AL MAZROWIAH, Bahrain — Patrick Reed shot 5-under 67 in the second round of the Bahrain Championship on the European tour on Friday and was 10 strokes behind clubhouse leader Calum Hill of Scotland.
Reed won the Dubai Desert Classic on Sunday and announced on Wednesday he was leaving LIV Golf.
The American will play on the European tour for the rest of the year, with the aim of finishing high enough in the Race to Dubai standings to earn full status on the PGA Tour in 2027.
Reed made seven birdies. Hill made 11 — and no bogeys — in his 61 to move onto 16-under par for the tournament and held a four-shot lead midway through the second round.
People with genetic mutations that leave them with an LDL cholesterol of 30 mg/dL live exceptionally long lives. Can we duplicate that effect with drugs?
Data extrapolated from large cholesterol-lowering trials using statin drugs suggest that the incidence of cardiovascular events like heart attacks would approach zero if LDL cholesterol could be forced down below 60 mg/dL for first-time prevention and around 30 mg/dL for those trying to prevent another one. But is lower actually better? And is it even safe to have LDL cholesterol levels that low?
We didn’t know until PCSK9 inhibitors were invented. Are PCSK9 Inhibitors for LDL Cholesterol Safe and Effective? I explore that issue in my video of the same name. PCSK9 is a gene that mutated to give people such low LDL cholesterol, and that’s how Big Pharma thought of trying to cripple PCSK9 with drugs. After a heart attack, intensive lowering of an individual’s LDL cholesterol beyond a target of 70 mg/dL does seem to work better than more moderate lowering. There were fewer cardiovascular deaths, heart attacks, or strokes at an LDL less than 30 mg/dL compared with 70 mg/dL or higher, and even compared to less than 70 mg/dL. There is a consistent risk reduction even when starting as low as an average of 63 mg/dL, and pushing LDL down to 21 mg/dL, remarkably, showed “no observed offsetting” of adverse side effects.
Maybe that shouldn’t be so surprising, since that’s about the level at which we start life. And there’s another type of genetic mutation that leaves people with LDL levels of about 30 mg/dL their whole lives, and they are known to have an exceptionally long life expectancy. So, where did we get this idea that cholesterol could fall too low?
The common claim that lowering cholesterol can be dangerous due to depletion of cell cholesterol is unsupported by evidence and does not consider the exquisite balancing mechanisms our body uses. After all, that’s how we evolved. Until recently, most of us used to have LDL levels around 50 mg/dL, so that’s pretty normal for the human species. The absence of evidence that low or lowered cholesterol levels are somehow bad for us contrasts with the overwhelming evidence that cholesterol reduction decreases risk for coronary artery disease, our number one killer.
What about hormone production, though? Since the body needs cholesterol for the synthesis of steroid hormones—like adrenal hormones and sex hormones—there’s a concern that there wouldn’t be enough. You don’t know, though, until you put it to the test. For decades, we’ve known that women on cholesterol-lowering drugs don’t have a problem with estrogen production and that lowering cholesterol doesn’t affect adrenal gland function. As well, it doesn’t impair testicular function in terms of causing testosterone levels to fall below normal. If anything, statin drugs can improve erectile function in men, which is what you’d expect from lowering cholesterol. But you’ll notice these studies only looked at lowering LDL to 70 mg/dL or below. What about really low LDL?
On PCSK9 inhibitors, you can get most people under an LDL of 40 mg/dL and some under 15 mg/dL! And there is no evidence that adrenal, ovarian, or testicular hormone production is impaired, even in patients with LDL levels below 15 mg/dL. The risk of heart attacks falls in a straight line as LDL gets lower and lower, even below 10 mg/dL, for example, without apparent safety concerns, but that’s over the duration of exposure to these drugs. The longest follow-up to date of those whose LDL, by way of using multiple medications, was kept less than 30 mg/dL is six years.
Now, we can take comfort in the fact that those with extreme PCSK9 mutations, leading to a lifelong reduction in levels of LDL to under 20 mg/dL their whole lives, remain healthy and have healthy kids. Cholesterol-affecting mutations are what cause the so-called “longevity syndromes,” but that doesn’t necessarily mean the drugs are safe. The bottom line is we should try to get our LDL cholesterol down as low as we can, but much longer follow-up data are necessary anytime a new class of drugs is introduced. So far, so good, but we’ve only been following the data for about 10 years. For example, we didn’t know statins increased diabetes risk until decades after they were approved and millions had been exposed. Also worth noting: PCSK9 inhibitors cost about $14,000 a year.
Why might healthy lifestyle choices wipe out 90% of our risk for having a heart attack, while drugs may only reduce risk by 20% to 30%?
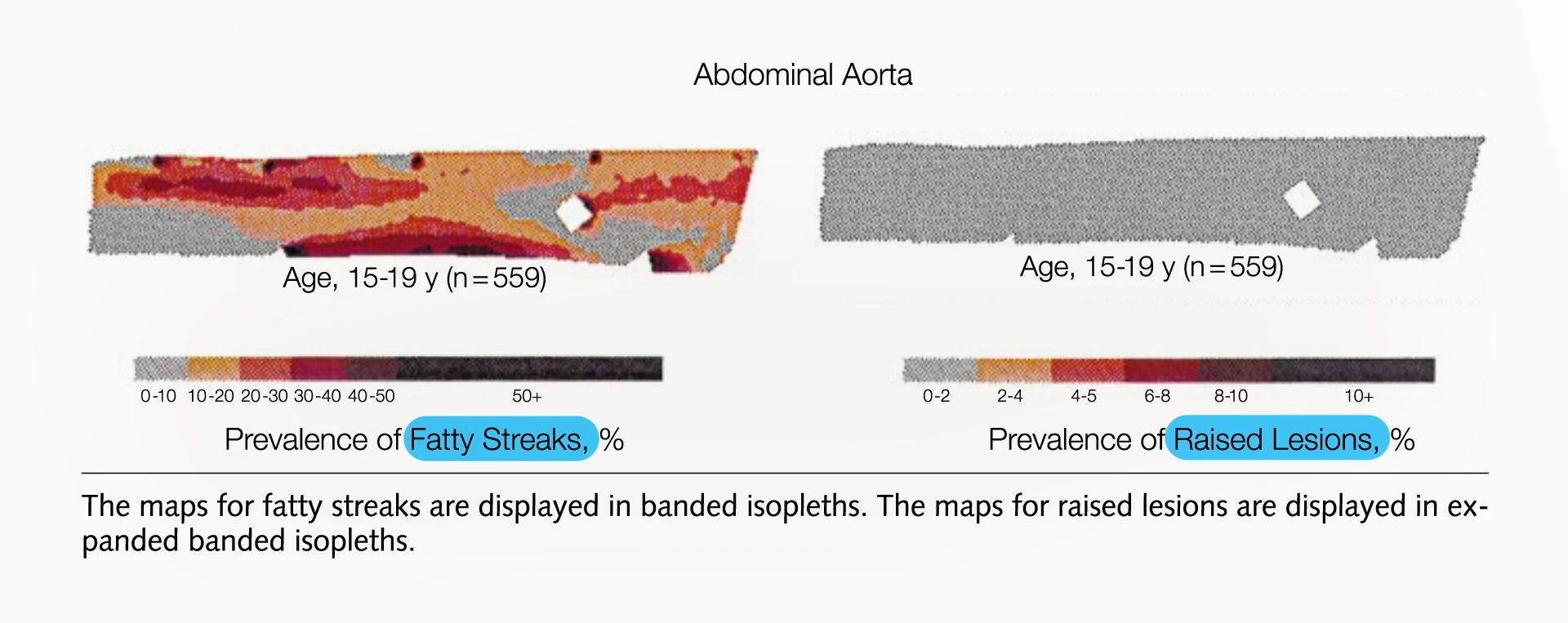
On the standard American diet, atherosclerosis—hardening of the arteries, the number one killer of men and women—has been found to start in our teens. Investigators collected about 3,000 sets of coronary arteries and aortas (the aorta is the main artery in the body) from victims of accidents, homicides, and suicides who were 15 to 34 years old and found that the fatty streaks in arteries can begin forming in our teens, which turn into atherosclerotic plaques in our 20s that get worse in our 30s and can then become deadly. In the heart, atherosclerosis can cause a heart attack. In the brain, it can cause a stroke. See the progression below and at 0:35 in my video Can Cholesterol Get Too Low?.
How common is this? All of the teens they looked at—100% of them—already had fatty streaks building up inside their arteries. By their early 30s, most already had those streaks blossoming into atherosclerotic plaques that bulged into their arteries. From ages 15 through 19, their aortas had fatty streaks building up throughout them, but no plaques yet, on average, as seen below and at 1:15 in my video.
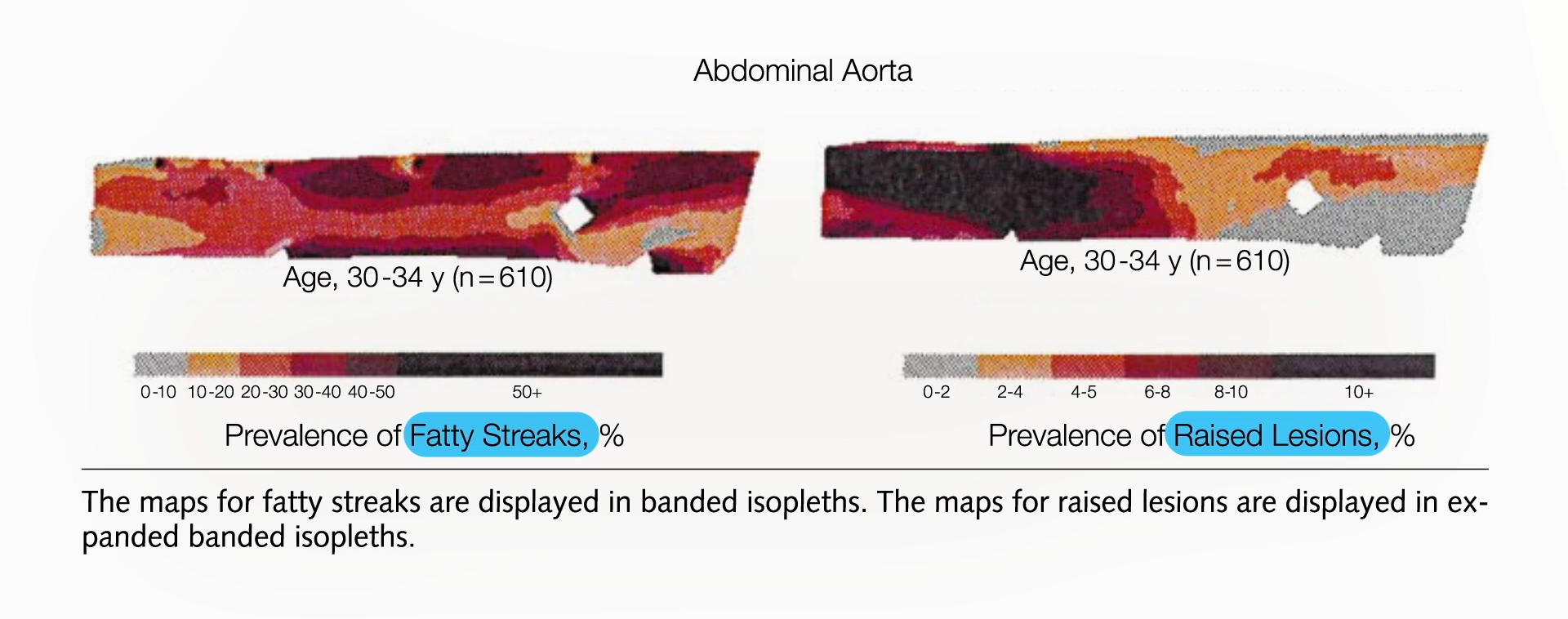
The plaques started appearing in their abdominal aorta in their early 20s and worsened by their late 20s, by which time fatty streaks had infiltrated throughout. By their early 30s, their arteries were in bad shape, as seen below and at 1:25 in my video.
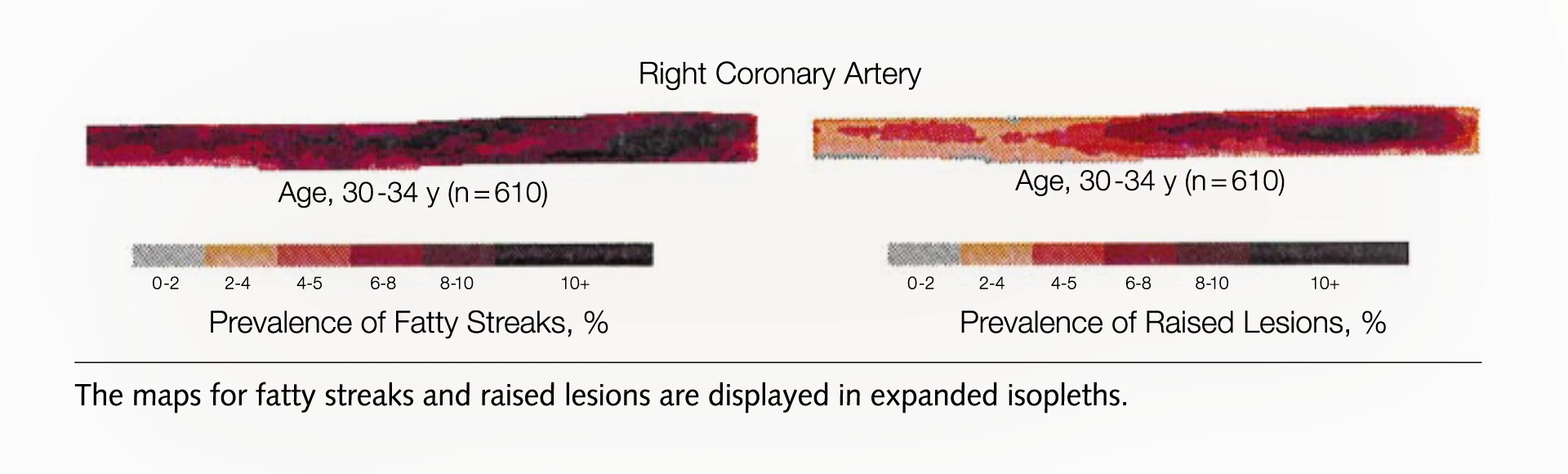
But that’s just the abdominal aorta, the main artery running through the torso that splits off into our legs. What about the coronary arteries that feed the heart?
Researchers found the same pattern: fatty streaks in teens, early signs of plaque in early 20s that progress with age, and by the early 30s, most people already had plaques in their coronary arteries, as seen below and at 1:47 in my video.
That’s why we shouldn’t wait until heart disease becomes symptomatic to treat it. If it starts in our youth, we should start treating it when we’re youths. If you knew you had a cancerous tumor, you wouldn’t want to wait until it grew to a certain size to treat it. If you had diabetes, you wouldn’t want to wait until you started going blind before you did something about it. So, how do you treat atherosclerosis? You lower LDL cholesterol through a diet low in saturated fat and cholesterol—a diet that’s low in eggs, meat, dairy, and junk.
If we want to stop this epidemic, we have to “alter our lifestyle accordingly, beginning in infancy or early childhood. Is such a radical proposal totally impractical?” (Eating more healthfully? Radical?!) It would take serious dedication to change our behavior, but atherosclerosis is our number one cause of death. In the case of cigarettes, we did pretty well, slashing smoking rates and dropping lung cancer rates. And, yes, healthy eating is safe. According to the Academy of Nutrition and Dietetics, the largest and oldest association of nutrition professionals in the world, even strictly plant-based diets are appropriate for all stages of life, starting from pregnancy. (NutritionFacts.org is among the websites recommended by the Academy for more information.)
The title of an important study published in the Journal of the American College of Cardiology declares: “Curing Atherosclerosis Should Be the Next Major Cardiovascular Prevention Goal.” What evidence do we have that a lifelong suppression of LDL will do it? There is a genetic mutation of a gene called PCSK9 that about 1 in 50 African Americans are lucky to be born with because it gives them about a 40% lower LDL cholesterol level their whole lives. Indeed, they were found to have dramatically lower rates of coronary heart disease—an 88% drop in risk compared to those without the genetic mutation, despite otherwise terrible cardiovascular risk factors on average. Most had high blood pressure and were overweight, almost a third smoked, and nearly 20% had diabetes, but that highlights how a lifelong history of low LDL cholesterol levels can substantially reduce the risk of coronary heart disease, even when there are multiple risk factors.
This near-90% drop in events like heart attacks or sudden death occurred at an average LDL level of 100 mg/dL, compared to 138 mg/dL in those without the genetic mutation. This means LDL can drop below even 100 mg/dL. Why does a drop in LDL cholesterol by about 40 mg/dL from a lucky genetic mutation lower the risk of coronary heart disease by nearly 90%, while the same reduction with statin drugs lowers it by only about 20%? The most probable explanation? Duration. When it comes to lowering LDL cholesterol, it’s not only about how low it is, but how long it’s been low.
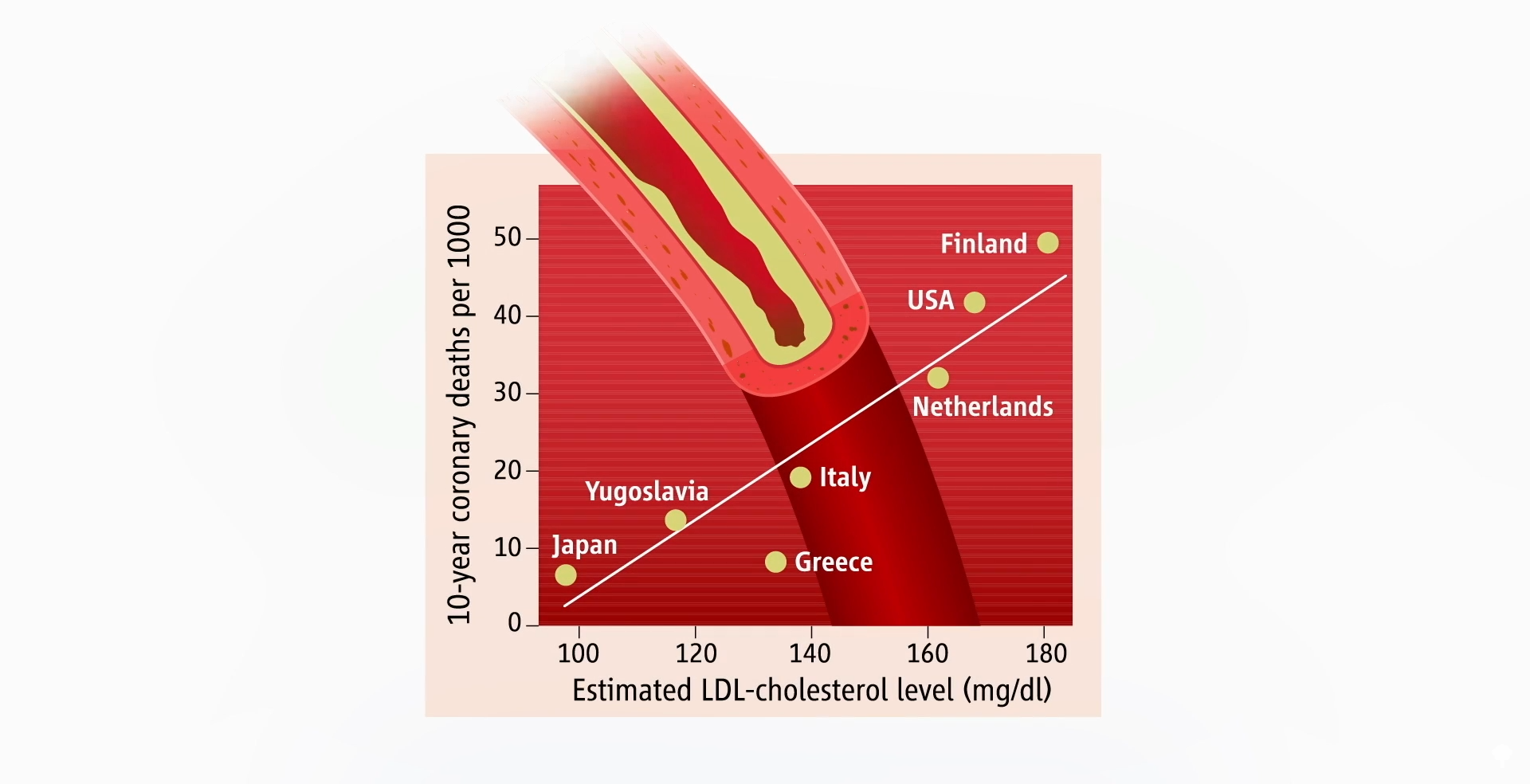
That’s why healthy lifestyle choices may wipe out about 90% of our risk for having a heart attack, while drugs may reduce it by only 20% to 30%. If you’re getting treated with drugs later in life, you may have to get your LDL under 70 mg/dL to halt the progression of coronary atherosclerosis. But if we start making healthier choices earlier, it may be enough to lower LDL cholesterol just to 100 mg/dL, which should be achievable for most of us. That’s consistent with country-by-country data that suggested death from heart disease would bottom out at a population average of about 100 mg/dL, as seen below and at 5:21 in my video.
But that’s only if you can keep your LDL cholesterol down your whole life.
If you’re relying on medication later in life to halt disease progression, you may need to get your LDL below 70 mg/dL, and if you’re trying to use drugs to reverse a lifetime of bad food choices, you may not get to zero coronary heart disease events until your LDL drops to about 55 mg/dL. If your heart disease is so bad that you’ve already had a heart attack but you’re trying not to die from another one, ideally, you might want to push your LDL down to about 30 mg/dL. Once you get that low, not only would you likely prevent any new atherosclerotic plaques, but you’d also help stabilize the plaques you already have so they’re less likely to burst open and kill you.
Is it even safe to have cholesterol levels that low, though? In other words, can LDL cholesterol ever be too low? We’ll find out next.
Shoveling snow? Over-exertion and cold temps can raise your heart risks
ON SATURDAY. TIP OFF FOR THAT GAME IS EIGHT. MIGHT HAVE TO DIG OUT IF YOU’RE HEADED TO THAT GAME. THE SNOW STILL FALLING. BUT FOR A LOT OF US MAYBE ALREADY STARTED OR WILL CONTINUE DOING IS THAT TASK OF SHOVELING. AND WHILE IT MAY BE LIGHT SNOW, THERE ARE STILL IMPORTANT HEALTH REMINDERS TO KEEP IN MIND. DOCTOR JORGE PLUTZKY IS THE DIRECTOR OF PREVENTATIVE CARDIOLOGY AT BRIGHAM AND WOMEN’S HOSPITAL. DOCTOR PLUTZKY, THANKS SO MUCH FOR BEING HERE WITH US THIS MORNING. SURE. THANK YOU. WHAT DO YOU WORRY ABOUT MOST WHEN YOU THINK ABOUT PEOPLE WHO ARE HEADING OUT TO MOVE ALL OF THAT SNOW AROUND? WELL, FOR SOME PEOPLE, IT MAY BE THE FIRST TIME THEY’RE EXERTING THEMSELVES TO THAT LEVEL. AND WE KNOW THAT SHOVELING SNOW IS A VERY HIGH LEVEL OF EXERTION. YOU CAN VERY QUICKLY. STUDIES SUGGEST WITHIN TEN MINUTES REACH 100% OF YOUR MAXIMUM HEART RATE. AND SO FOR PEOPLE WITH A HISTORY OF HEART DISEASE OR JUST RISK FACTORS, THAT CAN BE QUITE AN EXERTION. IT’S LIKE SETTLING, DOING A MAXIMAL STRESS TEST AND BRINGING ON ISSUES RELATED TO THAT. DOC, WHAT ARE SOME OF THE WARNING SIGNS THAT FOLKS OUT THERE MIGHT BE? YOU KNOW, WE TOUGH NEW ENGLANDERS WILL SAY, WELL, WE’LL WORK THROUGH IT. BUT, YOU KNOW, THERE ARE SIGNS THAT SOMETHING MAY BE SERIOUSLY HAPPENING AND YOU NEED TO BE ABLE TO TAKE A BREAK, HEAD ON INSIDE FOR A BIT. YES. YOU KNOW, THE CLASSIC SIGNS OF CHEST PAIN AND PERHAPS ASSOCIATED SHORTNESS OF BREATH, NAUSEA, RADIATION DOWN THE ARMS ARE CERTAINLY VERY VALID. BUT WE ALSO WANT PEOPLE TO PAY ATTENTION TO MORE SUBTLE SIGNS LIKE CHEST PRESSURE, ACHING IN THE JAW, JUST THE THE NAUSEA CAN STILL BE RELEVANT. AND SO LISTENING TO YOUR BODY SLOWING DOWN, TAKING BREAKS AND STOPPING IF YOU’RE FEELING ANY OF THOSE IS GOOD ADVICE AND HIGHLY WARRANTED, ESPECIALLY WHEN YOU’RE OUT THERE IN THE COLD, WHICH MAY BE ITS OWN FACTOR FOR WHY THESE ISSUES ARISE. THE COLD CAN CONSTRICT ARTERIES AND MAKE THINGS WORSE, AND THERE REALLY IS NO MESSING AROUND WITH THIS. AND WE KNOW HEART ISSUES PRESENT DIFFERENTLY. BUT ARE THERE? AND MAYBE YOU JUST SPOKE ABOUT THIS MORE SUBTLE SIGNS THAT PEOPLE SHOULD PAY ATTENTION TO DURING THIS KIND OF WEATHER. YEAH, IT’S THINGS LIKE I’M FEELING MORE SHORT OF BREATH THAN I THAN I WOULD EXPECT TO BE. I’M HAVING AN ACHE IN MY JAW OR IN MY NECK THAT IS SURPRISING AND FEELS DIFFERENT. THESE ARE ALL SIGNS TO PAY ATTENTION TO AND TO NOT PUSH IT, TO SORT THAT OUT. THE. THERE ARE VARIOUS STRATEGIES PEOPLE CAN TAKE TO HAVE LESS OF A LOAD, LIKE TAKING BREAKS, COVERING YOUR MOUTH SO YOU WARM THE AIR THAT’S ON ITS WAY IN TO NOT NECESSARILY SHOVEL AND LIFT, BECAUSE USING YOUR ARMS IS MORE OF AN EXERTION, BUT TO PUSH AND TO TO SWIPE. BUT YOU REALLY DO WANT TO LISTEN TO ANY, ANY SENSE YOU HAVE THAT SOMETHING’S OFF. INCLUDING THESE OTHER, YOU KNOW, SOMEWHAT ATYPICAL SYMPTOMS THAT AREN’T CLASSIC CHEST PAIN. EVEN THAT CHEST PRESSURE CAN BE A SIGN. IT’S BEEN FOUR YEARS SINCE WE HAD THIS AMOUNT OF SNOW, SO MAYBE FOLKS HAVEN’T HAD TO FACE IT FOR A WHILE. DOCTOR GEORGE, THANK YOU VERY MUCH. CARDIOLOGIST WITH MASS GENERAL BRIGHAM, WE THANK YOU FOR JOINING US THIS MORNING.
Digging out from the weekend’s massive snow and ice storm could be hazardous to your heart.Pennsylvania health officials announced three snow-removal-related deaths on Sunday. All were between the ages of 60 and 84. The Lehigh County coroner’s office cautioned people to take breaks and avoid over-exerting themselves.Shoveling snow is heavy, hard work — research has shown that doing it for even a short time can make the heart work as hard as it does during a major workout. Adding to that stress, the cold temperatures cause blood vessels, including those feeding the heart, to constrict. That raises blood pressure, which in turn increases the risk of a heart attack, stroke, or cardiac arrest, according to the American Heart Association.Snow shoveling is especially risky for anyone with known heart disease or who’s already survived a heart attack, as well as older adults and people with risk factors, including high blood pressure or cholesterol. People who think they’re healthy can get in trouble, too, with that combination of heavy exertion in cold weather – especially if they’re generally sedentary until a snowstorm comes along.The heart association advises that if you have to shovel, go slow and try to push the snow instead of lifting and throwing it. It also urges people to learn common warning signs of a heart attack and to call 911 if they experience them.
Digging out from the weekend’s massive snow and ice storm could be hazardous to your heart.
Pennsylvania health officials announced three snow-removal-related deaths on Sunday. All were between the ages of 60 and 84. The Lehigh County coroner’s office cautioned people to take breaks and avoid over-exerting themselves.
Shoveling snow is heavy, hard work — research has shown that doing it for even a short time can make the heart work as hard as it does during a major workout. Adding to that stress, the cold temperatures cause blood vessels, including those feeding the heart, to constrict. That raises blood pressure, which in turn increases the risk of a heart attack, stroke, or cardiac arrest, according to the American Heart Association.
Snow shoveling is especially risky for anyone with known heart disease or who’s already survived a heart attack, as well as older adults and people with risk factors, including high blood pressure or cholesterol. People who think they’re healthy can get in trouble, too, with that combination of heavy exertion in cold weather – especially if they’re generally sedentary until a snowstorm comes along.
The heart association advises that if you have to shovel, go slow and try to push the snow instead of lifting and throwing it. It also urges people to learn common warning signs of a heart attack and to call 911 if they experience them.
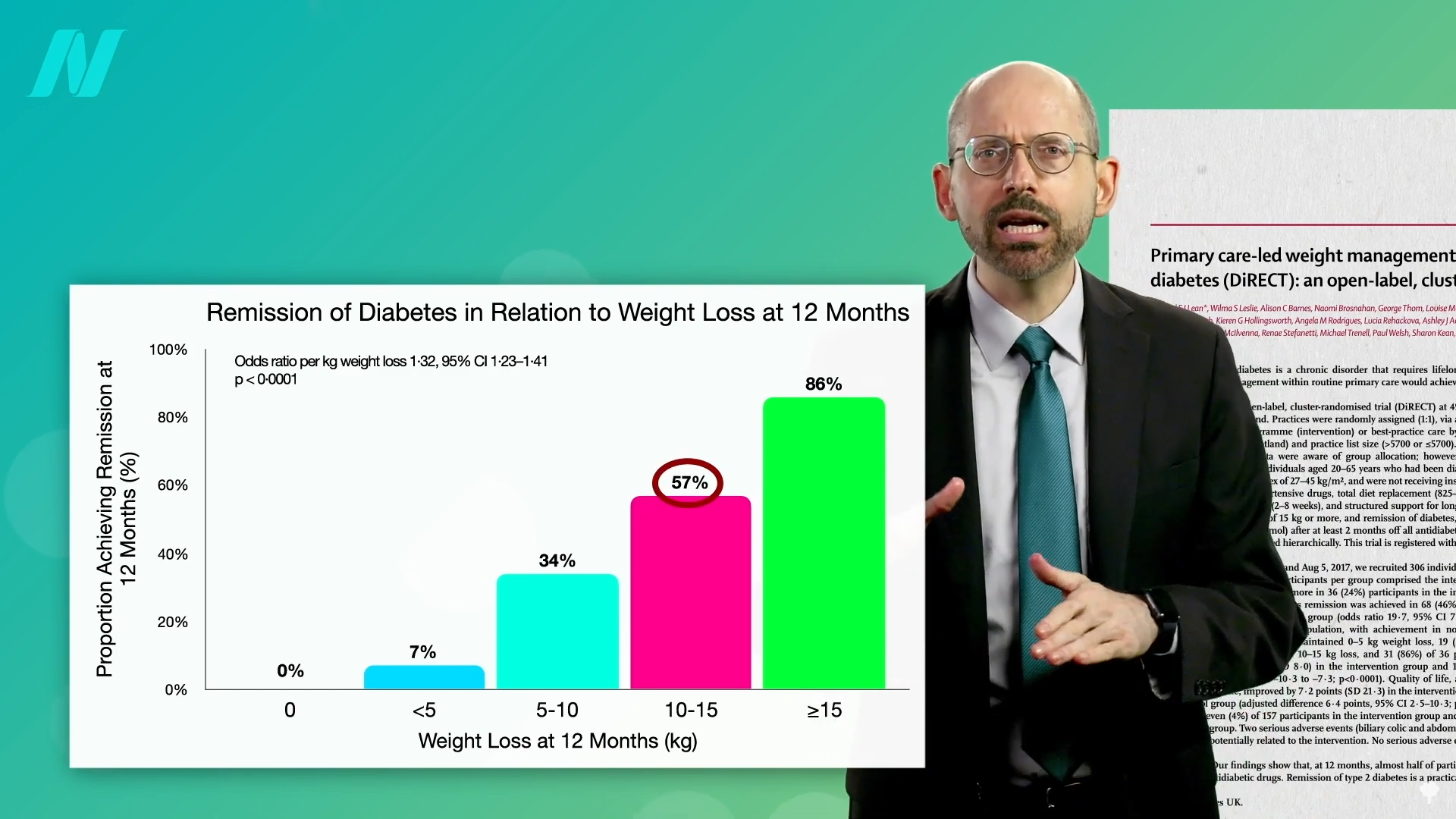
By losing 15% of their body weight, nearly 90% of those who have had type 2 diabetes for less than four years may achieve remission.
Currently, more than half a billion adults have diabetes, and about a 50% increase is expected in another generation. I’ve got tons of videos on the best diets for diabetes, but what about no diet at all?
More than a century ago, fasting was said to cure diabetes, quickly halting its progression and eliminating all signs of the disease within days or weeks. Even so, starvation is guaranteed to lead to the complete disappearance of you if kept up long enough. What’s the point of fasting away the pounds if they’re just going to return as soon as you restart the diet that created them in the first place? Might it be useful to kickstart a healthier diet? Let’s see what the science says.
Type 2 diabetes has long been recognized as a disease of excess, once thought to afflict only “the idle rich…anyone whose environment and self-support does not require of him some sustained vigorous bodily exertion every day, and whose earnings or income permit him, and whose inclination tempts him, to eat regularly more than he needs.” Diabetes is preventable, so might it also be treatable? If we’re dying from overeating, maybe we can be saved by undereating. Remarkably, this idea was proposed about 2,000 years ago in an Ayurvedic text:
“Poor diabetic people’s medicine He should live like a saint (Munni); He should walk for 800–900 miles. Or he shall dig a pond; Or he shall live only on cow dung and cow urine.”
That reminds me of the Rollo diet for diabetes proposed in 1797, which was composed of rancid meat. That was on top of the ipecac-like drugs he used to induce severe sickness and vomiting. Anything that makes people sick has only “a temporary effect in relieving diabetes” because it reduces the amount of food eaten. His diet plan—which included congealed blood for lunch and spoiled meat for dinner—certainly had that effect.
Similar benefits were seen in people with diabetes during the siege of Paris in the Franco‐Prussian War, leading to the advice to mangez le moins possible, which translates to “eat as little as possible.” This was formalized into the Allen starvation treatment, considered to be “the greatest advance in the treatment of diabetes prior to the discovery of insulin.” Before insulin, there was “The Allen Era.”
Dr. Allen noted that there are clinical reports of even severe diabetes cases clearing up after the onset of a “wasting condition” like tuberculosis or cancer, so he decided to put it to the test. He found that even in the most severe type of diabetes, he could clear sugar from people’s urine within ten days. Of course, that’s the easy part; it’s harder to maintain once they start eating again. To manage patients’ diabetes, he stuck to two principles: Keep them underweight and restrict the fat in their diet. A person with severe diabetes can be symptom-free for days or weeks, but eating butter or olive oil can make the disease come raging back.
As I’ve said before, diabetes is a disease of fat toxicity. Infuse fat into people’s veins through an IV, and, by using a high-tech type of MRI scanner, you can show in real time the buildup of fat in muscle cells within hours, accompanied by an increase in insulin resistance. The same thing happens when you put people on a high-fat diet for three days. It can even happen in just one day. Even a single meal can increase insulin resistance within six hours. Acute dietary fat intake rapidly increases insulin resistance. Why do we care? Insulin resistance in our muscles, in the context of too many calories, can lead to a buildup of liver fat, followed by fat accumulation in the pancreas, and eventually full-blown diabetes. “Type 2 diabetes can now be understood as a state of excess fat in the liver and pancreas, and remains reversible for at least 10 years in most individuals.”
When people are put on a very low-calorie diet—700 calories a day—fat can get pulled out of their muscle cells, accompanied by a corresponding boost in insulin sensitivity, as shown below and at 4:43 in my video Fasting to Reverse Diabetes.
The fat buildup in the liver has then been shown to decrease substantially, and if the diet is continued, the excess fat in the pancreas also reduces. If caught early enough, reversing type 2 diabetes is possible, which would mean sustained healthy blood sugar levels on a healthy diet.
With the loss of 15% of body weight, nearly 90% of individuals who have had type 2 diabetes for less than four years can achieve non-diabetic blood sugar levels, whereas it may only be reversible in 50% of those who’ve lived with the disease for longer than eight years. That’s better than bariatric surgery, where those losing even more weight had lower remission rates of 62% and 26%, respectively. Your forks are better than surgeons’ knives. Indeed, most people who have had their type 2 diabetes diagnosis for an average of three years can reverse their disease after losing about 30 pounds, as you can see below and at 5:37 in my video.
Of course, an extended bout of physician-supervised, water-only fasting could also get you there, but you would have to maintain that weight loss. One of the things that has been said with “certainty” is that if you regain the weight, you regain your diabetes.
To bring it full circle, “the initial euphoria about ‘medicine’s greatest miracle’”—the discovery of insulin in 1921—“soon gave way to the realisation” that, while it was literally life-saving for people with type 1 diabetes, insulin alone wasn’t enough to prevent such complications as blindness, kidney failure, stroke, and amputations in people with type 2 diabetes. That’s why one of the most renowned pioneers in diabetes care, Elliott Joslin, “argued that self-discipline on diet and exercise, as it was in the days prior to the availability of the drug [insulin], should be central to the management of diabetes….”
Congratulations, you’ve reached the final day of the Brain Health Challenge! Today, we’re asking you to do a few things that might feel a bit out of left field — like getting your blood pressure checked.
No, it isn’t as fun as playing Pips, but experts say it’s one of the most important things you can do for your brain. That’s because heart health and brain health are intrinsically linked.
High blood pressure, in particular, can damage brain cells, and it’s a significant risk factor for stroke and dementia. When blood pressure is too high, it places stress on the walls of arteries in the brain. Over time, that added stress can cause the blood vessel walls to thicken, obstructing blood flow. In other cases, the increased pressure causes the artery walls to thin and leak blood into the brain.
These changes to the blood vessels can sometimes cause a large stroke to occur. More commonly, the damage leads to micro-strokes and micro-hemorrhages, which cause fewer immediate problems and often go unnoticed. But if someone has hypertension for years or decades, these injuries can build up, and the person may start to experience cognitive impairment.
High blood pressure “is known as a silent killer for lots of reasons,” said Dr. Shyam Prabhakaran, the chair of neurology at the University of Chicago. “It doesn’t cause you any symptoms until it does.”
Because the damage accumulates over many years, experts say that managing blood pressure in midlife matters most for brain health. Hypertension can be addressed with medication or lifestyle changes, as directed by your doctor. But the first thing you need to do is know your numbers. If your blood pressure comes back higher than 120/80, it’s important to take it seriously, Dr. Prabhakaran said.
While you’re at it, there are a few other aspects of your physical health that you should check on.
Your eyes and ears are two of them. Hearing and vision loss have both been shown to increase the risk of dementia. Experts think that with less sensory information coming in to stimulate the brain, the regions that process hearing and vision can start to atrophy. What’s more, people with sensory loss often withdraw or are left out of social interactions, further depriving them of cognitive stimulation.
Oral health can also affect your brain health. Research has found a connection between regular flossing and reduced odds of having a stroke. That may be because good oral health can help to reduce inflammation in the body. The bacteria that cause gum disease have also been tied to an increased risk of Alzheimer’s.
And have you gotten your shingles vaccine? There is mounting evidence that it’s a powerful weapon for protecting against dementia. One study found that it lowered people’s odds of developing the condition by as much as 20 percent.
To wrap up this challenge, we want you to schedule a few medical appointments that benefit your brain, as well as your body.
After five days of feeding, exercising and challenging your brain, you are well on your way to better cognitive health. Thanks for joining me this week, and keep up the good habits!
Today, you’re going to do perhaps the single best thing for your brain.
When I asked neurologists about their top behaviors for brain health, they all stressed the importance of physical activity.
“Exercise is top, No. 1, when we’re thinking about the biggest bang for your buck,” said Dr. Gregg Day, a neurologist at the Mayo Clinic.
Numerous studies have shown that people who exercise regularly tend to perform better on attention, memory and executive functioning tests. There can be a small cognitive boost immediately after a workout, and the effects are sustained if people exercise consistently. And while staying active can’t guarantee you won’t develop dementia, over the long term, it is associated with a lower risk of it.
Researchers think that moving your muscles benefits your brain in part because of special signaling molecules called exerkines. During and after a workout, your muscles, fat and other organs release these molecules into the bloodstream, some of which make their way up to the brain. There, those exerkines go to work, helping to facilitate the growth of new connections between neurons, the repair of brain cells and, possibly, the birth of new neurons.
Exercise also appears to improve blood flow in the brain. That ramps up the delivery of good things to brain cells, like oxygen, glucose and those amazing exerkines. And it helps remove more bad things, namely toxic proteins, like amyloid, that can build up and damage brain cells, increasing the risk for Alzheimer’s.
All of the changes brought on by exercise are “essentially allowing your brain to age more slowly than if you’re physically inactive,” said Kirk Erickson, the chair of neuroscience at the AdventHealth Research Institute.
The benefits are particularly pronounced in the hippocampus, a region critical for learning and memory. In older adults, the hippocampus shrinks 1 to 2 percent a year, and it is one of the main areas affected by Alzheimer’s. Researchers think physical activity helps to offset some of that loss.
The best exercise you can do for your brain is the one you’ll do consistently, so find something that you enjoy and that fits easily into your life.
Walking is one option; two neurologists I spoke to said they got their exercise in by walking at least part of the way to their offices. Recent research suggests that just a few thousand steps a day can reduce the risk of dementia. It’s important to get your heart rate up, though, so “walk as though you’re trying to get somewhere on time,” said Dr. Linda Selwa, a clinical professor of neurology at the University of Michigan Medical School.
Or you could try swimming, cycling, Pilates, weight lifting, yoga, pickleball, dancing, gardening — any type of physical exertion can be beneficial.
If the thought of working out feels like a drag, try pairing it with something else you enjoy doing, like listening to an audiobook. This is a trick that Katherine Milkman, a professor who studies habits at The Wharton School of the University of Pennsylvania, calls “temptation bundling.”
For Day 3, we’re asking you to spend at least 20 minutes exercising for your brain. Go for a walk with your accountability partner if they’re nearby. (If not, call them and do a walk-and-talk.) Or let us find you a new workout to try, using the tool below. As usual, we can all meet in the comments to catch up and check in.
Welcome to the Brain Health Challenge! I’m Dana Smith, a reporter at The New York Times, and I’ll be your guide.
To live a healthy life, it’s crucial to have a healthy brain. In the short term, it keeps you sharp and firing on all cylinders. In the long term, it can reduce your risk of cognitive decline, dementia and stroke.
Practicing basic healthy behaviors, like eating nutritious food and getting regular exercise, is the best way to enhance your brain power and protect the longevity of your neurons. These types of lifestyle habits can benefit the brain at any age. And while they won’t guarantee that you’ll never develop dementia or another brain disease, severalclinicaltrials have shown that they can improve cognition or slow decline.
Every day this week, you’ll do an activity that’s good for your brain, and we’ll dig into the science behind why it works. Some of these activities can provide a small immediate cognitive benefit, but the bigger reward comes from engaging in them consistently over time. So along with the neuroscience lessons, we’ll include a few tips to help you turn these actions into lasting habits.
To keep you accountable, we’re encouraging you to complete this challenge with a friend. If you don’t have a challenge buddy, no problem: We’re also turning the comments section into one big support group.
There are so many fascinating ways your daily behaviors affect your brain. Take sleep, for example.
Lots ofstudies have shown that getting a good night’s rest (seven to eight hours) is associated with better memory and other cognitive abilities. That’s because sleep, especially REM sleep, is when your brain transfers short-term memories — things you learned or experienced during the day — into long-term storage.
Sleep is also when your brain does its daily housekeeping. While you rest, the brain’s glymphatic system kicks into high gear, clearing out abnormal proteins and other molecular garbage, including the protein amyloid, which is a major contributor to Alzheimer’s disease. A buildup of amyloid is one reason experts think that people who routinely get less sleep have a higher risk of dementia.
What other behaviors play a big role in brain health? For today’s activity, we’re going to test your knowledge with a quiz. Share your score with your accountability partner and in the comments below — I’ll be in there too, cheering you on.
If the microbiome of those eating plant-based diets protects against the toxic effects of TMAO, what about swapping gut flora?
“Almost 2,500 years ago, Hippocrates stated that ‘All disease begins in the gut.’” When we feed our gut bacteria right with whole plant foods, they feed us right back with beneficial compounds like butyrate, which our gut bugs make from fiber. On the other hand, if we feed them wrong, they can produce detrimental compounds like TMAO, which they make from cheese, eggs, seafood, and other meat.
We used to think that TMAO only contributed to cardiovascular diseases, like heart disease and stroke, but, more recently, it has been linked to psoriatic arthritis, associated with polycystic ovary syndrome, and everything in between. I’m most concerned about our leading killers, though. Of the top ten causes of death in the United States, we’ve known about its association with increased risk of heart disease and stroke, killers number one and five, but recently, an association has also been found between blood levels of TMAO and the risks of various cancers, which are our killer number two. The link between TMAO and cancer could be attributed to the inflammation caused by TMAO, but it could also be oxidative stress (free radicals), DNA damage, or a disruption in protein folding.
What about our fourth leading killer, chronic obstructive pulmonary disease (COPD), like emphysema? TMAO is associated with premature death in patients with exacerbated COPD, though it’s suspected that it’s due to them dying from more cardiovascular disease.
The link to stroke is a no-brainer—no pun intended. It is due to the higher blood pressure associated with higher TMAO levels, as well as the greater likelihood of clots forming in those with atrial fibrillation. Those with higher TMAO levels also appear to have worse strokes and four times the odds of death.
Killer number six is Alzheimer’s disease. Can TMAO even get up into our brains? Yes, TMAO is present in human cerebrospinal fluid, which bathes the brain, and TMAO levels are higher in those with mild cognitive dysfunction and those with Alzheimer’s disease dementia. “In the brain, TMAO has been shown to induce neuronal senescence [meaning, deterioration with age], increase oxidative stress, impair mitochondrial function, and inhibit mTOR signaling, all of which contribute to brain aging and cognitive impairment.”
Killer number seven is diabetes, and people with higher TMAO levels are about 50% more likely to have diabetes. Killer number eight is pneumonia, and TMAO predicts fatal outcomes in pneumonia patients even without evident heart disease. Kidney disease is killer number nine, and TMAO is strongly related to kidney function and predicts fatal outcomes there as well. Over a period of five years, more than half of chronic kidney disease patients who started out with average or higher TMAO levels were dead, whereas among those in the lowest third of levels, nearly 90% remained alive.
How can we lower the TMAO levels in our blood? Because TMAO originates from dietary sources, we could limit our intake of choline- and carnitine-rich foods. They’re so widespread in foods,” though we’re talking about meat, eggs, and dairy. “Therefore, restriction of foods rich in TMA-containing nutrients may not be practical.” Can we just get a vegan fecal transplant? “Vegan donors provided the investigators with a fresh morning fecal sample…”
If you remember, if you give a vegan a steak, despite all that carnitine, they make almost no TMAO compared to a meat-eater, presumably because the vegan hasn’t been fostering steak-eating bugs in their gut. See below and at 3:40 in my video Can Vegan Fecal Transplants Lower TMAO Levels?.
Remarkably, even if you give plant-based eaters the equivalent of a 20-ounce steak every day for two months, only about half start ramping up production of TMAO, showing just how far their gut flora has to change. The capacity of veggie feces to churn out TMAO is almost nonexistent. Instead of eating healthier, what about getting some vegan poop?
In a double-blind, randomized, controlled trial, research subjects either got vegan poop or their own poop back through a hose snaked down their nose, and it didn’t work.
First of all, the vegans recruited for the study started out making TMAO themselves, in contrast to the other study, where they didn’t make any at all. This may be because the earlier study required the vegans to have been vegan for at least a year, and this study didn’t. So, there wasn’t much of a change in TMAO running through their bodies two weeks after getting the vegan poop, but the vegan poop they got seemed to start out with some capacity to produce TMAO in the first place.
So, the failure to improve after the vegan fecal transplant “could be related to limited baseline microbiome differences and continuation of an omnivorous diet” after the vegan-donor transplant. What’s the point of trying to reset your microbiome if you’re just going to eat meat? Well, the researchers didn’t want to switch people to a plant-based diet since they knew that alone can change our microbiome, and they didn’t want to introduce any extra factors. The bottom line is that it seems there may not be any shortcuts. We may just have to eat a healthier diet.
Donald Glover is opening up about a recent health scare that forced him to cancel his tour last year. At the time, he described it as an “ailment,” but Glover said Saturday night at a performance that a doctor told him he’d had a stroke.
Glover, who performs under the moniker Childish Gambino, shared the information on stage at Tyler, the Creator’s Camp Flog Gnaw festival in Los Angeles. His remarks were shared widely on social media.
“You guys voted for a ‘where have I been monologue,’” Glover, 42, said. “I had a really bad pain in my head in Louisiana and I did the show anyway. I couldn’t really see well, so when we went to Houston, I went to the hospital and the doctor was like, ‘You had a stroke.’”
Glover said he felt like he was letting everyone down, lamenting that he still hasn’t been to Ireland. He also revealed that “they found a hole” in his heart and he had to have two surgeries.
“They say everybody has two lives and the second life starts when you realize you have one,” Glover said. “You got one life, guys, and I gotta be honest, the life I’ve lived with you guys has been such a blessing.”
His representatives did not immediately respond to request for comment.
Donald Glover is opening up about a recent health scare that forced him to cancel his tour last year. At the time, he described it as an “ailment,” but Glover said Saturday night at a performance that a doctor told him he’d had a stroke.
Glover, who performs under the moniker Childish Gambino, shared the information on stage at Tyler, the Creator’s Camp Flog Gnaw festival in Los Angeles. His remarks were shared widely on social media.
“You guys voted for a ‘where have I been monologue,’” Glover, 42, said. “I had a really bad pain in my head in Louisiana and I did the show anyway. I couldn’t really see well, so when we went to Houston, I went to the hospital and the doctor was like, ‘You had a stroke.’”
Glover said he felt like he was letting everyone down, lamenting that he still hasn’t been to Ireland. He also revealed that “they found a hole” in his heart and he had to have two surgeries.
“They say everybody has two lives and the second life starts when you realize you have one,” Glover said. “You got one life, guys, and I gotta be honest, the life I’ve lived with you guys has been such a blessing.”
CBS News has reached out to Glover’s representatives for additional comment.
Donald “Frue” McAvoy and his fiancée, Rachel Leaptrott, were taking it easy on a Sunday in early December 2023, making a cheese board and turning on a football game.
After one bite, McAvoy began to choke. He couldn’t swallow or breathe.
Leaptrott leapt into action. She cleared his throat, but realized that McAvoy’s pupils were locked in place. He was talking, but couldn’t see anything. Leaptrott’s daughter called 911.
“It’s like trying to remember a dream. That’s the best way I can describe it,” McAvoy said. “I remember bits and pieces. I get chills, because I couldn’t see and that was extremely scary. But the scariest thing I ever felt, I didn’t know if I’d ever see again.”
McAvoy, 36, had recently been plagued by headaches, a sore neck and exhaustion. The active gym owner thought he had a strained neck and might be getting the flu.
Paramedics said McAvoy was having a neurological issue. Doctors at the Mayo Clinic in Jacksonville, Florida, made a terrifying diagnosis: He was having a severe stroke.
Frue McAvoy, Rachel Leaptrott and her daughter before his stroke.
Frue McAvoy
A “life-changing” stroke
Time is of the essence when treating a stroke. McAvoy was given a clot-busting medication and rushed into surgery.
Dr. Rabih Tawk, a Mayo Clinic neurosurgeon, performed a thrombectomy to remove the clot and found McAvoy had a vertebral artery dissection that caused the stroke and stopped blood flow to his brain and spine. His airway had collapsed, causing the choking. Strokes in someone as young as McAvoy are unusual, but not impossible, Tawk said.
McAvoy came through surgery, but doctors wouldn’t know the extent of the stroke’s effects until he woke up. Tawk said an assessment indicated it would be “life-changing.”
“They did scans of his brain, and they described the MRI as ‘fireworks,’” Leaptrott said. “When you do a scan like that, it shows up as a big white spot and a big hit in one area, whereas for Frue, it was like spurts and different areas were hit. It looked like a fire burst through the scan. I only saw that scan once, and it was enough.”
Frue McAvoy in the hospital.
Frue McAvoy
For seven days, McAvoy was on a ventilator. It was replaced with breathing and feeding tubes that let him begin therapy. Assessments found that all of his motor skills had been impacted. He would need to relearn how to stand, walk, write and speak. He couldn’t see clearly.
Through it all, Leaptrott had just one wish: A hug on Christmas Day.
“I’ve got to do this”
Leaptrott’s request gave McAvoy a goal to focus on. He kept it in mind amid therapy, “prodding and pulling” and complications, including two pulmonary embolisms. At first, it took the support of two people just to help him balance in bed, but he pushed himself to relearn how to stand, walk and raise his arms.
“I just remember whatever they asked of me, I knew I had to do it to move on to the next thing,” McAvoy said. “I was hooked up to every wire you can think of, but you just trust that all those wires and everything they’re doing is going to lead you to better health.”
On Christmas Eve, more than three weeks after the stroke, Leaptrott got her wish.
Frue McAvoy and Rachel Leaptrott holding hands in the early days after his stroke.
Frue McAvoy
“I just said, ‘OK, I’ve got to do this. If this is the last thing I ever do, I’m going to give it to her,’” McAvoy remembered.
After 24 days at the Mayo Clinic, McAvoy was transferred to Brooks Rehabilitation Hospital. When he arrived, he couldn’t stand for more than 10 seconds.
He was enrolled in “Brooks Boot Camp,” which meant working with therapists, nurses and doctors for at least three hours a day in an individualized program, said physical therapist Stephanie Cabret. He started with goals like increasing his stamina and dressing himself, and eventually progressed to more difficult tasks like preparing food, said occupational therapist Shantal Wright. He also underwent vocal therapy and saw an eye specialist.
McAvoy said he focused on staying positive. He asked for extra therapy time whenever possible. He also shared his story online: An Instagram account previously dedicated to fitness became a progress log. Hundreds followed his journey, and McAvoy was able to connect with stroke survivors from around the country.
“It’s a family I never knew I had or expected to have at this age,” McAvoy said. “It’s just amazing to see how far we’ve all come and are still going.”
Frue McAvoy completes a walk at Brooks Rehabilitation.
Frue McAvoy
“Incredibly, incredibly grateful”
McAvoy was discharged from Brooks Rehabilitation in late January. He could walk down a 200-foot hallway alone. He then had three months of outpatient care.
Nearly two years later, McAvoy still struggles with the stroke’s impact. He uses a walker with a seat so he can rest if he gets tired, and he wears glasses now. He struggles with depth perception and can’t drive. But he is back to the activities he loved, including athletics: Four months after the stroke, he took part in a one-mile challenge run. Hours before speaking with CBS News, he and Leaptrott walked the Swinging Mile at Grandfather Mountain, the highest suspension footbridge in the country.
Rachel Leaptrott, Frue McAvoy and Leaptrott’s daughter.
Frue McAvoy
McAvoy regularly visits Brooks Rehabilitation’s Neuro Recovery Center, where therapists developed a program he can do on his own. The program adjusts as he does, so he constantly has new milestones to strive for. He is also still in touch with his care team and maintains his social media presence.
“With everything going on, I never thought I would hear myself speak again. When you’re in that quiet for so long, you really start thinking about life and what matters and what doesn’t,” McAvoy said. “If I get upset about something or frustrated or angry, I remind myself there was a point in time I couldn’t even express that. I’m just incredibly, incredibly grateful for how my journey has gone.”
HARRISBURG, Pa. (AP) — U.S. Sen. John Fetterman had what his office says was a “ventricular fibrillation flare-up” that caused him to feel light-headed and fall during an early morning walk Thursday.
Fetterman was doing well and hospitalized in Pittsburgh, his office said. He sustained minor injuries to his face and was under “routine observation” at the hospital while doctors fine-tune his medication regimen, his office said.
Cardiomyopathy can impede blood flow and potentially cause heartbeats so irregular they can be fatal. Atrial fibrillation can cause blood to pool inside a pocket of the heart, allowing clots to form. Clots then can break off, get stuck and cut off blood, causing a stroke.
Fetterman has said the stroke was atrial fibrillation. Fetterman, 55, underwent surgery after the stroke to implant a pacemaker with a defibrillator to manage the condition.
The lingering effects of his stroke include diminished auditory processing speed, called auditory processing disorder, which makes it harder to speak fluidly and quickly process spoken conversation into meaning.
Weeks after joining the Senate in 2023, Fetterman checked himself into the hospital for clinical depression. He was released six weeks later and has since urged people who are depressed to get professional help.
Post-stroke depression is common and treatable through medication and talk therapy, doctors say.
Copyright 2025 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.
Treat the underlying cause of chronic lifestyle diseases.
It’s been said that more than 2,000 years ago, Hippocrates declared, “Let food be thy medicine and medicine be thy food.” In actuality, it appears that he never actually said those words, but there’s “no doubt about the relevance of food…and its role in health and disease states” in his writings. Regardless, 2,000 years ago, disease was thought to arise from a bad sense of “humors,” as you can see here and at 0:32 in my video Lifestyle and Disease Prevention: Your DNA Is Not Your Destiny.
Now, we have science, and there is “an overwhelming body of clinical and epidemiological evidence illustrating the dramatic impact of a healthy lifestyle on reducing all-cause mortality”—meaning death from all causes put together—“and preventing chronic diseases such as coronary heart disease, stroke, diabetes, and cancer.” But don’t those diseases just run in our family? What if we just have bad genes?
According to the esteemed former chair of nutrition at Harvard, for most of the diseases that have contributed “importantly” to mortality in Western peoples, we’ve long known that non-genetic factors often account for at least 80% to 90% of risk. We know this because rates of the leading killers, like major cancers and cardiovascular diseases, vary up to 100-fold around the world, and, “when groups migrate from low- to high-risk countries, their disease rates almost always change to those of the new environment.” Modifiable behavioral factors have been identified, “including specific aspects of diet, overweight, inactivity, and smoking that account for over 70% of stroke and colon cancer, over 80% of coronary heart disease, and over 90% of adult-onset [type 2] diabetes”—diseases that can largely be prevented by our own actions.
If most of the power is in our own hands, why do we allocate massively more resources to treatment than prevention? And speaking of prevention, “even preventive strategies are heavily biased towards pharmacology rather than supporting improvements in diet and lifestyle that could be more cost-effective. For example, treatment of [high] serum cholesterol with statins alone could cost approximately 30 billion dollars per year in the United States and would have only a modest impact on coronary heart disease incidence. The inherent problem is that most pharmacologic strategies don’t address the underlying causes of ill health in Western countries, which are not drug deficiencies.”
Ironically, the chronic diseases that are most amenable to lifestyle treatment are the same ones most profitably treated by drugs. Why? If you don’t change your diet, you have to pop the pills every day for the rest of your life. So, the cash-cow drugs are the very drugs we need the least. “Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy, physicians often do not follow these recommendations.” “By ignoring the root causes of disease and neglecting to prioritize lifestyle measures for prevention, the medical community is placing people at harm.”
“Traditional medical care relies primarily on the application of pharmacologic and surgical interventions after the development of illness,” whereas lifestyle medicine relies primarily on “the use of optimal nutrition (a whole foods, plant-based diet) and exercise in the prevention, arrest, and reversal of chronic conditions leading to premature disability and death. It looks in a holistic way at the underlying causes of illness.”
Dr. Adriane Fugh-Berman, director of PharmedOut, a wonderful organization I’m proud to support, wrote a great editorial entitled “Doctors Must Not Be Lapdogs to Drug Firms.” “The illusion that the relationship between medicine and the drug industry is collegial, professional, and personal is carefully maintained by the drug industry, which actually views all transactions with physicians in finely calculated financial terms…The drug industry is happy to play the generous and genial uncle until physicians want to discuss subjects that are off limits, such as the benefits of diet or exercise, or the relationship between medicine and pharmaceutical companies…Let us not be a lapdog to Big Pharma. Rather than sitting contentedly in our master’s lap, let us turn around and bite something tender.”
Doctor’s Note
The organization I mentioned, PharmedOut, is a project of Georgetown University Medical Center.
For more on Lifestyle Medicine, see related videos below.
Having a “normal” cholesterol level in a society where it’s normal to die from a heart attack isn’t necessarily a good thing.
“Consistent evidence” from a variety of sources “unequivocally establishes” that so-called bad LDL cholesterol causes atherosclerotic cardiovascular disease—strokes and heart attacks, our leading cause of death. This evidence base includes hundreds of studies involving millions of people. “Cholesterol is the cause of atherosclerosis,” the hardening of the arteries, and “the message is loud and clear.” “It’s the Cholesterol, Stupid!” noted the editor of the American Journal of Cardiology, William Clifford Roberts, whose CV is more than 100 pages long as he has published about 1,700 articles in peer-reviewed medical literature. Yes, there are at least ten traditional risk factors for atherosclerosis, as seen below and at 1:11 in my videoHow Low Should You Go for Ideal LDL Cholesterol?, but, as Dr. Roberts noted, only one is required for the progression of the disease: elevated cholesterol.
Your doctor may have just told you that your cholesterol is normal, so you’re relieved. Thank goodness! But, having a “normal” cholesterol level in a society where it’s normal to have a fatal heart attack isn’t necessarily good. With heart disease, the number one killer of men and women, we definitely don’t want to have normal cholesterol levels; we want to have optimal levels—and not optimal by current laboratory standards, but optimal for human health.
Normal LDL cholesterol levels are associated with the hidden buildup of atherosclerotic plaques in our arteries, even in those who have so-called “optimal risk factors by current standards”: blood pressure under 120/80, normal blood sugars, and total cholesterol under 200 mg/dL. If you went to your doctor with those kinds of numbers, you’d likely get a gold star and a lollipop. But, if your doctor used ultrasound and CT scans to actually peek inside your body, atherosclerotic plaques would be detected in about 38% of individuals with those kinds of “optimal” numbers.
Maybe we should define an LDL cholesterol level as optimal only when it no longer causes disease. What a concept! When more than a thousand men and women in their 40s were scanned, having an LDL level under 130 mg/dL left them with atherosclerosis throughout their body, and that’s a cholesterol level at which most lab tests would consider normal.
In fact, atherosclerotic plaques were not found with LDL levels down around 50 or 60, which just so happens to be the levels most people had “before the introduction of western lifestyles.” Indeed, before we started eating a typical American diet, “the majority of the adult population of the world had LDLs of around 50 mg per deciliter (mg/dL)”—so that’s the true normal. “Present average values…should not be regarded as ‘normal.’” We don’t want to have a normal cholesterol based on a sick society; we want a cholesterol that is normal for the human species, which may be down around 30 to 70 mg/dL or 0.8 to 1.8 mmol/L.
“Although an LDL level of 50 to 70 mg/dl seems excessively low by modern American standards, it is precisely the normal range for individuals living the lifestyle and eating the diet for which we are genetically adapted.” Over millions of years, “through the evolution of the ancestors of man,” we’ve consumed a diet centered around whole plant foods. No wonder we have a killer epidemic of atherosclerosis, given the LDL level “we were ‘genetically designed for’ is less than half of what is presently considered ‘normal.’”
In medicine, “there is an inappropriate tendency to accept small changes in reversible risk factors,” but “the goal is not to decrease risk but to prevent atherosclerotic plaques!” So, how low should you go? “In light of the latest evidence from trials exploring the benefits and risks of profound LDLc lowering, the answer to the question ‘How low do you go?’ is, arguably, a straightforward ‘As low as you can!’” “‘Lower’ may indeed be better,” but if you’re going to do it with drugs, then you have to balance that with the risk of the drug’s side effects.
Why don’t we just drug everyone with statins, by putting them in the water supply, for instance? Although it would be great if everyone’s cholesterol were lower, there are the countervailing risks of the drugs. So, doctors aim to use statin drugs at the highest dose possible, achieving the largest LDL cholesterol reduction possible without increasing risk of the muscle damage the drugs may cause. But when you’re using lifestyle changes to bring down your cholesterol, all you get are the benefits.
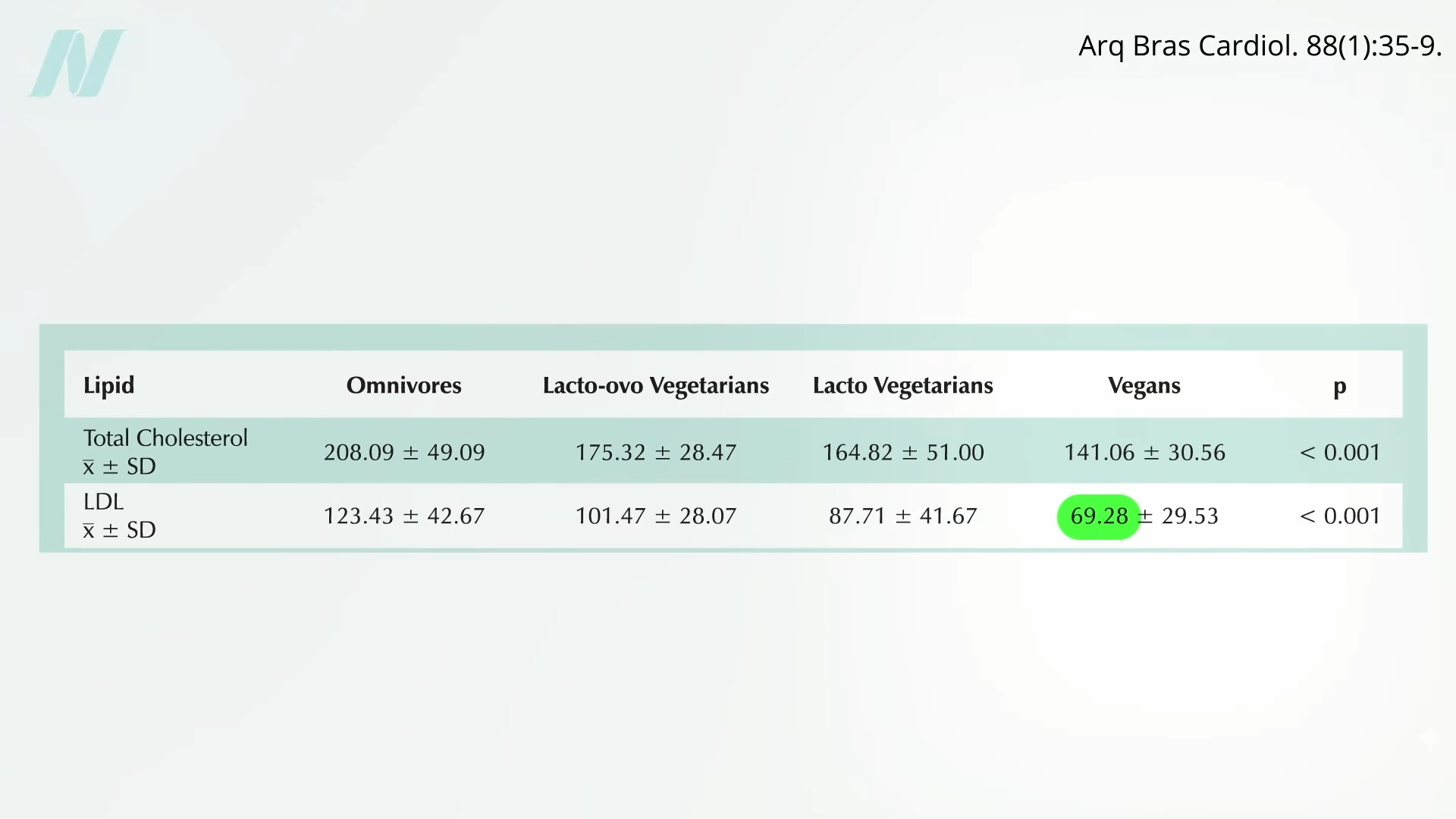
Can we get our LDL low enough with diet alone? Ask some of the country’s top cholesterol experts what they shoot for, “and the odds are good that many will say 70 or so.” So, yes, we should try to avoid the saturated fats and trans fats found in junk foods and meat, and the dietary cholesterol found mostly in eggs, but “it is unlikely anyone can achieve an LDL cholesterol level of 70 mg/dL with a low-fat, low-cholesterol diet alone.” Really? Many doctors have this mistaken impression. An LDL of 70 isn’t only possible on a healthy enough diet, but it may be normal. Those eating strictly plant-based diets can average an LDL that low, as you can see here and at 5:28 in my video.
No wonder plant-based diets are the only dietary patterns ever proven to reverse coronary heart disease in a majority of patients. And their side effects? You get to feel better, too! Several randomized clinical trials have demonstrated that more plant-based dietary patterns significantly improve psychological well-being and quality of life, with improvements in depression, anxiety, emotional well-being, physical well-being, and general health.
For more on cholesterol, see the related posts below.
Keeping your mouth healthy may help keep your heart and brain healthy too, according to new research.
In a study published Wednesday in Neurology Open Access, researchers found adults with gum disease may be more likely to have signs of damage to the brain’s white matter than people without gum disease.
“Gum disease is associated with a higher chance of inflammation, and inflammation has been tied to atherosclerosis as well as hardening of the small blood vessels, as we saw in this study,” study author Dr. Souvik Sen told CBS News. Arteriosclerosis is a disease that causes abnormal thickening of the artery walls.
In another study led by Sen and published in the same journal Wednesday, researchers found having both gum disease and cavities is linked to an 86% increased risk of stroke compared to people with healthy mouths.
“What the study suggested was that if you have cavities on top of gum disease, it is double trouble. It means your risk of stroke or adverse heart event doubles,” Sen said.
But, if someone takes care of their mouth — including brushing, flossing and regular dentist visits for preventative cleaning — risk decreases.
“Their risk of having a stroke dropped by as much as 81%, which is a very big finding,” Sen said of the research.
The research just shows an association, so it does not prove that poor oral health causes strokes — but these findings add to growing evidence that oral health may have a significant impact on cardiovascular health.
With 3.5 billion people worldwide suffering from gum disease or cavities, according to the World Health Organization, researchers say prevention and treatment could be an important part of stroke prevention. According to the American Heart Association, more than 795,000 people have a stroke each year in the U.S.
A Mayo Clinic visualization tool can help you decide if cholesterol-lowering statin drugs are right for you.
“Physicians have a duty to inform their patients about the risks and benefits of the interventions available to them. However, physicians rarely communicate with methods that convey absolute information, such as numbers needed to treat, numbers needed to harm, or prolongation of life, despite patients wanting this information.” That is, for example, how many people are actually helped by a particular drug, how many are actually hurt by it, or how much longer the drug will enable you to live, respectively.
If doctors inform patients only about the relative risk reduction—for example, telling them a pill will cut their risk of heart attacks by 34 percent—nine out of ten agree to take it. However, give them the same information framed as absolute risk reduction—“1.4% fewer patients had heart attacks”—then those agreeing to take the drug drops to only four out of ten. And, if they use the number needed to treat, only three in ten patients would agree to take the pill. So, if you’re a doctor and you really want your patient to take the drug, which statistic are you going to use?
The use of relative risk stats to inflate the benefits and absolute risk stats to downplay any side effects has been referred to as “statistical deception.” To see how one might spin a study to accomplish this, let’s look at an example. As you can see below and at 1:49 in my video, The True Benefits vs. Side Effects of Statins, there is a significantly lower risk of the incidence of heart attack over five years in study participants randomized to a placebo compared to those getting the drug. If you wanted statins to sound good, you’d use the relative risk reduction (24 percent lower risk). If you wanted statins to sound bad, you’d use the absolute risk reduction (3 percent fewer heart attacks).
Then you could flip it for side effects. For example, the researchers found that 0.3 percent (1 out of 290 women in the placebo group) got breast cancer over five years, compared to 4.1 percent (12 out of 286) in the statin group. So, a pro-statin spin might be a 24 percent drop in heart attack risk and only 3.8 percent more breast cancers, whereas an anti-statin spin might be only 3 percent fewer heart attacks compared to a 1,267 percent higher risk of breast cancer. Both portrayals are technically true, but you can see how easily you could manipulate people if you picked and chose how you were presenting the risks and benefits. So, ideally, you’d use both the relative risk reduction stat and the absolute risk reduction stat.
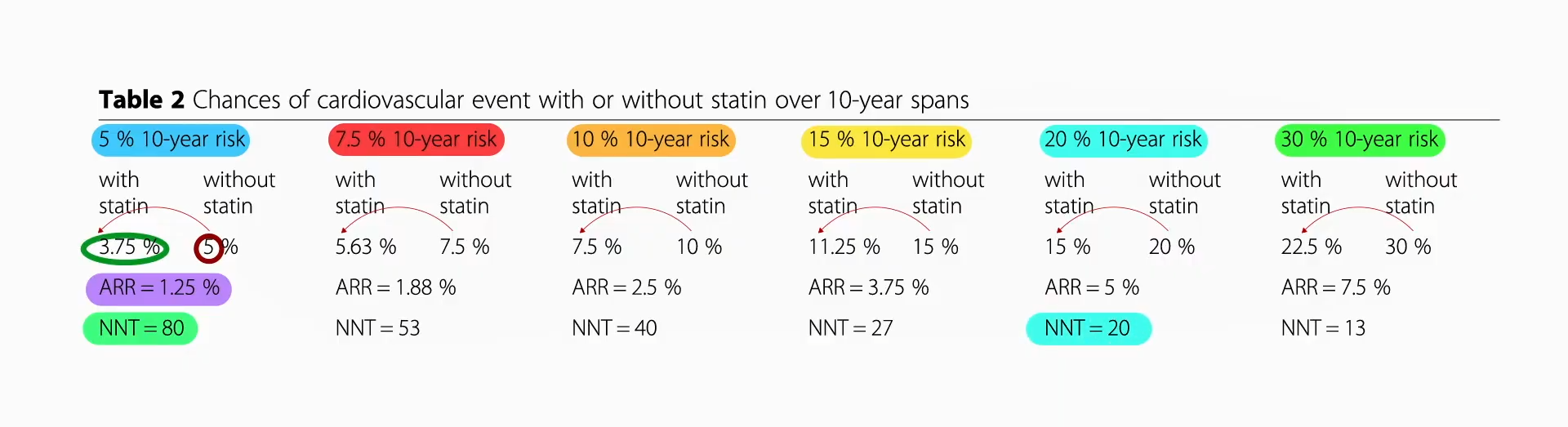
In terms of benefits, when you compile many statin trials, it looks like the relative risk reduction is 25 percent. So, if your ten-year risk of a heart attack or stroke is 5 percent, then taking a statin could lower that from 5 percent to 3.75 percent, for an absolute risk reduction of 1.25 percent, or a number needed to treat of 80, meaning there’s about a 1 in 80 chance that you’d avoid a heart attack or stroke by taking the drug for the next ten years. As you can see, as your baseline risk gets higher and higher, even though you have that same 25 percent risk reduction, your absolute risk reduction gets bigger and bigger. And, with a 20 percent baseline risk, that means you have a 1 in 20 chance of avoiding a heart attack or stroke over the subsequent decade if you take the drug, as seen below and at 3:31 in my video.
So, those are the benefits. In terms of risk, that breast cancer finding appears to be a fluke. Put together all the studies, and “there was no association between use of statins and the risk of cancer.” In terms of muscle problems, estimates of risk range from approximately 1 in 1,000 to closer to 1 in 50.
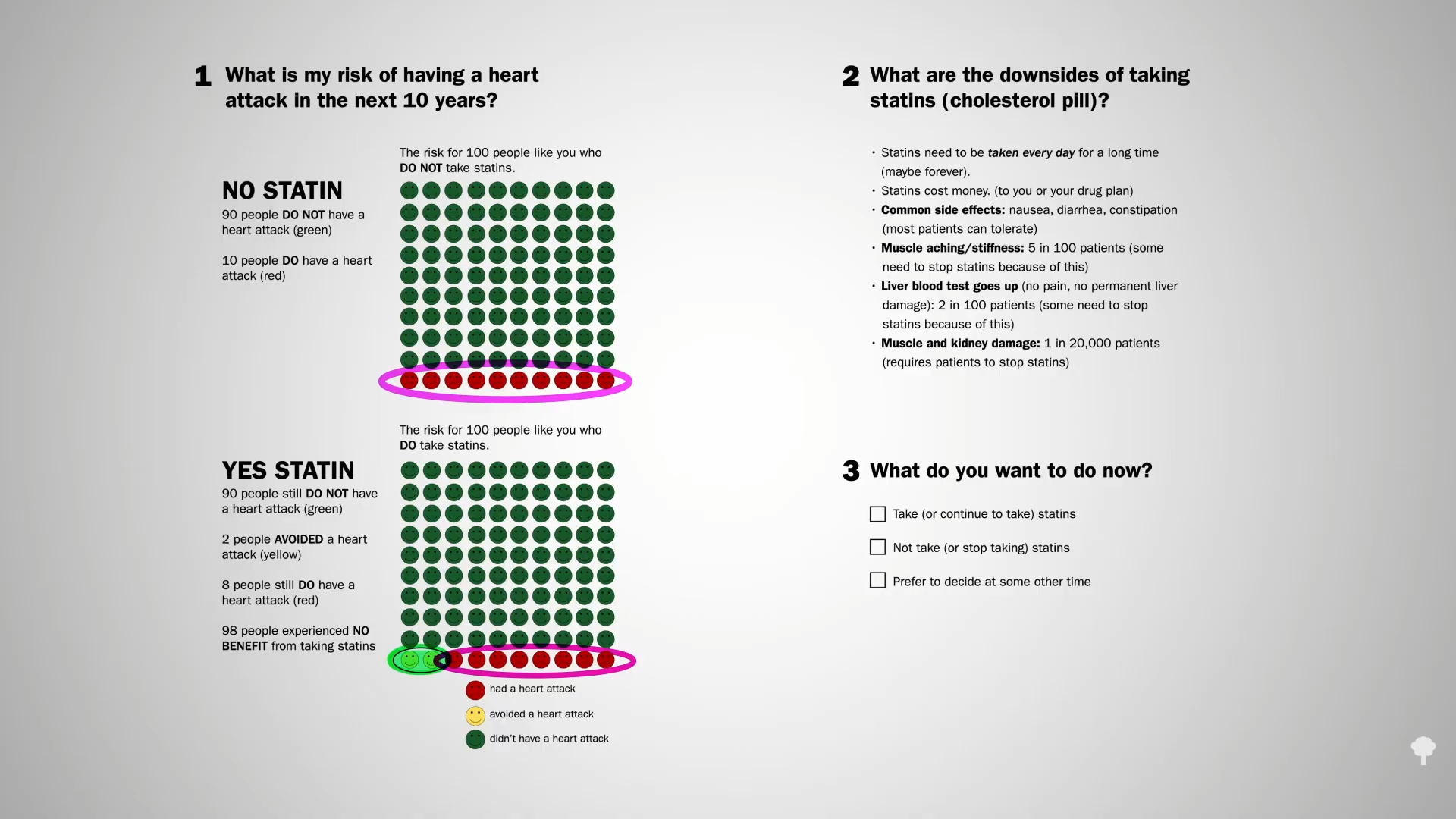
If all those numbers just blur together, the Mayo Clinic developed a great visualization tool, seen below and at 4:39 in my video.
For those at average risk, 10 people out of 100 who do not take a statin may have a heart attack over the next ten years. If, however, all 100 people took a statin every day for those ten years, 8 would still have a heart attack, but 2 would be spared, so there’s about a 1 in 50 chance that taking the drug would help avert a heart attack over the next decade. What are the downsides? The cost and inconvenience of taking a pill every day, which can cause some gastrointestinal side effects, muscle aching, and stiffness in about 5 percent, reversible liver inflammation in 2 percent, and more serious damage in perhaps 1 in 20,000 patients.
Note that the two happy faces in the bottom left row of the YES STATIN chart represent heart attacks averted, not lives saved. The chance that a few years of statins will actually save your life if you have no known heart disease is about 1 in 250.
If you want a more personalized approach, the Mayo Clinic has an interactive tool that lets you calculate your ten-year risk. You can get there directly by going to bit.ly/statindecision.
A chef from California’s Central Coast who had two strokes while traveling internationally on American Airlines was awarded more than $9 million after a federal jury concluded employees failed to follow their own protocols to help him.
In November 2021, Jesus Plasencia, a chef from Watsonville who was 67 at the time, was traveling with his wife, Ana Maria Marcela Tavantzis, on a flight to Madrid from Miami, according to a complaint they filed in federal civil court.
While the plane was still at the gate, Plasencia suffered a “mini stroke” and temporarily lost the ability to speak or pick up his phone, according to the complaint. His wife alerted a flight attendant and the pilot but instead of alerting medical personnel and following company policy, the lawsuit said the pilot dismissed her concerns, “joked with Plasencia, and cleared him for take-off.”
Plasencia then had a stroke while the plane was in the air; he was hospitalized after the plane landed in Spain and was in critical condition for more than three weeks before he went back to the U.S., according to court documents. He can’t speak or write and now “depends entirely on daily, significant, around-the-clock, in-home care and intensive rehabilitation,” according to the lawsuit.
On Thursday, a federal jury in San Jose said American Airlines was on the hook for $9.6 million for its employees failing to follow company protocol in the incident.
According to the complaint filed in 2023, the flight crew had asked other passengers to monitor Plasencia after he suffered a stroke during the flight, but didn’t tell the pilot about the medical emergency, so the flight wasn’t diverted.
The couple argued that because American Airlines crew hadn’t followed protocols, Plasencia was delayed getting care for nearly eight hours and could’ve potentially had a better outcome, according to the lawsuit.
“The safety and well-being of our passengers is our highest priority,” American Airlines said in a statement. “While we respect the jury’s decision, we disagree with the verdict and are currently evaluating next steps.”
Darren Nicholson of Burns Charest, who represented the couple in the lawsuit, argued that the airline didn’t follow stroke protocol, which calls for immediate medical assistance and diverting the aircraft.
“It is shocking that American Airlines responded so poorly to a medical emergency like this,” he said in a statement.
American Airlines was found liable by the jurors under the Montreal Convention, an international treaty that governs international air travel.
How can you calculate your own personal heart disease risk to help you determine if you should start on a cholesterol-lowering statin drug?
The muscle-related side effects from cholesterol-lowering statins “are often severe enough for patients to stop taking the drug. Of course, these side effects could be coincidental or psychosomatic and have nothing to do with the drug,” given that many clinical trials show such side effects are rare. “It is also possible that previous clinical trials”—funded by the drug companies themselves—“under-recorded the side effects of statins.” The bottom line is that there’s an urgent need to establish the true incidence of statin side effects.
“What proportion of symptomatic side effects in patients taking statins are genuinely caused by the drug?” That’s the title of a journal article that reports that, even in trials funded by Big Pharma, “only a small minority of symptoms reported on statins are genuinely due to the statins,” and those taking statins are significantly more likely to develop type 2 diabetes than those randomized to placebo sugar pills. Why? We’re still not exactly sure, but statins may have the double-whammy effect of impairing insulin secretion from the pancreas while also diminishing insulin’s effectiveness by increasing insulin resistance.
Even short-term use of statins may “approximately double the odds of developing diabetes and diabetic complications.” As shown below and at 1:49 in my video Who Should Take Statins?, fewer people develop diabetes and diabetic complications off statins over a period of about five years than those who do develop diabetes while on statins. “Of more concern, this increased risk persisted for at least 5 years after statin use stopped.”
“In view of the overwhelming benefit of statins in the reduction of cardiovascular events,” the number one killer of men and women, any increase in risk of diabetes, our seventh leading cause of death, would be outweighed by any cardiovascular benefits, right? That’s a false dichotomy. We don’t have to choose between heart disease and diabetes. We can treat the cause of both with the same diet and lifestyle changes. The diet that can not only stop heart disease, but also reverse it, is the same one that can reverse type 2 diabetes. But what if, for whatever reason, you refuse to change your diet and lifestyle? In that case, what are the risks and benefits of starting statins? Don’t expect to get the full scoop from your doctor, as most seemed clueless about statins’ causal link with diabetes, so only a small fraction even bring it up with their patients.
“Overall, in patients for whom statin treatment is recommended by current guidelines, the benefits greatly outweigh the risks.” But that’s for you to decide. Before we quantify exactly what the risks and benefits are, what exactly are the recommendations of current guidelines?
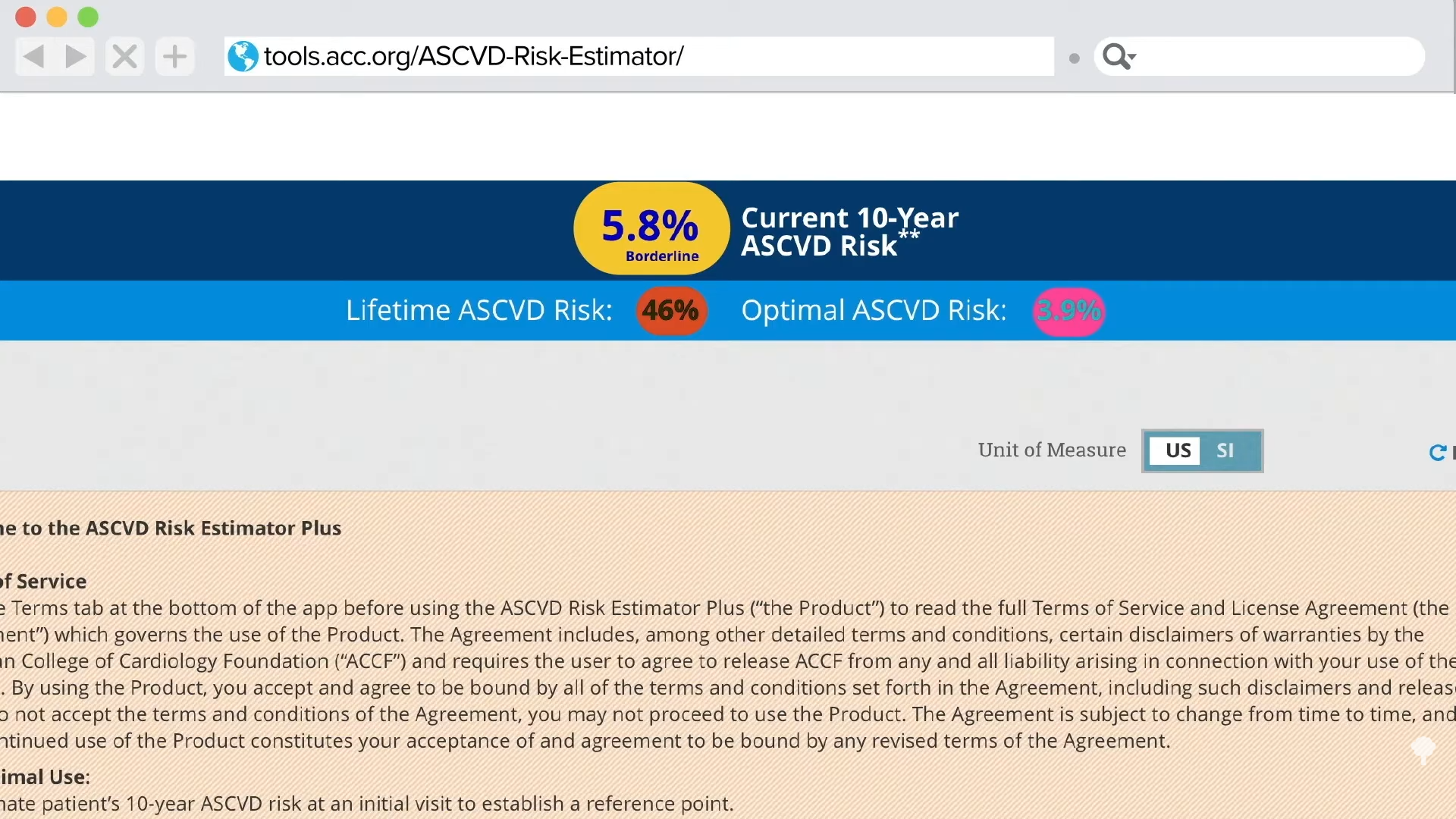
How should you decide if a statin is right for you? “If you have a history of heart disease or stroke, taking a statin medication is recommended, without considering your cholesterol levels.” Period. Full stop. No discussion needed. “If you do not yet have any known cardiovascular disease,” then the decision should be based on calculating your own personal risk. If you know your cholesterol and blood pressure numbers, it’s easy to do that online with the American College of Cardiology risk estimator or the Framingham risk profiler.
My favorite is the American College of Cardiology’s estimator because it gives you your current ten-year risk and also your lifetime risk. So, for a person with a 5.8 percent risk of having a heart attack or stroke within the next decade, if they don’t clean up their act, that lifetime risk jumps to 46 percent, nearly a flip of the coin. If they improved their cholesterol and blood pressure, though, they could reduce that risk by more than tenfold, down to 3.9 percent, as shown below and at 4:11 in my video.
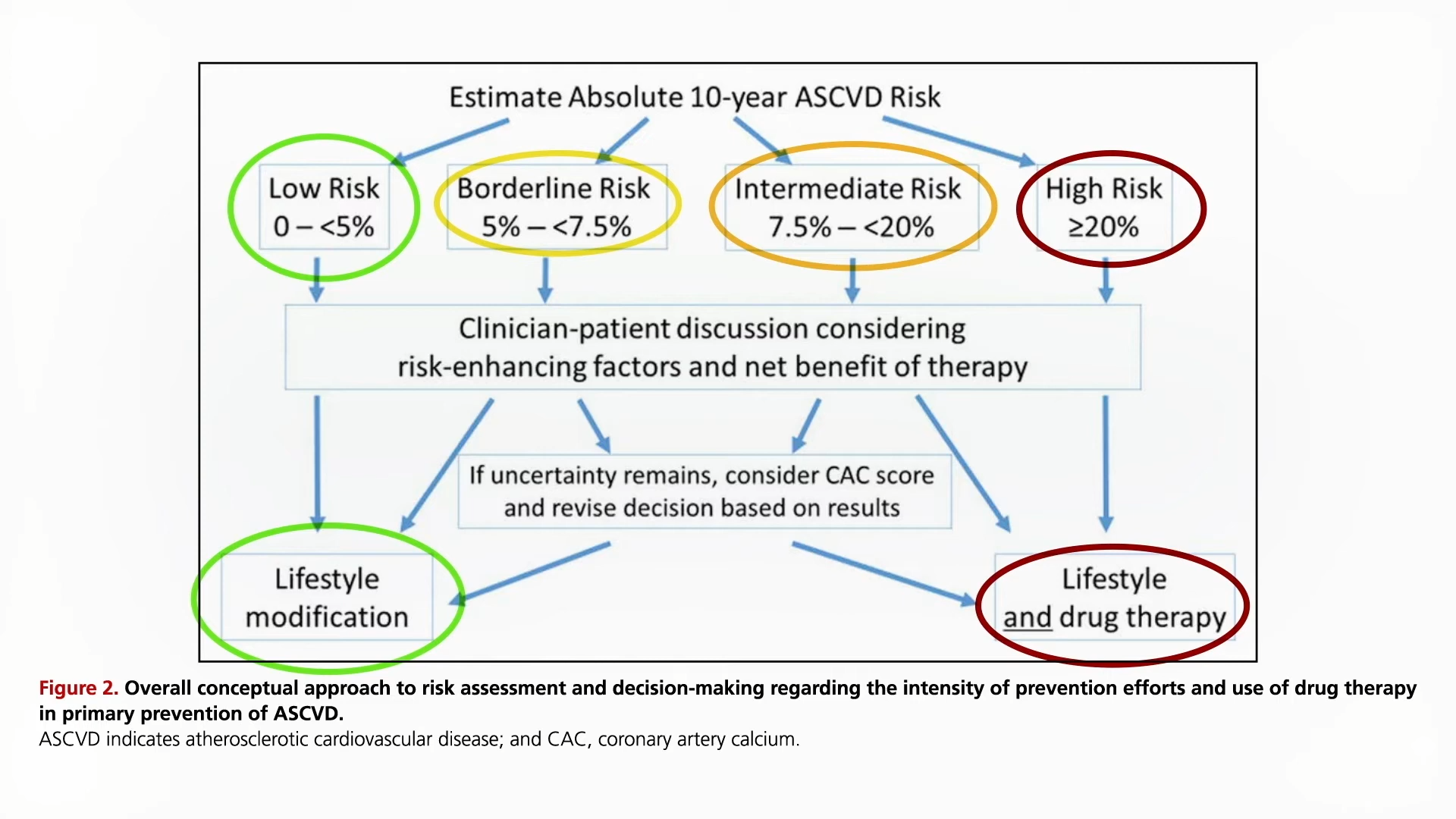
Since the statin decision is based on your ten-year risk, what do you do with that number? As you can see here and at 4:48 in my video, under the current guidelines, if your ten-year risk is under 5 percent, then, unless there are extenuating circumstances, you should just stick to diet, exercise, and smoking cessation to bring down your numbers. In contrast, if your ten-year risk hits 20 percent, then the recommendation is to add a statin drug on top of making lifestyle modifications. Unless there are risk-enhancing factors, the tendency is to stick with lifestyle changes if risk is less than 7.5 percent and to move towards adding drugs if above 7.5 percent.
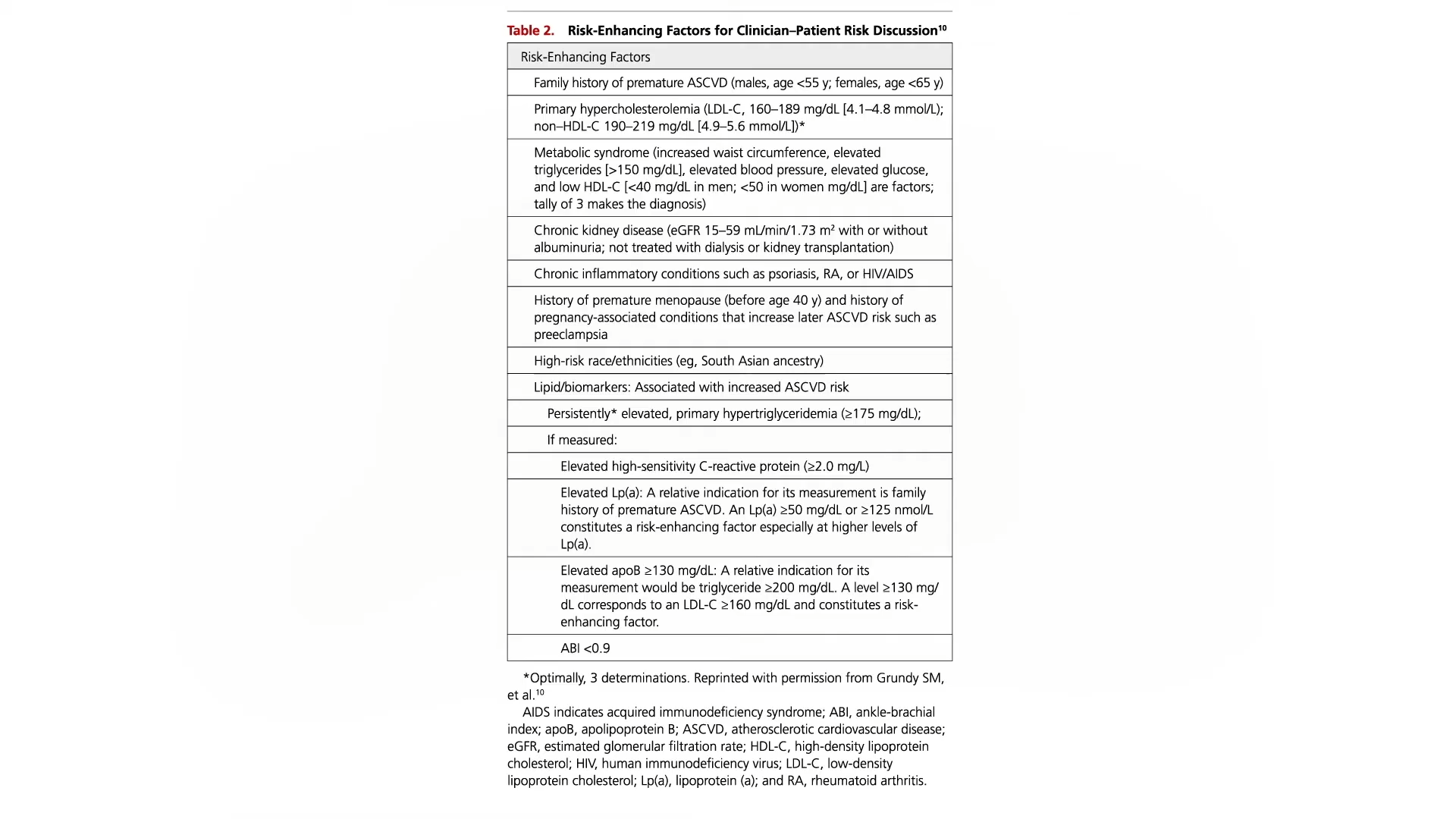
Risk-enhancing factors that your doctor should take into account when helping you make the decision include a bad family history, really high LDL cholesterol, metabolic syndrome, chronic kidney or inflammatory conditions, or persistently high triglycerides, C-reactive protein, or LP(a). You can see the whole list here and at 4:54 in my video.
If you’re still uncertain, guidelines suggest you consider getting a coronary artery calcium (CAC) score, but even though the radiation exposure from that test is relatively low these days, the U.S. Preventive Services Task Force has explicitly concluded that the current evidence is insufficient to conclude that the benefits outweigh the harms.