[ad_1]
More than 99% of people who suffer a heart attack, stroke, or heart failure have at least one risk factor beforehand—yet many have no idea until it’s too late. That’s part of the reason why heart disease has been the leading cause of death in the U.S. since at least 1950. Now, scientists hope that a new generation of tools—like a first-of-its-kind risk calculator—can turn those invisible warning signs into something people can see, understand, and act on years before the worst-case scenario strikes.
“This is a disease that’s impacted by choices we make in life. And I think that we as humans can make wiser choices if we understand our risk—and perhaps even more importantly, if we understand the connection between risk and the choices that we make,” says Dr. Matthew Tomey, a cardiologist at Mount Sinai Fuster Heart Hospital. “Understanding and communicating risk are profoundly difficult things to do, and it’s especially difficult for individuals who are younger and feel fine.”
Here’s a look at the new science of predicting heart risk, and what challenges remain.
A new way to assess risk earlier
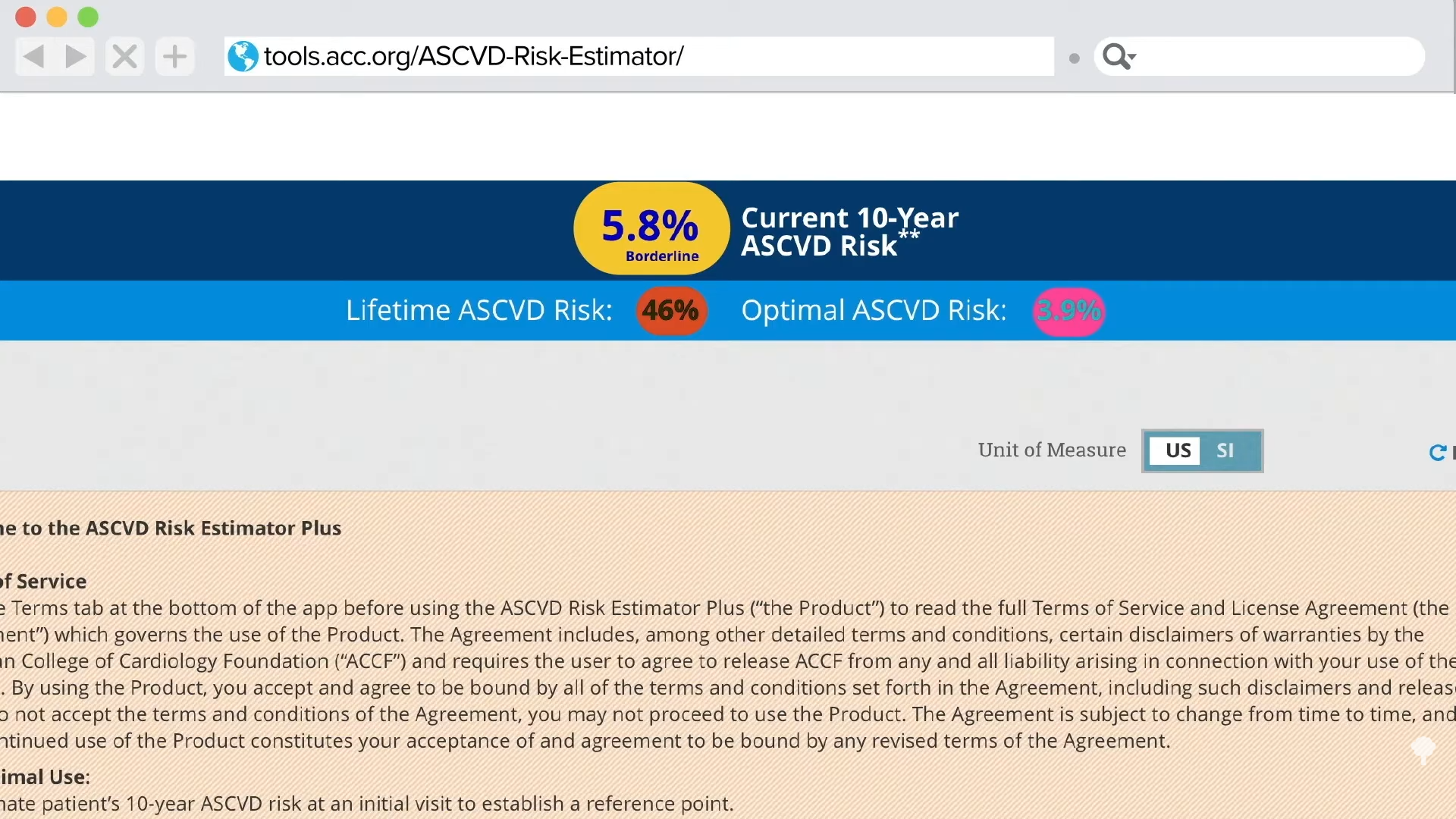
In a study published in 2025 in the Journal of the American College of Cardiology, researchers introduced a free online calculator that calculates a person’s 30-year risk of developing heart disease. It’s designed for adults ages 30 to 59, and people should ideally use it once a year, says senior study author Dr. Sadiya Khan, a professor of cardiovascular epidemiology at Northwestern Medicine.
The new calculator—which is based on the American Heart Association’s PREVENT equations—is an update to an older tool that estimated a person’s 10-year risk of a first-time atherosclerotic cardiovascular disease event, like a heart attack or stroke. The old version was geared toward people 40 or over, and research found that it often failed to identify a significant proportion of the people who ultimately went on to experience a heart attack.
Read More: What to Do If Your High Cholesterol Is Genetic
In addition to including younger adults and forecasting predictions further into the future, the new model predicts a broader range of outcomes, including heart failure.
“It’s really trying to push the envelope on prevention starting earlier,” Khan says. “We know that more and more young adults are facing obesity or diabetes or hypertension, and we want to make sure we’re starting that conversation early, so we’re not waiting until someone has a heart attack or presents in heart failure.”
The calculator is straightforward, as long as you have key health metrics in hand. Users plug in data like sex, age, body mass index, blood pressure, cholesterol, smoking status, and diabetes history, and then—based on that snapshot of their current stats—they’re provided with both a 10-year and 30-year percentage risk for developing heart disease.
The value of taking early action
Many experts consider the new online calculator a promising addition to the repertoire of tools available to help prevent heart disease. It’s meant to inspire conversations with clinicians, not replace care—an important distinction, says Dr. Nishant Shah, a preventive cardiologist at Duke University Medical Center.
The earlier these conversations start, the better, Shah says. He starts talking with people about their risk for heart disease around age 18, especially if they have a strong family history of disease. Online, easy-to-access tools like the calculator can open the door to those conversations—and meaningful change. “Talking about these things with patients before a problem happens is crucial,” he says. After patients learn their heart disease risk score, he educates them on preventive steps they can take, like exercising regularly, following a good diet, getting enough sleep, starting a medication like a statin if warranted, and keeping up with blood pressure and cholesterol screenings. “These are all really important things to prevent a surprise,” he says. “A story I hear a lot is, ‘He or she was doing great yesterday, and then today they just woke up dead.’ That’s what we’re trying to avoid.”
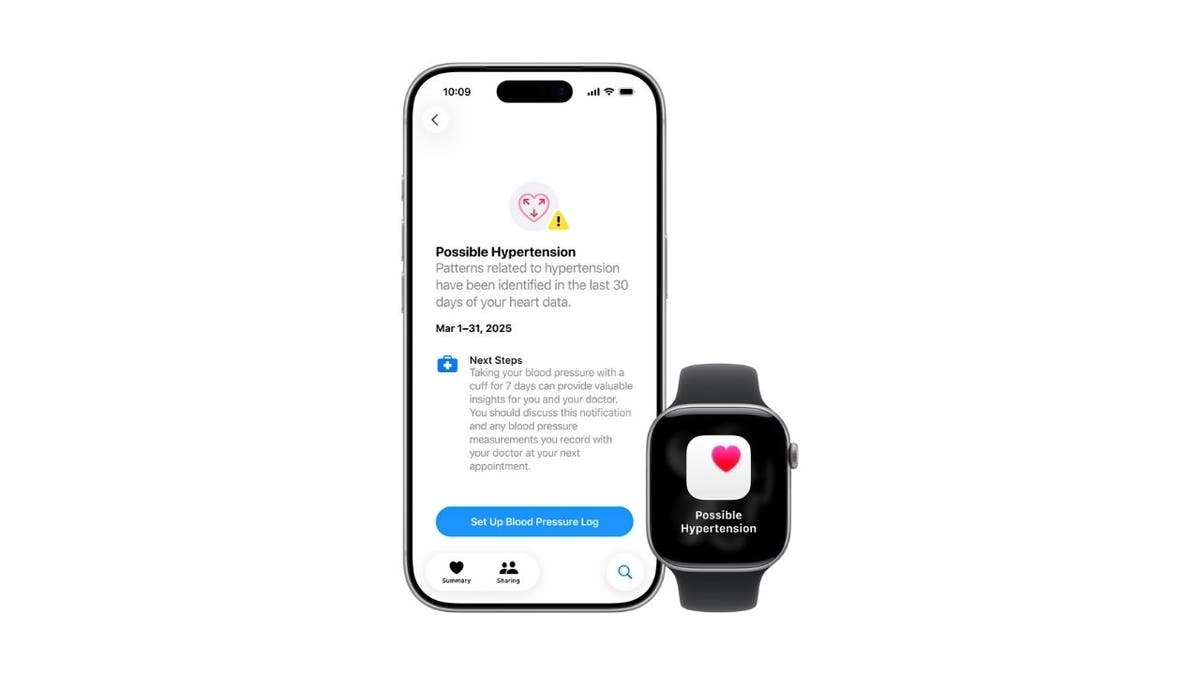
One of the key reasons why tools that predict risk can be so helpful is that many people simply aren’t aware of their likelihood of developing heart disease. “A lot of these risk factors are silent,” Shah says. “Someone could be running around with high blood pressure, and they’re not going to feel the effects of it until it gets super high. People don’t feel like something’s wrong; it’s different from if you have a rash on your face.” For some people, he adds, quantifying risk is all it takes to get engaged with protecting their heart—and potentially saving their life.
Lingering pain points
No single risk assessment will ever perfectly predict someone’s chance of having a heart event.
“By necessity, there’s no risk calculator that incorporates every relevant variable,” Tomey says. “The PREVENT equations are a really admirable advance in risk prediction, but they’re parsimonious in the number of variables and the nature of variables that they include.”
Other relevant factors, he says, include whether someone has calcification of a coronary artery or plaque in an artery; genetic risks; high levels of lipoprotein(a); and inflammation metrics, including C-reactive protein. It also doesn’t account for most lifestyle factors, like exercise and sleep quality. All of these “might be important asterisks in any number you get from the calculator,” says Tomey, whose research has found that the PREVENT equations underestimate risk in some people. “We can’t just hang our hats on scores like this,” he says. “It’s really important to understand the value that they bring, but they’re not some sort of guarantee of protection if you have a lower score.”
Plus, risk scores in general resonate differently depending on the person. Some people take them seriously, while others shrug them off or misunderstand them. These scores are “only fruitful in so much as they motivate you to make healthy choices,” Tomey says. If learning your risk score propels you to take stock of your daily choices, and how you can get healthier, then “that’s something that can materially improve individual health and public health.” Otherwise, it’s just a number.
A multi-pronged approach
There are other ways to predict heart risk, too. Some people benefit from knowing their coronary artery calcium score, for example, which is produced by a low-dose CT scan that detects calcium buildup in the heart’s arteries. That test can help diagnose early coronary artery disease and is often recommended for people with a family history of disease.
Compared to a risk calculator, “neither is superior,” says Dr. Luke Laffin, a preventive cardiologist at the Cleveland Clinic. “They’re complementary.”
In practice, doctors rarely rely on a single test. Regular checkups and labs are still informative, and some people benefit from stress tests, echocardiograms, and advanced lipid testing—like for lipoprotein(a) and apolipoprotein B. Clinicians can also assess risk through taking a thorough family history and understanding lifestyle patterns.
Read More: 9 Weird Symptoms Cardiologists Say You Should Never Ignore
No matter which tool or test makes the most sense, having a meaningful understanding of individual heart-disease risk gives people a chance to intervene sooner rather than later. “Everyone should have their cardiovascular risk calculated,” Laffin says. He says he’s seeing interest increase: As people become more invested in longevity, more younger people are showing up in his office and saying, “My dad died of a heart attack or had a heart attack in his 50s. What can I do to not befall that fate?”
“There are all kinds of ways to calculate risk, but this PREVENT calculator is the most contemporary version that we have,” Laffin says. “I’d encourage people to talk with their doctor about their risk, and that can help guide conversations about preventive actions they can take.”
[ad_2]
Angela Haupt
Source link