[ad_1]
Is the brain damage associated with milk consumption due to the banned pesticide heptachlor or the milk sugar galactose?
Parkinson’s disease is a neurodegenerative brain disorder that affects millions of people. What causes it? Well, if you look at lifestyle factors associated with Parkinson’s disease, dairy consumption is the strongest dietary factor associated with an increased risk of Parkinson’s disease. In fact, dairy products are the only food group consistently linked with a high risk of developing Parkinson’s. Five large prospective studies have confirmed the link. This includes the two Harvard cohorts, the Nurses’ Health Study and the Health Professionals Follow-up Study, which followed more than 100,000 people combined for decades in “the largest analysis of dairy and PD [Parkinson’s disease] to date,” analyzing more than 1,000 newly diagnosed cases. All the studies found a link between dairy and Parkinson’s, with most finding a significant link—about a 50% increase in risk overall in those drinking the most milk compared to those drinking the least, at a p-value below 0.00001, meaning there’s less than a 1 in 100,000 chance you’d randomly get a finding that extreme. You can see this in the chart below and at 1:13 in my video, The Role Milk May Play in Triggering Parkinson’s Disease.
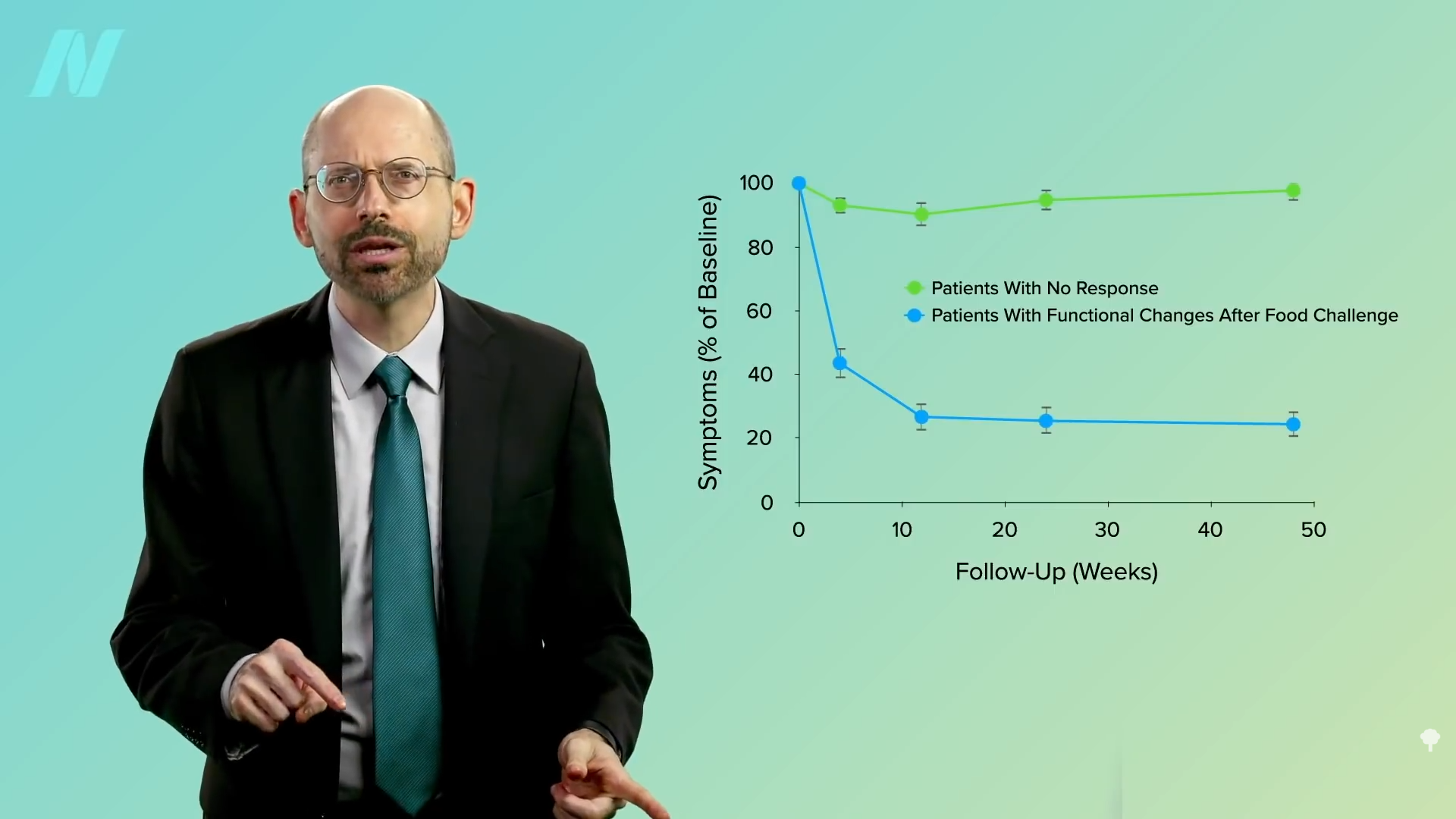
Okay, but why is there a link at all? “Despite clear-cut associations between milk intake and” incidence of Parkinson’s, “there is no rational explanation,” concluded one review. A year later, though, we got a clue: “Midlife milk consumption and substantia nigra neuron density at death.” What does that mean? Parkinson’s is caused primarily by the loss of a certain type of nerve cells in a critical part of the brain, with symptoms first appearing once most of these neurons have died. So one study looked at how much milk people drank when they were in their 40s, 50s, and 60s, and then examined their brains at autopsy and counted how many of those critical neurons they had left. In every single quadrant, neuron density was highest “in those who consumed no milk and lowest in those who consumed the most milk.” Even after removing the Parkinson’s cases, those drinking two cups (473 mL) of milk a day had up to 40% fewer nerve cells in most quadrants of that critical brain region. What’s in milk that could be wiping out brain cells? Among the people who drank the most milk, residues of the pesticide “heptachlor epoxide were found in 9 out of 10 brains.” So, maybe the finding of pesticide residues more commonly in the brains of those who drank the most milk could explain how milk could be cause-and-effect related to Parkinson’s disease risk.
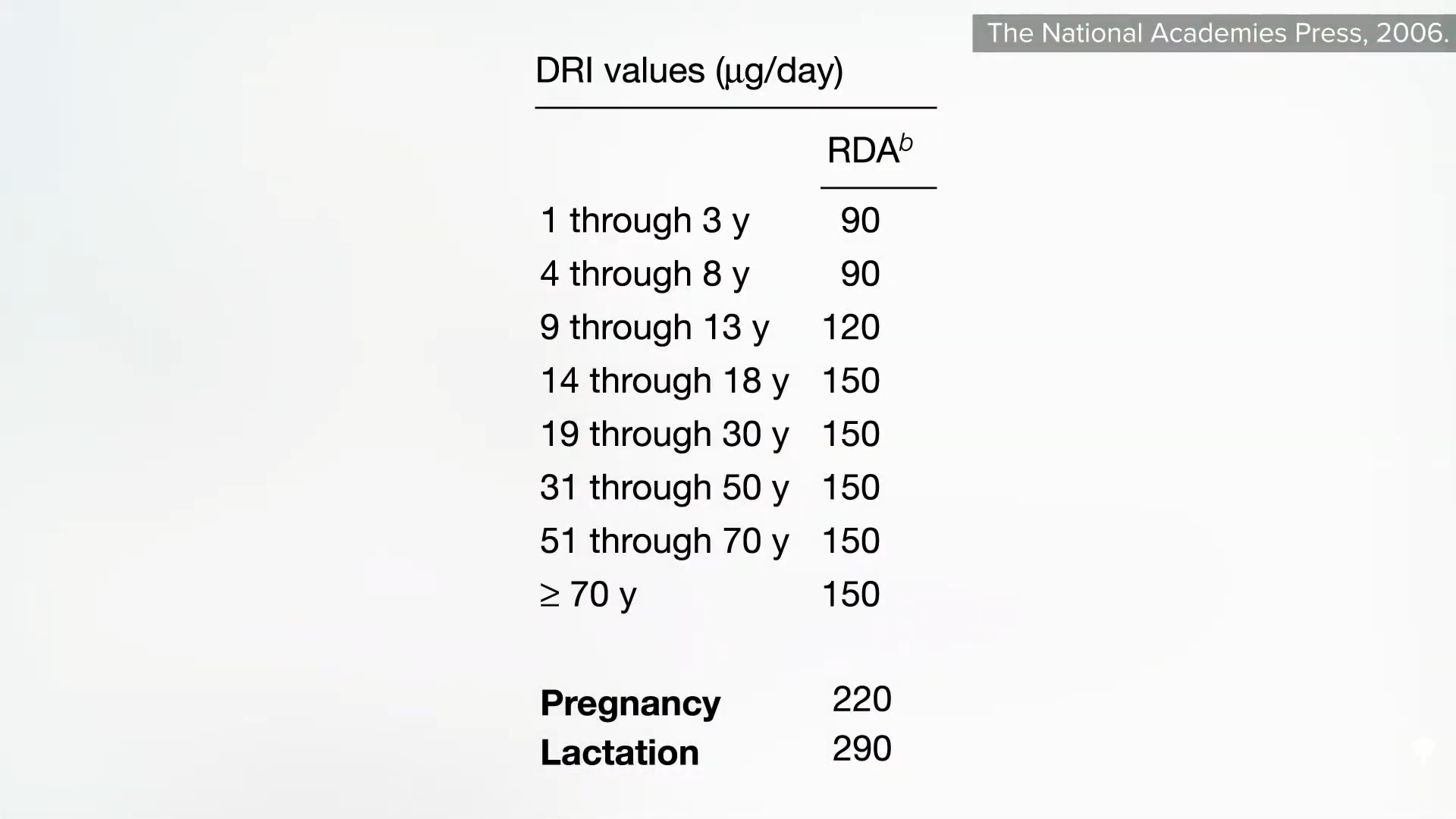
Now, that’s not the only potential explanation. In one of my videos, I talked about how meat contains that clumpy neurotoxic protein alpha-synuclein. Well, dairy products may contain trace amounts as well, but we don’t have confirmation of that. Could the milk sugar “galactose be the missing link?” Galactose is what the lactose in milk breaks down into once it’s in the body. It’s also what’s used to induce aging—to experimentally cause aging—in the brain. When you drink it, the galactose is picked up by your brain within a few hours, and for doses above 100 mg/kg, it appears that galactose can cause pathological alterations in brain cells, similar to those observed in Parkinson’s disease. This amount “can be reached and surpassed” by simply drinking two glasses (473 mL) of milk (the main dietary source of galactose) each day. And of all your brain cells, those dopaminergic neurons—the ones that you need to retain to prevent Parkinson’s—may be more vulnerable to galactose-induced damage because they are more vulnerable to oxidative stress.
Galactose may also explain the findings linking milk drinking with higher death rates. You may be thinking, “Well, duh—the saturated butterfat is just cutting people’s lives short,” but higher mortality with high milk consumption has been observed regardless of the milk fat content. Skim milk might be fat-free, but it’s not lactose-free.
Can’t you just drink lactose-free milk, like Lactaid? That has the lactase enzyme added to make lactose-free milk. But it just breaks down lactose into galactose in the carton rather than in your gut, so you’re still ingesting the same amount of galactose. Perhaps it’s no wonder that more milk intake at midlife may be linked to a greater rate of cognitive decline. Remember, researchers use galactose to create brain aging in the laboratory. D-galactose, a metabolic derivative of lactose, has been extensively used in animal models “to mimic cognitive aging” through oxidative stress. Compared to those who said they “almost never” drink milk, those drinking more than one glass (237 mL) a day appear more likely to suffer a decline in global cognitive function.
Doctor’s Note
Here’s the meat video I mentioned: The Role Meat May Play in Triggering Parkinson’s Disease.
You may remember that I’ve explored this before in Could Lactose Explain the Milk and Parkinson’s Disease Link?. Uric acid may also be a contender—see Parkinson’s Disease and the Uric Acid Sweet Spot.
For more on Parkinson’s disease, check out related posts below.
[ad_2]
Michael Greger M.D. FACLM
Source link
 We appear to
We appear to