If an alien life form landed on Earth tomorrow and called up some of the planet’s foremost experts on lactation, it would have a heck of time figuring out what, exactly, humans and other mammals are feeding their kids.
The trouble is, no one can really describe what milk is—least of all the people who think most often about it. They can describe, mostly, who makes it: mammals (though arguably also some other animals that feed their young secretions from their throat or their skin). They can describe, mostly, where it comes from: mammary glands via, usually, nipples (though please note the existence of monotremes, which ooze milk into abdominal grooves). They can even describe, mostly, what milk does: nourish, protect, and exchange chemical signals with infants to support development and growth.
But few of these answers get at what milk, materially, compositionally, is actually like. Bridget Young, an infant-nutrition researcher at the University of Rochester, told me milk was an “ecological system”; Alan S. Ryan, a clinical-research consultant, called it a “nutritional instrument.” Bruce German, a food scientist at UC Davis, told me milk was “the result of the evolutionary selective pressure on a unique feeding strategy,” adding, by way of clarification, that it was “a biological process.” A few researchers defaulted to using milk to explain something else. “It’s the defining feature of mammals,” says Melanie Martin, an anthropologist at the University of Washington. None of these characterizations were bad. But had I been that alien, I would have no idea what these people were talking about.
Read: We’ve never been good at feeding babies
What these experts were trying to avoid was categorizing milk as a “food”—the way that most people on Earth might, especially in industrialized countries where dairy products command entire supermarket aisles. “Overwhelmingly, when we think about milk, when we talk about milk, we think of nutrition,” says Katie Hinde, an evolutionary biologist at Arizona State University. That’s not the wrong way to think about it. But it’s also not entirely right.
The milk that mammals make is undoubtedly full of the carbs, fat, protein, vitamins, and minerals newborn mammals need to survive. And, across species, much of it does resemble the creamy, tart-tangy, lactose-rich whitish liquid that billions of people regularly buy. But to consider only milk’s nutrient constituents—to imply that it has a single recipe—is to do it “a disservice,” German told me. Mammalian milk is a manifestation of hundreds of millions of years of evolutionary tinkering that have turned it into a diet, and a developmental stimulus, and a conduit for maternal-infant communication, and a passive vaccine. It builds organs, fine-tunes metabolism, and calibrates immunity; it paints some of an infant’s first portraits of its mother, and telegraphs chemical signals to the microbes that live inside the gut. Milk can sustain echidnas that hatch from eggs, and wildebeest that can gallop within hours of birth; it can support newborn honey possums that weigh just three milligrams at birth, and blue-whale calves clocking in at up to 20 tons. Among some primates, it influences infants’ playfulness, and may shape their sleep habits and bias them toward certain foods. Some of its ingredients are found nowhere else in nature; others are indigestible, still others are alive.
Milk is also dynamic in a way that no other fluid is. It remodels in the hours, days, weeks, and months after birth; it changes from the beginning of a single stint of feeding to the end. In humans, scientists have identified “morning” milk that’s high in cortisol, and “night” milk that’s heavy in melatonin; certain primates have “boy milk and girl milk,” German told me, which support subtly different developmental needs. Tammar wallabies, which can nurse two joeys of different ages at once, even produce milks tailored to each offspring’s developmental stage; Kevin Nicholas, a biologist at Monash University, has found that when the joeys swap teats, the younger sibling’s growth accelerates. And when mothers and their offspring change, milk changes in lockstep. It reflects the mother’s stress level and physical health, taking on new flavors as her diet shifts; its fat content fluctuates, depending on how far apart bouts of nursing are spaced. Scientists are just beginning to understand how made-to-order milk might be: Some evidence suggests that maternal tissues may register, via the breast, when infants catch infections—and modify milk in real time to furnish babies with the exact immune cells or molecules they need.
“It’s a triad: mother, milk, and infant,” says Moran Yassour, a computational biologist at Hebrew University of Jerusalem. “Each one of them is playing a role, and the milk is active.” That dynamism makes milk both a miracle, and an enduring mystery—as unique and unreplicable as any individual parent or child, and just as difficult to define.
In its earliest forms, milk probably didn’t have much nutritional value at all. Scientists think the substance’s origins date back about 300 million years, before the rise of mammals, in a lineage of creatures that hatched their young from very delicate eggs. The structures that would later develop into mammary glands started out similar to the ones we use to sweat; the substance that would become proper milk pooled on the surface of skin and was slathered onto shells. The earliest milks probably had few calories and almost none of its hallmark lactose. But they were deeply hydrating, and teeming with immunity.
As our ancestors jettisoned egg laying for live birth, they began to extrude milk not just as a defensive shield for their offspring, but as a source of calories, vitamins, and minerals. The more that milk offered to infants, the more that it demanded of those that produced it: Mothers “dissolve themselves to make it,” German told me, liquefying their own fat stores to keep their babies fed, “which is impressive and scary at the same time.” In its many modern manifestations, milk is, in every mammal that produces it, a one-stop shop for newborn needs—“the only real time in life where we have hydration, nutrients, and bioactive factors that are all a single source,” says Liz Johnson, an infant-nutrition researcher at Cornell.
Each time mammals have splintered into new lineages, taking on new traits, so too has their milk. While most primates and other species that can afford to spend months doting on their young produce dilute, sugary milks that can be given on demand, other mammals have evolved milk that encourages more independence and is calorific enough to nourish in short, ultra-efficient bursts. Hooded seals, which have to wean their pups within four days of birth, churn out goopy milk that’s nearly sugar-free, but clocks in at about 60 percent fat—helping their offspring nearly double in weight by the time they swim away. Marsupial milk, meanwhile, is ultra-sweet, with double or triple the sugar content of what cows produce, and cottontail rabbits pump out a particularly protein-rich brew. (One thing milk can’t do? Be high in both sugar and fat, says Mike Power, a biological anthropologist at the Smithsonian Conservation Biology Institute, where he maintains a large repository of mammalian milk: “Nature has never been able to produce ice cream.”) Each species’ milk even has its own microbiome—a community of helpful bacteria that goes on to seed the newborn infant’s gut. Mammal milks are now so specialized to their species that they can’t substitute for one another, even between species that otherwise live similar lives.
Human milk—like other primate milk—is on the watery, sugary side. But its concentrations of immunity-promoting ingredients have no comparator. It bustles with defensive cells; it shuttles a stream of antibodies from mother to young, at levels that in some cases outstrip those of other great apes’ milk by a factor of at least 10. Its third-most-common solid ingredient is a group of carbohydrates known as human milk oligosaccharides, or HMOs, which aren’t digestible by our own cells but feed beneficial bacteria in the colon while keeping pathogens out. Roughly 200 types of oligosaccharides have been found in human milk—an inventory with more diversity, complexity, and nuance than that of any other mammalian species described to date, says Concepcion Remoroza, a chemist who’s cataloging the HMOs of different mammalian milks at the National Institute of Standards and Technology.
The sheer defensive firepower in our species’ milk is probably a glimpse into the challenges in our past, as humans crowded together to plant, fertilize, and harvest mass quantities of food, and invited domesticated creatures into our jam-packed homes. “We were basically concentrating our pathogens and our parasites,” Power told me, in ways that put infants at risk. Perhaps the millennia modified our milk in response, making those unsanitary conditions possible to survive.
Mammals would not exist without their milk. And yet, “we don’t actually know that much about milk,” down to the list of its core ingredients in our own species, says E. A. Quinn, an anthropologist at Washington University in St. Louis. Even for the breast-milk components that scientists can confidently identify, Quinn told me, “we don’t really have a good handle on what normal human values are.” Many studies examining the contents of breast milk have focused on Western countries, where the population skews wealthier, well nourished, and white. But so much varies from person to person, from moment to moment, that it’s tough to get a read on what’s universally good; likely, no such standard exists, at least not one that can apply across so many situations, demographics, and phases of lactation, much less to each infant’s of-the-moment needs.
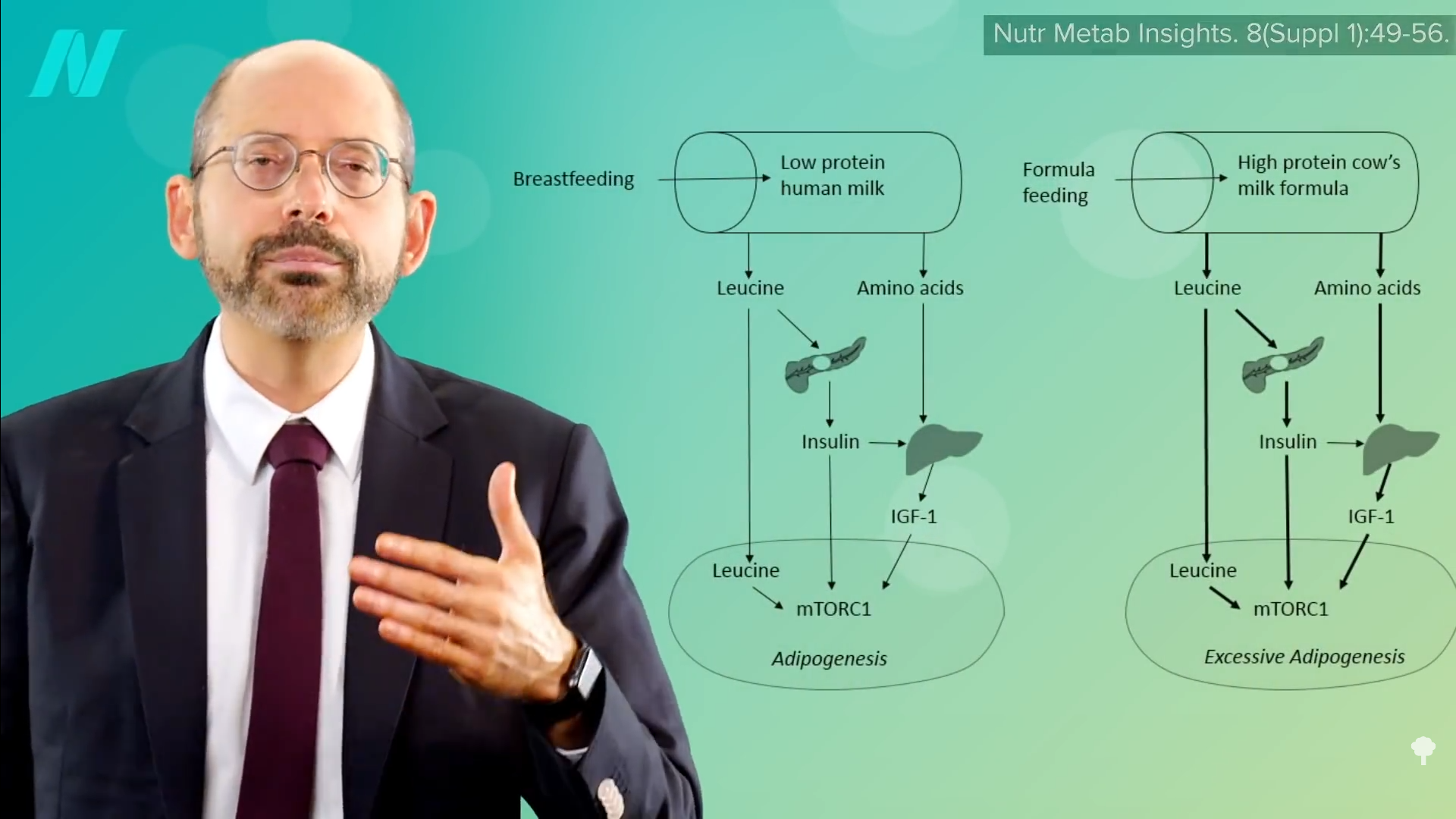
Milk’s enduring enigmas don’t just pose an academic puzzle. They also present a frustrating target—simultaneously hazy and mobile—for infant formulas that billions of people rely on as a supplement or substitute. Originally conceived of and still regulated as a food, formula fulfills only part of milk’s tripartite raison d’etre. Thanks to the strict standards on carb, fat, protein, vitamin, and mineral content set by the FDA and other government agencies, modern formulas—most of which are based on skim cow’s milk—do “the nourish part really well,” helping babies meet all their growth milestones, Bridget Young, the University of Rochester infant nutrition researcher, told me. “The protect and communicate part is where we start to fall short.” Differences in health outcomes for breastfed and formula-fed infants, though they’ve shrunk, do still exist: Milk-raised babies have, on average, fewer digestive troubles and infections; later in life, they might be less likely to develop certain metabolic issues.
Read: What parents did before baby formula
To close a few of those gaps, some formula companies have set their sights on some of milk’s more mysterious ingredients. For nearly a decade, Abbott, one of the largest manufacturers of formula in the United States, has been introducing a small number of HMOs into its products; elsewhere, scientists are tinkering with the healthful punch via live bacterial cultures, à la yogurt. A few are even trying a more animal-centric route. The company ByHeart uses whole cow’s milk as its base, instead of the more-standard skim. And Nicholas, the Monash University biologist, is taking inspiration from wallaby milk—complex, nutritious, and stimulating enough to grow organs of multiple species almost from scratch—which he thinks could guide the development of formulas for premature human infants not yet ready to subsist solely on mature milk.
All of these approaches, though, have their limits. Of the 200 or so HMOs known to be in human milk, companies have managed to painstakingly synthesize and include just a handful in their products; the rest are more complex, and even less well understood. Getting the full roster into formula will “never happen,” Sharon Donovan, a nutritional scientist at the University of Illinois at Urbana-Champaign, told me. Other protein- and fat-based components of milk, specially packaged by mammary glands, are, in theory, more straightforward to mix in. But those ingredients might not always behave as expected when worked onto a template of cow’s milk, which just “cannot be compared” to the intricacies of human milk, Remoroza told me. (In terms of carbs, fats, and protein, zebra milk is, technically, a better match for us.)
A company called Biomilq is trying a radical way to circumvent cows altogether: It’s in the early stages of growing donated human-mammary-gland cells in bioreactors, in hopes of producing a more recognizable analogue for breast milk, ready-made with our own species-specific mix of lactose, fats, and proteins, and maybe even a few HMOs, Leila Strickland, one of Biomilq’s co-founders, told me. But even Strickland is careful to say that her company’s product will never be breast milk. Too many of breast milk’s immunological, hormonal, and microbial components come from elsewhere in the mother’s body; they represent her experience in the world as an entire person, not a stand-alone gland. And like every other milk alternative, Biomilq’s product won’t be able to adjust itself in real time to suit a baby’s individual needs. If true milk represents a live discourse between mother and infant, the best Biomilq can manage will be a sophisticated, pretaped monologue.
Read: A bold and controversial idea for making breast milk
For all the ground that formula has gained, “no human recipe can replicate what has evolved” over hundreds of millions of years, Martin, of the University of Washington, told me. That may be especially true as long as formula continues to be officially regarded as a food—requiring it to be, above all else, safe, and every batch the same. Uniformity and relative sterility are part and parcel of mass production, yet almost antithetical to the variation and malleability of milk, Cornell’s Johnson told me. And in regulatory terms, foods aren’t designed to treat or cure, which can create headaches for companies that try to introduce microbes and molecules that carry even a twinge of additional health risk. Float the notion of a very biologically active addition like a growth factor or a metabolic hormone, and that can quickly “start to scare people a bit,” Donovan, of the University of Illinois at Urbana-Champaign, told me.
As companies have vied to make their formulas more milk-esque and complex, some experts have discussed treating them more like drugs, a designation reserved for products with proven health impact. But that classification, too, seems a poor fit. “We’re not developing a cure for infancy,” Strickland, of Biomilq, told me. Formula’s main calling is, for now, still to “promote optimal growth and development,” Ryan, the research consultant, told me. Formula may not even need to aspire to meet milk’s bar. For babies that are born full-term, who remain up-to-date on their vaccinations and have access to consistent medical care, who are rich in socioeconomic support, who are held and doted on and loved—infants whose caregivers offer them immunity, resources, and guidance in many other ways—the effect of swapping formula for milk “is teeny,” Katie Hinde, of Arizona State University, told me. Other differences noted in the past between formula- and breastfed infants have also potentially been exaggerated or misleading; so many demographic differences exist between people who are able to breastfeed their kids and those who formula-feed that tracing any single shred of a person’s adult medical history back to their experiences in infancy is tough.
The biggest hurdles in infant feeding nowadays, after all, are more about access than tech. Many people—some of them already at higher risk of poorer health outcomes later in life—end up halting breastfeeding earlier than they intend or want to, because it’s financially, socially, or institutionally unsustainable. Those disparities are especially apparent in places such as the U.S., where health care is privatized and paid parental leave and affordable lactation consultants are scarce, and where breastfeeding rates splinter unequally along the lines of race, education, and socioeconomic status. “Where milk matters the most, breastfeeding tends to be supported the least,” Hinde told me. If milk is a singular triumph of evolution, a catalyst for and a product of how all mammals came to be, it shouldn’t be relegated to a societal luxury.