OpenAI claims that 10% of the world’s population currently uses ChatGPT on a weekly basis. In a report published by on Monday, OpenAI highlights how it is handling users displaying signs of mental distress and the company claims that 0.07% of its weekly users display signs of “mental health emergencies related to psychosis or mania,” 0.15% expressed risk of “self-harm or suicide,” and 0.15% showed signs of “emotional reliance on AI.” That totals nearly three million people.
In its ongoing effort to show that it is trying to improve guardrails for users who are in distress, OpenAI shared the details of its work with 170 mental health experts to improve how ChatGPT responds to people in need of support. The company claims to have reduced “responses that fall short of our desired behavior by 65-80%,” and now is better at de-escalating conversations and guiding people toward professional care and crisis hotlines when relevant. It also has added more “gentle reminders” to take breaks during long sessions. Of course, it cannot make a user contact support nor will it lock access to force a break.
The company also released data on how frequently people are experiencing mental health issues while communicating with ChatGPT, ostensibly to highlight how small of a percentage of overall usage those conversations account for. According to the company’s metrics, “0.07% of users active in a given week and 0.01% of messages indicate possible signs of mental health emergencies related to psychosis or mania.” That is about 560,000 people per week, assuming the company’s own user count is correct. The company also claimed to handle about 18 billion messages to ChatGPT on a weekly basis, so that 0.01% equates to 1.8 million messages of psychosis or mania.
One of the company’s other major areas of emphasis for safety was improving its responses to users expressing desires to self-harm or commit suicide. According to OpenAI’s data, about 0.15% of users per week express “explicit indicators of potential suicidal planning or intent,” accounting for 0.05% of messages. That would equal about 1.2 million people and nine million messages.
The final area the company focused on as it sought to improve its responses to mental health matters was emotional reliance on AI. OpenAI estimated that about 0.15% of users and 0.03% of messages per week “indicate potentially heightened levels of emotional attachment to ChatGPT.” That is 1.2 million people and 5.4 million messages.
OpenAI has taken steps in recent months to try to provide better guardrails to protect against the potential that its chatbot enables or worsens a person’s mental health challenges, following the death of a 16-year-old who, according to a wrongful death lawsuit from the parents of the late teen, asked ChatGPT for advice on how to tie a noose before taking his own life. But the sincerity of that is worth questioning, given at the same time the company announced new, more restrictive chats for underage users, it also announced that it would allow adults to give ChatGPT more of a personality and engage in things like producing erotica—features that would seemingly increase a person’s emotional attachment and reliance on the chatbot.
Robbie Williams says that he’s been privately fighting a battle against what he calls “inside Tourette’s.” The British pop star and subject of Oscar-nominated film Better Man shared the news while appearing on the comedian Paul Welsh’s podcast, I’m ADHD! No You’re Not.
“I’ve just realized that I have Tourette’s, but they don’t come out,” Williams said on the podcast. “I was just walking down the road the other day and I realized that these intrusive thoughts are ‘inside Tourette’s.’”
Tourette syndrome, as defined by the CDC, is a condition of the nervous system often defined by sudden, repetitive sounds or movements, often known as tics, that can be triggered by factors such as stress, excitement, or tiredness.
Williams, who kicked off his Britpop Tour in May, says that he has been an “Olympian at masking” his symptoms, and that his condition makes performing live extremely difficult. “I have a very complicated relationship with touring and performing live,” he said on the podcast. “People say, ‘Oh, you going on tour? You must be really, really excited.’ Not really. I’m terrified.”
The “Angels” singer is aware that he may not present as someone who gets stage fright. “I will look full of bravado and look pompous and look smug and do these grand gestures, which have worked for me because they put my face on the poster and people still buy tickets,” he said. “But actually what’s happening is I feel like the opposite of that all the time, most of the time.”
While it may be difficult for him to perform live, Williams says that the condition is improving. “It’s getting better,” he said. “I would say it’s gotten better from 45 onwards. This particular tour that I’m now in, I’m very pleased to say, for me, is that I’m dead excited to do my show that I’m doing tomorrow and I was excited to do one last week.”
The 51-year-old is not the only famous singer who struggles with the neurological condition. Scottish singer-songwriter Lewis Capaldi in 2023 had to take a break from music after his tics prevented him from completing a performance at Glastonbury. Billie Eilish also recounted being affected by Tourette syndrome, which she was diagnosed with when she was 11. “If you film me for long enough, you’re going to see a lot of tics,” she told David Letterman on My Next Guest Needs No Introduction in 2022.
Williams credits his wife, Ayda Field Williams, for helping adjust his perspective on performing live, highlighting how she emphasized how lucky he is to perform for a living and how he may not always have the chance to play stadiums.
“And in that moment, thinking about maybe never being able to do it again because of waning popularity or death or whatever it is, in that moment, it just changed my perception,” he says. “But 80,000 people never changed my opinion about me.”
Fairfax County’s co-responder program, which expanded last year, has helped respond to over 2,000 calls since its inception, according to the county’s 2023 Diversion First annual report.
The program, which launched in 2021 and pairs a Fairfax County police officer with a crisis intervention specialist, expanded last year. It now has four teams that respond to calls between noon and midnight, seven days a week.
It also includes a Post Response Team, “which is comprised of a clinician and a peer recovery specialist to provide that post-crisis specialist,” said Lisa Potter, the county’s Diversion First manager.
As of Dec. 31, 2023, the co-responder teams were a part of over 2,100 calls for service, according to the 16-page report, which was recently published and offers a glimpse into the way county programs work to help prevent incarceration for those with mental illness, developmental disabilities and substance use disorders.
Of the over 2,100 calls, close to half of them were resolved in the field, according to the report, and about a quarter of them resulted in diversion from an arrest and/or hospitalization.
“When law enforcement is dispatched to a community situation and it turns out to be (a) primary mental health situation, they sometimes will stand down, and they will call the community services board to have a mental health counselor come out and interact with the individual,” said Daryl Washington, executive director of the Fairfax-Falls Church Community Services Board. “But with the co-responder, there’s not that need for that wait.”
Instead, Washington said, responders can quickly take action depending on what they’re seeing when they arrive at a scene.
The initiatives that fall under Diversion First aim to “decriminalize mental illness and individuals with substance use and developmental disabilities,” Washington said. Funding for them comes from the county government, the state and grants.
Broadly, Potter said the programs are helping divert thousands of people away from potential arrests every year. Of the people diverted to the Merrifield Crisis Response Center, 80% haven’t had a repeat visit in a year.
“We’re continuing to see a rise in the number of people that are diverted consistently each year, which is great,” Potter said.
The county has been deliberate in trying to strengthen “the first touch points that individuals have with our emergency and crisis system,” Washington said, and part of that is making sure the few dozen mental health calls coming into 911 every day are answered by someone who is trained to help.
There are a few mental health clinicians embedded in the 911 call center, Washington said, and the county has a separate partnership with HopeLink, another crisis call center. The crisis call center also has the ability to dispatch the county’s crisis response teams.
As part of the Diversion First efforts, capacity in the county’s Drug Treatment Court is doubling, from 25 to 50, and is launching a Young Adult 18-25 track.
“The drug court team was noticing that they were getting a lot of young adults, so we were able to procure funding to launch a new group specifically for young adults,” Potter said.
Explore the world of love through a variety of lenses. Here’s a collection of powerful films that each portray love and romance in a unique way, spanning multiple genres including drama, comedy, fantasy, animation, and sci-fi.
“Cinema is a mirror by which we often see ourselves.”
Alejandro Gonzalez Inarritu
Movies give us the opportunity to explore major themes in life in a meaningful and profound way.
A powerful film can lead to a better understanding of your own experiences. It can communicate thoughts and emotions that may have been challenging to express; and, at times, completely reshape our perspective on life.
For better or worse, movies play a pivotal role in shaping our beliefs and map of reality. We pick up ideas through films, sometimes absorbed at a very young age, and those ideas find their way into our daily lives influencing our choices and perspectives.
Filmmakers understand the transformative power of cinema, purposely using it to shake up people’s consciousness. The goal of a solid film is to create an experience that leaves you a different person by the end of it.
As viewers, it’s essential to be aware of a film’s effects both emotionally and intellectually. Often, the movies that linger in our thoughts long after watching are the most impactful and life-changing.
Here’s a collection of classic films about love and romance. Each movie has had a lasting influence on audiences in one way or another. It’s an eclectic list that spans multiple genres, including drama, comedy, animation, fantasy, mystery, and sci-fi.
Titanic (1997)
James Cameron’s epic tale blends love and tragedy against the historical backdrop of the Titanic’s sinking in 1912. The film weaves a captivating narrative of a forbidden romance blossoming amidst a natural disaster.
Eternal Sunshine of the Spotless Mind (2004)
In this mind-bending story, a man attempts to erase the memories of a lost love using cutting-edge technology, only to find fate conspiring to bring the couple back together repeatedly. The film explores the complexities of memory, love, and destiny.
Beauty and the Beast (1991)
Disney’s classic adaptation of the French fairy tale is celebrated for its beautiful animation and memorable songs. The film goes beyond appearances, illustrating the transformative power of true love.
Her (2013)
Set in a near-future world, “Her” tells the unconventional love story of a lonely man who forms a deep connection with his computer’s operating system. The film delves into themes of technology, loneliness, and the nature of human connection.
Before Sunrise (1995)
Richard Linklater’s film follows two young tourists who meet on a train in Europe and share an unforgettable night in Vienna. The movie explores the transient nature of connections and the profound impact of brief encounters.
Lost in Translation (2003)
Sofia Coppola’s film features a washed-up American celebrity and a young woman forging an unexpected bond in Tokyo. “Lost in Translation” navigates themes of loneliness, connection, and self-discovery.
Cinema Paradiso (1988)
An Italian filmmaker reflects on his past and learns how to channel his love in a different and creative way through his art and craftsmanship.
Past Lives (2023)
Two childhood friends reconnect after years apart, seeking to unravel the meaning behind their enduring connection. The film explores the complexities of friendship, time, and shared history.
Set in a dystopian future, “The Lobster” challenges societal norms by presenting a world where individuals must choose a romantic partner within 45 days or face transformation into an animal. The film satirizes the pressure to conform in matters of love.
Annie Hall (1977)
Woody Allen’s classic romantic comedy is a hilarious and heartfelt movie that explores neurotic love and the psychological obstacles we commonly face in marriage and long-term relationships.
Your Name. (2016)
A masterful anime that combines elements of science fiction, fantasy, and romance. It centers on a mysterious connection between a boy and girl who swap bodies, learn about each other’s lives, and search to find each other in real life.
A Woman Under the Influence (1974)
John Cassavetes’ uncomfortably raw and dramatic portrayal of the profound impact of mental illness on marriage and family, navigating the complexities with unflinching honesty.
The Fountain (2006)
Darren Aronofsky’s “The Fountain” explores love and mortality through three interconnected storylines spanning different time periods. The film delves into themes of eternal love and the quest for immortality, providing a visually stunning and emotionally resonant experience.
Scenes From a Marriage (1974)
Legendary director Ingmar Bergman’s deeply incisive and detailed chronicle of a rocky marriage’s final days.
Choose one movie and analyze it
Each of these films offers a different perspective on love while also pushing the boundaries of cinema and story-telling.
It’s fun to compare each story: How did the couples meet? What defined “love” for them? What obstacles did they face? Did the relationship work out in the end or not? Why?
While films are often seen as just a source of entertainment or healthy escapism, they can also be an avenue for self-improvement and growth.
The “Movie Analysis Worksheet” is designed to make you think about the deeper themes behind a film and extract some lessons from it that you can apply to your life.
Watch with a friend and discuss
If you don’t want to do the worksheet, just watch one of the movies with a friend (or loved one) – then discuss it after.
Watching a film together is an opportunity to share a new experience. It can also spark up interesting conversations. This is one reason why bonding through movies is one of the most common ways we connect with people in today’s world.
Which film will you check out?
Enter your email to stay updated on new content on self improvement:
“Love On The Spectrum” is a reality television show centered on how people with autism view, seek, and find love. It’s a fun, inspiring, and heartwarming series that we can all draw many lessons from.
Related Articles
Enter your email to stay updated on new content on self improvement:
About four years ago, a new patient came to see me for a psychiatric consultation because he felt stuck. He’d been in therapy for 15 years, despite the fact that the depression and anxiety that first drove him to seek help had long ago faded. Instead of working on problems related to his symptoms, he and his therapist chatted about his vacations, house renovations, and office gripes. His therapist had become, in effect, an expensive and especially supportive friend. And yet, when I asked if he was considering quitting treatment, he grew hesitant, even anxious. “It’s just baked into my life,” he told me.
Among those who can afford it, regular psychotherapy is often viewed as a lifelong project, like working out or going to the dentist. Studies suggest that most therapy clients can measure their treatments in months instead of years, but a solid chunk of current and former patients expect therapy to last indefinitely. Therapists and clients alike, along with celebrities and mediaoutlets, have endorsed the idea of going to therapy for extended stretches, or when you’re feeling fine. I’ve seen this myself with friends who are basically healthy and think of having a therapist as somewhat like having a physical trainer. The problem is, some of the most commonly sought versions of psychotherapy are simply not designed for long-term use.
Therapy comes in many varieties, but they all share a common goal: to eventually end treatment because you feel and function well enough to thrive on your own. Stopping doesn’t even need to be permanent. If you’ve been going to therapy for a long time, and you’re no longer in acute distress, and you have few symptoms that bother you, consider taking a break. You might be pleasantly surprised by how much you learn about yourself.
Therapy, in both the short and long term, can be life-altering. Short-term therapy tends to be focused on a particular problem, such as a depressed mood or social anxiety. In cognitive behavioral therapy, usually used for depressive and anxiety disorders, a clinician helps a client relieve negative feelings by correcting the distorted beliefs that he has about himself. In dialectical behavior therapy, commonly used to treat borderline personality disorder, patients learn skills to manage powerful emotions, which helps improve their mood and relationships. Both treatments typically last less than a year. If you start to get rusty or feel especially challenged by life events that come your way, you simply return for another brief stint. Termination is expected and normal.
Some types of therapy, such as psychodynamic therapy and psychoanalysis, are designed to last for several years—but not forever. The main goal of these therapies is much more ambitious than symptom relief; they aim to uncover the unconscious causes of suffering and to change a client’s fundamental character. At least one well-regarded study found that long-term therapy is both highly effective and superior to briefer treatment for people diagnosed with a clinically significant psychiatric illness; other papers have shown less conclusive evidence for long-term therapy. And few studies compare short and extended treatment for clients with milder symptoms.
In fact, there’s reason to believe that talk therapy in the absence of acute symptoms may sometimes cause harm. Excessive self-focus—easily facilitated in a setting in which you’re literally paying to talk about your feelings—can increase your anxiety, especially when it substitutes for tangible actions. If your neurotic or depressive symptoms are relatively mild (meaning they don’t really interfere with your daily functioning), you might be better served by spending less time in a therapist’s office and more time connecting with friends, pursuing a hobby, or volunteering. Therapists are trained to use the tools they’ve learned for certain types of problems, and many of the stress-inducing minutiae of daily life are not among them. For example, if you mention to your therapist that you’re having trouble being efficient at work, he might decide to teach you a stress-reduction technique, but your colleagues or boss might provide more specific strategies for improving your performance.
One of my childhood friends, whose parents were both psychoanalysts, went to weekly therapy appointments while we were growing up. He was a happy, energetic kid, but his parents wanted him and his sister to be better acquainted with their inner lives, to help them deal with whatever adversity came their way. My friend and his sister both grew up to be successful adults, but also highly anxious and neurotic ones. I imagine their parents would say the kids would have been worse without the therapy—after all, mental illness ran in their family. But I can find no substantial clinical evidence supporting this kind of “preventive” psychotherapy.
Beginning therapy in the first place is, to be clear, a privilege. Therapy is not covered by many insurance plans, and a very large number of people who could benefit from it can’t afford it for any duration. Only 47 percent of Americans with a psychiatric illness received any form of treatment in 2021; in fact, federal estimates suggest that the United States is several thousand mental-health professionals short, a gap that is likely to grow in the coming years. Stopping therapy when you’re ready opens up space for others who might need this scarce service more than you do.
I do not mean to suggest that a therapy vacation should be considered lightly, or that it’s for everyone. If you have a serious mental-health disorder, such as major depression or bipolar disorder, you should discuss with your mental-health provider whether ending therapy is appropriate for your individual situation. (Keep in mind that your therapist might not be ready to quit when you are. Aside from a financial incentive to continue treatment, parting with a charming, low-maintenance patient is not so easy.) My rule of thumb is that you should have minimal to no symptoms of your illness for six months or so before even considering a pause. Should you and your therapist agree that stopping is reasonable, a temporary break with a clear expiration date is ideal. At any time, if you’re feeling worse, you can always go back.
Psychiatrists do something similar with psychiatric meds: For example, when I prescribe a depressed patient an antidepressant, and then they remain stable and free of symptoms for several years, I usually consider tapering the medication to determine whether it’s still necessary for the patient’s well-being. I would do this only for patients who are at a low risk of relapse—for example, people who’ve had just one or two episodes, rather than many over a lifetime. Pausing therapy should be even less risky: The beautiful thing about therapy is that, unlike a drug, it equips you with new knowledge and skills, which you carry with you when you leave.
About a year after my patient and I first talked about ending therapy, I ran into him in a café. He told me that stopping had taken him six months, but now he was thriving. Maybe you, like my patient, are daunted by the idea of quitting cold turkey. If so, consider taking a vacation from treatment instead. It might be the perfect way to see how far you’ve really come.
One of my chronically depressed patients recently found a psychoactive drug that works for him after decades of searching. He took some psilocybin from a friend and experienced what he deemed a miraculous improvement in his mood. “It was like taking off a dark pair of sunglasses,” he told me in a therapy session. “Everything suddenly seemed brighter.” The trip, he said, gave him new insight into his troubled relationships with his grown children and even made him feel connected to strangers.
I don’t doubt my patient’s improvement—his anxiety, world-weariness, and self-doubt seemed to have evaporated within hours of taking psilocybin, an effect that has continued for at least three months. But I’m not convinced that his brief, oceanic experience was the source of the magic. In fact, some neuroscientists now believe that the transcendent, reality-warping trip is just a side effect of psychedelics—one that isn’t sufficient or even necessary to produce the mental-health benefits the drugs seem to provide.
For several years, researchers have understood that the hallucinatory effects of psychedelics can, in theory, be separated from the other ways the drugs affect our mental state and brain structure. But until recently, they have not been able to design a psychedelic that reliably produces only the neurocognitive effects and not the hallucinatory ones. That may soon change. A new generation of nonhallucinogenic psychedelics, at least one of which is currently being tested in humans, aims to provide all of the mental-health benefits of LSD, psilocybin, or Ecstasy without the trip. Trip-free psychedelics would be a great therapeutic boon, dramatically expanding the number of people who can experience the benefits of these drugs. They might also shed new light on how much psychedelics can alleviate psychic distress—and why they do so at all.
Over the past five years, studies have demonstrated that psilocybin has powerful antidepressant effects, and that MDMA (a.k.a. Ecstasy), in conjunction with psychotherapy, can relieve the symptoms of PTSD. Remarkably, just a few doses of either psilocybin or MDMA can produce a rapid, lasting improvement in depression and anxiety symptoms, meaning symptom relief within minutes or hours that lasts up to 12 weeks. (MDMA is what psychiatrists call an “atypical psychedelic”; it has a mix of psychedelic-like and amphetamine-like effects, producing a feeling of bliss rather than a transcendent or mystical state.) The FDA is widely expected to approve MDMA for supervised use sometime in 2024—an extraordinary turnabout for drugs that have long been stigmatized for their potential (if rare) serious harms.
From a clinical perspective, this psychedelic revolution is potentially miraculous. An estimated 23 percent of Americans have a mental illness, and a considerable number of them, like my patient, don’t get sufficient relief from therapy or existing medications. Drugs like psilocybin, ayahuasca, and LSD could help many of these patients—but others won’t be able to tolerate the trip. (By “trip,” I mean the variety of altered mental states that psychedelic drugs can cause, such as the transcendence and mystical experience of LSD and psilocybin, and the bliss and social openness of MDMA.) Drug-induced hallucinations are known to give certain people—like those with psychotic disorders or severe personality disorders—extreme anxiety or even lead to a psychotic break. That’s why clinical trials of psychedelics typically exclude those patients.
I don’t mean to discount the delight and power of a transcendent hallucination. Many people who’ve tripped on psychedelics describe the experience as among the most meaningful of their life. And in several studies of psilocybin for depression, the intensity of the trip correlates with the magnitude of the therapeutic effect. A trip is an extraordinary, consciousness-expanding experience that can offer the tripper new insight into her life and emotions. It also feels pretty damn good. But it’s far from the only effect the drugs have on the human brain.
During a trip, psychedelics are silently doing something even more remarkable than warping reality: They are rapidly inducing a state of neuroplasticity, in which the brain can more easily reorganize its structure and function. (Microdosing enthusiasts, who take subtherapeutic doses of drugs like psilocybin, claim to experience enhanced creativity. They may be getting neuroplastic effects without a trip, but as yet, little scientific evidence backs up that idea.) Neuroplasticity enhances learning, memory, and our ability to respond and adapt to our environment—and could be central to the therapeutic effects of psychedelics. In depression, for example, the prefrontal cortex (the brain’s reasoner in chief) loses some of its executive control over the limbic system (the brain’s emotional center). Drugs that enhance neuroplasticity allow new connections to be formed between the regions, which can help reset the relationship and put the prefrontal cortex back in control of emotion.
Like MDMA, ketamine—the animal tranquilizer, surgical anesthetic, and dissociative party drug that was also approved as a rapidly acting antidepressant in 2019—typically doesn’t produce hallucinations. But it does create a dissociative mental state, and it’s known to make neurons sprout new spines within hours of administration, a structural change that’s been linked with a reduction in depression-related behavior in animals. In humans, ketamine has been shown to boost mood—even if it’s administered when patients are unconscious. Severalstudies show that patients who receive ketamine during surgery wake up happier than they were before the operation. This suggests that you don’t need to consciously experience the dissociative effects in order to get the antidepressant benefits.
Scientists are on their way to finding out for sure. For the first time, researchers have purposively developed psychedelic drugs that appear to bring about the neuroplastic effects without producing a trip. These drugs stimulate the same serotonin receptor as traditional psychedelics: 5-HT2A, which, when triggered, causes the brain to produce more of a compound called BDNF, a kind of brain fertilizer that promotes neuronal growth and connectivity. But the nonhallucinogenic versions activate 5-HT2A without leading to a trip. (Binding and activating receptors isn’t an all-or-nothing phenomenon; different drugs can bind the same receptor in different ways, producing very different effects.)
Some of these trip-free psychedelics are new inventions. Last year, for example, scientists synthesized a new nonhallucinogenic psychedelic by imitating lisuride, an analog of LSD. (An analog is a chemical that is structurally very similar to the original compound, but has been modified to have a different function.) It doesn’t have a name yet—just a serial number, IHCH-7113—but it’s being studied in animals.
Other trip-free psychedelics have been around for decades, if not recognized as such: 2-Br-LSD, another nonhallucinogenic analog of LSD, was first synthesized in 1957 by the same chemist who created LSD. (It was meant to treat migraine.) Recent experiments show that 2-Br-LSD, like LSD, relieves depressive behavior in mice. But unlike LSD, it doesn’t make the mice twitch their heads—a sign that a substance will give humans hallucinations and other psychotic symptoms. More than 60 years after 2-Br-LSD’s invention, the Canadian company BetterLife Pharma is planning to study it as a treatment for major depression and anxiety.
LSD isn’t the only psychedelic inspiring imitators. Delix Therapeutics, a biotech company based in Boston, is using animal models to study tabernanthalog, which is an analog of the active psychedelic in ibogaine. Tabernanthalog has acute antidepressant and neuroplastic effects in animal models, and, like 2-Br-LSD, it doesn’t cause head twitching. Delix is also testing a drug that it’s calling DLX-1, which David Olson, one of Delix’s co-founders, told me is the first nonhallucinogenic psychedelic to be tested in humans; Phase 1 studies, he said, are nearly completed. Olson, who is also the director of the Institute for Psychedelics and Neurotherapeutics at UC Davis, calls the drugs he works on “psychoplastogens,” for their rapid neuroplasticity-inducing effects. He said that other nonhallucinogenic psychoplastogens that the company is working on are “close to entering clinical trials,” though how soon any of them might reach the market is unclear.
As of yet, the federal government has provided little funding for nonhallucinogenic-psychedelics research. Delix and other makers of these new psychedelics will have to submit an application to the FDA to get their drug approved, which generally requires that the new drug beats a placebo control in two randomized clinical trials. This can be a slow process, but the FDA can expedite it by designating the drug a “breakthrough therapy,” which is exactly what it did in 2018 with psilocybin.
In clinical trials, nontrip psychedelics will have at least one major advantage over their trip-inducing analogs: They can more easily be placebo-tested. Classic psychedelic research has been bedeviled by the simple fact that it is virtually impossible not to know that you are taking a classic psychedelic. Indeed, in clinical trials of MDMA and psilocybin, more than 90 percent of subjects who received the treatment correctly guessed that the drug they were given was real. This sort of defeats the purpose of placebo-testing psychedelics at all, because participants who receive the real drugs will expect to feel better. But the new nontrip psychedelics don’t produce the transcendent mental states that tend to “unblind” research subjects. They might produce more typical drug side effects, such as dry mouth or sedation, but that’s a far cry from a mystical experience.
Nontrip psychedelics may also have it easier with respect to regulation. If they don’t make you high or produce a transcendent state, they’ll likely have little appeal as recreational drugs. The Drug Enforcement Administration classifies LSD and psilocybin as Schedule I drugs, which makes them difficult for researchers to study and doctors to prescribe. Even ketamine is Schedule III and must be administered in a medical setting, which may be inconvenient for patients. Perhaps the DEA will take more kindly to nontrip psychedelics; if so, they’d be easier to access for patients and researchers alike. Plus, nonhallucinogenic psychedelics would not require the time and expense of a guide to monitor the experience. All said, the nontrip psychedelics might end up being a more popular, better-researched choice than traditional ones.
If the FDA really does approve MDMA next year, psychiatrists will have plenty of reason to celebrate. But I suspect that the future of psychedelic medicine will lean toward the wonder of pure neuroplastic potential and away from transcendence. Psychedelic trips will probably never disappear from society—for one thing, they are viewed as essential to some religious and cultural rituals. But perhaps they’ll come to be seen as less like therapy, and more like good old-fashioned fun.
SACRAMENTO, Calif. (AP) — More Californians with untreated mental illness and addiction issues could be detained against their will and forced into treatment under a new law signed by Gov. Gavin Newsom, a move to help overhaul the state’s mental health system and address its growing homelessness crisis.
The new law, which reforms the state’s conservatorship system, expands the definition of “gravely disabled” to include people who are unable to provide themselves basic needs such as food and shelter due to an untreated mental illness or unhealthy drugs and alcohol use. Local governments say current state laws leave their hands tied if a person refuses to receive help.
The law is designed to make it easier for authorities to provide care to people with untreated mental illness or addictions to alcohol and drugs, many of whom are homeless.
The bill was aimed in part at dealing with the state’s homelessness crisis. California is home to more than 171,000 homeless people — about 30% of the nation’s homeless population. The state has spent more than $20 billion in the last few years to help them, with mixed results.
Newsom is pushing his own plan to reform the state’s mental health system. Newsom’s proposal, which would overhaul how counties pay for mental and behavioral health programs and borrow $6.3 billion to pay for 10,000 new mental health treatment beds, are expected to go before voters next March.
“California is undertaking a major overhaul of our mental health system,” Newsom said in a signing announcement Tuesday. “We are working to ensure no one falls through the cracks, and that people get the help they need and the respect they deserve.”
The legislation, authored by Democratic Sen. Susan Eggman, is the latest attempt to update California’s 56-year-old law governing mental health conservatorships — an arrangement where the court appoints someone to make legal decisions for another person, including whether to accept medical treatment and take medications.
The bill was supported by the National Alliance on Mental Illness California and mayors of the biggest California cities, who said the existing conservatorship law has made it challenging to provide mental health treatment to those most in need.
Opponents of the bill, including disability rights advocates, worried the new law will result in more people being locked up and deprived them of their fundamental rights. Coercing a person into treatment could also be counterproductive, they said.
Eggman said detaining a person with mental illness against their will should only be used as a last resort. The legislation aims to provide an alternative to sending people with mental illness and addiction problems to the prison system.
“Our state prisons are full of people who, after they’ve been restored to competency, are in our state prisons because of serious mental health issues and drug addiction issues,” Eggman said in an interview. “I think that is the most inhumane way to treat the most vulnerable of us.”
The law takes effect in 2024, but counties can postpone implementation until 2026. The changes will serve as another tool to help the state reform its mental health system. Last year, Newsom signed a law that created a new court process where family members and others could ask a judge to come up with a treatment plan for certain people with specific diagnoses, including schizophrenia. That law would let the judge force people into treatment for up to a year. The court program, started this month in seven counties, also aimed at addressing the state’s homelessness crisis.
On a Thursday this past July, my husband and I drove to our county’s police academy training facility. A uniformed officer let us in. We were escorted through several hallways and into a conference room, where I was scheduled to speak representing our local National Alliance on Mental Illness office.
Standing at the front of the room, I introduced myself first with all my accomplishments ― my recent graduation from a certificate program at Columbia University, the classes and workshops I teach, and a 25-year marriage. Then I added: “And I live with chronic paranoid schizophrenia, which is why I’m here to talk to you today.”
I spoke for nearly an hour about the five types of hallucinations, the time the voices I heard identified themselves as God, Jesus and the Holy Spirit, and how I frequently thought my food was poisonous due to paranoia. I also touched on delusions I’ve had while psychotic.
It’s important for officers to hear the information of someone with lived experience of a severe mental illness, because they so often encounter people who are in a mental health crisis in the course of their duties. I want them to understand that psychosis can make people act erratically, but that in many cases, these people can be treated successfully.
To the best of my ability, I answered the officers’ questions about all aspects of living with schizophrenia. Many thanked me for coming, and for my vulnerability about a diagnosis that still has a great deal of misinformation and stigma associated with it.
I kept my mental illness a secret from friends, in-laws and employers for almost 20 years. Since 2015, I’ve been making part of my income by telling the details of what it’s like to live with schizophrenia. I talk to law enforcement, nursing students and people studying marriage and family therapy, and at treatment facilities for those who are living with a similar diagnosis.
Sharing my story helps certain groups understand mental illness better, and helps those living with it to feel less alone in their journey. The details I share can help professionals better understand what it’s like to have a break from reality.
In my late 20s, I started to have thoughts that people were out to get me. As the paranoia increased, I stopped eating and sleeping. My relatives brought me to a hospital, but it was several days before I agreed to inpatient treatment. My hospital stay led to a diagnosis of bipolar disorder with psychotic features. At the time, I had a lot of denial and shame about the labels that became a part of my identity.
Telling people I had a mental illness ― especially the men I was dating ― almost always ended with them disappearing from my life. I remember one man saying “I simply can’t handle this” when he ended things that very day, although I had never shown symptoms around him. I learned early on that mental illness was a deal breaker for many relationships.
When I met my current husband, he also had reservations about my diagnosis. When we first dated, I wasn’t compliant with my medication, so I moved in and out of severe episodes. I attempted suicide twice, and had many episodes of hearing voices, paranoia and delusions.
We stuck together, though, and even after he witnessed my symptoms, he kept supporting me. Not too long after we got together, I began to take my treatment more seriously, and we were able to focus on building a foundation for our soon-to-be marriage.
By this time, I had learned not to mention my illness to people, so it became a secret between my husband and me. My family knew, but we didn’t tell my husband’s family. We didn’t tell any of his co-workers, or the friends we started to make after we bought a condo near the Los Angeles city limits.
It wasn’t just the stigma and rejection I’d experienced that kept me silent about my struggles. It was also the internalization of the messages society had fed me about my condition and the people who live with it. I thought I was less lovable and likable, and that people who knew would view me as “crazy.”
“Telling people I had a mental illness ― especially the men I was dating ― almost always ended with them disappearing from my life.”
I had a stable period lasting almost 10 years, where I worked full-time, took classes and sat on committees for our city council. I had friends I worked with, hiked with and played racquetball with, and my husband and I regularly took trips overseas.
My psychiatrist then decided there was something amiss with my diagnosis, and took me off all medication. Within a year, I was hallucinating 24/7, not sleeping, and having a total break from reality. I remained psychotic for six months before doctors could stabilize me again.
These new doctors diagnosed me with chronic paranoid schizophrenia. It hit me and my husband like a punch. The day I got the news, we barely spoke. I remember my husband finally saying: “Well, there is nothing new about you today from yesterday.” That statement reassured me that he wasn’t going anywhere, even with this new information.
We doubled down on the secret, though, and became even more protective of our personal life and the realities of my illness. I imagined that if people had rejected me when I told them I had bipolar disorder, it would be even worse if I told them I had schizophrenia.
We’d kept this new secret between us and my family members for almost 10 years when my psychiatrist gave me a homework assignment to tell just one of my friends about my diagnosis. My psychiatrist recognized that if I was keeping a secret about something that affected my life so much, it would hold me back from being truly close to other people. She knew that hiding was isolating me from others.
My husband and I talked about it for weeks. We went back and forth on whether we even wanted to disclose my illness to anyone, after living with it undercover for so long. We talked about losing friends. We talked about the fact that once we told one friend, more would find out.
We finally decided to tell a social worker I had worked with closely at a YWCA.
Over brunch, my voice shaking, I said: “I have schizophrenia.” At first, he was a little taken aback and had some questions, but the conversation did not take over our brunch date. That night, I wrote an essay about my experience with mental illness for an online magazine. When it was published, I posted a link to it on Facebook ― and that was how my in-laws, our co-workers, and even friends who’d known me since high school found out that I was living with a mental illness.
We lost a few friends. I’m not sure if they thought “I can’t handle this,” like those early boyfriends, or if they were upset that we’d kept such a significant part of our lives from them. I often wonder if it hurt some people’s feelings to know that they were never as close to us as they may have thought because we were not living an authentic and fully open life.
I felt vulnerable and scared about finally disclosing my secret, but there was also a massive relief. For the first time since my early 30s, I could talk about myself without hiding big chunks of my reality and who I am.
I’ve been writing about life with schizophrenia ever since, and telling my story led to the position at NAMI that had me standing in front of dozens of police officers and explaining what it’s like to be in the middle of a mental health crisis.
My secret has become my tool, and I no longer hide it. I talk about it each time someone asks me to, or any time mental health is the topic. I feel like I am using a difficult situation to make a difference in other people’s lives, which gives meaning to my experience of having schizophrenia, and turns it into something that isn’t entirely negative.
I run into less stigma and more curiosity in 2023 than in all those years I lived splintered and cut off from true intimacy with relatives and friends. I am boldly myself ― my authentic self ― and I’m using that once tightly held secret to hopefully make the reality of mental illness less difficult for others like me.
For one week of every month, I have a very bad time. My back aches so badly I struggle to stand up straight. My mood swings from frantic to bleak. My concentration flags; it’s difficult to send an email. Then, my period starts, and the curse is lifted. I feel okay again.
Like some 1 to 7 percent of menstruating women, I meet the criteria for premenstrual dysphoric disorder, or PMDD. According to the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), a person with PMDD experiences marked emotional changes—such as sadness, anger, or anxiety—and physical or behavioral changes—such as difficulty concentrating, fatigue, or joint pain—in the week before their period. PMDD can also affect trans men and nonbinary people who menstruate.
When I first heard of PMDD, it was a revelation. Here was a concrete explanation for the pain and stress I was feeling every month. Better yet, there was a simple, effective treatment: common antidepressant drugs called selective serotonin reuptake inhibitors, or SSRIs, which can be prescribed for people to take only in the two weeks before their period. Birth-control pills, cognitive behavioral therapy, and calcium supplements may also help.
Then I heard about the controversy surrounding the diagnosis. When the American Psychiatric Association added a form of PMDD as a proposed disorder to the diagnostic manual in the 1980s—DSM-III-R—some scholars pushedback. They saw the diagnosis as part of the historical oppression of women, done in the name of mental health. The controversy reared up again as PMDD remained in the 1994 DSM-IV, where it was also listed under “Depressive Disorder Not Otherwise Specified.” Many people who menstruate experience emotional changes during their cycles, so defining it as a mental illness could have serious personal and societal consequences, critics argued. A 2002 Monitor on Psychology article, “Is PMDD real?,” quoted the late psychologist and author Paula Caplan: “Women are supposed to be cheerleaders,” she said. “When a woman is anything but that, she and her family are quick to think something is wrong.”
In the end, the APA weighed these concerns and pushed ahead, adding PMDD to the DSM-5 as an official diagnosis in 2013. But I found the criticism disquieting. Had I embraced a modern hysteria diagnosis? Were the symptoms I experienced even real?
Researchers have looked for hormonal differences between people who experience severe premenstrual distress and people who don’t. In some cases, they’ve found them: A 2021 meta-analysis found that people with PMDD tend to have lower levels of estradiol, a form of estrogen, between ovulation and menstruation. But other studies have shown little to no difference in hormone levels. “There are no biomarkers. There’s no test that can be done which helps identify someone with PMDD,” says Lynsay Matthews, who researches PMDD at University of the West of Scotland.
Instead, to receive treatment, people experiencing premenstrual distress have to monitor their own mind and body. PMDD diagnosis is based on a symptom diary kept over the course of multiple menstrual cycles.
The symptoms recorded in those diaries can be severe. In a 2022 survey, 34 percent of people with PMDD reported a past suicide attempt. More than half reported self-harm. “If someone has suicidal ideation or self-harm, or suicide attempts every month for 30 years, that wouldn’t be described as a normal female response to the menstrual cycle,” Matthews says.
There is evidence that SSRIs work for people with PMDD, in ways researchers don’t fully understand. “In some cases, hours after taking an effective SSRI, people can feel a lot better,” Matthews says, referring to PMDD patients. In contrast, people with depression usually need to take SSRIs for weeks before feeling the effects. Researchers know the drugs’ mechanism of action is different for PMDD—they just don’t know why. “When people find that out, they find it quite validating that it is a medical condition,” Matthews says.
Tamara Kayali Browne, a bioethicist at Deakin University, in Australia, agrees that some people experience serious distress in the week before their period—but disagrees with calling it a mental illness.
“The crux of the problem seems to be that we are in a patriarchal society that treats women very differently and puts a lot of women under a lot of significant, disproportionate stress,” Browne says. That disproportionate stress begins early. Eighty-three percent of a sample of Australian PMDD patients reported trauma in early life. It continues in adulthood. A Swedish survey of 1,239 people with PMDD found that raising children was associated with higher rates of premenstrual distress.
Between ovulation and menstruation, many people experience higher physical and emotional sensitivity. They may feel unwilling or unable to deal with the stressors they tolerate the rest of the month: the screaming baby, the messy partner. “Is it the time of the month where the truth comes out?” Browne suggests. Seen in this light, irritability, anxiety, and low mood are understandable reactions to life stressors, not symptoms of mental illness.
There is a long history of doctors labeling women crazy. There is also a long history of doctors dismissing women’s pain. Debates about premenstrual distress are caught in the middle.
When critics question PMDD and the less severe premenstrual syndrome, it can feel invalidating. “It’s time to stop questioning whether women’s experiences are real and instead start making them real priorities,” the journalists Emily Crockett and Julia Belluz wrote in response to an article that suggested PMS is culturally constructed.
At the same time, when left unchecked, casual sexism can seep into the medical discourse around PMDD. Early pharmaceutical advertisements marketing SSRIs for PMDD show how this works in practice. In 2000, Eli Lilly packaged fluoxetine hydrochloride in a pink-and-purple capsule and branded it Sarafem. Advertisements for the drug featured incapable, unreasonable women; one fights a shopping cart, another bickers with her (male) partner. “Think it’s PMS? Think again. It could be PMDD.” (The Sarafem brand has since been discontinued.)
What if we can question the structural factors that make life harder for women while providing medical support for people who are suffering? Could the critiques lead us to more, not fewer, options for people with PMDD?
Medical interventions can be lifesaving for people with PMDD. But they don’t address a society that places a heavy burden on the shoulders of people assigned female at birth.
Browne compares severe premenstrual distress to a broken leg. “If you have a broken leg, you really do need painkillers, because you’re experiencing pain,” she says. “But it’s not going to be helpful in the long term if you don’t deal with whatever the underlying cause is.” In the week before menstruation, the life stressors a person with PMDD deals with the rest of the month can feel unbearable. Those life stressors can and should be addressed alongside conventional medical treatment.
One common stressor is the caregiving load. “Parenting is not only a massive trigger, but it’s also the biggest burden or the biggest guilt that comes with having PMDD,” Matthews says. “Not only are you struggling yourself every month, but you also feel as though you’re failing your children every month.” The co-parent can help alleviate this burden. When fathers spend more time with their kids—and doing child-related chores—mothers tend to be less stressed about parenting.
Another stressor is relationship difficulties. The emotional changes that come with the premenstrual phase can make conflict with a partner more likely. They can also prompt the PMDD sufferer’s partner to dismiss those feelings. “Nowadays, a partner might still be inclined to say, ‘Wait a minute, I know it’s that time of your month again. You’re just being oversensitive,’” Browne points out. Women in relationships with women, who tend to be more understanding of premenstrual change than men, report a more positive experience of the week before their period.
Researchers have done great, necessary work to understand PMDD, work that should continue. How are people who experience premenstrual distress biologically different from people who don’t? Can we find new, more effective drugs to treat that distress?
In the meantime, we need to build a better world for people who experience premenstrual distress. Doctors can prescribe medicine, but managers can make accommodations in the workplace. Co-parents can take on more caregiving responsibility. And partners can provide love and support.
Two years after the state legalized recreational marijuana use, setting foot on a New York City street any time of day or night means being assaulted by the depressingly familiar odor of marijuana smoke — and the same is true in many US cities.
There was a policy debate on marijuana legalization, and the legalization side won.
But caution and reasoned discourse have taken a back seat to a gold rush by big-money backers reminiscent of Big Tobacco, abetted by states looking for new sources of tax revenue.
Marijuana proponents like to remind us: “The science is settled.”
But is it?
A recently released study that links heavy marijuana (or cannabis) use to schizophrenia makes some wonder if we should have second thoughts about what exactly we are doing to ourselves.
The answer is yes, we should — and not based on just one study.
The cannabis and schizophrenia study is based on an analysis of almost 7 million Danish health records from 1972 to 2021.
Researchers found a statistical correlation between those who became heavy/compulsive users of cannabis (developing so-called cannabis-use disorder) and a subsequent schizophrenia diagnosis.
Since legalization in New York and other cities, the smell of marijuana is all over the streets.Getty Images/iStockphoto
In 30% of all schizophrenia diagnoses of men aged 21 to 30, the individual was a heavy pot user; of the full sample, ages 16 to 49, the correlation was 15%…
This article was featured in One Story to Read Today, a newsletter in which our editors recommend a single must-read from The Atlantic, Monday through Friday. Sign up for it here.
On the night of June 17, 1998, a Cornell campus police officer named Ellen Brewer had just begun her shift when she noticed a tall, silhouetted figure moving slowly across the engineering quad. The man appeared to be dressed all in black. Brewer felt a whisper of danger. She slowed her car, and the shrouded figure began loping toward her. He raised a hand and hailed her as if she were a taxi driver. As he drew closer, she thought he must have been the victim of an assault, perhaps in need of medical assistance.
Explore the May 2023 Issue
Check out more from this issue and find your next story to read.
Suddenly, as if in a single stride, the man was at her window. He lowered his face, shiny with sweat, close to hers. He was muttering incoherently; his rust-colored beard and hair were wildly matted. He seemed to be saying that he might have killed someone, his girlfriend or perhaps a windup doll. Brewer radioed in the strange encounter, requested backup, and got out of her car.
She thought again that the disoriented man, whose clothes were bloody, had been attacked or maybe had fallen into one of the steep gorges that famously intersect the campus, but when she tried to steer him out of the road, he leaped back, a large hand clenched into a fist.
The police station was all of 100 yards away, on Campus Road, and officers were already coming toward them, some on foot, others in cars. They escorted the man, whose name was Michael Laudor, to Barton Hall, the looming stone fortress that the campus police shared with the athletics department.
Once inside, Michael didn’t need much prodding to answer questions, but whenever he mentioned possibly harming his girlfriend, whom he sometimes referred to as his fiancée, he added, “or a windup doll.”
When Sergeant Philip Mospan, the officer in charge that night, asked Michael if he was hurt, he received a simple no. In that case, “where did the blood all over your person come from?” Michael told him it was Caroline’s blood.
“Who is Caroline?” the sergeant asked.
“She’s my girlfriend,” Michael said. “I hurt her. I think I killed her.”
Was Michael sure about that?
He thought so, but asked, “Can we check on her?”
His concern seemed urgent and genuine, though puzzlingly he said this had happened in Hastings-on-Hudson, New York, 220 miles away.
Mospan prefaced his request to the Hastings-on-Hudson dispatcher by saying, “This may sound off the wall …” Because who kills someone in Westchester County, drives to Binghamton, and takes a bus to Ithaca, as Michael said he had done, only to surrender to campus police? The dispatcher asked him to wait a moment, and then a detective came on the line. “Hold him!” the detective said. “He did just what he said he did.” They had people at the apartment. The woman was dead, the scene ghastly.
And so it was that my best friend from childhood, who had grown up on the same street as me; gone to the same sleepaway camp, the same schools, the same college; competed for the same prizes and dreamed the same dream of becoming a writer, was arrested for murdering the person he loved most in the world.
When police officers from Hastings-on-Hudson showed up the next morning to bring Michael back there, they were surprised to find reporters, photographers, and TV cameras waiting outside the Ithaca jail. Jeanine Pirro, then the Westchester district attorney, who charged Michael with second-degree murder, would call him “the most famous schizophrenic in America,” a perverse designation, though strangely in tune with the aura of specialness that had characterized so much of his life, and that had shaped the expectations we’d grown up with. Michael was famous for brilliance. He’d gone to Yale Law School after developing schizophrenia, and was called a genius in The New York Times, which led to book and movie deals. Brad Pitt was attached to star.
Michael’s friends and family and his supporters at Yale had thought intelligence could save him, allow him to transcend the terrible disease that was causing his mind to detach from reality. Michael was arrested on a campus where he’d spent six happy weeks at an elite program for high-school kids in the summer of 1980, when we were 16. I sometimes wondered if he was trying to get back to a time when his mind was his friend and not his enemy, but a forensic psychiatrist who examined Michael for the prosecution set me straight: Michael thought his fiancée was a “nonhuman impostor” bent on his torture and death, and in his terrified delusional state, he had fled hours to Cornell hoping to evade destruction and call the police. In other words, he was seeking asylum.
Asylum was also what Michael needed in the months before he killed Carrie. Not “an asylum” in the defunct manner of the vast compounds whose ruins still dot the American landscape like collapsing Scottish castles, but a respite from tormenting delusions—that his fiancée was an alien, that his medication was poison. Because he was very sick but did not always know it, Michael had refused the psychiatric care that his family and friends desperately wanted for him but could not require him to get.
Michael needed a version of what New York City Mayor Eric Adams called for in November, when announcing an initiative to assess homeless individuals so incapacitated by severe mental illness that they cannot recognize their own impairment or meet basic survival needs—even if that means bringing them to a hospital for evaluation against their will. “For too long,” Adams proclaimed, “there’s been a gray area where policy, law, and accountability have not been clear, and this has allowed people in need to slip through the cracks. This culture of uncertainty has led to untold suffering and deep frustration. It cannot continue.”
Though 89 percent of recently surveyed New York City residents favored “making it easier to admit those who are dangerous to the public, or themselves, to mental-health facilities,” attacks on the mayor’s modest adjustments to city policy began immediately. News stories suggested that a great roundup of mentally ill homeless people was in the offing. “Just because someone smells, because they haven’t had a shower for weeks,” Norman Siegel, a former head of the New York Civil Liberties Union, told the Times, “because they’re mumbling, because their clothes are disheveled, that doesn’t mean they’re a danger to themselves or others.”
Never mind that these were not the criteria outlined in the Adams plan. Paul Appelbaum, the director of the Division of Law, Ethics, and Psychiatry at Columbia, says that the government has an interest in protecting people who are unable to meet their basic needs, and that he believes the mayor’s proposal has been largely misunderstood. “There’s an intrinsic humanitarian imperative not to stand by idly while these people waste away,” Appelbaum recently told Psychiatric News.
The people Adams is trying to help have been failed by the same legal and psychiatric systems that failed Michael. They all came of age amid the wreckage of deinstitutionalization, a movement born out of a belief in the 1950s and ’60s that new medication along with outpatient care could empty the sprawling state hospitals. Built in the 19th century to provide asylum and “moral care” to people chained in basements or abandoned to life on the streets, these monuments of civic pride had deteriorated over time, becoming overcrowded and understaffed “snake pits,” where patients were neglected and sometimes abused. Walter Freeman, notorious for the ice-pick lobotomy (which is exactly what it sounds like), was so horrified by the naked patients crammed into state hospitals, shockingly featured in a famous 1946 Life article, that he developed a new slogan: “Lobotomy gets them home.”
But getting people home was never going to be a one-step process. This would have been true even if the first antipsychotic medications, developed in the ’50s, had proved to be a pharmaceutical panacea. And it would have been true even if the neighborhood mental-health clinics that psychiatrists had promised could replace state hospitals had been adequately funded. During the revolutions of the ’60s, institutions were easier to tear down than to reform, and the idea of asylum for the most afflicted got lost along with the idea that severe psychiatric disorders are biological conditions requiring medical care. For many psychiatrists of the era, mental illness was caused by environmental disturbances that could be repaired by treating society itself as the patient.
The questions that should have been asked in the ’60s, and that might have saved Michael and Carrie, are relevant to Mayor Adams’s policies now: Will there be follow-up care, protocols for complying with treatment, housing options with supportive services and a way to fund them? Will there be psychiatrists and hospital beds for those who need them? But it would be ironic if all of the past failures at the federal, state, and local levels became an argument against making a first small step toward repair.
Michael Laudor and his fiancée, Caroline Costello, in a photo found by the police in their apartment in Hastings-on-Hudson (Photographer unknown; Tolga Tezcan / Getty)
If I had known Michael only as he appeared grimly on the front pages of the tabloids 25 years ago, or Caroline Costello as half of a smiling picture all the more tragic for being so full of innocence and hope, I would not have understood how much is at stake in the current efforts to improve the care given to people with severe mental illness. Neither Adams’s policies—nor the more comprehensive measures advanced by Governor Gavin Newsom, in California—will bring about a sweeping transformation; only incremental changes, and many accompanying efforts at all levels of government, will make a difference. And these will not be possible without a shift in the way people think about the problem.
Now when I think about the frenzied moments before Michael killed Carrie, when violence was imminent and intervention was necessary but impossible, I understand that it isn’t on the brink of crisis but earlier that something can be done—though only by a culture that is capable of making difficult choices and devoting the resources to implement them.
But I knew Michael before he thought Nazis were gunning for him. I knew him before the lurid headlines, the Hollywood deal, the publishing contract, and the New York Times profile that proclaimed him a genius. I knew him as a 10-year-old boy, when I was also 10 and he was my best friend.
The Cuckoo’s Nest
I met Michael as I was examining a heap of junk that the previous owners of the house we had just moved into in New Rochelle had left in a neat pile at the edge of our lawn. It was 1973. A boy with shaggy red-brown hair and large, tinted aviator glasses walked over to welcome me to the neighborhood. He was tall and gawky but with a lilting stride that was oddly purposeful for a kid our age, as if he actually had someplace to go.
His habit of launching himself up and forward with every step, gathering height to achieve distance, was so distinctive that it earned him the nickname “Toes.” He was also called “Big,” which is less imaginative than “Toes,” but how many kids get two nicknames? And Michael was big. Not big like our classmate Hal, who appeared to be attending fifth grade on the GI Bill, but big through some subtle combination of height, intelligence, posture, and willpower.
Even standing still, he would rock forward and rise up on the balls of his feet, trying to meet his growth spurt halfway. He stood beside me on Mereland Road in that unsteady but self‑assured posture, rising and falling like a wave. He was socially effective in the same way he was good at basketball—through uncowed persistence. I often heard in later years that people found him intimidating, but for me it was the opposite. Despite my shyness—or because of it—Michael’s self‑confidence put me at ease. I fed off his belief in himself.
Was Michael bouncing a basketball the day I met him? He often had one with him, the way you might take a dog out for a walk. I’d hear the ball halfway down the block, knocking before he knocked.
Even today, when I hear the taut report of a basketball on an empty street, the muffled echo thrown back a split second later like the after-pulse of a heartbeat, I have a visceral memory of Michael coming to fetch me for one‑on‑one or H‑O‑R‑S‑E, or simply to shoot around if we were too deep in conversation for a game or if I was tired of losing.
Michael might just as easily have had a book the day he introduced himself. He often had several tucked under one arm, and he would dump them unceremoniously at the base of the schoolyard basketball hoop. It was always an eclectic pile: Ray Bradbury, Hermann Hesse, Zane Grey Westerns, books his father assigned him—To Kill a Mockingbird or a prose translation of Beowulf—stirred in with the Dune trilogy and Doc Savage adventures.
Our fathers were both college professors, but Michael’s father, who taught economics, sported a leather bomber jacket and spoke in a booming Brooklyn manner. My father, who taught German literature, wore tweed jackets from Brooks Brothers, spoke with a soft Viennese accent, and named me and my sister for his parents, who had been murdered by the Nazis.
Michael had all four grandparents, something I’d seen only in Charlie and the Chocolate Factory. They did not all sleep in one bed, like Charlie’s grandparents, but he saw a lot of them. His Russian-born grandparents still lived in Brighton Beach, Brooklyn, where his father had grown up and his grandmother Frieda had stuffed money into a hole in the bathroom wall until a plumber came and stole it one day. Michael recounted stories about “crazy” Frieda with such amused affection that it was a shock when he told me, years later, that she had schizophrenia.
Every weekday morning during the school year, I’d walk to the bottom of our one‑block street, ring Michael’s bell, and wait for him to step groggily out from the household chaos. We’d hike up the hidden steps behind his house that led to the basketball court, climb a second flight of outdoor stairs, and slip into the school through a side door that felt like a private entrance.
Thanks to Michael, I became a big fan of Doc Savage, originally published in pulp-fiction magazines in the 1930s but reissued as cheap paperbacks starting in the ’60s. We joked about the archaic language and dated futurisms—long‑distance phone calls!—but Doc Savage, charged with righteous adrenaline, formed an important part of the archive of manly virtues that I received secondhand from Michael, who got them wholesale from his father, his grandfathers, old movies, and assorted dime novels.
Like Doc Savage, Michael had a photographic memory. He also read at breakneck speed. I was a fast talker but a slow reader; Michael burned through the assigned reading with such robotic swiftness that he was allowed to read whatever he wanted to, even during regular class time.
He kept stacks of paperbacks on his desk at school, working his way through fresh piles every day. He didn’t just read the books; he read them all at the same time, like Bobby Fischer playing chess with multiple opponents. After a few chapters of one, he’d reach for another and read for a while before grabbing a third without losing focus, as if they all contained pieces of a single, connected story.
I was a direct beneficiary of all that reading. He seemed to have almost as much of a compulsion to tell me about the books as he did to read them, and I acquired a phantom bookshelf entirely populated by twice-told tales I heard while we were shooting baskets, going for pizza, or walking around the neighborhood.
Left: Michael Laudor at the author’s house in New Rochelle, New York, 1976. Right: Farm Camp Lowy , in Windsor, New York, summer 1977. The author is second from the left in the second row, in a Yankees T-shirt; Michael sits two seats to his left, looking upward in a dark T-shirt. (Courtesy of Jonathan Rosen; Studiocasper / Getty; Petekarici / Getty)
Michael’s precocity made him seem like someone who had lived a full life span already and was just slumming it in childhood, or living backwards like Benjamin Button or Merlyn. My parents were amused by the speed with which he took to calling them Bob and Norma, and the ease with which he held forth on politics while I waited for him to finish so we could play Mille Bornes or go outside. I knew that the president was a crook—but Michael knew who Liddy, Haldeman, and Ehrlichman were and what they had done, matters he expounded as if Deep Throat had whispered to him personally in the schoolyard.
Michael also saw more R-rated movies than I did. In 1976, One Flew Over the Cuckoo’s Nest, which was about a sane wiseass named Randle McMurphy locked in a mental hospital by a crazy culture, won the Academy Award for Best Picture. Michael explained that the hospital tries drugging McMurphy into submission and shocking his brain until his body writhes, then finishes him off with a lobotomy, all because he won’t behave.
I’d never heard of a lobotomy, but Michael assured me it was real; they stuck an ice pick in your head and wiggled it until you went slack like a pithed frog, docile enough to be dissected alive. This was a far cry from the “delicate brain operation” that Doc Savage performed on criminals to make them good so they would not have to rot in prison.
The lobotomy in Cuckoo’s Nest reduces McMurphy to zombie helplessness. His friend Chief Bromden smothers him to death with a pillow and escapes out a window so the other inmates will still have a hero to believe in. Like a lot of things in the ’70s, the movie sent a mixed message, exposing the abuses of psychiatric hospitals while justifying the killing of a mentally impaired person.
The summer before college, I found myself filled with optimism. I’d always been the tortoise to Michael’s hare, but we both got into Yale, and for the ninth year in a row we would be going to the same school. I was surprised when Michael told me one afternoon, as we lounged on my parents’ patio, that he did not think we would see much of each other at Yale. When I asked him why, he told me that I was simply too slow.
We did see less of each other in college, but when I’d run into Michael on Metro-North, heading home for vacation, we’d talk in the old way, nonstop until New Rochelle.
Impatient as always, Michael decided to graduate in three years. He also informed me that he had decided to become rich, as if that were something you could declare like a major. He had been recruited by a Boston-based management consulting firm called Bain & Company, a place, he explained, where the supersmart became the superrich.
He was ironic about his choice to join the ranks of the young, upwardly mobile philistines the media had taken to calling yuppies, but wanted me to know that he was not abandoning intellectual or artistic aspirations: His plan was to spend a decade making gold bricks for Pharaoh, after which he would buy his freedom and become a writer.
I lost track of Michael during his time at Bain, though once or twice I’d hear my name on Mereland Road while home for a visit. Turning, I’d see him loping up the hill, grinning as if we were still fifth graders and his fancy trench coat was a costume.
But I learned later that he was having a rough time. The pressure at Bain was constant. Michael began complaining that his heart raced, his digestion was bad, and Machiavellian higher‑ups were “out to get him” but would never let him go because of his value to the firm, which seemed unlikely even for a place known as “the KGB of the consulting world.” He quit Bain in 1985 and began writing in earnest—the 10-year plan had become a one-year plan. Even after he quit, Michael thought his phone was being tapped and Bainies were spying on him.
Still, his life sounded like the fulfillment of a dream. He was living in the attic of a grand house with a private beach at the south end of New Rochelle owned by the parents of a friend. The mansion might have drifted north and west from the gilded north shore of Long Island. Michael called it “the Gatsby House” and claimed that he could see a green light glinting far out on the water as he stayed up late, writing stories and staring into the night. He wanted to be Fitzgerald and Gatsby both, the dreamer and the dream. Didn’t we all?
The friend’s parents happened to be Andy and Jane Ferber, community psychiatrists who had dedicated their life to liberating people with severe mental illness from state institutions. The Ferbers were at the center of an overlapping collection of friends and colleagues who referred to themselves as “the Network,” drawn together by their experience in community psychiatry and a sincere desire to leave the world better than they’d found it.
They’d been inspired by the Scottish psychiatrist R. D. Laing, who called insanity “a perfectly rational adjustment to an insane world,” and books such as Asylums, Erving Goffman’s 1961 landmark study that focused on the impact psychiatric institutions had on the behavior and personality of patients rather than on the illnesses that sent them there. A sociologist, Goffman frequently put the term mental illness in quotation marks, though he abandoned the practice in later writing, after his wife’s suicide.
Most of the Network had met in the ’60s, when President John F. Kennedy had vowed to replace the “cold mercy of custodial isolation” with the “open warmth of community concern.” The Community Mental Health Act of 1963, which Kennedy signed on October 31 of that year, promised that an “emphasis on prevention, treatment, and rehabilitation will be substituted for a desultory interest in confining patients in an institution to wither away.” It was the institution’s turn to wither away, replaced by the sort of communal care offered by the center that Jane Ferber had run in downtown New Rochelle, with its workshops, visits to patients in board-and-care facilities, and drop-in services.
One problem was that nobody knew how to prevent severe mental illness; another was that rehabilitation was not always possible, and could only follow treatment, which was easily rejected. And despite having been created to replace hospitals caring for the most intractably ill, community mental-health centers, as their name suggested, aimed to treat the whole of society, a broad mandate that favored a population with needs that could be addressed during drop-ins. “It wasn’t that we weren’t interested in dealing with difficult cases,” writes the psychologist Roger B. Burt, looking back at the community center he ran in Baltimore in the late ’60s, but that he and his idealistic colleagues feared that “to blindly accept ‘dumping’ [of severely ill patients from the old asylums] would have bled the staff of time and taken services away from people who would benefit from it.” The only recourse for families caring for severely ill relatives in acute distress was to call the police, who would arrest them.
The police didn’t like this, and who can blame them? They did not sign up to be caretakers of people suffering psychotic episodes. Meanwhile, the most vulnerable members of the community were being criminalized.
The Network’s values were well expressed in Crisis: A Handbook for Systemic Intervention, which Jane Ferber and a colleague had published in the late ’70s, written for mental-health professionals who “feel in some way oppressed by the existence of mental hospitals, jails, reform schools, hierarchical corporations or governments of covert nepotism.”
One of the manual’s case histories described an elderly woman with “regressive psychosis” who had been wandering the halls of her Upper West Side boardinghouse naked. Members of Jane’s team were called in to help get the woman into a nursing home; instead, they coached her on “how to avoid being committed.” They gave her tips like “wear your clothes at all times” and “evacuate in the toilet instead of the floor,” and they reminded her to smile at the nurses “no matter what.”
Keeping people out of the hospital was the hospitals’ policy too, even if it had more to do with legal constraints and available beds than faith in community care. Around the time that Michael moved into the Gatsby house, there were newspaper stories about a woman with schizophrenia named Joyce Brown who had been hospitalized against her will as part of a new program to prevent people from dying on the streets, a sort of precursor to Mayor Adams’s initiative. The program included a broader interpretation of commitment laws and promised appropriate housing upon discharge.
Brown slept on a sidewalk grate; ran into traffic; defecated on herself; screamed racial epithets at Black men (though she was Black herself); and tore up dollar bills, set them on fire, and urinated on them. But a judge ordered her released. He agreed with her lawyers at the New York Civil Liberties Union, headed by Norman Siegel at the time, and said that her behavior was the result of homelessness rather than its cause. Though burning money “may not satisfy a society increasingly oriented to profit‑making and bottom‑line pragmatism,” the judge wrote, Brown’s behavior was “consistent with the independence and pride she vehemently insists on asserting.”
Her sisters, who had struggled to care for Brown in their homes before psychosis, drug abuse, and violent behavior had made it impossible, came to a different conclusion. If the judge believed that a Black woman shrieking obscenities and lifting her skirt to show passersby her naked buttocks was living a life of “independence and pride,” they said after the ruling, he must be a racist who thought such degradation was “good enough for her, not for him or his kind.” If that were his sister on the street, they had no doubt, he “would not stand for it.”
Daniel Patrick Moynihan, who had served on President Kennedy’s mental-health task force as a young assistant secretary of labor, had helped draft the report that led to the Community Mental Health Act. Years later, as a U.S. senator representing New York, he looked back with deep regret. In a 1989 letter to the Times, written in a city “filled with homeless, deranged people,” he wondered what would have happened if someone had told Kennedy, “Before you sign the bill you should know that we are not going to build anything like the number of community centers we will need. One in five in New York City. The hospitals will empty out, but there will be no place for the patients to be cared for in their communities.” If the president had known, Moynihan wrote, “would he not have put down his pen?”
The Locked Ward
While I was studying English literature in graduate school at UC Berkeley, and learning from Foucault that mental illness is a “social construct” invented to imprison enemies of the state, Michael was being hounded by Nazis in New Rochelle. Even if they were imaginary, they ran him off the road when he was driving and tried to run him down when he was walking. Characters from a thriller he was writing stalked him. Even after he burned the novel, he brought a baseball bat into bed with him.
Jane found Michael a psychiatrist from the Network whose intellectual manner appealed to him. He went home to his parents’ house but remained a part of the Network’s extended family.
One cold winter morning before work in 1987, my father saw him in the flapping remnant of his fancy trench coat, walking distractedly up Mereland Road like someone with no place to go in a hurry. My father was waiting outside for his ride to the train station. The closer Michael got, the worse he looked, and my father asked him what was wrong.
I haven’t been well, Michael told him, uncharacteristically laconic. My father was deeply affected by Michael’s drawn and distracted features, his almost palpable aura of affliction. My father wanted to stay and talk more, but his ride arrived. He got in the car with the feeling that he was abandoning someone in crisis.
A few days later, my parents called me. They sounded so grave and strange that I thought my grandmother must have died, but my father said they were calling about Michael Laudor. The formal use of his full name was an acknowledgment of how far apart we’d drifted and a portent of bad news: Michael was in the psychiatric unit of Columbia-Presbyterian.
My mother told me that Michael thought his parents were Nazis, and that he’d been patrolling his house with a kitchen knife. Ruth had been unable to convince Michael that she was his mother and not a Nazi, so she’d locked herself in her bedroom and called the police.
As soon as I got off the phone, I called the Laudors. I still knew the number by heart, though it had been years since I’d dialed it. Michael’s father, Chuck, encouraged me to call Michael, who was up on 168th Street in a locked ward. This was the first time I’d heard that terrible phrase. No phones in the rooms, just a payphone in the corridor.
Sometimes, Chuck said, the doctors gave Michael special drugs, and if he was “tuned in,” he would talk. The notion affected me almost as much as “locked ward.” The idea that someone so verbal needed to be “tuned in” was hard to imagine.
I dialed the number Chuck gave me, and Michael answered in a groggy voice, as if he’d been waiting by the payphone and fallen asleep. I was afraid he wouldn’t recognize me or want to talk—I’d been afraid he wouldn’t be able to talk—but he knew me right away and sounded pleased, in a weary way, that I was on the phone.
His voice was leaden and far off, but I felt the muffled intensity of his familiar presence. “I’ve never been in prison before,” he said ruefully when I asked how he was doing. The “day room” was full of noise and cigarette smoke, the TV on all the time. “I don’t like smoky rooms with televisions,” he told me, “but they say if you want to leave, you have to go there and interact.”
It sounded bleak. Was there nothing else to do?
“Eight a.m. breakfast. Twelve p.m. lunch. Five p.m. dinner.”
It was only after I’d laughed that I realized this might not be deadpan humor, just deadpan delivery. Disconcertingly, I wasn’t sure. Michael hadn’t lost his old way of saying things, and I was still listening with ingrained expectations. Could he still be ironic? Could he still tell a joke?
I wanted to apologize for laughing, but didn’t. I felt Michael’s need to talk, to tell me things more than to converse. He was “tuned in,” as Chuck put it, though to a different frequency from the one I was used to.
“Dr. Ferber says I have a delicate brain,” he told me with a hint of pride that only enhanced the pathos of his abject situation.
I’d called half-hoping that Michael wouldn’t come to the phone, but I heard myself asking if he wanted a visitor. He was eager for one. We agreed that I’d visit on the coming Tuesday. I gave him my phone number in Manhattan and had to repeat each number very slowly.
“It’s hard to work the pen right now,” he said.
A taciturn attendant with keys on a ring like a jailer’s in a movie unlocked the heavy door of Michael’s ward. The door had a small, thick window at eye level. The attendant locked the door behind us, and I felt a clinch of claustrophobia. Locked ward was not a metaphor.
I followed the attendant. Michael was sitting rigidly on his bed, trancelike. His parents, in chairs near the bed, leaped up when I came in. Ruth hugged me hard and Chuck shook my hand. After they left the room to give us a chance to talk, Michael seemed marginally more relaxed, but he was apparently past thinking they were Nazis. He shifted uncomfortably on the bed, an occasional tremor running through his body.
At this point, no one had yet named Michael’s illness for me, saying only that he’d had “a break.” Michael referred to himself as paranoid, but who isn’t? The doctors were giving him drugs, he told me, but not much beyond that. He felt like a television set with bad reception; nobody knew what to do except move the antenna around and bang on one side and then the other, hoping the picture would improve.
Before he wound up in the hospital, he had applied to the top seven law schools in the country. They’d all accepted him, though by then he was in no condition to do anything about it, so he’d asked his brother to reject all of them except Yale, which he deferred for a year.
It was, in a way, a typical Michael story: He had rejected the law schools, not the other way around.
Michael said it was easier to walk than to sit, so we went out into the corridor and walked up and down together. He carried himself with effortful stillness, cautiously erect. At one point he led me to a barred window that looked out over fire escapes, water towers, the windowless back ends of buildings exposed by demolition, things not meant to be seen.
“Look what’s become of me,” he said pitiably, as if he were the view.
Michael volunteered that he could leave whenever he wanted to, because he had—at his father’s urgent insistence—signed himself in. This surprised me, not only because he hated being there but also because of the dramatic story I’d heard about his arrival.
It would not have occurred to me that someone marching around with a kitchen knife might not be considered a danger to himself or others. Michael had carried the knife, and slept with the baseball bat, because he’d thought his parents had been replaced by surgically altered Nazis who had murdered them and wanted to kill him. His psychiatrist considered that defensive, not aggressive, behavior.
The doctors at Columbia-Presbyterian believed he ought to be there. The longer they could keep him, the more time he would have to receive treatment and to heal, a process much slower than the temporary abatement of florid symptoms that medication provided. He was persuaded to stay, or was at least afraid to leave.
Visiting Michael, I found it impossible to pretend that he was suffering from a “social construct.” I disliked the hospital, but even with its heavy locked door, I knew it wasn’t a branch of the “carceral state” devised by a power‑mad society to torment him.
Michael spent eight months in the locked ward at Columbia-Presbyterian, which, he murmured guiltily, cost even more than Yale. His long stay gave his doctors time to find the least incapacitating dose of the powerful drugs that were supposed to have eliminated mental hospitals years before.
Michael’s medication was calibrated carefully enough that he was no longer convinced Josef Mengele was preparing to remove his brain without anesthesia. He had his suspicions, but, as he later said, he’d stopped trying to bash his skull against the sink in a preemptive effort to destroy his own brain. Now when hallucinations came calling, Michael could often recognize them for what they were and “change the channel,” as he put it.
Michael left the hospital to live among the ruins of multiple systems. He would have to continue taking antipsychotic medication, though 15 percent of people with schizophrenia were “treatment resistant,” according to the psychiatrist E. Fuller Torrey, the author of the 1983 book Surviving Schizophrenia: A Family Manual. “Treatment resistant” referred to patients who weren’t helped by medication, not those who resisted taking it. That percentage was much higher than 15 percent, in part because the conviction that you weren’t sick was often an aspect of the illness, especially at times of acute psychosis.
Before Michael’s psychotic break tipped the balance one way, and medication tipped it back the other, he had seemed to both know and not know what was happening to him—a state strangely mirrored by those around him, who had also recognized and ignored his illness by turns. I’d experienced for myself how rational his reasoning manner made unreasonable things appear. Ruth and Chuck had helped Michael install debugging devices on his phone, and by the time they realized that they’d been played by his delusions, he’d reclassified them as double agents.
I felt sadness when I saw Michael struggling through an intermediate existence after he got out of the hospital. His slowed speech, stiff formality, and dark suit, a hand‑me‑down from his former self, made me think of an undertaker in an old movie. I also felt sympathy, aversion, affection, and fear in unfamiliar and shifting combinations. When I saw him on Mereland, his collar was half up and half down. I wanted to smooth it down for him, or lift up the other side, but did neither.
Halfway
Michael moved into a halfway house in White Plains called Futura House. Suburbs didn’t like halfway houses or group homes, and New York suburbs had been very successful at excluding them. Michael’s mother said he was lucky to get into one, given how many fewer spaces there were than people seeking them.
The real trouble with halfway houses was that they were short‑term solutions for people with long‑term needs. Residents might do everything expected of them, take their medication, and follow all the rules, and still not be ready to move on after the one‑ or two‑year limit.
Supportive housing that combined psychiatric and social services with affordable lodging hardly existed at the time. People might shuttle between transitional housing, a family home, a hospital, a board‑and‑care facility, the home of a different relative, followed by another hospital, though never for long. Federal benefits excluded state hospitals, creating an incentive for states to offload costly patients. The process would start again, but never moving in a straight line as it followed the course of an illness that waxed and waned, and responded better or worse to medication at different times. The disability checks Michael received, and the Medicaid payments he was eligible for, did not create a community, let alone a caring one. Checks and pills were what remained of a grand promise, the ingredients of a mental-health-care system that had never been baked but were handed out like flour and yeast in separate packets to starving people.
Most of Michael’s disability check went straight to the halfway house. He was poor, he said, and not in a temporary or bohemian way.
As part of its congressional testimony in the 1980s about the crisis in care for people with schizophrenia, the National Institute of Mental Health prepared a chart showing that only 17 percent of adults with schizophrenia were getting outpatient care; 6 percent were living in state hospitals, 5 percent in nursing homes, and 14 percent in short‑term inpatient facilities. That left a full 58 percent of the schizophrenic population unaccounted for. Would Michael end up among the lost population?
Michael didn’t like Futura House, but he still heard its loud clock ticking. Every few months, he had a “resident review,” where counselors talked about a “life plan” and “vocational readiness.” (Futura House and the day program at St. Vincent’s Hospital had relationships with local businesses.) The counselors emphasized small steps, low stress, and a noncompetitive environment. Not necessarily forever, but definitely for now. One possibility, endorsed by the psychiatrists at the hospital, was for Michael to work as a cashier at Macy’s, a suggestion that fell like a hammer blow of humiliation.
Michael told the story of his father taking him to Macy’s, where they watched beleaguered clerks get pushed around by impatient customers, as an epiphanic moment. The verdict was clear: Yale Law School would be a lot less stressful.
Prometheus at Yale
For the network watching over Michael, choosing Yale Law School was a no-brainer. He might be suffering from a thought disorder, but his brilliance would save him. Michael agreed: “I may be crazy,” he liked to say, “but I’m not stupid.” It was hard to believe that Michael could go straight from a program of slow steps and daily skills, like using a checkbook and planning a meal, to the top-ranked law school in the country. But if you agreed that Macy’s would destroy him, it followed that Yale would set him free. I believed this. Michael’s parents believed this. So did the law school’s dean, Guido Calabresi, and the professors who became Michael’s mentors.
Michael was as quick to tell his professors about his schizophrenia as he was determined to keep it from his classmates. He made it clear that he didn’t want sympathy or special consideration, and his professors, who understood that he was asking for both, were deeply affected by his intelligence and vulnerability.
He told them how he awoke each morning to find his room on fire, lying in fear until his father called to convince him that the flames weren’t real. “Does it burn?” his father asked after telling him to put out a hand. “Does it burn? No? Good!” Then he ordered Michael to do the same with his other hand. “Is it hot? Does it burn? Does it burn?” Little by little, until Michael was standing upright on the burning floor.
His professors all heard the story of the burning room and repeated it to one another as a parable of his struggle and strength. He was like Prometheus having his liver eaten by an eagle every morning, growing it back every night in time to be tortured again at dawn.
Michael, photographed for The New York Times at Yale Law School, October 25, 1995. The image the Times conveyed, in this photo and in the article that it accompanied, belied the depth of Michael’s continuing struggles. (Jim Estrin / The New York Times / Redux; T_Kimura / Getty)
It was a feature of Michael’s confessional style that his account of disabling mental illness communicated extraordinary mental ability, so that even after his professors realized he could not do the work, their sense of his brilliance remained. As one of his mentors later explained, many of the law school’s real success stories didn’t become lawyers at all. He thought Michael could be an eloquent advocate for people with schizophrenia, someone who had been to Yale Law School rather than someone who was a Yale lawyer.
But Yale lawyer was a phrase Michael already applied to himself. Recalling his struggle with the day-program doctors, Michael would say: “Why would I bag groceries when I could be a Yale lawyer?” Becoming a Yale lawyer was the whole point.
The Laws of Madness
Michael and Carrie had overlapped as undergraduates but began dating when Michael was in law school and Carrie, a literature major with a knack for computers, was living in New Haven and working for IBM. The mutual friend who brought them together loved and admired them both, but had doubts about them becoming a couple. He had lived with Michael his first summer during law school and remembered asking his roommate through a locked door if he wanted to come out for dinner, only to learn that Michael feared that he would be on the menu.
Michael waited months before telling Carrie he had schizophrenia; if she suspected something before that, she didn’t say. She wouldn’t have been the first person to not notice, or to ascribe symptoms such as surface tremors and apocalyptic utterances to the hidden depths of a complex soul.
Carrie wept when Michael told her. She did not reproach him for having kept his illness a secret. She showed no anger or fear or regret, only pain for his pain. She wept at the unfairness of what he had suffered in the past and was still suffering. She knew it was a terrible illness, but she loved him, and that was that.
Michael’s dream was to be a professor at Yale. He reported proudly that the law school had created a postgraduate fellowship just for him, in recognition of his genius. But there remained a certain gap between his ambitions and his mentors’ hopes for him. “I have thought to myself from time to time,” one of Michael’s professors told me: “Gee, if I hadn’t been so busy being proud of what a great place the Yale Law School was to have admitted Michael Laudor, I might have paid closer attention to him.”
When Michael began applying for teaching jobs, he was unable to explain in interviews why he had never clerked for a judge or worked at a law firm beyond a single summer that had not gone well. Advised to avoid any mention of schizophrenia—a “career killer”—Michael said that such work lacked the intellectual stimulation he required. He got no offers at all, a bitter setback.
But in the fall of 1995, while Michael was still mourning his father, who had died of cancer, something happened that changed his fortunes almost overnight. On November 9, The New York Times ran an article called “A Voyage to Bedlam and Part Way Back.” A second headline modified the first: “Yale Law Graduate, a Schizophrenic, Is Encumbered by an Invisible Wheelchair.”
The reporter, Lisa W. Foderaro, offered a sort of alternative résumé: “Mr. Laudor, 32 and by all accounts a genius, is a schizophrenic who emerged from eight months in a psychiatric unit at Columbia‑Presbyterian Medical Center to go to Yale Law School.” The story centered on Michael’s newfound determination to find a job as a law-school professor without denying or disguising his schizophrenia.
When Michael came out of the closet, he came out all the way. “Dubbing himself a ‘flaming schizophrenic,’ ” Foderaro wrote, “Mr. Laudor said that his decision to make his illness public and work closely with others with mental disabilities was a political and religious one.”
It was a glowing profile that captured Michael’s wry sense of humor (“I went to the most supportive mental health care facility that exists in America: the Yale Law School”) as well as his knack for harrowing formulations: “My reality was that at any moment, they”—the Nazi doctors—“would surgically cut me to death without any anesthesia.” He recalled the pain of his hospitalization with touching frankness: “I spent my 26th birthday there crying on my bed.”
He poured his private life onto the pages of the Times, confiding even his experience of the interview with liberated eloquence: “I feel that I’m pawing through walls of cotton and gauze when I talk to you now,” Michael told Foderaro. “I’m using 60 or 70 percent of my effort just to maintain the proper reality contact with the world.”
Brilliance was the fulcrum of the story, the point at which Michael was lifted above the stereotypes of schizophrenia, much as intelligence had elevated him above ordinary expectations before he got sick. “Far from knowing that Mr. Laudor had a severe mental illness,” Foderaro wrote, “the other students were somewhat in awe.”
The article threw into stark relief the indignities of interviewing for jobs. “One interviewer asked if he was violent,” Foderaro wrote, “which Mr. Laudor said reflected a common and painful stereotype.” I understood Michael’s indignation, but I also knew that before he was medicated, Michael had armed himself with a knife in fear of his impostor parents. I wished the article had addressed the question even a little instead of leaving it to Michael to dismiss in a way that made you feel as if even to ask was an insult.
One of the things that haunted me about Michael’s breakdown was how frightened his parents had been. Without a father capable of bluffing and threatening Michael into signing himself in for his own good, he might not have gotten those eight months of care he’d so desperately needed.
Michael sounded exhilarated and slightly manic when we talked on the phone that winter. Book editors were in a bidding war for a memoir Michael was going to write, called The Laws of Madness, which was also going to be a Ron Howard movie. The deals would net him more than $2 million.
Like the Times profile, his 80‑page book proposal caused an electric stir. How often did anyone narrate schizophrenia from the inside out? Michael described what it had felt like to discover that his parents were evil imitations of themselves: “I soon burst in at 3 in the morning to accuse my parents of being impostors, of having killed my real parents while they themselves were neo‑Nazi agents altered by special surgery and trained to mimic my parents.”
The tone was reminiscent of countless sci-fi stories Michael had summarized for me in the schoolyard—he’d seen a secretary at Bain with “blood dripping from her teeth as her clawed hands reached for me”—but the proposal rose from the depths of such delusions, tracing the archetypal tale of a young man’s triumph and a father’s love. Even as it offered glimpses of bloody fangs and Nazi spies, the narrative arc bent toward Yale Law School. Michael’s agent escorted him to publishing houses, where he spoke with undaunted fluency.
When an editor asked Michael if he still hallucinated, he told her, “I’m hallucinating right now.” The room grew quiet as Michael described a burning waterfall emptying into a lake of fire. He also saw a peaceful house with shutters and vines. Michael explained that he managed these and other competing images by arranging them on a great screen in his mind, in a hierarchy of terror from greatest to least.
The movie people found his method of controlling his hallucinations a perfect cinematic conceit.
Michael made little progress on his memoir, possibly none. The movie, meanwhile, raced along like the river outside the window of his apartment in Hastings-on-Hudson, where he had moved with Carrie. It wasn’t the first time a screenwriter had needed to base a movie on a book that didn’t exist. It could even be an advantage.
But for Michael, leaving his story to Hollywood was unthinkable. The closer The Laws of Madness got to becoming a movie, the more important the book became, a chance to restore the dream of creative achievement that had gone up in smoke.
In an effort to bolster Michael’s resolve, his editor Hamilton Cain took the train to Hastings‑on‑Hudson. Cain brought a tape recorder, hoping an interview might jump‑start the process. He and Michael envisioned a series of sessions.
The interview began with Michael talking about Mereland Road and me: “There were only six or seven houses in the most immediate part of our neighborhood, our street. I was inseparable from a friend who moved in when I was in fifth grade, Jonathan.” We were both going to be writers, he told Cain: “He’s done it; he is a novelist. I was sure that I, too, would be one.”
Cain and Michael talked all day. The apartment grew dim as the December sun crossed the river and disappeared behind New Jersey. Michael had never turned on the lights, and made no move to do so as the winter dusk crept inside. Cain was scribbling in the interior gloom, eager to capture a few last thoughts from what he felt had been a very successful session. Suddenly Michael spoke in a voice that seemed to have dropped an octave. Startled, Cain looked up and saw Michael, still sitting across from him, rocking back and forth.
“I’m very tired,” Michael said in a deep, denatured voice. “I think you’d better go.”
“We’ll wrap it up,” Cain said, turning back to his notebook. He was scribbling fast when he became aware that Michael had risen and come over to the couch where Cain was sitting. He sensed his looming presence, rocking back and forth. Cain felt the hairs on the back of his neck stand straight. Michael was towering over him, his face utterly transformed.
“Is everything okay?” Cain asked.
“I think you should go now,” Michael said, his voice deep and slow. “I’m really, really tired.”
Cain was all speed, gathering up his tape recorder, notebook, backpack, coat, but by the time he was at the door saying good-bye, Michael had recovered his old self and insisted, with customary gallantry, on walking him to the train station. He talked easily on the short walk, and at the platform gave Cain a hug.
Neither of them mentioned the anomalous moment in the gloom. Still, the impression troubled Cain, and stayed with him on the train back to the city.
“We Can’t Do Anything”
To the seasonedobservers of the Network watching over Michael, his relationship with Carrie was one more example of his exceptional nature. In their experience, it was unusual for people with schizophrenia to sustain long‑term relationships.
For Carrie’s colleagues, the equation was reversed: Michael’s illness was evidence of Carrie’s exceptional nature. But she did not like to talk about the times when she came home from work and Michael refused to let her into their apartment, because he didn’t believe she was who she said she was. No matter how much Carrie insisted, she couldn’t convince him of the truth. How could he trust her words when he didn’t believe it was her body? At such times, the terror and fury on the other side of the door were enough to send her to a friend’s couch. Those were hard nights.
That the tough times were getting worse was no secret to the members of the Network, who now watched over Carrie as well.
One evening in June 1998, Jane Ferber had dinner with her friend Myrna Rubin and conveyed her distress about Michael’s backward slide. Myrna had heard that Michael had stopped taking his medication and that nobody had been able to get him to go back on it, but she was shocked when she heard that he thought Carrie was an alien. Still, delusions were no more a justification for forced medication than refusing medication was a justification for forced hospitalization. The only question was whether Michael was violent, and the Network didn’t see him that way.
Elizabeth Ferber, Jane’s daughter, had been hearing reports about Michael’s decline from her mother. That he was losing control was disturbing, but it was the constrained intensity of her mother’s voice, the sadness and resignation, that affected her most. Surely now was the time to act.
But when Elizabeth demanded to know what was being done, her mother told her, “We can’t do anything.”
What Elizabeth heard in her mother’s voice wasn’t fear of Michael, but fear for him. The danger that weighed most heavily on the members of the Network was that Michael would suffer a break from which he might never recover—that he would end up in the revolving door of endless hospitalizations. They doubted the efficacy of the system but feared its capacity for destruction, and they desperately wanted to save him from it.
On Wednesday, June 17, the day before her work team was flying to Chicago for a big meeting, Carrie called her office to say she had a personal emergency and would not be coming in. It was unusual for Carrie to miss a day of important preparation, but her boss had no doubt she would be there the next morning with her materials in order.
Too Late
It was a day of frantic phone calls and failed efforts at intervention. Michael had been bombarding his mother, making wild accusations and irrational threats. After Michael ranted about suicide and murder, Ruth called back in a panic. Michael picked up, and Ruth told him to give the phone to Carrie. Michael said he couldn’t do that, because he’d killed her.
Ruth called the police at 4:17 p.m. She urged speed and gave few details. The desk sergeant heard the panic in her voice and put out a radio call to check on the welfare of a couple in the River Edge apartments.
Officers rang Michael and Carrie’s bell and got no response. The door was locked, so they radioed their sergeant, who called Lieutenant Vince Schiavone, the department’s executive officer, at home. Schiavone told them to get the key from the super and check out the place at once.
June 18, 1998: Detectives escort Michael into the Hastings-on-Hudson police station, after driving him back from Ithaca the day after he killed Carrie. (Mitch Jacobson / AP / Shutterstock; LiliGraphie / Getty)
The officers found a woman’s body in the kitchen, lying in a pool of blood. There were multiple stab wounds, and her throat had been cut. Schiavone visited the crime scene briefly, then drove with an officer to New Rochelle to deliver the news to 28 Mereland Road in person. Ruth peered through the glass, opened the door, and asked, “Is she …?”
“Yes,” Schiavone told her. “She is.”
Ruth burst into tears. Schiavone would never forget the look on her face. It seemed to say, Oh my God, we didn’t move fast enough.
“I knew something like this could happen,” Ruth said, explaining that her son had schizophrenia. “But he was getting happy. They were going to be married …”
Her anguish was intense. They’d been trying to get him the help he needed, she said. Not that he wasn’t getting help already. She wanted Schiavone to know, he felt, that they’d been working on this, and it had gotten away from them somehow.
The medical examiner’s report, released quickly, told its stark forensic story. The death was a homicide. The cause was “sharp force injuries of head, neck, back and upper extremity involving lungs, aorta, esophagus and thyroid cartilage.”
An additional piece of information deepened the tragedy: Carrie was pregnant.
Michael’s photo was on the cover of the New York Post under a massive one‑word headline, printed in white-on-black “knockout type”: PSYCHO.
Seeing Michael looking out from the far side of that tabloid window like the Son of Sam was shocking. The photo filled the left side of the page; the right half announced, also in white‑on‑black type: “Twisted genius charged with savage slaying of pregnant fiancee.” At the bottom right was a picture of Carrie smiling with hopeful innocence. A footer running the width of the page flagged coverage of Michael’s ill‑fated movie: “Universal Studio honchos on hot seat page 32.”
Michael was charged with second‑degree murder. Because of the nature of the crime, no bail was set. But Michael’s lawyer did request that Michael receive psychiatric treatment. Now that he’d killed someone, it was no longer necessary to prove that he was an imminent danger to himself or others—he could finally get the care and medication he needed. The state, eager to have him fit to stand trial for murder, would provide him with both.
“Untreated Psychosis Kills”
A month after Carrie’s killing, another gruesome event eclipsed and extended Michael’s story. A 41-year-old man named Russell Weston Jr. walked into the Capitol in Washington, D.C., and shot a police officer in the back of the head with a .38‑caliber revolver. He exchanged shots with another officer, wounding him and a tourist, then raced down a corridor and through a door that led to a suite of offices used by Majority Whip Tom DeLay, where he shot a plainclothes detective in the chest, killing him.
It did not take long to discover that Weston had rejected treatment for paranoid schizophrenia and was severely delusional. He had stormed the Capitol to access an override console for the Ruby Satellite System, stored in the Senate safe, which was the only way to avert the cannibal apocalypse and plague that were about to destroy the world.
Despite their radically different backgrounds, Michael Laudor was immediately joined to Russell Weston: Both suffered from a severe mental illness, had rejected medication, and in the grip of psychosis had killed people.
Torrey, the psychiatrist, wrote about the two men for The Wall Street Journal in an article called “Why Deinstitutionalization Turned Deadly.” The stories of the “Yale Law School graduate” and the “drifter,” the psychiatrist wrote, “are only the most publicized of an increasing number of violent acts by people with schizophrenia or manic‑depressive illness who were not taking the medication they need to control their delusions and hallucinations.”
Weston’s anguished father, Russell Sr., was quoted in a New York Times column about the impossibility of helping his son: “He was a grown man. We couldn’t hold him down and force the pills into him.” Weston’s father could do nothing, Frank Rich wrote, because “a comprehensive system of mental‑health services, including support for parents with sick adult children who refuse treatment, doesn’t exist. If it had, the Westons might have had more success in rescuing their son—as might the equally loving family of Michael Laudor.”
For politicians, the outrage of after was easier than the work of before. President Bill Clinton denounced the violence of an unmedicated psychotic man nobody felt authorized to treat as “a moment of savagery at the front door of American civilization.” Diagnosed in his late 20s, Weston had spent 53 days in a state hospital in 1996 after threatening an emergency-room worker. Once he no longer seemed imminently dangerous, he had been released with pills that he eventually stopped taking, perhaps because he did not consider himself mentally ill.
“The total number of individuals with active symptoms of schizophrenia or manic‑depressive illness is some 3.5 million,” Torrey wrote. “The National Advisory Mental Health Council has estimated that 40% of them—roughly 1.4 million people—are not receiving any treatment in any given year. It is therefore not a question of whether someone will follow Michael Laudor and Russell Weston into the headlines. It is merely a question of when.”
Torrey did not see Michael’s killing of Carrie as a “tragic inevitability,” which is how the law professor who had once imagined Michael becoming an advocate for people with schizophrenia described it to me years later.
Nor did Torrey believe that the 1,000 annual homicides he attributed to people with severe unmedicated mental illness should indict the population of those with similar diagnoses. But he did want to prevent those homicides, as well as an even larger number of suicides, and he wanted to reduce the growing number of mentally ill homeless people, and do something about a prison population swelled by people suffering from mental illness who received no care. His sister had schizophrenia, and he did think there was a difference between being in your right mind and being out of it.
The arguments Torrey made about Michael in TheWall Street Journal in 1998 informed the Treatment Advocacy Center, which he created that year to focus on the medical, moral, and legal imperatives of treating people whose severe mental illness prevents them from knowing they need help. Now 85, Torrey was recently profiled in The New York Times, which credited him with inspiring assisted outpatient treatment programs—present in 47 states—as well as Mayor Adams’s new initiative and a larger transformation in the understanding of severe mental illness at the policy level.
Last spring, Adams appointed Brian Stettin, who had been working as the Treatment Advocacy Center’s policy director, to be his administration’s senior adviser on severe mental illness—a title that itself announces a policy shift. Adams hired Stettin not long after he published an op-ed in the Daily News about the death of Michelle Go, who had been pushed in front of a subway train in January 2022 by a man who’d been hospitalized more than 20 times.
Stettin noted that the man who killed Go should have been in an assisted outpatient treatment program, but had fallen through the holes of a porous system. He began his article by recalling Kendra Webdale, who also had been pushed in front of a subway train and killed 23 years earlier. A young assistant attorney general at the time, Stettin had been tasked by his new boss, New York Attorney General Eliot Spitzer, with drafting legislation to prevent horrors like the one that had befallen Webdale. Her killer had been hospitalized 13 times in two years and on one occasion had literally walked into Bellevue Hospital demanding help. The man, who suffered from severe mental illness, wanted to return to housing on the grounds of Creedmoor Psychiatric Center, in Queens, but to qualify, he would have to be hospitalized there first, and he couldn’t be hospitalized, because no beds were available. He was given the phone number of a mobile crisis unit by a social worker, who noted that he had no phone.
When they asked Webdale’s parents to lend their daughter’s name to legislation creating assisted outpatient treatment programs across New York State, Spitzer and Stettin discovered that the family had received letters of support not only from parents who had lost children to violence but from parents who had written to say of the killer, “That might have been my son.” Webdale’s mother wanted to know what the attorney general was going to do for those parents.
I experienced something similar when I spent time with Nick and Amanda Wilcox, whose daughter, Laura, a 19-year-old sophomore at Haverford College, was killed in 2001 while working at a mental-health clinic during her Christmas break. Laura’s Law is California’s version of Kendra’s Law, passed county by county with the tireless support of the Wilcoxes, who faced opposition from the ACLU and fellow Quakers, who consider assisted outpatient treatment programs a threat to civil liberties.
It was heartbreaking to stand in Laura’s childhood bedroom and hear the terrible comfort the Wilcoxes took in learning that the pen their daughter had gripped so tightly in death suggested that she had died instantly. I knew they had refused to seek the death penalty for their daughter’s killer—who killed two more people at a nearby restaurant, where he believed he was being poisoned. But hearing them say “He’s in the right place”—a state mental hospital—after he was found not competent to stand trial, and realizing it was treatment they wished for him, was a humbling astonishment. The anger they expressed was directed at a system that had resisted committing a severely ill, dangerous man known to have an apartment filled with unregistered guns, in part to avoid the cost of sending him to a county with a suitable facility.
I was the childhood friend of someone who had killed a woman not unlike the Wilcoxes’ daughter. Amanda gave me advice about reaching out to Carrie’s parents. “Say you’re sorry for what your friend did,” she told me. “That’s what I would want to hear.” Although Carrie’s family wrote back to tell me it was simply too painful to talk about, I was grateful I’d been able to express my sorrow.
E. Fuller Torrey sees what is happening in New York and California—where Governor Gavin Newsom has signed the Community Assistance, Recovery, and Empowerment (CARE) Act—as part of a sea change. He has no illusions about the challenges—New York State still hasn’t recovered all of the 1,000 psychiatric beds repurposed for COVID use during the pandemic—but he believes that change starts with the recognition that denying care to people too impaired to know they need it is a medical and moral failure. He thought it a hopeful portent that when a disability-rights group tried to block the CARE Act, the group’s Sacramento offices were picketed by relatives, friends, and other supporters of people with severe mental illness carrying signs saying UNTREATED PSYCHOSIS KILLS and HOSPITALS NOT PRISONS. When I asked Torrey what he considers the biggest threat to reform, he said pessimism, the resigned conviction that after 40 years of failed efforts, nothing can be done.
Katherine Koh is a psychiatrist at Massachusetts General Hospital. As part of the street team at the Boston Health Care for the Homeless Program, she works with the most neglected population in the country, people struggling to meet basic needs even if they are not suffering from a mental illness. Though she spoke of involuntary commitment as “a difficult, nuanced, and thorny issue” that “haunts and plagues” her, she told me that the biggest improvements in people’s mental health can happen when they are involuntarily hospitalized, provided there is a plan in advance and care afterward.
Koh also told me a story that she’d heard from her mentor, Jim O’Connell, the founding physician at Boston Health Care for the Homeless. The story is about a woman he spent many years caring for on the street, who was often on the psychiatric brink, though O’Connell, determined to honor her autonomy and dignity, never committed her. Finally, the police did it for him. After the hospital, and time spent stably housed, the woman moved on to other systems of support, slowly recovered her balance, began working again, and eventually joined the board of an organization that sponsored the event where she and O’Connell reunited after many years. When the woman saw him—as Koh recalled her teacher’s vivid recounting—she said, “You son of a bitch! You left me out on the street for 10 years!” And then a further lesson: “If I were bleeding, you would have taken me in. But since it was my brain, you left me out there.”
Laurie Flynn, who was the executive director of the National Alliance on Mental Illness when Michael killed Carrie, burst into tears when she learned what had happened. Michael had been a hero to many at NAMI, the largest grassroots organization in America dedicated to supporting people with severe mental illness and their families. He had seemed so emblematic of a new era, promising the rejection of shame and stigma, that the “Michael Laudor Tragedy,” as Flynn called it, became part of a complex reckoning that filled many in the organization with the understandable fear of stigma.
Violence and mental illness have been legally entangled ever since dangerousness, rather than illness, became the de facto prerequisite for hospitalization. If a hospital could produce a bed, or mandate treatment, only for someone actively threatening harm, you could hardly blame the general population for mixing up the very sick and the very violent, or mental hospitals and prisons. Today the Twin Towers Correctional Facility, in Los Angeles, is described—by the L.A. County Sheriff’s Department—as “the nation’s largest mental health facility.”
And you can hardly blame advocates for wanting to erase even the suggestion of violence as a precondition for eliminating stigma. But denying all distinctions can be as destructive as exaggerating them. Many of the critics of Adams’s proposal highlighted the involuntary hospitalization of mentally ill people “even if they posed no threat to others,” as if hospitalizing a gravely ill person who didn’t threaten someone’s life made no sense.
For Flynn, the problem is a system that forces families to “sit and watch someone they love deteriorate, unable to get them help until they are dangerous.” Acknowledging distinctions, in order to address people’s needs, will do more than denial does to reduce stigma. It will also keep people alive.
In the Daily News op-ed, Stettin wrote, “There are fundamental differences between the 4% of the population with severe diagnoses and the rest of us who experience various mental health challenges over the course of our lives. A big one is that without treatment, people with severe mental illness lose their connection to reality.” He is at pains to emphasize that the mayor’s initiative is directed at a fractional subset of that percentage, people without shelter who are too sick to care for themselves or recognize their own impaired condition.
It has been 25 years since Michael killed Carrie. For most of that time, he has been in a secure psychiatric facility surrounded by a 16‑foot‑high fence topped with razor wire. He lives with 280 other men and women sent there by court order, attended to by twice that number of staff.
Michael was found not responsible by “means of mental defect,” bolstered by the finding of Park Dietz, the forensic psychiatrist hired by the prosecution, who was known for his narrow definition of insanity. Dietz had found both John Hinckley and Jeffrey Dahmer legally sane, but he determined that Michael truly thought he was killing a doll or a robot.
I know there is no going back to the time before Michael killed Carrie, just as there is no going back to the monumental hospitals that long ago ceased to be worthy of the concept of asylum that created them. Just as there can be no going back to the utopian vision of the people who destroyed them, whose faith in their own expertise and dream of community care failed to fulfill their promise to the people whose desperate need had justified the demolition.
I also know that there can be no going forward without a reckoning, however partial and imperfect. Not to apportion blame, but to make it easier to change or clarify a law, or to narrow the focus of an initiative—while expanding its resources—to address a fraction of the population whose illnesses are so severe, they can make sufferers unaware of their own deterioration. Above all, it should be harder to impose imaginary solutions on real problems.
Two years before Michael killed Carrie, a Times article had quoted him, identified as a legal scholar with a history of schizophrenia, expressing outrage that a medical student—who had stopped taking medication for his bipolar disorder and was alarming psychiatrists and fellow students with what they considered violent and threatening behavior—had “lost five weeks of his life” to forced hospitalization. The article was called “Medical Student Forced Into a Hospital Netherworld,” but who among Michael’s friends would not wish now that the same had happened to him, if five weeks could have helped return him to the treatment he needed, saved Carrie’s life, and prevented Michael’s destruction?
I remain haunted by my last phone conversation with Michael before he killed Carrie. He was vague, equivocal, even as we picked a date to see each other that I suspected, perhaps hoped, would pass like the others. “I have to go,” he said abruptly. “I’m having bad thoughts I need to not be having.”
I knew something was dreadfully wrong, but I buried that abject statement, and kept myself from considering its meaning.
Tom Smith lost his daughter to mental illness in 2003. He touches on the importance of self-esteem in a society that often compares, continuing to shed light on mental health stigma.
Unconditional love lies at the heart of helping a loved one with mental health issues develop positive self-esteem. But as a society we are geared toward conditional love: in overt and subtle ways, we learn how to love on the condition that someone else’s behavior and attitudes meet our expectations.
But the delicate line between necessary, healthy expectations and conditional love is hard to identify and even more complicated to apply effectively. Parents, for example, generally expect that their children meet certain behavioral, educational, and social standards. At the same time, they strive to love their children unconditionally. It’s common to hear adults recalling their own childhood and testifying to their parents’ failure to separate their expressions of love from their performance or behavior expectations for the child.
We don’t always learn unconditional love at home.
Through adolescence and into adulthood, we may not experience unconditional love, either. Competition at school, the workplace, in sports, in social circles, and even in entertainment and arts — all contribute to a society that constantly compares. Someone is “better” (which means someone else is “worse”), someone wins while others lose, some people presumably succeed and others fail. This message is everywhere — in popular media, in advertising, and in our language. We are expected to behave, think, and feel in particular ways, or be shunned, minimized, ignored, or condemned.
The stigma against mental illness thrives in this environment, unfortunately. Nor does this atmosphere promote learning how to love unconditionally. But loving unconditionally is precisely what family and friends of people with mental illness need to do.
How do we do this?
Maintain a positive attitude. Compliment your loved one often. Avoid making comparisons. Don’t take the person’s insults, disrespect, anger, and rejection too personally. Make a habit of showing that you genuinely care about their well-being. Wish them well in all their endeavors, help them achieve appropriate goals, listen to them closely and try to understand the world from their perspective.
To love unconditionally means to care for, respect, understand, and forgive another person regardless of their response to your efforts. “Regardless” is the hard part. Loving a person with mental health problems requires a commitment to this kind of love, even as we know that we will sometimes fail.
A healthy self-esteem is essential to a balanced life, and this strategy is worth lots of time, discussion, and effort. Self-esteem is an immeasurable asset to people with mental illness. It can be the emotional anchor that allows them to monitor their medication, use counseling effectively, regulate their schedule, know their strengths and limits, and seek and accept help when needed.
Family and friends are in position to help with this development, since they are in regular contact. They know their loved one’s personality, thought patterns, habits, preferences, and feelings. Practicing unconditional love, they can create a supportive environment where their loved one has the best chance of experiencing the benefits of a healthy self-esteem.
—–
Tom Smith is the cofounder of the Karla Smith Foundation, which supports parents and loved ones of mentally ill people. He is author of several articles and books, including God on the Job and Alive in the Spirit.
When someone becomes homeless, the instinct is to ask what tragedy befell them. What bad choices did they make with drugs or alcohol? What prevented them from getting a higher-paying job? Why did they have more children than they could afford? Why didn’t they make rent? Identifying personal failures or specific tragedies helps those of us who have homes feel less precarious—if homelessness is about personal failure, it’s easier to dismiss as something that couldn’t happen to us, and harsh treatment is easier to rationalize toward those who experience it.
Explore the January/February 2023 Issue
Check out more from this issue and find your next story to read.
But when you zoom out, determining individualized explanations for America’s homelessness crisis gets murky. Sure, individual choices play a role, but why are there so many more homeless people in California than Texas? Why are rates of homelessness so much higher in New York than West Virginia? To explain the interplay between structural and individual causes of homelessness, some who study this issue use the analogy of children playing musical chairs. As the game begins, the first kid to become chairless has a sprained ankle. The next few kids are too anxious to play the game effectively. The next few are smaller than the big kids. At the end, a fast, large, confident child sits grinning in the last available seat.
You can say that disability or lack of physical strength caused the individual kids to end up chairless. But in this scenario, chairlessness itself is an inevitability: The only reason anyone is without a chair is because there aren’t enough of them.
Now let’s apply the analogy to homelessness. Yes, examining who specifically becomes homeless can tell important stories of individual vulnerability created by disability or poverty, domestic violence or divorce. Yet when we have a dire shortage of affordable housing, it’s all but guaranteed that a certain number of people will become homeless. In musical chairs, enforced scarcity is self-evident. In real life, housing scarcity is more difficult to observe—but it’s the underlying cause of homelessness.
In their book, Homelessness Is a Housing Problem, the University of Washington professor Gregg Colburn and the data scientist Clayton Page Aldern demonstrate that “the homelessness crisis in coastal cities cannot be explained by disproportionate levels of drug use, mental illness, or poverty.” Rather, the most relevant factors in the homelessness crisis are rent prices and vacancy rates.
Colburn and Aldern note that some urban areas with very high rates of poverty (Detroit, Miami-Dade County, Philadelphia) have among the lowest homelessness rates in the country, and some places with relatively low poverty rates (Santa Clara County, San Francisco, Boston) have relatively high rates of homelessness. The same pattern holds for unemployment rates: “Homelessness is abundant,” the authors write, “only in areas with robust labor markets and low rates of unemployment—booming coastal cities.”
Why is this so? Because these “superstar cities,” as economists call them, draw an abundance of knowledge workers. These highly paid workers require various services, which in turn create demand for an array of additional workers, including taxi drivers, lawyers and paralegals, doctors and nurses, and day-care staffers. These workers fuel an economic-growth machine—and they all need homes to live in. In a well-functioning market, rising demand for something just means that suppliers will make more of it. But housing markets have been broken by a policy agenda that seeks to reap the gains of a thriving regional economy while failing to build the infrastructure—housing—necessary to support the people who make that economy go. The results of these policies are rising housing prices and rents, and skyrocketing homelessness.
It’s not surprising that people wrongly believe the fundamental causes of the homelessness crisis are mental-health problems and drug addiction. Our most memorable encounters with homeless people tend to be with those for whom mental-health issues or drug abuse are evident; you may not notice the family crashing in a motel, but you will remember someone experiencing a mental-health crisis on the subway.
I want to be precise here. It is true that many people who become homeless are mentally ill. It is also true that becoming homeless exposes people to a range of traumatic experiences, which can create new problems that housing alone may not be able to solve. But the claim that drug abuse and mental illness are the fundamental causes of homelessness falls apart upon investigation. If mental-health issues or drug abuse were major drivers of homelessness, then places with higher rates of these problems would see higher rates of homelessness. They don’t. Utah, Alabama, Colorado, Kentucky, West Virginia, Vermont, Delaware, and Wisconsin have some of the highest rates of mental illness in the country, but relatively modest homelessness levels. What prevents at-risk people in these states from falling into homelessness at high rates is simple: They have more affordable-housing options.
With similar reasoning, we can reject the idea that climate explains varying rates of homelessness. If warm weather attracted homeless people in large numbers, Seattle; Portland, Oregon; New York City; and Boston would not have such high rates of homelessness and cities in southern states like Florida, Georgia, Alabama, and Mississippi such low ones. (There is a connection between unsheltered homelessness and temperature, but it’s not clear which way the causal arrow goes: The East Coast and the Midwest have a lot more shelter capacity than the West Coast, which keeps homeless people more out of view.)
America has had populations of mentally ill, drug-addicted, poor, and unemployed people for the whole of its history, and Los Angeles has always been warmer than Duluth—and yet the homelessness crisis we see in American cities today dates only to the 1980s. What changed that caused homelessness to explode then? Again, it’s simple: lack of housing. The places people needed to move for good jobs stopped building the housing necessary to accommodate economic growth.
Homelessness is best understood as a “flow” problem, not a “stock” problem. Not that many Americans are chronically homeless—the problem, rather, is the millions of people who are precariously situated on the cliff of financial stability, people for whom a divorce, a lost job, a fight with a roommate, or a medical event can result in homelessness. According to the Los Angeles Homeless Services Authority, roughly 207 people get rehoused daily across the county—but 227 get pushed into homelessness. The crisis is driven by a constant flow of people losing their housing.
The homelessness crisis is most acute in places with very low vacancy rates, and where even “low income” housing is still very expensive. A study led by an economist at Zillow shows that when a growing number of people are forced to spend 30 percent or more of their income on rent, homelessness spikes.
Academics who study homelessness know this. So do policy wonks and advocacy groups. So do many elected officials. And polling shows that the general public recognizes that housing affordability plays a role in homelessness. Yet politicians and policy makers have generally failed to address the root cause of the crisis.
Few Republican-dominated states have had to deal with severe homelessness crises, mainly because superstar cities are concentrated in Democratic states. Some blame profligate welfare programs for blue-city homelessness, claiming that people are moving from other states to take advantage of coastal largesse. But the available evidence points in the opposite direction—in 2022, just 17 percent of homeless people reported that they’d lived in San Francisco for less than one year, according to city officials. Gregg Colburn and Clayton Aldern found essentially no relationship between places with more generous welfare programs and rates of homelessness. And abundantotherresearch indicates that social-welfare programs reduce homelessness. Consider, too, that some people move to superstar cities in search of gainful employment and then find themselves unable to keep up with the cost of living—not a phenomenon that can be blamed on welfare policies.
But liberalism is largely to blame for the homelessness crisis: A contradiction at the core of liberal ideology has precluded Democratic politicians, who run most of the cities where homelessness is most acute, from addressing the issue. Liberals have stated preferences that housing should be affordable, particularly for marginalized groups that have historically been shunted to the peripheries of the housing market. But local politicians seeking to protect the interests of incumbent homeowners spawned a web of regulations, laws, and norms that has made blocking the development of new housing pitifully simple.
This contradiction drives the ever more visible crisis. As the historian Jacob Anbinder has explained, in the ’70s and ’80s conservationists, architectural preservationists, homeowner groups, and left-wing organizations formed a loose coalition in opposition to development. Throughout this period, Anbinder writes, “the implementation of height limits, density restrictions, design review boards, mandatory community input, and other veto points in the development process” made it much harder to build housing. This coalition—whose central purpose is opposition to neighborhood change and the protection of home values—now dominates politics in high-growth areas across the country, and has made it easy for even small groups of objectors to prevent housing from being built. The result? The U.S. is now millions of homes short of what its population needs.
Los Angeles perfectly demonstrates the competing impulses within the left. In 2016, voters approved a $1.2 billion bond measure to subsidize the development of housing for homeless and at-risk residents over a span of 10 years. But during the first five years, roughly 10 percent of the housing units the program was meant to create were actually produced. In addition to financing problems, the biggest roadblock was small groups of objectors who didn’t want affordable housing in their communities.
Los Angeles isn’t alone. The Bay Area is notorious in this regard. In the spring of 2020, the billionaire venture capitalist Marc Andreessen published an essay, “It’s Time to Build,” that excoriated policy makers’ deference to “the old, the entrenched.” Yet it turned out that Andreessen and his wife had vigorously opposed the building of a small number of multifamily units in the wealthy Bay Area town of Atherton, where they live.
The small-c conservative belief that people who already live in a community should have veto power over changes to it has wormed its way into liberal ideology. This pervasive localism is the key to understanding why officials who seem genuinely shaken by the homelessness crisis too rarely take serious action to address it.
The worst harms of the homelessness crisis fall on the people who find themselves without housing. But it’s not their suffering that risks becoming a major political problem for liberal politicians in blue areas: If you trawl through Facebook comments, Nextdoor posts, and tweets, or just talk with people who live in cities with large unsheltered populations, you see that homelessness tends to be viewed as a problem of disorder, of public safety, of quality of life. And voters are losing patience with their Democratic elected officials over it.
In a 2021 poll conducted in Los Angeles County, 94 percent of respondents said homelessness was a serious or very serious problem. (To put that near unanimity into perspective, just 75 percent said the same about traffic congestion—in Los Angeles!) When asked to rate, on a scale of 1 to 10, how unsafe “having homeless individuals in your neighborhood makes you feel,” 37 percent of people responded with a rating of 8 or higher, and another 19 percent gave a rating of 6 or 7. In Seattle, 71 percent of respondents to a recent poll said they wouldn’t feel safe visiting downtown Seattle at night, and 91 percent said that downtown won’t recover until homelessness and public safety are addressed. There are a lot of polls like this.
As the situation has deteriorated, particularly in areas where homelessness overruns public parks or public transit, policy makers’ failure to respond to the crisis has transformed what could have been an opportunity for reducing homelessness into yet another cycle of support for criminalizing it. In Austin, Texas, 57 percent of voters backed reinstating criminal penalties for homeless encampments; in the District of Columbia, 75 percent of respondents to a Washington Post poll said they supported shutting down “homeless tent encampments” even without firm assurances that those displaced would have somewhere to go. Poll data from Portland, Seattle, and Los Angeles, among other places, reveal similarly punitive sentiments.
This voter exasperation spells trouble for politicians who take reducing homelessness seriously. Voters will tolerate disorder for only so long before they become amenable to reactionary candidates and measures, even in very progressive areas. In places with large unsheltered populations, numerous candidates have materialized to run against mainstream Democrats on platforms of solving the homelessness crisis and restoring public order.
By and large, the candidates challenging the failed Democratic governance of high-homelessness regions are not proposing policies that would substantially increase the production of affordable housing or provide rental assistance to those at the bottom end of the market. Instead, these candidates—both Republicans and law-and-order-focused Democrats—are concentrating on draconian treatment of people experiencing homelessness. Even in Oakland, California, a famously progressive city, one of the 2022 candidates for mayor premised his campaign entirely on eradicating homeless encampments and returning order to the streets—and managed to finish third in a large field.
During the 2022 Los Angeles mayoral race, neither the traditional Democratic candidate, Karen Bass, who won, nor her opponent, Rick Caruso, were willing to challenge the antidemocratic processes that have allowed small groups of people to block desperately needed housing. Caruso campaigned in part on empowering homeowners and honoring “their preferences more fully,” as Ezra Klein put it in The New York Times—which, if I can translate, means allowing residents to block new housing more easily. (After her victory, Bass nodded at the need to house more people in wealthier neighborhoods—a tepid commitment that reveals NIMBYism’s continuing hold on liberal politicians.)
“We’ve been digging ourselves into this situation for 40 years, and it’s likely going to take us 40 years to get out,” Eric Tars, the legal director at the National Homelessness Law Center, told me.
Building the amount of affordable housing necessary to stanch the daily flow of new people becoming homeless is not the project of a single election cycle, or even several. What can be done in the meantime is a hard question, and one that will require investment in temporary housing. Better models for homeless shelters arose out of necessity during the pandemic. Using hotel space as shelter allowed the unhoused to have their own rooms; this meant families could usually stay together (many shelters are gender-segregated, ban pets, and lack privacy). Houston’s success in combatting homelessness—down 62 percent since 2011—suggests that a focus on moving people into permanent supportive housing provides a road map to success. (Houston is less encumbered by the sorts of regulations that make building housing so difficult elsewhere.)
The political dangers to Democrats in those cities where the homelessness crisis is metastasizing into public disorder are clear. But Democratic inaction risks sparking a broader political revolt—especially as housing prices leave even many middle- and upper-middle-class renters outside the hallowed gates of homeownership. We should harbor no illusions that such a revolt will lead to humane policy change.
Simply making homelessness less visible has come to be what constitutes “success.” New York City consistently has the nation’s highest homelessness rate, but it’s not as much of an Election Day issue as it is on the West Coast. That’s because its displaced population is largely hidden in shelters. Yet since 2012, the number of households in shelters has grown by more than 30 percent—despite the city spending roughly $3 billion a year (as of 2021) trying to combat the problem. This is what policy failure looks like. At some point, someone’s going to have to own it.
This article appears in the January/February 2023 print edition with the headline “The Looming Revolt Over Homelessness.” When you buy a book using a link on this page, we receive a commission. Thank you for supporting The Atlantic.
New York City Mayor Eric Adams announced a plan on Tuesday to involuntarily remove homeless people with mental illnesses from the streets and subways and force them to receive a psychiatric evaluation.
At a news conference on Tuesday, Adams said the city has a “moral obligation” to help all homeless people with mental illnesses get treatment and care. The plan authorizes police officers to involuntarily hospitalize homeless people who appear to be mentally ill or pose a threat to themselves or others. Involuntary hospitalization is required even if the homeless person doesn’t appear to pose an imminent threat to the public.
“The very nature of their illness keeps them from realizing they need intervention and support. Without that intervention, they remain lost and isolated from society, tormented by delusions and disordered thinking,” Adams said.
Adams said the plan would address a “crisis we see all around us.”
According to the Coalition for the Homeless, the unhoused population in New York City in recent years has reached its highest levels since the Great Depression, with a near-record 20,764 single adults sleeping in shelters each night in September 2022. The National Alliance on Mental Health found that 20.8% of homeless people in the U.S. have a serious mental illness.
A surge of attacks on New York City streets and subways has raised alarm in recent years, with many of the assaults involving homeless people. Last month, Adams laid blame for the attacks on mental illnesses. Adams and other elected officials have been pushed to take action on issues surrounding homelessness and mental health.
“As a city, this work — at the intersection of public safety and mental illness — represents part of the larger strategy, which is centered on providing everyone living with serious mental illness the basic building blocks of recovery: Health care, a home, and a community,” the city’s health commissioner, Ashwin Vasan, said in a tweet in support of Adams’ efforts.
But the plan to involuntarily remove and hospitalize homeless people raised some concerns and criticism. Maria Town, the president and CEO of the American Association of People With Disabilities, said in a tweet that the plan is a violation of rights and aims to make homeless people less visible rather than improve their outcome.
New York City Council member Tiffany Cabán also said in a tweet that the plan is “deeply problematic” and that deadly situations are often created by the wrong responder and response rather than the mental health crisis itself.
“Consent is key & health infrastructure is necessary. Voluntary consent offered by the appropriate responders paired [with] ample and appropriate options. Transport to emergency rooms is often not the best answer and there needs to be deep investment in safe respites, clinics, [outpatient commitments] and more,” she said in the tweet.
Adams was on the receiving end of criticism from advocates and progressives earlier this year for clearing homeless encampments and using policing tactics in efforts to respond to homeless New Yorkers and improve public safety.
No, I don’t mean the emotion (although that’s part of it).
I’m talking about Seasonal Affective Disorder.
Luckily, we have some tips and tricks for treating SAD that our Online Coaching Clients use. Today, we’ll share them with you too.
Here’s what we’ll cover:
Disclaimer: We’re going to be discussing some issues that may be difficult for some going through a tough time. If you (or someone you know) aren’t coping so well, PLEASE see the links at the bottom of this article with some resources from all around the world. Obviously, we recommend discussing this information with your health professional – none of this is a diagnosis, but rather a starting point for discussion.
BUT, armed with the right weapons, we can ward off the winter monster, or even keep it in full hibernation.
From here, mental health wizard and resident NF Family Rebel Correspondent, Dan Schmidt, will take it away:
Most of us feel a little glum in winter…it’s natural to feel a little down.
Cold mornings, less time outside, and often it’s not as easy to get out and do our favorite things:
So for a lot of us, winter just sucks a little.
We’ve known something was up since the 6th century, but SAD remained a mythical creature until the 1980s in the West when it became officially recognized as a mood disorder. While we’re still not 100% sure of how it works; it’s pretty clear to see that SAD especially thrives in cooler, darker climates.
For example, studies show[1] SAD’s prevalence in the U.S. ranges from around 1% in Florida to 9% in Alaska. Looking around the world, in Oslo, Norway, around 14% of the population will be impacted by SAD,[2] while us lucky buggers Down Under are barely impacted at all, with estimates that only around 1 in 300 Aussies (0.33%)[3] will experience SAD during the “winter.”
Yes, SAD can occur for some people during summer and other seasons, but this is particularly rare compared to winter prevalence.
Common SAD symptoms include:
low mood for most of the day.
loss of interest in your usual activities.
drowsiness and low energy (lethargy).
fatigue, irritability, and severe mood swings.
Irregular sleep patterns (too much and/or too little)
eating more than usual, especially craving sugar and carbohydrates, leading to weight gain.
loss of interest in things you normally enjoy doing.
intrusive or disturbing thoughts.
Depression is not just a fancy word for feeling “bummed out”, and SAD is just as serious as any other depression and needs to be dealt with promptly and effectively. (See the end of the article for a list of mental health services links.)
“But how do I know the difference between general winter glumness, or if I’m being mauled by the SAD beast like Leo in the Revenant?”
Ask yourself these questions:
“Do you feel like you can’t get yourself out of this rut?”
“Have you lost an interest in things that you usually enjoy?”
“Have you felt this way for more than two weeks?”
If so, then it could be time to have a chat with a professional and perhaps seek treatment. Once again, SAD is just as real and can be just as devastating as Major Depressive Disorder; the only difference is the yearly regular onset.
This bitter beast can take over someone’s entire well-being, and if left untreated, the consequences can be devastating.
So let’s learn how we can slay the SAD, or even better, keep it in hibernation this year, so we nerds can continue to conquer all year round.
As with any injury or illness boss battle, you need to use the right medicine weapon to save the day. And there are many weapons you can equip yourself with to slay SAD.
Here is how to treat Seasonal Affective Disorder:
#1) GET SOME LIGHT
Light helps the body produce serotonin (hormone that affects mood) and reduces the production of melatonin (hormone that makes you sleepy).[4]
Starting with natural light is best, even though it’s not always easy.If the sun happens to be peeking out from the clouds, try and get outside for a nice walk. Even on cold or cloudy days, outdoor light can help, particularly in the morning. Just make sure you bundle up properly. The Norwegians have a saying “There is no bad weather, only bad clothing!”
Also, making your work and home environments as light and airy as possible and sitting near windows can help too.
If you feel you’re just simply not able to get enough natural light, ‘Light Therapy’is generally one of the first weapons picked up to slay SAD.[5] It can start alleviating symptoms in just a few days. It’s incredibly simple, and sitting under bright fluorescent globes or in front of a therapy lamp (again, particularly in the morning) has shown to be effective against SAD[6] (Anecdotal, but I once met a young woman who started to feel better just by increasing the wattage of her bedroom light globes).
Be forewarned that Light Therapy is not appropriate for everyone, including people with bipolar disorder – talk to a professional if this is a route you want to take.
#2) EXERCISE AND DIET
Surprise, surprise, our old friends come to the rescue once again. It’s clear[7] that exercise is key in keeping the blues at bay, so rug up and take a long walk, and be sure to work out when possible.
Exercise and other types of physical activity help relieve stress and anxiety, both of which can increase SAD symptoms.
If you’re really keen to take on winter, try the Winter Is Coming Workout, and start building that summer body early. For those who don’t like the freezing weather, that’s cool (get it?), you can always do Steve’s 20-minute hotel room workout (pro tip: you don’t actually need to be staying in a hotel room to do the workout… that was $250 I’ll never get back).
As for nutrition – while there is no well-established link between healthy nutritional practices and a reduction in SAD symptoms. BUT, studies HAVE shown links between healthy eating – like the Mediterranean diet – and a decrease in general depression.[8]
So anything we can do to eat healthy this time of year may certainly help.
Plus, Steve has already highlighted that if you’re going to eat unhealthy foods during winter, let’s at least be smart about it and negate the impact the holidays have on our waistlines. Try your best to provide a counterbalance to those comfort foods, and keep your diet as close as you can to what it is the rest of the year.
#3) GET SOME VITAMIN D
When exposure to sunlight is low, your body makes less Vitamin D.[9] According to this study,[10] Vitamin D deficiency affects nearly HALF of the world population. It is important for overall health. Our friends over at Examine say that if your diet is decent and there’s only one supplement you’re taking, it should probably be Vitamin D during these upcoming months.
The research is a little mixed when it comes to Vitamin D’s effectiveness in battling SAD,[11] but some studies[12] do show an improvement to everyone’s depression scale scores (those with or without SAD). Overall, if you aren’t getting enough sunlight in the winter, consider picking up some Vitamin D!
Recommendations differ for the amount of Vitamin D needed – or if you even need it – so further blood work and a talk with your doctor is a good choice here.
Meditation has been shown to help alleviate symptoms of depression.[13] Now, you don’t have to shed all your worldly possessions and go live in the mountains:
But if you’re suffering from the winter blues, a simple mindfulness practice may help. Even just a few minutes a day can go a long way.
If you want, Nerd Fitness Journey has a meditation adventure to help you build up the habit.
It’s free to try, right here:
#5) EMBRACE THE SEASON
Going back to foreign sayings – there’s a Danish concept of “hygge.”
While there’s no direct English translation, it essentially means coziness and comfort
Things like:
Wrapping yourself up in a blanket.
Enjoying a good book.
Or sitting by a warm fire.
So instead of lamenting the change of seasons – EMBRACE these other experiences that we get to enjoy.
#6) THERAPY
Talk Therapy (Psychotherapy) and cognitive behavioral therapy sound scary but really aren’t.
Psychotherapy focuses on helping you to build skills to deal with the stresses in your life, along with identifying and changing negative thinking patterns.
Therapies such as these assist with relearning some of the patterns and thoughts in your life that aren’t doing you any good.
It can feel daunting and really weird ‘opening up’ to a stranger at first.
But having a coach to talk through your negative thoughts and feelings, someone who can teach you to manage those better, is generally quite effective.
Most people will notice an improvement in as little as two weeks. Really, the “weird” stigma is usually the biggest barrier to even doing the thing in the first place!
#7) MEDICATION
Finally, some people with SAD benefit from antidepressant treatment, especially if symptoms are severe. We’re not here to offer any medical advice, so please see your doctor if you think medication may assist you.
It’s normal to have some days when you feel down, and the holiday season can be especially hard for some.
When short days and miserable weather are piled on top of this, it’s easy to see why ‘winter blues’ is so common. But if you feel down for days at a time and you can’t get motivated to do activities you normally enjoy, please speak to someone and see your doctor. This is especially important if your sleep patterns and appetite have changed, you feel a sense of hopelessness, you have intrusive thoughts, or you turn to alcohol/substances for comfort or relaxation.
Above all, take care of yourself this winter:
Be sure to get enough rest, and take the time to relax.
Reach out to a trusted friend, family member, or health professional if you feel you’re having a tough time.
And if someone reaches out to you, remember: We are Rebels, we fight conventional wisdom and smash stigmas. Never leave a fellow nerd behind.
If you feel the bitter, arctic beast starting to rise from its summer slumber, remember that you are not alone, and there are ways to slay the frosty fiend. You are strong enough to beat this, and the entire Rebellion has your back.
Want a little more from us?
If you want to continue your journey with Nerd Fitness, we have three great ways for you to do so:
#1) Our Online Coaching Program: a coaching program for busy people to help them make better food choices, stay accountable, and get healthier, permanently.
You can schedule a free call with our team so we can get to know you and see if our coaching program is right for you. Just click on the button below for more details:
#2) If you want an exact roadmap for getting fit, check out NF Journey. Our fun habit-building app helps you exercise more frequently, eat healthier, and level up your life (literally).
Plus, we have Missions specifically designed to help you stay active, no matter what the weather is like outside.
Try your free trial right here:
#3) Join the Rebellion! We need good people like you in our community, the Nerd Fitness Rebellion.
Sign up in the box below to enlist and get our Rebel Starter Kit, which includes all of our “work out at home” guides, the Nerd Fitness Diet Cheat Sheet, and much more!
Get your Nerd Fitness Starter Kit
The 15 mistakes you don’t want to make.
Full guide to the most effective diet and why it works.
Complete and track your first workout today, no gym required.
Alright, that does it for me. Rebels, take care of yourself and each other.
Do you have your own secret weapon to slay the SAD? We’d love to hear from all you Rebels about how you keep your mind healthy during winter; the more ideas we all have, the better! Let us know in the comments!
– Dan
PS – If you, or someone you know, would like further support, here are some excellent links and services that will get you started in the right direction:
The Virtual Center for Velo-Cardio-Facial Syndrome collaborates with the Center for Precision Neuropsychiatry based in the Department of Psychiatry at Columbia University Vagelos College of Physicians and Surgeons
Press Release –
updated: Oct 23, 2019
MANLIUS, N.Y., October 23, 2019 (Newswire.com)
– A landmark study is calling for at least 50 people in the U.S. with Velo-Cardio-Facial Syndrome (VCFS)-related psychosis to provide blood samples to create the world’s largest VCFS biobank to date of tiny spheres of neural tissue called “cerebral organoids.” Given that current medications used to treat VCFS-related psychosis are largely ineffective, researchers hope to discover novel and effective treatments for this condition by studying these cerebral organoids.
The Center for Precision Neuropsychiatry, founded by Sander Markx, M.D., and based in the Department of Psychiatry at Columbia University Vagelos College of Physicians and Surgeons, is collaborating in this research with the Virtual Center for Velo-Cardio-Facial Syndrome, founded by Robert J. Shprintzen, Ph.D. VCFS was first described in 1978 by Dr. Shprintzen and he was the first to report that psychosis is a common clinical feature of the syndrome.
VCFS, also known as DiGeorge syndrome, Shprintzen syndrome, and 22q11.2 Deletion Syndrome, is caused by a deletion of DNA from one copy of a specific region of chromosome 22 containing more than two dozen genes. It is the most common genetic multiple congenital anomaly syndrome and the most common genetic cause of psychosis. About one-third of people with VCFS develop psychosis and 1-2% of all patients with schizophrenia have a 22q11.2 microdeletion.
The researchers hope to learn more about how psychosis develops, how better treatments might be identified for this condition, and why people with VCFS develop mental illness at such a high rate. Ultimately, their intent is to develop effective treatments for people at high genetic risk for developing psychiatric illness.
A total of 50 participants with VCFS who are genetically confirmed to have a 22q11.2 deletion and are diagnosed with a psychotic disorder will be asked to provide a small blood sample for this study. In addition, the researchers will ask an unaffected first-degree family member of the donor (either same-sex sibling or same-sex parent) to contribute a blood sample to serve as a control subject. Phlebotomists will visit the participants to draw the blood in the comfort of their homes or location of their choice.
While some of the study participants will come from a pool of cases currently registered at the Virtual Center, more may be needed: the study is open to interested parties diagnosed with VCFS who live in the 48 U.S. contiguous states. VCFS patients who meet the requirements and want to participate in the study can register at www.vcfsmentalillness.org or email info@vcfscenter.org for further information.
Sander Markx, M.D., Assistant Professor of Psychiatry at Columbia University Vagelos College of Physicians and Surgeons and Principal Investigator, has a long-standing interest in VCFS. “We need to reach a better understanding of what goes on in the developing brain that ultimately gives rise to the increased risk for psychosis in patients with this genetic condition,” he states. “Improved understanding will help us develop novel, more efficacious medications that target specific disease mechanisms so we can achieve better clinical outcomes with fewer side effects for our patients. We hope that our process will guide future treatment for mental and cognitive disorders and ultimately reveal basic biology of debilitating disorders, such as schizophrenia and autism.”
As Robert J. Shprintzen, Ph.D., President and Chairman of the Board at the Virtual Center for VCFS, observes, “This study is of significant importance for sufferers of VCFS all over the world. Although VCFS is the most common genetic cause of psychosis and the genetic mutation that causes VCFS has been known for more than 25 years, so far, treatments for these problems have largely been ineffective. We expect that our collaborative research with eminent colleagues at one of the most highly regarded psychiatric facilities in the world will translate to more effective patient care.”
Additional information about the blood draw
The blood sample from the subject and his/her relative will be used to develop iPSCs and organoids to better understand VCFS biology and responses to medications. For each case, it will be determined whether he/she suffers from a psychotic condition. Following this initial study, the team plans to run clinical trials of medications that show promise in the organoid response.
The study will use induced pluripotent stem cells (iPSCs) obtained from donor blood. White blood cells are reprogrammed to become stem cells and those stem cells are grown into cerebral organoids, which will be exposed to drug libraries to determine how the brain tissue responds. This type of research, called translational research, yields results that could ultimately help lead to the identification and development of new treatments for this debilitating condition.
About The Virtual Center for Velo-Cardio-Facial Syndrome, Inc.
The Virtual Center for Velo-Cardio-Facial Syndrome, Inc. is an open-access 501(c)3, internet-based charitable organization that provides personalized information to people whose lives have been touched by VCFS and who are seeking applicable research and clinical expertise regarding the management of the syndrome. There is no charge for this service, which is funded by voluntary donations.
About Velo-Cardio-Facial Syndrome
Velo-Cardio-Facial syndrome (VCFS) is the most common genetic multiple congenital anomaly disorder in humans. It is caused by a microdeletion of DNA from chromosome 22, typically encompassing approximately 40 genes. It is known by a number of other names, including DiGeorge syndrome, conotruncal anomalies face syndrome, Sedlačková syndrome and, more recently, 22q11.2 Deletion Syndrome. Approximately 200 distinct congenital anomalies and disorders are associated with VCFS. Recent data has shown that more than 1 in every 1,000 pregnancies have the deletion from chromosome 22 that causes VCFS. Because so many problems can occur in people with VCFS, it is difficult to have all of the specialists with special knowledge of the syndrome needed for required diagnosis and management together in one location. The Virtual Center allows experts to spread knowledge and information pertinent to individual cases anywhere in the world, thereby sharing expertise and educating local practitioners at the same time.
Press Contacts:
The Virtual Center for Velo-Cardio-Facial Syndrome, Inc.
Robert J. Shprintzen, Ph.D. E-mail: info@vcfscenter.com Tel: 315-559-4685 Web: www.vcfsmentalillness.org
Fortress Strategic Communications for The Virtual Center for Velo-Cardio-Facial Syndrome, Inc.
Evan Bloom, CEO Tel: 315-744-4912 E-mail: evan@fortresscomms.com Web: www.fortresscomms.com
Source: The Virtual Center for Velo-Cardio-Facial Syndrome, Inc.


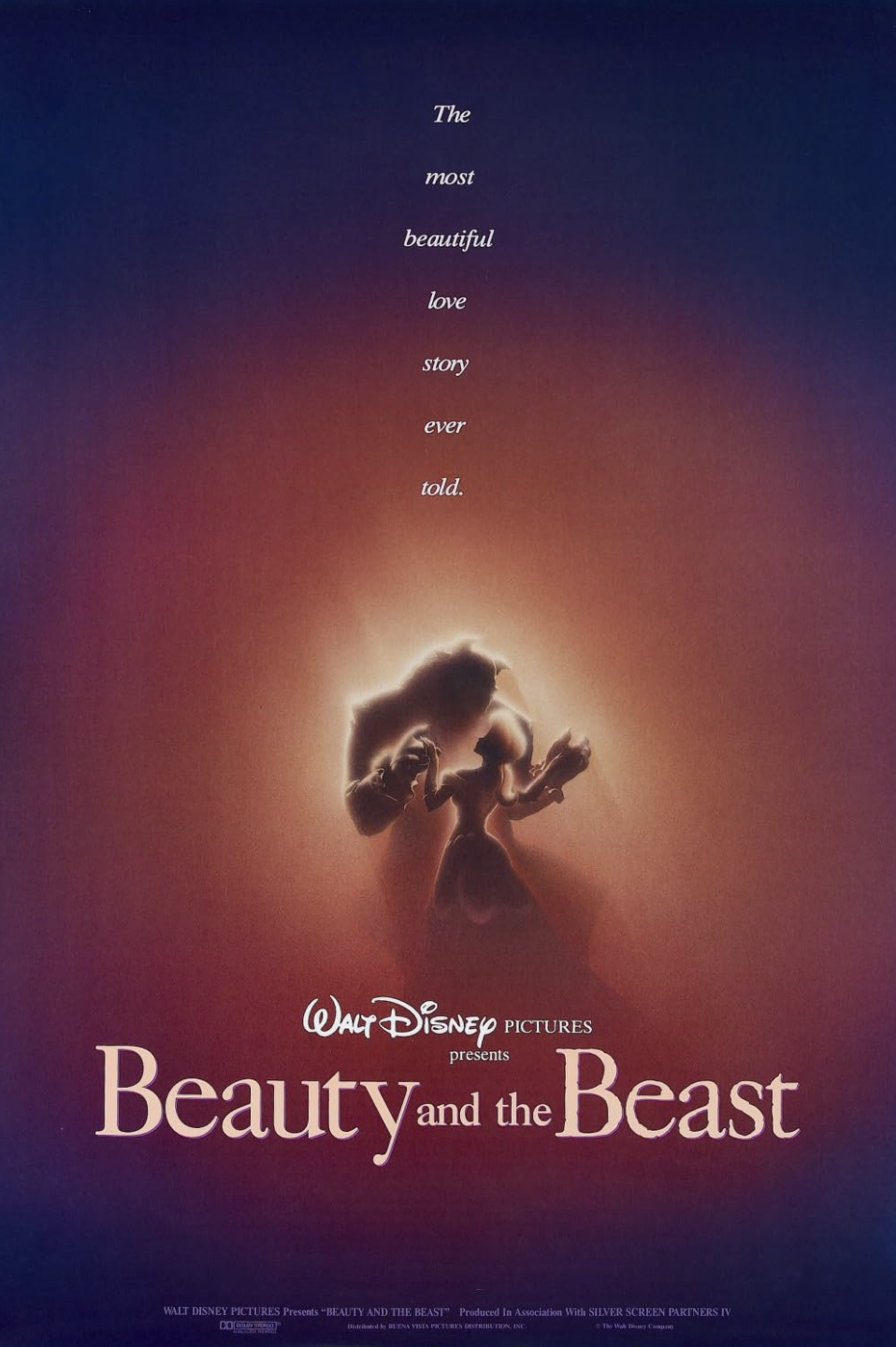
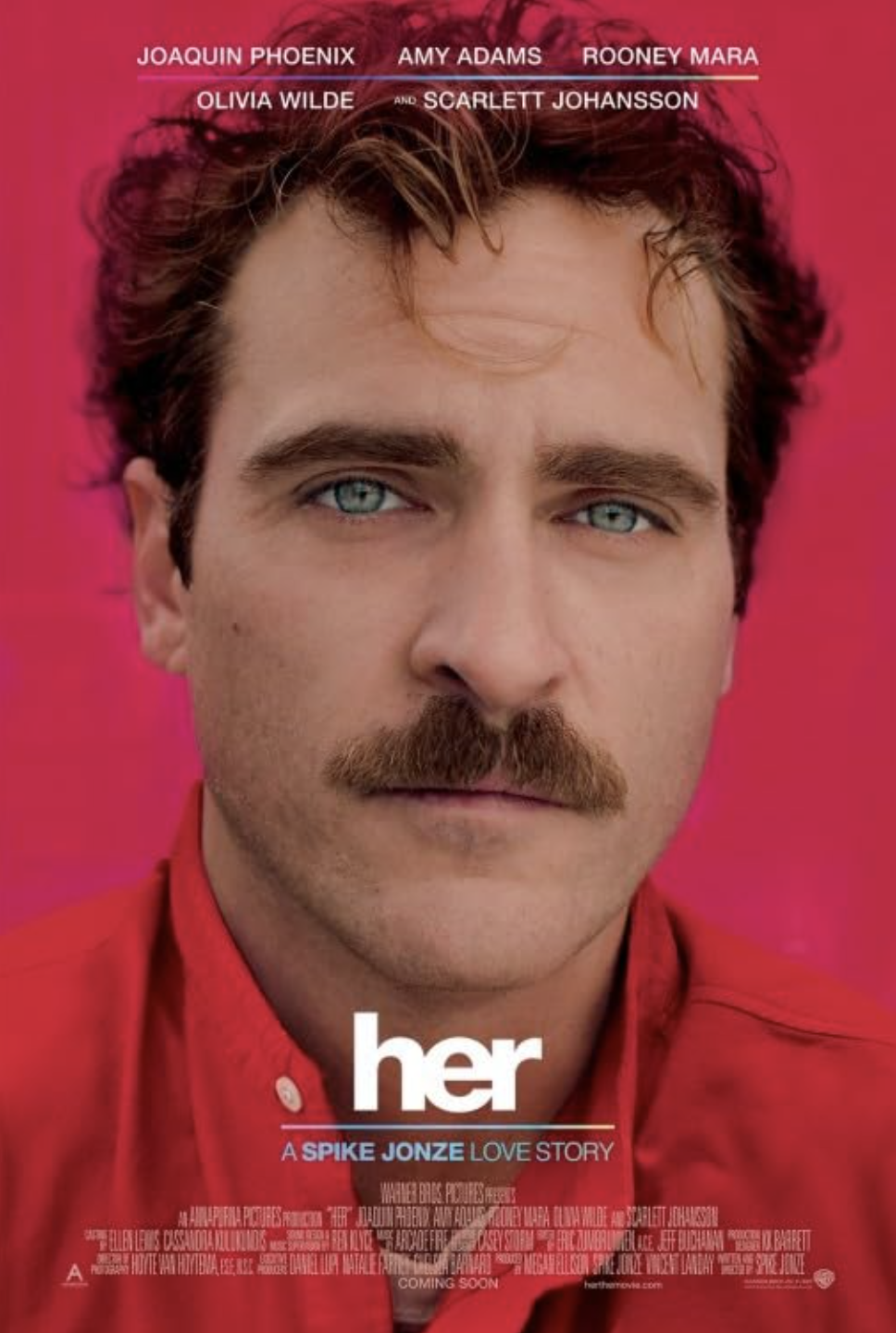
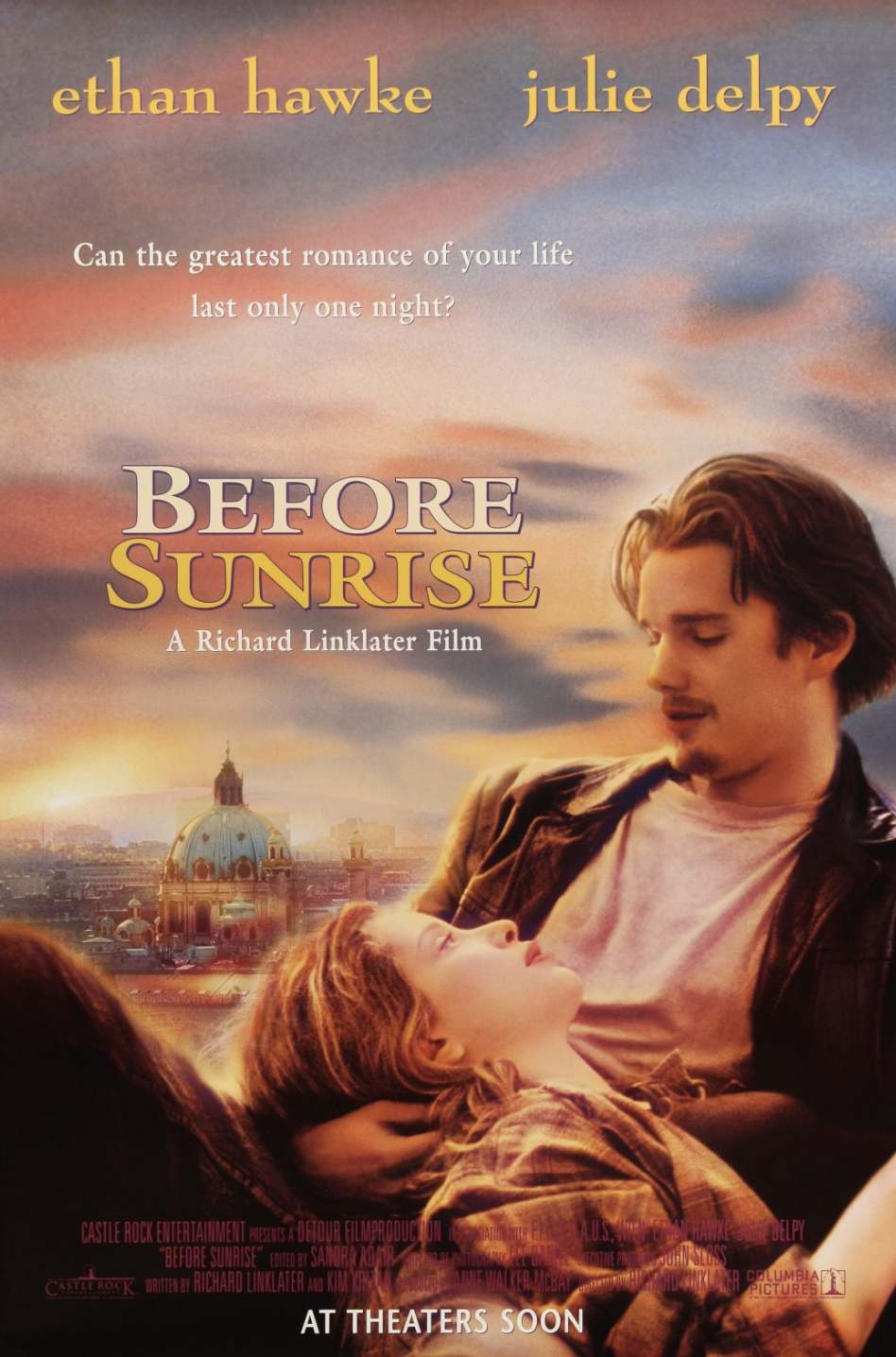
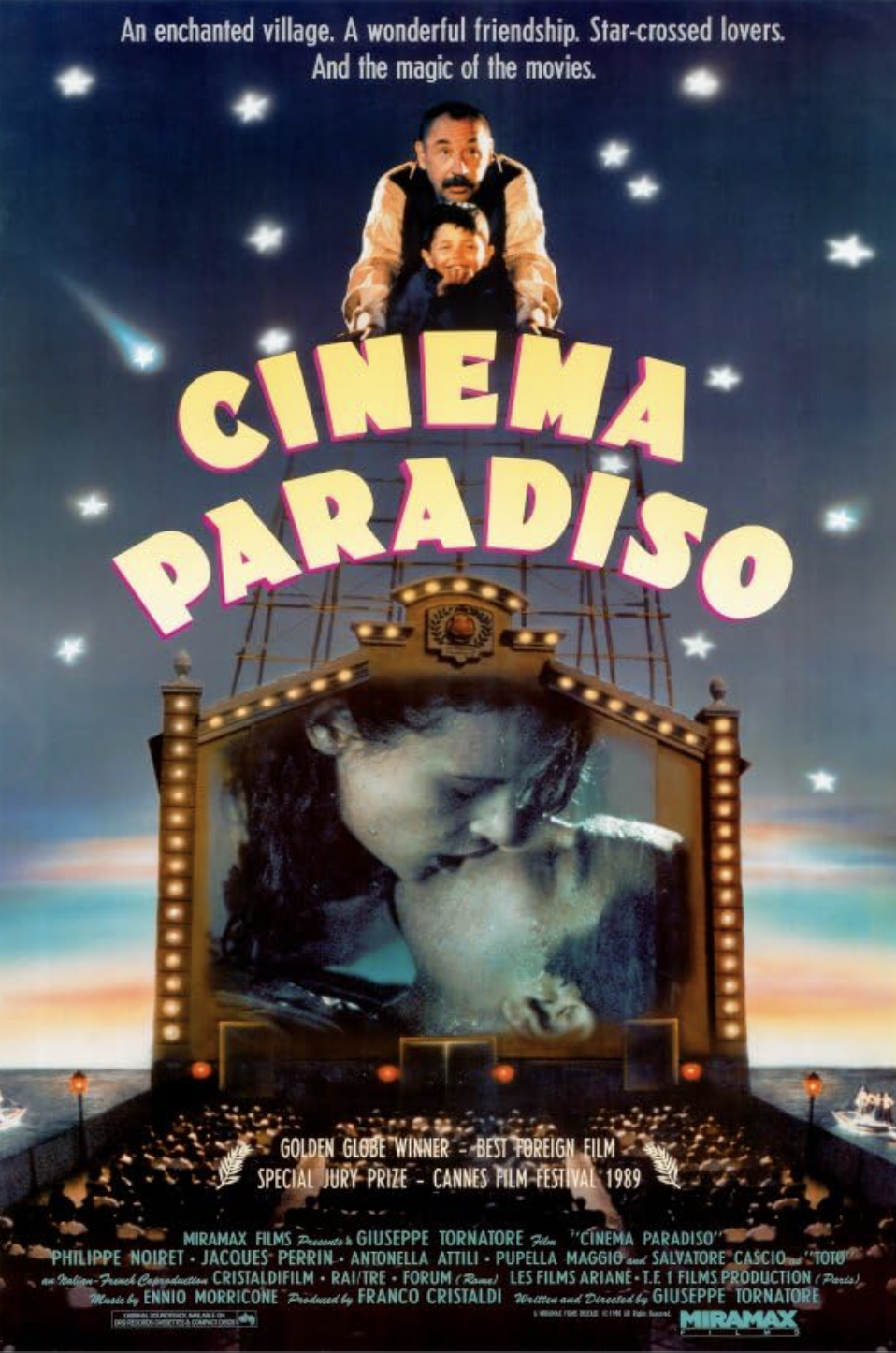










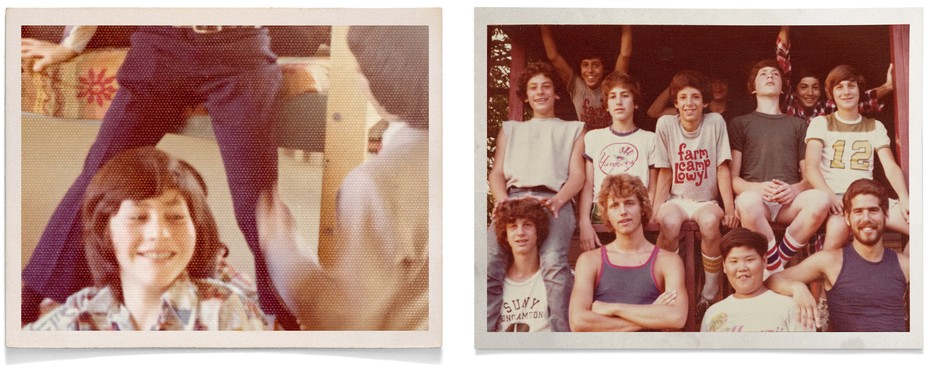
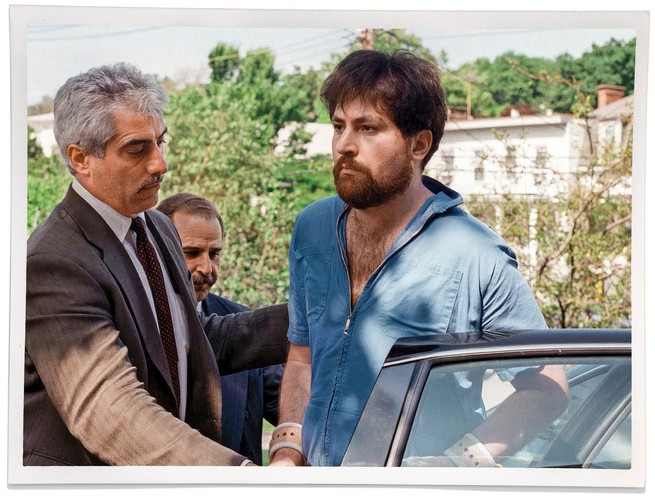

 Through adolescence and into adulthood, we may not experience unconditional love, either. Competition at school, the workplace, in sports, in social circles, and even in entertainment and arts — all contribute to a society that constantly compares. Someone is “better” (which means someone else is “worse”), someone wins while others lose, some people presumably succeed and others fail. This message is everywhere — in popular media, in advertising, and in our language. We are expected to behave, think, and feel in particular ways, or be shunned, minimized, ignored, or condemned.
Through adolescence and into adulthood, we may not experience unconditional love, either. Competition at school, the workplace, in sports, in social circles, and even in entertainment and arts — all contribute to a society that constantly compares. Someone is “better” (which means someone else is “worse”), someone wins while others lose, some people presumably succeed and others fail. This message is everywhere — in popular media, in advertising, and in our language. We are expected to behave, think, and feel in particular ways, or be shunned, minimized, ignored, or condemned.