

Abnormal blood clotting was one of the first mysterious health effects to emerge in the COVID pandemic, first, as an effect of the natural infection, and later, as a side effect of the COVID jabs.
By mid-March 2021, barely four months after the rollout of the COVID injections, 19 European countries plus Thailand1 had suspended the use of AstraZeneca’s injection, either in full or in part, following reports of deadly blood clots.2,3
Contrary to the Moderna and Pfizer shots, the AstraZeneca jab uses a viral vector — a genetically modified and supposedly noninfectious chimpanzee cold virus — to deliver double-stranded DNA for the SARS-CoV-2 spike protein into your cells.4
Earlier that month, The Defender had reported5 U.K. data showing the AstraZeneca jab was responsible for 77% more adverse events and 25% more deaths than the Pfizer shot. Around that same time, doctors at Oslo University Hospital also announced that the blood clotting disorders experienced by some recipients of the AstraZeneca shot were in fact caused by the injection.6 A March 18, 2021, article in Science Norway read, in part:7
“‘Our theory that this is a powerful immune response most likely triggered by the vaccine, has been confirmed,’ says professor and chief physician Pål Andre Holme … ‘In collaboration with experts in the field from the University Hospital of North Norway HF, we have found specific antibodies against blood platelets that can cause these reactions … the chief physician explains …
When asked to clarify why he says ‘most likely’ in the quote, Holme confidently responds that the reason for these rare cases of blood clots has been found.
‘We have the reason. Nothing but the vaccine can explain why these individuals had this immune response,’ he states. [Norwegian national newspaper] VG also asks how Holme can know that the immune response is not caused by something other than the vaccine.
‘There is nothing in the patient history of these individuals that can give such a powerful immune response. I am confident that the antibodies that we have found are the cause, and I see no other explanation than it being the vaccine which triggers it,’ he responds.”
Study Details Mechanism of Action
In early December 2021, a team of international scientists published a paper8 detailing the mechanism behind the AstraZeneca jab’s propensity to trigger blood clots. As reported by the Daily Mail at the time:9
“A team of international experts, involving researchers from AstraZeneca, say that in a very small number of cases — about one in 100,000 in the UK — the vaccine can set off a chain reaction which leads to the body confusing its own blood platelets for fragments of virus …
They found that the shell of the vector vaccine — the weakened cold virus used to teach cells how to neutralize COVID — sometimes acts like a magnet and attracts platelets, a protein found in the blood.
For reasons the scientists are still probing, the body then mistakes these platelets as a threat and produces antibodies to fight them. The combination of the platelets and the antibodies clumping together leads to the formation of dangerous blood clots …
Essentially, after being delivered into the body adenovirus binds with a specific protein in the blood, known as platelet factor 4 (PF4), which is normally used by the body to promote coagulation in case of injury.
Using incredibly detailed images of the adenovirus in the vaccine the scientists demonstrated the adenovirus in the Oxford-AstraZeneca is negatively charged, and could attract positively charged proteins like a magnet.
The researchers believe that in a case of ‘mistaken identity’ the body’s immune system considers this platelet cluster as threat and releases antibodies to attack it, clumping together to it and triggering potentially life threatening blood clots. This condition is called vaccine-induced immune thrombotic thrombocytopenia (VITT).”
The following graphic was published in the Daily Mail to illustrate the potentially deadly chain reaction.
How Long Does Risk Remain?
As for how long the risk of blood clotting remains is unknown. In mid-September 2022, the American Heart Association reported that the risk of abnormal blood clotting remains elevated nearly a year after natural infection:10
“People who got COVID-19 had a higher risk of dangerous blood clots for close to a year later, according to a large new study11 on the aftereffects of a SARS-CoV-2 infection …
COVID-19 was linked to a sharply increased risk of blood clot-related issues — including heart attack and stroke — immediately after diagnosis compared to people who never had COVID-19 [and] … that risk remained higher for some problems up to 49 weeks later …
Researchers found that the first week after a COVID-19 diagnosis, the risk of an arterial blood clot — the kind that could cause a heart attack or ischemic stroke by blocking blood flow to the heart or brain — was nearly 22 times higher than in someone without COVID-19. That risk dropped sharply, to less than four times higher, in the second week.
‘Between 27 and 49 weeks, there is an approximately 30% increased risk for arterial clots,’ [senior author, professor of medical statistics and epidemiology at the University of Bristol, Jonathan] Sterne said. ‘But the elevation is greater for longer’ for clots in veins, which include deep vein thrombosis and pulmonary embolism, when a clot travels to the lungs.
In the first week after a COVID-19 diagnosis, the risk of such venous problems was 33 times higher. By the third and fourth weeks after diagnosis, the risk was still about eight times higher. And between 27 and 49 weeks later, the risk was still 1.8 times higher than in somebody who had never had COVID-19.”
If the risk of blood clotting remains high for nearly a year after natural infection, it seems reasonable to suspect the risk is dramatically elevated far longer in those who got one or more COVID shots, as their bodies are now producing the toxic spike protein internally, and there’s no known off-switch.
We still do not know how long the human body continues to produce spike protein after a COVID jab. And, while AstraZeneca was singled out as the main culprit of blood clots, Pfizer’s and Moderna’s mRNA jabs are no safer in this regard.
Pfizer’s COVID Jab Linked to Blood Clotting Disorder
As early as June 2021, Israeli research suggested there was a link between the Pfizer shot and thrombotic thrombocytopenic purpura (TTP), which is very similar to vaccine-induced immune thrombotic thrombocytopenia or VITT. A list of distinguishing features between the syndromes can be found on UpToDate.com.12 As reported by The Defender:13
“Scientists with the Institute of Hematology at Shamir Medical Center said they began researching the possible link after reports of a sudden increase in TTP across Israel — four cases detected in one month compared to two or three cases per year. TTP is an autoimmune disorder that causes blood clots to form in small blood vessels throughout the body …
The medical team said they found a ‘chronological connection’ between vaccination and the onset of TTP symptoms. They stressed this occurred in both new patients and in patients with pre-existing TTP whose disease had been in remission but flared up soon after getting the vaccine …
As The Defender reported in April, U.S. regulatory officials were alerted as far back as December 2020 that the Pfizer and Moderna vaccines — like AstraZeneca and J&J COVID vaccine — could pose similar risks of blood clots.”
Even before the rollout of the shots, experts warned that blood clots and cardiovascular problems were predictable. Among them were Dr. Patrick Whelan, a pediatric specialist, who in a letter14 to the U.S. Food and Drug Administration warned that the shots could “cause microvascular injury and blood clots throughout the body including the brain, heart, liver and kidneys, in ways that were not assessed in the safety trials.”
He pointed out that studies looking at the natural infection had found that “viral proteins appear to cause tissue damage without actively replicating virus,” and if that was true, he suspected the spike protein produced in response to the jabs might also cause the same kind of damage. Today, ample evidence points to Whelan’s suspicions being correct.
Jabs May Raise Risk of COVID Death Over Time
Studies are now also coming out with evidence that the shots may be causing antibody dependent enhancement (ADE), and that they kill heart and brain cells. Starting with the ADE evidence, a Swedish study,15 using data from the entire Swedish population over the age of 12, a total of 9,153,456 people, found that two doses were 43% protective against Omicron infection at week 4. By week 14, protection had dropped to zero.
Effectiveness against COVID-related hospitalization remained around 80% until week 25, but dropped to 40% by week 40. While these data are highlighted in the abstract, a more intriguing finding remains buried in the text that few take the time to read. As reported by investigative journalist Alex Berenson:16
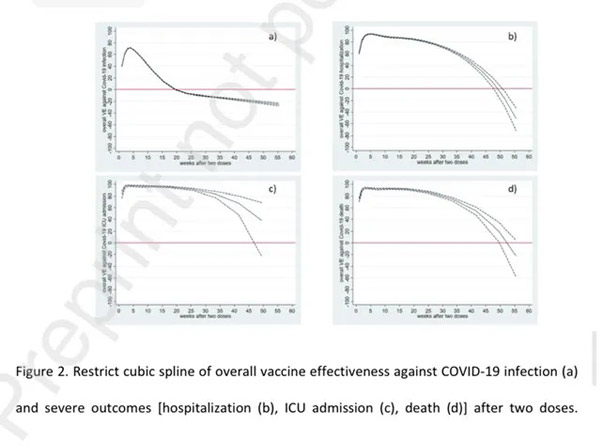
“Based on one statistical analysis [cubic spline method] vaccinated people had a HIGHER risk of death or hospitalization from COVID roughly a year after receiving their second dose. The charts — b and d below — show that vaccine protection against death and hospitalization begins to decline slowly after about five months and then plunges about nine months …
This data provides real-world evidence of possible vaccine-caused ‘antibody dependent enhancement.’ In ADE, vaccines cause our immune systems to produce antibodies that help a virus or other pathogen to attack us …
(The top chart shows the relative risk of infection, hospitalization, intensive care, and death by week after two vaccine doses. The red line marks zero effectiveness; when the blue line falls below it, it is suggesting vaccinated people are at higher risk of infection.)”
When they used another statistical method called standard polynomial regression, the shots remained moderately effective against hospitalization and death over time, falling to 45% protection against death around nine months, after which the effectiveness mysteriously started trending upward again.
According to Berenson, the lead author of the paper did not endorse either method as superior to the other. When asked for comment, Dr. Yiyi Xu told Berenson they “need more data to know which finding might be correct,” and that, at present, “the estimation is quite uncertain for both analyses.”
COVID Shots Kill Brain and Heart Cells
Another recent paper17 links the COVID shots to lethal myocarditis (heart inflammation) and encephalitis (brain inflammation). As reported by Steve Kirsch:18
“The paper is entitled: ‘A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19.’ It was published yesterday, Oct 1, and … already has over 100,000 views of the abstract and over 6,000 views of the full text.”
The report details the case of a 76-year-old man with Parkinson’s disease (PD) who died three weeks after receiving his third COVID shot. His first injection was the AstraZeneca jab, received in May 2021, which was followed by two doses of Pfizer in July and December 2021 respectively.
Autopsy confirmed his Parkinson’s diagnosis, but it also revealed several unexpected conditions contributing to his death, including:
|
Aspiration pneumonia |
Systemic arteriosclerosis |
|
Acute vasculitis (vascular inflammation) in both the brain and the heart |
Multifocal necrotizing encephalitis (meaning tissue death all over the brain) |
|
Chronic cardiomyopathy (heart disease), and |
Mild acute lympho-histiocytic myocarditis (a rare form of myocarditis that occurs wen lymphocytes, white blood cells, enter and inflame the heart muscle) |
Testing for SARS-CoV-2 antigens (spike and nucleocapsid proteins) revealed the inflammation was in response to spike protein only, particularly in the endothelial cells of small blood vessels. As noted by the authors:19
“Since no nucleocapsid protein could be detected, the presence of spike protein must be ascribed to vaccination rather than to viral infection. The findings corroborate previous reports of encephalitis and myocarditis caused by gene-based COVID-19 vaccines.”
Irrefutable Evidence the COVID Shots Can Kill
Kirsch goes on to cite other evidence showing the COVID shots can kill, including a report20 titled “On COVID Vaccines: Why They Cannot Work, and Irrefutable Evidence of Their Causative Role in the Deaths After Vaccination,” written by Drs. Sucharit Bhakdi and Arne Burkhardt.
Bhakdi and Burkhardt claim to have developed a way to test for spike protein in human tissue, and say they’ve found spike protein in the tissues of people who have been injured and/or killed by the jabs.
Of the 15 bodies their team examined for this report — all of whom had died seven days to six months post-jab — 14 (93%) were found to have been killed by the COVID shot.21 The video above reviews their findings. All 14 had clear evidence of the body attacking itself, including the heart, with fatal consequences.
Resources for Those Injured by the COVID Jabs
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system. The same goes for anyone who has taken one or more COVID jabs and has had the good fortune of not experiencing debilitating side effects.
Your health may still be impacted long-term, so don’t take any more shots. When it comes to treatment, there are still more questions than answers, but many of the treatments that worked against severe COVID-19 infection also seem to ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
Two doctors who have started tackling the treatment of COVID jab injuries in earnest include Dr. Michelle Perro (DrMichellePerro.com), whom I’ve interviewed on this topic, and Dr. Pierre Kory (DrPierreKory.com).
Both agree that eliminating the spike protein your body is now continuously producing is a primary task. Perro’s preferred remedy for this is hydroxychloroquine, while Kory typically uses ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
As a founding member of the Front Line COVID-19 Critical Care Alliance (FLCCC), Kory helped develop the FLCCC’s post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com22 (hyperlink to the correct page provided above).
Other Helpful Treatments and Remedies
In previous articles, I’ve also covered a number of treatments and remedies that can be helpful for COVID jab injuries, such as:
• Hyperbaric oxygen therapy, especially in cases involving stroke, heart attack, autoimmune diseases and/or neurodegenerative disorders. To learn more, see “Hyperbaric Therapy — A Vastly Underused Treatment Modality.”
• Time-restricted eating — Kory believes there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells naturally, over time. One of the strategies he recommends for this is TRE (time restricted eating), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins. Another strategy that can do the same thing would be sauna therapy.
Most people eat more than 12 hours a day, which is a recipe for metabolic disaster. The ideal window for most everyone is 16 to 18 hours of continuous fasting with the least meal at least three hours before bed. If you are overweight, shoot for 18 hours of fasting each day; if you’re of normal weight, 16 hours.
• Lower your omega-6 intake — Linoleic acid is consumed in amounts 10 times above the ideal in well over 95% of the population, and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. You can review this previous post for more information.
• Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. At 15 to 80 milligrams a day for those suffering from long-haul COVID could go a long way toward resolving some of the fatigue many suffer post-jab. Methylene blue is actually the parent molecule for hydroxychloroquine and has been used to treat malaria since 1890.
It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
• Near-infrared light, as it triggers production of melatonin in your mitochondria23 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,24 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
Dr. Mercola
Source link