[ad_1]
In this pioneering study of the ketogenic diet, all patients improved and most were discharged on less medication.
[ad_2]
Nutrition | ReportWire publishes the latest breaking U.S. and world news, trending topics and developing stories from around globe.

[ad_1]
In this pioneering study of the ketogenic diet, all patients improved and most were discharged on less medication.
[ad_2]

[ad_1]
I am pleased to share a new paper my colleagues and I published in Frontiers in Psychiatry describing the potential benefits of a ketogenic diet in patients with bipolar disorder, major depression, and schizoaffective disorder. University of Toulouse psychiatrist Dr. Albert Danan found that a whole-foods ketogenic diet was safe, feasible, and associated with unprecedented improvements in mental and physical health in hospitalized patients with serious mental illness.
Dr. Danan’s patients are primarily people of French and North African descent with serious, persistent mental illness, all of whom also suffer from metabolic illnesses such as obesity, hypertension, and type two diabetes.
After witnessing marked improvement in seizures and autism behaviors in a family member within several weeks of having adopted a ketogenic diet, Dr. Danan became interested in the potential of the diet to improve the psychiatric and metabolic status of his most treatment-resistant patients, regardless of diagnosis. He created a metabolic psychiatry treatment program within his local hospital where patients with chronic mental illness who had exhausted standard psychiatric therapies could attempt a ketogenic diet in a supportive, medically supervised environment.
Dr. Danan admitted 31 of his patients with major depression, bipolar disorder, or schizophrenia to the Clinique du Castelviel in Toulouse where they were served a ketogenic diet in lieu of standard hospital fare. The program he implemented limits total carbohydrate intake to a maximum of 20 grams per day, and was based on the ketogenic diet protocol used by Dr. Eric Westman in his metabolic research at Duke University. [A description of the diet is included in the Supplemental Materials section of the paper.]
Symptoms of depression and psychosis improved in all 28 patients who followed the diet for longer than two weeks, with improvements becoming noticeable within three weeks or less. Almost half (43%) of patients achieved clinical remission according to the Clinical Global Impressions Scale (CGI-S) which measures illness severity, and 64% were discharged from the hospital on less psychiatric medication. Dr. Danan had never witnessed this degree of improvement before in any of these patients—most of whom he had worked with for years or even decades, and all of whom had previously been hospitalized under his care one or more times.
Patients also experienced significant improvements in markers of metabolic health, including blood pressure, blood glucose, triglycerides, and weight:
All but one patient lost weight including 96% of those who were taking antipsychotics, and nearly half achieved clinically significant weight loss [defined as ≥5% reduction in body weight]. This welcome outcome alone makes a compelling case for the implementation of the KD [ketogenic diet] in people who are taking antipsychotic medications, whether or not psychiatric symptoms improve in response to the KD, as counteracting antipsychotic-induced weight gain is extremely difficult.
Until now, the evidence in support of ketogenic diets specifically for psychiatric conditions has been limited to hypothesis papers, animal studies, and a small but growing number of individual case reports.
As this was not a controlled trial, the extent to which the ketogenic diet may or may not have directly contributed to the outcomes reported cannot be ascertained. However, since this is the first time that a group of patients this large and this diagnostically diverse has ever been treated with a ketogenic diet in a hospital setting, these clinical observations serve to bridge the gap between existing case reports and the controlled clinical trials already underway at other institutions around the world.
When asked to reflect on his experience as principal investigator of this study, Dr. Danan said:
During my career, I’ve been struck by the limits of conventional therapies in psychiatry. Most patients relapse and have a poor quality of life. Most of them suffer from dramatic weight gain, obesity, diabetes, hypertension, and metabolic syndrome. Loss of life expectancy in this population can be measured in decades. This is a matter of public health and much more attention must be paid to these problems.
Introducing nutritional measures, particularly the ketogenic diet, helped me considerably to improve the results of therapy. Patients began improving their metabolic status by losing weight, improving blood pressure, etc., but most importantly, I observed real improvements in their psychiatric symptoms such as hallucinations, delusions, and mood instability.
After having led this study I’m convinced that nutritional measures can have a profound impact and lead to very important benefits, which makes me say that this represents the future direction to develop in psychiatric care.
Albert Danan MD conceived of and implemented the intervention and generated clinical data and observations. Georgia Ede MD conducted the literature review and wrote the manuscript. Eric C. Westman MD and Laura R. Saslow PhD performed statistical analyses. You can read the study for free here.
Note: A version of this article was previously published on Psychology Today.
[ad_2]

[ad_1]
I am pleased to share a new paper my colleagues and I published in Frontiers in Psychiatry describing the potential benefits of a ketogenic diet in patients with bipolar disorder, major depression, and schizoaffective disorder. University of Toulouse psychiatrist Dr. Albert Danan found that a whole-foods ketogenic diet was safe, feasible, and associated with unprecedented improvements in mental and physical health in hospitalized patients with serious mental illness.
Dr. Danan’s patients are primarily people of French and North African descent with serious, persistent mental illness, all of whom also suffer from metabolic illnesses such as obesity, hypertension, and type two diabetes.
After witnessing marked improvement in seizures and autism behaviors in a family member within several weeks of having adopted a ketogenic diet, Dr. Danan became interested in the potential of the diet to improve the psychiatric and metabolic status of his most treatment-resistant patients, regardless of diagnosis. He created a metabolic psychiatry treatment program within his local hospital where patients with chronic mental illness who had exhausted standard psychiatric therapies could attempt a ketogenic diet in a supportive, medically supervised environment.
Dr. Danan admitted 31 of his patients with major depression, bipolar disorder, or schizophrenia to the Clinique du Castelviel in Toulouse where they were served a ketogenic diet in lieu of standard hospital fare. The program he implemented limits total carbohydrate intake to a maximum of 20 grams per day, and was based on the ketogenic diet protocol used by Dr. Eric Westman in his metabolic research at Duke University. [A description of the diet is included in the Supplemental Materials section of the paper.]
Symptoms of depression and psychosis improved in all 28 patients who followed the diet for longer than two weeks, with improvements becoming noticeable within three weeks or less. Almost half (43%) of patients achieved clinical remission according to the Clinical Global Impressions Scale (CGI-S) which measures illness severity, and 64% were discharged from the hospital on less psychiatric medication. Dr. Danan had never witnessed this degree of improvement before in any of these patients—most of whom he had worked with for years or even decades, and all of whom had previously been hospitalized under his care one or more times.
Patients also experienced significant improvements in markers of metabolic health, including blood pressure, blood glucose, triglycerides, and weight:
All but one patient lost weight including 96% of those who were taking antipsychotics, and nearly half achieved clinically significant weight loss [defined as ≥5% reduction in body weight]. This welcome outcome alone makes a compelling case for the implementation of the KD [ketogenic diet] in people who are taking antipsychotic medications, whether or not psychiatric symptoms improve in response to the KD, as counteracting antipsychotic-induced weight gain is extremely difficult.
Until now, the evidence in support of ketogenic diets specifically for psychiatric conditions has been limited to hypothesis papers, animal studies, and a small but growing number of individual case reports.
As this was not a controlled trial, the extent to which the ketogenic diet may or may not have directly contributed to the outcomes reported cannot be ascertained. However, since this is the first time that a group of patients this large and this diagnostically diverse has ever been treated with a ketogenic diet in a hospital setting, these clinical observations serve to bridge the gap between existing case reports and the controlled clinical trials already underway at other institutions around the world.
When asked to reflect on his experience as principal investigator of this study, Dr. Danan said:
During my career, I’ve been struck by the limits of conventional therapies in psychiatry. Most patients relapse and have a poor quality of life. Most of them suffer from dramatic weight gain, obesity, diabetes, hypertension, and metabolic syndrome. Loss of life expectancy in this population can be measured in decades. This is a matter of public health and much more attention must be paid to these problems.
Introducing nutritional measures, particularly the ketogenic diet, helped me considerably to improve the results of therapy. Patients began improving their metabolic status by losing weight, improving blood pressure, etc., but most importantly, I observed real improvements in their psychiatric symptoms such as hallucinations, delusions, and mood instability.
After having led this study I’m convinced that nutritional measures can have a profound impact and lead to very important benefits, which makes me say that this represents the future direction to develop in psychiatric care.
Albert Danan MD conceived of and implemented the intervention and generated clinical data and observations. Georgia Ede MD conducted the literature review and wrote the manuscript. Eric C. Westman MD and Laura R. Saslow PhD performed statistical analyses. You can read the study for free here.
Note: A version of this article was previously published on Psychology Today.
[ad_2]

[ad_1]
I am pleased to share a new paper my colleagues and I published in Frontiers in Psychiatry describing the potential benefits of a ketogenic diet in patients with bipolar disorder, major depression, and schizoaffective disorder. University of Toulouse psychiatrist Dr. Albert Danan found that a whole-foods ketogenic diet was safe, feasible, and associated with unprecedented improvements in mental and physical health in hospitalized patients with serious mental illness.
Dr. Danan’s patients are primarily people of French and North African descent with serious, persistent mental illness, all of whom also suffer from metabolic illnesses such as obesity, hypertension, and type two diabetes.
After witnessing marked improvement in seizures and autism behaviors in a family member within several weeks of having adopted a ketogenic diet, Dr. Danan became interested in the potential of the diet to improve the psychiatric and metabolic status of his most treatment-resistant patients, regardless of diagnosis. He created a metabolic psychiatry treatment program within his local hospital where patients with chronic mental illness who had exhausted standard psychiatric therapies could attempt a ketogenic diet in a supportive, medically supervised environment.
Dr. Danan admitted 31 of his patients with major depression, bipolar disorder, or schizophrenia to the Clinique du Castelviel in Toulouse where they were served a ketogenic diet in lieu of standard hospital fare. The program he implemented limits total carbohydrate intake to a maximum of 20 grams per day, and was based on the ketogenic diet protocol used by Dr. Eric Westman in his metabolic research at Duke University. [A description of the diet is included in the Supplemental Materials section of the paper.]
Symptoms of depression and psychosis improved in all 28 patients who followed the diet for longer than two weeks, with improvements becoming noticeable within three weeks or less. Almost half (43%) of patients achieved clinical remission according to the Clinical Global Impressions Scale (CGI-S) which measures illness severity, and 64% were discharged from the hospital on less psychiatric medication. Dr. Danan had never witnessed this degree of improvement before in any of these patients—most of whom he had worked with for years or even decades, and all of whom had previously been hospitalized under his care one or more times.
Patients also experienced significant improvements in markers of metabolic health, including blood pressure, blood glucose, triglycerides, and weight:
All but one patient lost weight including 96% of those who were taking antipsychotics, and nearly half achieved clinically significant weight loss [defined as ≥5% reduction in body weight]. This welcome outcome alone makes a compelling case for the implementation of the KD [ketogenic diet] in people who are taking antipsychotic medications, whether or not psychiatric symptoms improve in response to the KD, as counteracting antipsychotic-induced weight gain is extremely difficult.
Until now, the evidence in support of ketogenic diets specifically for psychiatric conditions has been limited to hypothesis papers, animal studies, and a small but growing number of individual case reports.
As this was not a controlled trial, the extent to which the ketogenic diet may or may not have directly contributed to the outcomes reported cannot be ascertained. However, since this is the first time that a group of patients this large and this diagnostically diverse has ever been treated with a ketogenic diet in a hospital setting, these clinical observations serve to bridge the gap between existing case reports and the controlled clinical trials already underway at other institutions around the world.
When asked to reflect on his experience as principal investigator of this study, Dr. Danan said:
During my career, I’ve been struck by the limits of conventional therapies in psychiatry. Most patients relapse and have a poor quality of life. Most of them suffer from dramatic weight gain, obesity, diabetes, hypertension, and metabolic syndrome. Loss of life expectancy in this population can be measured in decades. This is a matter of public health and much more attention must be paid to these problems.
Introducing nutritional measures, particularly the ketogenic diet, helped me considerably to improve the results of therapy. Patients began improving their metabolic status by losing weight, improving blood pressure, etc., but most importantly, I observed real improvements in their psychiatric symptoms such as hallucinations, delusions, and mood instability.
After having led this study I’m convinced that nutritional measures can have a profound impact and lead to very important benefits, which makes me say that this represents the future direction to develop in psychiatric care.
Albert Danan MD conceived of and implemented the intervention and generated clinical data and observations. Georgia Ede MD conducted the literature review and wrote the manuscript. Eric C. Westman MD and Laura R. Saslow PhD performed statistical analyses. You can read the study for free here.
Note: A version of this article was previously published on Psychology Today.
[ad_2]

[ad_1]
The CHIP program (now called Pivio) has attempted to take the pioneering lifestyle medicine work of Pritikin and Ornish and spread it out into the community.
England has been keeping mortality statistics since 1665 when one person was “killed by a fall down stairs at St. Thomas Apostle.” That same week, though, nearly 4,000 people died of the plague.
Today, the modern plague is heart disease, the number one killer of men and women, but it wasn’t always this way. If you dig into those old statistics, heart disease was already killing off 5 to 10 percent of the population by the middle of the last century, but it “was practically unknown at the beginning of the [20th] century.” Consider the natural history of coronary heart disease in the 1920s and 1930s. As you can see at 0:45 in my video What Is the Optimal Diet?, it skyrocketed tenfold in both men and in women. What was going on? We get a clue in a study that divided people by socioeconomic class. (You can tell the paper was written about 1950 because the subjects are identified as “Males” and “Wives.”) The richest folks had up to triple the heart disease of the poorest. Did it have something to do with their rich diets? You don’t know, until you put it to the test. In doing so, we discover “the natural cure of coronary heart disease,” found decades ago by Nathan Pritikin, who developed the eponymous plant-based diet and lifestyle program, followed by Dean Ornish and then Caldwell Esselstyn at the Cleveland Clinic, but how many know of the name Hans Diehl?
Dr. Diehl was the first director of research at the Pritikin Center back in 1976. He was inspired by the amazing results they were getting—amazing results like those gotten by a certain Grandma Frances Greger. Diehl “recognized the limitations of [live-in] residential programs, including their cost…and the ‘artificial’ living environment that made sustaining the learned behaviors more difficult for participants when they returned to their home setting. In response, Diehl developed CHIP”—now known as the Complete Health Improvement Program—“as an affordable 30-day lifestyle intervention to be delivered to individuals in their community.
Ten years in, Dr. Esselstyn encouraged Dr. Diehl to publish their results in the American Journal of Cardiology. “Coronary Risk Reduction Through Intensive Community-Based Lifestyle Intervention: The Coronary Health Improvement Project (CHIP) Experience” famously started with a quote from the pioneer of coronary bypass surgery who described it as “only a palliative treatment. The incidence of coronary disease will only be decreased by proper preventive measures.”
We know that “vigorous cholesterol lowering” can slow, arrest, or even reverse atherosclerosis, but it only works if you do it. Live-in programs work because you can control people’s diets, but they’re expensive and people may go back home to toxic food environments. So, instead of them coming to you, what if you go to them in the community?
The original program was 16 evening sessions over four weeks. “The major focus of the program was to encourage participants to adopt the Optimal Diet,” and they were also “encouraged to exercise 30 minutes a day.” Most importantly, however, they were to “embrace” centering their diet around whole plant foods. Now, that was the optimal—a whole food plant-based diet—but “the program did not prescribe a dietary dogma but instead encouraged participants to move along the spectrum toward the ad libitum consumption of vegetables, fruits, whole grains, and legumes”—incorporating more whole, healthy plant foods into their diets. They didn’t provide meals, just advice and encouragement. And, after only four weeks, there was an average weight loss of about six pounds, blood pressures went down about six points, bad LDL cholesterol went down 16 to 32 points, and fasting blood sugars dropped as well, as you can see below and at 3:36 in my video.
“Often, participants were able to decrease or discontinue antidiabetic, hypolipidemic [cholesterol-lowering], and antihypertensive [blood pressure–lowering] medication,” making their findings even more extraordinary. Indeed, they achieved better numbers on fewer drugs.
Live-in programs, such as the Pritikin Longevity Center and the McDougall Program, are great in that you can optimize the clinical benefits, but they can cost thousands of dollars and cause many participants to miss work. On the other hand, CHIP is cheap, and people can live at home, so they aren’t spoon-fed a perfect diet for a few weeks at some spa only to go back to their cupboards of cookies. CHIP is a free-living program, teaching people how to eat and stay healthy within their home environments. At least, that’s the theory. These remarkable results were after just four weeks in the program. “The true test, however, will be to what extent people adhere to their new lifestyle and sustain their health benefits,” looking forward to weeks, months, or even more than a year later, which we’ll explore in my video Flashback Friday: The Weight-Loss Program That Got Better with Time.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
We’re back to epidemiology this week, but it’s an interesting one. The paper is called “Dietary fats and their sources in association with the risk of bladder cancer: A pooled analysis of 11 prospective cohort studies” (Ref 1). The paper was published in January 2022, but it was recently reported by the UK Independent newspaper, which is when it came to my attention (Ref 2).
The paper opened with the global position on bladder cancer. It is the 10th most commonly diagnosed cancer worldwide, with approximately 573,000 new cases and 213,000 deaths each year (Ref 3). Approximately 75% of bladder cancer cases are nonmuscle invasive bladder cancer (NMIBC) “characterized by frequent recurrences, which requires intensive treatments and follow-up measures, posing a large burden on the national health care budgets and patient’s quality of life” (Ref 1).
The introduction to the paper noted that previous research has reported that fluids, fruit, vegetables and yogurt are associated with reduced risk of BC, while a ‘Western diet’ has been associated with a higher risk. This study set out to examine the effect of fat intake from different dietary sources on bladder cancer. It found and pooled data from 11 population studies. These included the countries involved in the European Prospective Investigation into Cancer (EPIC), which are Denmark, France, Germany, Italy, The Netherlands, Norway, Spain, Sweden, and United Kingdom. Plus, the Netherlands cohort study and the North America VITamins and Lifestyle cohort study (VITAL).
[ad_2]
Zoe
Source link

[ad_1]


 Zaytinya’s menu reflects the rich regional diversity of classical Turkish, Greek, and Lebanese cuisines. They use authentic ingredients and traditional techniques. Truly an epic restaurant. The decor and ambiance are even as great as the food!
Zaytinya’s menu reflects the rich regional diversity of classical Turkish, Greek, and Lebanese cuisines. They use authentic ingredients and traditional techniques. Truly an epic restaurant. The decor and ambiance are even as great as the food!
 For lunch, we had Sea Scallops, Octopus Santorini, and Lamb with Tabouli. It was all so fresh and full of flavor!
For lunch, we had Sea Scallops, Octopus Santorini, and Lamb with Tabouli. It was all so fresh and full of flavor! They are known for “Mezze” which are small plates of the Eastern Mediterranean, regionally known as maza or meze.
They are known for “Mezze” which are small plates of the Eastern Mediterranean, regionally known as maza or meze.  Zaytinya is truly an authentic Mediterranean restaurant. Everything is made fresh in the kitchen using authentic & clean ingredients. You can truly taste the freshness!
Zaytinya is truly an authentic Mediterranean restaurant. Everything is made fresh in the kitchen using authentic & clean ingredients. You can truly taste the freshness! If you are in the D.C. area I highly recommend checking out Zaytinya. Coming soon to NYC!
If you are in the D.C. area I highly recommend checking out Zaytinya. Coming soon to NYC![ad_2]

[ad_1]


 This past week in Orlando I tried Purple Ocean Superfood Bar for the first time and it was EPIC! Josiah, the owner is from Puerto Rico and created Purple Ocean Superfood Bar in order to not only bring home a little closer but also to promote well-being through healthy eating. Purple Ocean not only brings the Caribbean feel of Puerto Rico to Orlando but is a healthy option for locals as well.
This past week in Orlando I tried Purple Ocean Superfood Bar for the first time and it was EPIC! Josiah, the owner is from Puerto Rico and created Purple Ocean Superfood Bar in order to not only bring home a little closer but also to promote well-being through healthy eating. Purple Ocean not only brings the Caribbean feel of Puerto Rico to Orlando but is a healthy option for locals as well.
 Purple Ocean is mostly vegan (except honey), they use 80% organic products, and have gluten-free options. They serve the most amazing acai bowls I have ever seen – they come in a pineapple shell! Each acai bowl is named after a surf break in Puerto Rico – how cool! The bowls taste as good as they look! Purple Ocean also serves 3 different plant-based burgers, fries, and a variety of smoothie and drink options.
Purple Ocean is mostly vegan (except honey), they use 80% organic products, and have gluten-free options. They serve the most amazing acai bowls I have ever seen – they come in a pineapple shell! Each acai bowl is named after a surf break in Puerto Rico – how cool! The bowls taste as good as they look! Purple Ocean also serves 3 different plant-based burgers, fries, and a variety of smoothie and drink options.


 I tried both the Roasted Garlic Quinoa burger and a Beyond Meat burger. Beyond meat is definitely a major upgrade for other plant-based meat options on the market. It’s super tasty and if you are wanting to have a “burger” every once in a while this is a great plant-based option. However, their quinoa burger would be my choice if something like this is available. It is made in house and comes with vegan cheese, lettuce, tomato, sautéed onions, avocado, and you can ask for a gluten-free bun. All of their burgers are cooked in avocado oil.
I tried both the Roasted Garlic Quinoa burger and a Beyond Meat burger. Beyond meat is definitely a major upgrade for other plant-based meat options on the market. It’s super tasty and if you are wanting to have a “burger” every once in a while this is a great plant-based option. However, their quinoa burger would be my choice if something like this is available. It is made in house and comes with vegan cheese, lettuce, tomato, sautéed onions, avocado, and you can ask for a gluten-free bun. All of their burgers are cooked in avocado oil.

 For acai we tried the Survivor Bowl. It’s loaded with all kinds of fruits and you can get superfood toppings added, we also had the Tres Palmas bowl which comes with granola, banana, pineapple, mango, and coconut oil. Everything was amazing!
For acai we tried the Survivor Bowl. It’s loaded with all kinds of fruits and you can get superfood toppings added, we also had the Tres Palmas bowl which comes with granola, banana, pineapple, mango, and coconut oil. Everything was amazing!

 I cannot recommend this place enough if you are looking for a healthy place to eat in Orlando! Purple Oceans is the spot since they have both sweet and savory – something for everyone. Plus the decor is so tropical and makes you feel like you’re in Puerto Rico. Give them a try next time you’re in Orlando, they have 3 locations, one brick + mortar, and the other two are permanent food trucks, how fun!
I cannot recommend this place enough if you are looking for a healthy place to eat in Orlando! Purple Oceans is the spot since they have both sweet and savory – something for everyone. Plus the decor is so tropical and makes you feel like you’re in Puerto Rico. Give them a try next time you’re in Orlando, they have 3 locations, one brick + mortar, and the other two are permanent food trucks, how fun!
[ad_2]

[ad_1]
The secretin story holds an important lesson that extends far beyond autism.
“Many families, if not a majority of families” with a child suffering from autism spectrum disorder (ASD) “pursue dietary and nutritional approaches as components of treatment. Estimates of the use of alternative therapies range from 28 to 95 percent, with special diets or dietary supplements the most frequently cited approach. Why so common? My video Alternative Treatments for Autism explores the issue.
“Perhaps acting on suspicion or distrust of standard medical practices, a desire not to have their children ‘drugged’ or the desire to seek curative treatment because of the frustration with deficiencies in traditional medical interventions, therapies based on dietary interventions appeal to parents of children with autism as more safe, natural, and holistic approaches to treating their children”—but it also could be simply because the drugs don’t work.
“Pharmacological interventions in ASD are mainly aimed to reduce commonly associated symptoms, including inattention, impulsivity, hyperactivity, compulsions, anxiety, sleep disturbances, irritability, self-injury, and aggression”—calm them down and help them sleep—but they have no effect on “the core symptoms of ASD,” like the social withdrawal and abnormal behaviors. “Only two drugs have been approved by the US Food and Drug Administration for the treatment of autism…and both target an associated behavior problem, irritability, rather than the core deficits in social skills and repetitive behavior. Both drugs also have significant side effects, including weight gain and sedation. It’s no surprise, therefore, that parents seek complementary and alternative medicine (CAM) therapies to try to help their affected children.” Okay, but do the alternatives work any better?
In the alternative medicine literature, you’ll see a lot of this kind of attitude: Evidence schmevidence! As long as the treatment isn’t harmful, why not give it a try? Or, going even further to suggest trying a treatment even if the evidence is stacked against it, because—who knows?—maybe your kids are the exception. I’m sympathetic to that thinking. “Unfortunately, there are many unscrupulous charlatans who are eager to take advantage of parents desperate to try anything that sounds like it might help their children with autism. We [researchers] receive several emails a week from practitioners offering ‘the cure’ for autism (often for the ‘low, low price’ of $299). We are often horrified at how these emails use guilt and guile to encourage families to try these untested treatments because ‘if you really loved your child, wouldn’t you want to leave no stone unturned?’”
When challenged, “many practitioners of these supposed cures will say things like ‘I know it works,’ ‘I’ve seen it work,’ or ‘I don’t want to spend time and money testing it when I could be helping children right away.’ We [researchers] urge parents to run, not walk, away from any treatment that claims to be too good for science.” Indeed, “all treatments should be subjected to the rigor of well-designed, double-blind, placebo-controlled clinical trials.” Our children deserve no less.
Parents try them anyway, often without even telling their physicians, “noting a perceived unwillingness to consider potential benefits [of alternatives] among clinicians,” which I think arises because we’ve been burned so many times before. “High-profile examples of ineffective or dangerous CAM therapies led to a general mistrust of and distaste for anything believed to be” outside the box.
Take the secretin story: “Improved social and language skills”—that is, improved core autism symptoms—”after secretin administration in patients with autistic spectrum disorders.” Secretin is a gut hormone involved in digestion and used in a diagnostic test for pancreatic function. Researchers just happened to be doing this test on some children who just happened to have autism, and, to their surprise, within weeks of administering the test, there was “dramatic improvement in their behavior, manifested by improved eye contact, alertness, and expansion of expressive language.”
Understandably, this sparked a media “frenzy,” and parents scrambled to find the stuff, which “led to a black market for the drug…What makes an interesting television program may not, of course, be the same as what makes good science.” You’ve got to put it to the test.
A randomized controlled trial on the effect of secretin on children with autism was done, and “no significant effects” were found. The study used porcine secretin, though—pig hormones. Might human secretin would work better? No, apparently not. There was a “lack of benefit” from human secretin, too. But, as you can see below and at 4:27 in my video, the data initially appeared to show that secretin totally worked. One shot of secretin, and autism behaviors dropped within days! The same thing happened when the placebo was injected, though, which is why we do placebo-controlled studies.
“The widespread circulation of [those] anecdotal reports of the benefits of secretin in the treatment of autism may have raised expectations among parents and care providers and biased them toward perceiving improvement,” explaining the effects of the placebo injection. In this way, “ineffective treatments for autism are often promoted and widely accepted” even if there’s no evidence to back them up, exemplified by the fact that “most parents [in the study] remained interested in secretin as a form of treatment for their child’s autism even after being told that we [the researchers] found no evidence of benefit.” They were told it didn’t work, but they just couldn’t give up hope. So, the autism community continued to press and clung to the thought that it just has to work.
In the end, 16 randomized placebo-controlled trials were performed involving more than 900 children, and no evidence of benefit was found. “No studies revealed significantly greater improvements in measures of language, cognition, or autistic symptoms when compared with placebo.”
“In the absence of effective and affordable treatments for autism, parents of children with this disorder are extremely vulnerable to extravagant claims of potential cures.” In the case of secretin, it was like a perfect storm of factors that propagated the myth, which “prompted a frenzy of secretin purchases by thousands of parents, often at hundreds or even thousands of dollars per dose. The ‘secretin story’ exemplifies the importance of subjecting proposed treatments to scientific scrutiny in contrast to accepting anecdotal reports as proof of efficacy.”
Sometimes alternative approaches work, and sometimes they don’t. You don’t know until you put them to the test.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
We’re told that we need to wear sunscreen as the primary way to protect ourselves from skin damage, but many sunscreens contain chemicals that are harmful to our health. There are many ways that we can enjoy the sun responsibly and that includes what we eat and how we interact with the sun. There is a wide array of foods that offer sun protection and most of them are easily available in the summertime. Nature is smart like that – in fact, there are many surprising health benefits of sunshine, too!
We’ve demonized sunshine when it’s really not the enemy. In truth, the earth and the humans, plants, and animals that live on it need sunshine for survival. The sun is our primary source of Vitamin D, which is made in our skin after sun exposure. Vitamin D is crucial for immunity, mental health, hormone production, bone health, and sleep. While we can receive Vitamin D from foods as well, the sun is one of the simplest and no-cost ways to get it.
Sunlight also helps to regulate our circadian rhythms, improve our mood and cognition, and even reduce our risk of certain cancers.
If we’re going to reap the benefits of sunshine, it’s important to be responsible about it. The right amount is beneficial to our health – but too much of it, especially without practicing safe sun exposure, can be detrimental. Some of the things you can do to enjoy the sun safely include:
Diet plays an important role in sun protection by providing us with nutrients that ward off damage and help our skin become resilient. Include these best foods for sun protection in your diet to receive a healthy dose of nutrients that can help arm your skin against the sun.

Blueberries, and all berries for that matter, are a rich source of antioxidants. Sunlight exposes us to UV radiation, but the free radical-fighting properties of antioxidant foods help to protect us from that sun damage. Blueberries are also a wonderful source of Vitamin C that helps to strengthen and boost collagen production.
Find blueberry recipe inspiration right here!

Hemp seeds, as well as chia seeds and flax seeds, are a rich source of omega 3 fatty acids, which help our skin maintain its integrity, keeping it smooth, strong and supple. Omega 3s are also highly anti-inflammatory, so these foods can help with healing if a sunburn occurs.
Add hemp seeds to smoothies, or use them as a topper for soups, stews, cereals, dairy-free yogurt, granola, or nut butter on toast. One of our faves is this hemp chocolate spread.

Carrots and red bell peppers are both high in beta-carotene, which our bodies convert into Vitamin A, a nutrient that supports vision, skin and mucosal healing. Research shows that beta-carotene shields us from sunburn; however, these sun-protective effects kick in after a minimum of 10 weeks of consuming beta-carotene, so start chowing down on these veggies stat!
Try these carrot cake energy bites for carrot-y goodness.

Gorgeous tomatoes of all shapes, sizes, and colours are abundant in the summertime for good reason – their concentration of the pigment lycopene helps to protect us from sunburns. Studies have found that research participants who ate tomato paste daily for 10 weeks were much less susceptible to sunburns than groups who hadn’t consumed tomato paste. We especially adore consuming tomatoes in salsa and tomato sauce.
Now you have another reason to enjoy the bounty of tomatoes this summer, don’t you think?

Dark leafy green vegetables are an incredible source of antioxidants, which can help offset the damage from UV rays. Studies have shown that lutein and zeaxanthin – specific antioxidants found in greens – prevent skin wrinkles and protect us from the sun. Research also shows that eating dark leafy greens can decrease our risk of skin cancer.
You can add greens to virtually any meal. We also love making kale chips!

If you’re looking for another reason to eat more chocolate, here it is: the antioxidants found in cacao powder help prevent sun damage. In one study, women who were given a high-flavanol chocolate beverage for 12 weeks were less sensitive to UV radiation than women who consume a low-flavanol beverage. This same study showed that consuming chocolate improved blood flow to the skin, as well as enhanced skin texture and structure. Score!
You can get started with these incredible dairy-free chocolate recipes.

Green tea is rich in polyphenols, particularly one called epigallocatechin-3-gallate (EGCG), which offers natural sun protection, helps to destroy free radicals, and may inhibit skin tumors. When applied topically, EGCG preparations can reduce skin redness. If it’s hot outside, simply chill your green tea to make iced tea, or use it in smoothies.
Find more ways to use green tea – and all different kinds of teas – in your cooking and baking.

These small but mighty fish are packed with selenium, an antioxidant that may help prevent damage from UVB rays. They are also rich in amino acids (protein) that help with healing and repair, as well as anti-inflammatory Omega 3s. Evidence indicates that Mediterranean-style diets, which include plenty of fish, nuts and seeds, olive oil and vegetables, help to protect against melanoma.

Sunflower seeds are high in Vitamin E, which has antioxidant properties that help to protect the skin against damage. Eat as a snack, fold into trail mix, or make sunflower seed butter with them.
A nutritious diet plays a key role in our overall health and building resilience, as well as providing support to us when we are outside in nature. These best foods for sun protection are packed with nutrients, delicious, and easy to incorporate into our everyday lives.

[ad_2]
Academy of Culinary Nutrition
Source link

[ad_1]
A bit of ugly delicious, iron rich, #plantbased eating to start the week. Sautéed smoky black beans with spinach, tomato, spices and a sprouted bread (you can enjoy with sourdough/wholewheat bread or even on top of quinoa)
NUTRITION per serve (not including bread)
Protein : 14.2g
Fibre: 17.3g
Calcium: 177mg
Iron: 5.6mg
Magnesium: 140mg
To make: heat approx 1/2 tsp garlic infused oil in fry pan, add 1 large tomato, 2-3 cups baby spinach and sauté 2 minutes, add 3/4 cup cooked black beans, 1/2 tsp Smokey paprika, pinch chilli flakes and iodised salt, and cook a further 2 minutes. Top with 2tbsp fresh chopped parsley and black pepper and serve on a sprouted / sourdough / whole-wheat bread.
The addition of tomato in this recipe (vitamin c rich) helps the absorption of plant based heme iron. You could also benefit by eating a c-rich kiwi fruit after as a nice sweet finish too!
[ad_2]
Jacqueline Alwill
Source link

[ad_1]
Travels to Bali this time were different to previous trips as we now have two very little people in tow, so we made the most of lunches and super early dinners or ordering in. If you go and this is your family, download @grabfoodid app to get food delivered and don’t order based on ratings, order based on where you know is good. The app has an overwhelming amount of options.
Our favourites in Canggu where we stayed for the full week:
@mason.bali – kid friendly and epic food
@milkandmadu.family always awesome
@yukibali_ phenomenal Japanese – our date lunch
@luigishotpizzabali – best pizza you may well eat!
@doppiocafebali – ate lots here especially easy for the girls
@alkalinebali – raw / vegan options
@cratecafe best brekky and smoothies
@balibuda – great for healthy food / airport snacks
Zin hotel – easy for kiddy dinner pick up
@theavocadofactory – yum lunch with jet
@revolver.bali for great coffee
Heaps of fresh whole fruit from warungs
Days spent at @finnsrecclub – easy yummy food there, then sunset drink one day at @finnsbeachclub where I felt 20 for about 3 seconds  fun though
fun though 
Quite tricky getting baby / toddler snacks besides fruit that isn’t laced with refined sugar – @pepito.market had best options.
Plenty of lazy mornings at our lovely accom @fellavillas where Tia cooked traditional indonesian dishes for us.
By no means an exhaustive list but hope it helps some of you along your travels.






[ad_2]
Jacqueline Alwill
Source link

[ad_1]
Does carnitine, a nutrient in red meat, endanger your cardiovascular health? This quick read tells you what you need to know.
[ad_2]

[ad_1]
A new study by researchers at Tufts University and the Cleveland Clinic and published in the American Heart Association journal Atherosclerosis, Thrombosis, and Vascular Biology claims that higher red meat intake is associated with increased risk for heart attacks and strokes (ASCVD or atherosclerotic cardiovascular disease), partly because it contains carnitine, a nutrient found only in animal source foods (ASF), particularly in red meat. More than 50 news outlets have already picked up this article. How important are these new findings? Should you worry that eating red meat could cause you to have a stroke or a heart attack?
Unfortunately, this happens to be a nutrition epidemiology study, so it is simply not capable of providing meaningful information about this question that we can use to guide our food choices.
No nutrition epidemiology study can be taken seriously because the methodology used is wholly unscientific. [To learn more, please see: The Problem with Epidemiological Studies.]
Science requires data. Data, by definition, must be objective and quantifiable. Nutrition epidemiologists do not generate dietary data because they do not measure actual food intake. Instead, they use memory-based questionnaires that force people to estimate their intake of a select list of foods over long periods of time.
These excerpts below, taken from this new study, tell you everything you need to know about how this plant-biased sausage was made:
“Usual dietary habits over the past year were assessed in 1989 to 1990 using a validated 99-item picture-sort-food frequency questionnaire (FFQ) adapted from the National Cancer Institute, and again in 1995 to 1996 using a validated Willett semiquantitative FFQ.
For each FFQ, participants were asked to indicate how often, on average, they had eaten given amounts of various foods during the past year. [my emphasis]”
Notice:
*It’s unclear which version of Professor Willett’s FFQ was used because the authors provide three different citations. Below is a description of the 131-item FFQ taken from ref. #37:
“The semiquantitative FFQ is designed to assess dietary variables that are hypothesized to affect the occurrence of heart disease and cancer. It includes 131 food items with specific serving sizes that are described using natural portions (eg, one banana, two slices of pizza) or standard weight and volume measures of servings commonly consumed in this study population. For each food item, participants indicated their average frequency of consumption over the past year in terms of the specified serving size by checking one of the nine frequency categories. The selected frequency category for each food item was converted to a daily intake. For example, a response of “two to four per week” was converted to 0.429 servings a day (three per week). [my emphasis]”
Translation: the authors “convert” ballpark guesses into concrete quantities down to the third decimal place, thereby creating the illusion of precision.
Even if the information gathered was accurate (which is not possible given the methodology), the strength of the associations (represented by the hazard ratios) between meat and heart disease risk are all well below 2.0, the threshold recommended by the Bradford-Hill criteria as one of (many) prerequisites for establishing causality (1.0 = no association). Notice also that the lower limit of the confidence intervals (noted in parentheses following each bolded value) approach 1.0:
“After multivariable-adjustment, higher intakes of unprocessed red meat, total meat, and total ASF associated with higher ASCVD risk, with hazard ratios (95% CI) per interquintile range of 1.15 (1.01–1.30), 1.22 (1.07–1.39), and 1.18 (1.03–1.34), respectively.”
Using the first “data” point as an example: the hazard ratio was 1.15 (far below 2.0) and the confidence interval ranged from 1.01 to 1.30, meaning that the actual value could fall anywhere within that range. The lower limit is 1.01…just a whisker above 1.0; these are truly trivial and therefore meaningless associations.
Furthermore, if their theory about meat and TMAO were correct (which it’s not), then fish should have been much more strongly associated with ASCVD risk, because fish naturally contains high amounts of TMAO, whereas the carnitine in meat has to first be converted to TMAO in the intestine by gut bacteria. Yet this new study found no association between fish and ASCVD:
“Processed meat intake associated with a nonsignificant trend toward higher ASCVD (1.11 [0.98–1.25]); intakes of fish, poultry, and eggs were not significantly associated. [my emphasis]”
Norwegian fishery scientists have rightfully taken issue with this illogical “fish contains lots of TMAO but don’t fear fish, fear red meat” argument in more than one scientific rebuttal, including this one:
“Microbial Trimethylamine-N-Oxide as a Disease Marker: Something Fishy?” which concludes “We suspect that the TMAO story may be a red herring.”
Fishy indeed…
Nutrition epidemiology studies will continue to pollute the stormy seas of nutrition science unless and until academic journal editors decide to categorically reject them as unscientific and unpublishable. It should be considered scientific malpractice to subject the public to these epidemi-illogical, data-free hypotheses about food and human health.
Notes:
The Cleveland Clinic first began studying the potential relationship between red meat, carnitine, TMAO, and heart disease back in 2013. If you are curious to learn more, you can read my explanation and critique of that convoluted study here: “Does Carnitine from Red Meat Cause Heart Disease?.” (I must admit I had a little fun with it).
If nutrition epidemiology interests you, my forthcoming book Change Your Diet, Change Your Mind (2023) will devote a full chapter to the topic. This is necessary because, in order to arrive at a useful definition of what a brain-healthy diet is, we must first disrobe and discard the entire field of nutrition epidemiology. Since the lion’s share of what we have been led to believe about food and human health springs from this deeply flawed methodology, the way to the truth about what foods keep us healthy must begin with a clean slate.
[ad_2]

[ad_1]
A new study by researchers at Tufts University and the Cleveland Clinic and published in the American Heart Association journal Atherosclerosis, Thrombosis, and Vascular Biology claims that higher red meat intake is associated with increased risk for heart attacks and strokes (ASCVD or atherosclerotic cardiovascular disease), partly because it contains carnitine, a nutrient found only in animal source foods (ASF), particularly in red meat. More than 50 news outlets have already picked up this article. How important are these new findings? Should you worry that eating red meat could cause you to have a stroke or a heart attack?
Unfortunately, this happens to be a nutrition epidemiology study, so it is simply not capable of providing meaningful information about this question that we can use to guide our food choices.
No nutrition epidemiology study can be taken seriously because the methodology used is wholly unscientific. [To learn more, please see: The Problem with Epidemiological Studies.]
Science requires data. Data, by definition, must be objective and quantifiable. Nutrition epidemiologists do not generate dietary data because they do not measure actual food intake. Instead, they use memory-based questionnaires that force people to estimate their intake of a select list of foods over long periods of time.
These excerpts below, taken from this new study, tell you everything you need to know about how this plant-biased sausage was made:
“Usual dietary habits over the past year were assessed in 1989 to 1990 using a validated 99-item picture-sort-food frequency questionnaire (FFQ) adapted from the National Cancer Institute, and again in 1995 to 1996 using a validated Willett semiquantitative FFQ.
For each FFQ, participants were asked to indicate how often, on average, they had eaten given amounts of various foods during the past year. [my emphasis]”
Notice:
*It’s unclear which version of Professor Willett’s FFQ was used because the authors provide three different citations. Below is a description of the 131-item FFQ taken from ref. #37:
“The semiquantitative FFQ is designed to assess dietary variables that are hypothesized to affect the occurrence of heart disease and cancer. It includes 131 food items with specific serving sizes that are described using natural portions (eg, one banana, two slices of pizza) or standard weight and volume measures of servings commonly consumed in this study population. For each food item, participants indicated their average frequency of consumption over the past year in terms of the specified serving size by checking one of the nine frequency categories. The selected frequency category for each food item was converted to a daily intake. For example, a response of “two to four per week” was converted to 0.429 servings a day (three per week). [my emphasis]”
Translation: the authors “convert” ballpark guesses into concrete quantities down to the third decimal place, thereby creating the illusion of precision.
Even if the information gathered was accurate (which is not possible given the methodology), the strength of the associations (represented by the hazard ratios) between meat and heart disease risk are all well below 2.0, the threshold recommended by the Bradford-Hill criteria as one of (many) prerequisites for establishing causality (1.0 = no association). Notice also that the lower limit of the confidence intervals (noted in parentheses following each bolded value) approach 1.0:
“After multivariable-adjustment, higher intakes of unprocessed red meat, total meat, and total ASF associated with higher ASCVD risk, with hazard ratios (95% CI) per interquintile range of 1.15 (1.01–1.30), 1.22 (1.07–1.39), and 1.18 (1.03–1.34), respectively.”
Using the first “data” point as an example: the hazard ratio was 1.15 (far below 2.0) and the confidence interval ranged from 1.01 to 1.30, meaning that the actual value could fall anywhere within that range. The lower limit is 1.01…just a whisker above 1.0; these are truly trivial and therefore meaningless associations.
Furthermore, if their theory about meat and TMAO were correct (which it’s not), then fish should have been much more strongly associated with ASCVD risk, because fish naturally contains high amounts of TMAO, whereas the carnitine in meat has to first be converted to TMAO in the intestine by gut bacteria. Yet this new study found no association between fish and ASCVD:
“Processed meat intake associated with a nonsignificant trend toward higher ASCVD (1.11 [0.98–1.25]); intakes of fish, poultry, and eggs were not significantly associated. [my emphasis]”
Norwegian fishery scientists have rightfully taken issue with this illogical “fish contains lots of TMAO but don’t fear fish, fear red meat” argument in more than one scientific rebuttal, including this one:
“Microbial Trimethylamine-N-Oxide as a Disease Marker: Something Fishy?” which concludes “We suspect that the TMAO story may be a red herring.”
Fishy indeed…
Nutrition epidemiology studies will continue to pollute the stormy seas of nutrition science unless and until academic journal editors decide to categorically reject them as unscientific and unpublishable. It should be considered scientific malpractice to subject the public to these epidemi-illogical, data-free hypotheses about food and human health.
Notes:
The Cleveland Clinic first began studying the potential relationship between red meat, carnitine, TMAO, and heart disease back in 2013. If you are curious to learn more, you can read my explanation and critique of that convoluted study here: “Does Carnitine from Red Meat Cause Heart Disease?.” (I must admit I had a little fun with it).
If nutrition epidemiology interests you, my forthcoming book Change Your Diet, Change Your Mind (2023) will devote a full chapter to the topic. This is necessary because, in order to arrive at a useful definition of what a brain-healthy diet is, we must first disrobe and discard the entire field of nutrition epidemiology. Since the lion’s share of what we have been led to believe about food and human health springs from this deeply flawed methodology, the way to the truth about what foods keep us healthy must begin with a clean slate.
[ad_2]

[ad_1]
A new study by researchers at Tufts University and the Cleveland Clinic and published in the American Heart Association journal Atherosclerosis, Thrombosis, and Vascular Biology claims that higher red meat intake is associated with increased risk for heart attacks and strokes (ASCVD or atherosclerotic cardiovascular disease), partly because it contains carnitine, a nutrient found only in animal source foods (ASF), particularly in red meat. More than 50 news outlets have already picked up this article. How important are these new findings? Should you worry that eating red meat could cause you to have a stroke or a heart attack?
Unfortunately, this happens to be a nutrition epidemiology study, so it is simply not capable of providing meaningful information about this question that we can use to guide our food choices.
No nutrition epidemiology study can be taken seriously because the methodology used is wholly unscientific. [To learn more, please see: The Problem with Epidemiological Studies.]
Science requires data. Data, by definition, must be objective and quantifiable. Nutrition epidemiologists do not generate dietary data because they do not measure actual food intake. Instead, they use memory-based questionnaires that force people to estimate their intake of a select list of foods over long periods of time.
These excerpts below, taken from this new study, tell you everything you need to know about how this plant-biased sausage was made:
“Usual dietary habits over the past year were assessed in 1989 to 1990 using a validated 99-item picture-sort-food frequency questionnaire (FFQ) adapted from the National Cancer Institute, and again in 1995 to 1996 using a validated Willett semiquantitative FFQ.
For each FFQ, participants were asked to indicate how often, on average, they had eaten given amounts of various foods during the past year. [my emphasis]”
Notice:
*It’s unclear which version of Professor Willett’s FFQ was used because the authors provide three different citations. Below is a description of the 131-item FFQ taken from ref. #37:
“The semiquantitative FFQ is designed to assess dietary variables that are hypothesized to affect the occurrence of heart disease and cancer. It includes 131 food items with specific serving sizes that are described using natural portions (eg, one banana, two slices of pizza) or standard weight and volume measures of servings commonly consumed in this study population. For each food item, participants indicated their average frequency of consumption over the past year in terms of the specified serving size by checking one of the nine frequency categories. The selected frequency category for each food item was converted to a daily intake. For example, a response of “two to four per week” was converted to 0.429 servings a day (three per week). [my emphasis]”
Translation: the authors “convert” ballpark guesses into concrete quantities down to the third decimal place, thereby creating the illusion of precision.
Even if the information gathered was accurate (which is not possible given the methodology), the strength of the associations (represented by the hazard ratios) between meat and heart disease risk are all well below 2.0, the threshold recommended by the Bradford-Hill criteria as one of (many) prerequisites for establishing causality (1.0 = no association). Notice also that the lower limit of the confidence intervals (noted in parentheses following each bolded value) approach 1.0:
“After multivariable-adjustment, higher intakes of unprocessed red meat, total meat, and total ASF associated with higher ASCVD risk, with hazard ratios (95% CI) per interquintile range of 1.15 (1.01–1.30), 1.22 (1.07–1.39), and 1.18 (1.03–1.34), respectively.”
Using the first “data” point as an example: the hazard ratio was 1.15 (far below 2.0) and the confidence interval ranged from 1.01 to 1.30, meaning that the actual value could fall anywhere within that range. The lower limit is 1.01…just a whisker above 1.0; these are truly trivial and therefore meaningless associations.
Furthermore, if their theory about meat and TMAO were correct (which it’s not), then fish should have been much more strongly associated with ASCVD risk, because fish naturally contains high amounts of TMAO, whereas the carnitine in meat has to first be converted to TMAO in the intestine by gut bacteria. Yet this new study found no association between fish and ASCVD:
“Processed meat intake associated with a nonsignificant trend toward higher ASCVD (1.11 [0.98–1.25]); intakes of fish, poultry, and eggs were not significantly associated. [my emphasis]”
Norwegian fishery scientists have rightfully taken issue with this illogical “fish contains lots of TMAO but don’t fear fish, fear red meat” argument in more than one scientific rebuttal, including this one:
“Microbial Trimethylamine-N-Oxide as a Disease Marker: Something Fishy?” which concludes “We suspect that the TMAO story may be a red herring.”
Fishy indeed…
Nutrition epidemiology studies will continue to pollute the stormy seas of nutrition science unless and until academic journal editors decide to categorically reject them as unscientific and unpublishable. It should be considered scientific malpractice to subject the public to these epidemi-illogical, data-free hypotheses about food and human health.
Notes:
The Cleveland Clinic first began studying the potential relationship between red meat, carnitine, TMAO, and heart disease back in 2013. If you are curious to learn more, you can read my explanation and critique of that convoluted study here: “Does Carnitine from Red Meat Cause Heart Disease?.” (I must admit I had a little fun with it).
If nutrition epidemiology interests you, my forthcoming book Change Your Diet, Change Your Mind (2023) will devote a full chapter to the topic. This is necessary because, in order to arrive at a useful definition of what a brain-healthy diet is, we must first disrobe and discard the entire field of nutrition epidemiology. Since the lion’s share of what we have been led to believe about food and human health springs from this deeply flawed methodology, the way to the truth about what foods keep us healthy must begin with a clean slate.
[ad_2]

[ad_1]
There have been at least eight randomized, double-blind, placebo-controlled trials of ginger for pain.
You may recall that I’ve previously explored the use of spinach for athletic performance and recovery, attributed to its “anti-inflammatory effects.” Most athletes aren’t using spinach to beat back inflammation, though; they use drugs, typically non steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, which is used by up to 95 percent of collegiate athletes and three quarters of kids playing high school football. They aren’t only using it for inflammation, though, but also prophylactically “prior to athletic participation to prevent pain and inflammation before it occurs. However, scientific evidence for this approach is currently lacking, and athletes should be aware of the potential risks in using NSAIDs as a prophylactic agent,” which include gastrointestinal pain and bleeding, kidney damage, and liver damage.
There was one study in particular that freaked everyone out: A study of thousands of marathon runners found that those taking over-the-counter pain killers before the race had five times the incidence of organ damage. Nine were hospitalized—three with kidney failure after taking ibuprofen, four with gastrointestinal bleeding after taking aspirin, and two with heart attacks, also after aspirin ingestion. In contrast, none of the control group ended up in the hospital. No pain killers, no hospital. What’s more, the analgesics didn’t even work. “Analysis of the pain reported by respondents before and after racing showed no major identifiable advantages” to taking the drugs, so it appeared there were just downsides.
What about using ginger instead? That’s the subject of my video Ground Ginger to Reduce Muscle Pain. In that marathon study, as you can see below and at 1:33 in my video, the most common adverse effect of taking the drugs was gastrointestinal cramping. Ginger, in contrast to aspirin or ibuprofen-type drugs, may actually improve gastrointestinal function. For example, endurance athletes can suffer from nausea, and ginger is prized for its anti-nausea properties.
Okay, but does it work for muscle pain?
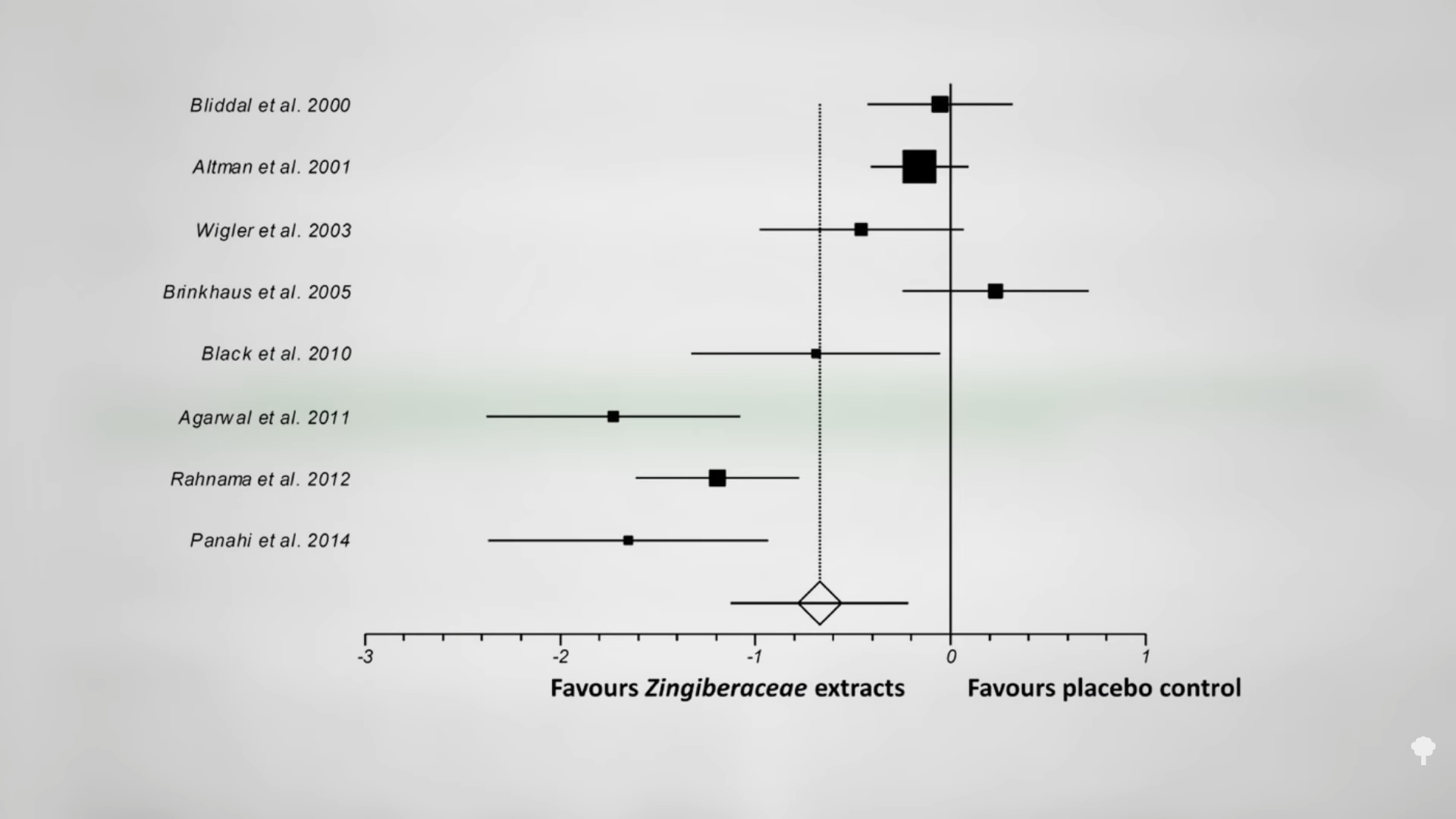
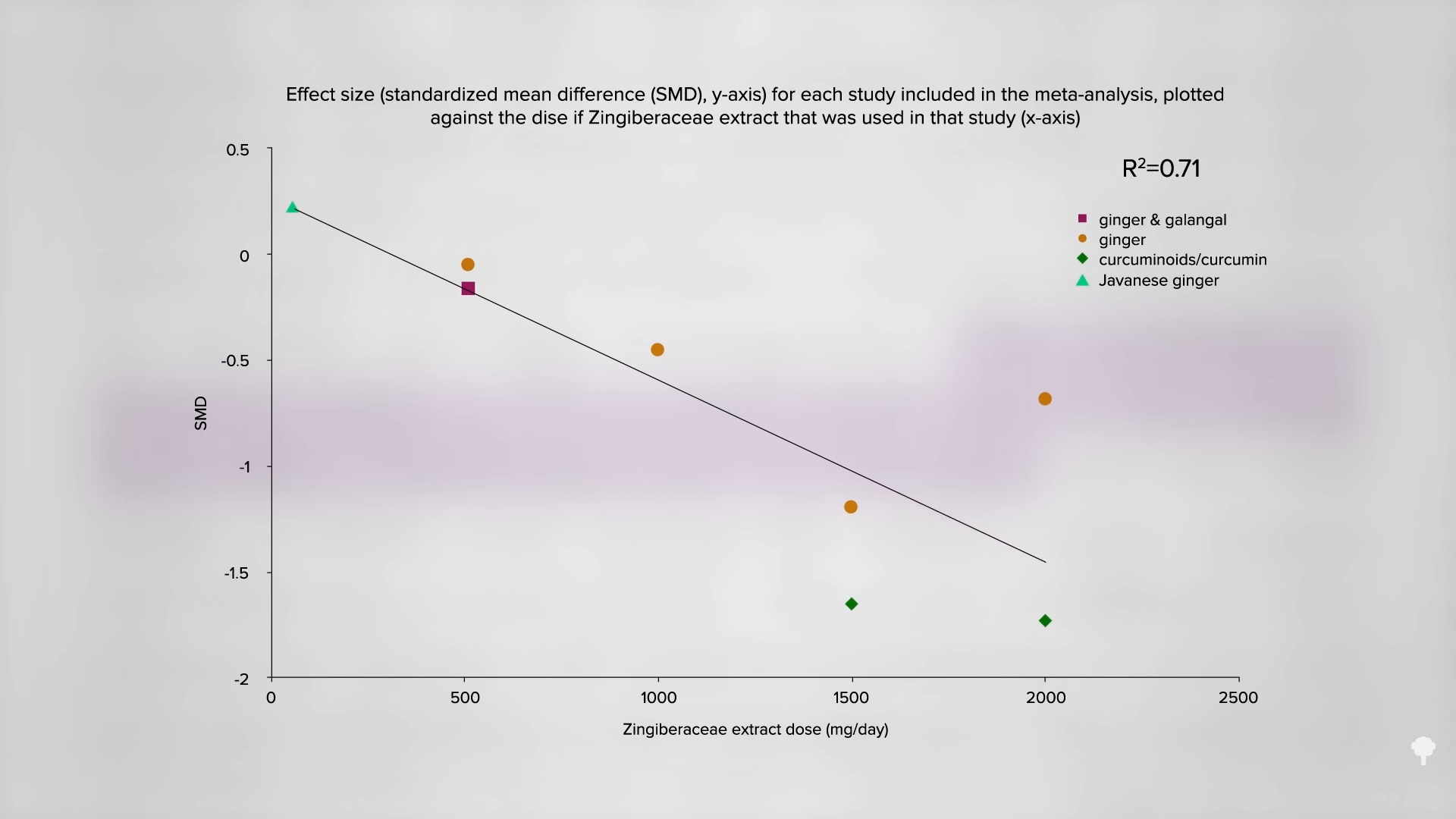
There have been at least eight randomized, double-blind, placebo-controlled trials of ginger for pain—for everything from osteoarthritis to irritable bowel to painful periods. I’ve made videos about all of those, as well as its use for migraine headaches. Overall, ginger extracts, like the powdered ginger spice you’d get at any grocery store, were found to be “clinically effective” pain-reducing agents with “a better safety profile than non-steroidal anti-inflammatory drugs.” As you can see below and at 2:22 in my video, the ginger worked better in some of the studies than in others, which is “likely to be at least partly due to the strong dose-effect relationship that [was] identified and the wide range of doses used among the studies under analysis (60-2000 mg of extract/day).”
In terms of reduction of pain, as you can see below and at 2:32 in my video, the best results were achieved with one and a half or two grams a day, which is a full teaspoon of ground ginger.
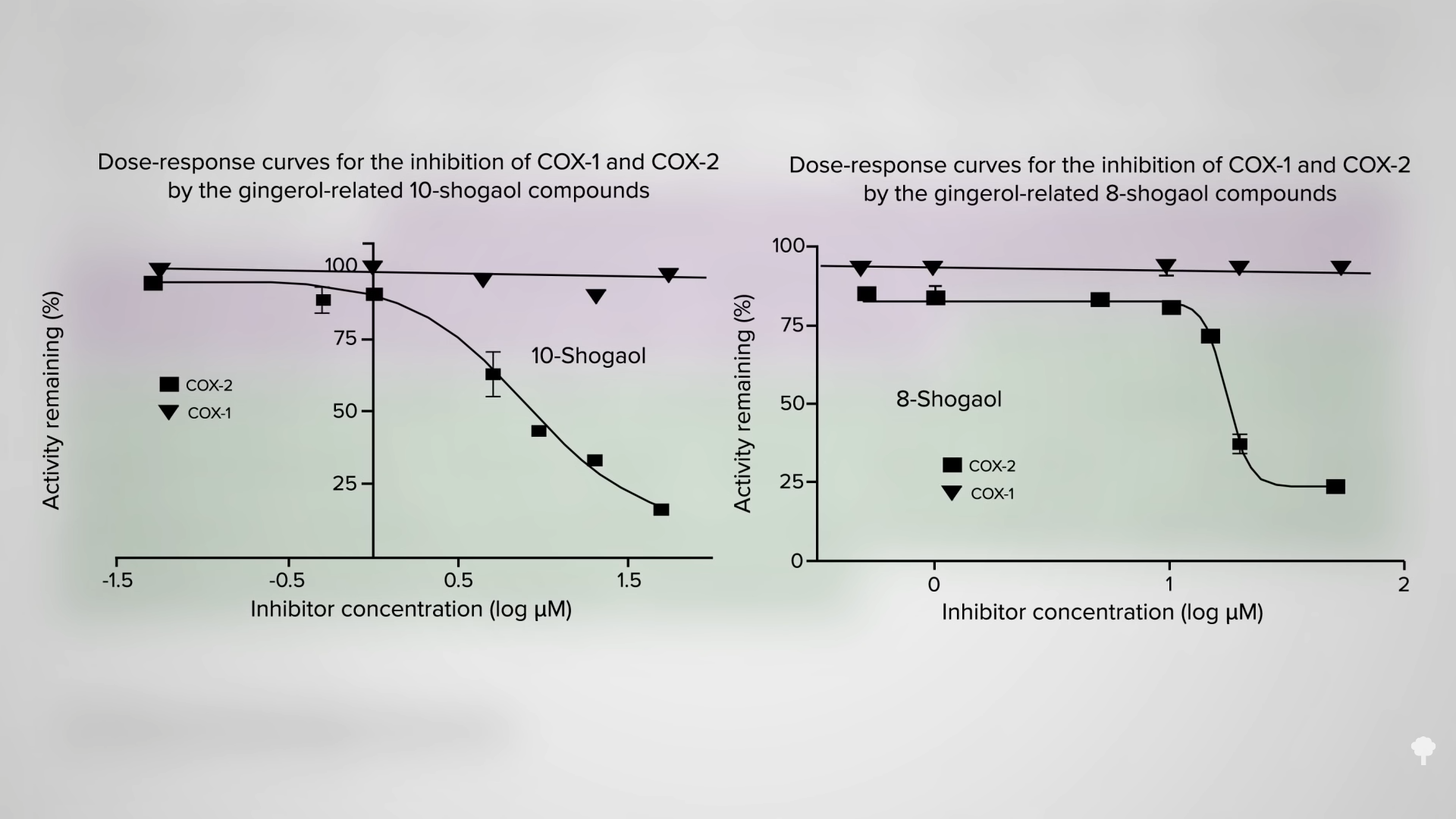
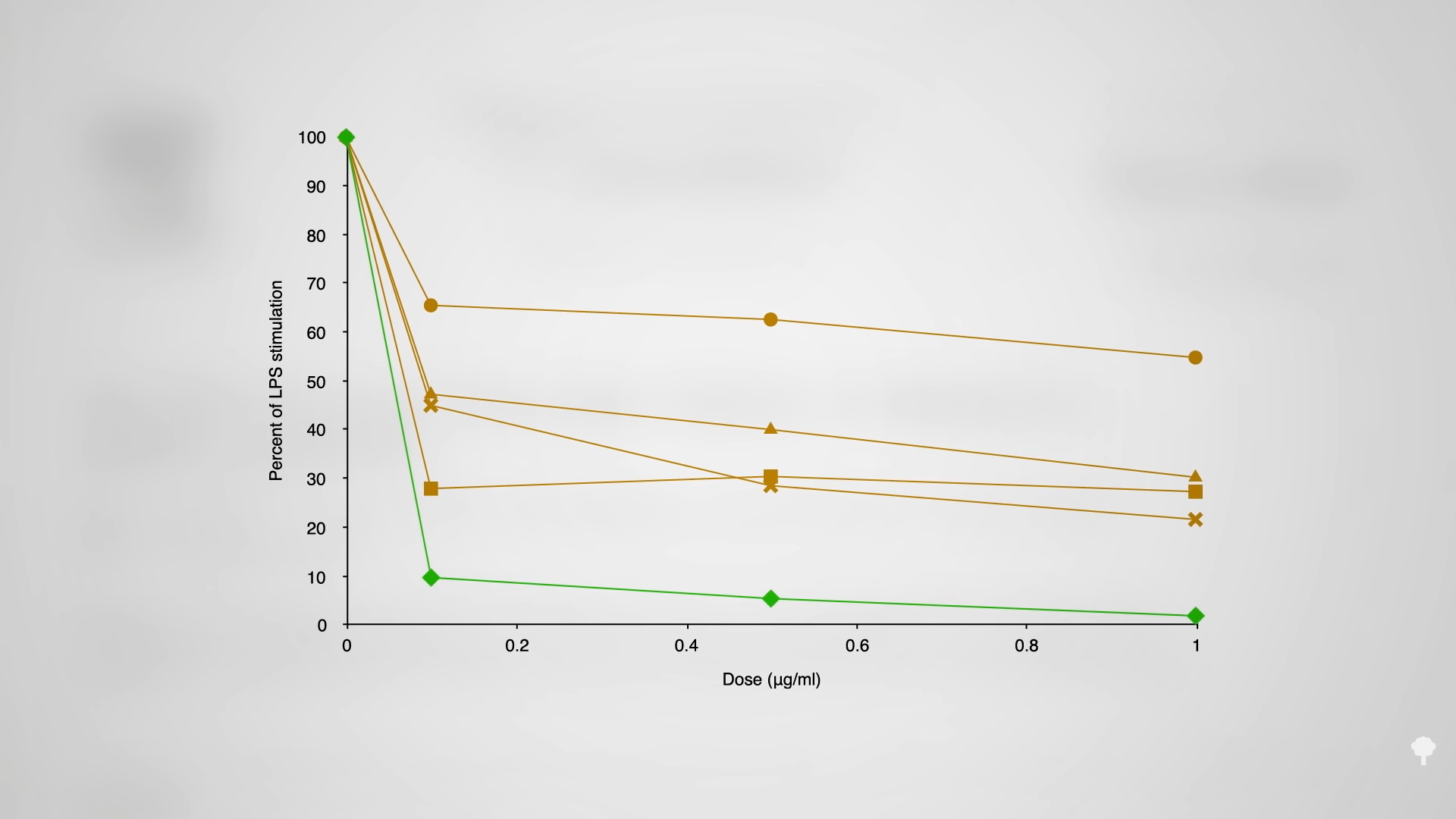
The drugs work by suppressing an enzyme in the body called cyclooxygenase-2 (COX-2), which triggers inflammation. The problem is that they also suppress cyclooxygenase-1 (COX-1), which does good things like protect the lining of your stomach and intestines. “Since inhibition of COX-1 is associated with gastrointestinal irritation, selective inhibition of COX-2”—the inflammatory enzyme—“should help minimize this side effect” and offer the best of both worlds. And, that’s what ginger seems to do. As you can see below and at 3:11 in my video, two ginger compounds had no effect against COX-1, the “good” enzyme, but could dramatically cut down on COX-2, the pro-inflammatory one.
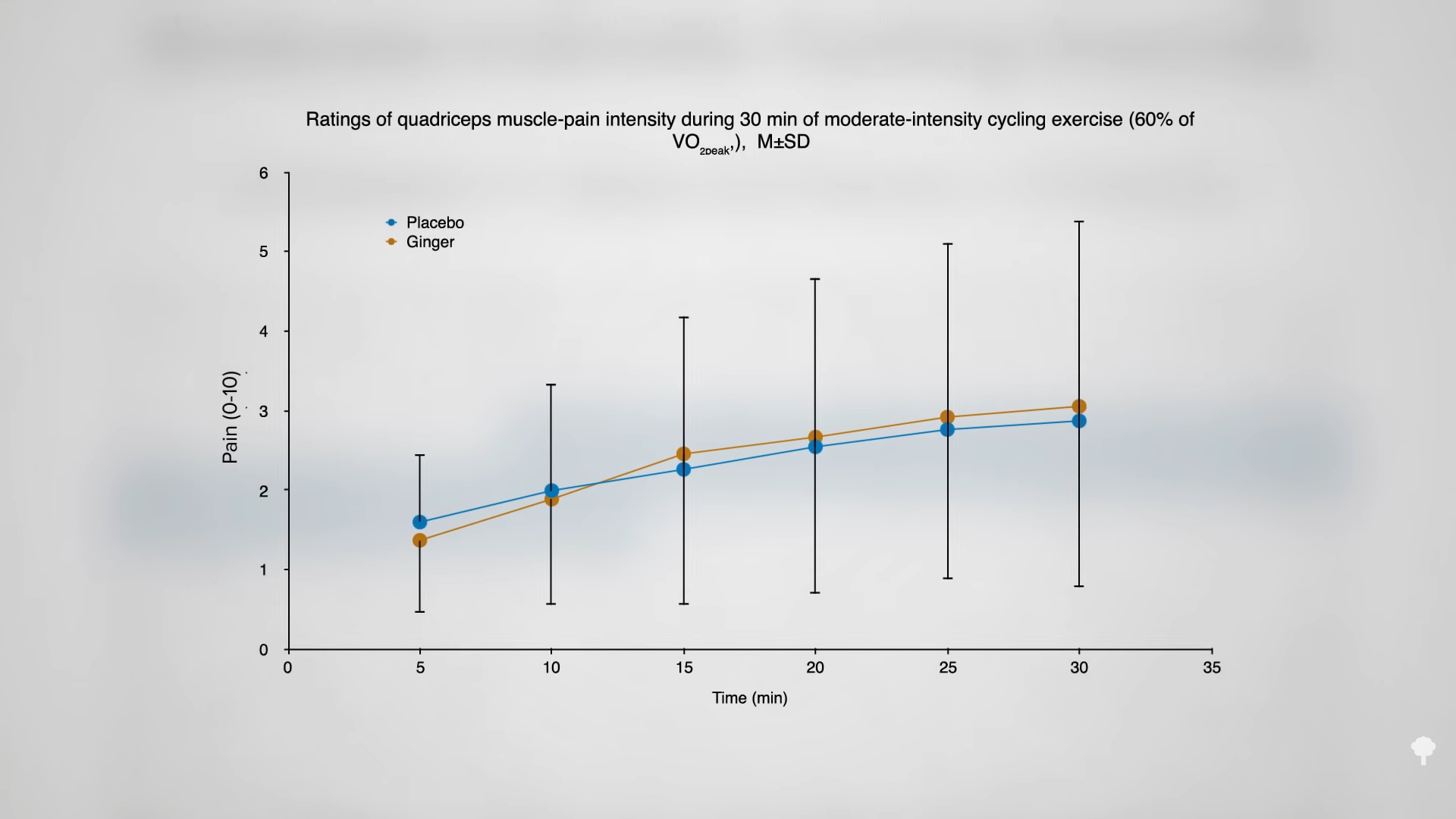
Okay, but does ginger work for muscle pain? Not acutely, apparently. You can’t just take it like a drug. When folks were given a teaspoon of ginger before a bout of cycling, there was no difference in leg muscle pain over the 30 minutes, as you can see below and at 3:34 in my video. “However, ginger may attenuate the day-to-day progression of muscle pain.” Taking ginger five days in a row appears to “accelerate the recovery of maximal strength following a high-load…[weight-lifting] exercise protocol.” When you put all the studies together, it seems “a single dose of ginger has little-to-no discernable effects on muscle pain,” but if you take a teaspoon or two for a couple days or weeks, perhaps in a pumpkin smoothie or something, you may be able to reduce muscle pain and soreness, and “accelerate recovery of muscular strength…”
Is fresh ginger preferable to powdered? Maybe not. As you can see below and at 4:12 in my video, there are all sorts of compounds in ginger with creative names as gingerols, gingerdiols, and gingerdiones, but the most potent anti-inflammatory component may be compound called shogaols.
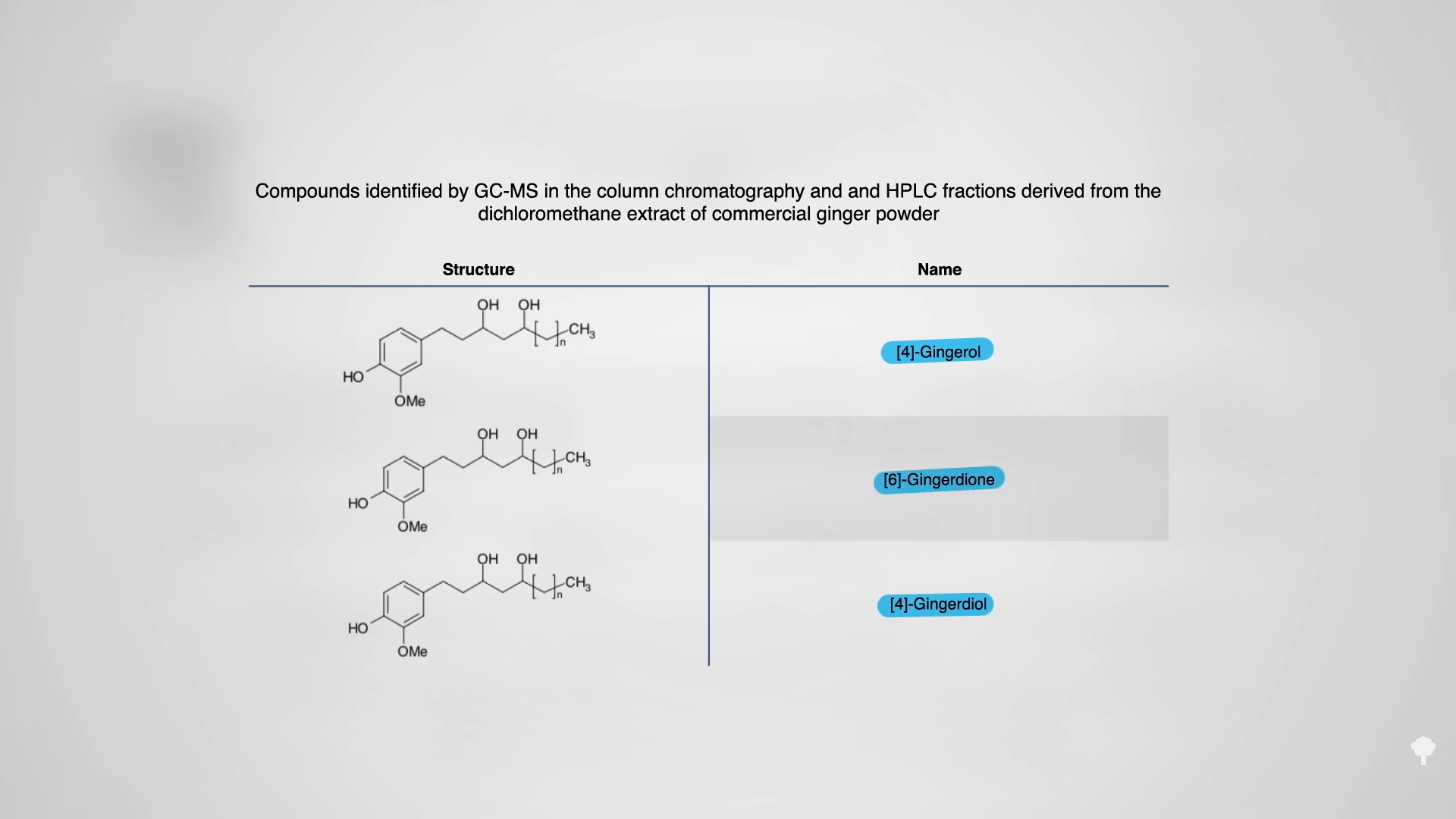
Interestingly, dried ginger contains more than fresh, which “justifies the uses of dry ginger in traditional systems of medicine for the treatment of various illnesses due to oxidative stress and inflammation.” In that case, why not just give the extracted shogaol component in a pill by itself? As you can see below and at 4:41 in my video, each of the active ginger components individually reduce inflammation, some more than others, but the whole ginger is greater than the sum of its parts.
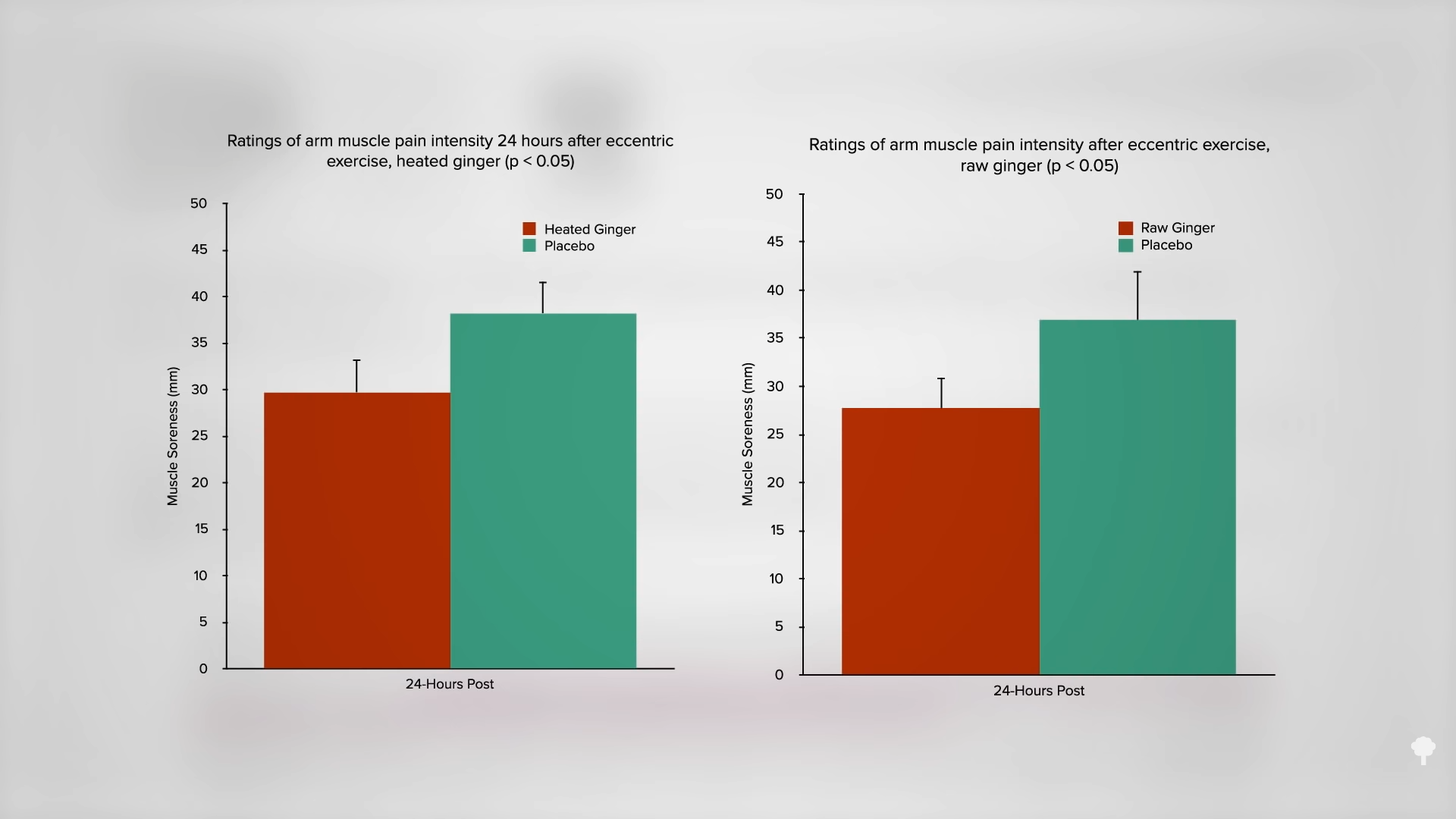
However, you can boost shogaol content of whole ginger by drying it, as they are the major gingerol dehydration products. Indeed, they’re created when ginger is dried. Heating ginger may increase shogaol concentration even more, so could heated ginger work better against pain than raw? You don’t know, until you put it to the test. A study examined the effects on muscle pain of 11 days of a teaspoon of raw ginger versus ginger that had been boiled for three hours. As you can see below and at 5:22 in my video, there was a significant reduction in muscle soreness a day after pumping iron in the cooked ginger group—and the same benefit was achieved with the raw ginger. Either way, “daily consumption of raw and heat-treated ginger resulted in moderate-to-large reductions in muscle pain following exercise-induced muscle injury.”
Here’s the link to the video I mentioned: Flashback Friday: Foods to Improve Athletic Performance and Recovery.
[ad_2]
Michael Greger M.D. FACLM
Source link

[ad_1]
When nutritional research is dominated by epidemiology, controlled trials are welcome and always worth reviewing. This week’s note is the latest dietary trial involving Professor Christopher Gardner, who has been prolific in this field. Gardner was the senior author for the DIETFITS study, which we reviewed three times previously (Ref 1). Gardner was the lead author of this week’s paper, which was called “Effect of a ketogenic diet versus Mediterranean diet on glycated hemoglobin [HbA1c] in individuals with prediabetes and type 2 diabetes mellitus: The interventional Keto-Med randomized crossover trial” (Ref 2).
As befits a good title, we know from the heading that this study sought to establish whether the keto diet or the Mediterranean diet performed better in people with borderline or diagnosed type 2 diabetes (T2D). The key outcome of interest was HbA1c, which is a measure of the sugar in the blood over the past three months. Finally, we know that it was a crossover trial, which means that all participants tried both diets. As a result, we don’t need to take into account how different people were in each part of the trial; everyone took part in both interventions. We will see that the title didn’t allow for nuance and that the Mediterranean diet was an adapted Mediterranean diet and there was another (medications) twist.
[ad_2]
Zoe
Source link

[ad_1]
This one is easy. Swap your boring oats for something a little more exotic. Dress them up instead with adding 2x tbsp of healthy including a combination of sunflower seeds/pepitas/shredded coconut/hemp seeds/linseed and almond meal. Make sure you use milk instead of water to up the protein content of the meal. Finish with a shake of cinnamon and a splash of kefir.
Our Lane Cove Dietitian Tatiana has got your sorted here. She has put up a tasty but nutritious recipe here packed full of veggies and some crumbled feta. You will be feeling full and content heading off to seize your day!
Add a twist to your regular scrambled eggs. Ditch the butter and add some silken tofu to add some extra protein and fibre. Option to serve with some grainy sourdough bread, smashed avocado and roasted cherry tomatoes.
Many bakeries offer this type of bread or most supermarkets sell Bill’s bread which is a great option! Toast and then top with ricotta and freshly sliced banana.
An excellent option! Its also very easy to keep your berries frozen and then defrost ready to add as a topping
We hope you enjoy our suggestions 🙂
Ashleigh
[ad_2]
Ashleigh Brunner
Source link

[ad_1]
2 red onions
2 large sweet potato
1 large bunch of kale
500g button mushrooms
3 cloves of garlic
1 tablespoon dried oregano or thyme
4 tablespoons of extra virgin olive oil
12 eggs
285g jar marinated roasted capsicum
100g block feta cheese
Preheat oven to 220 degrees Celsius
Peel and then dice the sweet potato into cubes and slice the red onion
Place sweet potato and onion into a baking tray with 2 tablespoons of olive oil, crack of salt and pepper
Bake for 20 minutes or until potatoes have cooked through
Meanwhile, slice the mushrooms and chop the kale into pieces
Heat a large frypan with 1 tablespoon of olive oil and sauté 2 cloves of garlic
Add mushrooms and dried oregano and cook until soft and brown. Remove from pan
Add 1 tablespoon olive oil into the pan with the last garlic clove (crushed) and sauté
Add kale leaves and stems and sauté until leaves wilt
In a large bowl crack and whisk the eggs and season with pepper
Add all the cooked vegetables as well as the marinated capsicum strips into the egg mixture
Mix together quickly and pour into a oven dish lined with baking paper
Crumble over block of feta and cook for 20 minutes or until eggs are cooked all the way through
ENJOY 🙂
[ad_2]
Ashleigh Brunner
Source link
