Sixty-five percent of educators use AI to bridge resource gaps, even as platform fatigue and a lack of system integration threaten productivity, according to Jotform‘s EdTech Trends 2026 report.
Based on a survey of 50 K-12 and higher education professionals, the report reveals a resilient workforce looking for ways to combat the effects of significant budget cuts and burnout. The respondents were teachers, instructors, and professors split about equally between higher education and K-12.
While 56 percent of educators are “very concerned” over recent cuts to U.S. education infrastructure, 65 percent are now actively using AI. Of those using AI, nearly half (48 percent) use it for both student learning and administrative tasks, such as summarizing long documents and automating feedback.
“We conducted this survey to better understand the pain points educators have with technology,” says Lainie Johnson, director of enterprise marketing at Jotform. “We were surprised that our respondents like their tech tools so much. Because while the tools themselves are great, their inability to work together causes a problem.”
Key findings from the EdTech Trends 2026 report include:
The integration gap: Although 77 percent of educators say their current digital tools work well, 73 percent cite a “lack of integration between systems” as their primary difficulty. “The No. 1 thing I would like for my digital tools to do is to talk to each other,” one respondent noted. “I feel like often we have to jump from one platform to another just to get work done.”
Platform fatigue: Educators are managing an average of eight different digital tools, with 50 percent reporting they are overwhelmed by “too many platforms.”
The burden of manual tasks: Despite the many digital tools they use, educators spend an average of seven hours per week on manual tasks.
AI for productivity: Fifty-eight percent of respondents use AI most frequently as a productivity tool for research, brainstorming, and writing.
Data security and ethics: Ethical implications and data security are the top concerns for educators when implementing AI.
eSchool Media staff cover education technology in all its aspects–from legislation and litigation, to best practices, to lessons learned and new products. First published in March of 1998 as a monthly print and digital newspaper, eSchool Media provides the news and information necessary to help K-20 decision-makers successfully use technology and innovation to transform schools and colleges and achieve their educational goals.
The extent of risk from bariatric weight-loss surgery may depend on the skill of the surgeon.
After sleeve gastrectomy and Roux-en-Y gastric bypass, the third most common bariatric procedure is a revision to fix a previous bariatric procedure, as you can see below and at 0:16 in my video The Complications of Bariatric Weight-Loss Surgery.
Up to 25% of bariatric patients have to go back into the operating room for problems caused by their first bariatric surgery. Reoperations are even riskier, with up to 10 times the mortality rate, and there is “no guarantee of success.” Complications include leaks, fistulas, ulcers, strictures, erosions, obstructions, and severe acid reflux.
The extent of risk may depend on the skill of the surgeon. In a study published in The New England Journal of Medicine, bariatric surgeons voluntarily submitted videos of themselves performing surgery to a panel of their peers for evaluation. Technical proficiency varied widely and was related to the rates of complications, hospital readmissions, reoperations, and death. Patients operated on by less competent surgeons suffered nearly three times the complications and five times the rate of death.
“As with musicians or athletes, some surgeons may simply be more talented than others”—but practice may help make them perfect. Gastric bypass is such a complicated procedure that the learning curve may require 500 cases for a surgeon to master the procedure. Risk for complications appears to plateau after about 500 cases, with the lowest risk found among surgeons who had performed more than 600 bypasses. The odds of not making it out alive may be double under the knife of those who had performed less than 75 compared to more than 450, as seen below and at 1:47 in my video.
So, if you do choose to undergo the operation, I’d recommend asking your surgeon how many procedures they’ve done, as well as choosing an accredited bariatric “Center of Excellence,” where surgical mortality appears to be two to three times lower than non-accredited institutions.
It’s not always the surgeon’s fault, though. In a report entitled “The Dangers of Broccoli,” a surgeon described a case in which a woman went to an all-you-can-eat buffet three months after a gastric bypass operation. She chose really healthy foods—good for her!—but evidently forgot to chew. Her staples ruptured, and she ended up in the emergency room, then the operating room. They opened her up and found “full chunks of broccoli, whole lima beans, and other green leafy vegetables” inside her abdominal cavity. A cautionary tale to be sure, but perhaps one that’s less about chewing food better after surgery than about chewing better foods before surgery—to keep all your internal organs intact in the first place.
Even if the surgical procedure goes perfectly, lifelong nutritional replacement and monitoring are required to avoid vitamin and mineral deficits. We’re talking about more than anemia, osteoporosis, or hair loss. Such deficits can cause full-blown cases of life-threatening deficiencies, such as beriberi, pellagra, kwashiorkor, and nerve damage that can manifest as vision loss years or even decades after surgery in the case of copper deficiency. Tragically, in reported cases of severe deficiency of a B vitamin called thiamine, nearly one in three patients progressed to permanent brain damage before the condition was caught.
The malabsorption of nutrients is intentional for procedures like gastric bypass. By cutting out segments of the intestines, you can successfully impair the absorption of calories—at the expense of impairing the absorption of necessary nutrition. Even people who just undergo restrictive procedures like stomach stapling can be at risk for life-threatening nutrient deficiencies because of persistent vomiting. Vomiting is reported by up to 60% of patients after bariatric surgery due to “inappropriate eating behaviors.” (In other words, trying to eat normally.) The vomiting helps with weight loss, similar to the way a drug for alcoholics called Antabuse can be used to make them so violently ill after a drink that they eventually learn their lesson.
“Dumping syndrome” can work the same way. A large percentage of gastric bypass patients can suffer from abdominal pain, diarrhea, nausea, bloating, fatigue, or palpitations after eating calorie-rich foods, as they bypass your stomach and dump straight into your intestines. As surgeons describe it, this is a feature, not a bug: “Dumping syndrome is an expected and desired part of the behavior modification caused by gastric bypass surgery; it can deter patients from consuming energy-dense food.
My book How Not to Diet is focused exclusively on sustainable weight loss. Check it out from your local library, or pick it up from wherever you get your books. (All proceeds from my books are donated to charity.)
A randomized controlled trial investigates diet and psychological well-being.
“Psychological health can be broadly conceptualized as comprising 2 key components: mental health (i.e., the presence of absence of mental health disorders such as depression) and psychological well-being (i.e., a positive psychological state, which is more than the absence of a mental health disorder,” and that is the focus of an “emerging field of positive psychology [that] focuses on the positive facts of life, including happiness, life satisfaction, personal strengths, and flourishing.” This may translate to physical “benefits of enhanced well-being, including improvements in blood pressure, immune competence, longevity, career success, and satisfaction with personal relationships.”
What is “The Contribution of Food Consumption to Well-Being,” the title of an article in Annals of Nutrition & Metabolism? Studies have “linked the consumption of fruits and vegetables with enhanced well-being.” A systematic review of research found evidence that fruit and vegetable intake “was associated with increased psychological well-being.” Only an association?
There is “a famous criticism in this area of research—namely, that deep-down personality or family upbringing might lead people simultaneously to eat in a healthy way and also to have better mental well-being, so that diet is then merely correlated with, but incorrectly gives the appearance of helping to cause, the level of well-being.” However, recent research circumvented this problem by examining if “changes in diet are correlated with changes in mental well-being”—in effect, studying the “Evolution of Well-Being and Happiness After Increases in Consumption of Fruit and Vegetables.” As you can see below and at 1:37 in my video Fruits and Vegetables Put to the Test for Boosting Mood, as individuals began eating more fruits and veggies, there was a straight-line increase in their change in life satisfaction over time.
“Increased fruit and vegetable consumption was predictive of increased happiness, life satisfaction, and well-being. They were up to 0.24 life-satisfaction points (for an increase of 8 portions a day), which is equal in size to the psychological gain of going from unemployment to employment.” (My Daily Dozen recommendation is for at least nine servings of fruits and veggies a day.)
That study was done in Australia. It was repeated in the United Kingdom, and researchers found the same results, though Brits may need to bump up their daily minimum consumption of fruits and vegetables to more like 10 or 11 servings a day.
As researchers asked in the title of their paper, “Does eating fruit and vegetables also reduce the longitudinal risk of depression and anxiety?” Improved well-being is nice, but “governments and medical authorities are often interested in the determinants of major mental ill-health conditions, such as depression and high levels of anxiety, and not solely in a more typical citizen’s level of well-being”—for instance, not just life satisfaction. And, indeed, using the same dataset but instead looking for mental illness, researchers found that “eating fruit and vegetables may help to protect against future risk of clinical depression and anxiety,” as well.
A systematic review and meta-analysis of dozens of studies found “an inverse linear association between fruit or vegetable intake and risk of depression, such that every 100-gram increased intake of fruit was associated with a 3% reduced risk of depression,” about half an apple. Yet, “less than 10% of most Western populations consume adequate levels of whole fruits and dietary fiber, with typical intake being about half of the recommended levels.” Maybe the problem is we’re just telling people about the long-term benefits of fruit intake for chronic disease prevention, rather than the near-immediate improvements in well-being. Maybe we should be advertising the “happiness’ gains.” Perhaps, but we first need to make sure they’re real.
We’ve been talking about associations. Yes, “a healthy diet may reduce the risk of future depression or anxiety, but being diagnosed with depression or anxiety today could also lead to lower fruit and vegetable intake in the future.” Now, in these studies, we can indeed show that the increase in fruit and vegetable consumption came first, and not the other way around, but as the great enlightenment philosopher David Hume pointed out, just because the rooster crows before the dawn doesn’t mean the rooster caused the sun to rise.
To prove cause and effect, we need to put it to the test with an interventional study. Unfortunately, to date, many studies have compared fruit to chocolate and chips, for instance. Indeed, study participants randomized to eat fruit showed significant improvements in anxiety, depression, fatigue, and emotional distress, which is amazing, but that was compared to chocolate and potato chips, as you can see below and at 4:26 in my video. Apples, clementines, and bananas making people feel better than assorted potato chips and chunky chocolate wafers is not exactly a revelation.
This is the kind of study I’ve been waiting for: a randomized controlled trial in which young adults were randomized to one of three groups—a diet-as-usual group, a group encouraged to eat more fruits and vegetables, or a third group given two servings of fruits and vegetables a day to eat in addition to their regular diet. Those in the third group “showed improvements to their psychological well-being with increases in vitality, flourishing, and motivation” within just two weeks. However, simply educating people to eat their fruits and vegetables may not be enough to reap the full rewards, so perhaps greater emphasis needs to be placed on providing people with fresh produce—for example, offering free fruit for people when they shop. I know that would certainly make me happy!
What if the very hormone designed to help you survive is actually the reason you’re struggling to thrive?
My mother relentlessly saved and sacrificed so that she could enjoy her life in retirement. But two years into retirement, she was diagnosed with early onset Alzheimer’s.
Here’s what I’ve learned since becoming a Functional Diagnostic Nutrition Practitioner: she didn’t just “get” Alzheimer’s two years after retirement. It was building and building for years before that. She was making it worse with lifestyle choices: the over-exercising that women in their 40s and 50s often do, eating trans fats during the low-fat craze of the 80s and 90s.
Had I known what I know now, her outcome might have been different.
This is why I’m passionate about functional health. This is why thousands of practitioners are learning to identify and address the root causes of dysfunction before they become disease. If we can reach people in that gray space (when things are out of balance but before they become diagnosable conditions), we can change their trajectory. We can save lives.
As functional health practitioners, we see it every day: clients who’ve tried everything, followed every protocol, cleaned up their diet, and taken all the right supplements, yet they’re still stuck in that frustrating place of “I’m okay, but I’m not great.”
The missing piece? Understanding cortisol and its profound impact on every system in the body.
If you’ve ever wondered why some clients get amazing results while others plateau, or why you yourself might be experiencing symptoms that doctors dismiss as “normal aging,” this deep dive into cortisol will change everything.
What Is Wellness, Really?
Before we dive into cortisol, let’s get clear on what we’re actually working toward. At FDN, we don’t believe in “fine” or “okay.” We believe in abundant vitality.
Picture this as a spectrum:
The Right Side (The Medical Model): Symptoms → Sickness → Disease → Death
The Middle (Neutral Health): No symptoms, but no energy either. This is the “I’m fine, I guess” zone where most people live.
The Left Side (True Wellness): High energy, optimal function, metabolic fire, abundant vitality, joy for life.
Here’s the thing: neutral health equals a neutral life. When you’re operating from “I’m okay, I don’t have any complaints,” you’re not building empires, writing books, raising joyful kids, or showing up as your best self in relationships.
Good health, abundant vitality, is your birthright. It’s not just for the lucky few.
The Body’s Incredible Healing Power (And What’s Limiting It)
Your body is a self-healing machine. You know this because when you get a cut, it heals. When you break a bone, it mends. When you catch a cold, you recover.
But this healing ability isn’t infinite. If it were, we’d never age or die.
So what’s the difference between what your body can heal and what it can’t?
It’s a savings versus spending problem.
Think of your body as having a bank account called “Vital Reserve.” This is your innate intelligence: your body’s natural ability to function at 100% and fix imbalances before they become problems.
Where do you spend this precious currency? On your environment.
This has always been the case. Our paleolithic ancestors spent their Vital Reserve on not knowing if food would be available, dealing with harsh weather, avoiding predators, and navigating tribal conflicts.
Today? We spend it on mental-emotional stress, environmental toxins, and poor lifestyle habits that are constantly draining our account.
The main spender of Vital Reserve is stress.
The Modern Stress Problem: It’s Not What You Think
When most people think of stress, they picture this: work deadlines, traffic, relationship conflicts, financial pressure. And yes, these mental-emotional stressors are huge.
But there are two other categories most people completely miss:
Physical Stressors:
Sitting too long
Blue light exposure from screens
Too much coffee
Not exercising enough (or exercising too much)
Needing wine to fall asleep
Poor sleep quality
Environmental Stressors:
Depleted soils
EMF exposure
Chemicals in food, water, and air
Toxins our paleolithic ancestors never encountered
Plus, there’s the existential stress of modern life: What’s my purpose? How do I make my life meaningful when I’ll likely be forgotten in 100 years?
All of these are constantly withdrawing from your Vital Reserve account.
Meet Cortisol: Your Body’s “Energy on Credit” System
Cortisol is your primary stress hormone, and it’s actually designed to help you survive. When your environment throws stressors at you, cortisol says, “We need to put internal spending on hold and take all available resources to deal with this external threat.”
Cortisol breaks the body down for quick energy. We call this “catabolic.”
Why would your body have a mechanism for breaking itself down? Because sometimes you need energy RIGHT NOW. When your boss says, “This project is actually due in 30 minutes,” you can’t drive to the store, buy food, cook it, eat it, digest it, and then produce energy. You need quick fuel immediately.
So cortisol reaches for easy-to-break-down tissues like cartilage, tendons, connective tissue, and muscle, converting them to blood sugar.
Here’s the kicker: Cortisol is also a natural painkiller and anti-inflammatory. It masks the damage it’s doing, which is why it makes you feel amazing in the moment: clear thinking, quick reactions, pain-free movement.
Think of cortisol as your body’s credit card. You’re borrowing energy now and promising to pay it back later through rest, recovery, and healing.
When “Energy on Credit” Becomes a Problem
Throughout history, humans dealt with stress that was intense but occasional and short-lived. A wild animal attack, a natural disaster, a tribal conflict: these were serious but temporary.
Take a moment to think about this: Does this describe the stress in your life?
For most of us, stress is intense, constant, and never-ending. We wake up stressed, work stressed, drive home stressed, and lie in bed stressed about tomorrow’s stress.
This creates what we call “catabolic debt”: you’re constantly running up charges on your cortisol credit card without ever paying it back.
Chronic stress is not within our biological design.
Consider this: Anthropological studies show paleolithic humans worked only 15-20 hours per week. How many of you work only 15-20 hours per week? (And remember, “work” includes housework, childcare, and all the other responsibilities that don’t stop when you leave the office.)
They lived in close communities with cooperative resource sharing and had each other’s backs. Think about your own life: Do you know your neighbors? If you do, would they really have your back if things got serious?
Most of us are duplicating resources instead of sharing them. We’re all figuring out our own childcare, making our own meals, maintaining our own everything. There’s no interdependence, no shared load.
The cost of modern life is enormous:
70-80% of doctor visits are for stress-related illnesses
People with high anxiety are 4-5 times more likely to die from heart attack or stroke
Stress contributes to 50% of all illnesses
The Stress Response Curve: Your Roadmap to Understanding Where You Are
This is where it gets really interesting. Understanding this curve will change how you see your health (and your clients’ health) forever.
We all start in the green zone: Homeostasis. When you experience occasional stressors, cortisol and adrenaline spike, you handle the situation, then return to baseline to rest and repair.
But when stress becomes chronic, you move into the orange zone: Acute Stress. You’re constantly producing cortisol and adrenaline, never returning to homeostasis.
Here’s the thing: on your way up this curve, you feel AMAZING. Remember when you could pull all-nighters and still ace exams? When you could eat junk food without consequences? When you had laser focus for 12-16 hours straight?
That’s the acute phase. You’re running on cortisol, and it feels like superpowers.
Then you hit Peak Production. Your body says, “We’ve put way too much on the cortisol credit card. We have to cut back.”
Now you fall into the Compensatory Phase. Your cortisol numbers might look normal to a doctor, but the distribution is all wrong. Maybe you have too much in the morning and crash by afternoon, or you spike at night and can’t sleep.
Plus, you have a relativity problem. You’re used to feeling like Superman from the acute phase, so normal cortisol levels feel terrible by comparison.
Continue down this path, and you reach the Exhaustive Phase. Like a phone on low battery mode, everything still works but at 30% capacity and not for long. You’re devoting everything to just getting through the day.
The Hidden Cost: What Happens to Your Body’s Core Systems
At FDN, we focus on six foundational systems that chronic stress systematically shuts down. We call them the H-I-D-D-E-N systems, and understanding what happens to each one under chronic stress is crucial for practitioners:
H – Hormones DHEA is your anabolic hormone: the one responsible for building you back up after cortisol breaks you down. This is how you pay off your cortisol credit card. But when stress is constant, DHEA steps back and says, “I’ll come back when it’s safe to focus internally, but right now we need to keep spending on the environment.” DHEA becomes chronically low, which means your healing potential becomes chronically low.
Then sex hormones get the message: “We don’t have enough resources to fund fertility right now.” Sex hormones plummet, taking motivation and joy for life with them. This is when you get to that neutral state where you’re thinking, “I have dreams I want to pursue, but it’s just too much effort. I’ll just watch Netflix instead.”
I – Immune Your immune system is expensive to run. Under chronic stress, it says, “I cost a ton of money, so I’m going to operate at 30% capacity and not for very long.” Now you’re getting sick often, it takes forever to heal, you can’t shake that cough, and if anyone around you is sick, you know you’re going down.
D – Digestion Digestion costs a lot of energy to function properly. When you’re spending everything on stress, digestion goes into low-power mode. Now you’re only digesting at 30% capacity. Even if you’re eating the cleanest diet in the world, you can’t use it. You’re not getting the building blocks to repair or the nutrients your body needs to power metabolic functions at full capacity.
D – Detoxification Detoxification is another huge system that’s expensive to run. When your body’s bank account is overdrawn from cortisol debt, detox says, “I don’t have enough money to find these toxins, bind them up, and effectively remove them. So I’ll put them in storage instead.” Your body shoves toxins into fat cells, brain tissue, and bones, creating a toxic backlog that makes you feel slow, gives you acne, throws off digestion, and impairs hormone production.
E – Energy Production Your mitochondria can’t function optimally when all resources are diverted to stress response. This leads to that “tired but wired” feeling where you’re exhausted but can’t actually rest.
N – Nervous System Sleep, mood, and cognitive function all suffer. This is where we see the brain fog, insomnia, anxiety, and depression that so many people struggle with.
The fundamental principle of FDN: These systems don’t operate in isolation. You can’t just say, “Oh, you have classic hormone symptoms, so let’s run a hormone test.” You miss immunity, digestion, detoxification: all the other systems contributing to what we call “Metabolic Chaos.”
This is why the “take this supplement for that symptom” approach rarely works long-term. You’re not dealing with isolated problems: you’re dealing with systemic dysfunction where multiple systems are compromised simultaneously.
Real-Life Case Studies: The Stress Curve in Action
Let’s look at three real clients to see how this plays out. As FDN practitioners, we use what we call “clinical correlation,” which means we never look at lab numbers in isolation. We always consider how someone feels alongside their test results.
Case Study 1: Adam – The Acute Phase Crash
Profile: 35-year-old male, broker at a mid-size investment firm, former athlete still crushing CrossFit workouts
Symptoms: Weight gain, trouble concentrating, loss of muscle mass despite rigorous workouts, headaches
Doctor’s Assessment: “Your results are unremarkable. This is normal aging.”
Lab Results:
Cortisol sum: 9 (acute phase)
Four-point pattern: Way too high in morning, drops low at noon, crashes severely in afternoon, bounces back up at night
The Reality: How do we know Adam isn’t on the left side of the stress curve going up into acute phase? His symptoms tell us everything. If he were on the way up, he’d feel amazing and wouldn’t be in our office. Instead, he’s on the right side coming down from peak production.
His cortisol pattern explains everything: sky-high morning cortisol makes him feel wired and anxious, the afternoon crash leaves him unable to concentrate (not ideal for an investment broker), and the nighttime spike disrupts his sleep.
Even though his DHEA looks “normal,” when we compare it to his cortisol level of 9, he’s clearly catabolic dominant. He’s breaking down faster than he’s building up, which explains why his intense CrossFit sessions aren’t building muscle: they’re just adding more stress to an already overloaded system.
The Reality: Caitlyn’s cortisol sum looks normal, but the distribution is completely dysfunctional. She can barely drag herself out of bed in the morning, crashes hard in the afternoon (imagine trying to accurately record legal proceedings when your cortisol is plummeting), and lies awake at night because her cortisol spikes just when it should be lowest.
She also has a relativity problem. When she was in the acute phase, she felt like Superman. Now that she’s in compensatory with “normal” cortisol levels, she feels terrible by comparison. Her DHEA is low, confirming she’s still in catabolic debt despite the lower cortisol numbers.
Case Study 3: Maggie – The Exhaustive Phase Crisis
Profile: 43-year-old chef at a popular five-star restaurant, diagnosed with hypothyroid
Symptoms: Weight gain in hips and belly, trouble keeping up at work, depression, irregular menstrual cycle
Lifestyle: Working 60+ hours per week, consistently sleeping only 5 hours per night
Medical Status: Seeing a counselor, considering antidepressant medication
Lab Results:
Cortisol sum: 3.1 (exhaustive phase)
Four-point pattern: Way too low in morning, drops low at noon, slight bounce in afternoon, drops again at night
DHEA: Very low
Clinical correlation: Still catabolic dominant despite low cortisol
The Reality: Maggie’s body is operating like a phone on low battery mode: everything still works, but at 30% capacity and not for long. Her thyroid has downregulated because there’s literally not enough energy in the system to maintain normal function.
The depression isn’t just psychological: it’s physiological. Her body can’t afford to fund optimal brain function. Even though her cortisol is very low and her DHEA is very low, she’s still cortisol dominant and in catabolic debt.
This is why understanding the stress curve is so crucial. Three people, three different phases, three different approaches needed.
The Path Forward: Why Understanding Cortisol Changes Everything
Here’s why this matters for you as a health practitioner:
1. It explains why some clients plateau. If you’re not addressing the stress component, you’ll hit a ceiling on healing no matter how perfect the diet or supplement protocol.
2. It validates your clients’ experiences. When someone says, “I used to be able to handle so much more,” or “I don’t feel like myself anymore,” you now understand the physiology behind it.
3. It gives you a roadmap for intervention. Different phases require different approaches. Someone in the acute phase needs different support than someone in the exhaustive phase.
4. It highlights the importance of comprehensive testing. A single cortisol measurement tells you almost nothing. You need the full pattern plus clinical correlation.
The FDN Approach: Test, Don’t Guess
At FDN, we don’t just talk about stress: we measure it. We use what we call “clinical correlation,” which means we never look at lab numbers in isolation. We always consider how someone feels alongside their test results.
We look at:
Four-point cortisol patterns throughout the day (not just a single measurement)
DHEA levels and the cortisol-to-DHEA ratio
How stress is affecting all the H-I-D-D-E-N systems
The complete picture of metabolic chaos
Progress tracking with tools like the Metabolic Chaos Scorecard
Then we address it systematically through our DRESS protocol:
D – Diet: Personalized nutrition based on lab findings, not generic “healthy eating” advice
R – Rest: Sleep optimization and recovery strategies tailored to your stress phase
E – Exercise: Right-sized movement for your current capacity (over-exercise is just as harmful as under-exercise)
S – Stress Reduction: Targeted techniques for your specific stressors: mental/emotional, physical, environmental, and lifestyle factors
S – Supplementation: Targeted support based on actual lab results, not guesswork
This isn’t about generic protocols. It’s about understanding exactly where someone is on the stress curve and what their body needs to heal.
Key Takeaways for Health Practitioners
Cortisol isn’t the enemy. A lot of people talk about cortisol as if it’s the villain—commercials make it sound like cortisol just makes you “old and fat.” That’s not what cortisol does. Cortisol is a vital hormone for navigating stress. The problem is chronic stress disrupting its natural rhythm.
Understanding the stress curve is diagnostic gold. It explains why clients feel the way they do and gives you a framework for intervention. Different phases require different approaches.
Clinical correlation is everything. You can’t just look at lab numbers in isolation. A cortisol sum of 5 might be “normal” to a doctor, but if your client feels terrible and the distribution is dysregulated, that tells you the real story.
You can’t ignore stress and expect lasting results. No matter how perfect your diet protocol or how targeted your supplements, chronic stress will cap healing potential. There’s a ceiling you’ll never break through if you don’t address the stress component.
The body’s systems are interconnected. You can’t just “fix hormones” without addressing how stress is affecting immunity, digestion, detoxification, and all the other H-I-D-D-E-N systems. This is why comprehensive testing and systematic protocols are crucial.
Metabolic Chaos requires a systematic approach. When multiple systems are compromised simultaneously, you need a framework like DRESS that addresses all aspects of healing, not just isolated symptoms.
Your Next Steps
If you’re ready to master functional lab testing and learn how to identify and address cortisol dysregulation in your practice, FDN provides the training, community, and ongoing support you need.
Because here’s the truth: your clients deserve more than “fine.” They deserve abundant vitality. And you deserve the confidence that comes from knowing exactly how to help them achieve it.
When you understand cortisol (really understand it), you hold the key to unlocking transformation for every client who walks through your door.
Ready to become the practitioner who always knows what to do next?
The answer lies in data-driven functional health. The answer lies in understanding that robust health isn’t just about the absence of symptoms: it’s about the presence of vitality.
And it starts with the hormone you can’t ignore: cortisol.
Want to learn more about becoming a Functional Diagnostic Nutrition Practitioner?
Discover how our comprehensive training program gives you the tools to master cortisol testing, interpretation, and protocols that get results. Because when you know how to test, you never have to guess. View an indepth case study here.
Caloric restriction can boost levels of brain-derived neurotrophic factor (BDNF), which is considered to play a critical role in mood disorders.
For more than a century, fasting has been espoused as a treatment of supposed “great utility in the preservation of health,” especially rejuvenating the body and, above all, the mind. When people fast for even 18 hours, though, they may get hungry and irritable. After one or two days, positive mood goes down and negative mood goes up, and after three days, fasters can increasingly feel sad, self-blame, and suffer a loss of libido. Then, something strange starts to happen: People experience a “fasting-induced mood enhancement…reflected by decreased anxiety, depression, fatigue, and improved vigor.” Studies tend to show this across the board. Once you get over the hump, fasters frequently experience “an increased level of vigilance and a mood improvement, a subjective feeling of well-being, and sometimes of euphoria.” And, no wonder, as, by then, endorphin levels may rise by nearly 50 percent, as seen here and at 1:06 in my video Friday Favorites: Fasting to Treat Depression.
This enhancement of mood, alertness, and calm makes a certain amount of evolutionary sense. Our body wants us to feel poorly initially so we continue to eat, day to day, when food is available, but if we go a couple of days without food, our body realizes we can’t just mope in our cave; we need to get motivated to go out and find some calories.
So, can fasting be used for mood disorders, like depression? It’s great that people can feel better after a few days of fasting, but the critical question revolves around the “persistence of mood improvement over time” once fasting ends and eating resumes. The little published evidence we have comes out of Japan and the former Soviet Union, and some of it is just ridiculous, like this study that included women with a variety of symptoms, which the researchers blame mostly on marital conflict, as you can see below and at 2:08 in my video. Husband not treating you right? How about some “electroshock therapy”? That didn’t seem to help much, so what about “hunger therapy”? Of course, starving the women made them hungry, but that’s what Thorazine is for. If they keep getting injected with an antipsychotic to calm them down, they can sail right through. So, what happened in the study? What would we even do with those results?
Another study, however, skipped the Thorazine. The participants fasted for ten days, but they were also kept in bed all day on “absolute bed rest,” completely isolated and “prohibited from seeing other people except the attending doctor and nurse…also denied access to television, radio, newspapers or any other forms of information.” So, if people got better or worse, it would be impossible to tease out the effects of the fasting component on its own. But researchers found that they apparently did get better, with efficacy reportedly demonstrated in 31 out of 36 patients suffering from depression, as seen here and at 2:56 in my video.
The researchers concluded that fasting therapy may provide an alternative to the use of antidepressant drugs, “thinking the fasting therapy may be a kind of shock therapy.” People are so relieved to be eating again, to get out of solitary confinement, and to even just get out of bed that they report feeling better. That was at the time of discharge, though. How did they feel the next day, the next week, the next month? Fasting is, by definition, unsustainable, so what we want to ideally see are some kind of longer-lasting effects.
Researchers did a follow-up with a few hundred patients, not just a few months later, but after a few years. Of the 69 who were evidently suffering from depression, 90 percent reported feeling good or excellent results at the end of the ten-day fast, and, remarkably, years later, 87 percent of the 62 individuals who replied claimed that they were still doing well. Now, there was no control group, so we don’t know if they would have done just as well or even better without the fast, and it was all self-reporting, so there may have been a response bias where participants tried to please the researchers. Who knows? Maybe they were afraid they’d get sent back to solitary if they didn’t respond affirmatively. We have no idea, but we do have good evidence for the short-term mood benefits.
Why would fasting improve feelings of depression? In addition to the endorphins and the surge in serotonin, the so-called happiness hormone, when we fast, there is a bump in brain-derived neurotrophic factor (BDNF), which is considered to play a crucial role in mood disorders. Researchers have perked up rodents with it, but we aren’t rats or mice. What about us? Humans with major depression have lower levels of BDNF circulating in their bloodstream. Autopsy studies of suicide victims show only about half the BDNF in certain key brain regions, compared to controls, suggesting it may play an important role in suicidal behavior, as seen here and at 4:38 in my video.
We can boost BDNF with antidepressant drugs and electroshock; we can also boost it with caloric restriction. We can get a 70 percent boost in levels after three months of cutting 25 percent of calories out of our daily diet, as shown below and at 4:51.
Is there anything we can add to our diets to boost BNDF levels so we can get the benefits without the hunger? We’ll find out next.
Why should fasts lasting longer than 24 hours and particularly for three or more days only be done under the supervision of a health professional and preferably in a live-in clinic?
Fasting for a week or two can actually interfere with the loss of body fat, as shown at the start of my video Is Fasting for Weight Loss Safe?. But, eventually, after the third week of fasting, fat loss starts to overtake the loss of lean body mass in obese individuals, as seen in the graph below and at 0:14 in my video. Is it safe to go that long without food?
Proponents speak of fasting as a cleansing process, but some of what is being purged from our bodies are essential vitamins and minerals. People who are heavy enough can fast up to 382 days without calories, but no one can go even a fraction of that long without vitamins. Scurvy, for example, can be diagnosed within as few as four weeks without any vitamin C. Beriberi, deficiency of thiamine (vitamin B1), may start even earlier in fasting patients. And, once it manifests, it can result in brain damage within days, which can eventually become irreversible.
Even though fasting patients report problems such as nausea and indigestion after taking supplements, all of the months-long fasting cases I’ve discussed previously were given daily multivitamins and mineral supplementation as necessary. Without supplementation, hunger strikers and those undergoing prolonged fasts for therapeutic or religious purposes (like the Baptist pastor hoping “to enhance his spiritual powers for exorcism”) have ended up paralyzed, become comatose, or worse.
Nutrient deficiencies aren’t the only risk. After reading about all of the successful reports of massive weight loss from prolonged fasting in the medical literature, one doctor decided to give it a try with his patients. Of the first dozen he tried it on, two died. In retrospect, the two patients who died had started out with heart failure and had been on diuretics. Fasting itself produces pronounced diuresis, meaning loss of water and electrolytes through the urine, so it was the combination of fasting on top of the water pills that likely depleted their potassium and triggered their fatal heart rhythms. The doctor went out of his way to point out that both of the people who died started out “in severe heart failure, complicated by gross obesity; but both had improved greatly whilst undergoing starvation therapy.” That seems like a small consolation since they were both dead within a matter of weeks.
Not all therapeutic fasting fatalities were complicated by concurrent medication use, though. One researcher writes: “At first he did very well and experienced the usual euphoria…His pulse, blood pressure, and electrolytes remained satisfactory, but in the middle of the third week of treatment, he suddenly collapsed and died. This line of treatment is certainly tempting because it does produce weight loss and the patient feels so much better, but the report of case-fatalities”—the whole part about killing people—“must make it a very suspect line of management.”
Contrary to the popular notion that the heart muscle is specially spared during fasting, the heart appears to experience similar muscle wasting. This was “described in the victims of the Warsaw ghetto” during World War II in a remarkable series of detailed studies carried out by the ghetto physicians before they themselves succumbed. In a case entitled “Gross Fragmentation of Cardiac Fiber After Therapeutic Starvation for Obesity,” a 20-year-old woman successfully “achieved her ideal weight” after losing 128 pounds by fasting for 30 weeks. “After a breakfast of one egg,” she had a heart attack and died. On autopsy, as you can see below and at 3:44 in my video, the muscle fibers in her heart showed evidence of widespread disintegration. The pathologists suggested that fasting regimens “should no longer be recommended as a safe means of weight reduction.” Breaking the fast appears to be the most dangerous part. After World War II, as many as one out of five starved Japanese prisoners of war tragically died following liberation. Now known as “refeeding syndrome,” multiorgan system failure can result from resuming a regular diet too quickly. This is because there are critical nutrients such as thiamine and phosphorus that are used to metabolize food. Therefore, in the critical refeeding window, if too much food is taken before these nutrients can be replenished, demand may exceed supply. Whatever residual stores you still carry can be driven down even further, with potentially fatal consequences. This is why rescue workers are taught to always give thiamine before food to victims who have been trapped or otherwise unable to eat. Thiamine is responsible for the yellow color of “banana bags,” a term you might have heard used in medical dramas to describe an IV fluid concoction often given to malnourished alcoholics to prevent a similar reaction. (You can see a photo of them below and at 4:53 in my video.) Anyone “with negligible food intake for more than five days” may be at risk of developing refeeding problems. Medically-supervised fasting has gotten much safer now that there are proper refeeding protocols. We now know what warning signs to look for and who shouldn’t be fasting in the first place, such as those who have advanced liver or kidney failure, porphyria, uncontrolled hyperthyroidism, and pregnant and breastfeeding women. The most comprehensive safety analysis of medically supervised, water-only fasting was recently published by the TrueNorth Health Center in California. Out of 768 visits to its facility for fasts up to 41 days, were there any adverse events? There were 5,961 of them! Most of these were mild, known reactions to fasting, such as fatigue, nausea, insomnia, headache, dizziness, upset stomach, and back pain. Only two serious events were reported, and no fatalities. You can see the chart below and at 5:58 in my video. “Fasting periods lasting longer than 24 hr, and particularly those lasting 3 or more days, should be done under the supervision of a physician and preferably in a [live-in] clinic.” In other words, don’t try this at home! This is not just legalistic mumbo-jumbo. For example, normally, your kidneys dive into sodium conservation mode during fasting, but should that response break down, you could rapidly develop an electrolyte abnormality that may only manifest with non-specific symptoms, like fatigue or dizziness, which could easily be dismissed until it’s too late.
The risks of any therapy must be premised on the severity of the disease. The consequences of obesity are considered so serious that effective therapies could have “considerable acceptable toxicity.” For example, many consider major surgery for obesity to be a justifiable risk, but the keyword is effective.
Therapeutic fasting for obesity has largely been abandoned by the medical community not only because of its uncertain safety profile but its questionable short- and long-term efficacy. Remember, for a fast that only lasts a week or two, you might be able to lose as much body fat or even more on a low-calorie diet than a no-calorie diet.
Alexis Misko’s health has improved enough that, once a month, she can leave her house for a few hours. First, she needs to build up her energy by lying in a dark room for the better part of two days, doing little more than listening to audiobooks. Then she needs a driver, a quiet destination where she can lie down, and days of rest to recover afterward. The brief outdoor joy “never quite feels like enough,” she told me, but it’s so much more than what she managed in her first year of long COVID, when she couldn’t sit upright for more than an hour or stand for more than 10 minutes. Now, at least, she can watch TV on the same day she takes a shower.
In her previous life, she pulled all-nighters in graduate school and rough shifts at her hospital as an occupational therapist; she went for long runs and sagged after long flights. None of that compares with what she has endured since getting COVID-19 almost three years ago. The fatigue she now feels is “like a complete depletion of the essence of who you are, of your life force,” she told me in an email.
Fatigue is among the mostcommon and mostdisabling of long COVID’s symptoms, and a signature of similar chronic illnesses such as myalgic encephalomyelitis (also known as chronic fatigue syndrome or ME/CFS). But in these diseases, fatigue is so distinct from everyday weariness that most of the people I have talked with were unprepared for how severe, multifaceted, and persistent it can be.
For a start, this fatigue isn’t really a single symptom; it has many faces. It can weigh the body down: Lisa Geiszler likens it to “wearing a lead exoskeleton on a planet with extremely high gravity, while being riddled with severe arthritis.” It can rev the body up: Many fatigued people feel “wired and tired,” paradoxically in fight-or-flight mode despite being utterly depleted. It can be cognitive: Thoughts become sluggish, incoherent, and sometimes painful—like “there’s steel wool stuck in my frontal lobe,” Gwynn Dujardin, a literary historian with ME, told me.
Fatigue turns the most mundane of tasks into an “agonizing cost-benefit analysis,” Misko said. If you do laundry, how long will you need to rest to later make a meal? If you drink water, will you be able to reach the toilet? Only a quarter of long-haulers have symptoms that severely limit their daily activities, but even those with “moderate” cases are profoundly limited. Julia Moore Vogel, a program director at Scripps Research, still works, but washing her hair, she told me, leaves her as exhausted as the long-distance runs she used to do.
And though normal fatigue is temporary and amenable to agency—even after a marathon, you can will yourself into a shower, and you’ll feel better after sleeping—rest often fails to cure the fatigue of long COVID or ME/CFS. “I wake up fatigued,” Letícia Soares, who has long COVID, told me.
Between long COVID, ME/CFS, and other energy-limiting chronic illnesses, millions of people in the U.S. alone experience debilitating fatigue. But American society tends to equate inactivity with immorality, and productivity with worth. Faced with a condition that simply doesn’t allow people to move—even one whose deficits can be measured and explained—many doctors and loved ones default to disbelief. When Soares tells others about her illness, they usually say, “Oh yeah, I’m tired too.” When she was bedbound for days, people told her, “I need a weekend like that.” Soares’s problems are very real, and although researchers have started to figure out why so many people like her are suffering, they don’t yet know how to stop it.
Fatigue creates a background hum of disability, but it can be punctuated by worse percussive episodes that strip long-haulers of even the small amounts of energy they normally have.
Daria Oller is a physiotherapist and athletic trainer, so when she got COVID in March 2020, she naturally tried exercising her way to better health. And she couldn’t understand why, after just short runs, her fatigue, brain fog, chest pain, and other symptoms would flare up dramatically—to the point where she could barely move or speak. These crashes contradicted everything she had learned during her training. Only after talking with physiotherapists with ME/CFS did she realize that this phenomenon has a name: post-exertional malaise.
Post-exertional malaise, or PEM, is the defining trait of ME/CFS and a common feature of long COVID. It is often portrayed as an extreme form of fatigue, but it is more correctly understood as a physiological state in which all existing symptoms burn more fiercely and new ones ignite. Beyond fatigue, people who get PEM might also feel intense radiant pain, an inflammatory burning feeling, or gastrointestinal and cognitive problems: “You feel poisoned, flu-ish, concussed,” Misko said. And where fatigue usually sets in right after exertion, PEM might strike hours or days later, and with disproportionate ferocity. Even gentle physical or mental effort might lay people out for days, weeks, months. Visiting a doctor can precipitate a crash, and so can filling out applications for disability benefits—or sensing bright lights and loud sounds, regulating body temperature on hot days, or coping with stress. And if in fatigue your batteries feel drained, in PEM they’re missing entirely. It’s the annihilation of possibility: Most people experience the desperation of being unable to move only in nightmares, Dujardin told me. “PEM is like that, but much more painful.”
Medical professionals generally don’t learn about PEM during their training. Many people doubt its existence because it is so unlike anything that healthy people endure. Mary Dimmock told me that she understood what it meant only when she saw her son, Matthew, who has ME/CFS, crash in front of her eyes. “He just melted,” Dimmock said. But most people never see such damage because PEM hides those in the midst of it from public view. And because it usually occurs after a delay, people who experience PEM might appear well to friends and colleagues who then don’t witness the exorbitant price they later pay.
That price is both real and measurable. In cardiopulmonary exercise tests, or CPETs, patients use treadmills or exercise bikes while doctors record their oxygen consumption, blood pressure, and heart rate. Betsy Keller, an exercise physiologist at Ithaca College, told me that most people can repeat their performance if retested one day later, even if they have heart disease or are deconditioned by inactivity. People who get PEM cannot. Their results are so different the second time around that when Keller first tested someone with ME/CFS in 2003, “I told my colleagues that our equipment was out of calibration,” she said. But she and others have seen the same pattern in hundreds of ME/CFS and long-COVID patients—“objective findings that can’t be explained by anything psychological,” David Systrom, a pulmonologist at Brigham and Women’s Hospital, told me. “Many patients are told it’s all in their head, but this belies that in spades.” Still, many insurers refuse to pay for a second test, and many patients cannot do two CPETs (or even one) without seriously risking their health. And “20 years later, I still have physicians who refute and ignore the objective data,” Keller said. (Some long-COVID studies have ignored PEM entirely, or bundled it together with fatigue.)
Oller thinks this dismissal arises because PEM inverts the dogma that exercise is good for you—an adage that, for most other illnesses, is correct. “It’s not easy to change what you’ve been doing your whole career, even when I tell someone that they might be harming their patients,” she said. Indeed, many long-haulers get worse because they don’t get enough rest in their first weeks of illness, or try to exercise through their symptoms on doctors’ orders.
People with PEM are also frequently misdiagnosed. They’re told that they’re deconditioned from being too sedentary, when their inactivity is the result of frequent crashes, not the cause. They’re told that they’re depressed and unmotivated, when they are usually desperate to move and either physically incapable of doing so or using restraint to avoid crashing. Oller is part of a support group of 1,500 endurance athletes with long COVID who are well used to running, swimming, and biking through pain and tiredness. “Why would we all just stop?” she asked.
Some patients with energy-limiting illnesses argue that the names of their diseases and symptoms make them easier to discredit. Fatigue invites people to minimize severe depletion as everyday tiredness. Chronic fatigue syndrome collapses a wide-ranging disabling condition into a single symptom that is easy to trivialize. These complaints are valid, but the problem runs deeper than any name.
Dujardin, the English professor who is (very slowly) writing a cultural history of fatigue, thinks that our concept of it has been impoverished by centuries of reductionism. As the study of medicine slowly fractured into anatomical specialties, it lost an overarching sense of the systems that contribute to human energy, or its absence. The concept of energy was (and still is) central to animistic philosophies, and though once core to the Western world, too, it is now culturally associated with quackery and pseudoscience. “There are vials of ‘energy boosters’ by every cash register in the U.S.,” Dujardin said, but when the NIH convened a conference on the biology of fatigue in 2021, “specialists kept observing that no standard definition exists for fatigue, and everyone was working from different ideas of human energy.” These terms have become so unhelpfully unspecific that our concept of “fatigue” can encompass a wide array of states including PEM and idleness, and can be heavily influenced by social forces—in particular the desire to exploit the energy of others.
As the historian Emily K. Abel notes in Sick and Tired: An Intimate History of Fatigue, many studies of everyday fatigue at the turn of the 20th century focused on the weariness of manual laborers, and were done to find ways to make those workers more productive. During this period, fatigue was recast from a physiological limit that employers must work around into a psychological failure that individuals must work against. “Present-day society stigmatizes those who don’t Push through; keep at it; show grit,” Dujardin said, and for the sin of subverting those norms, long-haulers “are not just disbelieved but treated openly with contempt.” Fatigue is “profoundly anti-capitalistic,” Jaime Seltzer, the director of scientific and medical outreach at the advocacy group MEAction, told me.
Energy-limiting illnesses also disproportionately affect women, who have long been portrayed as prone to idleness. Dujardin notes that in Western epics, women such as Circe and Dido were perceived harshly for averting questing heroes such as Odysseus and Aeneas with the temptation of rest. Later, the onset of industrialization turned women instead into emblems of homebound idleness while men labored in public. As shirking work became a moral failure, it also remained a feminine one.
These attitudes were evident in the ways two successive U.S. presidents dealt with COVID. Donald Trump, who always evinced a caricature of masculine strength and chastised rivals for being “low energy,” framed his recovery from the coronavirus as an act of domination. Joe Biden was less bombastic, but he still conspicuously assured the public that he was working through his COVID infection while his administration prioritized policies that got people back to work. Neither man spoke of the possibility of disabling fatigue or the need for rest.
Medicine, too, absorbs society’s stigmas around fatigue, even in selecting those who get to join its ranks. Its famously grueling training programs exclude (among others) most people with energy-limiting illnesses, while valorizing the ability to function when severely depleted. This, together with the tendency to psychologize women’s pain, helps to explain why so many long-haulers—even those with medical qualifications, like Misko and Oller—are treated so badly by the professionals they see for care. When Dujardin first sought medical help for her ME/CFS symptoms, the same doctor who had treated her well for a decade suddenly became stiff and suspicious, she told me, reduced all of her detailed descriptions to “tiredness,” and left the room without offering diagnosis or treatment. There is so much cultural pressure to never stop that many people can’t accept that their patients or peers might be biologically forced to do so.
No grand unified theory explains everything about long COVID and ME/CFS, but neither arethese diseases total mysteries. In fact, plenty of evidence exists for at least two pathways that explain why people with these conditions could be so limited in energy.
First, most people with energy-limiting chronic illnesses have problems with their autonomic nervous system, which governs heartbeat, breathing, sleep, hormone release, and other bodily functions that we don’t consciously control. When this systemis disrupted—a condition called “dysautonomia”—hormones such as adrenaline might be released at inappropriate moments, leading to the wired-but-tired feeling. People might suddenly feel sleepy, as if they’re shutting down. Blood vessels might not expand in moments of need, depriving active muscles and organs of oxygen and fuel; those organs might include the brain, leading to cognitive dysfunction such as brain fog.
Second, many people with long COVID and ME/CFS have problems with generating energy. When viruses invade the body, the immune system counterattacks, triggering a state of inflammation. Both infection and inflammation can damage the mitochondria—the bean-shaped batteries that power our cells. Malfunctioning mitochondria produce violent chemicals called “reactive oxygen species” (ROS) that inflict even more cellular damage. Inflammation also triggers a metabolic switch toward fast but inefficient ways of making energy, depleting cells of fuel and riddling them with lactic acid. These changes collectively explain the pervasive, dead-battery flavor of fatigue, as “the body struggles to generate energy,” Bindu Paul, a pharmacologist and neuroscientist at Johns Hopkins, told me. They might also explain the burning, poisoned feelings that patients experience, as their cells fill with lactic acid and ROS.
These two pathways—autonomic and metabolic—might also account for PEM. Normally, the autonomic nervous system smoothly dials up to an intense fight-and-flight mode and down to a calmer rest-and-digest one. But “in dysautonomia, the dial becomes a switch,” David Putrino, a neuroscientist and rehabilitation specialist at Mount Sinai, told me. “You go from sitting to standing and your body thinks: Oh, are we going hunting? You stop, and your body shuts down.” The exhaustion of these dramatic, unstable flip-flops is made worse by the ongoing metabolic maelstrom. Damaged mitochondria, destructive ROS, inefficient metabolism, and chronic inflammation all compound one another in a vicious cycle that, if it becomes sufficiently intense, could manifest as a PEM crash. “No one is absolutely certain about what causes PEM,” Seltzer told me, but it makes sense that “you have this big metabolic shift and your nervous system can’t get back on an even keel.” And if people push through, deepening the metabolic demands on a body that already can’t meet them, the cycle can spin even faster, “leading to progressive disability,” Putrino said.
Other factors might also be at play. Compared with healthy people, those with long COVID and ME/CFS have differences in the size, structure, or function of brainregionsincluding the thalamus, which relays motor signals and regulates consciousness, and the basal ganglia, which controls movement and has been implicated in fatigue. Long-haulers also have problems with blood vessels, red blood cells, and clotting, all of which might further staunch their flows of blood, oxygen, and nutrients. “I’ve tested so many of these people over the years, and we see over and over again that when the systems start to fail, they all fail in the same way,” Keller said. Together, these woes explain why long COVID and ME/CFS have such bewilderingly varied symptoms. That diversity fuels disbelief—howcould one disease cause all of this?—but it’s exactly what you’d expect if things as fundamental as metabolism go awry.
Long-haulers might not know the biochemical specifics of their symptoms, but they are uncannily good at capturing those underpinnings through metaphor. People experiencing autonomic blood-flow problems might complain about feeling “drained,” and that’s literally happening: In POTS, a form of dysautonomia, blood pools in the lower body when people stand. People experiencing metabolic problems often use dead-battery analogies, and indeed their cellular batteries—the mitochondria—are being damaged: “It really feels like something is going wrong at the cellular level,” Oller told me. Attentive doctors can find important clues about the basis of their patients’ illness hiding amid descriptions that are often billed as “exaggerated or melodramatic,” Dujardin said.
Some COVID long-haulers do recover. But several studies have found that, so far, most don’tfully return to their previous baseline, and many who become severely ill stay that way. This pool of persistently sick people is now mired in the same neglect that has long plagued those who suffer from illnesses such as ME/CFS. Research into such conditions are grossly underfunded, so no cures exist. Very few doctors in the U.S. know how to treat these conditions, and many are nearing retirement, so patients struggle to find care. Long-COVID clinics exist but vary in quality: Some know nothing about other energy-limiting illnesses, and still prescribe potentially harmful and officially discouraged treatments such as exercise. Clinicians who better understand these illnesses know that caution is crucial. When Putrino works with long-haulers to recondition their autonomic nervous system, he always starts as gently as possible to avoid triggering PEM. Such work “isn’t easy and isn’t fast,” he said, and it usually means stabilizing people instead of curing them.
Stability can be life-changing, especially when it involves changes that patients can keep up at home. Over-the-counter supplements such as coenzyme Q10, which is used by mitochondria to generate energy and is depleted in ME/CFS patients, can reduce fatigue. Anti-inflammatory medications such as low-dose naltrexone may have some promise. Sleep hygiene may not cure fatigue, but certainly makes it less debilitating. Dietary changes can help, but the right ones might be counterintuitive: High-fiber foods take more energy to digest, and some long-haulers get PEM episodes after eating meals that seem healthy. And the most important part of this portfolio is “pacing”—a strategy for carefully keeping your activity levels beneath the threshold that causes debilitating crashes.
Pacing is more challenging than it sounds. Practitioners can’t rely on fixed routines; instead, they must learn to gauge their fluctuating energy levels in real time, while becoming acutely aware of their PEM triggers. Some turn to wearable technology such as heart-rate monitors, and more than 30,000 are testing a patient-designed app called Visible to help spot patterns in their illness. Such data are useful, but the difference between rest and PEM might be just 10 or 20 extra heartbeats a minute—a narrow crevice into which long-haulers must squeeze their life. Doing so can be frustrating, because pacing isn’t a recovery tactic; it’s mostly a way of not getting worse, which makes its value harder to appreciate. Its physical benefits come at mental costs: Walks, workouts, socializing, and “all the things I’d do for mental health before were huge energy sinks,” Vogel told me. And without financial stability or social support, many long-haulers must work, parent, and care for themselves even knowing that they’ll suffer later. “It’s impossible not to overdo it, because life is life,” Vogel said.
“Our society is not set up for pacing,” Oller added. Long-haulers must resist the enormous cultural pressure to prove their worth by pushing as hard as they can. They must tolerate being chastised for trying to avert a crash, and being disbelieved if they fail. “One of the most insulting things people can say is ‘Fight your illness,’” Misko said. That would be much easier for her. “It takes so much self-control and strength to do less, to be less, to shrink your life down to one or two small things from which you try to extract joy in order to survive.” For her and many others, rest has become both a medical necessity and a radical act of defiance—one that, in itself, is exhausting.
If something went wrong with your heart, would you know it?
Not all heart problems come with clear warning signs. There is not always an alarming chest clutch followed by a fall to the floor like you see in movies. Some heart symptoms don’t even happen in your chest, and it’s not always easy to tell what’s going on.
“If you’re not sure, get it checked out,” says Charles Chambers, MD, director of the Cardiac Catheterization Laboratory at Penn State Hershey Heart and Vascular Institute.
That’s especially true if you are 60 or older, are overweight, or have diabetes, high cholesterol, or high blood pressure, says Vincent Bufalino, MD, an American Heart Association spokesman. “The more risk factors you have,” he says, “the more you should be concerned about anything that might be heart-related.”
Especially watch out for these problems:
1. Chest Discomfort
It’s the most common sign of heart danger. If you have a blocked artery or are having a heart attack, you may feel pain, tightness, or pressure in your chest.
“Everyone has a different word for that feeling,” Chambers says. “Some people say it’s like an elephant is sitting on them. Other people say it’s like a pinching or burning.”
The feeling usually lasts longer than a few minutes. It may happen when you’re at rest or when you’re doing something physical.
If it’s just a very brief pain — or if it’s a spot that hurts more when you touch or push on it — it’s probably not your heart, Chambers says. You should still get it checked out by a doctor. If the symptoms are more severe and don’t go away after a few minutes, you should call 911.
Also, keep in mind you can have heart problems — even a heart attack — without chest pain. That’s particularly common among women.
2. Nausea, Indigestion, Heartburn, or Stomach Pain
Some people have these symptoms during a heart attack. They may even vomit, Chambers says.
Women are more likely to report this type of symptom than men are.
Of course, you can have an upset stomach for many reasons that have nothing to do with your heart. It could just be something you ate, after all. But you need to be aware that it can also happen during a heart attack.
So if you feel this way and you’re at risk for heart problems, let a doctor find out what’s going on, especially if you also have any of the other symptoms on this list.
3. Pain that Spreads to the Arm
Another classic heart attack symptom is pain that radiates down the left side of the body.
“It almost always starts from the chest and moves outward,” Chambers says. “But I have had some patients who have mainly arm pain that turned out to be heart attacks.”
4. You Feel Dizzy or Lightheaded
A lot of things can make you lose your balance or feel faint for a moment. Maybe you didn’t have enough to eat or drink, or you stood up too fast.
But if you suddenly feel unsteady and you also have chest discomfort or shortness of breath, get medical help right away.
“It could mean your blood pressure has dropped because your heart isn’t able to pump the way it should,” Bufalino says.
5. Throat or Jaw Pain
By itself, throat or jaw pain probably isn’t heart related. More likely, it’s caused by a muscular issue, a cold, or a sinus problem.
But if you have pain or pressure in the center of your chest that spreads up into your throat or jaw, it could be a sign of a heart attack. Call 911 and seek medical attention to make sure everything is all right.
6. You Get Exhausted Easily
If you suddenly feel fatigued or winded after doing something you had no problem doing in the past — like climbing the stairs or carrying groceries from the car — make an appointment with your doctor right away.
“These types of significant changes are more important to us than every little ache and pain you might be feeling,” Bufalino says.
Extreme exhaustion or unexplained weakness, sometimes for days at a time, can be a symptom of heart disease, especially for women.
7. Snoring
It’s normal to snore a little while you snooze. But unusually loud snoring that sounds like a gasping or choking can be a sign of sleep apnea. That’s when you stop breathing for brief moments several times at night while you are still sleeping. This puts extra stress on your heart.
Your doctor can check whether you need a sleep study to see if you have this condition. If you do, you may need a CPAP machine to smooth out your breathing while you sleep.
8. Sweating
Breaking out in a cold sweat for no obvious reason could signal a heart attack. If this happens along with any of these other symptoms, call 911 to get to a hospital right away. Don’t try to drive yourself.
9. A Cough That Won’t Quit
In most cases, this isn’t a sign of heart trouble. But if you have heart disease or know you’re at risk, pay special attention to the possibility.
If you have a long-lasting cough that produces a white or pink mucus, it could be a sign of heart failure. This happens when the heart can’t keep up with the body’s demands, causing blood to leak back into the lungs.
Ask your doctor to check on what’s causing your cough.
10. Your Legs, Feet, and Ankles Are Swollen
This could be a sign that your heart doesn’t pump blood as effectively as it should.
When the heart can’t pump fast enough, blood backs up in the veins and causes bloating.
Heart failure can also make it harder for the kidneys to remove extra water and sodium from the body, which can lead to bloating.
11. Irregular Heart Beat
It can benormal for your heart to race when you are nervous or excited or to skip or add a beat once in a while.
But if you have started feeling palpitations, check in with your doctor. Call 911 if you have palpitations or an irregular heartbeat that persists or if you also have any chest pain or pressure, dizziness, or shortness of breath.
“In most cases, it’s caused by something that’s easy to fix, like too much caffeine or not enough sleep,” Bufalino says. But occasionally, it could signal a condition called atrial fibrillation that needs treatment. So ask your doctor to check it out.
In 2013, when I was an English professor at a community college, teaching became difficult. I struggled to speak during class. I had some general weakness and trouble breathing. I had to drive between classes because I could no longer walk between them.
I told a nurse practitioner about my mobility issues, but she brushed me off. I was probably imagining things, she told me. But I knew these symptoms weren’t normal. Most 32-year-olds don’t need a cane, walker, or wheelchair to get around.
My “imaginary” problems progressed quickly. And the following year, after a lot more tests, a doctor diagnosed me with myasthenia gravis (MG).
The Good and Bad of Life After MG
I was a bit of a workaholic in my former life. Things are completely different now. I had to stop teaching because my symptoms are so serious. I’m 40 now, but I lost my academic career in my 30s.
MG also took much of my independence and some of my hobbies. I used to write my own songs. But I can’t sing them anymore. Losing all that, and more, has been devastating.
Yet I’ve learned a deep lesson of gratitude. I find joy wherever I can. I know I never would’ve done that if I didn’t have this disease.
Now I try to savor moments every day. Sometimes I sit in my yard, just watching the birds and leaves. It’s a good form of mindfulness. I started painting again — I never had spare time for my art when I worked a lot.
And I still love music. I play the piano and keep up my vinyl collection.
Plus, I tap into my research and writing background. I use those skills to raise awareness about MG and share stories about my journey through chronic illness.
I also have postural orthostatic tachycardia syndrome, or POTS, an autonomic nervous system disorder. And I advocate online for the dysautonomia, MG, and rare disease communities.
How Do I Have Fun?
I’ll save my energy to play the piano, paint, or do something creative. Sometimes my husband and I will go for walks outside, and I’ll use my power chair. And like everyone else, I enjoy spending time with friends and family.
When I have to do something overwhelming — I have a lot of medical appointments, tests, and infusions — I plan a reward for myself after. It’s a lot easier to get through the hard parts of my illness when I have something to look forward to.
My reward can be something small, like watching a movie, buying a new album from a favorite artist, or eating something I enjoy. I’m a chocolate lover. But when I have to travel for appointments, my husband and I will plan what take-out food we’ll get. That makes it feel a little more fun.
What Treatments Help My MG Symptoms?
I take meds throughout the day, including an immunosuppressant. I also get IVIg infusions every week, a treatment that affects my antibodies in a way that helps my immune system.
Every day I use a BiPap (bilevel positive airway pressure) machine to help me breathe.
I also had a thymectomy in early September. That’s a surgery to remove the thymus gland. This procedure may help ease symptoms for some people with MG. It’s not right for everyone, but my doctor and I decided it’s my best chance for long-term improvement.
When I’m not recovering from surgery, I try to stay active and build up my strength. Right now, I’m working on walking longer distances. I do short walks inside my house or outdoors nearly every day. I also stretch regularly, which helps manage some of my chronic pain from injuries.
What Are My Other Strategies to Manage MG?
I follow a pretty strict routine each day. I try to eat my meals at the same time. That helps me stay on track with my treatment schedule — it’s essential to take my medication and infusion at the right time.
If I have to make a call, I’ll schedule it in the morning and plan to rest afterward. But I have to be careful about how much I speak. Talking, especially on the phone, can make my weakness worse very fast. Respiratory problems are a big issue for me.
Sometimes I can’t fully recover if I push myself too hard. So it’s second nature for me to take breaks throughout the day. But it’s not possible to avoid my triggers all the time. That includes stress and overexertion.
I’ll go into survival mode when I feel like I’m on the verge of a serious flare. I do what I call “militant” resting — I seriously limit how much I speak and move. I’ll stay on my BiPap. I may have to get my IVIg infusion earlier than usual to avoid a hospitalization.
How Do I Get Support?
My husband is my caregiver and has been for the last 6 years. He helps me with lots of things. I haven’t been able to drive in many years, so I often rely on him to go places. And he does all the cooking and a vast majority of the cleaning.
But he has a full-time job, and I know he gets tired. We try to make sure he gets breaks, too.
I’m also grateful for my family and friends who offer their support.
I’d never heard of MG when I was diagnosed. And I’m guessing most other people haven’t either. It brings me joy when someone tells me they’ve researched my condition or treatment. I know it means they’ll have a better understanding of what my life is really like.
You have MG. Now What?
A rare disease diagnosis can be the beginning of a new life. It’s OK to grieve what you’ve lost. But prepare yourself for the changes ahead. How will you accomplish everyday tasks? How will you manage your schedule?
It’s important to pace yourself. Plan for appointments and treatments. Schedule some recovery time after each task.
You may have to reframe how you think about rest. You aren’t being lazy. Breaks aren’t wasted time. Your body and mind need them, especially if you want to avoid flares.
Chronic illness can feel like a marathon. There may not be a finish line, and you may not be able to make it through the way you did before. But give yourself time and space to adapt to your new body and life.
Up to 2.5 million Americans have myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). While researchers tie it to problems involving the brain, immune system, and energy metabolism, the causes of the illness and a cure remain undiscovered. The term systemic exertional intolerance disease (SEID) can also be used for this condition. Dana J. Brimmer, PhD, a visiting scientist at the CDC, explains what doctors do know.
Q: What is this disease?
Brimmer: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a serious, long-term illness that can radically alter patients’ lives and last for years. People with ME/CFS often have [symptoms that include moderate, severe, and substantial] pain, [debilitating] fatigue, and sleep problems.
While there is no cure, a diagnosis can help patients and families by giving them a better understanding of ME/CFS and knowledge about managing symptoms. In addition, [the National Academy of Sciences (NAS)] now gives doctors the guidance they need to evaluate and manage the condition.
What are the symptoms?
According to the [NAS], ME/CFS has five main symptoms:
A large drop in ability to perform a person’s usual activities that lasts for more than 6 months and is accompanied by fatigue
Symptoms that get worse after doing physical or mental activities that would have been “usual” before they became ill (also known as post-exertional malaise, or PEM)
Difficulty thinking, processing information, or concentrating
Symptoms that worsen when a person stands up but improve when lying down (also known as orthostatic intolerance)
Many patients with ME/CFS say that PEM is the symptom that interferes with their lives the most. PEM is not always predictable, so it’s hard to plan activities. For example, a person with ME/CFS may be able to go to the grocery store without problems on some days. But on others, the trip could confine them to bed rest for several days after. People with ME/CFS may also have pain, a sore throat, or flu-like symptoms.
What if a person suspects ME/CFS?
Talk to a doctor. Only a health care provider can make a diagnosis. Since symptoms vary, some patients find it helpful to keep track of symptoms and bring a list to the first appointment. People can find information about ME/CFS on the websites of the CDC and the National Institutes of Health (NIH).
How can I support someone with ME/CFS?
ME/CFS affects patients, families, and friends. The most important support you can provide is to understand that the illness is real and has long-term consequences. The severity of ME/CFS varies by person — for example, some people can still work, but others are very sick and homebound.
The illness can also vary for a single patient — sometimes she may appear “fine,” while other times, she may be too ill to do normal activities. Try to understand these ups and downs, and ask what you can do to help.
By the Numbers
2x: Number of women who have ME/CFS as compared to men, although people of both sexes can have the condition.
30s and 40s: Ages when the condition most often appears. But it also can affect young kids, teens, and older adults.
$17 billion to $24 billion: Amount in annual medical bills and lost income due to ME/CFS in the U.S.
Find more articles, browse back issues, and read the current issue of WebMD Magazine.
Have you felt exhausted lately? Can you barely make it up the stairs without getting winded even though you’re physically fit? If so, you might be lacking in iron — especially if you’re a woman.
Although many people don’t think of iron as being a nutrient, you might be surprised to learn that low iron is the most common nutritional deficiency in the U.S. Almost 10% of women are iron deficient, according to figures from the Centers for Disease Control and Prevention.
Let’s look at why iron is so important to your body, what can happen if you’re not getting enough of it, and when you need to take an iron supplement.
Why Do You Need Iron?
Iron is an essential mineral. “The major reason we need it is that it helps to transport oxygen throughout the body,” says Paul Thomas, EdD, RD, a scientific consultant to the National Institutes of Health, Office of Dietary Supplements.
Iron is an important component of hemoglobin, the substance in red blood cells that carries oxygen from your lungs to transport it throughout your body. Hemoglobin represents about two-thirds of the body’s iron. If you don’t have enough iron, your body can’t make enough healthy oxygen-carrying red blood cells. A lack of red blood cells is called iron deficiency anemia.
Without healthy red blood cells, your body can’t get enough oxygen. “If you’re not getting sufficient oxygen in the body, you’re going to become fatigued,” Thomas says. That exhaustion can affect everything from your brain function to your immune system’s ability to fight off infections. If you’re pregnant, severe iron deficiency may increase your baby’s risk of being born too early, or smaller than normal.
Iron has other important functions, too. “Iron is also necessary to maintain healthy cells, skin, hair, and nails,” says Elaine Chottiner, MD, clinical assistant professor and director of General Hematology Clinics at the University of Michigan Medical Center said in an email interview.
How Much Iron Do You Need?
How much iron you need each day depends on your age, gender, and overall health.
Infants and toddlers need more iron than adults, in general, because their bodies are growing so quickly. In childhood, boys and girls need the same amount of iron — 10 milligrams daily from ages 4 to 8, and 8 mg daily from ages 9 to 13.
Starting at adolescence, a woman’s daily iron needs increase. Women need more iron because they lose blood each month during their period. That’s why women from ages 19 to 50 need to get 18 mg of iron each day, while men the same age can get away with just 8 mg.
After menopause, a woman’s iron needs drop as their menstrual cycle ends. After a woman begins menopause, both men and women need the same amount of iron — 8 mg each day.
You might need more iron, either from dietary sources or from an iron supplement, if you:
Have kidney failure (especially if you are undergoing dialysis, which can remove iron from the body)
Have an ulcer, which can cause blood loss
Have a gastrointestinal disorder that prevents your body from absorbing iron normally (such as celiac disease, Crohn’s disease, or ulcerative colitis)
Take too many antacids, which can prevent your body from absorbing iron
Have had weight loss (bariatric) surgery
Work out a lot (intense exercise can destroy red blood cells)
If you are a vegetarian or vegan, you may also need to take an iron supplement, because the body doesn’t absorb the type of iron found in plants as well as it absorbs the iron from meat.
How Do You Know If You’re Iron Deficient?
“People often don’t know they have anemia until they have signs or symptoms — they appear pale or ‘sallow,’ are fatigued, or have difficulty exercising,” Chottiner says.
Severe iron deficiency can cause difficulty in swallowing
If you’re tired and dragging, see your doctor. “It’s fairly easy to detect and diagnose the different stages of iron deficiency with a simple blood test,” Thomas says. Women who are pregnant and people with a gastrointestinal disorder such as Crohn’s, ulcerative colitis, or celiac disease should have their iron tested on a regular basis.
Do You Need to Take an Iron Supplement?
If your iron is low, eating a diet that is high in iron-rich foods such as fortified cereals, red meat, dried fruit, and beans may not be enough to give you what you need. Your doctor might recommend that you take an iron supplement.
Prenatal vitamins usually include iron, but not all prenatal vitamins contain the recommended amount. Check with your doctor before taking any supplement.
While you are taking iron supplements, your doctor should test your blood to see if your iron levels have improved.
Can Iron Supplements Cause Side Effects?
Iron supplements can cause side effects, usually stomach upset such as nausea, vomiting, diarrhea, dark stools, or constipation. Pregnant women are especially susceptible to constipation. Adding extra fiber to your diet can help relieve this symptom. A stool softener may also make you feel better.
Starting with a low dose of iron and then gradually increasing the dose to the daily recommended amount may help minimize side effects. If your iron supplements are bothering your stomach, your doctor can adjust the dose or form of iron you use. You can also try taking the supplements with food.
Can You Take Too Much Iron?
Unlike some supplements, when the subject is iron, more is definitely not better. Adults shouldn’t take any more than 45 mg of iron a day unless they are being treated with iron under close medical supervision.
For children, iron overdose can be especially toxic. “Iron supplements have killed young children because their needs for iron compared to an adult’s are relatively low,” Thomas says. If you take iron supplements, it is very important to keep them in a high, locked cabinet, far out of your children’s reach. Symptoms of iron poisoning include severe vomiting, diarrhea, abdominal pain, dehydration, and bloody stool in children.
It’s difficult for adults to overdose on iron just from food and supplements, because an adult body has systems in place to regulate the amount of iron it absorbs. However, people with the inherited condition hemochromatosis have trouble regulating their iron absorption.
Although most people only absorb about 10% of the iron they consume, people with hemochromatosis absorb up to 30%. As a result, the iron in their body can build up to dangerous levels. That excess iron can deposit in organs such as the liver, heart, and pancreas, which can lead to conditions like cirrhosis, heart failure, and diabetes. For that reason, people with hemochromatosis should not take iron supplements.
Oct. 11, 2022 – Weeks after Jeannie Volpe caught COVID-19 in November 2020, she could no longer do her job running sexual assault support groups in Anniston, AL, because she kept forgetting the details that survivors had shared with her. “People were telling me they were having to revisit their traumatic memories, which isn’t fair to anybody,” the 47-year-old says.
Volpe has been diagnosed with long-COVID autonomic dysfunction, which includes severe muscle pain, depression, anxiety, and a loss of thinking skills. Some of her symptoms are more commonly known as brain fog, and they’re among the most frequent problems reported by people who have long-term issues after a bout of COVID-19.
Many experts and medical professionals say they haven’t even begun to scratch the surface of what impact this will have in years to come.
“I’m very worried that we have an epidemic of neurologic dysfunction coming down the pike,” says Pamela Davis, MD, PhD, a research professor at Case Western Reserve University’s School of Medicine in Cleveland.
In the 2 years Volpe has been living with long COVID, her executive function – the mental processes that enable people to focus attention, retain information, and multitask – has been so diminished that she had to relearn to drive. One of the various doctors assessing her has suggested speech therapy to help Volpe relearn how to form words. “I can see the words I want to say in my mind, but I can’t make them come out of my mouth,” she says in a sluggish voice that gives away her condition.
All of those symptoms make it difficult for her to care for herself. Without a job and health insurance, Volpe says she’s researched assisted suicide in the states that allow it but has ultimately decided she wants to live.
“People tell you things like you should be grateful you survived it, and you should; but you shouldn’t expect somebody to not grieve after losing their autonomy, their career, their finances.”
The findings of researchers studying the brain effects of COVID-19 reinforce what people with long COVID have been dealing with from the start. Their experiences aren’t imaginary; they’re consistent with neurological disorders – including myalgic encephalomyelitis, also known as chronic fatigue syndrome, or ME/CFS – which carry much more weight in the public imagination than the term brain fog, which can often be used dismissively.
Studies have found that COVID-19 is linked to conditions such as strokes; seizures; and mood, memory, and movement disorders.
While there are still a lot of unanswered questions about exactly how COVID-19 impacts the brain and what the long-term effects are, there’s enough reason to suggest people should be trying to avoid both infection and reinfection until researchers get more answers.
Worldwide, it’s estimated that COVID-19 has contributed to more than 40 million new cases of neurological disorders, says Ziyad Al-Aly, MD, a clinical epidemiologist and long COVID researcher at Washington University in St. Louis. In his latest study of 14 million medical records of the U.S. Department of Veterans Affairs, the country’s largest integrated health care system, researchers found that regardless of age, gender, race, and lifestyle, people who have had COVID-19 are at a higher risk of getting a wide array of 44 neurological conditions after the first year of infection.
He noted that some of the conditions, such as headaches and mild decline in memory and sharpness, may improve and go away over time. But others that showed up, such as stroke, encephalitis (inflammation of the brain), and Guillain-Barre syndrome (a rare disorder in which the body’s immune system attacks the nerves), often lead to lasting damage. Al-Aly’s team found that neurological conditions were 7% more likely in those who had COVID-19 than in those who had never been infected.
What’s more, researchers noticed that compared with control groups, the risk of post-COVID thinking problems was more pronounced in people in their 30s, 40s, and 50s – a group that usually would be very unlikely to have these problems. For those over the age of 60, the risks stood out less because at that stage of life, such thinking problems aren’t as rare.
Another of study of the veterans’ system last year showed that COVID-19 survivors were at a 46% higher risk of considering suicide after 1 year.
“We need to be paying attention to this,” says Al-Aly. “What we’ve seen is really the tip of the iceberg.” He worries that millions of people, including youths, will lose out on employment and education while dealing with long-term disabilities – and the economic and societal implications of such a fallout. “What we will all be left with is the aftermath of sheer devastation in some people’s lives,” he says.
Igor Koralnik, MD, chief of neuro-infectious disease and global neurology at Northwestern University in Chicago, has been running a specialized long COVID clinic. His team published a paper in March 2021 detailing what they saw in their first 100 patients. “About half the population in the study missed at least 10 days of work. This is going to have persistent impact on the workforce,” Koralnik said in a podcast posted on the Northwestern website. “We have seen that not only patients have symptoms, but they have decreased quality of life.”
For older people and their caregivers, the risk of potential neurodegenerative diseases that the virus has shown to accelerate, such as dementia, are also a big concern. Alzheimer’s is already the fifth leading cause of death for people 65 and older.
In a recent study of more than 6 million people over the age of 65, Davis and her team at Case Western found the risk of Alzheimer’s in the year after COVID-19 increased by 50% to 80%. The chances were especially high for women older than 85.
To date, there are no good treatments for Alzheimer’s, yet total health care costs for long-term care and hospice services for people with dementia topped $300 billion in 2020. That doesn’t even include the related costs to families.
“The downstream effect of having someone with Alzheimer’s being taken care of by a family member can be devastating on everyone,” she says. “Sometimes the caregivers don’t weather that very well.”
When Davis’s own father got Alzheimer’s at age 86, her mother took care of him until she had a stroke one morning while making breakfast. Davis attributes the stroke to the stress of caregiving. That left Davis no choice but to seek housing where both her parents could get care.
Looking at the broader picture, Davis believes widespread isolation, loneliness, and grief during the pandemic, and the disease of COVID-19 itself, will continue to have a profound impact on psychiatric diagnoses. This in turn could trigger a wave of new substance abuse as a result of unchecked mental health problems.
Still, not all brain experts are jumping to worst-case scenarios, with a lot yet to be understood before sounding the alarm. Joanna Hellmuth, MD, a neurologist and researcher at the University of California, San Francisco, cautions against reading too much into early data, including any assumptions that COVID-19 causes neurodegeneration or irreversible damage in the brain.
Even with before-and-after brain scans by University of Oxford researchers that show structural changes to the brain after infection, she points out that they didn’t actually study the clinical symptoms of the people in the study, so it’s too soon to reach conclusions about associated cognitive problems.
“It’s an important piece of the puzzle, but we don’t know how that fits together with everything else,” says Hellmuth. “Some of my patients get better. … I haven’t seen a single person get worse since the pandemic started, and so I’m hopeful.”
Sugar-free soft drinks, which have been around in various forms for almost 40 years, still have their problems. Remember Tab? Remember Coke Zero? Yes, they tasted sweet and saved you drinking some 40 teaspoons of sugar from each 375 ml can, but are they really healthier than regular soft drinks?
Brownie points
When you choose a diet drink, you may end up indulging in other sweet, kilojoule-dense options because you’ve been ‘good’. So, you’ll often see someone sipping a sugar-free drink while eating a chocolate bar, croissant or brownie. It confuses our brains.
Weight loss … or weight gain?
Sugar substitutes do little in the way of weight loss. In fact, the opposite may be true: some diet-beverage drinkers gain weight and have an increased risk of chronic diseases.
A 2010 study published in Physiology & Behavior concluded that regularly consuming sugar-sweetened drinks could lead to weight gain and an increased risk of developing type 2 diabetes.
In 2013, however, researchers had 200 people replace their sugary drinks with diet varieties or water for 6 months. Their conclusion? The sugar-free-beverage drinkers actually ate fewer desserts than the water drinkers. So there’s that.
A too-sweet taste?
When you drink them regularly, no-sugar soft drinks get you used to a sweet taste. This is a long-term problem for weight loss, as well as for people with type 2 diabetes, metabolic syndrome and cardiovascular disease. If your body is used to getting a super-sweet hit from diet soft drinks, it makes managing appetite much more difficult.
The sweetness signal tells our bodies to prepare for kilojoules (or calories) and our appetite is generated in readiness, but no kilojoules arrive. So we’re likely go out and consume other foods. In other words, sweeteners prep our bodies for a sugar fix but then don’t deliver. So sweeteners interfere with the learned responses that normally contribute to glucose and energy homeostasis.
How safe are they?
We know these sweeteners are safe, but what we don’t know are their long-term effects on appetite. So let’s just say, the scientific jury is still out on their long-term effects.
The bottom line
The key is only having sugar-free soft drinks as an occasional treat, not every day or when you feel thirsty. Long term, we don’t really know what these sweeteners are doing to our bodies. One or two is fine (say, if you’re going out to a club), but regularly consuming these zero-sugar drinks may lead to long-term overconsumption of other foods.


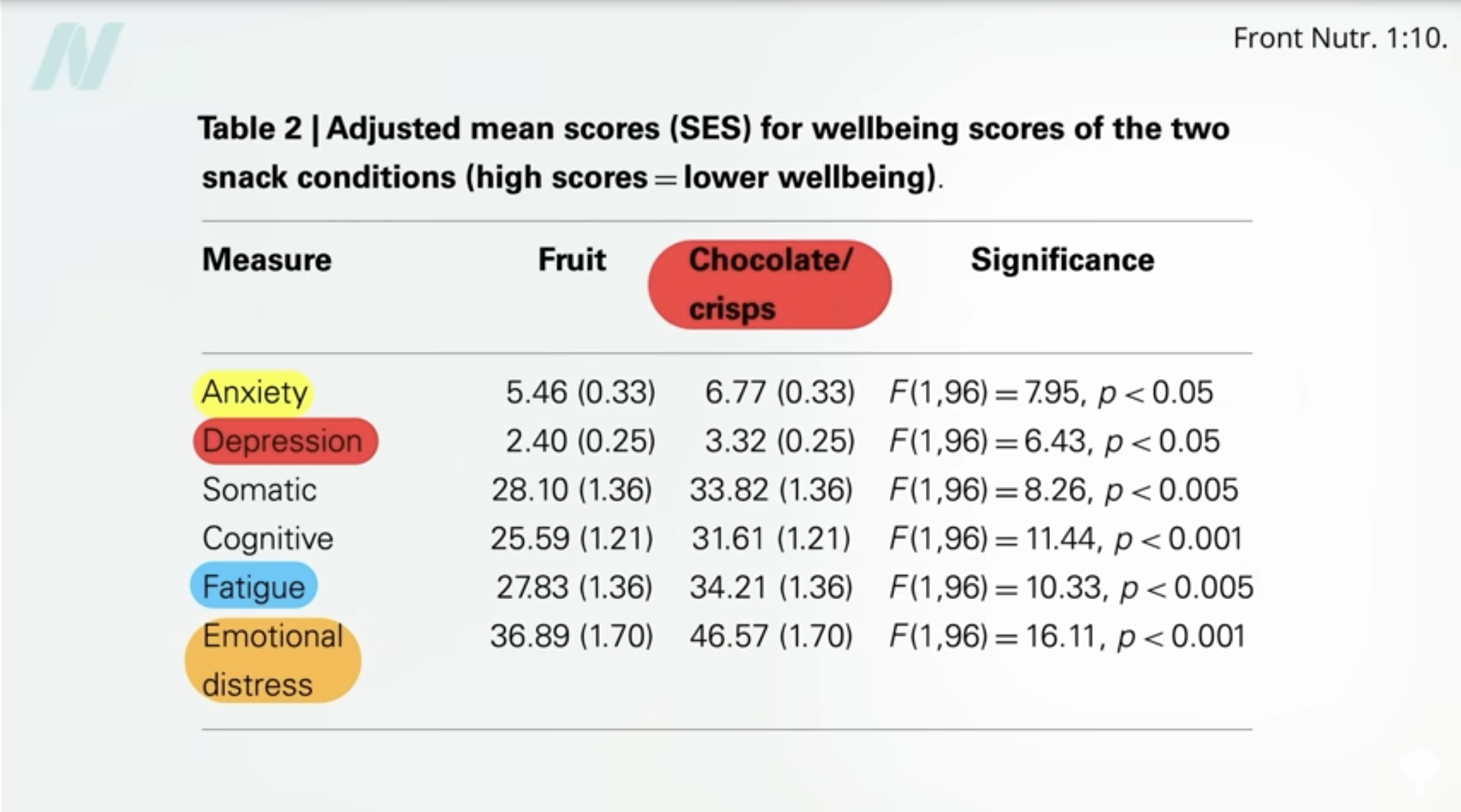



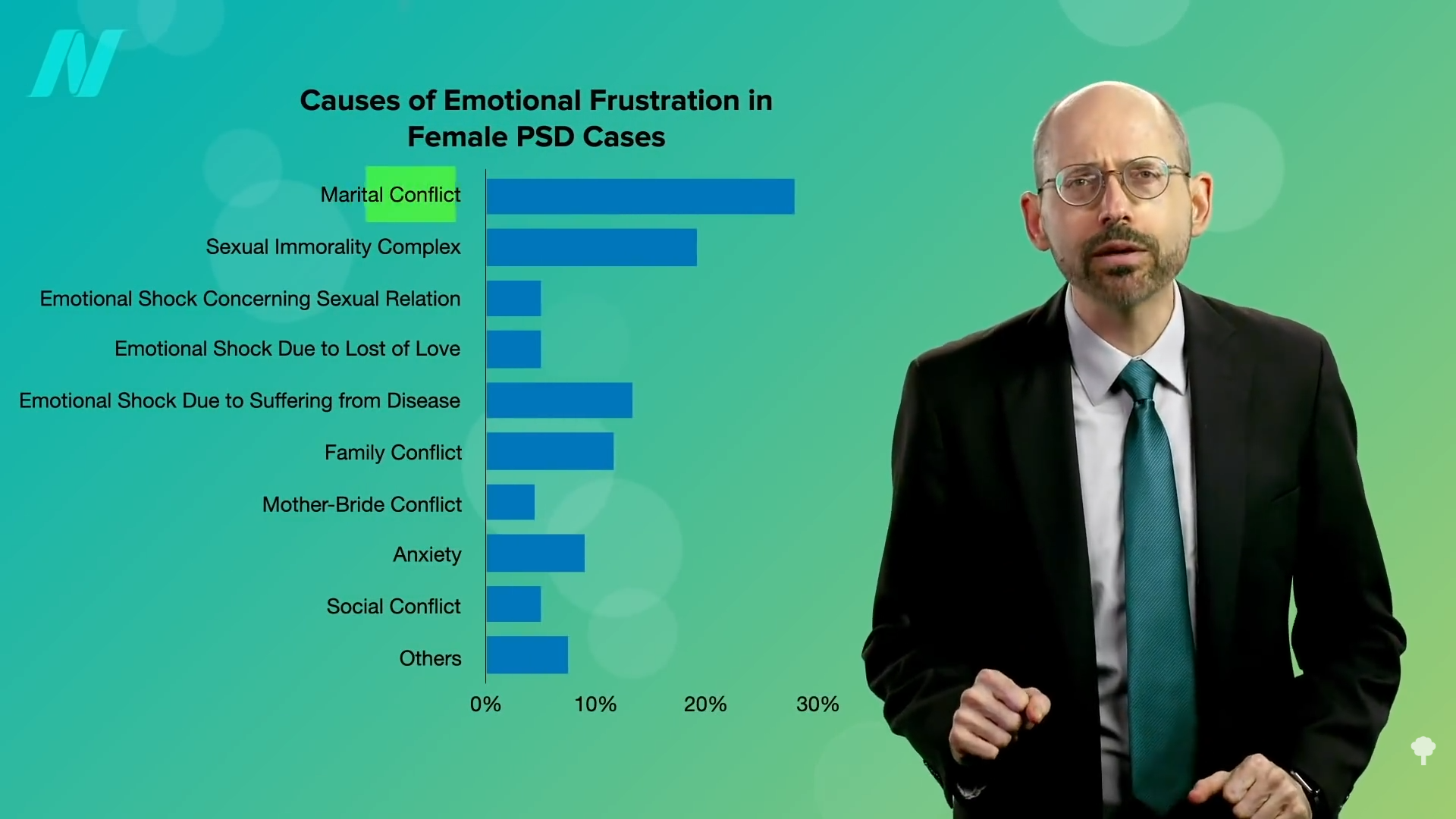
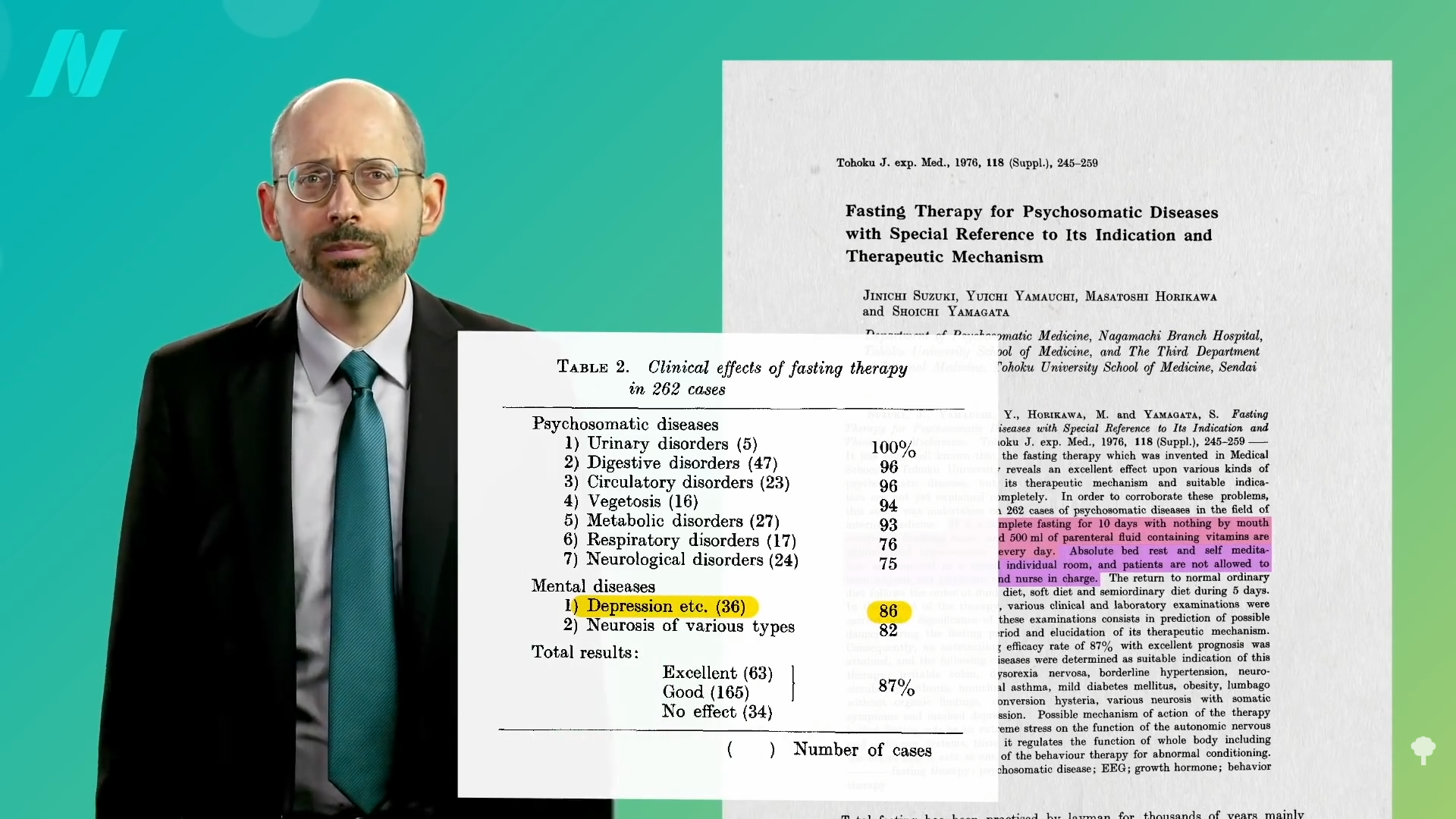
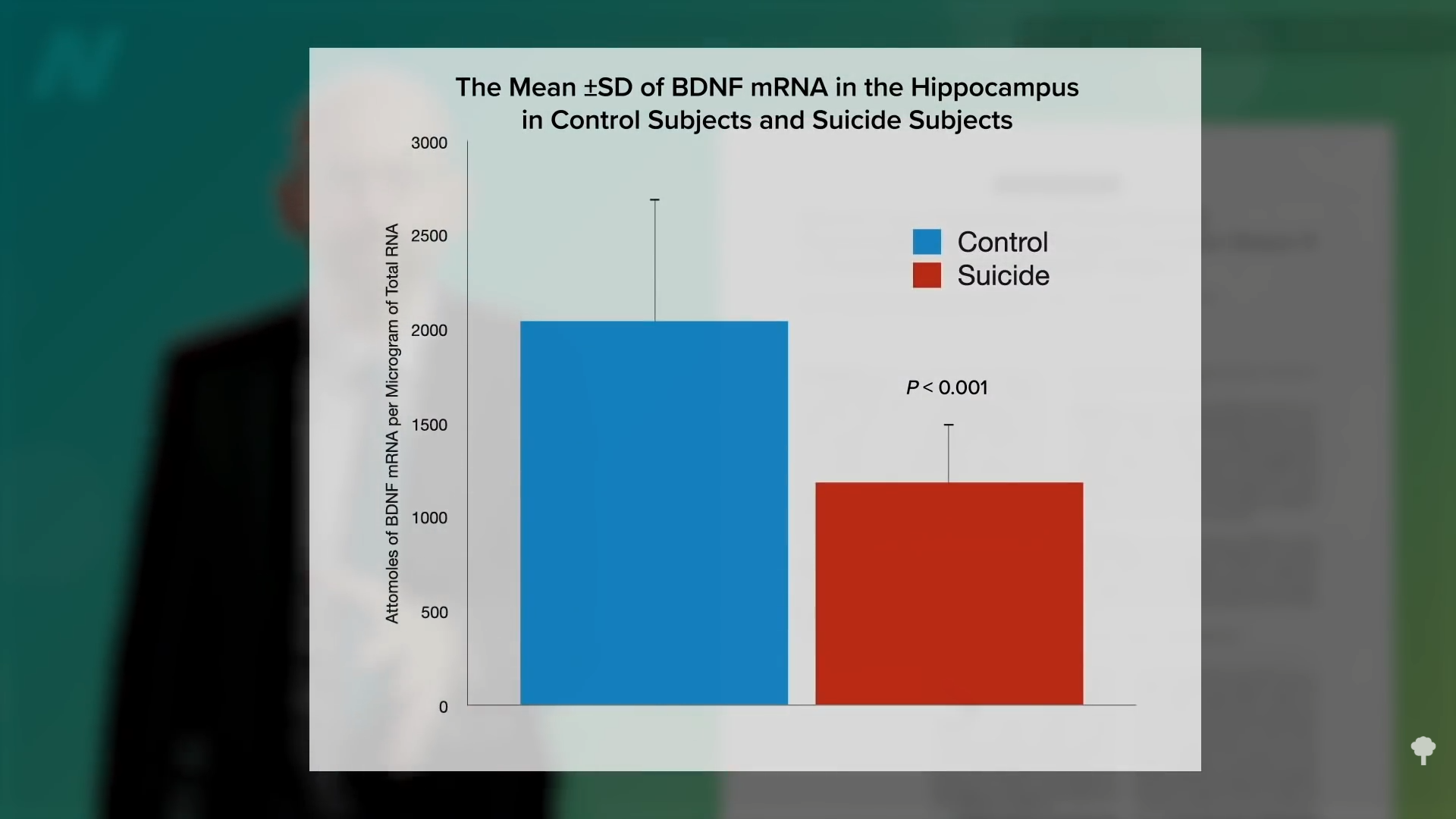
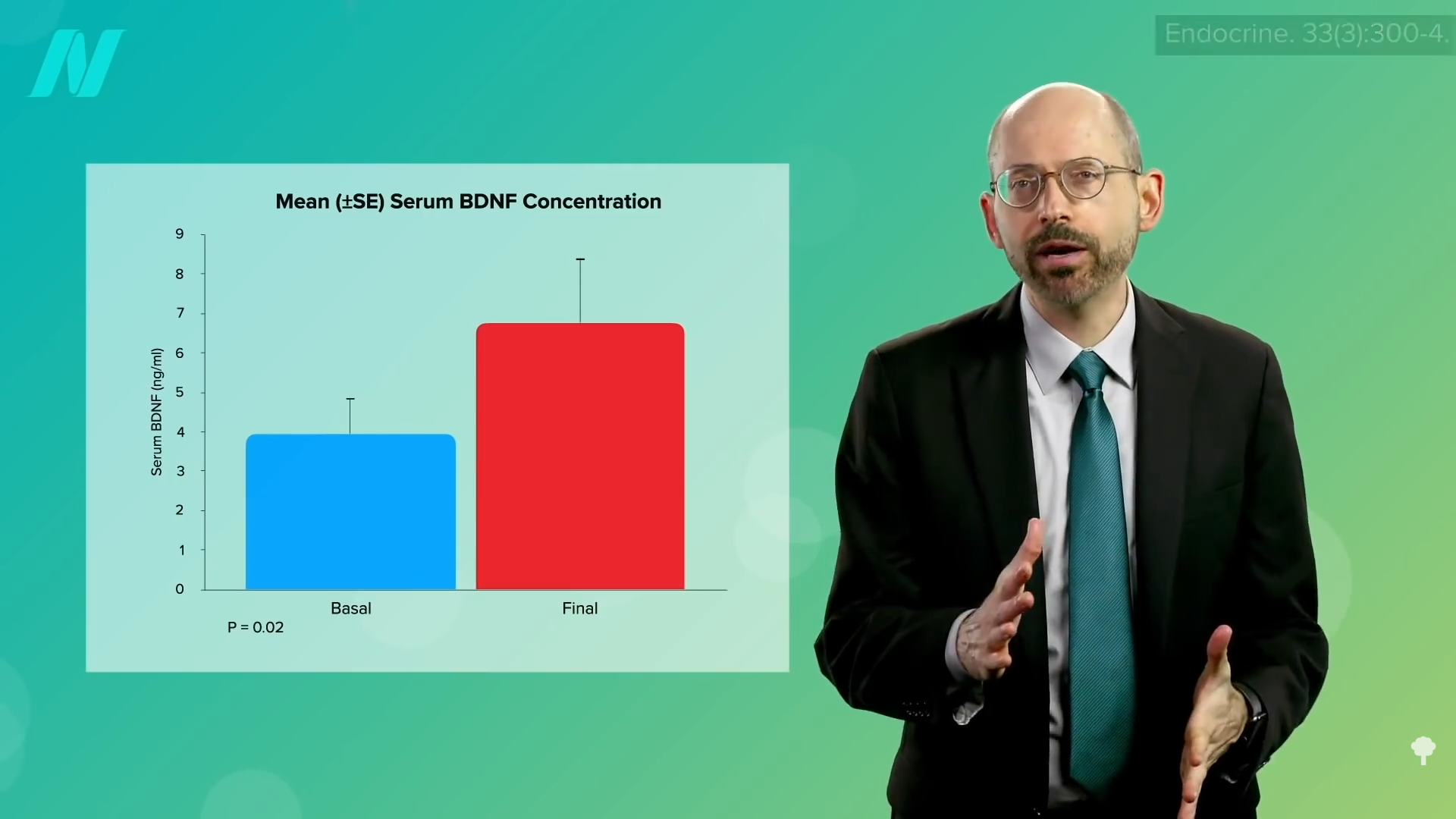

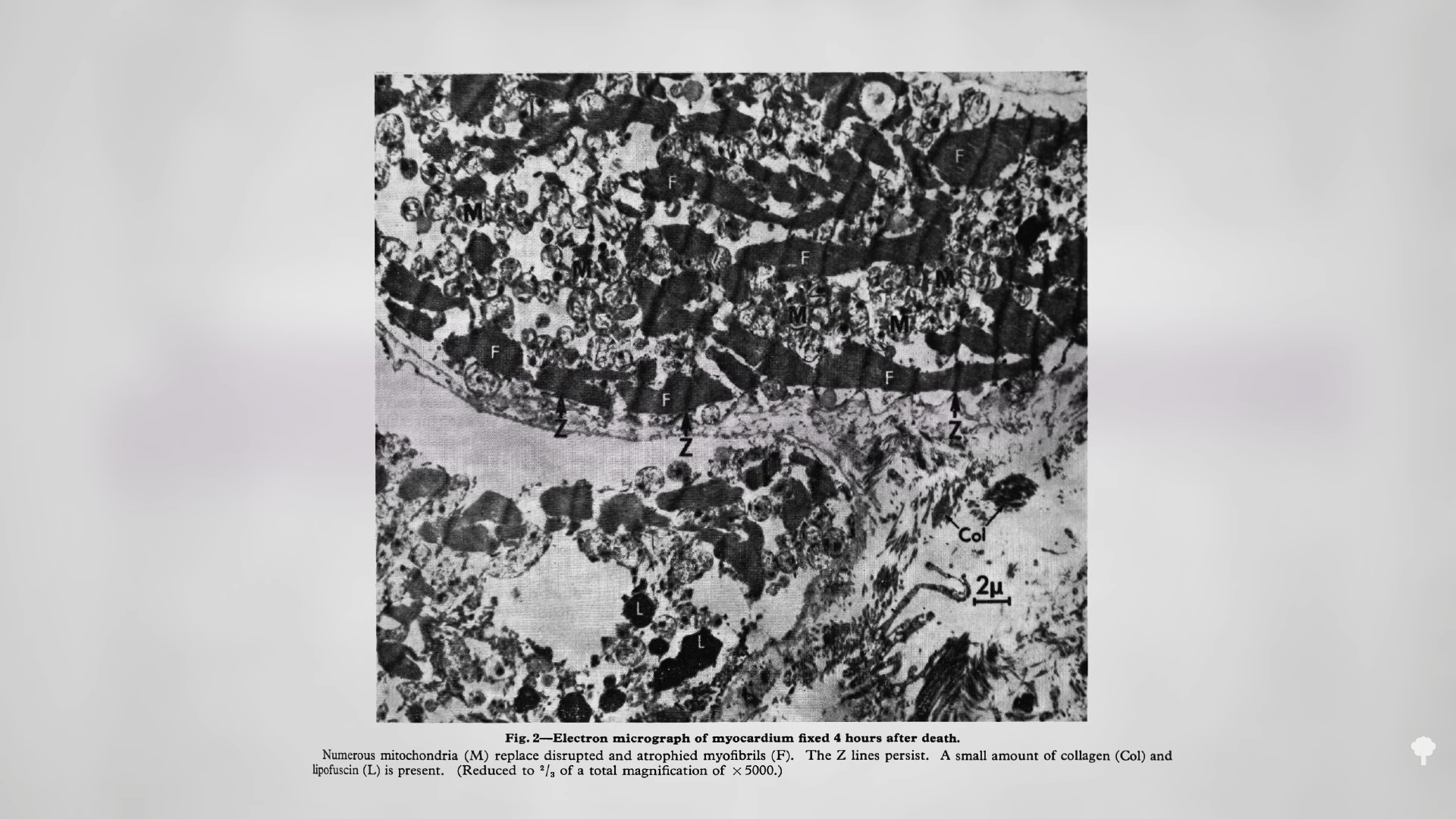
 Medically-supervised fasting has
Medically-supervised fasting has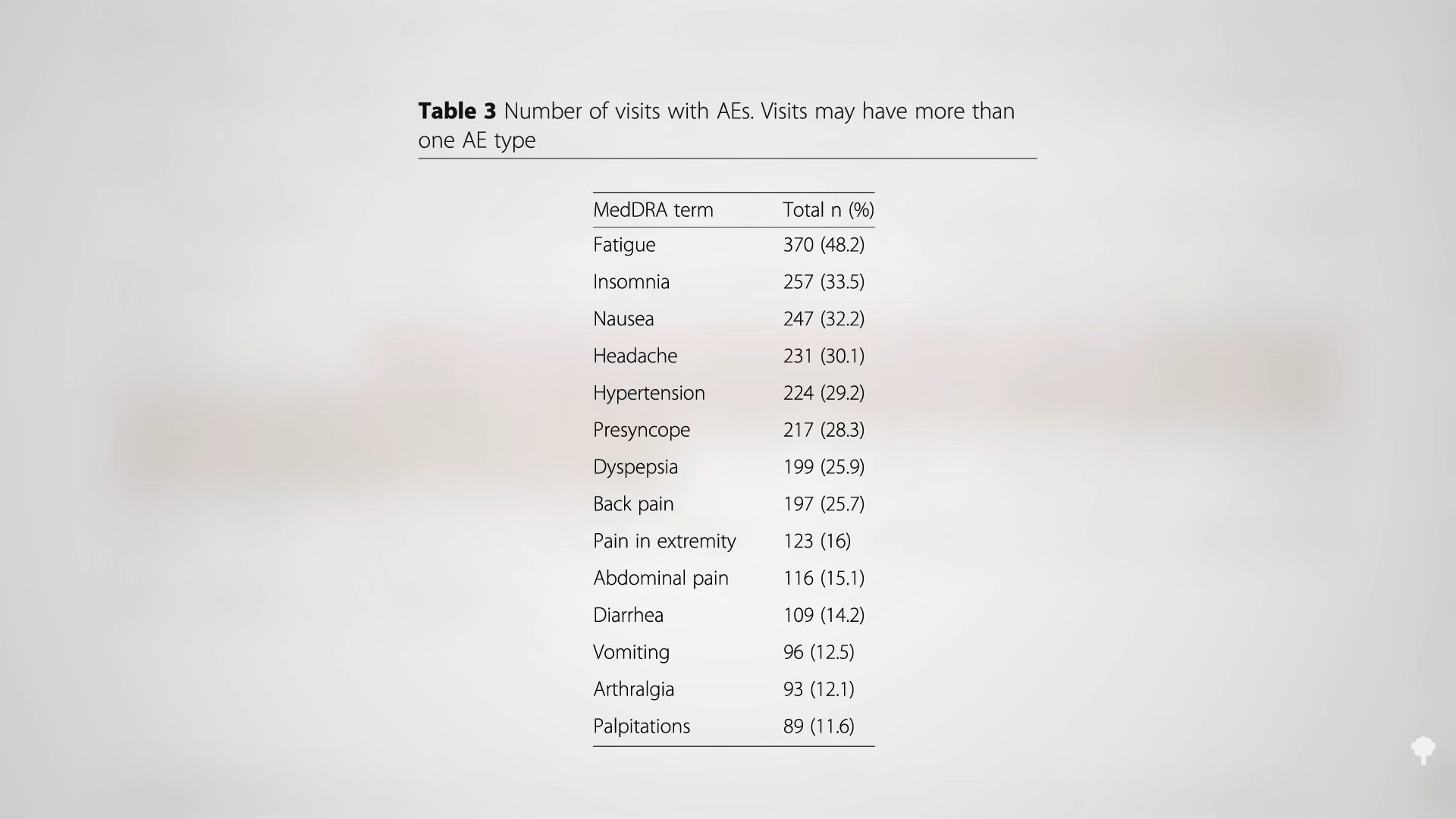 “
“






