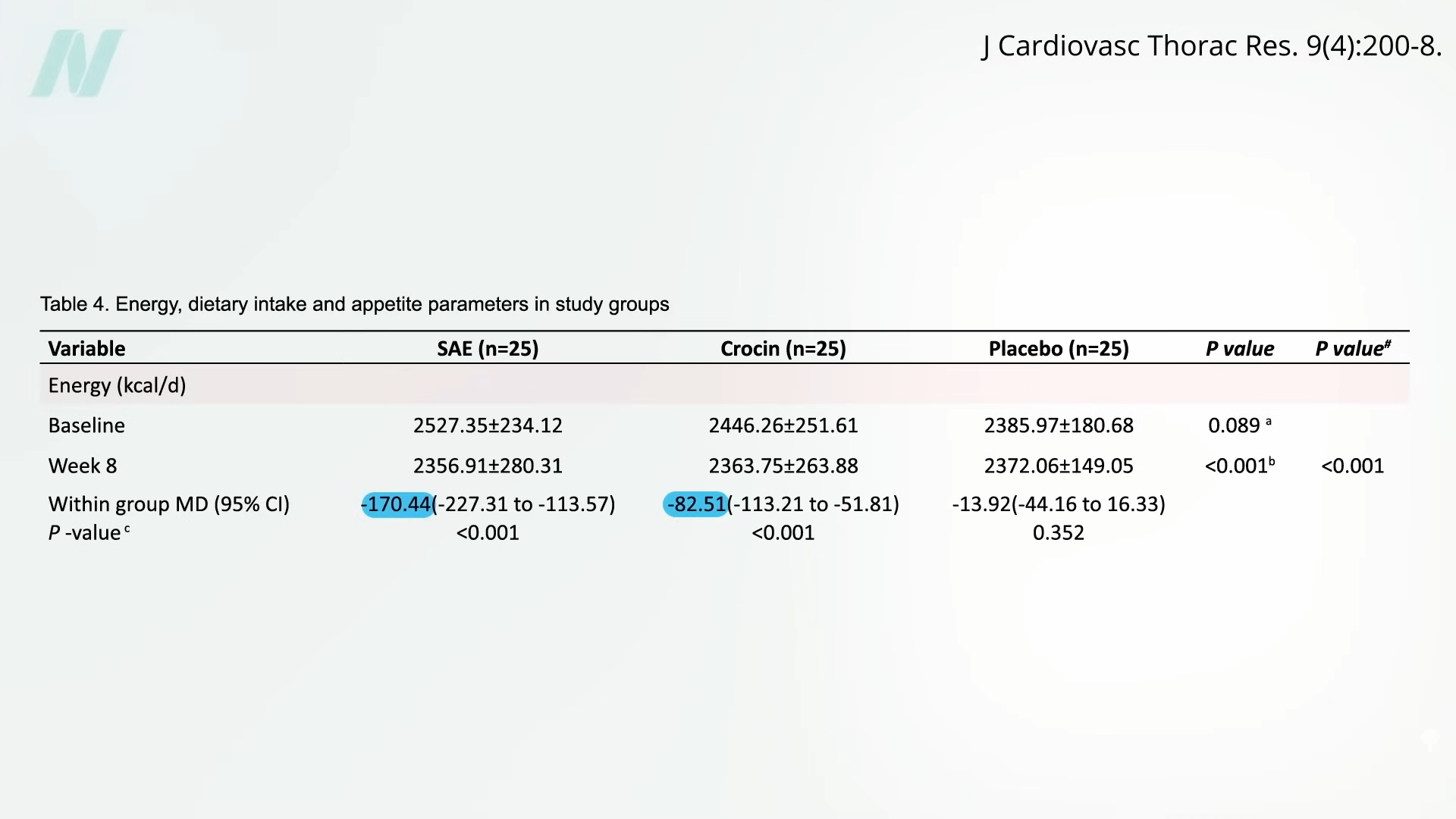
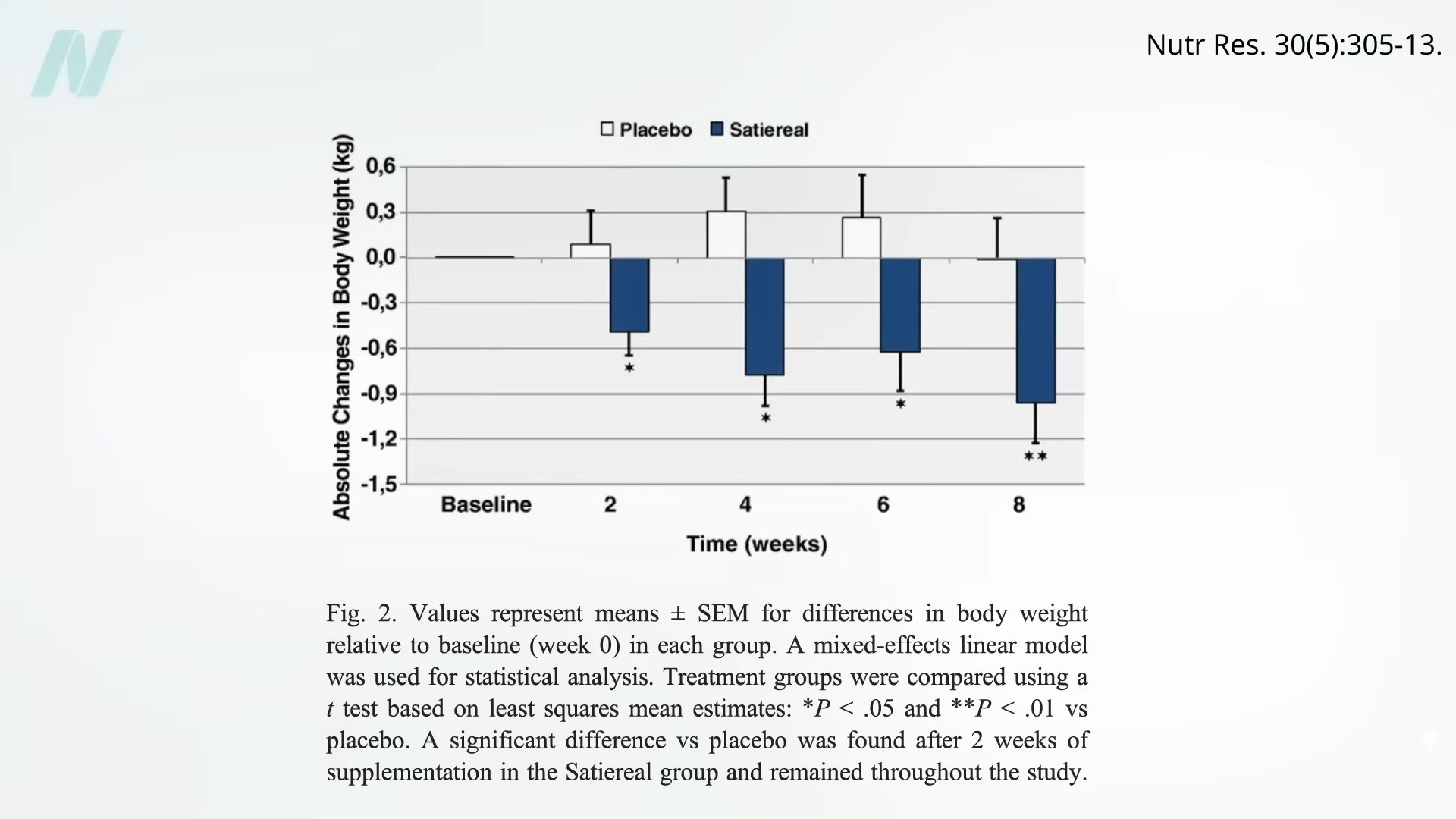
Saffron is another spice found to be effective for treating a major cause of suffering—depression, in this study, with a side effect of decreased appetite. Indeed, when put to the test in a randomized, double-blind, placebo-controlled trial, saffron was found to lead to significant weight loss, five pounds more than placebo, and an extra inch off the waist in eight weeks. The dose of saffron used in the study was the equivalent of drinking a cup of tea made from a large pinch of saffron threads.
That also led to weight loss, but it didn’t do as well as the full saffron extract and only beat the placebo by two pounds and half an inch off the waist. The mechanism appeared to be appetite suppression, as the crocin group ended up averaging about 80 fewer calories a day, whereas the full saffron group consumed an average of 170 fewer daily calories, as you can see below and at 1:21 in my video.
A similar study looked specifically at snacking frequency. The researchers thought that the mood-boosting effects of saffron might cut down on stress-related eating. Indeed, eight weeks of a saffron extract halved snack intake, compared to a placebo. There was also a slight but statistically significant weight loss of about two pounds, as you can see here and at 1:41 in my video, which is pretty remarkable, given that tiny doses were utilized—about 100 milligrams, which is equivalent to about an eighth of a teaspoon of the spice.
The problem is that saffron is the most expensive spice in the world. It’s composed of delicate threads sticking out of the saffron crocus flower. Each flower produces only a few threads, so about 50,000 flowers are needed to make a single pound of spice. That’s enough flowers to cover a football field. So, that pinch of saffron could cost a dollar a day.
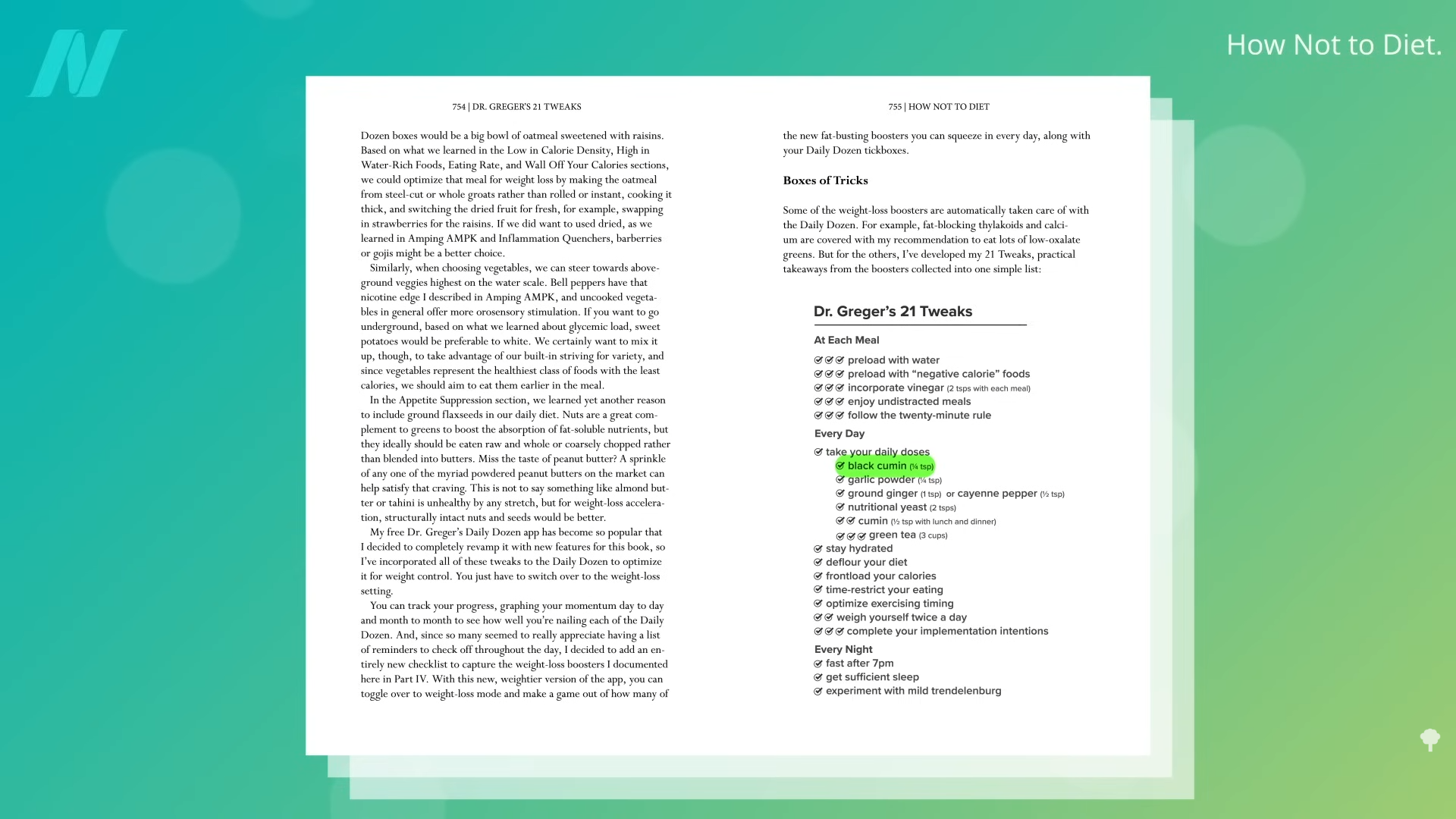
That’s why, in my 21 Tweaks to accelerate weight loss in How Not to Diet, I include black cumin, instead of saffron, as you can see here and at 2:30 in my video. And, at a quarter teaspoon a day, the daily dose of black cumin would only cost three cents.
What about just regular cumin? Used in cuisines around the world from Tex-Mex to South Asian, cumin is the second most popular spice on Earth after black pepper. It is one of the oldest cultivated plants with a range of purported medicinal uses, but only recently has it been put to the test for weight loss. Those randomized to a half teaspoon at both lunch and dinner over three months lost about four more pounds and an extra inch off their waist. The spice was found to be comparable to the obesity drug known as orlistat.
If you remember, orlistat is the “anal leakage” drug sold under the brand names Alli and Xenical. The drug company apparently prefers the term “faecal spotting” to describe the rectal discharge it causes, though. The drug company’s website offered some helpful tips, including: “It’s probably a smart idea to wear dark pants, and bring a change of clothes with you to work.” You know, just in case their drug causes you to poop in your pants at the office.
I think I’ll stick with the cumin, thank you very much.
In GLP-1s: Miracle or Mistake, Jennifer Woodward returns to discuss the innovative use of peptides, particularly GLP-1s, in health optimization. Jennifer, who has successfully used these compounds to address her own health challenges and those of her clients, describes how peptides can transform health by addressing issues such as hormonal imbalances, inflammation, and food addiction. Jennifer emphasizes that these treatments should be considered supplementary to a foundational healthy lifestyle, including proper diet, rest, exercise, stress management, and proper supplementation, rather than as standalone miracle solutions.
The conversation also touches on the controversial nature of the burgeoning peptide market, underscoring the importance of sourcing peptides through safe and regulated channels. Jennifer warns against the dangers of obtaining peptides from questionable online sources and advocates for using compounding pharmacies that require prescriptions and offer comprehensive support.
The discussion includes the therapeutic potential of peptides for various addictions, including alcohol and food, highlighting how they can aid in reducing compulsive behaviors by modulating brain chemistry. The episode concludes with insights on how Functional Diagnostic Nutrition Practitioners can ethically and legally guide clients interested in peptides, without overstepping their scope of practice.
GLP-1s, Miracle or Mistake: Topics
00:00 Welcome to the Health Detective Podcast
00:33 Introducing Today’s Guest: Jennifer Woodward
02:02 Diving into Peptides and GLP-1s
02:56 Jennifer’s Personal Journey with GLP-1s
04:12 The Impact of GLP-1s on Health and Wellness
07:59 Evolving Perspectives on Health and Supplements
13:49 Understanding Peptides: What They Are and How They Work
16:38 Real-Life Success Stories with Peptides
22:24 GLP-1s: Who Can Benefit and How
26:50 Microdosing Tirzepatide: An Overview
27:41 Subjectivity and Controversy in Microdosing
29:06 Side Effects and Dosage Considerations
29:46 Audience Interaction and Questions
30:47 Exploring the Wolverine Stack
32:51 Addiction and GLP-1s
35:25 Sourcing Peptides Safely
39:40 Empowering Clients with Peptide Knowledge
43:47 Ethical Considerations and Final Thoughts
Where to Find Jennifer Woodward
Go to our Health Detective Podcasts for more informational and functional health-oriented podcasts like this one.
While anti-inflammatory food lists usually focus on leafy greens and berries, nutrition experts say this orange squash deserves a spot at the top
(Photo: Ayana Underwood/Canva)
Published October 16, 2025 01:29AM
When you search for anti-inflammatory foods, most results suggest adding tomatoes, green leafy vegetables, strawberries, whole grains, and fatty fish like salmon to your diet. While these are fantastic recommendations, they’re a bit uninspiring. When I learned that pumpkin has anti-inflammatory properties, I was pleasantly surprised and grateful that I already had the plump gourd in my cupboard.
I buy canned pumpkin every week to prepare frozen treats for my pup, Ollie, because research shows that the fiber content in pumpkin (about three grams per cup) can promote better digestion and combat diarrhea in dogs.
After speaking with two sports dietitians, I learned that pumpkin is also great for humans. Here’s how adding more pumpkin to your diet can aid your overall health and performance.
How Inflammation Affects the Body
Inflammation is the body’s immune response to an illness or injury. It can occur outside the body—like if you scrape a knee and get a scab—or inside the body due to a variety of health or lifestyle reasons, such as having an underlying disease like obesity, sleeping poorly, eating a diet high in processed foods, drinking alcohol, smoking cigarettes, or over-exercising and straining your muscles.
To heal, the body releases a range of substances (mainly hormones and inflammatory molecules) that dilate blood vessels to help blood and immune cells reach the injured tissue. This process facilitates healing, but it can also irritate nerves along the way, causing pain, swelling, and redness near the affected tissue.
Short-term inflammation, which is sudden and temporary, is typically no big deal, but long-term chronic inflammation (which can persist for months, even years) can be a huge problem. If left untreated, the body can’t heal. The inflammation will compound, which can lead to serious health issues (such as stroke and cancer), an impaired immune system, and, in the case of overtraining, muscle fatigue, impaired performance, and a higher risk of injuries, says Allison Childress, a sports dietitian and associate professor in the department of Nutritional Sciences at Texas Tech University.
Why Is Pumpkin Such a Potent Anti-Inflammatory Food?
To recover quickly and lower your risk for certain diseases, you want to eat foods that can naturally reduce inflammation, says Natalie Allen, a dietitian and clinical associate professor of nutrition and dietetics in the School of Health Sciences at Missouri State University.
Pumpkin Has a High Antioxidant Profile
Pumpkin is loaded with antioxidants like beta-carotene, substances that prevent or delay cell damage, says Allen. They do this by reducing oxidative stress, a condition where molecules called free radicals grow out of control and damage your organs and tissue, says Childress. This, in turn, lowers levels of inflammation in your body, which is crucial not only for your overall health but for muscle recovery as well.
After a strenuous workout, your muscles experience mild inflammation, and eating foods with antioxidants can reduce it, Allen explains. The result? Faster recovery and fewer injuries.
Pumpkin Is Nutrient-Dense
The next perk: pumpkin is full of fiber. Research shows that fiber enhances the diversity of your gut microbiome, the community of microbes that live in your digestive tract, helping decrease inflammation in your body, says Childress.
Pumpkin is a great source of potassium (one cup of canned pumpkin contains 505 mg of potassium, 15 and 20 percent of the recommended daily value for men and women, respectively), which is an important electrolyte your body expels through your sweat, says Childress. Replenishing electrolytes after an intense workout can “reduce exercise-related inflammation and muscle soreness,” she says. It can also prevent muscle cramps, adds Allen.
Additionally, one cup of pumpkin contains about 11 mg of vitamin C; that’s roughly 13 percent and 15 percent of the daily recommended value for men and wommen, respectively. “When we think about soft tissue repair, like ligaments and tendons and muscles, vitamin C is a key nutrient,” says Childress. As long as you’re also eating enough protein, she adds, consuming vitamin C can help your muscles, bones, and cartilage recover and grow.
How Much Pumpkin Do You Need to Reap Its Anti-Inflammatory Benefits?
Roughly half to one cup per day. However, for many, this much pumpkin isn’t realistic, Allen says. So you can aim to hit these daily recommended values by consuming a mix of vitamin A sources, including sweet potatoes, carrots, squash, and peppers. The goal is to eat about 5.5 cups of orange vegetables each week.
The Best Ways to Add Pumpkin to Your Diet
Pumpkin isn’t just for pies—it can be added to so many snacks and meals.“Pumpkin purée, in my professional opinion, is as good as if you got a pumpkin, roasted it, and puréed it yourself,” says Childress.
So, add a cup of pumpkin purée to a smoothie, make protein bites or balls using a mix of rolled oats, pumpkin purée, pumpkin pie spice, flour, and chocolate chips or nuts. You can spread pumpkin purée over a piece of toast and drizzle it with honey, peanut butter, almond butter, or Greek yogurt.
Add a half cup to your morning oatmeal, add it into your pancake mix, or whip up a pumpkin hummus for an afternoon snack. Or, hey, do what I do for my dog and freeze a dollop of pumpkin alongside Greek yogurt and peanut butter (it’s actually extremely tasty).
You can also cook real pumpkin as you would spaghetti squash—carve out the seeds and strings, pour some olive oil on it, and roast it in the oven for about 45 minutes at 350℉. As for pumpkin seeds, you can toss them in salads, parfaits, or trail mix, Allen recommends. Just make sure to chew them thoroughly; otherwise, they’ll pass right through you, and you’ll lose out on the benefits, says Childress.
When Is the Best Time to Eat Pumpkin?
Allen says the best time to eat pumpkin is within an hour after working out, especially when paired with a protein or carbohydrate, because your body is primed to absorb nutrients more effectively, says Allen.
But if you miss that window, don’t worry. Pumpkin is just as nutritious any time of day, says Allen. “It’s a very nutrient-rich food and you don’t need very much of it to get a lot of bang for your buck,” she says.
Please note: This blog contains descriptions of sexual assault.
“Recent reports of medical students performing pelvic exams for training purposes on anesthetized women without their consent”—or their knowledge—“have produced a firestorm of controversy and calls for greater regulation.” However, that “burst of public outcry” was in the mid-1990s. California was the first state to make the practice illegal, but the “early gains quickly petered out.”
As I discuss in my videoEnding the Hidden Practice of Pelvic Exams on Unconscious Women Without Their Consent, “This practice, common since the late 1800s, was largely unchallenged until a 2003 study reported that 90 percent of medical students who completed obstetrics and gynecology (ob-gyn) rotations at four Philadelphia-area medical schools performed pelvic exams on anesthetized women for educational purposes.” (A subsequent study found the percentage to be lower than that in other areas of the country.) The bottom line? “Pelvic Exams Done on Anesthetized Women Without Consent: Still Happening.” How can this continue into 2025? Medical ethicists have called such practices “immoral and indefensible.” “At the end of the day, this is a practice that should come to an abrupt and immediate halt.” Some schools vowed they’d end the practice, but, unfortunately, these early victories quickly stalled. At the same time, a handful of schools revamped their policies, an equal number of hospitals and medical schools publicly dug in, defending the practice.
The Association of Professors of Gynecology and Obstetrics wrote: “As medical educators, we must balance our obligation to develop the next generation of physicians with women’s freedom to decide from whom they receive treatment and what aspects of their care are performed by learners.” “Some especially blunt teaching faculty contend that ‘public’ patients”—those without health insurance—“owe it to the facility and society to participate since they receive free or subsidized care.” Regulations to curb this practice are said to be “placing inappropriate and unnecessary barriers in the way of medical students who need to learn fundamental medical skills” and therefore “should be resisted.” Unsurprisingly, medical students still perform pelvic exams on anesthetized women.
Professional medical societies have given lip service to the concept of asking for explicit consent, but despite the recommendations, “evidence…suggests that the practice is alive and well.” And the “unauthorized use of women is not a localized phenomenon confined to a handful of errant medical schools,” a few bad med school apples, but an international problem.
Even with the emergence of the #MeToo movement and even after Larry Nasser, the infamous USA gymnastics doctor, was sentenced to 40 to 175 years in prison for touching women’s genitalia without their consent, “there are still women who are being used as teaching subjects for these exams without their permission, without their consent.”
A 2020 update from Yale’s Center for Bioethics was entitled: “A Pot Ignored Boils On: Sustained Calls for Explicit Consent of Intimate Medical Exams.” It reads, “Over the last 30 years, several parties—both within and external to medicine—have increasingly voiced opposition to these exams. Arguments from medical associations, legal scholars, ethicists, nurses, and some physicians have not compelled meaningful institutional change.” Yes, there is the lip service paid by medical associations recommending bans on pelvic exams without consent, but those statements are “advisory and incomplete. Associations simply do not have the capacity to compel systemic change, as evidenced by institutions’ inaction.” In response to the medical profession’s inability to police itself, many states have passed legislation to protect patients from this practice.
But, of course, if you are anesthetized, how would you even know if medical students are lining up or not? “Teaching hospitals take patients who are in the worst position to know what’s occurring—they are unconscious—and use them in ways that leave no physical signs and are often undocumented in the patients’ medical records.” So, when the media loses interest, as it has decade after decade, “what incentive is there for teaching faculty or hospitals to voluntarily change?” Perhaps, “when physicians start being threatened with litigation, they’ll start obtaining informed consent.” As one commentator wrote, “Hospital administrators who allow medical students in their facilities to perform pelvic examinations on unconsenting anesthetized women ought to consult with their legal counsel concerning the definition of rape in their jurisdiction.”
“The solution is simple: Just ask.” Ask women for permission. It’s their body, their choice. “But recent experience has shown that meaningful and complete hospital-by-hospital change is unlikely to come until a hospital or doctor pays a substantial award [in some lawsuit] for this error in ethical judgment. We believe that day is coming soon, lest that ignored pot finally boil over.
“Some defend it as harmless and say asking for consent would make it more likely that patients would say no, denying students a crucial part of their training.” When I first wrote about this practice more than 20 years ago in my book Heart Failure about my time in medical school, I talked about how I had gotten the same comments from my classmates: “A well-then-how-are-we-going-to-learn response. To even present such a question is to lose a bit of one’s humanity. The answer, of course, is we should learn from women who give their consent! And to do that—God forbid—we might actually have to first establish a relationship with the patient, a trust—talk to them even. We may have to treat them like human beings.”
It’s unconscionable that medical students are legally allowed to practice pelvic exams on anesthetized women without their consent. Even if you live in one of the states where this practice is technically illegal, how do you know the law will be respected once you’re unconscious? Maybe medical students should wear bodycams.
Anxiety/Depression/Eating Disorder and Amino Acid Therapy: Summary
In Anxiety/Depression/Eating Disorder and Amino Acid Therapy, Laurie Hammer, a functional nutritional therapist and neuro nutrient specialist focuses on addressing brain toxicity, depression, anxiety, eating disorders, and autoimmune conditions through holistic methods. She shares her personal journey of overcoming cancer, celiac disease, bulimia, and depression, revealing how these experiences drive her passion to help others, particularly mothers dealing with the overwhelming demands of life.
Laurie emphasizes the significant role of amino acid therapy in addressing mental health issues and how it changed her life. She explains that trauma and other health issues can deplete amino acids and replenishing these can offer significant relief. Laurie details how she sends clients amino acid kits and uses symptom-based surveys to determine the most effective combinations. This initial relief allows clients to make further health improvements, like addressing root causes of inflammation and changing their diet.
Laurie also addresses the historical context of amino acid use and shares a success story of a client who transitioned off multiple medications through her guidance. For those interested in learning more, she recommends Julia Ross’s book “The Mood Cure” and invites listeners to connect on Instagram or through her website. Laurie ends the podcast emphasizing the importance of sleep for overall health.
Anxiety/Depression/Eating Disorder and Amino Acid Therapy: Topics
00:00 Welcome to the Health Detective Podcast
00:51 Introducing Laurie Hammer: Overcoming Health Challenges
01:43 Laurie’s Personal Struggles with Bulimia
05:08 The Turning Point: Seeking Help and Discovering Holistic Methods
12:19 Amino Acid Therapy: A Game Changer
21:46 Laurie’s Journey to Healing and Helping Others
24:24 Introduction to Lab Testing in Practice
24:48 The Science Behind Neurotransmitter Testing
25:29 Amino Acid Therapy: An Overview
27:21 Effectiveness and Nuances of Amino Acid Therapy
28:46 Mental Health and Amino Acid Therapy
33:50 History of SSRIs and Amino Acid Therapy
39:16 Client Success Stories and Testimonials
44:55 Final Thoughts and Next Steps
Where to Find Laurie Hammer
Go to our Health Detective Podcasts for more informational and functional health-oriented podcasts like this one.
* “The EAT Lancet diet” was published in January 2019. The diet (with ranges) was specified to the gram and calorie. Animal food intake (meat fish, eggs and dairy) could be zero.
* I analysed the nutrition content of the diet. Even using the maximum intake of animal foods allowed, the diet was severely nutritionally deficient. The most significant concerns were retinol, vitamin B12, vitamin D, vitamin K, calcium, iron, and omega-3 essential fatty acids.
* I submitted a letter to the Lancet pointing out the deficiencies. They refused to publish it.
* On 2nd October 2025, an update of the EAT Lancet diet was published. It is now called “The Planetary Health Diet.”
* This post shares the original diet, nutrient analysis and list of deficiencies. It then reports on the 2025 diet and compares the two diets to highlight what has changed and to see if the nutritional deficiencies have been addressed. Using the Supplementary Appendix called “What is a healthy diet?“, this note reviews if deficiencies have been addressed or explained.
Introduction
A report was published in The Lancet on 17th January 2019. The report was commissioned by The Lancet. The report was written by 37 people from 16 different countries and was 3 years in the making (Ref 1). The report launched something interchangeably called “The healthy reference diet” and/or “The EAT Lancet diet”, or just “The EAT diet.”
The report contained a table detailing the recommended diet. On the day of publication, I put the specified food items into a tool that worked with the USDA (United States Department of Agriculture) all-foods database. This analysed the nutrient composition of the recommended diet. Animal food intake was positioned as 0 to X grams, because the authors were content for people to follow a vegan diet with no animal foods whatsoever. Even using the maximum intake of animal foods allowed, the diet was severely nutritionally deficient.
On 26th January 2019, I submitted a letter to The Lancet detailing the nutritional deficiencies (Ref 2). On 7th March 2019, I received a reply from The Lancet saying, “I am sorry to say that we are unable to accept it for publication.” They weren’t sorry at all. That was their choice. They didn’t want criticism posted alongside their (commissioned) flagship diet.
On 2nd October 2025, an update of the EAT Lancet diet was published. It is now called “The Planetary Health Diet” – abbreviated to PHD (Ref 3). In the 76 page report, PHD occurs 164 times and “planetary” a further 153 times. I don’t know where to start on the arrogance and hubris of multiple authors who think that they can tell the world what to eat and why.
This week’s note reviews the revised diet to see if the original nutritional deficiencies have been corrected. Spoiler alert – they haven’t. I don’t need to repeat the nutritional analysis, as the revised diet is so close to the original. This note, therefore, shares the original diet, nutrient analysis and list of deficiencies. It then reports on the 2025 diet and compares the two diets to highlight what has changed.
Five supplementary appendices were published alongside the 2025 update. Appendix 1 tried to address nutrients needed and nutrients delivered. This note analyses that document to see if nutritional deficiencies have been addressed or explained.
Join us as we celebrate the completion of the Functional Diagnostic Nutrition (FDN) course with one of our graduates. In this video, hear about her year-long journey, why she turned down naturopathic school, and how she discovered FDN through an unconventional way on Instagram. Learn about her health struggles, including endometriosis and PCOS, and how the FDN course helped her not only improve her own health but also provide better guidance to her clients. We discuss her background, her thoughts on the course structure, and her future aspirations including a move to Florida and involvement in a supplement business. Get insights into the importance of liver health, the benefits of a self-paced course, and the strong support system within the FDN community. Don’t miss out on this inspiring conversation about overcoming challenges, the value of continuous learning, and the importance of aligning with your true values.
00:00 Course Completion Excitement 00:25 Discovering the Course 01:56 Course Benefits and Personal Health 03:36 Educational Background and Career Path 08:41 Future Plans and Aspirations 11:53 Business Strategies and Pricing 16:18 Discussing Course Improvements 17:00 Importance of Course Updates 18:05 Completion Rates and Student Support 20:10 Highlighting the Liver’s Role 21:55 Building and Managing a Business 25:12 Future Plans and Opportunities 26:53 Concluding Remarks and Farewell
In this episode, Reed interviews Kailey, an accomplished IIN graduate who recently completed the FDN course. Kailey shares her journey, starting from her initial discovery of FDN through Instagram, to the detailed expectations she had for the course—particularly in the areas of lab testing and clinical correlation. She highlights how FDN exceeded her expectations and discusses the challenges and successes she experienced during the course. Kailey also talks about her shift from working in marketing to becoming a full-time health coach, the ways in which the FDN training has enhanced her practice, and her future plans. Notably, she explains how she utilized tools like Notion to improve her learning experience and manage client information effectively. Reed offers insights into the ongoing support and community within FDN and seeks Kailey’s advice on enhancing the course further.
00:00 Introduction and Congratulations 00:15 Discovering FDN 01:11 Course Expectations and Experiences 02:33 Transitioning to FDN 03:04 Impact on Career and Pricing 04:08 Marketing Job and Health Journey 05:31 Future Plans with FDN 08:24 FDN Community and Support 12:42 Tools for Success 19:59 Final Thoughts and Congratulations
Join Reed as he interviews Debbie, a newly minted FDN graduate, who shares her inspiring journey from a 20-year career as a nurse practitioner to discovering Functional Diagnostic Nutrition (FDN). Debbie talks about the challenges she faced, the unique aspects of the FDN course, and the skills and certifications that have transformed her professional and personal life. She also offers insights into how FDN filled gaps in her practice and discusses the potential for future collaborations and improvements within the FDN community. This episode is a deep dive into the value of FDN and its impact on healthcare practices.
00:00 Introduction and Congratulations 00:22 Discovering FDN: A Life-Changing Journey 01:29 Professional Background and FDN Impact 02:20 FDN Course Experience and Challenges 06:29 Future Aspirations with FDN 08:31 Pricing and Packaging Strategies 14:53 Course Feedback and Suggestions 22:05 Final Thoughts and Graduation
In this heartwarming interview, a nurse with a Doctorate in Nursing Practice shares her transformative experience with an FDN course. Highlighting her extensive career in pediatric healthcare, she discusses the practical application of the course in real life and how it connected various aspects of her knowledge. She emphasizes feeling reinvigorated and inspired to help others in new ways, moving from traditional healthcare towards functional health. The conversation covers her expectations, experiences, and future plans in functional health, along with her intent to balance her current job and new business venture. Tune in for an authentic and insightful discussion on transitioning careers, the value of continuous learning, and the potential of functional health practices.
00:00 Introduction and Course Completion 00:42 Discovering the Program 01:51 Educational Background and Career 02:22 Functional Health Journey 04:16 Expectations and Experiences 05:25 Future Plans and Business Vision 13:23 Feedback and Suggestions 18:32 Final Thoughts and Opportunities
Fall’s favorite ingredient isn’t just for pie—it’s my new secret protein weapon
(Photo: Recipes: Ashia Aubourg; Design: Ayana Underwood/Canva)
Published October 10, 2025 03:04AM
Pumpkin season returns every year with lattes, pies, and donuts in tow. But beyond the sweet nostalgia, can the orange squash actually fuel an active lifestyle? It turns out that the four protein pumpkin recipes I found can.
“Pumpkin offers a wide range of vitamins and antioxidants that can support your body,” says Yvette Hill, a registered dietitian nutritionist based in Boulder, Colorado. One cup of pumpkin purée provides 7 grams of fiber, 505 milligrams of phosphorus, 63 milligrams of calcium, and over 10 milligrams of vitamin C.
Pair pumpkin with protein, and you’ve got a superfood. “Protein helps build muscle, supports your immune system, and keeps you feeling fuller for longer,” says Hill. That’s a serious advantage if you’re heading out for a long hike or want to recover faster after getting banged up while traversing on rocky terrain.
Hill recommends aiming for 20 to 30 grams of protein per meal. If that sounds like a lot, don’t stress, snacks count too. Spread your intake throughout the day and you’ll hit your goal more easily than you think.
If you’re ready for something more exciting and satisfying than the usual pumpkin muffins, smoothies, and lattes this season has to offer, try these fun and nutritious, nutritionist-approved pumpkin recipes below.
1. Pumpkin Pie Overnight Oats with Chia Seeds
Overnight oats made with Greek yogurt, almond milk, pumpkin purée, maple syrup, vanilla extract, chia seeds, and pumpkin pie spice. (Photo: Ashia Aubourg)
I recently tested this pumpkin pie overnight oats recipe for a story about balancing blood sugar. It was delicious, so I was excited to learn that it doubles as a high-protein breakfast.
In a bowl, whisk together Greek yogurt, almond milk, pumpkin purée, vanilla, and maple syrup. Stir in the oats, chia seeds, and pumpkin spice until thoroughly mixed.
Scoop the mixture into a sealable jar or container and store it in the fridge overnight, or for at least four hours.
“The oats, chia seeds, and Greek yogurt make this breakfast a good source of protein,” says Hill—a single serving provides nearly 18 grams—enough to keep you full through the morning.
To level it up, Hill suggests mixing in 1/4 cup of peanut butter and 1/4 cup of almonds. That combo can push the total to over 40 grams of protein.
The Verdict: Filling and Decadent
I’ve made this recipe before, and it couldn’t be more straightforward. If you meal prep regularly, it deserves a spot in your rotation. It takes about five minutes to assemble, then the fridge handles the rest. The oats set into a mousse-like texture with that familiar, cozy pumpkin spice flavor. I took Hill’s tip and stirred in a spoonful of peanut butter, which added richness and a hint of salt that balances its sweetness without overpowering the pumpkin. I ate it right before a hike and stayed full the entire trek.
2. Pumpkin Butter Chickpeas
Stewed chickpeas made with yellow onion, garlic, ginger, garam masala, curry powder, turmeric, cayenne pepper, other spices, chickpeas, coconut milk, pumpkin purée, tomato paste, butter, and cilantro. (Photo: Ashia Aubourg)
After a big hike, I usually go for butter chicken. It’s one of my go-to takeout meals. So when I came across a chickpea version, I had to try it. Instead of tomatoes, the creator uses pumpkin purée to build the sauce, and that twist sealed the deal. I skipped ordering out and cooked it myself.
2 tablespoons salted butter (coconut oil if you follow a vegan diet)
1/4 cup fresh cilantro, roughly chopped
Recipe:
Heat the olive oil in a large pan over medium heat. Add the onions and cook for five minutes or until fragrant. Add the garlic and ginger, cooking for an additional two minutes. Stir in the garam masala, curry powder, turmeric, cayenne, and a pinch of salt and pepper. Cook for about one more minute.
Add the chickpeas and toss to coat with the spices.
Stir in the coconut milk, pumpkin purée, tomato paste, butter, and 1/2 a cup of water. Simmer for five minutes, until the sauce has thickened slightly. Remove from the heat and stir in the cilantro. Season with salt and pepper, to taste.
Serve the chickpeas on their own or with rice, naan, or quinoa.
This dish holds up on its own, says Hill. There are approximately seven ounces of chickpeas in one serving of this dish, which provides around 13 grams of protein. In one serving, the coconut milk adds an extra three grams of protein. For an extra protein boost, Hill suggests serving this curry over half a cup of quinoa. That simple addition adds over 11 more grams, bringing the total to 27 grams, turning this comfort food into a protein superfood.
The Verdict: Hearty Comfort Food with a Little Spice
I went for a hike and didn’t walk away with any injuries, but the soreness hit hard, which is pretty normal for me. This pain sometimes lingers into the next morning, so I wanted something quick and restorative for dinner once I got home. This meal came together in just 30 minutes, and I couldn’t stop going back for more. The chickpeas, coated in a rich, pumpkin butter sauce, tasted slightly sweet with just enough heat from the pinches of cayenne pepper. The next day, although I still felt a little sore, I had the energy actually to move through my day.
3. Pumpkin Protein Balls
Snack bites made with oats, almond butter, pumpkin purée, vanilla protein powder, ground flaxseed, chia seeds, maple syrup, cinnamon, pumpkin pie spice, and chocolate chips. (Photo: Ashia Aubourg)
I always keep a stash of protein bites in the fridge. Whether it’s pro climber Sasha DiGiulian’s bars or cheese sticks, I like having something quick and satisfying within reach. So, when I found a recipe that combines oats, peanut butter, pumpkin purée, and other good ingredients into bite-sized fuel, I knew I had to try it.
Yield: 12 balls
Ingredients:
3/4 cup old-fashioned rolled oats
1/4 cup almond butter
1/4 cup pumpkin purée
1 scoop (25 grams) vanilla protein powder
1/2 tablespoon ground flaxseed
1/2 teaspoon pumpkin pie spice
1 teaspoon chia seeds
3 tablespoons maple syrup
Pinch of cinnamon
1 tablespoon chocolate chips
Recipe:
Add all the ingredients to a bowl and stir until well combined.
Once mixed, use a small ice cream scoop or tablespoon to dig out and form the dough into 12 balls.
Store in an airtight container in the refrigerator for up to one week or in the freezer for up to three months.
This snack provides a solid source of protein from oats, chia seeds, almond butter, and a scoop of powder. Each bite packs around five grams of protein, making it an easy win for pre- or post-workout recovery or trail fuel. While the recipe calls for vanilla protein powder, chocolate or coffee-flavored powders work just as well to keep things interesting.
The Verdict: Easy and Delectable
Even though I write about protein all the time (and fully understand its benefits), I don’t always hit 20 grams per meal. Life gets busy. What I like about these bites is that they offer small wins throughout the day. Grabbing two or three puts me halfway to my protein goal before dinner even starts. And they’re so good. These bites taste like pumpkin oatmeal cookies with a gooey, cookie-dough-like texture.
4. Pumpkin Bolognese
Bolognese pasta made with onions, garlic, carrots, celery, oregano, ground beef, tomato paste, pumpkin purée, and seasonings. (Photo: Ashia Aubourg)
Bolognese is a classic Italian pasta dish built with ground beef, aromatics, and a rich tomato base. But a version from the blog Mon Petit Four caught my eye. Instead of red sauce, it uses pumpkin purée. I had to try it.
Yield: 6 servings
Ingredients:
1 box of pasta
1 tablespoon extra virgin olive oil
1/2 large onion, diced
2 cloves garlic, minced
1 medium carrot, finely chopped
1 celery stalk, finely chopped
1 teaspoon dried oregano
1 pound ground beef
1/2 cup tomato paste
3/4 cup pumpkin purée
salt and pepper, to taste
reserved pasta water
Recipe:
Cook the pasta according to the package directions, adding one tablespoon of salt to the water in the pot. Drain the pasta, reserving some of the pasta water.
In a large pan over medium heat, warm the olive oil. Add the diced onion and cook until translucent, about three minutes. Add the garlic, carrot, celery, and dried oregano. Sauté for five minutes, until the vegetables become tender.
Add the ground beef and break it up into smaller pieces. Cook the beef until it’s browned, then add the tomato paste and pumpkin purée. Add a generous pinch of salt and pepper. Stir everything together and let the paste and purée cook with the beef for a couple of minutes.
Add some of the reserved pasta water, one ladle at a time (about 1/4 cup), until the sauce is as thick or loose as you like it. Allow the sauce to simmer on low heat for a minute.
If your pan is big enough, toss the pasta with the sauce in the pan. If not, then pour the sauce over the spaghetti.
Hill gives the recipe high marks as is. One serving of this dish contains approximately three ounces of ground beef, providing nearly 16 grams of protein. For an extra boost, she recommends substituting regular pasta with pasta made from red lentils. That simple switch can increase the total protein content from three grams in the regular pasta to nearly 15 grams in one serving of this dish. So, if you didn’t get your protein intake in at lunch, don’t worry—dinner has you covered.
The Verdict: A Tasty Way to Upgrade Bolognese
This pumpkin Bolognese hit all the right notes: rich, satisfying, and just as flavorful as the traditional version, with a little extra creaminess from the purée. The sauce leaned slightly sweet, as expected, so I added a few shakes of red pepper flakes to bring some heat. It left me full and fueled. The next morning, I headed out for a beach jog, feeling strong, a reminder that pumpkin pulls double duty: it’s both a seasonal comfort food in the kitchen and a performance fuel on the trail.
We had the pleasure of talking with Ale Graf about her work, food, and National Hispanic Heritage Month. We hope you enjoy this interview and her recipe for Hibiscus Chamoy.
As someone who creates Mexican dishes with a plant-based twist, how is food an important part of your culture and how you share your culture with others?
Food is so much more than nourishment—it’s how we love, connect, and remember who we are. For Mexicans, food is truly part of our DNA. From ancient times, when our ancestors offered food to the gods, to modern-day sobremesas with family and friends, sharing food is how we express love. I grew up surrounded by women who talked about recipes the way others talk about dreams. My mother, grandmother, and aunts were always planning the next meal or discovering a new dish. Now I do the same with my siblings. Even though my food today is mostly plant-based, its essence is the same: to bring people together. Through my recipes, I want to recreate that sense of belonging, of always having enough to share and always leaving room for one more at the table. That’s what comemos means to me. It’s not about nostalgia; it’s about showing what being Mexican really looks and tastes like today.
When did you start cooking and developing your own recipes? How do you educate people about making beautiful Mexican dishes using plant-based ingredients? Are people ever surprised to learn your recipes are plant-based?
I started 23 years ago, right after my son was diagnosed with a dairy allergy. That moment changed everything. I had to relearn how to cook. I leaned into spices, explored new vegetables, and discovered different cooking methods. What began as a necessity quickly turned into a passion. I even enrolled in an online course to get certified as a plant-based cook. As my kids grew, so did my curiosity and creativity in the kitchen. Educating others has always been fun for me. I don’t lead with “plant-based” or “vegan”; I lead with flavor. I’ll serve someone a bowl of bean soup, and, after they’ve devoured it, I’ll smile and say, “Congrats, you just had your first vegan meal.” It’s always a surprise for them, and that’s the magic— showing how beautiful, satisfying, and deeply Mexican plant-based food can be.
What are some plant-based ingredients and/or vegan dishes that you’d like to highlight as part of Mexican food traditions? Anything you’d especially like people to know about these foods?
Masa, hands down. It’s the heart of so many beloved Mexican dishes—sopes, huaraches, tlacoyos—and it’s naturally plant-based. What I love most is how versatile it is. You can shape masa into antojitos, but you can also use it to make dumplings and cakes, or get creative and reinterpret global dishes with a Mexican twist. Take a good sope and layer it with mashed potatoes or creamy refried beans, top with salsa, guacamole, shredded lettuce, pickled onions—whatever you love. That’s the beauty of Mexican food; it’s endlessly customizable. You can set up a spread with all kinds of toppings and let everyone build their own plate. It’s not just delicious. It’s inclusive, joyful, and rooted in sharing.
What do you envision as the way forward to encourage people to eat more fruits and vegetables and return to traditional Hispanic eating patterns?
I think the real barrier is the labels and the absolutes. When we frame eating habits as all-or-nothing, people tune out. But if we shift the focus to just one healthy, vibrant meal at a time—one that’s full of colorful fruits and vegetables that add texture, flavor, and joy—then it feels more approachable and exciting. Traditional Hispanic food already celebrates plant-forward ingredients like chiles, tomatoes, squash, beans, and corn. If we bring those foods back to the center of the plate in a way that feels natural, not forced, people will reconnect with them. It’s about showing how beautiful and delicious these meals can be, not preaching about what they “should” eat.
What does National Hispanic Heritage Month mean to you?
To me, National Hispanic Heritage Month is a time to learn, grow, and open our hearts to other cultures. It’s a reminder that the Hispanic community is not monolithic. We come from so many different countries, regions, and traditions, each with its own stories, flavors, and rhythms. This month is about recognizing that richness and also embracing how much we can learn from one another. It’s a time to celebrate our shared values and our differences, and, ultimately, a time to shine a light on how much more we have in common than we often realize.
Please tell us a little bit about your work and career.
I’m a published cookbook author and food blogger passionate about creating healthy, plant-forward meals, some Mexican, that bring people together. My journey started 23 years ago when my son was diagnosed with a dairy allergy. That experience led me to explore plant-based cooking, earn a certification, and eventually launch my blog Piloncillo & Vainilla in 2013, followed by Ale Cooks in English.
I live in Houston with my family, where I continue to cook, create, and celebrate food as the heart of connection.
2 cups hydrated hibiscus flowers 1 cup dried cherries or dried cranberries 3 tablespoons ground chile ancho subs or any other chili powder (or to taste) 1 tablespoon date syrup or date sugar 1 cup water or hibiscus water ¼ cup lime juice (or to taste) Pinch of Tajin (optional)
Instructions
Simmer the Ingredients: Start by adding the hibiscus flowers, dried fruit, chiles, and date syrup or date sugar to a blender, then add 1 cup of boiling water. (You can use a glass or stainless-steel bowl.)
Blend to Perfection: Blend until smooth. If needed, add ¼ cup water to adjust the consistency.
Season and Adjust: Finish with the lime juice, and add a pinch of Tajin if you’d like.
Store and Serve: Pour into a clean jar, seal tightly, and refrigerate. It keeps well for up to a month in the fridge, so you’ll have plenty of time to experiment with it on different dishes!
Pain, Fatigue, and Bloating Aren’t Random: Summary
In Pain, Fatigue, and Bloating Aren’t Random, Dawn, a health advocate and practitioner, shares about her mission to teach women that these common symptoms are not normal but are indicators of the body’s need for help. Dawn shares her personal journey of watching close family members struggle with health issues when traditional medicine couldn’t provide answers. Over time, her search for better health led her to embrace the Functional Diagnostic Nutrition (FDN) philosophy and other healing modalities, eventually becoming a board-certified health and wellness coach and an FDN practitioner herself. Dawn emphasizes the importance of reducing systemic inflammation through lifestyle changes, dietary adjustments, and supplementation to improve overall health and maintain the ability to enjoy life activities without painful symptoms.
Dawn explains how her work significantly changed after incorporating FDN protocols, particularly the use of targeted lab tests like the MRT (Mediator Release Test) and the GI MAP to identify food sensitivities and gut health issues. These tests provide concrete proof of underlying health problems, making it easier for clients to understand the root causes of their symptoms. Dawn shares the example of a client who experienced renewed energy and weight loss after just a few weeks of dietary changes based on lab results. She also discusses the systemic inflammation panel that she offers, which helps identify the underlying drivers of chronic inflammation, such as infections or toxin overload, allowing for more targeted interventions.
The episode concludes with Dawn encouraging listeners to prioritize foundational health practices such as getting adequate sunlight exposure to support circadian rhythm and overall wellness. She shares a heartwarming story of a client who overcame infertility and conceived a child after working with her. Dawn’s approach is rooted in education and empowerment, ensuring that clients understand their bodies and can advocate for themselves.
Pain, Fatigue, and Bloating Aren’t Random: Topics
00:00 Introduction to the Health Detective Podcast
Please note: This blog contains descriptions of sexual assault.
From Heart Failure, a book I wrote about my time at Tufts University School of Medicine: “I am all gloved up, fifth in line. At Tufts, medical students—particularly male students—practice pelvic exams on anesthetized women without their consent and without their knowledge. Women come in for surgery and, once they’re asleep, we all gather around; line forms to the left…We learn more than examination skills. Taking advantage of the woman’s vulnerability—as she lay naked on a table unconscious—we learn that patients are tools to exploit for our education.”
Using female patients to teach pelvic exams without their consent or knowledge remains “a dirty little secret about medical schools.” It is an “age-old” practice that continues to this day in med schools around the world. It’s been referred to as “the ‘vending machine’ model of pelvic exams, in which medical students line up to take their turn…” “Only it’s not a vending machine; it’s a woman’s vagina.”
It’s been called “an outrageous assault upon the dignity and autonomy of the patient…The practice shows a lack of respect for these patients as persons, revealing a moral insensitivity and a misuse of power.” Indeed, “it is yet another example of the way in which physicians abuse their power and have shown themselves unwilling to police themselves in matters of ethics, especially with regard to female patients.” Said a residency-program director at the Johns Hopkins University School of Medicine, “I don’t think any of us even think about it. It’s just so standard as to how you train medical students.”
What happened when this practice came to light in New Zealand? The chair of the New Zealand Medical Association got on television and said: “‘Until recently it wasn’t an issue…I’m very sorry that women feel they’ve been assaulted and violated in this way. That was never our intention.’ He had no idea then, asked the [TV] presenter, that women might object? ‘All I can say is that there have been no objections…’ ‘Could the reason be,’ asked the interviewer logically, “that it’s very hard for an anesthetized woman to know what’s going on?’”
The practice has been defended publicly by many medical schools and hospitals, contending “this touching is entirely appropriate and clearly falls well within the patient’s ‘implied consent’ to carry out the operation.” After all, “patients are aware they are entering a teaching hospital and therefore know that trainees will be actively participating in their care.” However, “researchers have found that many patients do not know when they have interacted with medical students, or even whether they are in a teaching hospital.” How can this be? “Deliberate lies and deception.”
“A survey of medical students found that 100% of them had been introduced to patients as ‘doctor’ by members of the clinical team,” and, as they go through training, there is, as a journal article is titled, an “Erosion in Medical Students’ Attitudes About Telling Patients They Are Students.” “Additionally, as medical students complete their clinical years of training, their sense of responsibility to inform patients that they are students is found to decrease,” especially if there is an opportunity to perform an invasive procedure. That may be why medical students seem to develop a “don’t ask, don’t tell” policy when it comes to seeking consent for pelvic examinations on anesthetized patients. More than a third of 1,600 medical students surveyed across the country strongly disagreed with the statement “Hospitals should obtain explicit permission for student involvement in pelvic exams,” as seen below and at 4:03 of my video Medical Students Practice Pelvic Exams on Anesthetized Women Without Their Consent.
After all, doctors “argue that performing a pelvic examination is no more intimate than placing one’s hands inside an abdomen during general surgery or attempting to intubate a patient” and assert that sticking your fingers in a woman’s vagina is “just as intimate” as an ophthalmologist looking into the back of your eye; any claim to the contrary is just “another attempt to justify the obsession with political correctness.” Said one medical school professor, “Personally, I would prefer to see a new generation of well-trained doctors…rather than a nation of women whose vaginas are protected from battery by medical students.”
The national survey concluded: “Patients admitted to teaching hospitals do not, however, by the mere act of admission relinquish their rights as human beings to have ultimate control over their own body and to be involved in decisions concerning their health care.”
Is it possible that women just don’t care? Studies show that up to 100% of women asked said they would want to know that vaginal exams were being performed by medical students. Since patients care deeply about being asked, why can’t we at least ask their permission? “We can’t ask women,” the medical school faculty replied. “If we do, they might say no.”